Embed Size (px)
Citation preview

1077
Case Series
Coronally Advanced Flap Procedure for Root Coverage. Is Flap Thickness a Relevant Predictor to Achieve RootCoverage? A 19-Case SeriesCarlo Baldi,* Giovanpaolo Pini-Prato,† Umberto Pagliaro,‡ Michele Nieri,§ Daniele Saletta,§
Leonardo Muzzi,‖ and Pierpaolo Cortellini¶
This clinical study was designed to determinewhether the thickness of the flap can influence rootcoverage when gingival recessions associated withtraumatic toothbrushing are treated using a coro-nally advanced flap (CAF). Nineteen patients, agedfrom 25 to 57 years, with high levels of oral hygiene(full-mouth plaque scores <20%) were selected for thestudy. Each patient contributed with one Miller ClassI or II maxillary or mandibular recession. A total of 19recessions ≥2 mm were treated. After local anesthesiaand before flap elevation, the exposed root surfacewas planed with a sharp curet. A trapezoidal full-and partial-thickness flap was then elevated, dis-placed coronally, and sutured to cover the treatedroot surface. Before suturing, flap thickness was mea-sured in the alveolar mucosa with a gauge. Aftersurgery, all patients were recalled for control and pro-fessional prophylaxis once a week during the firstmonth and monthly up to the third month. The meaninitial recession depth was 3.0 ± 0.9 mm. Mean flapthickness (FT) was 0.7 ± 0.2 mm. Three months later,mean recession depth was 0.6 ± 0.6 (P <0.0001) andmean recession reduction was 2.4 ± 0.7 mm. Meanroot coverage was 82 ± 17%. Flap thickness >0.8 mmwas associated with 100% of root coverage. Theresults of this study indicate that there is a direct rela-tion between flap thickness and recession reduction(P <0.0001). J Periodontol 1999;70:1077-1084.
KEY WORDS Gingival recession/surgery; surgical flaps; toothroot/surgery; toothbrushing/adverse effects.
Root coverage procedures, free grafts or pedicleflaps, are successful if the grafted tissues survive onthe exposed surface. The survival of grafted tissues iscritical on the avascular root surface. Vascularizationof grafted tissues plays an important role in the heal-ing process of these surgical procedures. Human1
and animal2 studies investigated the alteration of gin-gival circulation and revascularization following pedi-cle flaps during the healing period. Mörmann andCiancio1 published a fluorescein angiographic clinicalstudy which investigated the change in circulationfollowing different surgical incisions or flaps both inthe gingiva and in the alveolar mucosa of severalpatients. They stated that, in order to assure the sur-vival of the pedicle flap, more blood vessels must beincluded in the grafted soft tissues.
Caffesse et al.2 studied revascularization followingthe lateral sliding flap procedure on 2 rhesus mon-keys. The reestablished vascular network wasrelated to the vessel’s patency in the pedicle flapand to the formation of anastomoses at the surgicalinterface between the capillaries of the flap and thecapillaries from the connective tissue, bone, andperiodontal ligament of the recipient area.
The main blood supply of the gingiva is directedcaudo-cranially from the vestibule to the gingivalmargin. It is mainly derived from the supraperiostealblood vessels which, in the free gingiva, anastomosewith blood vessels; from the alveolar bone; and theperiodontal ligament.3 Blood supply of the alveolarmucosa mainly derives from supraperiosteal vessels.
The surgical execution of a coronally advancedflap procedure (CAF)4-8 for root coverage requiresan intrasulcular incision and 2 vertical releasing inci-sions to raise a full-thickness gingival flap up to themucogingival junction; a partial-thickness flap, api-cal to the mucogingival junction, obtained by a hori-zontal incision to separate the flap from theunderlying periosteum and a mesio-distal and apicaldissection under the alveolar mucosa to facilitatemobility, and the coronal displacement of the flap.
