Embed Size (px)
Citation preview

1
Corneal Optical Regularization and Biomechanical Stabilization in
Keratoconus and Irregular Astigmatism by Use of Topography-Guided
Custom Ablation and Corneal Cross-Linking
Xiangjun Chen, MD
Aleksandar Stojanovic, MD
A Doctor of Philosophy (Ph.D) thesis
University of Oslo, SynsLaser Kirurgi,
Norway
June 2016

© Aleksandar Stojanovic and Xiangjun Chen, 2017
Series of dissertations submitted to the Faculty of Medicine, University of Oslo
ISBN 978-82-8333-356-5
All rights reserved. No part of this publication may be reproduced or transmitted, in any form or by any means, without permission.
Cover: Hanne Baadsgaard Utigard. Print production: Reprosentralen, University of Oslo.

Corneal Optical Regularization and Biomechanical Stabilization in
Keratoconus and Irregular Astigmatism by Use of Topography-Guided
Custom Ablation and Corneal Cross-Linking
CONTENTS
1. ACKNOWLEDGEMENTS 7
2. ABBREVIATIONS 9
3. LIST OF PAPERS 11
4. LIST OF FIGURES AND TABLES 13
4.1 Figures 13
4.2 Tables 14
5. GENERAL INTRODUCTION 15
5.1 The Ocular Surface 15
5.1.1 Structure and Function 15
5.1.2 The Cornea 16
5.1.2.1 Structure and function 16
5.1.2.2 The epithelium 17
5.1.2.3 Bowman´s membrane 19
5.1.2.4 The stroma 19
5.1.2.5 Descemet´s membrane 20
5.1.2.6 The endothelium 20
5.1.2.7 Dua´s layer 20
5.2 Corneal Biomechanics 21
5.3 Corneal Optics 22
5.3.1 Eye Optics 22
5.3.1.1 Refractive components and accommodation 22
5.3.1.2 Myopia 23
5.3.1.3 Hyperopia 23
5.3.1.4 Astigmatism 23
5.3.2 Corneal Optics 24
5.3.3 Irregular Astigmatism 24

4
5.3.4 Treatment of Irregular Astigmatism 25
5.4 Diagnostics- Assessment of Various Technologies for Measurement and Analysis of
Corneal Optical Properties and Morphology 27
5.4.1 Wavefront Aberrometry 27
5.4.2 Corneal Topography and Imaging 28
5.4.2.1 Placido-based corneal topography 28
5.4.2.2 Elevation-based corneal topography 28
5.4.2.3 Interpretation of corneal topographic maps 29
5.4.2.4 Topography in keratoconus 30
5.4.3 OCT and OCT-based topography 32
5.4.4 In Vivo Confocal Microscopy 33
5.4.5 Corneal Biomechanical Measurements 34
5.5 Keratoconus 42
5.5.1 Definition, Etiology and Epidemiology 42
5.5.2 Pathogenesis 43
5.5.2.1 Biochemical and inflammatory factors 43
5.5.2.2 Structural and compositional changes 44
5.5.3 Staging 45
5.5.3.1 Classic clinical diagnosis and staging 45
5.5.3.2 Modern imaging methods 46
5.6 Interventions- Treatment of Refractive Errors and Keratoconus 47
5.6.1 Corneal Laser Refractive Surgery 47
5.6.1.1 Overview and history 47
5.6.1.2 Types of excimer laser ablation design 48
5.6.1.3 Surgical techniques 49
5.6.2 Treatment of Keratoconus 57
5.6.2.1 Conservative treatment 57
5.6.2.2 Surgical options 58
5.6.3 CXL in Combination with Excimer Laser Custom Ablation 66
6. AIMS OF THE PRESENT STUDY 69
6.1 Overall Aims of the Study 69
6.2 Aims of the Individual Studies 69
7. MATERIALS AND METHODS 71
7.1 Patients 71

5
7.2 Surgical Techniques 71
7.2.1 Transepithelial Topography-Guided Custom Ablation 71
7.2.2 Epithelium-On Corneal Collagen Cross-Linking 72
7.2.3 Combined Topography-Guided Transepithelial Custom Ablation and Corneal Collagen
Cross-Linking 74
7.3 Clinical Measurements 74
7.3.1 General Ophthalmologic Evaluation 75
7.3.2 Corneal Epithelial and Stromal Thickness Profile Measurements 75
7.3.3 Corneal Dynamic Scheimpflug Analyzer Measurements 75
7.4 Data Analysis 76
7.4.1 Visual Acuity Analysis 76
7.4.2 Vector Analysis 76
7.4.3 Statistical Analysis 77
8. SUMMARY OF RESULTS 79
8.1 Paper I 79
8.2 Paper II 79
8.3 Paper III 79
8.4 Paper IV 80
8.5 Paper V 80
8.6 Paper VI 81
8.7 Paper VII 82
8.8 Paper VIII 82
8.9 Paper IX 83
9. GENERAL DISCUSSION 84
9.1 Rationale for Transepithelial Topography-Guided Custom Ablation in Treatment of
Irregular Astigmatism 84
9.1.1 Custom Ablation 84
9.1.1.1 Aspheric ablation profile 84
9.1.1.2 Topography-guided custom ablation 86
9.1.1.3 Epithelial remodelling 88
9.1.1.4 Transepithelial TGCA 92
9.2 Effect of Transepithelial TGCA in the Treatment of Irregular Astigmatism 99
9.3 Combined Treatment of Transepithelial TGCA and CXL in Treatment of the Keratoconus
99

6
9.3.1 Corneal Biomechanics in Virgin and Post-PRK Eyes 99
9.3.2 CXL in Treatment of Keratectasia 102
9.3.3 Combination of Transepithelial TGCA and CXL in Treatment of Keratectasia 105
9.4 Ethics 107
10. FUTURE PERSPECTIVES 107
10.1 Corneal Biomechanical Property Measurement with the CorVis ST 107
10.2 Stromal Surface Topography-Guided Custom Ablation 107
11. CONCLUSIONS 107
11.1 General conclusion 107
11.2 Conclusions of the individual papers 108
12. ERRATA 110
13. REFERENCES 111
14. PAPERS 146

7
1. ACKNOWLEDGEMENTS
We would like to acknowledge all the direct and indirect participants in this PhD project and
to express our sincere gratitude to them. The names below represent those who we are
thankful the most.
Our sincere thanks go to Amund Ringvold and Tor Påske Utheim, who have been the source
of inspiration for this endeavor through their positive reinforcement and support. Amund
encouraged the start of this PhD-project and Tor became our main supervisor. Tor’s
extraordinary ability to spread his urge for scientific knowledge made the collaboration with
him an invaluable and wonderful experience.
Qinmei Wang and Shihao Chen from Wenzhou Medical University in China were our
dedicated research partners, while their chosen master degree students in ophthalmology,
Ling Wang, Jia Zhang, Linyan Zheng, Lili Zhao, Yanjun Hua, Tao Jiang, Wen Zhou, Ting
Zhang, Nan Jin, Jingting Wang, Di Hu, Yang Zhou, Yanhua Liu, Xiaorui Wang, and Jing
Liang, who have been spending their refractive surgery rotation at SynsLaser clinic from 2006
on, contributed enormously in data collection and data analysis for all the studies used in this
project.
Terje Christoffersen from the eye department of the University Hospital North Norway
contributed his continuous support in making the clinical studies connected with the
department possible.
Tore Nitter was always there to borrow us his extraordinary scientific mind, never hesitating
to take on any scientific challenge. Jon Roger Eidet has been helpful in revision of the
manuscripts and offering useful suggestions during our PhD study.
We also thank Borghild Roald, the co-supervisor of the PhD-project for her generous support.

8
Xiangjun Chen and Aleksandar Stojanovic
University of Oslo, SynsLaser Kirurgi,
Oslo, Norway
2016

9
2. ABBREVIATIONS
AL Axial length
AS-OCT Anterior segment optical coherence tomography
BAC Benzalkonium chloride
CA Custom ablation
CDVA Corrected distance visual acuity
CH Corneal hysteresis
CK Conductive keratoplasty
CRF Corneal resistance factor
CorVis ST Corneal visualization Scheimpflug technology
CXL Corneal collagen crosslinking
D Diopter
DA Deformation amplitude
FLEX Femtosecond lenticule extraction
FS Femtosecond
FS-LASIK Femtosecond laser assisted-laser in situ keratomileusis
HOAs Higher-order aberrations
IA Irregular astigmatism
ICC Intraclass correlation coefficient
ICRS Intrastromal corneal ring segments
IOP Intraocular pressure
IOPg Goldmann-correlated IOP
10
IOPcc Corneal compensated IOP
IVCM In vivo confocal microscopy
LASIK Laser in situ keratomileusis
LASEK Laser-assisted subepithelial keratectomy
LogMAR Logarithm of the minimum angle of resolution
LOAs Lower-order aberrations
MMC Mitomycin-C
ORA Ocular response analyzer
PIOL Phakic intraocular lenses
PRK Photorefractive keratectomy
ReLEx Refractive lenticule extraction
RGP Rigid gas permeable lens
RMS Root mean square
SD Standard deviation
SE Spherical equivalent
SimK Simulated keratometry
SMILE Small incision lenticule extraction
TGCA Topography-guided custom ablation
T-PTK Transepithelial phototherapeutic keratectomy
UDVA Uncorrected distance visual acuity

11
3. LIST OF PAPERS
I. A Stojanovic, L Wang, MR Jankov, TA Nitter, Q Wang.
Wavefront optimized versus custom-Q treatments in surface ablation for myopic
astigmatism with the WaveLight Allegretto Laser.
J Refract Surg. 2008 Oct;24(8):779-89.
II. X Chen, A Stojanovic, Y Liu, Y Chen, Y Zhou, TP Utheim
Postoperative changes in corneal epithelial and stromal thickness profiles after
photorefractive keratectomy in treatment of myopia.
J Refract Surg. 2015 Jul;31(7):446-53. doi: 10.3928/1081597X-20150623-02.
III. X Chen, A Stojanovic, X Wang, J Liang, D Hu, TP Utheim.
Epithelial Thickness Profile Change after Combined Topography-guided
Transepithelial Photorefractive Keratectomy and Corneal Crosslinking in Treatment of
Keratoconus
J Refract Surg. (accepted for publication)
IV. A Stojanovic, S Chen, X Chen, F Stojanovic, J Zhang, T Zhang, TP Utheim.
One-step transepithelial topography-guided ablation in the treatment of myopic
astigmatism
PLoS One. 2013 Jun 17;8(6):e66618. doi: 10.1371/journal.pone.0066618. Print 2013.
V. X Chen, A Stojanovic, D Sminonsen, X Wang, Y Liu, TP Utheim.
Topography Guided Transepithelial Surface Ablation in Treatment of Moderate to
High Astigmatism
J Refract Surg. 2016;32(6):418-425
VI. X Chen, A Stojanovic, W Zhou, X Wang, TP Utheim, F Stojanovic, Q Wang.
Transepithelial, topography-guided ablation in treatment of visually disturbing
irregular astigmatism and/or scattering in LASIK-flap/interface complications
J Refract Surg. 2012 Feb;28(2):120-6. doi: 10.3928/1081597X-20110926-01. Epub
2011 Sep 30.

12
VII. X Chen, A Stojanovic, Y Hua, JR Eidet, D Hu, J Wang, TP Utheim.
Reliability of Corneal Dynamic Scheimpflug Analyser Measurements in Virgin and
Post-PRK Eyes
PLoS One. 2014 Oct 10;9(10):e109577. doi: 10.1371/journal.pone.0109577.
eCollection 2014.
VIII. A Stojanovic, X Chen, N Jin, T Zhang, F Stojanovic, S Ræder, TP Utheim.
Safety and efficacy of epithelium-on corneal collagen cross-linking using a
multifactorial approach to achieve proper stromal riboflavin saturation
J Ophthalmol. 2012;2012:498435. doi: 10.1155/2012/498435. Epub 2012 Jul 30.
IX. A Stojanovic, J Zhang, X Chen, TA Nitter, S Chen, Q Wang.
Topography-guided Transepithelial Surface Ablation Followed by Corneal Collagen
Crosslinking Performed in a Single Combined Procedure for the Treatment of
Keratoconus and Pellucid Marginal Degeneration
J Refract Surg. 2010 Feb;26(2):145-52. doi: 10.3928/1081597X-20100121-10. Epub
2010 Feb 12.
13
4. LIST OF FIGURES AND TABLES 4.1 Figures Figure 1. The tear film. It consists of three layers: lipid, aqueous, and mucin. Courtesy of
Haakon Raanes, The Oslo School of Architecture and Design, Norway.
Figure 2. Five distinct layers of the cornea. A sixth layer (Dua`s layer) has recently been
proposed. Courtesy of Dr. Magnus Fritzvold, Akershus University Hospital, Norway.
Figure 3. The X, Y, Z hypothesis of corneal epithelial maintenance. The desquamated cells
(Z component) are continuously replaced not only by the basal cells (X) that divide, but also
by cells migrating in from the periphery (Y). Courtesy of Dr. Magnus Fritzvold, Akershus
University Hospital, Norway.
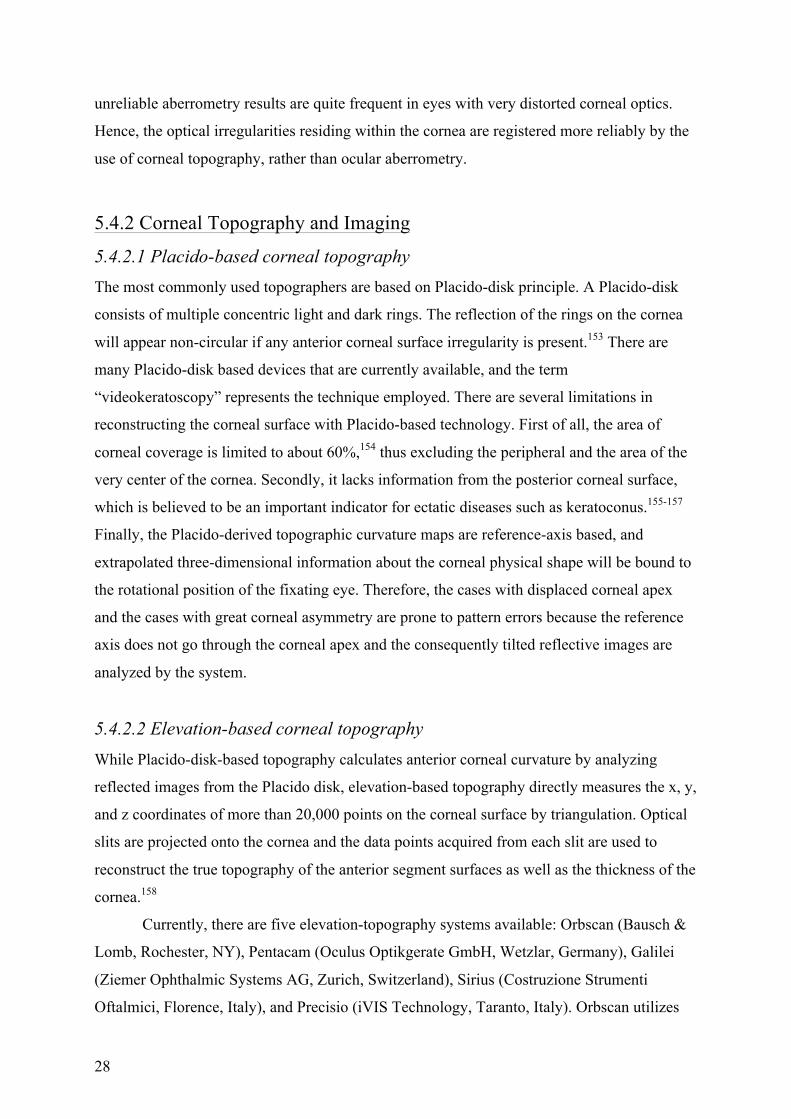
Figure 4. Placido based topography (left, axial map; right, instantaneous map) showing
inferior steepening in a keratoconic eye.
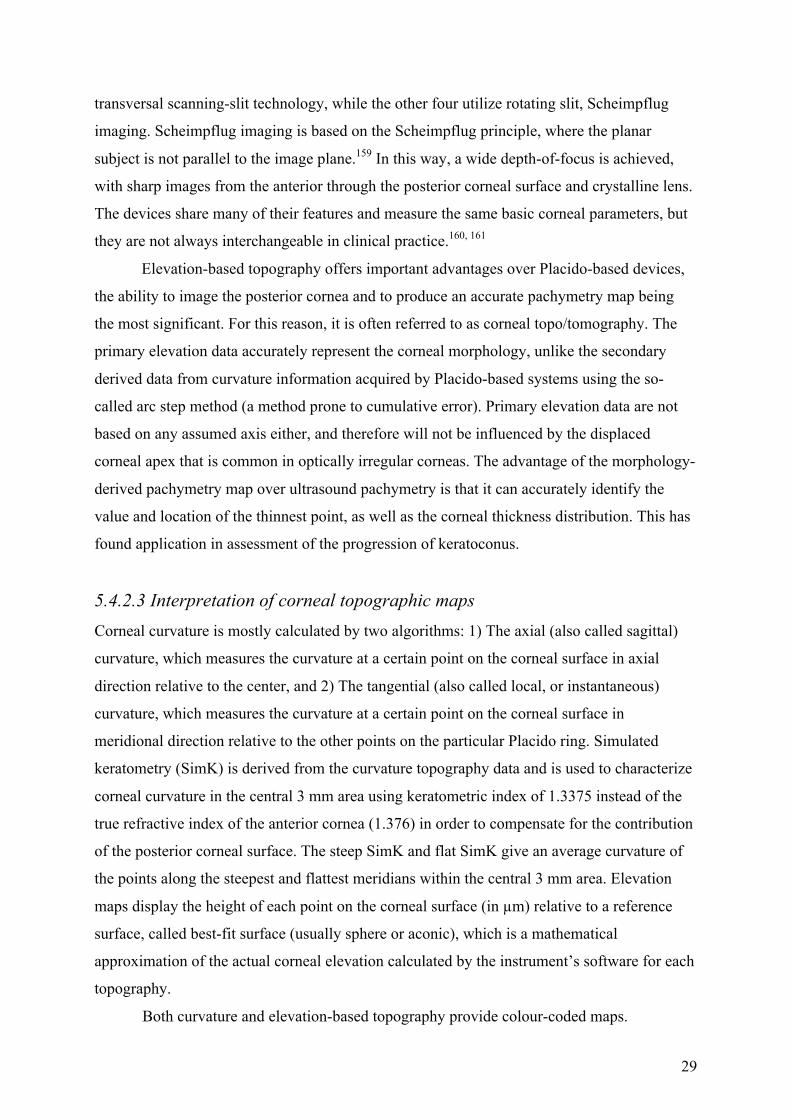
Figure 5. Elevation-based topo/tomography showing increased maximum elevation in the
anterior (upper left) and posterior surfaces (upper right) in the same keratoconic eye as
demonstrated in Figure 4a. The locations of these two points coincide with the point with
thinnest pachymetry (lower right).
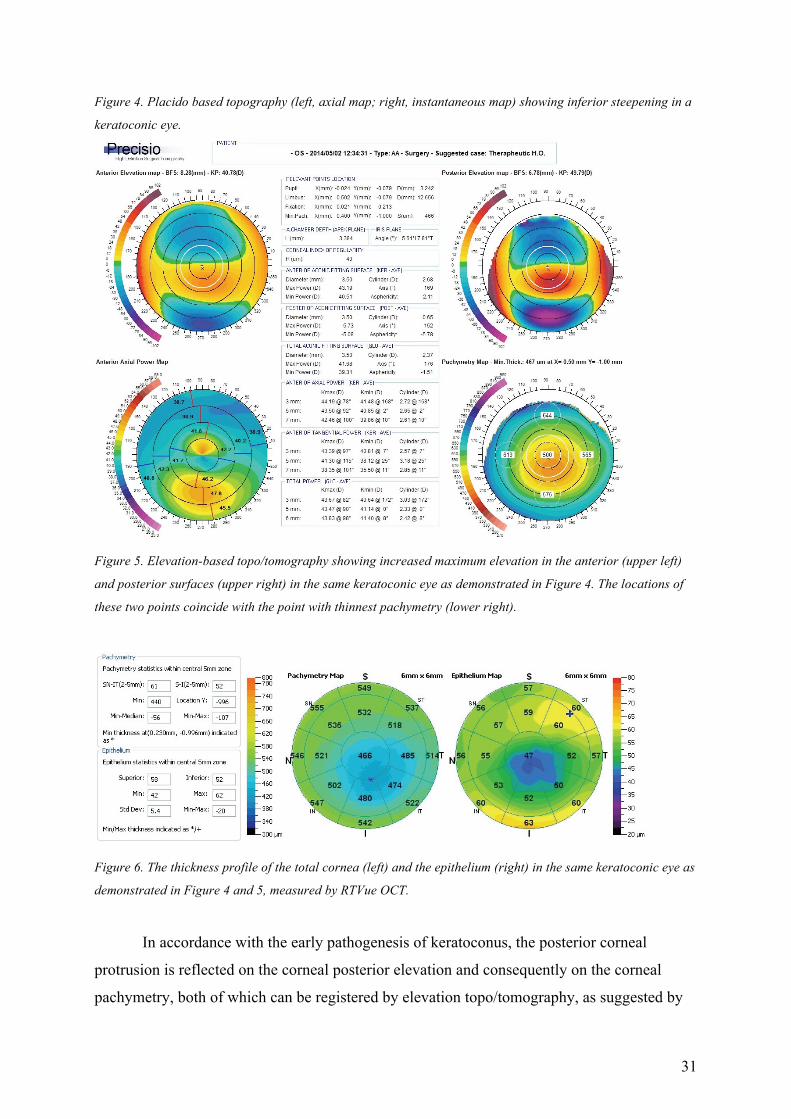
Figure 6. The thickness profile of the total cornea (left) and the epithelium (right) in the same
keratoconic eye as demonstrated in Figure 4 and 5, measured by RTVue OCT.
Figure 7. The output of ORA measurement: the signal peak (the red and blue curves) in the
left side presents the moment where the first inward applanation was reached, whereas the
peak in the right side represents the moment where the second outward applanation was
reached during the measurement. The green curve shows the change of the pressure of the air
pulse in time.
Figure 8. The CorVis ST utilizes the Scheimpflug camera to record the dynamic procedure of
the corneal response to an air puff. A) The first applanation is achieved. B) The cornea
reaches its highest concavity. C) The second applanation is achieved when the cornea
rebounds to its original position from the highest concavity.
Figure 9. A representative output of the CorVis ST measurement showing the dynamic
deformation amplitude (upper left), applanation length (upper middle) and corneal velocity
(upper right) during the course of deformation and recovery, as well as the parameters
measured at the time when first and second applanation, and highest concavity is reached (the
lower table).

