Embed Size (px)
Citation preview

British Heart Journal, 1979, 41, 249-252
Corrected transposition of great vessels and Ebstein'sanomaly of tricuspid valveEchocardiographic findings
JAMES G. HENRY, SEYMOUR GORDON, AND GERALD C. TIMMIS
From the Division of Cardiovascular Diseases, William Beaumont Hospital, Royal Oak, Michigan, USA
SUMmARY A case is reported concerning echocardiographic findings in a patient with congenitalcorrected transposition of the great vessels and Ebstein's anomaly of the tricuspid valve. Thispresented an unusual opportunity to study atrioventricular valve closure in a patient in whom theEbstein's malformation involved the systemic atlioventricular valve. The mitral to tricuspid valveclosure interval was 68 milliseconds and represented significant delay in tricuspid valve closure. Thisclosure interval is similar to closure intervals previously reported for patients with Ebstein's anomalywithout ventricular inversion.
Recent echocardiographic studies have detailedthe timing of atrioventricular valve closure inEbstein's anomaly of the tricuspid valve (Kotlerand Tabatznik, 1971; Lundstr6m, 1973; Farookiet al., 1976; Milner et al., 1976). These studiesindicate the diagnostic value of delayed tricuspidclosure. The mechanism of delayed tricuspidclosure is speculative (Lundstr6m, 1973; Milner etal., 1976). The patient described here providedan opportunity to study atrioventricular valveclosure in ventricular inversion (congenital correctedtransposition of the great vessels) and Ebstein'smalformation of the systemic atrioventricular valve.
Case report
A 22-month-old girl was admitted for furthercardiovascular diagnostic studies. A diagnosis ofcorrected transposition of the great vessels andregurgitation of the systemic atrioventricular valvehad been made by cardiac catheterisation andangiocardiography at 3 weeks of age. In the ensuing21 months, she showed slow growth and frequentrespiratory infections. Re-evaluation at 22 monthsrevealed a small, thin, acyanotic toddler in nodistress. There was a hyperdynamic impulse in theleft parasternal area. A pansystolic murmur waspresent at the lower left sternal border and apex. Anapical mid-diastolic murmur was present. Thesecond heart sound was single and accentuated. The
liver was palpable 2 cm below the right costalmargin.An electrocardiogram revealed a QRS duration of
0-10 s (lead II). Slurring of the upstroke of the Rwave was present in leads I, V5, and V6.
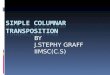
Cardiac catheterisation (Table) disclosed moderatepulmonary arterial hypertension, raised pulmonaryarterial wedge pressures, and a marginally signifi-cant increase in oxygen saturation between systemicvenous and pulmonary arterial blood. Cineangio-cardiography with selective opacification of sys-temic and pulmonary ventricles showed ventricularinversion and 1-transposition of the great vessels.Displacement of the tricuspid valve leaflets distallyinto the sinus of the right ventricle was noted(Fig. 1), producing an angiographic picture pre-viously described in Ebstein's malformation of thetricuspid valve with ventricular inversion (Jaffee,
Table Catheterisation data
Site % Oxygen Pressure (mmHg)- saturation systolic/diastolic
Superior vena cava 64Inferior vena cava 71Right atrium 72 a = 6, v = 5, mean = 3Left ventricle 72 49/5Pulmonary artery 72 51/24 mean = 36Pulmonary capillary 98 a = 24, v - 24, mean = 18Right ventricle 96 78/6Aorta 96 79/53 mean - 67
249
on Novem
ber 6, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.41.2.249 on 1 F
ebruary 1979. Dow
nloaded from