These surgical incisions could impair blood supplyto the flap and the coronal displacement of the flapand sutures could stretch the residual vessels. To
J Periodontol • September 1999
* Private practice, Prato, Italy.† Dental School, University of Florence, Florence, Italy.‡ Private practice, Campi Bisenzio, Italy.§ Private practice, Florence, Italy.‖ Department of Periodontology, University of Siena, Siena, Italy.¶ School of Dental Medicine, University of Bern, Switzerland.
PD7009/8240 6/30/00 11:11 AM Page 1077

1078
minimize these circulatory alterations Mörmann andCiancio1 suggest that: “1. Flaps should be broadenough at their base to include major gingival vessels.2. A flap’s length to width ratio should not exceed2�1. 3. Minimal tension should be produced by sutur-ing. 4. Partial-thickness flap preparations to coveravascular areas should not be too thin so that moreblood vessels are included in them. 5. The apical por-tion of periodontal flaps should be full thickness whenpossible.” In order to increase the vascularization ofthe base of the flap, Pini Prato et al.9 proposed atrapezoidal full-partial thickness flap when using CAFin combination with guided tissue regeneration proce-dures to treat gingival recessions. As reported byAllen, the large base of the flap, obtained by perform-ing 2 oblique and divergent releasing incisions, guar-antees a greater vascularization of the flap.10
In a comparative clinical study on the treatment ofmolar degrees 1 or 2 facial furcation involvementswith barrier membranes, Anderegg et al.11 measuredthe thickness of the mucoperiosteal flaps to evaluatewhether the thickness of the tissue used to cover themembrane might influence the development of reces-sion during healing. They noted that in sites where themembrane was covered with thin soft tissues (<1 mm)recession occurred with greater frequency than sitescovered with thicker tissues (>1 mm). They concludedthat “it is not unreasonable to consider that thin flapsare at greater risk than thick flaps for ischemia andnecrosis.”
So far, there is no evidence demonstrating a rela-tionship between the thickness of the flap and theamount of root coverage after mucogingival surgery.
The aim of the present clinical study is to deter-mine if the thickness of flap can influence the reces-sion reduction following coronally advanced flap(CAF) surgery.
MATERIALS AND METHODSStudy PopulationNineteen patients, 6 males and 13 females, agedbetween 25 and 57 years (mean age 32.0 ± 7.8), 5of whom were smokers, with 16 maxillary and 3mandibular recessions, were treated with coronallyadvanced flap between January and December1996. Each patient contributed with one recession.The patients were selected from individuals referredto the Department of Periodontology of the Uni-versity of Siena Dental School. The patients agreedto participate in the study and signed an appropriateconsent form in agreement with the HelsinkiDeclaration on human experimentation.
The entry criteria were: 1) non-compromised sys-temic health and no contraindications for periodontal
surgery; 2) presence of maxillary or mandibular iso-lated buccal recessions (≥2 mm) classified as MillerClass I or II;12 3) presence of identifiable cemento-enamel junction (CEJ); 4) presence of tooth vitalityand absence of restorations and superficial caries inthe area to be treated; 5) no periodontal surgicaltreatment in the previous 24 months on the involvedsites; 6) full-mouth plaque score (FMPS)13 <20% andfull-mouth bleeding score (FMBS)14 <20%; and 7)absence of plaque and bleeding on probing at thesurgical site.
All patients received oral hygiene instructions to eliminate habits related to the etiology of therecession.
The 16 maxillary recessions were located on 5 pre-molars, 7 canines, 1 lateral and 3 central incisors,while the 3 mandibular recessions were located on 1 canine and 2 lateral incisors.
Surgical ProceduresAll surgical procedures were performed by a singleoperator with more than 10 years of periodontalexperience.