14
Figure 10. Four types of corneal laser refractive surgery techniques. Top view: (a) Epithelial
removal in surface ablation. (d) Flap cut in LASIK. (g) Flap and lenticule cut in FLEX. (j)
Cap and lenticule cut in SMILE using. Side view: (b) Cornea after epithelial removal in
surface ablation. (c) Excimer laser ablation of the stroma in surface ablation. (e) Flap cut in
LASIK. (f) Flap lift and subsequent excimer laser ablation on the stroma in LASIK. (h) Flap
and lenticule cut in FLEX. (i) Flap lift and lenticule removal in FLEX. (k) Cap and lenticule
cut, and side cut in SMILE. (l) Lenticule removal through the side cut in SMILE.
Figure 11. Topography-guided surface ablation in treatment of subepithelial irregularity
masked by epithelial remodelling. (a) Epithelium masking a stromal irregularity; (b)
Mechanical or alcohol-aided epithelial removal exposes irregular surface; (c) When
topography representing the epithelial surface is used as the basis for the treatment planning,
and the treatment itself is performed on the stroma after the epithelial removal, a new
irregular surface is produced; (d) When the same topography is used for planning of
transepithelial ablation that removes both the epithelium and the stroma as a single entity, a
regularized surface shape will be “transferred” to the stroma below the irregularity (dotted
line).
Figure 12. Slit lamp verification of the stromal riboflavin saturation before the UVA-
irradiation.
Figure 13. Schematic drawing of the ablation plan of the topography-guided transepithelial
ablation in keratoconic eyes. The green layer represents the epithelium. The top and bottom
dashed lines represent the epithelial surface and the desired postoperative surface. The spaces
between the top and middle dashed lines represent the lamellar part of the ablation, and the
space between the middle and bottom dashed lines represents the refractive part of the
ablation. The lamellar part of the ablation in the area of the cone consists of both the
epithelium and stroma, due to the epithelial thinning over the cone.
4.2 Tables
Table 1. Amsler-Krumeich Classification for Grading Keratoconus.
Table 2. Summarized outcomes of recent studies reporting PRK-outcomes in treatment of
myopic astigmatism in virgin eyes.
Table 3. Literature review of studies presenting results of laser corneal refractive surgery for
moderate to high astigmatism correction.

15
5. GENERAL INTRODUCTION 5.1 The Ocular Surface
5.1.1 Structure and Function The ocular surface comprises cornea and bulbar and tarsal conjunctiva, extending to the
mucocutaneous junctions of the lid margins. It protects the ocular structures from the external
world and optimizes the optical properties of the eye. The ocular surface is covered with tear
film secreted by the lacrimal and meibomian glands and conjunctiva.1, 2 The tear film consists
of three layers: the outermost lipid layer produced by the meibomian glands, the intermediate
aqueous layer secreted by the main and accessory lacrimal glands, and the innermost mucin
layer secreted by the surface epithelium and the conjunctival goblet cells (Figure 1).
Figure 1. The tear film. It consists of three layers: lipid, aqueous, and mucin. Courtesy of Haakon Raanes, The
Oslo School of Architecture and Design, Norway.
The intermediate aqueous layer is the largest (7 µm), followed by the lipid (0.1 µm)
and the mucin (0.02 to 0.05 µm) layers (Figure 1).3 Tears are also composed of enzymes,
immunoglobulins, various metabolites, and exfoliated epithelial and polymorphonuclear cells.
By serving as a permeability barrier to the corneal epithelium4 and by cleaning, lubricating
and nourishing the ocular surface, and providing physical and immune protection against

16
infection, tear film ensures the normal function and structure of the ocular surface to maintain
a clear cornea for vision.3, 5-8
Most of the refractive power of the eye is derived from the air-tear film interface
where the greatest change in the refractive index resides. The pre-corneal tear film also fills
and flattens the microscopic depressions of the corneal surface created by the reticulations on
the epithelial surface,9 playing a key role in the maintenance of a smooth and regular optical
surface.4, 10 Disturbance of the tear film can affect the optical quality and visual performance
of the eye.4, 11, 12
Tear film maintenance is dependent on adequate tear production and distribution.
Qualitative and quantitative alterations in the volume, composition, and structure of the tear
film can cause dry eye disease. In 2007, the Dry Eye Workshop (DEWS) defined dry eye as
“a multifactorial disease of the tears and ocular surface that results in symptoms of
discomfort, visual disturbance, and tear film instability with potential damage to the ocular
surface, accompanied by increased osmolarity of the tear film and inflammation of the ocular
surface.13 The two major subtypes of dry eye disease are aqueous-deficient dry eye disease,
resulting from a decrease in lacrimal gland secretion, and evaporative dry eye disease, in
which there is excessive evaporative water loss. Dry eye disease affects 5% to 34% of all
people globally, and prevalence increases with age.14
The status of the ocular surface and tear film before refractive surgery can impact
surgical outcomes in terms of potential complications during and after surgery, refractive
outcome, optical quality, and postoperative dry eye.15 Postoperative dry eye is one of the most
common complaints after corneal refractive surgery.16-23 It is believed to have a multifactorial
aetiology, consisting of neurotrophic epitheliopathy, altered tear film coverage of the changed
corneal contour, and an inflammatory desiccation of ocular surface.24 Although usually
transient, it negatively affects the quality of life and is the primary reason for patient
dissatisfaction with the refractive surgery outcome.25-28 Patients with dry eye after refractive
surgery also have higher risks for refractive regression and ocular surface damage.22, 29, 30
Identifying patients with dry eye disease prior to surgery and treating them pre- and
postoperatively can lead to improved outcomes in refractive surgery.31-35
5.1.2 The Cornea
5.1.2.1 Structure and function The cornea consists of transparent avascular tissue that acts as the primary infectious and
17
structural barrier of the eye. The average adult cornea is 0.52 mm thick in the center and
about 0.65 mm thick at the periphery. The horizontal diameter of the cornea is 11.5 to 12 mm,
and it is approximately 1 mm larger than the vertical diameter.36, 37
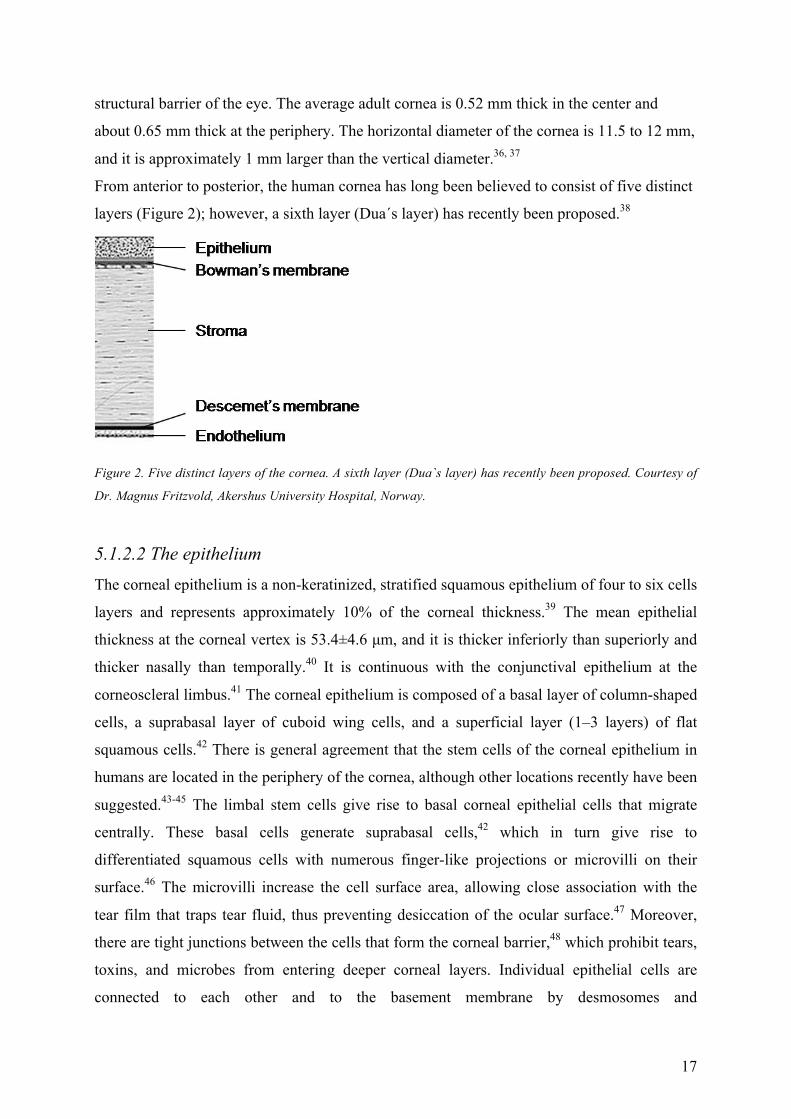
From anterior to posterior, the human cornea has long been believed to consist of five distinct
layers (Figure 2); however, a sixth layer (Dua´s layer) has recently been proposed.38
Figure 2. Five distinct layers of the cornea. A sixth layer (Dua`s layer) has recently been proposed. Courtesy of
Dr. Magnus Fritzvold, Akershus University Hospital, Norway.
5.1.2.2 The epithelium The corneal epithelium is a non-keratinized, stratified squamous epithelium of four to six cells
layers and represents approximately 10% of the corneal thickness.39 The mean epithelial
thickness at the corneal vertex is 53.4±4.6 μm, and it is thicker inferiorly than superiorly and
thicker nasally than temporally.40 It is continuous with the conjunctival epithelium at the
corneoscleral limbus.41 The corneal epithelium is composed of a basal layer of column-shaped
cells, a suprabasal layer of cuboid wing cells, and a superficial layer (1–3 layers) of flat
squamous cells.42 There is general agreement that the stem cells of the corneal epithelium in
humans are located in the periphery of the cornea, although other locations recently have been
suggested.43-45 The limbal stem cells give rise to basal corneal epithelial cells that migrate
centrally. These basal cells generate suprabasal cells,42 which in turn give rise to
differentiated squamous cells with numerous finger-like projections or microvilli on their
surface.46 The microvilli increase the cell surface area, allowing close association with the
tear film that traps tear fluid, thus preventing desiccation of the ocular surface.47 Moreover,
there are tight junctions between the cells that form the corneal barrier,48 which prohibit tears,
toxins, and microbes from entering deeper corneal layers. Individual epithelial cells are
connected to each other and to the basement membrane by desmosomes and
18
hemidesmosomes, respectively. These structures are important in mediating cell migration in
response to epithelial injury.49 Under normal conditions, the corneal epithelium is renewed
every 9–12 months.50 This contrasts with the human epidermis, where the replacement takes
place approximately once a month.51
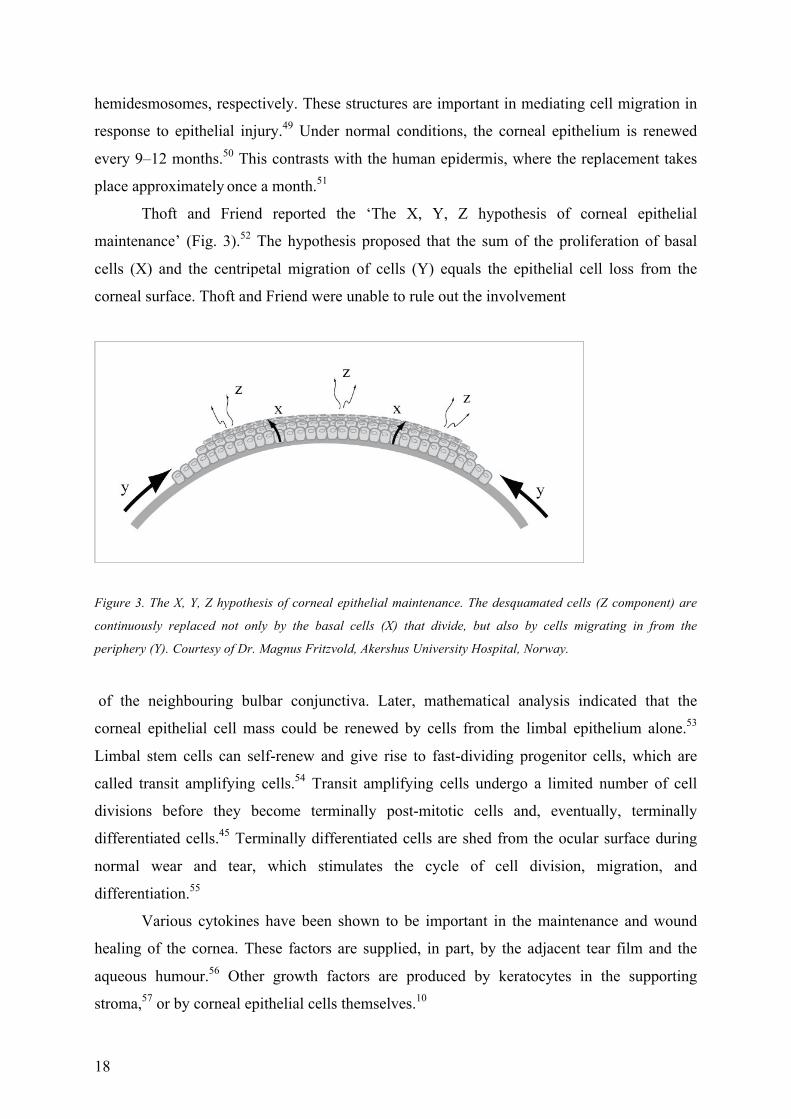
Thoft and Friend reported the ‘The X, Y, Z hypothesis of corneal epithelial
maintenance’ (Fig. 3).52 The hypothesis proposed that the sum of the proliferation of basal
cells (X) and the centripetal migration of cells (Y) equals the epithelial cell loss from the
corneal surface. Thoft and Friend were unable to rule out the involvement
Figure 3. The X, Y, Z hypothesis of corneal epithelial maintenance. The desquamated cells (Z component) are
continuously replaced not only by the basal cells (X) that divide, but also by cells migrating in from the
periphery (Y). Courtesy of Dr. Magnus Fritzvold, Akershus University Hospital, Norway.
of the neighbouring bulbar conjunctiva. Later, mathematical analysis indicated that the
corneal epithelial cell mass could be renewed by cells from the limbal epithelium alone.53
Limbal stem cells can self-renew and give rise to fast-dividing progenitor cells, which are
called transit amplifying cells.54 Transit amplifying cells undergo a limited number of cell
divisions before they become terminally post-mitotic cells and, eventually, terminally
differentiated cells.45 Terminally differentiated cells are shed from the ocular surface during
normal wear and tear, which stimulates the cycle of cell division, migration, and
differentiation.55
Various cytokines have been shown to be important in the maintenance and wound
healing of the cornea. These factors are supplied, in part, by the adjacent tear film and the
aqueous humour.56 Other growth factors are produced by keratocytes in the supporting
stroma,57 or by corneal epithelial cells themselves.10

19
5.1.2.3 Bowman´s membrane Bowman´s membrane is a clear acellular layer consisting of collagen fibrils with a diameter of
20-25 nm and proteoglycans. These fibrils are not ordered in bundles; individual fibrils run in
various directions to form a thick, dense, felt-like sheet that is about 8-12 µm thick. The
collagen fibrils in the posterior layer of the Bowman´s sheet are gradually assembled in
bundles and merge into the collagen lamellae of the stroma.58 The Bowman´s membrane is
more resistant to damage than the corneal epithelium.47 However, unlike the corneal
epithelium, it cannot regenerate after injury.47 Instead, fibrous scar tissue is formed, resulting
in opacity. Bowman´s membrane is not necessary for the formation of normal epithelium, and
its physiological role remains somewhat unclear.47
5.1.2.4 The stroma The stroma accounts for about 90% of the total corneal thickness.42 The parallel arrangement
of lamellae formed from heterodimeric complexes of type I and type V collagen fibrils
maintains the transparency of the cornea.41 The organization of collagen fibrils in the human
cornea has been studied using electron microscopy,58 X-ray diffraction or scattering,59, 60 and
second harmonic generation imaging microscopy.61 The collagen fibrils have a diameter of
25-35 nm, and are packed in parallel-arranged layers or lamellae.62 Adjacent lamellae lie at
different angles, between 0 and 90°.63 The human corneal stroma consists of over 300-stacked
lamellae through its central thickness. As the cornea thickens away from the vertex, the
number of lamellae increases, reaching about 500 throughout the stromal thickness at the
limbus.64 The collagen lamellae are thin (about 0.2-1.2 µm) and narrow (about 0.5-30 µm) in
the anterior third of the stroma, run mostly obliquely to the corneal surface, and are more
irregularly interwoven. Furthermore, parts of the anterior lamellae are inserted into Bowman’s
layer.65-67 In the posterior stroma, collagen lamellae become thicker (0.2-2.5 µm) and wider
(100-200 µm) and tend to be arranged parallel to the corneal surface, preferentially oriented
along the superior-inferior and nasal-temporal corneal meridians.58, 59, 61, 68
It is envisaged that these properties of the anterior lamellae contribute to balance the
intraocular pressure, maintain corneal curvature, make stronger transverse shear properties
and increase tensile strength compared to the posterior stroma; while the preferentially
aligned fibrils in the posterior stroma take up the additional tensile stress along the superior-
inferior and nasal-temporal meridians exerted by the rectus muscles and the orbicularis.69-73