20ames G. Henry, Seymour Gordon, and Gerald C. Timmis
Fig. 1 Anteroposterior projection ofsystemic ventricular cineangiocardiogramn.The ventricle is coarsely trabeculated andhas an infundibulum separating the systemicatrioventricular valve from the aortic valve.The black arrow indicates the atrioventri-cular valve ring. The 3 white arrowsindicate the displaced tricusfid valveleaflet. Note distinct tricuspid regurgitationinto the enlarged left atrium. Ao, aorta;LA, left atrium; RV, anatomical right
d ventricle.
1976). Pronounced tricuspid regurgitation wasobserved.
ECHOCARDIOGRAPHIC TECHNIQUE ANDRESULTSEchocardiographic recordings were performedwith an Ekoline 20 ultrasonoscope and a 3-5 mHz1/4 in transducer. A Cambridge strip chart recorderwas used with 100 mm per second paper speed and40 millisecond time lines.The patient was examined in the supine position.
The atrioventricular valves were identified by theirrelation to semilunar valves as described by Solingeret al. (1974). The posterior, left atrioventricularvalve (tricuspid) was easily recorded in the 3rdand 4th intercostal spaces in a wide area from theleft sternal border to the left midclavicular line. Theanterior, right atrioventricular valve (mitral) wasrecorded only with medial angulation at the lowerleft sternal border.
Atrioventricular valve closure was identified bythe point of coaptation of leaflets, or in the case ofthe tricuspid valve, that instant at which the tworecorded leaflets sharply terminated their rapidapproximation at the onset of systole (Mc and Tc inFigs 2 and 3).The interval between echocardiographic closure
of the mitral and tricuspid valves (McTcI) wasdetermined as follows:The interval between the Q wave of the electro-
cardiogram and mitral closure (Q-Mc) was deter-mined by measurement of the interval to the nearest
5 milliseconds in 5 successive complexes withnearly identical RR intervals and taking the averagevalue. The interval between the Q wave of theelectrocardiogram and tricuspid closure (QTc) wasdetermined in the same manner. McTcI was ob-tained by subtracting mean QMc from mean QTc.Heart rates during recordings for determination ofQMc and QTc were similar, averaging 111 and 114per minute, respectively.The value obtained for McTcI was 68 milli-
seconds.
Discussion
The patient reported here has ventricular andatrioventricular valvular inversion. Thus the pos-terior, systemic atrioventricular valve is tricuspid.In addition, this posterior atrioventricular valve hadthe angiographic appearance of Ebstein's anomaly(Jaffee, 1976).
This case report is of value in two respects:(1) It represents one of the few reported in-
stances of echocardiographic closure of the anterioratrioventricular valve before closure of the posterioratrioventricular valve. To our knowledge thissequence of atrioventricular valve closure has beenreported in only one normal subject (Milner et al.,1976) and has been reported as the usual finding inonly one congenital cardiac defect, classical com-plete transposition of the great vessels (Milner et al.,1976).
250
on Novem
ber 6, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.41.2.249 on 1 F
ebruary 1979. Dow
nloaded from

Echocardiography in corrected transposition with Ebstein's anomaly
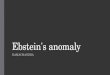
Fig. 2. Mitral valve echoes in corrected transposition of the great vessels. Echo, echo-cardiogram, ECG electrocardiogram; Mc, mitral closure point; q, initiation of Q wave ofthe electrocardiogram.
Fig. 3 Tricuspid valve echoes in corrected transposition of the great vessels. Echo, echocardiogram; EGG, electrocardiogram; Phono, phonocardiogram; q, initiation of Q wave ofthe electrocardiogram; Tc, tricuspid closure point; TV, tricuspid valve echoes.
251
OW -Z"R
on Novem
ber 6, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.41.2.249 on 1 F
ebruary 1979. Dow
nloaded from

James G. Henry, Seymour Gordon, and Gerald C. Timmis
(2) Delayed tricuspid valve closure was demon-strated echocardiographically in this patient withventricular (and therefore atrioventricular valvular)inversion and Ebstein's anomaly of the tricuspidvalve. The delay in tricuspid valve closure expressedas the McTc interval was 68 milliseconds and is inthe range reported for Ebstein's anomaly withoutventricular inversion (Kotler and Tabatznik, 1971;Lundstr6m, 1973; Farooki et al., 1976; Milner et
al., 1976). Thus delayed tricuspid valve closure isapparently a feature of Ebstein's malformation ofthe tricuspid valve in ventricular inversion as wellas in ventricular noninversion.
Further echocardiographic studies in patientswith and without Ebstein's malformation, ventricu-lar inversion, and great vessel malformations will berequired to, test the diagnostic value of the observa-tions cited in this case report.
References
Farooki, Z., Henry, J., and Green, E. (1976). Echocardio-graphic spectrum of Ebstein's anomaly of the tricuspidvalve. Circulation, 53, 63-68.
Jaffee, R. (1976). Systemic atrioventricular valve regurgitationin corrected transposition of the great vessels. Angiographicdifferentiation of operable and nonoperable valve deformi-ties. American Journal of Cardiology, 37, 395-402.
Kotler, M., and Tabatznik, B. (1971). Recognition of Ebstein'sanomaly by ultrasound technique (abstract). Circulation, 43and 44, Suppl. II, 34.
Lundstrom, N-R. (1973). Echocardiography in the diagnosisof Ebstein's anomaly of the tricuspid valve. Circulation, 47,597-605.
Milner, S., Meyer, R., Venables, A., Korfhagen, J., andKaplan, S. (1976). Mitral and tricuspid valve closure incongenital heart disease. Circulation, 53, 513-518.
Solinger, R., Elbl, F., and Minhas, K. (1974). Deductiveechocardiographic analysis in infants with congenital heartdisease. Circulation, 50, 1072-1096.
Requests for reprints to Dr James G. Henry,William Beaumont Hospital, 3601 W. ThirteenMile Road, Royal Oak, Michigan 48072, USA.
252
on Novem
ber 6, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.41.2.249 on 1 F
ebruary 1979. Dow
nloaded from