After local anesthesia (lydocain with adrenaline andnoradrenaline 1:50.000) and before the elevation ofthe flap, both the exposed and the intrasulcular rootsurfaces were gently planed with sharp Gracey 7-8curets# to reduce root convexity. Immediately after,the root surface was washed for 60 seconds withwater spray. An intrasulcular incision was then madewith a blade# on the buccal aspect of the involvedtooth. This incision was horizontally extended to theadjacent papillae avoiding the gingival margin of theadjacent teeth. Two oblique releasing incisions werecarried out from the mesial and distal extremities ofthe horizontal incision beyond the mucogingival junc-tion. A trapezoidal full-thickness flap was raised up,with a periosteal elevator,# towards the mucogingivaljunction. Then a partial-thickness dissection was car-ried out apically towards the marginal bone crest leav-ing the underlying periosteum in place. In addition amesio-distal and apical dissection parallel to thevestibular lining mucosa was performed with a bladeto release residual muscle tension and to facilitate thepassive coronal displacement of the flap. At thismoment the thickness of the flap was measured byanother operator with a modified Iwansson gauge atthe mid-point of the distance between the mucogingi-val junction (MGJ) and the base of the flap (see datacollection). The Iwansson gauge was modified, elimi-nating the spring, to avoid an excessive pressure onthe soft tissue. The papillae adjacent to the involved
Case Series
Flap Thickness in Root Coverage Treatment Volume 70 • Number 9
# Hu-Friedy, Chicago, IL.
PD7009/8240 6/30/00 11:11 AM Page 1078

1079
Case Series
J Periodontol • September 1999 Baldi, Pini-Prato, Pagliaro, et al.
Figure 1.(a) Base of the flap (FB); length of the flap (FL); and gingival margin(GM). (b) Thickness of the flap (FT).
tooth were de-epithelialized. The flap was then coro-nally displaced and adapted to cover the CEJ.
Suturing of oblique releasing incisions was per-formed, with 5-0 silk sutures, as described by Allenand Miller,4 while the coronal mesial and distalextremities of the flap were secured by 2 singlesutures placed in the interdental areas. Additionalinterrupted sutures were applied, when necessary, toclose the oblique releasing incisions in the alveolarmucosa. No periodontal dressing was applied.
Postsurgical CareImmediately following surgery, use of ice packs wasrecommended for 3 hours. All patients wereinstructed to discontinue toothbrushing, avoidtrauma around the surgical site, and reduce smok-ing. In case of pain, the use of nimesulide (100 mgtwice daily) was recommended. A 0.12% chlorhexi-dine digluconate solution rinse was prescribed 4times (60 seconds) daily for the first 10 days.
The sutures were removed after 10 days. Thepatients were instructed to clean the surgical siteswith a cotton pellet soaked in a 0.12% chlorhexidinedigluconate solution 4 times daily for 10 days.
Three weeks after surgery, the patients wereinstructed to resume mechanical tooth cleaning ofthe treated areas using a soft toothbrush and a care-ful roll technique.
The patients were recalled for control and prophy-laxis after 1, 2, 3, and 4 weeks, and at 2 and 3 months.
Data CollectionAll measures were recorded by the same calibratedinvestigator, with more than 10 years of periodontalexperience, using a UNC 15 periodontal probe# and3× magnification lens. The measurements recordedwith the periodontal probe were rounded to thenearest 0.5 mm.
Before surgery (baseline) the following data werecollected at the mid-buccal point of the involvedtooth: recession depth (Rec): the distance betweenCEJ and the gingival margin (GM); probing depth(PD): the distance between GM and the bottom ofthe pocket; clinical attachment level (CAL): the dis-tance between CEJ and bottom of the pocket; andwidth of keratinized tissue (KT): the distancebetween GM and the mucogingival junction (MGJ).
During surgery, after the execution of the 2oblique releasing incisions and before the elevationof the flap, the following data were recorded (Fig. 1):flap base (FB): the distance between the apicalextremities of the two releasing incisions; and flaplength (FL): the distance between GM and FB at thedeepest point of the recession.