20
The collagen lamellar arrangement has also been reported to be different between the
central and limbal area of the cornea in the posterior third of the cornea. The central cornea
maintained the preferred superior-inferior and nasal-temporal orientation of collagen to within
about 1 mm from the limbus, where a circular or tangential disposition of fibrils interlaced
with significant numbers of mature elastic fibres occur.60, 68 The circumferential
reinforcement of fibrils is thought to help to withstand the increased tension in that region
brought about by the differing curvatures of the cornea and sclera. Furthermore, while the
mean fibril diameter remains constant across all corneas, the mean fibril spacing across the
central cornea measured 5-7% lower than in the peripheral cornea.74
Keratocytes, which represent the main cell type in the stroma and mostly reside in the
anterior stroma, are involved in maintaining the extracellular matrix environment. They are
able to synthesize collagen molecules and glycosaminoglycans, as well as matrix
metalloproteases — all of which are crucial in maintaining stromal homeostasis. Keratocytes
also produce crystalline proteins that maintain corneal transparency.75
5.1.2.5 Descemet’s membrane Endothelial cells continuously “secrete” Descemet’s membrane. It is about 3µm thick at birth
but increases in thickness throughout life, reaching 10-12 μm in adulthood. It functions as a
protective barrier against infections and eye injuries.
5.1.2.6 The endothelium The intact human endothelium is a monolayer, a honeycomb-like appearing mosaic when
viewed from the posterior side. It is responsible for maintaining the stroma in a relatively
dehydrated state. Human endothelial cell density is approximately 3500 cells/mm2 at birth and
decreases at an average rate of 0.6% per year throughout life.76 The number of endothelial
cells also decreases with trauma, inflammation, and other pathological processes. Endothelial
cells have no mitotic capability in vivo; however, when the cell density decreases the
remaining cells have the ability to “stretch” and take over the space of the degenerated
endothelial cells.
5.1.2.7 Dua´s layer A recently described corneal layer was named after Professor Harminder S. Dua, who

21
discovered it.38 It is a 15 microns thick, well-defined, acellular layer in the pre-Descemet's
cornea. The membrane is sufficiently strong to withstand a pressure of approximately 700-
950 mm Hg. Its recognition may have considerable impact on posterior corneal surgery and
understanding of corneal biomechanics and posterior corneal pathology.38
5.2 Corneal Biomechanics Biomechanical properties refer to the dynamic response of the biological tissue to mechanical
stress, and the resulting deformation after stress. It is related to the structure and function of
the tissue. Elasticity represents how a material deforms in response to an external stress and
returns to its original shape along the same stress-strain pathway when the imposed stress is
removed. Viscosity is the resistance of a fluid to flow. It is determined by water content,
macromolecular components, and interactions between macromolecules. In highly viscous or
gel-like substances, molecules are strongly connected to each other and, thus, are not very
flexible.
Biomechanically, the cornea can be considered a bi-composite material consisting of
collagen fibrils and the ground substance (proteoglycans and glucosaminoglycans), in which
the fibers are embedded. The collagen fibrils provide elastic reinforcing structure while the
ground substance provides viscoelasticity.77 When loaded, the cornea demonstrates some
instantaneous deformation (purely elastic behaviour) followed by progressive deformation
(viscoelastic behaviour).78 It is important to keep in mind that the corneal stiffness and
viscoelasticity are not directly related, and alterations in tissue structure can lead to
independent changes in both.78
The highly anisotropic and distinctive arrangement of collagen fibers and the specific
collagen-matrix interaction are important factors for the anisotropic biomechanical properties
of the cornea. The biomechanics of the corneal stroma have been investigated by the
measurement of pulling force of corneal strips,79, 80 mercury droplet markers’ displacement
with increasing intraocular pressure,81 optical coherence tomography elastography,82
ultrasonic techniques,83 supersonic shear wave elastography,84 corneal hysteresis,85-87 as well
as Brillouin microscopy88, 89 and atomic force microscopy.90-92 These studies have revealed
that the anterior stroma is stiffer than the posterior stroma. The anterior stroma has also been
found not to swell in response to an artificial edema-inducing condition.69 Dowson et al.93
demonstrated increasing tensile strength moving from the central cornea towards the
periphery. In vitro pressure-induced regional mechanical performance of the cornea and
22
limbus measurements by Hjortdal et al.81 showed that the highest elastic moduli were found at
the center and para-center in the meridional direction, and at the limbus in the circumferential
direction.
Changes in the collagen fibrillar morphology and arrangement, as well as changes in
the collagen-matrix interaction, may lead to alterations in corneal biomechanical properties in
certain conditions. During ageing, there is an increase in the cross-linking among collagen
molecules, an increase in the diameter of collagen fibrils, glycation-induced expansion of
intermolecular spacing, as well as a decrease in the interfibrillar spacing of the corneal
collagen.94, 95 Therefore, one would expect a tendency toward biomechanical strengthening of
the cornea with ageing. Corneal stiffness of diabetic eyes may increase due to increased cross-
linking through glycosylation and lysyl oxidase enzymatic activity.96
In keratoconus corneas, reduced mean diameter and interfibrillar spacing of the
collagen fibrils,97 slippage of collagen lamellae,98, 99 as well as a loss of the normal
interwoven structure of the lamellae,100 may result in biomechanical instability of the tissue.73
Corneal refractive surgery may also induce corneal biomechanical changes.101, 102 Finally, the
photo polymerization effect of riboflavin-ultraviolet radiation A (UVA) corneal cross-linking
(CXL) induces cross-links at the collagen fibril surface and in the protein network
surrounding the collagen.103 Nevertheless, the biophysical and biochemical factors
determining corneal stiffness, elasticity, viscosity, and damping are not fully understood,72
and further studies are warranted.
5.3 Corneal Optics In addition to functioning as a barrier, the cornea is the most important optical component of
the eye, refracting the light and focusing it onto the retina with minimum scatter and optical
degradation.
5.3.1 Eye Optics
5.3.1.1 Refractive components and accommodation The human eye is similar to a camera, consisting of: the main refracting component (the
cornea), a variable aperture (the pupil), adjustable focusing (the crystalline lens) and a dark
(posterior) chamber. These optical elements form images on a layer of photosensitive retinal
tissue, which converts patterns of light into neuronal signals. Many attempts have been made
to simplify the optical system of the human eye. For instance, in Gullstrand’s eye model, the
total refractive power of the eye is 58.64 diopters (D), with 43 D contributed by the cornea
23
and 19 D contributed by the lens, while the axial length of the eye is 24 mm.37 The eye
changes its refractive power to focus on near objects by a process called accommodation,
which is a result of the optical power change of the crystalline lens. According to the
Helmholtz theory of accommodation, contraction of the ciliary muscle leads to thickening and
increased curvature of the crystalline lens, due to relaxation of the lenticular capsule.
In a relaxed accommodative state, the combined optical power of the cornea and
crystalline lens must match the axial length of the eye in order to provide a sharp focus of a
distance object on the retina (emmetropia). When a mismatch occurs, the images will be out
of focus, which is commonly called ammetropia (refractive error).
5.3.1.2 Myopia Myopia is the type of defocus where the total refractive power is too high relative to the axial
length of the eye, leading to images of distant objects focusing in front of the retina. Myopia
is the most common eye disorder worldwide.104 The prevalence and progression seem to be
affected by many variables such as ethnicity, sex, familial disposition, age of onset, degree of
myopia, near-reading activities, outdoor activities, as well as education level.105-108 Midelfart
and colleagues found the prevalence of myopia in Norway to be 35.0% in the young adult
population and 30.3% in the middle-aged group in 1996-1997.109
5.3.1.3 Hyperopia In contrast to the myopia, the total refractive power in hyperopia is too low relative to their
axial length. Consequently, the images of distant objects are focused behind the retina.
However, young hyperopes are usually not bothered by their hyperopia because they can
easily “move” the defocused images to the retina by using their accommodation, which is still
of large amplitude. Midelfart et al. found the prevalence of hyperopia in Norway to increase
with age from 13.2% (20–25 years) to 17.4% (40–45 years).109
5.3.1.4 Astigmatism An eye with astigmatism produces two orthogonally symmetrical lines of foci instead of a
focal point. The focal distance between the lines decides the amount of astigmatism. Astigmatism cannot be corrected by changing viewing distance or accommodation. Lower
order aberrations (LOAs), defocus and regular astigmatism can be corrected by spectacles,
contact lenses, and refractive surgery.

24
5.3.2 Corneal Optics Although the cornea is represented in Gullstrand’s model as one refractive surface with 43 D
power, the light entering the eye is actually refracted by both the anterior and the posterior
surface of the cornea. The anterior corneal surface is flatter than the posterior surface. The
mean radius of curvature of the anterior and posterior surface is 7.8 mm and 6.8 mm,
respectively. However, the anterior surface has much greater optical power (48.8 D) than the
posterior surface (-5.8 D) due to larger differences in refractive indices between the air and
the cornea than between the cornea and the aqueous.110
The curvature of the anterior surface of the cornea normally decreases from the vertex
to the periphery; i.e. the cornea is not spherical. The term asphericity (Q-value) is used to
define the shape of the cornea in terms of change in curvature. Q= a2/b2-1, where a and b
represent the radius of curvature of central and peripheral cornea, respectively. A spherical
cornea that has the same radius over the whole area will generate a field of focal points
instead of one point, because the peripheral light rays (that are not perpendicular to the
cornea) are refracted more than the central rays. This phenomenon is called spherical
aberration. If the spherical shape is changed to prolate, where the radius of the curvature is
increasing towards periphery (Q<0), the peripheral light rays are relatively less refracted, and
the spherical aberration is reduced. On the contrary, the spherical aberration is increased with
oblate shape, where the radius of curvature becomes smaller towards the periphery (Q>0) and
the peripheral light rays are more refracted. The ideal asphericity for the anterior surface of
the cornea to eliminate spherical aberration for a distant object would be a prolate ellipsoid
with Q= -0.528. However, several investigators have shown that the mean Q-value of the
anterior cornea over a 6-mm zone is -0.26 (0.00 to-0.50).111 The normal human cornea with a
Q-value of -0.26 is rarely free of spherical aberration itself, but in balance with the slightly
negative asphericity of the crystalline lens, it contributes to achieve a minimal spherical
aberration of the total optical system of the eye.112
5.3.3 Irregular Astigmatism Since the anterior cornea provides almost two-thirds of the eye’s focusing power,
imperfections of the corneal surface will have a significant impact on retinal image quality,113
causing optical anomalies known as aberrations, which are responsible for inferior optical
performance of the eye.114 Corneal irregular astigmatism is a type of refractive anomaly, in
which the orientation of the principal meridians and/or the power change across the cornea
25
from point to point. It occurs primarily in keratoconus, or secondary to iatrogenic keratectasia,
decentered or otherwise complicated corneal refractive surgery, corneal scarring (post
traumatic, post keratitis) etc.115 The irregularities cause distortedly projected images on the
retina, perceived as visual disturbances such as glare, halos, starburst, multiple images, and
reduced contrast sensitivity.116
To analyze and define the irregular astigmatism, a decomposition of the complex
optical irregularities may be performed and then represented in terms of wavefront aberrations
that correlate to the quality of vision. Wavefront is an imaginary three-dimensional surface
representing corresponding points of the light rays vibrating in unison. The difference
between the wavefront from the optical system with refractive anomalies, and the wavefront
from the ideal optical system defines wavefront aberrations. A typical way to describe the
wavefront aberration is in terms of a Zernike polynomial series.117, 118 Each Zernike
polynomial can describe only a limited family of shapes. For example, one Zernike
polynomial may describe how much the surface tilts, while another may describe how much
the edge may turn up or down, etc. Hence, Zernike decomposition can provide a good
description of the cornea’s optical properties. Zernike coefficients represent the weight of
each of the components on the wavefront aberrations. The aberration components represented
by Zernike terms are grouped into lower order aberrations (LOAs) and higher order
aberrations (HOAs). The higher the order is, the more subtle the irregularities are that can be
described. The lower order terms correspond to conventional refractive errors: first order
terms represent prism, while the second order terms represent defocus and astigmatism.
Higher order terms include other more complex monochromatic aberrations, like coma (the
3rd order), with the opposite power at the opposite ends of one meridian, spherical aberration
(4th order), etc. Generally speaking, odd-order higher order aberrations are non-rotationally
symmetric, while even-order are rotationally symmetric aberrations. Wavefront aberrometry,
which measures the ocular wavefront aberration, as well as the corneal topography, are the
most effective means to evaluate the corneal irregular astigmatism.
5.3.4 Treatment of Irregular Astigmatism Correction of irregular astigmatism remains a difficult challenge. Spherical or sphero-
cylindrical spectacle glasses can only help to move the images onto the retinal plane, but they
cannot resolve the visual disturbances caused by distorted images. Soft contact lenses provide
marginally better visual acuity than spectacle correction, with the level of residual aberrations
26
still remaining high due to modelling of the soft contact lens to the corneal surface.119 Rigid
gas permeable (RGP) contact lenses have been reported to be able to provide a significant
improvement in visual acuity for patients with irregular astigmatism.119-121 The shape of RGP
is unaffected by the underlying corneal surface. The tear fluid (n=1.336) formed beneath the
RGP lens has a similar refractive index to the cornea (n=1.376) and therefore neutralizes most
(1.336/1.376=97%) of the aberrations of the anterior corneal surface.119 However, discomfort
often associated with the use of RGP can have a negative impact on the patient’s quality of
life.122, 123 For these patients, surgical intervention becomes a necessity.
Excimer laser surgery on the cornea, guided by topography or wavefront, is now a
method of choice for the treatment of corneal irregular astigmatism. This will be elaborated in
chapter 5.6.1. In addition, there are several other possible options for reshaping the irregular
cornea and improving the regularity of the corneal surface.
Thermal keratoplasty is based on shrinkage of the stromal collagen to achieve a
change in corneal shape. The thermal energy can be applied by a Holmium-laser,124-127 or by a
technique called conductive keratoplasty (CK), where resistance to the electrical current flow
through the tissue generates thermal energy.128 The CK-technique has been reported to be
effective in reshaping the cornea in eyes with keratoconus, without serious complications.129
However, the mentioned methods did not show a predictable dose response between the
applied energy and the induced refractive change, but they showed considerable regression.
Lately, a new device and technique that involves the application of microwaves to the corneal
surface was used to change the refractive state of the cornea by changing the pathway and
thereby the curvature of the collagen fibers. The changes in refraction were reported to be
more predictable, but were also temporary, regressing over the course of 3 months.130 Vega-
Estrada A and his colleagues131 combined the microwave thermal keratoplasty with corneal
collagen cross-linking (CXL) to smoothen the irregular anterior cornea in keratoconic eyes.
The use of intrastromal corneal ring segments (ICRS) is another way to reshape the
cornea and mostly improve the irregular component of astigmatism and corrected distance
visual acuity (CDVA). The concept was introduced in 1978, and the ICRS were first
implanted in human eyes in 1991 to correct myopia.132-134 They are currently used to improve
vision in keratoconus and corneal ectasia,135-139 mostly in combination with spectacles,
contact lenses, or phakic intraocular lenses (PIOL).140, 141 The tunnels for implantation of
ICRS could be created mechanically or by femtosecond (FS) laser. Several studies have
demonstrated no significant difference in terms of visual, refractive, and keratometric
outcomes between the two tunnelling techniques.135-139 Mechanical tunnelling, however,

27
seems to result in more complications, including increased incidence of epithelial defects and
greater risk of corneal perforation.135, 136 There are three commonly used models of ICRS:
Intacs (Additional Technology, Inc.), Kerarings (Mediphacos Ltda.), and Ferrara rings
(Mediphacos, Inc., Belo Horizonte, Brazil). The models differ in cross-sectional shape,
diameter, arc length, and thickness. In general, for a greater degree of flattening, thicker ring
segments and closer placement of the ring to the visual axis142 are used. Whereas some studies
reported stable long-term outcomes of ICRS implantation in keratoconic eyes,143, 144 Vega-
Estrada et al.143, 145 found that the short-term improvement achieved by ICRS implantation
was lost after 5 years in progressive keratoconic eyes. The authors therefore suggested that
the implantation of ICRS might not arrest the progression of keratoconus.
5.4 Diagnostics – Assessment of Various Technologies for
Measurement and Analysis of Corneal Optical Properties and
Morphology Current corneal assessment technologies make the process of corneal evaluation fast and
precise. The most commonly used instruments, including aberrometers, corneal topographers
(either Placido-disk-, slit-scanning- or Scheimpflug-imaging-based), and optical coherence
tomography (OCT), will be introduced in this chapter.
5.4.1 Wavefront Aberrometry Measuring and representing the optical irregularities in term of wavefront aberrations is one
way to assess the quality of the eye´s optical system. Wavefront aberrometers perform a high-
resolution spatial auto refraction across the area of the pupillary opening, rendering a map of
wavefront aberrations expressed in micrometers of deviation (root-mean-square [RMS]) from
the ideal wavefront plane.146 The principles used in the commercially available devices
include ray tracing,147 automatic retinoscopy,148 Hartmann-Shack149 and Tscherning.150
Because of the dynamic nature of the accommodation and the age-related physiological
changes in crystalline lens, considerable variation in the aberrometry results may occur from
exam to exam during the same session and from exam to exam over a period of time.151, 152
For this reason and due to the “crossover effect” (local optical distortion exceeding a certain
magnitude registered by a “wrong” lenslet of the lenslet array sensor in a Hartman-Shack
aberrometer)146, as well as due to the limitations of the pupil-dependent measurement area,
28
unreliable aberrometry results are quite frequent in eyes with very distorted corneal optics.
Hence, the optical irregularities residing within the cornea are registered more reliably by the
use of corneal topography, rather than ocular aberrometry.
5.4.2 Corneal Topography and Imaging
5.4.2.1 Placido-based corneal topography The most commonly used topographers are based on Placido-disk principle. A Placido-disk
consists of multiple concentric light and dark rings. The reflection of the rings on the cornea
will appear non-circular if any anterior corneal surface irregularity is present.153 There are
many Placido-disk based devices that are currently available, and the term
“videokeratoscopy” represents the technique employed. There are several limitations in
reconstructing the corneal surface with Placido-based technology. First of all, the area of
corneal coverage is limited to about 60%,154 thus excluding the peripheral and the area of the
very center of the cornea. Secondly, it lacks information from the posterior corneal surface,
which is believed to be an important indicator for ectatic diseases such as keratoconus.155-157
Finally, the Placido-derived topographic curvature maps are reference-axis based, and
extrapolated three-dimensional information about the corneal physical shape will be bound to
the rotational position of the fixating eye. Therefore, the cases with displaced corneal apex
and the cases with great corneal asymmetry are prone to pattern errors because the reference
axis does not go through the corneal apex and the consequently tilted reflective images are
analyzed by the system.
5.4.2.2 Elevation-based corneal topography While Placido-disk-based topography calculates anterior corneal curvature by analyzing
reflected images from the Placido disk, elevation-based topography directly measures the x, y,
and z coordinates of more than 20,000 points on the corneal surface by triangulation. Optical
slits are projected onto the cornea and the data points acquired from each slit are used to
reconstruct the true topography of the anterior segment surfaces as well as the thickness of the
cornea.158
Currently, there are five elevation-topography systems available: Orbscan (Bausch &
Lomb, Rochester, NY), Pentacam (Oculus Optikgerate GmbH, Wetzlar, Germany), Galilei
(Ziemer Ophthalmic Systems AG, Zurich, Switzerland), Sirius (Costruzione Strumenti
Oftalmici, Florence, Italy), and Precisio (iVIS Technology, Taranto, Italy). Orbscan utilizes
29
transversal scanning-slit technology, while the other four utilize rotating slit, Scheimpflug
imaging. Scheimpflug imaging is based on the Scheimpflug principle, where the planar
subject is not parallel to the image plane.159 In this way, a wide depth-of-focus is achieved,
with sharp images from the anterior through the posterior corneal surface and crystalline lens.
The devices share many of their features and measure the same basic corneal parameters, but
they are not always interchangeable in clinical practice.160, 161
Elevation-based topography offers important advantages over Placido-based devices,
the ability to image the posterior cornea and to produce an accurate pachymetry map being
the most significant. For this reason, it is often referred to as corneal topo/tomography. The
primary elevation data accurately represent the corneal morphology, unlike the secondary
derived data from curvature information acquired by Placido-based systems using the so-
called arc step method (a method prone to cumulative error). Primary elevation data are not
based on any assumed axis either, and therefore will not be influenced by the displaced
corneal apex that is common in optically irregular corneas. The advantage of the morphology-
derived pachymetry map over ultrasound pachymetry is that it can accurately identify the
value and location of the thinnest point, as well as the corneal thickness distribution. This has
found application in assessment of the progression of keratoconus.
5.4.2.3 Interpretation of corneal topographic maps Corneal curvature is mostly calculated by two algorithms: 1) The axial (also called sagittal)
curvature, which measures the curvature at a certain point on the corneal surface in axial
direction relative to the center, and 2) The tangential (also called local, or instantaneous)
curvature, which measures the curvature at a certain point on the corneal surface in
meridional direction relative to the other points on the particular Placido ring. Simulated
keratometry (SimK) is derived from the curvature topography data and is used to characterize
corneal curvature in the central 3 mm area using keratometric index of 1.3375 instead of the
true refractive index of the anterior cornea (1.376) in order to compensate for the contribution
of the posterior corneal surface. The steep SimK and flat SimK give an average curvature of
the points along the steepest and flattest meridians within the central 3 mm area. Elevation
maps display the height of each point on the corneal surface (in µm) relative to a reference
surface, called best-fit surface (usually sphere or aconic), which is a mathematical
approximation of the actual corneal elevation calculated by the instrument’s software for each
topography.
Both curvature and elevation-based topography provide colour-coded maps.

30
Warmer colours (reds, oranges) represent steeper corneas (higher dioptric power) in the
curvature map, points above the reference surface in the elevation map, and areas with thinner
cornea in the pachymetric map. Cooler colours (blues, violets), however, represent flatter
corneas (lower dioptric power), points below the reference surface, and area with thicker
cornea in respective maps. Greens and yellows represent medium values in all of the maps.
However, different topographers use different numbers of steps and colour coding as their
default, making it difficult to compare the results from different topographers.
Anterior corneal optical irregularities measured either by Placido-disk- or elevation-based-
topography162 may be analyzed, decomposed and presented as wavefront data,163 for the
diagnosis and definition of irregular astigmatism. Higher amounts of vertical coma and larger
values of odd-order RMS have been reported in patients with keratoconus or keratoconus
suspect.164-169
5.4.2.4 Topography in keratoconus Keratoconus shows a characteristic topographic pattern. The anterior corneal surface is
characterized by a focal steepening over the inferior mid-peripheral zone, which is surrounded
by a zone of progressively decreasing curvature,170, 171 described as asymmetric bowtie with
skewed axis or asymmetric bowtie with inferior steepening (Figure 4).156 The anterior
elevation map shows the physical location of the cone as a focally increased elevation, located
mostly in the inferotemporal quadrant.172, 173 Various topographers feature a plethora of
keratometric indices for the easy identification of keratoconus patterns. Some indices
describing anterior corneal surface irregularity derived from Scheimpflug images such as
index of height decentration, and index of surface variance, have been identified as robust
indicators for keratoconus severity and progression.174
31
Figure 4. Placido based topography (left, axial map; right, instantaneous map) showing inferior steepening in a
keratoconic eye.
Figure 5. Elevation-based topo/tomography showing increased maximum elevation in the anterior (upper left)
and posterior surfaces (upper right) in the same keratoconic eye as demonstrated in Figure 4. The locations of
these two points coincide with the point with thinnest pachymetry (lower right).
Figure 6. The thickness profile of the total cornea (left) and the epithelium (right) in the same keratoconic eye as
demonstrated in Figure 4 and 5, measured by RTVue OCT.
In accordance with the early pathogenesis of keratoconus, the posterior corneal
protrusion is reflected on the corneal posterior elevation and consequently on the corneal
pachymetry, both of which can be registered by elevation topo/tomography, as suggested by

32
numerous studies.155, 157, 175, 176 It was reported that the maximum posterior elevation155, 156 and
posterior elevation of the thinnest corneal point157 was significantly higher, and the central
pachymetry and thinnest pachymetry are significantly thinner155, 157, 175 in keratoconus than in
normal eyes, and that these points coincide, even in the mildest forms of keratoconus (Figure
5). This suggests that the first detectable sign of keratoconus is a bowing of the posterior
corneal surface detected by tomography. The annular pachymetric distribution was also
demonstrated to be a sensitive parameter for distinguishing even the mildest form of
keratoconus from normal eyes.157, 175
5.4.3 OCT and OCT-based Topography Apart from scanning-slit tomography and rotating Scheimpflug imaging, the optical coherent
tomography is another non-contact 3-dimensional (3-D) optical imaging technology that can
be used for assessment of the cornea and the anterior segment. OCT is an optical method
based on low coherence interferometry. It compares the time-delay of infrared light reflected
from the anterior segment structures against a reference reflection. This interference pattern
leads to a cross-sectional image of the anterior segment of the eye with a high resolution.177
After the images have been captured and saved to the computer, various parameters can be
measured including corneal thickness, anterior chamber depth, anterior chamber angle, and
angle-to-angle distance.178
There are currently two different types of OCTs applied in ophthalmology: time-
domain OCT, in which varying the position of the reference mirror produces cross-sectional
images, and Fourier-domain OCT, in which the reference mirror is fixed and Fourier
transformation of the spectral interferogram generates the cross-sectional images. Because the
Fourier-domain systems, such as the RTVue 100 (Optovue, Inc., Fremont, CA), do not
depend on mechanical movement of a reference mirror and detect signals from the entire
depth range in parallel rather than serially, they achieve higher speed without losing signal-to-
noise ratio.177
OCT technology can provide corneal structural analysis and may be used to assess a
wide range of anterior segment features from the cross-sectional images, including evaluation
of the flap- and the residual stromal bed thickness and keratectasia after laser in situ
keratomileusis (LASIK),179 as well as localization of the demarcation line within the stroma
after CXL.178 Anterior segment OCT (AS-OCT) has demonstrated a good repeatability and
reproducibility of the central and peripheral cornea thickness mapping.180, 181 Pachymetry

33
mapping with the AS-OCT has been suggested as a helpful screening and early diagnostic
tool for keratoconus.180, 182
Recently, a new, high speed, swept-source anterior segment spectral domain OCT based
corneal topo/tomographer, CASIA (Casia SS-1000; Tomey, Nagoya, Japan), has been
developed.183-185 Its high speed scanning (0.34 second in corneal map mode) may contribute
to minimization of the artefacts caused by ocular movements during the examination,186 while
its 1310 nm wavelength of the light source allows better penetration into the opaque tissues
such as cloudy corneas compared to visible light,187, 188 making it a better suited tool for the
examination of corneal pathology than the existing corneal topo/tomographers. Both the short
duration of the exam and the use of infrared instead of visible light significantly increase the
comfort of examination and allows the patients to hold their eyes widely open, contributing to
better coverage of the examined cornea. It has been reported that the success rate of precisely
digitizing the corneal surfaces in keratoconic eyes was 95% using the AS-OCT-based corneal
topo/tomography.183
The most unique application of OCT in diagnosis of keratoconus is mapping of the
corneal epithelial thicknesses. The corneal epithelium is a mouldable and active corneal layer,
being regulated by the blinking action and the force applied by the eyelid. It maintains the
optical quality of the eye by remodelling itself to compensate for any changes in the stromal
surface shape,189 such as those occurring after myopic and hyperopic laser ablation,190, 191
orthokeratology,192 secondary stromal irregularities193 and in keratoconus.194-196 Therefore,
information about the thickness distribution of the corneal epithelium may help to identify
irregularity of the stromal surface, as in subclinical keratoconus, before it is detectable on
corneal topo/tomography. The recent studies of clinical in vivo epithelial mapping by OCT
demonstrated a typical epithelial remodelling pattern with keratoconus, with the epithelium
being thinner inferotemporally and thicker supranasally, compared to that of normal eyes
(Figure 6). This suggests that the AS-OCT-derived epithelial mapping has a critical potential
in the diagnosis of early and progressive keratoconus.194, 195 The concept of use of epithelial
mapping as a part of structural analysis of cornea and its application to various diagnostic and
even surgical purposes has been introduced and developed by Reinstein using high frequency
ultrasound technology.196 However, that technology did not reach the level of commercial
availability. AS-OCT proved to be more practical in that respect, primarily due to its ease of
use and the comfort of non-contact, quick and easy to perform examinations.
5.4.4 In Vivo Confocal Microscopy (IVCM)
34
The modern in vivo confocal laser scanning microscopy employs a laser light source that
focuses on one point of the object through a pinhole diaphragm. The reflected laser light is
separated by a beam splitter from the incident laser beam path and is deflected through a
second confocal diaphragm to reach a photosensitive detector.197 In this way, the scattered
light from outside the focal plane is highly suppressed, and only the objective layer located at
the focal plane contributes to the image, enabling imaging in high resolution.
The IVCM can be used to analyze the images of the corneal structures.198-201 Its non-
invasive nature enables real-time in vivo evaluation of the cornea at the cellular level.202 The
z-axis position of these images can be used to calculate corneal sublayer’s thicknesses.203, 204
Clinically, the in vivo confocal microscopy has been used to study normal and diseased
corneas,200, 205-207 and corneas following surgery203, 208, 209 or contact lens use.210, 211
Corneal wound healing after refractive surgery is a complex cascade.212 During laser
refractive surgery, damage to the epithelium has been shown to cause the release of various
kinds of cytokines and chemokines,213-218 inducing keratocyte apoptosis and modulating the
subsequent stromal repair response.216, 219 An intensified corneal wound healing reaction can
occasionally lead to undesirable complications, such as regression of the refractive outcome
and haze.220, 221 One important feature of IVCM is its ability to objectively quantify corneal
backscatter, which is used to define stromal reaction, keratocyte activation, and objective haze
grading.222-224 The IVCM has also been applied to evaluate corneal nerve regeneration after
corneal refractive surgery.225-228
Only a small area of the cornea is imaged with confocal microscopy, and a tracking
system is not present in current devices. As a result, positional repeatability is low.229
Therefore, the reliability of the data obtained with confocal microscopy should be facilitated
by repeated measurements.
5.4.5 Corneal Biomechanical Measurements Despite the great needs for the corneal biomechanical measurements at the individual level,
most of our current knowledge comes from ex vivo experimental studies performed with
stress-strain and other mechanical tests.79, 80, 90-92 In vitro measurements have proven to be
largely dependent on the technique used and experimental conditions (time post-mortem,
hydration conditions, storage solutions, etc.). As the compelling clinical need for
biomechanical information has increased, various in vivo techniques have been under active
development.
35
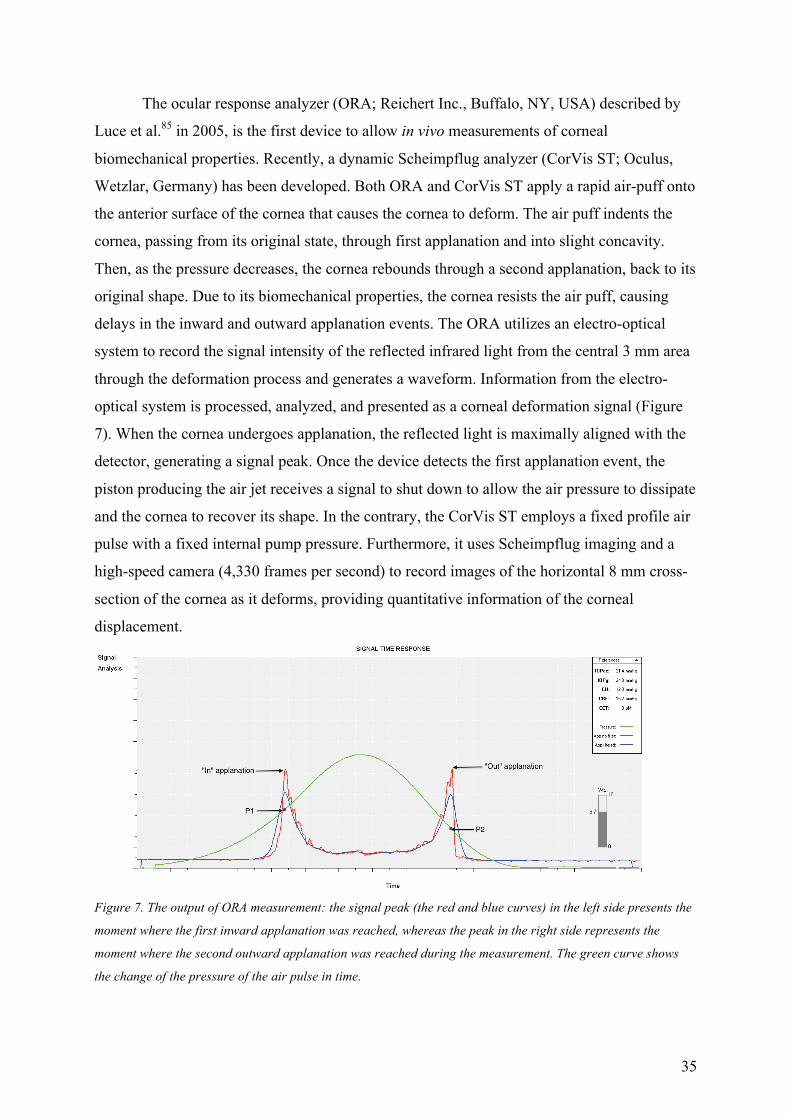
The ocular response analyzer (ORA; Reichert Inc., Buffalo, NY, USA) described by
Luce et al.85 in 2005, is the first device to allow in vivo measurements of corneal
biomechanical properties. Recently, a dynamic Scheimpflug analyzer (CorVis ST; Oculus,
Wetzlar, Germany) has been developed. Both ORA and CorVis ST apply a rapid air-puff onto
the anterior surface of the cornea that causes the cornea to deform. The air puff indents the
cornea, passing from its original state, through first applanation and into slight concavity.
Then, as the pressure decreases, the cornea rebounds through a second applanation, back to its
original shape. Due to its biomechanical properties, the cornea resists the air puff, causing
delays in the inward and outward applanation events. The ORA utilizes an electro-optical
system to record the signal intensity of the reflected infrared light from the central 3 mm area
through the deformation process and generates a waveform. Information from the electro-
optical system is processed, analyzed, and presented as a corneal deformation signal (Figure
7). When the cornea undergoes applanation, the reflected light is maximally aligned with the
detector, generating a signal peak. Once the device detects the first applanation event, the
piston producing the air jet receives a signal to shut down to allow the air pressure to dissipate
and the cornea to recover its shape. In the contrary, the CorVis ST employs a fixed profile air
pulse with a fixed internal pump pressure. Furthermore, it uses Scheimpflug imaging and a
high-speed camera (4,330 frames per second) to record images of the horizontal 8 mm cross-
section of the cornea as it deforms, providing quantitative information of the corneal
displacement.
Figure 7. The output of ORA measurement: the signal peak (the red and blue curves) in the left side presents the
moment where the first inward applanation was reached, whereas the peak in the right side represents the
moment where the second outward applanation was reached during the measurement. The green curve shows
the change of the pressure of the air pulse in time.

36
In ORA, the first inward applanation pressure is called “P1” and the second outward
applanation pressure is called “P2” (Figure 7). The average of P1 and P2 provides a
Goldmann-correlated intraocular pressure (IOPg). The difference between P1 and P2 is
termed corneal hysteresis (CH=P1-P2). Corneal hysteresis (CH) represents the ability of the
cornea to absorb and dissipate energy (damping capacity), which is in contrast to its stiffness,
elasticity, or rigidity. It is the result of the viscous damping within corneal tissues that is
created by the viscosity of glycosaminoglycans and proteoglycans, as well as by a collagen
matrix interaction. Corneal resistance factor (CRF) is derived from the formula (P1-kP2),
where k is a constant that is strongly associated with CCT. The CRF is a parameter that was
empirically developed to be strongly associated with corneal stiffness230 and is believed to be
a measurement of the overall corneal resistance (total viscoelastic properties) of the cornea
during measurement.85, 231 Corneal compensated IOP (IOPcc) is an empirical IOP
measurement (IOPcc=P2 –c1xP1+c2, where c1 and c2 are constants), which is less affected
by corneal biomechanical properties on IOP measurement compared with other tonometry
techniques.
The CH and CRF are two most commonly analyzed metrics in the ORA to describe
the biomechanical properties of the cornea. The repeatability and reproducibility of the
measurements have been proven to be good for both CH and CRF.87, 232, 233 In addition, the
Waveform Score may provide information on the reliability of the signals in ORA. Lam et
al.234 proposed that a score < 3.50 might indicate an unreliable signal that should be
discarded.
In published data, the CH and CRF showed a positive correlation with CCT.86, 233, 235-
237 It is postulated that a thicker healthy cornea contains more collagen fibers and ground
substance, resulting in a greater resistance against deformation and a higher damping
capacity. The IOP represents an additional force that restores the cornea to its original
position. There is inverse correlation between IOPcc and CH.233 In contrast, there is positive
correlation between IOPcc and CRF,233 indicating that resistance against deformation of the
cornea is higher in eyes with higher IOP values. As a consequence of age-related collagen
cross-linking, corneal stiffness increases with ageing,94 whereas simultaneous and gradual
diminution of proteoglycan and glycosaminoglycans of the viscous ground substance occurs,
resulting in decreased CH.238-241 Whether other factors may affect CH and CRF, such as
ethnicity,242, 243 gender,240 diurnal variation,233, 244-246 glaucoma,241, 247 diabetes,248-253 the eyes
refractive status,254-257 and corneal curvature, remains controversial.258-260

37
The CH and CRF decreases in keratoconic eyes.86, 261, 262 It may be partially due to the
decrease in corneal thickness, but may be primarily due to the altered structure of
proteoglycans and glycosaminoglycans in keratoconic eyes. As the keratoconus progresses,
the proteoglycan content of the stroma increases, whereas fibril diameter is reduced, leading
to weakening lateral cohesion.97 Still, there is a large overlap between normal eyes and
keratoconic eyes in CH and CRF,263 and it was demonstrated that CH and CRF alone might
not be sufficient to identify keratoconus suspect cornea.262
The CH and CRF decrease after corneal refractive surgery, and greater attempted
corrections correlate with greater reductions in CH and CRF.264-267 A combination of
thickness reduction and change in the viscoelastic properties of the cornea may be responsible
for the decrease. In LASIK, the flap creation itself causes a reduction in CH.231 Other studies,
however, found no difference between the surface ablation procedure and LASIK;101, 231, 265
therefore, the authors suggested that it was mainly the tissue removal that accounted for the
induced changes.101, 268, 269
Recently, it has been postulated that the shape of the applanation signal (the elevation
of the first and second peak, as well as undulation of the signal) may yield important
information in addition to CH and CRF,269-271 and it should be considered in the interpretation
of results. The waveform analysis might have increased sensitivity to biomechanical changes
in the cornea. For example, no statistically significant changes in CH and CRF measurements
were detected after CXL in patients with keratoconus and post-LASIK ectasia,272-274 whereas
analysis of the waveform of the ORA signal showed a statistically significant increase of the
P2 area after CXL.261, 274 The waveform parameters may be useful to differentiate between
healthy and diseased biomechanical conditions.268, 269 They demonstrated a good ability to
distinguish between keratoconus and normal eyes, or between keratoconus and post-LASIK
eyes.268 Nevertheless, how these parameters represent the biomechanical properties of the
cornea is still unknown and further studies are needed to evaluate the biomechanical
relevance and clinical importance of these parameters.
Unlike ORA, in which the signal intensity of the reflected infrared light is used for
analysis, the CorVis ST utilizes the data acquired from the Scheimpflug camera during the
measurement. The measured parameters can be grouped by three distinct phases: first inward
applanation, highest concavity (maximal deformation), and second outward applanation. At
the two applanation phases, values of length of the flattened cornea (A1L, A2L), time elapsed
to reach applanation (A1T, A2T) and the velocity (A1V, A2V) of the cornea at those
moments are registered. At the phase of highest concavity, it records the deformation

38
amplitude (DA) at the corneal apex, the distance of the two apexes (peak distance) of the
cornea, radius of curvature, and the time taken to reach it (Figure 8 and Figure 9). At the time
of the first applanation, the strength of the air pulse at the time of the first applanation is
determined, based on which a calibration factor is used to calculate an IOP value.
Figure 8. The CorVis ST utilizes the Scheimpflug camera to record the dynamic procedure of the corneal
response to an air puff. A) The first applanation is achieved. B) The cornea reaches its highest concavity. C) The
second applanation is achieved when the cornea rebounds to its original position from the highest concavity.