During surgery, after the elevation of the flap, flapthickness (FT) (Fig. 1) was measured at the mid-pointof the distance between the MGJ and FB by means ofa modified Iwansson gauge (Fig. 2).
At 1, 2, 3 and 4 weeks and 2 and 3 months post-surgery, Rec and KT were collected at the same mid-buccal point of the involved tooth.
At 3 months, PD and CAL were recorded.
Statistical AnalysisQuantitative data were summarized as mean ± stan-dard deviation. Differences between baseline and
PD7009/8240 6/30/00 11:11 AM Page 1079
3-month recession were analyzed by means ofStudent t test for paired observations.
Multiple linear regression was performed usingrecession reduction as the outcome variable and thethickness of the flap and initial recession as theindependent variables.
Model diagnostics included analysis of standard-ized residual, partial regression leverage plot,search of X outliers and Y outliers. The significanceof the contribution of each factor to the model wereassessed using computer software.**
RESULTSNineteen patients showing 19 Miller Class I or II gin-gival recessions were treated by means of CAFsurgery. Results are reported in Table 1.
At baseline the mean recession depth was 3.0 ±0.9 mm (range 2 to 5.5 mm), the mean KT widthwas 2.9 ± 1.2 mm, the mean PD was 1.2 ± 0.4 mm,and the mean CAL was 4.2 ± 1.0 mm.
At time of surgery the mean FB was 13.3 ±1.8 mm and the mean FL was 7.6 ± 0.9 mm. Flap’sbase to length ratio mean was 1.8 ± 0.3 mm. Themean FT was 0.7 ± 0.2 mm (range 0.4 to 1.1 mm).Eleven cases showed a flap thickness <0.8 mm, 8 cases ≥0.8 mm.
Three months after surgery the mean recessiondepth was 0.6 ± 0.6 mm. The difference betweenbaseline and 3 months recession depth was 2.4 ±0.7 mm (P <0.0001). Mean root coverage was 82 ±17%. Seven teeth (37%) showed complete root cover-age. Mean KT width was 2.7 ± 1.1 mm and mean KTdifference was −0.2 ± 0.8 mm (P = n.s.). Mean PD was0.8 ± 0.3 mm and the mean PD difference was 0.4 ±0.5 mm (P = 0.0053). Mean CAL was 1.4 ±0.6 mm and mean CAL reduction was 2.8 ±0.8 mm (P <0.0001).
Multiple linear regres-sion showed a significantassociation between re-cession reduction andboth the thickness of theflap (P <0.0001) and theinitial recession depth (P<0.0001) (Fig. 3 andTable 2).
All the sites with flapthickness greater than 0.8 mm showed completeroot coverage (Fig. 4);the sites with flap thick-ness less than 0.8 mm
Table 1.
Mean (±SD) Measurements (mm) and Differences (19 patients)
Measurement Baseline 3 Months Difference
Recession depth 3.0 ± 0.9 (2.0-5.5) 0.6 ± 0.6* (0.0-1.5) 2.4 ± 0.7*Keratinized tissue width 2.9 ± 1.2 (1.0-5.0) 2.7 ± 1.1 (1.0-4.5) −0.2 ± 0.8Probing depth 1.2 ± 0.4 (0.5-2.0) 0.8 ± 0.3* (0.5-1.5) 0.4 ± 0.5*Clinical attachment level 4.2 ± 1.0 (3.0-7.5) 1.4 ± 0.6* (0.5-2.5) 2.8 ± 0.8*Flap base 13.3 ± 1.8 (10.0-16.0)Flap length 7.6 ± 0.9 (5.0-9.0)Flap base/flap length ratio 1.8 ± 0.3 (1.2-2.4)Flap thickness 0.7 ± 0.2 (0.4-1.1)
* Significant difference from baseline (P <0.05).
Flap Thickness in Root Coverage Treatment Volume 70 • Number 91080
Case Series
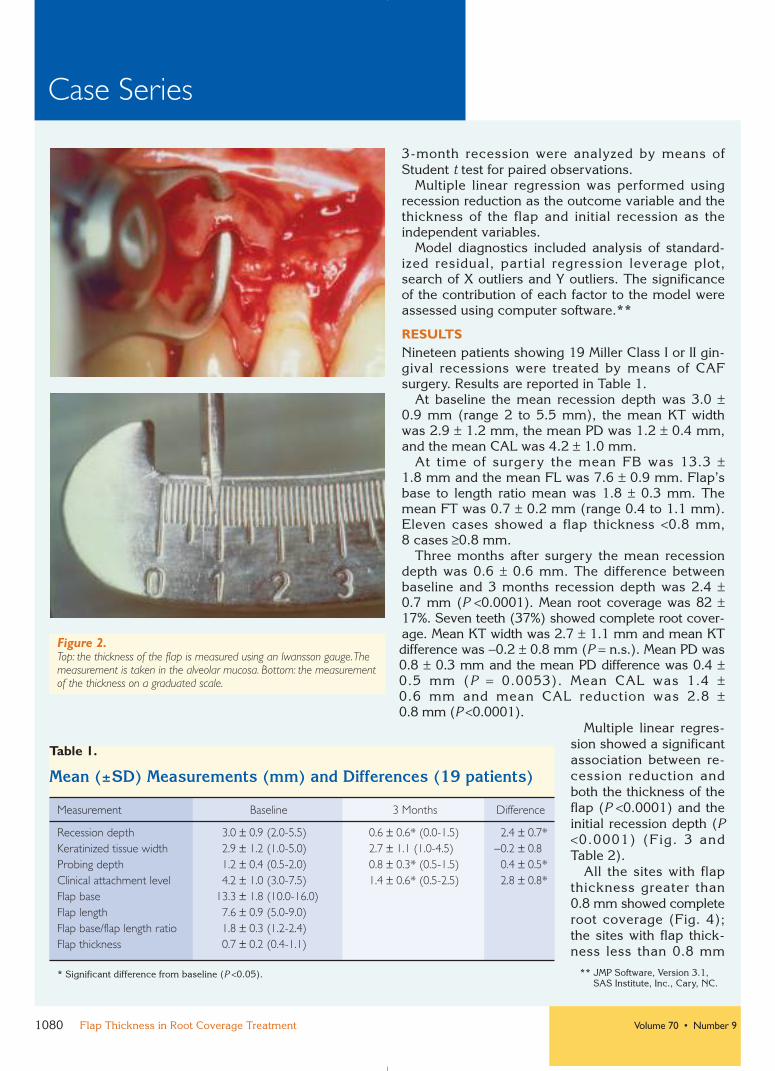
Figure 2.Top: the thickness of the flap is measured using an Iwansson gauge.Themeasurement is taken in the alveolar mucosa. Bottom: the measurementof the thickness on a graduated scale.
** JMP Software, Version 3.1,SAS Institute, Inc., Cary, NC.
PD7009/8240 6/30/00 11:11 AM Page 1080

1081
Case Series
J Periodontol • September 1999 Baldi, Pini-Prato, Pagliaro, et al.
Figure 3.Partial regression leverage plot for flap thickness (FT).The linearrelationship between recession reduction (RecRed) and FT is shownwhen the other regressor (recession at baseline) is used.The dottedlines represent 95% confidence interval of the regression line.
Figure 4.Recession (2.5 mm) on maxillary central incisor (upper left). Flap thickness is 1 mm (upper right). After suturing (lower left).100% of root coverage 3 months later (lower right).
Table 2.
Multiple Linear Regression Analysis forRecession Reduction (Rec Red)
Parameter Estimates Estimate Standard Error Significance
b0 (Intercept) −1.09 0.32 0.0037b1 (Rec) 0.72 0.07 <0.0001b2 (FT) 1.90 0.29 <0.0001
Model Rec Red = β0 + β1 Rec + β2 FTR2 = 0.89
showed partial root coverage (Fig. 5). Two out of 3sites with flap thickness equal to 0.8 mm showed com-plete root coverage.