39
Figure 9. A representative output of the CorVis ST measurement showing the dynamic deformation amplitude
(upper left), applanation length (upper middle) and corneal velocity (upper right) during the course of
deformation and recovery, as well as the parameters measured at the time when first and second applanation,
and highest concavity is reached (the lower table).
The measurement of CCT, IOP, A1T, and DA with the CorVis ST has been reported
to be reliable,275-278 while the other parameters demonstrated relatively large deviation. One
study showed that in healthy eyes, the IOP measured with CorVis ST did not differ
statistically from the Pascal dynamic contour tonometry (DCT; Swiss Microtechnology AG,
Port, Swizerland), whereas it provided statistically higher IOP values compared to both
Goldmann applanation tonometry and ORA. The difference was influenced by CCT and age,
but not affected by corneal curvature or spherical equivalent.279 However, another study
showed that IOP measured with CorVis ST was on average 2.2 mmHg lower compared to
ORA-derived IOPg or IOPcc.280 Although both use an air-puff approach, the CorVis
parameters showed poor correlation with CH and CRF obtained by ORA measurements in
healthy eyes,280 indicating that they are fundamentally different.
Shorter A1T and larger DA in CorVis ST measurements may indicate less rigid
corneas. Studies showed that the DA is strongly affected by the IOP,281 but there are
disagreement on whether the DA and AIT are affected by age276, 280, 282-284 or diabetes.253
In a recent paper, Hassan et al. carried out a comparison of the corneal biomechanical
parameters variation between PRK and LASIK using the CorVis ST; they observed that most
of the biomechanical parameters were unchanged one month after LASIK and PRK compared
to the preoperative data.285 Another study286 showed that during the small incision lenticule
extraction (SMILE) procedure, the deformation parameters (A1T, A2T, DA, and IOP) did not
change after stromal-lenticule creation with FS laser, but changed significantly after the
40
lenticule extraction. Mastropasqual et al.287 reported increased DA and A1T seven days after
SMILE procedure; however, at 1 and 3 months, these values did not show statistically
significant alterations. The authors thereby hypothesized that a substantial modification of
corneal biomechanics occurs in the very first follow-up time after the surgery and that the
new biomechanical balance is relatively quickly established. Furthermore, one study
compared the corneal deformation parameters after SMILE, laser-assisted subepithelial
keratectomy (LASEK), and FS-LASIK reported significant higher DA, and shorter A1T after
FS-LASIK compared to LASEK. No significant differences were detected in these two
variables between LASEK and SMILE groups, or between the SMILE and FS-LASIK
groups.288
The standard Corvis ST parameters are different in groups of KC and normal subjects,
but they are widely dependent on IOP and CCT.289 When IOP was excluded from analysis,
greater DA correlated significantly with thinner CCT in both healthy eyes and KC eyes. In
pachymetry and IOP-matched comparison, the DA was statistically greater in KC eyes,276, 290,
291 whereas A1T was shorter in KC eyes.289, 290 However, they did not reach the level of good
predictive accuracy for the detection of keratoconus. Temporal symmetry factor (Tsym) is the
ratio of loading and unloading areas under the cornel deformation against the curve.292 Tsym
was shown to be highly sensitive to the CXL treatment in the in vitro porcine eye study by
Kling et al.292 However, an in vivo human eye study by Tian et al. did not show a significant
difference between the KC group and control group.291
It has been shown that the type of mount used in an experimental setting affected the
corneal deformation response to an air puff. The A1T was shorter, and the DA was higher
under the same internal pressure in human donor corneas mounted intact as a whole-globe
compared to when mounted in an artificial anterior chamber. Therefore, in vivo air-puff
examinations may be affected by scleral stiffness in addition to the cornea.293 In a recent
study, the impact of orbital muscles was found to have a greater impact on deformation than
the sclera.281 Therefore, some parameters focusing on delineating the whole globe motion
from the corneal deformation were introduced. For example, the corneal contour deformation
(CCD) was introduced as a measure of the recoil effect of the eye caused by the air pulse
indentation,291 and deflection amplitude as the deformation amplitude corrected for whole eye
movement at the highest concavity.289
The corneal dynamic deformation recorded by the CorVis ST has the potential to
provide useful information on corneal biomechanics. As the CorVis ST is a relatively new
technology, studies with CorVis ST are limited, and the reliability of the measurements needs

41
to be improved. Further improvements in reliably measured relevant CorVis ST parameters
and exploration of the applicability and capabilities of this technique in characterizing corneal
biomechanics are warranted.
Optical coherence elastography has also been used for the assessment of corneal
biomechanics. Generally, this technique employs a loading device to induce tissue
deformation and utilize the OCT-based displacement-detection technique to monitor the
dynamic response of the tissue.294, 295 Recently, shear wave imaging OCT (SWI-OCT) is
utilized to image the low-amplitude Lamb wave (elastic wave whose particle motion lies in
the plane perpendicular to the object) that is induced using a focused air-puff device with
short-duration and low-pressure air stream.296 The phase velocities of the Lamb wave at the
major frequency components were quantified, and related to the biomechanical properties (for
example, higher stiffness has higher phase velocity at major frequency components). Hence,
they were considered to be an effective indicator of corneal elastic properties. Its application
in vivo clinical studies remains to be explored.
The above-mentioned measurements involving physical deformation of the cornea are
inherently coupled with IOP and other geometrical factors. Furthermore, the measurements of
ORA and CorVis ST rely on large magnitude (millimeter-scale) global deformations of the
eye, which causes a non-linear corneal response to the mechanical stimulation, leading to
inaccurate measurements. Finally, the lack of depth-resolved detection limits the clinical
usefulness of these techniques.
A recent technique named Brillouin microscopy claims to be able to determine
intrinsic viscoelastic properties decoupled from the structural information and applied
pressure.297, 298 Brillouin light-scattering is an inelastic scattering process arising from the
interaction between incident light and spontaneous acoustic phonons in the sample material.
As the propagation speeds of acoustic phonons are related to the material´s mechanical
properties, measuring the frequency shift induced by the acousto-optic interaction allows the
elastic properties to be determined. Brillouin microscopy measures the frequency shift by
employing ultrahigh-resolution spectrometry. The frequency shift Ω is related to the
longitudinal elastic modulus M´ by the expression M´=1/4 Ω2 λ2 (ρ /n2), where λ is the optical
wavelength in air, ρ is the mass density, and n is the refractive index. Studies by Scarcelli et
al.88, 299 demonstrated a good log-log linear relationship between the longitudinal modulus M´
determined from the Brillouin shift and conventional Young´s (or shear) moduli E´ measured
at low frequencies: log (M´) = a・log (E´) +b, where a and b are material-dependent
coefficients. Brillouin scattering microscopy is a novel optical technology that enables three-
42
dimensional mechanical imaging. Bovine eye297 and human cornea studies89, 300 demonstrated
that in healthy corneas, the Brillouin shift was highest in the anterior corneal region and
decreased gradually toward the endothelium, with much less variation laterally at the same
depth. The anterior cornea showed moderate decay, and the posterior stroma showed steep
decline over depth. In the cone region of the keratoconus eyes, the anterior portion had lower
Brillouin shift, and the shift decayed in a more rapid fashion across the corneal depth
compared to that of the healthy corneas. In addition, much higher cornea-to-cornea variability
in terms of Brillouin shift and changes through depth was presented in the cone region of the
keratoconus cornea compared with healthy controls. The profiles measured outside the cone
region in the periphery were different from those of the cone region, and rather similar to
those of healthy corneas. The CXL procedure resulted in a substantial increase of Brillouin
modulus in the stroma by 10%.297 The measurement is performed optically without the need
for acoustic transducers or physical contact with the cornea, enabling in vivo study of the
human eye.300 One of the limitations of the current Brillouin instruments for use in the clinic
is its relatively long acquisition time. A single full axis scan across the eye takes about 1
minute, although the scan time could be reduced to <10 seconds at the expense of the scan
range or sampling intervals.300 The speed improvement in the future will facilitate its clinical
application.
With the increased focus on the biomechanics of the cornea in recent years, the
development of new instrumentation that might aid in the diagnosis of ocular disease and
clinical assessment of corneal biomechanical properties is of great interest. Understanding of
corneal biomechanical properties is extremely important to improve clinical diagnostic
procedures, as well as to optimize treatment modalities. The development of biomechanical
measurement techniques will be of great help in setting up optical models for refractive
surgery.
5.5 Keratoconus
5.5.1 Definition, Etiology and Epidemiology Keratoconus is a disease caused by weakening of the cornea due to abnormalities in its
structure and/or composition. The internal pressure in the eye causes the weakened cornea to
bulge from its normal shape, and the resultant conical protrusion of the cornea causes
significant irregular astigmatism and visual impairment. Keratoconus is usually a bilateral,
though often asymmetrical condition. After the initial diagnosis of keratoconus in one eye, it

43
may take years for the condition to become apparent in the fellow eye.301 It has been
suggested that the term “forme fruste keratoconus” be used for such less affected fellow eyes
that display no clinical findings except for certain topographic changes. In contrast, the term
“keratoconus suspect” should be reserved for eyes with suspicious topographic patterns,
wherein the fellow eye of the individual does not have keratoconus.302
The prevalence of keratoconus in the general population has been reported to range
from 57-229 per 100,000170, 303-305 and the incidence is higher among Asians than
Caucasians.304, 306 Since more young adults are having screening topographies taken upon
corneal refractive surgery evaluation, it is likely that the incidence and prevalence of
keratoconus in recent years has increased most likely due to improved and earlier diagnostics.
The exact etiology of keratoconus is not well understood yet, but it was found to be associated
with atopic diseases,307 vernal keratoconjunctivitis,308 eye rubbing,309 floppy eyelids,310 Down
syndrome311 and non-inflammatory connective tissue disorders, such as Ehlers–Danlos
syndrome312 and osteogenesis imperfecta.313 The relationship between the cause and the effect
is often unclear in the etiology of keratoconus. Some associations like environmental
influence and mechanical trauma may potentially lead to the condition, but others may point
towards a common genetically determined cause. A recent article systematically reviewed the
current knowledge on genetic risk factors associated with keratoconus and concluded that a
number of genetic susceptibility loci are implicated and that there is a genetic heterogeneity
rather than a single major gene-effect responsible for development and progression of
keratoconus.314 An international group of 36 experts published a global consensus on
keratoconus and ectatic corneal disease. They concluded that the pathophysiology of
keratoconus is likely to include environmental, biomechanical, genetic, and biochemical
disorders, but that there is no primary pathophysiologic explanation for keratoconus.315
5.5.2 Pathogenesis
5.5.2.1 Biochemical and inflammatory factors It has been suggested that an abnormality in the degradative pathway of macromolecules may
be responsible for keratoconus. Focus was initially centered on an imbalance between matrix
metalloproteinases and their endogenous inhibitors, tissue inhibitors of matrix
metalloproteinases. The matrix metalloproteinases are a family of enzymes that degrade a
wide variety of extracellular materials, including collagens, proteoglycans, fibronectin,
laminin and elastin. Chan and colleagues,316 in a recent review, concluded that an up-
44
regulation of selected matrix metalloproteinases and cathepsins, as well as decreased level of
their inhibitors such as tissue inhibitors of matrix metalloproteinases, play a role in corneal
thinning in keratoconus. The prominent up-regulated matrix metalloproteinases and
cathepsins include matrix metalloproteinase-14,317, 318 matrix metalloproteinase-13 and
cathepsin K,319 B and G.320
Keratoconus has conventionally been held to be a non-inflammatory condition.
However, recent studies on cytokines and enzyme levels suggest that inflammation likely
plays a greater role in the progression and development of keratoconus than previously
assumed. It has been confirmed that rather than a global increase in proinflammatory
cytokines, it is a complex imbalance between proinflammatory and anti-inflammatory
molecules that disrupts the corneal homeostasis in eyes with keratoconus.321 Studies that
analyzed inflammatory molecules in the tears of patients with keratoconus have found that
interleukin-6 (IL-6) and tumour necrosis factor alpha (TNF-alpha) are overexpressed,
indicating that the pathogenesis of keratoconus may involve chronic inflammatory events.318,
321
The up-regulated degradative enzymes and overexpressed inflammatory molecules
may result in tissue damage and further weakening in keratoconic cornea, but the source of
those components remains unclear. One theory suggests that the components are released
upon keratocyte apoptosis, as a reaction to chronic triggers such as ongoing epithelial
injury.322 This theory is consistent with the findings of keratoconus association with contact
lens wearing and eye rubbing.
5.5.2.2 Structural and compositional changes Biomechanical strength of the cornea is maintained by the intricate composition of the
collagen network. Anterior stroma seems to have the most important role in keeping the
unique shape of the cornea because of the higher degree of lamellar interweaving and a
distinct population of lamellae inserting into Bowman’s layer. In eyes with keratoconus, the
structure and composition of the collagen network is disrupted. It has been pointed out that
the development of keratoconus involves a high degree of inter- and probably intra-lamellar
displacement and slippage that leads to stretching and thinning of the central cornea and
associated changes in corneal curvature.98 A marked loss or decrease in anterior lamellar
interweaving and the sutural lamellae that are inserted into Bowman’s layer has been detected
in keratoconic corneas.98 Furthermore, a reduction in the overall amount of protein in the
keratoconic corneas compared with normal controls has been reported.323, 324 This is further
45
supported by Koa and his colleagues,325 who demonstrated that the total collagen content in
keratoconic corneas was about 50% of the normal. In addition, they observed a substantial
increase in collagenase activity in keratoconic corneas grown in organ culture.325
In conclusion, keratoconus is a multifactorial disorder, with environmental, behavioural, and
multiple genetic components contributing to its development. However, all of the findings
point to essential pathology, which is a reduced mechanical stability of the cornea. A number
of studies compared mechanical properties, including rigidity, stress-to-strain and strain-to-
failure in extracted corneal tissue, and indicated that the keratoconic corneas are both weaker
and less elastic compared to the normal corneas.326-328 The loss of biomechanical stability is
thought to result in decreased resistance to intraocular pressure, which gives keratoconic
corneas their characteristic protruded shape and consequent morphologic and optical changes.
5.5.3 Staging
5.5.3.1 Classic clinical diagnosis and staging Slit-lamp biomicroscopy still serves as a means for examining gross tissue changes in
keratoconus, such as the Fleischer ring (iron deposits around the base of the cone), Vogt’s
striae, paracentral corneal thinning and protrusion, rupture in Bowman’s layer, and stromal
scars beneath the breaks in Bowman’s layer.170, 301 In the past, the diagnosis and grading of
keratoconus were commonly based on central corneal thickness measurements, keratometric
readings, and the degree of myopization, as in the Amsler-Krumeich classification (Table
1).166, 329 In addition to slit-lamp biomicroscopy, ultrasonic pachymetry and videokeratoscopy
were the most commonly used screening tools. The aforementioned global consensus group315
summarized the definition and diagnostic of keratoconus as follows:
• The findings mandatory to diagnose keratoconus:
o Abnormal posterior elevation
o Abnormal corneal thickness distribution
o Clinically non-inflammatory corneal thinning
• Diagnosis of Keratoconus:
o Full tomographic corneal thickness map
o Slit-lamp examination
o Anterior curvature map

46
o Anterior and posterior elevation maps
Posterior corneal elevation abnormalities must be present to diagnose early or subclinical
keratoconus. Central pachymetry is the least reliable indicator (determinant) for diagnosing
keratoconus (keratoconus can be present in a cornea with normal central thickness)
• Ectasia progression (defined by a consistent change in at least 2 of the following
parameters, where the magnitude of the change is above the normal noise of the
testing system):
o Progressive local protrusion and steepening of the anterior corneal surface
o Progressive local protrusion of the posterior corneal surface with coinciding
location with the anterior protrusion
o Progressive thinning and/or an increase in the rate of corneal thickness change
from the periphery to the thinnest point
o Although progression is often accompanied by a decrease in CDVA, a change
in both uncorrected visual acuity (UDVA) and CDVA is not required to
document progression
• Risk factors for keratoconus:
o Down syndrome
o Family history
o Ocular allergy
o Ethnic factors (Arabian and Asian)
o Mechanical factors, e.g., eye rubbing and floppy eyelid syndrome
o Atopy
o Connective tissue disorders (Marfan syndrome)
o Ehlers–Danlos syndrome
o Leber’s congenital amaurosis
o Pregnancy
Table 1. Amsler-Krumeich Classification for Grading Keratoconus
STAGE FINDINGS
1 Eccentric steepening

47
Myopia, induced astigmatism, or both <5.00 D
Mean central K readings <48 D
2 Myopia, induced astigmatism, or both from 5.00 to 8.00 D
Mean central K readings <53.00 D
Absence of scarring
Corneal thickness >400 micron
3 Myopia, induced astigmatism, or both from 8.00 to 10.00 D
Mean central K reading >53.00 D
Absence of scarring
Corneal thickness 300-400 micron
4 Refraction not measurable
Mean central K readings >55.00 D
Central corneal scarring
Corneal thickness<200 micron
5.5.3.2 Modern imaging methods The detection of moderate to severe keratoconus is fairly easy with the classic diagnostic
tools; however, a variety of advanced imaging technologies are needed for discriminating
eyes with early keratoconus or with risk factors for keratoconus from the normal population
or other conditions. Corneal topography, one of the most important diagnostic imaging tools
for keratoconus, has evolved from Placido-based- to scanning-slit- and to Scheimpflug-based
imaging technology. Wavefront aberrometry also contributed to the early detection of
keratoconus by detecting its characteristic optical properties and hence differentiating it from
normal eyes. Also, optical coherence tomography (OCT) and OCT-based topography are
becoming increasingly more useful in imaging the early indicators of keratoconus. A detailed
presentation of modern imaging techniques is made in section 5.4.2 of this manuscript.
5.6 Interventions–Treatment of Refractive Errors and
Keratoconus
5.6.1 Corneal Laser Refractive Surgery
5.6.1.1 Overview and history The excimer laser reshaping of cornea was first introduced to ophthalmology and refractive

48
surgery over 25 years ago.330 Since then, the technique has been under development, and is
now considered safe for vision correction. Excimer lasers are gas lasers that emit pulses of
light within the UV spectral range. In corneal refractive surgery, the wavelength of 193 nm,
obtained by mixing argon and fluorine gases (ArF-excimer), is most widely used. During
excimer laser ablation, the UV light produces high-energy photons that break organic
molecular bonds within corneal tissue at a precisely controlled x,y position on the corneal
surface.331 Solid-state lasers are an alternative to excimer lasers, where a solid-state diode
emits UV radiation at 210 or 213nm wavelength.332, 333
Excimer laser is capable of “cold cutting” the corneal tissues. It causes a
photochemical reaction resulting in the ablation of corneal tissues without thermal damage to
the adjacent remaining structures. The method allows incisions of controlled depth and shape
to be made in the cornea. A defined volume of a defined shape from a defined area of a
cornea can be removed by ablating the tissue to a pre-determined depth.330
To date, excimer laser systems have achieved important advances in the areas of beam
profile refinement and homogenization, beam delivery (full beam, scanning slit, and flying
spot delivery) and refinements of other laser beam parameters, such as pulse duration,
frequency, energy, fluence and ablation rate. Eye tracking and iris recognition systems have
been developed to compensate for eye movements during laser treatment (in the X–Y
horizontal plane and cyclotorsion on lying supine).
5.6.1.2 Types of excimer laser ablation design According to the laser ablation pattern design, two main modalities exist, the “standard” and
the “custom” ablation (CA). The standard ablation involves central corneal flattening or
steepening according to predetermined formula based only on the subject’s spherocylindrical
refractive error (LOAs), while CA attempts to reshape the corneal surface to fit the individual
eye’s optics and/or anatomy and that way it addresses the HOAs as well. In the current
project, CA is based on the information derived from the topography of the anterior corneal
surface, so called topography-guided custom ablation (TGCA). In theory, both the LOAs and
HOAs of the whole eye could be corrected by using the information derived from the ocular
wavefront aberrometry measurements, used in wavefront-guided CA. In practice, however,
there are limitations to the latter technology: the eye is a dynamic optical system, while the
ocular wavefront measurements are based on only one “snap-shot” of that dynamic system.
Furthermore, the measurement range of ocular wavefront aberrometers is limited, making
them unsuitable for measurements of larger amounts of aberrations originating from irregular

49
corneas. The TGCA may, in contrast, be used in highly irregular corneas and in cases with
media opacities, as it is based on measurements of the corneal surface (corneal HOAs).
5.6.1.3 Surgical techniques Surface Ablation
Excimer laser surgery for correcting refractive errors was originally introduced in the
form of photorefractive keratectomy (PRK),334-336 which is performed after complete removal
of the central epithelium using mechanical debridement or alcohol and application of the
excimer laser to the denuded stroma for refractive correction (Figure 10). Published long-term
outcomes for surface ablation show its safety and predictability in patients with the ranges of
low and moderate myopia337-339 and thinner corneas.340 The main drawbacks of PRK are the
significant postoperative pain, relatively slow visual recovery and postoperative haze
development, especially in treatment of high myopia.341, 342
Healing of the cornea is followed by the release of inflammatory cytokines by the
damaged epithelium216 which in turn results in apoptosis, as well as in the proliferation and
degeneration of the underlying stromal keratocytes.343, 344 Histologically, haze appears to be
associated with highly reflective myofibroblastic cells and with disorganized collagen
deposition of amorphous glycosaminoglycans. Modern PRK-techniques attempt to modulate
the corneal wound healing reaction by aiming for a smooth post-ablation surface by use of
high laser-frequency, small laser-beam diameter, randomized flying-spot delivery345 and/or
various additional smoothing techniques that seem to be associated with reduced corneal
haze.346 The postoperative application of mitomycin-C has been demonstrated to significantly
delay keratocyte repopulation in the anterior stroma and to prevent corneal haze that way.347,
348
Various means for pain relief after PRK has also been developed over the years. The
use of topical non-steroidal anti-inflammatory drugs (NSAIDs) and small amounts of topical
anaesthetics seem to be safe and effective in improving postoperative comfort after PRK.349
Bandage contact lens use during reepithelialization and surface cooling before and
immediately after the laser treatment seem to result in pain relief as well.350
Disturbed integrity of the basement membrane underneath the basal epithelial cells has
been proposed as a key factor in the corneal repair process and development of haze.346, 351
Therefore, PRK modifications that preserve the epithelium as a flap were proposed to
accelerate visual rehabilitation and reduce induced corneal haze. These treatments include

50
LASEK, where the corneal epithelial flap is separated manually from Bowman’s layer
assisted by alcohol application and replaced after ablation352 and Epi-LASIK, where the
epithelial flap is produced by an automated mechanical device (epikeratome) with a blunt
blade.353 However, studies showed that there is no significant difference in refractive and
corneal structural outcomes up to one year postoperatively between patients treated for
myopia with PRK with MMC and LASEK/Epi-LASIK.354, 355
Other modifications of the PRK procedure have also been attempted to improve the
outcome. Transepithelial photorefractive keratectomy (T-PRK) uses an excimer laser to ablate
the epithelium before the refractive ablation of the underlying stroma.356 The excimer laser
epithelial removal in T-PRK can be performed separately by adding a phototherapeutic
keratectomy (PTK) before the refractive ablation of the stroma, or as a part of integrated one-
step transepithelial refractive procedure. The former has been reported to induce more
postoperative discomfort and more intense wound healing in terms of haze and keratocyte
apoptosis in the early postoperative period compare to LASEK.357 However, the latter was
reported to result in faster epithelial healing, lower postoperative pain score and significantly
less haze formation compared to alcohol-assisted PRK.358, 359 Possible explanations might be
that the integrated ablation mitigates the risk of corneal hydration changes between epithelial
removal and subsequent stromal ablation steps, as well as due to a smaller deepithelialization
area.
In addition, T-PRK is the only type of surface ablation that can successfully deal with
the consequences of epithelial remodelling by treating the epithelium and stroma as a single
entity in an uninterrupted single ablation. This sets special requirements for the excimer laser
with respect to the ablation speed, energy and fluence in order to achieve compatible ablation
rate between the epithelium and the stroma. A detailed explanation will be presented in the
next session.