The percentage of root coverage of all sitesrelated to flap thickness is reported in Figure 6.
DISCUSSIONThe aim of the present study was to determine if thethickness of the flap could influence the clinicalresults in terms of recession reduction with a coro-nally advanced flap (CAF).
PD7009/8240 6/30/00 11:11 AM Page 1081

1082
The surgical design to raise a CAF includes 3 mainincisions: 1) an intrasulcular incision interrupts thecrestal and periodontal ligament vessels; 2) the verti-cal releasing incisions reduce the vascularization ofthe flap laterally; and 3) a further reduction of theresidual blood supply is determined by the surgicalincisions executed to separate the flap from the under-lying periosteum. The latter influences the thickness ofthe flap. Therefore, the designed full-(gingiva)/partial-(alveolar mucosa) thickness flap is mainly vascular-ized by supraperiosteal vessels which come from thebase of the flap in the caudo-cranial direction.
This residual vascular system is of fundamentalimportance in determining the survival of the flapand particularly of the marginal gingiva, which is thefarthest area of the flap from the base of the pedicle.After the surgical procedure the gingiva is posi-tioned on the avascular root surface and receives asmaller amount of blood supply because of thecaudo-cranial pattern of vascularization. The thickerthe flap, the greater the vascularization of the mar-ginal gingiva.
In the present study, the thickness of the flap wasmeasured at the alveolar mucosa in order to evalu-ate whether its increased thickness, presumablyassociated with greater vascularization, couldimprove the outcome of CAF.
The results of the present study indicate that flapthickness is significantly (P <0.0001) associated withroot coverage of shallow recessions.
A linear regression analysis (Fig. 3 and Table 2)shows that both initial recession and thickness of theflap are important predictive variables for recessionreduction (R2 = 0.89). Based on this model andusing initial recession as a covariate, with eachincrement in thickness of 0.1 mm, recession wasreduced by approximately 0.2 mm (b2 = 1.90) in the19 treated sites.
In this study, flap thickness >0.8 mm was associ-ated with complete root coverage and flap thickness<0.8 mm was associated with partial root coverage,0.8 mm can be considered as the critical flap thick-ness above which the expected clinical outcome iscomplete root coverage (Fig. 6). The limited sample
Case Series
Flap Thickness in Root Coverage Treatment Volume 70 • Number 9
Figure 5.Recession (3.5 mm) on maxillary first premolar (upper left). Flap thickness is 0.6 mm (upper right). After suturing (lower left).57% of root coverage 3 months later (lower right).
PD7009/8240 6/30/00 11:11 AM Page 1082

1083
Case Series
J Periodontol • September 1999 Baldi, Pini-Prato, Pagliaro, et al.
Figure 6.Percent of root coverage and flap thickness of all (19) treated recessions. Cases with a flap thickness >0.8 mm achieved 100% root coverage.
size of our study does not allow us to draw definitiveconclusions and studies with a larger number ofcases should be undertaken.
When considering results in terms of recessionreduction, this study showed a mean recessionreduction of 2.4 ± 0.7 mm and mean root coverageof 82% after 3 months. These results are concordantwith those in literature4-8 in which the percentage ofroot coverage ranges from 60%7 to 99%.5
These interesting results were obtained using atrapezoidal full-partial thickness flap with a largebase.9 This surgical procedure allows an increase ofthe flap base/flap length ratio (FB/FL), which in thepresent study was approximately 2:1. A high FB/FLratio is expected to improve both flap vascularizationand survival of the grafted tissues.1
All patients were satisfied with their estheticappearance.
In conclusion, the present study indicates that: 1) flap thickness is a significant predictor (P <0.0001)of the clinical outcome of root coverage and recessionreduction for shallow gingival recessions treated bythe coronally advanced flap (CAF) procedure; and 2) the shallow probing depths and the CAL gain after3 months confirm that CAF is a predictable surgicaltechnique for treatment of gingival recessions.
ACKNOWLEDGMENTSThe authors would like to acknowledge Dr. LisaWiechmann for her help in the preparation of thismanuscript.
PD7009/8240 6/30/00 11:11 AM Page 1083

1084
REFERENCES1. Mörmann W, Ciancio SG. Blood supply of human
gingiva following periodontal surgery. A fluoresceinangiographic study. J Periodontol 1977;48:681-692.
2. Caffesse RG, Kon S, Castelli WA, Nasjleti CE.Revascularization following the lateral sliding flapprocedure. J Periodontol 1984;55:352-359.
3. Lindhe J, Karring T. Anatomy of the periodontium. In:Lindhe J, Karring T, Lang NP, eds. Clinical Perio-dontology and Implant Dentistry, 3rd ed. Copenhagen:Munksgaard; 1997:19-68.
4. Allen EP, Miller PD. Coronal positioning of existinggingiva: Short-term results in the treatment of shallowmarginal tissue recession. J Periodontol 1989;60:316-319.
5. Harris RJ, Harris AW. The coronally positioned pediclegraft with inlaid margins: A predictable method toobtaining root coverage of shallow defects. Int JPeriodontics Restorative Dent 1994;14:229-241.
6. Wennström JL, Zucchelli G. Increased gingivaldimensions. A significant factor for successful outcomeof root coverage procedures? A 2-year prospectiveclinical study. J Clin Periodontol 1996;23:770-777.
7. Trombelli L, Scabbia A, Wikesjö UME, Calura G. Fibringlue application in conjunction with tetracycline rootconditioning and coronally positioned flap procedure inthe treatment of human gingival recession defects. J Clin Periodontol 1996;23:861-867.
8. Trombelli L, Tatakis DN, Scabbia A, Zimmerman GJ.Comparison of mucogingival changes followingtreatment with coronally positioned flap and guidedtissue regeneration procedures. Int J PeriodonticsRestorative Dent 1997;17:449-455.
9. Pini Prato G, Tinti C, Vincenzi G, Magnani C, CortelliniP, Clauser C. Guided tissue regeneration versusmucogingival surgery in the treatment of human buccalgingival recession. J Periodontol 1992;63:919-928.
10. Allen EP. Use of mucogingival surgical procedure to enhance esthetic. Dent Clin North Am 1988;32:307-330.
11. Anderegg CR, Metzler DG, Nicoll BK. Gingiva thick-ness in guided tissue regeneration and associatedrecession at facial furcation defects. J Periodontol1995;66:397-402.
12. Miller PD. A classification of marginal tissue recession.Int J Periodontics Restorative Dent 1985;5(2):9-13.
13. O’Leary TJ, Drake RB, Naylor JE. The plaque controlrecord. J Periodontol 1972;43:38-42.
14. Ainamo J, Bay I. Problems and proposals for recordinggingivitis and plaque. Int Dent J 1975;25:229-235.
Send reprint requests to: Dr. Giovanpaolo Pini-Prato, VialeMatteotti, 11, 50121 Florence, Italy. Fax: 39 55 572881;e-mail: [email protected]
Accepted for publication January 23, 1999.
Case Series
Flap Thickness in Root Coverage Treatment Volume 70 • Number 9
PD7009/8240 6/30/00 11:11 AM Page 1084









![SWISS INSTRUMENTS PM - Utrecht Dental · Diamond-tipped perio instruments for in-depth root debridement using direct vision [>“Flap”] – for smoothing restoration overhangs as](https://img.dokumen.tips/doc/110x75/5f512c2d8187f67f49776edb/swiss-instruments-pm-utrecht-dental-diamond-tipped-perio-instruments-for-in-depth.jpg)



