51
Figure 10. Four types of corneal laser refractive surgery techniques. Top view: (a) Epithelial removal in surface
ablation. (d) Flap cut in LASIK. (g) Flap and lenticule cut in FLEX. (j) Cap and lenticule cut in SMILE using.
Side view: (b) Cornea after epithelial removal in surface ablation. (c) Excimer laser ablation of the stroma in
surface ablation. (e) Flap cut in LASIK. (f) Flap lift and subsequent excimer laser ablation on the stroma in
LASIK. (h) Flap and lenticule cut in FLEX. (i) Flap lift and lenticule removal in FLEX. (k) Cap and lenticule cut,
and side cut in SMILE. (l) Lenticule removal through the side cut in SMILE.
LASIK
LASIK was introduced in early 1990s.360, 361 Shortly after its introduction, it became the
dominant procedure in corneal refractive surgery.362 In LASIK, a microkeratome or an FS
laser is used to cut a hinged corneal flap, followed by excimer ablation on the stromal bed and
finally repositioning of the flap (Fig 10).360, 361 Keeping the central corneal epithelium intact
increases comfort during the early postoperative period, and reduces the wound healing
response, which correlates with a lower rate of haze development.343, 363, 364 Studies have
shown that LASIK is safe, effective, and predictable for treating myopia and myopic
astigmatism.365, 366
While the microkeratome performs the cutting, the FS laser creates incisions by both
cleaving (blunt wedge dissection) and ablation (subtractive dissection). Peak laser energy
forms plasma, which causes ablation, then the shock wave with a cavitation bubble causes
cleavage. Thousands of laser pulses are connected together in a raster pattern to create a
cleavage plane. The lowest possible energy from FS laser that still can produce plasma is
preferred to avoid the side effects of heating. Reduction in pulse duration (higher frequency),
reduction in beam diameter, and use of shorter wavelengths are preferred to achieve the

52
smoothest possible FS laser cuts. The application of FS laser to LASIK flap creation has
increased greatly since its introduction. It has been suggested that the use of FS laser for flap
creation has improved the safety and predictability of the lamellar incision step367 and it yields
a more uniform interface and more adherent fit to stromal bed,368 resulting in a reduced risk of
postoperative complications as well as reduced variability in the level of optical scattering.369
The use of the FS laser has also reduced the complications such as epithelial ingrowth and
flap striae, however, other specific complications have emerged, such as vertical gas
breakthrough, opaque bubble layer, and transient light-sensitivity syndrome.367
Although rare, flap or interface complications such as incomplete, decentered,
buttonholed or lacerated flaps, improperly replaced free-cap, striae, wrinkles or folds along
with diffuse lamellar keratitis (DLK) or recurrent epithelial ingrowth, can lead to visually
disturbing irregular astigmatism and/or optical scattering,370 thereby resulting in a reduced
visual performance such as haloes/glare, multiplopia, starburst, and decreased CDVA.114, 371
Treatment of the inferior visual performance occurring with LASIK flap or interface
complications remains one of the most difficult challenges in refractive surgery. Since the
source of the inferior vision could be either irregular astigmatism caused by the underlying
pathology (irregular flap, wrinkles, folds, scarring after DLK, epithelial ingrowths, etc.) or the
optical scattering (within the flap, LASIK interface, or both), an ideal treatment will require: 1)
Measurement technologies to map the location and the depth of the pathology to be ablated;
and 2) Topography-guided treatment technology to regularize the corneal surface and treat the
irregular corneal optics with minimal waste of corneal tissue.
Re-lifting of the original flap and performing laser ablation on the original stromal bed,
which is the most commonly used and effective method for treatment of residual refractive
errors after LASIK, will not be the right approach in cases where the pathology lies within the
flap, because that pathology would remain untouched. Various types of traditional surface
ablation (that include epithelial removal) on top of the flap have been used for the treatment
of LASIK complications.372-374 However, they do not take into account one factor that may
increase the unpredictability of the outcomes: epithelial remodelling. As described earlier, the
epithelium grows thicker over depressed stroma and thinner over elevated stroma in an
attempt to re-establish a smoother and more symmetrical corneal optical surface.189 This
masking effect causes a discrepancy in morphology between the epithelial and stromal surface
(Fig 11). Due to the mentioned discrepancy, topography-guided surface ablations, if
performed after epithelial removal, will result in erroneous ablation, because the treatment
plan is based on preoperative topography measured on the epithelium-covered corneal surface,

53
while the treatment itself is applied on the stromal surface.
Figure 11. Topography-guided surface ablation in treatment of subepithelial irregularity masked by epithelial
remodelling. (a) Epithelium masking a stromal irregularity; (b) Mechanical or alcohol-aided epithelial removal
exposes irregular surface; (c) When topography representing the epithelial surface is used as the basis for the
treatment planning, and the treatment itself is performed on the stroma after the epithelial removal, a new
irregular surface is produced; (d) When the same topography is used for planning of transepithelial ablation
that removes both the epithelium and the stroma as a single entity, a regularized surface shape will be
“transferred” to the stroma below the irregularity (dotted line).
Transepithelial phototherapeutic keratectomy (T-PTK) will “transfer” the epithelial
shape to stroma and eliminate the discrepancy between epithelial and stromal surfaces,193
54
under the assumption of similar ablation rate between epithelium and stroma. Topography-
guided ablation combined with T-PTK, as Custom Transepithelial “no-touch” (cTEN)
ablation, will treat the surface irregularities, as well as the possible refractive errors, to
achieve the targeted corneal morphology and optics.375, 376 Structural imaging technology,
such as OCT, which can precisely map the epithelial depth as well as the flap pathology, can
further facilitate the topography-guided transepithelial ablation in treatment of post-LASIK
corneal irregularities.377 In conclusion, a treatment combing T-PTK with topography-guided
ablation with the assistance of corneal structural imaging system may be an ideal tool for the
treatment of damaged corneal optics following LASIK-flap or interface complications.
Refractive Lenticule Extraction (ReLEx)
FS laser creates corneal incisions, which are lamellar (used for LASIK-flap creation), as well
as vertical and curved. As previously mentioned, in recent years, FS laser has largely replaced
mechanical microkeratome in LASIK-flap creation due to its high safety, efficiency, precision
and versatility in creation of lamellar incisions.378
Lately, a new application of the FS laser, termed refractive lenticule extraction
(ReLEx),379 has been developed for corneal refractive surgery. In ReLEx, the FS laser is used
to create an intra-stromal refractive lenticule. Depending on the technique for the subsequent
lenticule removal, ReLEx can be performed by using two procedures: FS lenticule extraction
(FLEX) and small-incision lenticule extraction (SMILE). In FLEX which is mostly
considered an evolutionary step towards SMILE, a LASIK-like flap is created to access and
remove the refractive lenticule. Whereas in SMILE, no flap is created and the lenticule is
extracted through a 2 to 4 mm long side cut.380-383 (Figure 10)
To create a refractive-accurate lenticule, the accuracy of the FS laser interface cut
must be sufficiently high. Currently, the ReLEx procedures can only be carried out with the
VisuMax FS laser (Carl Zeiss Meditec AG, Jena, Germany) due to its high reproducibility,
regularity and uniformity.384-387 Laser parameters (i.e., pulse energy, spot distance,
frequency)388 and laser-firing patterns389, 390 in VisuMax have been refined to improve the
surface quality and the optical quality of the lenticules to make procedures like ReLEx
SMILE possible. More advanced surgical maneuvers are needed in SMILE compared to
FLEX to separate the lenticule from overlying and underlying stroma through a small
incision. Still, the SMILE is the procedure of choice with VisuMax due to its concept of
keeping the anterior cornea untouched and minimizing trauma to the corneal surface. 22, 225, 391,
392

55
SMILE and LASIK have common advantages of minimal postoperative pain and
relatively quick postoperative visual recovery, compared to surface ablation. Therefore,
comparisons are frequently made between these two procedures. Unlike in LASIK, where the
performance of the excimer laser ablation can be affected by the variation in ambient
humidity and stromal hydration change during the surgery,393-395 the refractive lenticule cut by
FS laser in SMILE is executed prior to any interference with stroma. This may contribute to a
greater predictability in refractive outcomes.380, 396 Long-term refractive and visual outcomes
are comparable or in favour of SMILE compared to FS-LASIK;383, 397, 398 however, the visual
recovery after SMILE is usually a little slower than after LASIK.383, 390 The reason for the
delayed recovery is still not clear. In vivo confocal microscopy demonstrated a greater
increase of backscattered light intensity after SMILE compared to FS-LASIK at one week,
one month, and three months, postoperatively.399 More micro distortions in Bowman´s layer
were also observed by OCT after SMILE than after FS-LASIK. Both the interface scatter and
micro distortions in Bowman´s layer may contribute to the slightly reduced visual acuity in
the early postoperative period.
One potential limitation of the SMILE technique is that no automatic eye
registration/tracking is used during the procedure, which may increase the risk of decentration
and induction of higher order aberrations. Lack of torsional alignment control may also
reduce the effect of astigmatic correction. By analyzing the pre-/postoperative anterior
elevation difference maps, Li et al. 400 reported a mean of 0.17± 0.09 mm decentration with
SMILE, which was associated with induction of postoperative coma. Nevertheless, a study by
Lazaridis et al.401 demonstrated that the centration of the treatment zone measured by a
Pentacam thickness difference map was better for patient-controlled fixation during SMILE
than active eye tracker-assisted FS-LASIK (0.315±0.211 mm vs. 0.516 ± 0.254 mm). Some
studies found less induction of HOAs after FLEX381-383 and SMILE397, 398 compared to FS-
LASIK, and postoperative contrast sensitivity was reported to be better after SMILE
compared to FS-LASIK.381, 397 Regarding the myopic astigmatism correction, Ivarsen et al.402
reported a small under-correction of 13% per diopter of attempted correction in low
astigmatism, and 16% per diopter of attempted correction in high astigmatism.
Biomechanical tensile strength of the anterior central corneal stroma was found to be
nearly twice that of the posterior stroma.70, 71, 297, 403 With SMILE, preservation of the most
superficial stroma is expected to provide the least disturbance to corneal biomechanics,404
compared to both LASIK and surface ablation. Mathematical model by Reinstein et al.405 and
a finite-element anisotropic collagen fiber-dependent model of myopic surgery by Sinha Roy

56
et al.404 demonstrated that the SMILE may cause less biomechanical weakening to the cornea
than comparable corrections involving LASIK flaps. Clinical in vivo measurements with ORA
failed to detect differences in induced changes in CH and CRF between SMILE and FS-
LASIK,406 or between SMILE and FLEX.235, 407 However, some studies408, 409 found less of a
decrease of CH, CRF after SMILE than LASIK. Another study comparing the corneal
deformation parameters after SMILE, LASEK and FS-LASIK measured with CorVis
dynamic Scheimpflug analyzer reported significant higher deformation amplitude, and shorter
1st applanation time after FS-LASIK compared to LASEK, whereas no significant differences
were detected in these two variables between LASEK and SMILE groups, or between the
SMILE and FS-LASIK groups.288 It remains to be explored whether the discretions between
theoretical model and different clinical measurements were due to the insensitivity of the
parameters used for measuring corneal biomechanics or the study population.
Disruption of the corneal nerves is one of the contributing factors for postoperative
dry eye.410 The combination of a large circumferential cut through the corneal surface during
flap making with subsequent excimer photoablation of the stroma in LASIK significantly
severs the corneal nerves.411 The decrease in corneal sensation after FS-LASIK and FLEX has
been reported to be similar, because they both require the creation of a flap.225 The
substantially shorter side cut used for lenticule extraction in SMILE may lead to better
preservation of anterior corneal nerves and reduce the incidence of postoperative dry eye
symptoms. The SMILE technique resulted in less anterior stromal nerve plexus disruption and
significantly less reduction in corneal sensation compared to FS-LASIK and FLEX.225, 384, 412-
414 The other dry eye tests, such as tear break-up time (TBUT), Schirmer test, tear osmolarity,
and subjective symptoms showed comparable results or in favour of SMILE.413, 415, 416
One potential advantage of the SMILE technique is that the removed lenticule allows
the possibility of re-implantation at a future time. Pradhan et al.417 first described
endokeratophakia, in which a SMILE lenticule from a myopic patient was implanted into a
recipient eye through a small incision to correct hyperopia. Thereafter, Ganesh et al.418
introduced the technique of cryopreservation of corneal lenticules extracted after SMILE,
which can be implanted into an FS laser-created intra-stromal pocket for hyperopic
correction.
Perioperative complications of SMILE include minor epithelial abrasions at the
incision, difficulties in removing the lenticule, small tears at the incision, cap perforation,
central epithelial abrasion, suction loss, and remnant intrastromal lenticule.419-421 The
postoperative complications include haze, dryness of the corneal surface, interface

57
inflammation, interface infiltrates, epithelial ingrowth, and irregular astigmatism.421 Loss in
CDVA seemed to depend on laser settings (lower spot energy and closer spacing compared to
higher spot energy and wider spacing has resulted in higher loss) and the skill of the
surgeon.421 Although the percentage of eyes with loss in CDVA was relatively high after three
months, CDVA was restored to preoperative values in all eyes after approximately one year.
Retreatments after SMILE are currently performed with surface ablation, or with LASIK by
converting the cap into a flap using a Circle-cut. Topography-guided PRK was used to
successfully treat visually disturbing irregular astigmatism after SMILE in some cases.422
However, subepithelial haze development in PRK performed on SMILE-cap appears to be a
challenge, even in cases with limited ablation depth. The authors suggested an extended time
span between SMILE and PRK and perioperative application of mitomycin C in order to
reduce the incidence of haze formation. Lately, Donate and Thaeron423 also introduced a sub-
cap-lenticule-extraction technique that permits the surgeon to use the previously created
interface as the new superior plane of the new lenticule for enhancement.
5.6.2 Treatment of Keratoconus The treatment of keratoconus is aimed at halting the progression of the disease and achieving
visual rehabilitation.
5.6.2.1 Conservative treatment In the early stages, the refractive error in keratoconus can usually be corrected to a
satisfactory level by the use of spectacles and/or soft contact lenses. As the disease advances,
the changes in corneal shape and consequent irregular astigmatism result in suboptimal visual
quality with spherocylindrical correction, necessitating the use of hard contact lenses. Hard
lenses may be adequate to provide clear vision at that point, but when the cornea becomes
scarred or too steep, as the condition progresses, special contact lens designs becomes a
necessity, with so called intralimbal hard lenses or miniscleral lenses for moderate cases and
scleral lenses for advanced cases with large, decentered cones.424, 425 Other designs include
piggyback lenses that involve fitting of a soft lens underneath a hard lens, and hybrid contact
lenses, which have a hard lens in the center and a soft skirt. A global consensus group315 made
the following guidelines for nonsurgical management of keratoconus:
• Guidance should be given to patients regarding the importance of not rubbing one’s
eyes, the use of topical anti-allergic medication in patients with allergy, and the use of

58
preservative-free topical lubricants in the case of ocular irritation to decrease the
impulse to eye rub.
• Spectacle correction based on subjective refraction and aberrometry for optical
correction in early disease.
• Contact and scleral lenses, although they do not slow or halt progression of
keratectasia, are very important in visual rehabilitation in keratoconus:
o Rigid contact lenses should be used in cases of unsatisfactory vision with
glasses or conventional soft contact lenses. Rigid-gas-permeable lenses (RGP)
are preferred and should be tried initially.
o In a patient who has failed RGPs, alternative contact lens options would be:
hybrid lens (rigid center, soft skirt); toric, bitoric, and keratoconus design soft
contact lens; keratoconus design corneal rigid gas-permeable contact lens;
piggy-back; corneoscleral, miniscleral, and semiscleral contact lens; and
scleral lens
5.6.2.2 Surgical options Intracorneal Ring Segments (ICRS) Implantation
ICRS are implanted in order to improve the irregular astigmatism by “stretching” and
levelling of the corneal surface. Clinical studies reported a significant flattening of the central
cornea, with improvement in uncorrected and corrected distance visual acuity after
implantation of ICRS.138, 426-429 An improvement in contact lens-tolerance by regularization of
the anterior corneal contour is another benefit that may be obtained from this procedure.
Corneal Transplantation
In advanced keratoconus with deep corneal scarring, very protuberant cones and very thin
cornea, where CXL and/or ICRS are not viable and contact lenses not tolerated, corneal
transplantation is eventually necessary for visual rehabilitation, especially if the vision in the
other eye is significantly impaired as well. Penetrating keratoplasty (PKP), which involves the
full-thickness removal of the patient’s central cornea and replacement with a graft, has been
successfully used for several decades.430-433 Data from the Australian Corneal Graft Registry,
one of the largest graft registries, show a 91% successful graft rate 1 year post PKP and a
74% success rate at 5 years for all diagnoses that are normally indicated for corneal graft.434
Deep anterior lamellar keratoplasty is a surgical procedure that involves removal of the
59
corneal stroma down to Descemet’s membrane and replacement with a donor cornea.435, 436
This technique offers an alternative to PKP with a lower risk of graft rejection, potentially
earlier visual rehabilitation, and better wound strength.435-437
Low Invasive Option - Corneal Collagen Cross-linking (CXL)
The decrease in rigidity of the keratoconic cornea is attributed to the decrease and
disorganization of the collagen network within the stroma. Corneal collagen cross-linking
with riboflavin/ultraviolet-A (UVA, 370 nm), introduced a decade ago, is a minimally
invasive procedure for the treatment of keratectasia via increasing the mechanical and
biomechanical stability of the stromal tissue.438-442 The aim of CXL is to halt or slow down
the progression of keratoconus by creating additional chemical cross-links between collagen
fibrils and other extracellular matrix proteins in the corneal stroma through localized photo
polymerization.443-445 Lately, CXL has also been combined with surgical optical corrections,
such as ICRS and photorefractive keratectomy (PRK), in order to halt the development of
keratoconus and at the same time also to improve visual acuity rather than just preserve the
current state.446, 447
In CXL, exposure of the riboflavin to UVA-irradiation results in absorption of energy
and its excitement into a triplet state that undergoes either an aerobic, type 2 reaction, or an
anaerobic, type 1 reaction.448 According to Kamaev and colleagues,448 an oxygenated
environment causes the formation of singlet molecular oxygen, which then acts on tissues to
produce additional cross-linked bonds. After a quick consumption of oxygen, which occurs
only within several seconds, depending on UV-power and temperature, among other factors,
it is suggested that the main photochemical kinetics mechanism is the direct interaction
between the riboflavin triplets and reactive groups of corneal proteins, which leads to cross-
linking of the proteins, mainly through radical reactions.448 These then induce the formation
of new covalent bonds between the amino acids among the neighbouring collagen
molecules449, 450 and among proteoglycan (PG) core proteins, as well as limited linkages
between collagen and PG core proteins.451 Concurrently, riboflavin also offers a shielding
effect to the deeper ocular structures, such as the corneal endothelium, the lens and the
retina.452
The “standard protocol” of CXL described by Wollensak and colleagues450 consists of
removal of the corneal epithelium in a diameter of 9 mm, and saturation of the cornea by
applying drops of 0.1% isotonic riboflavin solution in 20% dextran solution. The cornea is
then exposed to UVA light (365 nm) with an irradiance of 3 mW/cm2 for 30 minutes, which

60
corresponds to a total radiant exposure of the cornea of 5.4 J/cm2. The corneal epithelium
with its tight junctions and hydrophobic character is the most important barrier to penetration
of hydrophilic macromolecules like riboflavin.453 Thus, with the conventional CXL, removal
of the intact corneal epithelium before the application of riboflavin is considered crucial to
enable sufficient intrastromal diffusion of riboflavin.443, 454, 455
The safety and efficacy of the conventional CXL has been confirmed by numerous
studies.450, 452, 454, 456, 457 However, the epithelial removal seems to be responsible for most of
the complications reported to date with CXL.458 To avoid potential complications due to
epithelial removal, Boxer-Wachler and Pinelli suggested a modification of the technique with
the epithelium kept intact (epithelium on).459 Substances such as benzalkonium chloride,
ethylenediaminetetraacetic acid (EDTA) and trometamol, especially when combined, enhance
epithelial permeability of hydrophilic macromolecules, such as riboflavin.460-463 By adding
enhancers to help riboflavin penetrate into the corneal stroma through the intact epithelium,
CXL can be performed without epithelial debridement (transepithelial CXL).464 In a non-
randomized comparative study, Pinelli and colleagues reported no significant difference in the
analyzed parameters between the “epithelium-on” group and the standard one.458
Transepithelial CXL has been proposed (but not proven) to reduce early postoperative pain,
temporary worsening of vision, as well as complications such as infectious keratitis after
conventional CXL.465 Additionally, thinner corneas may be treated safer by transepithelial
compared to the conventional CXL, since the endothelium is better protected by UVA-
filtering effect of the intact epithelium. Meanwhile, strong doubts were raised concerning the
efficacy of the transepithelial (“epithelium-on”) CXL.466
The critical limitation of CXL in thin corneas is the lack of sufficient corneal thickness
for the UVA-radiation to be absorbed and attenuated before it reaches the endothelium. The
cell damage threshold of UVA-irradiation combined with riboflavin is 10 times higher than
with UVA-irradiation alone.467 Wollensak et al.467 demonstrated that when the combination of
UVA and riboflavin is used in corneas thinner than 400 µm, the cytotoxicity threshold of 0.35
mW/cm2 for the endothelial cell damage can be reached. In conventional CXL procedure, the
treatment parameters (0.1% riboflavin- dextran 20.0% solution and 3 mW/cm2 of UVA for 30
minutes) are assumed to treat the anterior 300 µm of the corneal stroma.454, 468 Hence, only
patients with a de-epithelialized corneal thickness of at least 400 µm are subjected to this
treatment. The downside of this limitation is that eyes with advanced stages of keratectasia
often have corneas thinner than 400 µm. Populations of Asian and African origin with
inherently thinner corneas469, 470 may be especially affected by this limitation. Various
61
modifications have been suggested to circumvent that, including application of hypoosmolar
riboflavin solution,471 transepithelial CXL,464, 472 CXL with custom epithelial debridement,473
and contact lens-assisted CXL.474
Conventional Collagen Cross-linking
Kymionis et al.475 applied conventional CXL procedure in 14 thin corneas with minimum
corneal thickness of less than 400 µm (range 340-399 µm) after epithelial removal.
Improvement in UDVA, CDVA, and reduction in mean keratometry readings were recorded
during the 12 months follow-up. However, despite the absence of clinically evident
complications, significant reduction of endothelial cell density from 2733 to 2411 cells/mm2
was observed postoperatively. The film of 0.1% isoosmolar riboflavin with 20% dextran was
measured to be approximately 70 µm thick after 1 minute of instillation and remained stable
for 22 minutes.476 With the riboflavin-dextran film, the UVA irradiance in human corneal
stroma at 400 µm was measured as 0.21 mW/cm2, which is much lower than the previously
mentioned cytotoxicity level on which the set limitation of minimal deepithelialized stromal
thickness of 400 µm is based. Hence, the absorption and shielding of UVA by the riboflavin
film may have prevented damage to the endothelium. Nevertheless, a longer follow-up and
larger patient series are essential to evaluate the safety and efficacy of conventional CXL in
clinical application in thin corneas.
Hypoosmolar Riboflavin Solution
The cornea has an inert swelling pressure,477 meaning that the corneal stroma has the
tendency to increase its volume in an isooncotic environment. The deepithelialized cornea can
swell to double its normal thickness when irrigated with a hypoosmolar solution.478 Hafezi
and co-workers479 applied this method to increase corneal thickness before CXL in thin
corneas. After epithelial removal, 0.1%-20% dextran isoosmolar riboflavin was applied to the
cornea for 30 minutes. The 0.1% dextran-free hypoosmolar riboflavin was then administered
until the corneal thickness at the thinnest point reached 400 µm, before the initiation of UVA
irradiation. The authors reported a stabilization of keratectasia in 20 eyes treated with this
approach. A later study by Raiskup et al.471 applied 0.1% hypoosmolar riboflavin after
epithelial debridement until the riboflavin saturated cornea reached the minimum of 400 µm.
In this study, one year after the treatment, CDVA and keratometric value remained unchanged
and no damage to the cornea in the form of detectable scarring lesions in the stroma was
registered. Similar results were reported by Wu et al.480 On the contrary, in eyes treated with
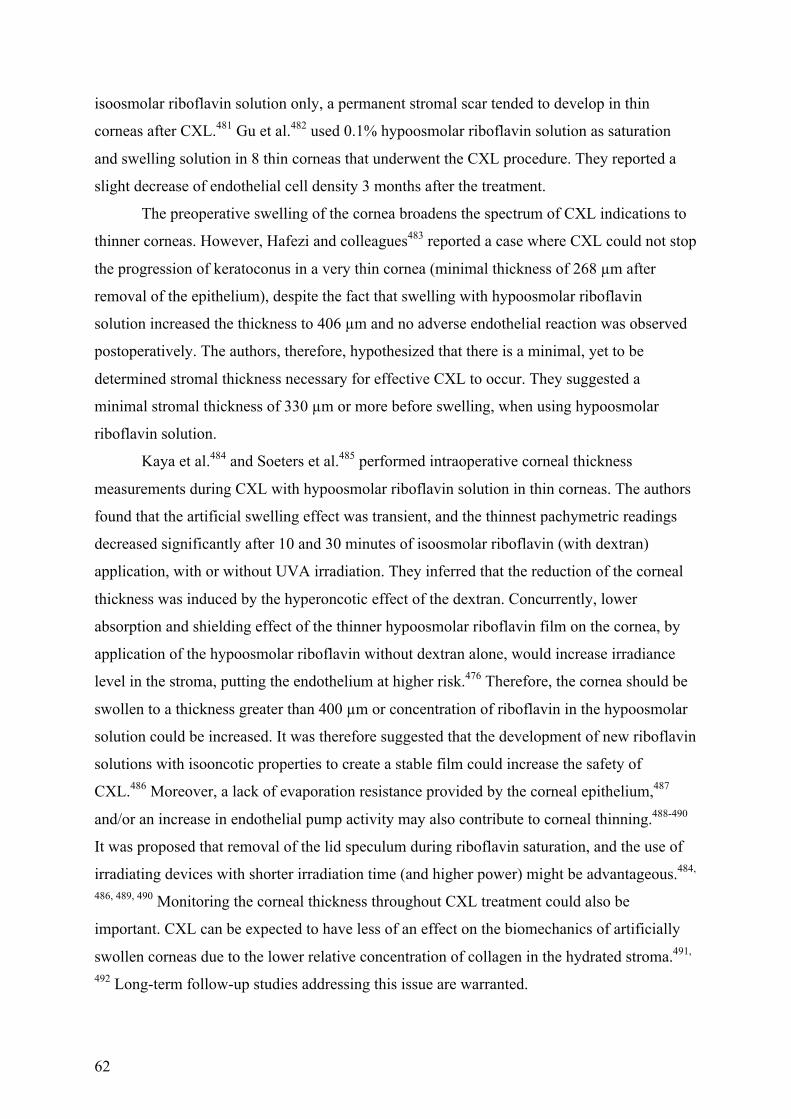
62
isoosmolar riboflavin solution only, a permanent stromal scar tended to develop in thin
corneas after CXL.481 Gu et al.482 used 0.1% hypoosmolar riboflavin solution as saturation
and swelling solution in 8 thin corneas that underwent the CXL procedure. They reported a
slight decrease of endothelial cell density 3 months after the treatment.
The preoperative swelling of the cornea broadens the spectrum of CXL indications to
thinner corneas. However, Hafezi and colleagues483 reported a case where CXL could not stop
the progression of keratoconus in a very thin cornea (minimal thickness of 268 µm after
removal of the epithelium), despite the fact that swelling with hypoosmolar riboflavin
solution increased the thickness to 406 µm and no adverse endothelial reaction was observed
postoperatively. The authors, therefore, hypothesized that there is a minimal, yet to be
determined stromal thickness necessary for effective CXL to occur. They suggested a
minimal stromal thickness of 330 µm or more before swelling, when using hypoosmolar
riboflavin solution.
Kaya et al.484 and Soeters et al.485 performed intraoperative corneal thickness
measurements during CXL with hypoosmolar riboflavin solution in thin corneas. The authors
found that the artificial swelling effect was transient, and the thinnest pachymetric readings
decreased significantly after 10 and 30 minutes of isoosmolar riboflavin (with dextran)
application, with or without UVA irradiation. They inferred that the reduction of the corneal
thickness was induced by the hyperoncotic effect of the dextran. Concurrently, lower
absorption and shielding effect of the thinner hypoosmolar riboflavin film on the cornea, by
application of the hypoosmolar riboflavin without dextran alone, would increase irradiance
level in the stroma, putting the endothelium at higher risk.476 Therefore, the cornea should be
swollen to a thickness greater than 400 µm or concentration of riboflavin in the hypoosmolar
solution could be increased. It was therefore suggested that the development of new riboflavin
solutions with isooncotic properties to create a stable film could increase the safety of
CXL.486 Moreover, a lack of evaporation resistance provided by the corneal epithelium,487
and/or an increase in endothelial pump activity may also contribute to corneal thinning.488-490
It was proposed that removal of the lid speculum during riboflavin saturation, and the use of
irradiating devices with shorter irradiation time (and higher power) might be advantageous.484,
486, 489, 490 Monitoring the corneal thickness throughout CXL treatment could also be
important. CXL can be expected to have less of an effect on the biomechanics of artificially
swollen corneas due to the lower relative concentration of collagen in the hydrated stroma.491,
492 Long-term follow-up studies addressing this issue are warranted.

63
Transepithelial Collagen Cross-linking
In a bilateral study, Filippello et al. used trometamol and sodium EDTA as enhancers and
applied transepithelial CXL in 20 keratectatic eyes with a mean corneal thickness (including
epithelium) of 412±21 µm.464 The transepithelial CXL treatment appeared to halt the
progression of keratoconus in all treated eyes over 18 months follow-up. It also yielded
statistically significant improvements in all visual and topographic outcome measures,
whereas the contralateral untreated eyes demonstrated worsening of all parameters. Spadea et
al.,493 who used a similar protocol in thin corneas, confirmed its effect in the stabilization of
keratoconic eyes. However, the visual and topographic improvement was minimal. No
endothelial cell damage was observed in either of the studies.
Wollensak et al. estimated a 64% increase in corneal rigidity in human corneas with
transepithelial CXL using topical anesthetics and benzalkonium chloride as enhancers, versus
a 320% increase when using CXL with de-epithelialization.494 The safety and reproducibility
of the study by Filippello et al. have recently been questioned495 since the postoperative
demarcation line depth in their study464 was only approximately 100 µm, in contrast to about
300 µm in conventional CXL with epithelial debridement. It is unclear whether the shallower
demarcation line using the transepithelial approach was due to limited penetration of
riboflavin into the stroma or that it was a result of reduced UVA-light penetration by
shielding from riboflavin-impregnated intact corneal epithelium. Iontophoresis-assisted
transepithelial CXL, using a non-invasive delivery system based on a small electric current,
was recently designed to enhance the penetration of riboflavin into the corneal stroma.472
Preclinical results showed that the iontophoresis was able to increase the concentration of
riboflavin in the corneal stroma compared to enhancer-assisted transepithelial CXL, but did
not reach concentrations previously reached with conventional epithelium-off CXL. The
demarcation line after iontophoresis-assisted transepithelial CXL appeared to be less easily
distinguishable and shallower than in conventional CXL; however, it demonstrated features
more similar to that after conventional CXL in terms of depth and visualization, compared to
enhancer-assisted transepithelial CXL.496, 494 In general, there is consensus within the
scientific community that the current transepithelial CXL protocols are not as effective as
conventional epithelium-off CXL.462, 463, 497
Custom Epithelial Debridement Technique
Kymionis et al.473 performed CXL with custom pachymetry-guided epithelial debridement in
one keratoconic eye and one post-LASIK keratectatic eye with the thinnest stroma of less than

64
400 µm. In this modified CXL approach, 8.0 mm diameter of corneal epithelium was
removed, leaving a small, localized area of corneal epithelium corresponding to the thinnest
area over the apex of the cone. The authors suggested the use of hypoosmolar riboflavin
during UVA-irradiation to avoid corneal stromal dehydration as well as to maintain the
stromal riboflavin concentration. Nine months postoperatively, the topography remained
stable, and no endothelial cell density alteration was detected in the treated eyes. However, a
later study by Kaya et al.498 suggested that the epithelium over the cone area spared the
stroma underneath from the CXL effect. Four weeks after the treatment, stromal haze and
demarcation line were detected in the corneal areas with epithelial debridement, but not in the
areas with intact epithelium; de-epithelialized stroma outside the cone region displayed total
keratocyte apoptosis and honeycomb-like edema, whereas it was minimal beneath the intact
epithelium.498 In contrast, Mazzotta et al.499 demonstrated keratocyte apoptosis at an average
depth of 160 µm under the epithelial island compared to 250 µm under the de-epithelialized
area in 10 eyes with a 1-year follow-up.
A previous study demonstrated that the stromal uptake of riboflavin after grid pattern
full-thickness epithelial debridement was heterogeneous, with full penetration to the stroma
immediately beneath the areas of epithelial debridement and no penetration to the stroma
beneath the intact epithelium.500 Inadequate riboflavin saturation together with the ability of
the epithelium to absorb the UVA radiation501 may lead to reduced CXL effect in the cone
area and affect the efficacy of the whole procedure. The long-term efficacy of this modified
CXL procedure with a larger number of patients needs to be assessed.
Contact Lens-assisted Collagen Cross-linking
Contact lens-assisted CXL (CACXL) was introduced by Jacob et al.474 A Soflens daily
disposable soft contact lens (14 mm diameter, 8.6 mm basal curvature; Bausch & Lomb) with
a thickness of 90 µm, made of hilafilcon and without a UV filter, was immersed in isoosmolar
riboflavin 0.1% in dextran for 30 minutes, before it was applied onto the de-epithelialized,
riboflavin-saturated cornea. The UVA-radiation of 3.0 mW/cm2 for 30 minutes was initiated
after confirmation that the minimum corneal thickness including the contact lens and
riboflavin film was greater than 400 µm. The riboflavin solution was instilled every 3 minutes
during the UVA-radiation to maintain corneal saturation and to keep the pre-corneal and pre-
contact lens riboflavin film uniform. The pre-corneal riboflavin film with contact lens created
an absorption medium in the pre-corneal space by artificially increasing the thickness of the
“riboflavin-filter”.

65
In the 14 eyes treated with CACXL, the authors reported an average increase of the
minimum corneal thickness by 108 µm if the contact lens and riboflavin film were included.
At a mean follow-up time of 6.1±0.3 months (range: 6-7 months), the mean postoperative
depth of the stromal demarcation line was measured at 252.9 µm. No significant endothelium
loss or signs of postoperative endothelial damage were observed. No significant change in the
CDVA, or mean maximum keratometric value was detected postoperatively, although 1 D
decrease of maximum keratometric value was observed in 4 eyes (28.5%).
The advantage of CACXL is that it is not dependent on the swelling properties of the
cornea and that the cornea is not subjected to edema, which may cause Descemet membrane
folds and endothelial damage. However, the surface irradiance at the level of the corneal
stroma is reduced by 40% to 50% in CACXL secondary to absorption by the riboflavin film
and soaked contact lens. Furthermore, oxygen diffusion, which has been demonstrated to be
crucial in the CXL process, might be hindered by the contact lens. As a result, the effect of
CXL may be reduced. The small patient population, short follow-up and absence of a control
group are the limitations of the study.
The overall safety of the protocols for CXL in thin corneas presented above is good, as
most of them managed to halt the progression of keratectasia without postoperative
complications. Furthermore, modification of the tonicity and concentration of the
photosensitizing riboflavin and modification of the UV energy and/or power have been
proposed. Iseli et al.502 suggested that a higher riboflavin concentration may be applied for
improved protective screening of the endothelium in thin corneas. Accelerated CXL (UVA
irradiation at 30 mW/cm2 for 3 minutes) has recently been reported to stabilize the
progression of keratoconus in 34 thin corneas, without endothelial cell density loss during the
12 months of follow-up.503 Furthermore, in accelerated CXL, pulsed UV light seems to result
in a higher effect compared to continuous UV light, presumably due to the optimization of
oxygen availability.504 Oxygen concentrations measured in the corneal stroma showed that the
certain combination of “on” and “off” time would facilitate the continuous replenishment of
oxygen,505 leading to an increased CXL effect without the necessity to increase UV energy.506
Thus, using the pulsed mode during UVA irradiation may maximize the efficacy of CXL,
while maintaining or improving the safety profile of the procedure. This may be especially
beneficial in treating thin corneas.
The evidence of safety and efficacy regarding the use of modified CXL protocols is
still limited to a handful of studies. Future long-term follow-up studies with a larger number
of participants are warranted.
66
5.6.3 CXL in Combination with Excimer Laser Custom Ablation Labiris et al.507 studied the negative impact of keratoconus on quality of life. They reported
that keratoconus deteriorates vision even in stage one, with or without decreased best-
corrected visual acuity due to coma-dominant irregular astigmatism, and light scatter.
Therefore, besides the corneal biomechanical instability, the visual impact of the irregular
astigmatism must be taken into consideration in the treatment of keratoconus.
Customized ablation has been shown to be promising in reducing irregular
astigmatism and improving visual acuity in non-keratoconic eyes.376, 508 It is generally
considered that keratoconus or subclinical keratoconus are absolute contraindications to
LASIK,509 whereas some studies demonstrated that PRK in selected cases of latent and forme
fruste keratoconus to a maximum grade two was safe and effective.510-515 Khochtali et al.516
reported a case where one eye of a patient underwent PRK, while keratoconus developed in
the untreated eye. They postulated that: 1) the ablation of the central anterior stroma and
Bowman`s layer, where histopathologic alterations are prevalently seen in keratoconus, may
halt the disease; and 2) the excimer laser ablation of the cornea may have a similar stiffening
effect to corneal collagen cross-linking. Nevertheless, concerns remain that tissue removal by
PRK may further decrease the biomechanical strength of the already weakened keratoconic
cornea, increasing the risk for progression of the disease. Since CXL has been shown to
successfully retard or eliminate the progression of keratoconus, a combined treatment may
achieve both optical regularization and biomechanical stabilization of the cornea.
The PRK and CXL can be performed separately with some time interval or
simultaneously at the same day. Kanellopolous et al.517 compared CXL with subsequent
topography-guided PRK performed 6 months later, with the CXL and PRK performed in a
combined procedure on the same day. The authors concluded that same-day simultaneous
topography-guided PRK and CXL performed superiorly with a better CDVA, greater
spherical equivalent and keratometric reduction, and less corneal haze. Another two factors
make a simultaneous combined procedure appealing: 1) the patients can avoid two separate
surgeries and 2) subsequent PRK ablation of the previously cross-linked anterior cornea is
avoided.517
The simultaneous combination of PRK with CXL proved to result in better UDVA,
lower refractive error, and lower keratometric values than the CXL alone.518 Furthermore, the
incidence of haze was reportedly minimal after this procedure,519 due to depopulation of

67
keratocytes in the cross-linked anterior stroma, which may reduce the possibility of haze
formation.520, 521
PRK before CXL generally includes epithelial removal by using 20% alcohol,517 a
surgical brush,519 or an excimer laser,518, 522 and laser ablation itself with517, 519 or without522
the application of Mitomycin-C 0.02% at the end. A limit of maximum ablation depth of
around 50 µm is considered to ensure enough residual stromal thickness for a safe subsequent
CXL procedure.517, 521, 523, 524
Preliminary results suggest that when certain precautions are met, the safety and
efficacy profiles of the simultaneous combined treatment of PRK with CXL are excellent.517-
519, 521, 522, 525, 526 This technique is also applied to post-LASIK ectasia and pellucid marginal
degeneration,527, 528 after excimer laser-assisted lamellar keratoplasty for keratoconus,529
immediately after530 or sequentially525, 531 after the implantation of ICRS.
The aforementioned global keratoconus consensus group summarized their recommendations
for the surgical treatments of keratoconus as follows:315
Different Case Scenarios:
• Young (e.g., 15-year-old) patient with stable keratoconus with satisfactory vision with
glasses: Prescribe glasses only or in combination with contact lenses or CXL
• Young (e.g., 15-year-old) patient with progressive keratoconus with satisfactory
vision with glasses: Perform CXL and prescribe glasses or contact lenses
• Older (e.g., 55-year-old) patient with stable keratoconus with satisfactory vision with
glasses: Prescribe glasses only or with contact lenses.
• Older (e.g., 55-year-old) patient with progressive keratoconus with satisfactory vision
with glasses: Perform CXL only or with prescription of glasses/contact lenses.
• Patient with stable keratoconus with unsatisfactory vision with glasses but satisfactory
vision with rigid contact lenses and tolerates them well: Prescribe contact lenses
(including scleral lenses).

68
• Patient with stable keratoconus with unsatisfactory vision with glasses and contact and
scleral lenses, or who does not tolerate contact or scleral lenses: Perform lamellar
keratoplasty. Consider ICRS in eyes with adequate corneal thickness and minimal to
no scarring.
• Patient with stable severe keratoconus with unsatisfactory vision with glasses and
contact and scleral lenses (this patient has moderate anterior corneal scarring but no
evidence of previous corneal hydrops): Perform lamellar keratoplasty
• Patient with severe keratoconus with unsatisfactory vision with glasses and contact
and scleral lenses (this patient has moderate anterior and deep corneal scarring with
evidence of previous corneal hydrops): penetrating keratoplasty.

69
6. AIMS OF THE PRESENT STUDY 6.1 Overall Aims of the Study The primary overall objectives of the study were to (1) evaluate the effect of transepithelial
TGCA in the treatment of refractive errors; (2) the effect of transepithelial TGCA in the
treatment of irregular astigmatism; and (3) the combined treatment of transepithelial TGCA
and CXL in optical regularization and biomechanical stabilization of keratoconus.
6.2 Aims of the Individual Studies
Study I To explore the change in corneal asphericity after excimer laser treatments by
comparing wavefront optimized and custom-Q ablations.
Study II To assess the change of epithelial thickness profile after transepithelial TGCA
treatment for myopia.
Study III To assess the change of epithelial thickness profile in keratoconic eyes after the
combined procedure of central corneal regularization with transepithelial
TGCA and accelerated CXL in the treatment of keratoconus.
Study IV To evaluate the safety and efficacy of transepithelial TGCA in the treatment of
myopia.
Study V To evaluate the safety and efficacy of transepithelial TGCA in the treatment of
moderate to high astigmatism.
Study VI To evaluate the efficacy and safety of transepithelial TGCA in treating visually
disturbing irregular astigmatism and/or scattering caused by various LASIK-
flap/interface complications.
Study VII To assess the biomechanical properties in virgin eyes and eyes after
transepithelial TGCA.
70
Study VIII To evaluate the safety and efficacy of the “epithelium-on” CXL in arresting
keratoconus.
Study IX To evaluate a combination of topography-guided custom ablation and CXL in a
single procedure for the treatment of keratectasia.

71
7. MATERIALS AND METHODS 7.1 Patients The participants recruited in the studies were patients searching for/undergoing refractive
surgery at SynsLaser Clinic, Tromsø/Oslo, Norway (Papers 1, 2, 4, 5, 6, and 7), and
keratoconus patients who underwent “epithelium-on” CXL, or a combined procedure of
transepithelial TGCA and CXL at the University Hospital of North Norway, Tromsø, Norway
(Papers 3, 8, and 9).
Inclusion criteria for studies 1, 2, 4, 5, and 7 were: age ≥18 years; no soft contact lens
wear for 1 week (hard contact lens for 4 weeks) before the baseline examination; SE between
-0.5 and -10.00 diopters (D) with ≤ 6.00 D of refractive astigmatism; stable refractive error
(change of SE ≤ 0.50 D) for ≥ 2 years; and CDVA of 20/25 or better. Exclusion criteria were:
eye pathology, including keratoconus or keratoconus suspect (detected by corneal topo-
/tomography); previous eye surgery; glaucoma; diabetes; and systemic diseases that could
affect corneal wound healing (e.g. collagen vascular diseases).
For study 6, the inclusion criteria were: symptomatic eyes with LASIK flap/interface
complications, residual stromal thickness ≥ 300 microns and no topographic signs suggestive
of keratectasia. Nine of these eyes had previous unsuccessful retreatments by commonly used
techniques such as flap-re-lift or re-cut, followed by wavefront guided custom ablation.
Inclusion criteria for studies 3, 8, and 9 were: 1) documented progression of keratoconus
during the last 12 months before treatment (increase of astigmatism or myopia by 1.00 D or
increase in average SimK by 1.50 D); and 2) minimum corneal thickness of no less than 400
μm at the thinnest point measured by ultrasound pachymetry. Exclusion criteria were: 1)
history of herpes virus keratitis; 2) severe dry eye; 3) concurrent corneal infections; 4)
previous ocular surgery; and 5) hard contact lens wear ≤ 4 weeks before the baseline
examination.
7.2 Surgical Techniques
7.2.1 Transepithelial Topography-Guided Custom Ablation The Corneal Interactive Programmed Topographic Ablation software (CIPTA, iVIS
Technology, Taranto, Italy) was used to generate transepithelial custom ablation plans for
each eye based on subjective refraction and corneal topography measured with the Precisio
topo/tomographer (Precisio, iVIS Technology, Taranto, Italy). The optical zone size of the

72
ablation was suggested by the pMetrics dynamic pupillometry (iVIS Technology, Taranto,
Italy). Preoperative topography was also used to customize transition zone size to provide a
smooth transition between the ablated and non-ablated areas of the cornea. The CIPTA-
planned transepithelial ablation consisted of refractive and lamellar components; the function
of the latter was removal of the epithelium. The refractive component was derived by the
intercept between a desired postoperative regular aconic surface and the preoperative corneal
topography; with the tissue above the intersection to be ablated. The desired postoperative
regular aconic surface represented a resolution of the vectors of the manifest and the
preoperative corneal astigmatism. The default value for the lamellar component was 52µm,
which could be adjusted based on preoperative measurements of epithelial thickness and/or
clinical judgment. The refractive and lamellar components of the procedure were combined
and executed as a single, uninterrupted ablation. The ablations were centered on the corneal
vertex.
The ablation plan is executed by a 0.6 mm dual-flying-spot 1KHz (2 x 500Hz)
excimer laser system (iRES, iVIS Technology, Taranto, Italy). Among others the laser
employs automatic intra-operative illumination adjustment, so the light intensity is
automatically modulated to achieve the pupil size registered during the acquisition of
topography. This contributes to precise registration along with the iris/scleral vessel-based
dynamic cyclotorsional-, in addition to synchronous x,y-pupil-tracking. After registration of
the iris and scleral vessels by the laser’s x,y and cyclotorsional tracker, the corneal surface
was gently dried with a lint-free, pre-soaked merocel to achieve a reflective, homogeneous,
“dry” surface, upon which the laser ablation was performed. After the ablation, Mitomycin C
0.02% was applied to the cornea for 15 in eyes which maximum stromal ablation depth
exceeding 100 µm. At the end of the surgery, 1-2 drops of Dexamethasone with
Chloramphenicol mixture (Spersadex med kloramfenikol, Laboratoires Thea, Clermont-
Ferrand, France) and 1 drop of Bromfenac 0.9% (Yellox, Croma-Pharma GmbH, Leobendorf,
Austria) eye drops were applied, followed by a bandage contact lens (Acuvue Oaysis,
Johnson & Johnson Vision Care, Inc., FL, USA). Bromfenac 0.9% BID was used 2 days
before and 3 days after the surgery. Dexamethasone with Chloramphenicol QID was used the
first 2 weeks, and then replaced by a low potency steroid Rimexolone 1% (Vexol, Alcon
Laboratories, Surrey, United Kingdom) eye drops in tapering doses for another 3 weeks. The
bandage contact lens was removed from the cornea between postoperative days 5 and 7.
7.2.2 Epithelium-On Corneal Collagen Cross-linking

73
To reduce the risk for UV exposure of retroiridal eye structures, miosis was induced by
applying two drops of pilocarpine 2% (Pilokarpin, Ophtha AS, Norway). It was followed by
the application of two drops of local anesthetic proparacaine 0.5%, (Alcaine, Alcon Norway
AS), two drops of local antibiotic gentamycin 0.3% (Garamycin, Schering-Plough AS,
Norway) followed by proparacaine again, with one drop every minute for five minutes. All
drops were preserved by BAC (0.001% for Pilokarpin, 0.005% for Garamycin and 0.01% for
Alcaine), aiming to increase the epithelial permeability by chemically disrupting the tight
junction proteins. A round Merocel sponge (Medtronic, Inc., Minneapolis, MN) 5 mm in
diameter was inserted into the conjunctival sac to provide a depot of riboflavin, and to
produce micro-abrasions of the superficial epithelial layers caused by friction upon patient
blinking. Thereafter, two drops of proparacaine and two drops of 0.5% aqueous riboflavin
solution without dextran (Vitamin B2; Streuli, Uznach, Switzerland) were applied alternating
every 30 seconds, until the riboflavin saturation was verified by the slit-lamp inspection of the
cornea and by the determination of the presence of riboflavin-flare in the anterior chamber
(Figure 12). Under the same examination, the staining of the epithelial micro-abrasions was
verified. The initial slit-lamp saturation evaluation was performed 25 minutes after the first
application of riboflavin and repeated every five minutes until the saturation was confirmed.
During the premedication and riboflavin induction time, the patient was instructed to blink
normally between eye drop instillation and to remain in a comfortable sitting position. The
Merocel sponge was then removed and corneal thickness measured with ultrasound
pachymetry, at which point the patient was placed in supine position. Irrigation with isotonic
balanced salt solution (BSS) was performed before the UVA-irradiation in order to avoid the
shielding effect of riboflavin covering the epithelium. An eyelid speculum was then inserted
and a ring-shaped Merocel shield k20-5021 (Katena Products, Inc. Denville, NJ) was applied
to protect the limbal region and its stem cells from UVA radiation.
The cornea was subjected to UVA radiation for 30 minutes with a wavelength of 365
nm at a working distance of 5 cm. The UV-X lamp (IROC AG, Zürich, Switzerland) provided
an irradiance of 3 mW/cm2 within a circular diameter of 9 mm. During the irradiation, BSS
was applied every three minutes and proparacaine drops were added as needed. After the
UVA irradiation, two drops of atropine 1% (Atropin minims, Chauvin, England) and 2 drops
of gentamycin were applied. The cornea was protected with a soft bandage contact lens for
12-18 hours. Instructions were given to apply a mixture of 0.1% dexamethasone and 0.5%
chloromycetin (Spersadex med Kloramfenikol, Novartis, Norway) eye drops four times daily
for seven days, as well as to use artificial tears as needed.
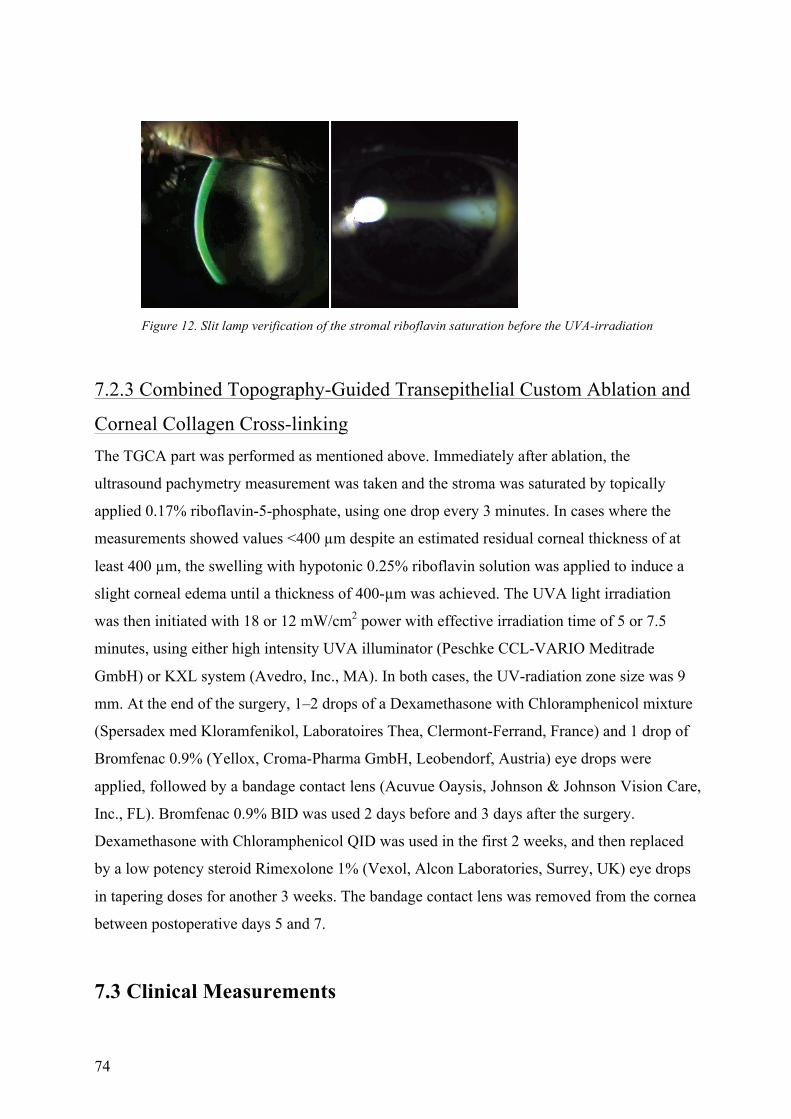
74
Figure 12. Slit lamp verification of the stromal riboflavin saturation before the UVA-irradiation
7.2.3 Combined Topography-Guided Transepithelial Custom Ablation and
Corneal Collagen Cross-linking The TGCA part was performed as mentioned above. Immediately after ablation, the
ultrasound pachymetry measurement was taken and the stroma was saturated by topically
applied 0.17% riboflavin-5-phosphate, using one drop every 3 minutes. In cases where the
measurements showed values <400 µm despite an estimated residual corneal thickness of at
least 400 µm, the swelling with hypotonic 0.25% riboflavin solution was applied to induce a
slight corneal edema until a thickness of 400-µm was achieved. The UVA light irradiation
was then initiated with 18 or 12 mW/cm2 power with effective irradiation time of 5 or 7.5
minutes, using either high intensity UVA illuminator (Peschke CCL-VARIO Meditrade
GmbH) or KXL system (Avedro, Inc., MA). In both cases, the UV-radiation zone size was 9
mm. At the end of the surgery, 1–2 drops of a Dexamethasone with Chloramphenicol mixture
(Spersadex med Kloramfenikol, Laboratoires Thea, Clermont-Ferrand, France) and 1 drop of
Bromfenac 0.9% (Yellox, Croma-Pharma GmbH, Leobendorf, Austria) eye drops were
applied, followed by a bandage contact lens (Acuvue Oaysis, Johnson & Johnson Vision Care,
Inc., FL). Bromfenac 0.9% BID was used 2 days before and 3 days after the surgery.
Dexamethasone with Chloramphenicol QID was used in the first 2 weeks, and then replaced
by a low potency steroid Rimexolone 1% (Vexol, Alcon Laboratories, Surrey, UK) eye drops
in tapering doses for another 3 weeks. The bandage contact lens was removed from the cornea
between postoperative days 5 and 7.
7.3 Clinical Measurements
75
7.3.1 General Ophthalmologic Evaluation All patients underwent complete ophthalmologic evaluation pre- and postoperatively,
including slit lamp biomicroscopy, Scheimpflug-based corneal topo-/tomography (Precisio,
iVIS Technology, Taranto, Italy), Placido-based corneal topography and wavefront
aberrometry (Nidek OPD II, Nidek Co. Ltd, Aichi, Japan), eye tonometry (Icare tonometer,
Revenio Group Corporation, Helsinki, Finland), subjective spectacle refraction, UDVA, and
CDVA (Paper 2-9).
7.3.2 Corneal Epithelial and Stromal Thickness Profile Measurements We employed the RTVue-100 SD-OCT system with a corneal adaptor module, running on
software version A6 (9.0.27). It features a 26,000-Hz scanning with 5 µm axial resolution and
15 µm transverse resolution.532 The cornea was imaged using Pachymetry pattern (6-mm scan
diameter, 8 meridians, 1024 axial-scans each) centered on the pupil. The 8 radial meridional
scans were employed by the system software to produce three-dimensional thickness maps by
interpolation. Data output included thickness maps of the total cornea and the epithelium,
across a diameter of 6-mm. Each map is divided into 17 sectors: One central circle, centered
around the pupil, which is 2-mm in diameter (centre), 8 octants within an annulus between 2
and 5 mm circles (paracentre), and 8 octants within an annulus between 5 and 6 mm circles
(mid-periphery) (Figure 6). For each of these sectors, average thickness is displayed over the
corresponding area (Papers 2 and 3).
Additionally, in study 3, epithelial thickness at the central, superior and inferior region,
minimum (Min) and maximum (Max) values, the difference between minimum and maximum
epithelial thickness (Min-Max), and map standard deviation (St Dev) were recorded from the
output of the measurements. Furthermore, we defined a minimum epithelial thickness area
(MinArea) as either the pupil central 2 mm diameter zone, or the continuous paracentral zones
with epithelial thickness of ≥ 3 µm thinner than the adjacent zones, depending on the location
of the thinnest epithelium preoperatively. The area of the remaining zones in the paracentre
was defined as ParaRest. The postoperative epithelial thickness measurements at the same areas
were calculated and compared with those of the preoperative values. Three measurements
were obtained on a single visit, of which the two best quality images were chosen, and the
average value was used for further analysis.
7.3.3 Corneal Dynamic Scheimpflug Analyzer Measurements

76
The CorVis ST software version 1.00r30 rev. 771 was used in study 7. When the eye was
aligned and the Scheimpflug image was in focus, the air puff was released automatically and
the cornea was imaged during the deformation event. The air pulse (lasting approximately 20
ms) forced the cornea inwards through applanation until it achieved its highest concavity
(concavity phase). On its return, the cornea underwent a second applanation before achieving
its natural shape. In total, approximately 140 images of the two-dimensional cross-section of
the cornea were collected. By software tracing of the anterior and posterior corneal
boundaries in individual image frames, parameters describing the corneal deformation
response were automatically generated by the instrument.
The CorVis ST measurements were performed three times by technician A and once
by technician B. The measurement sequence between the technicians was randomized using a
randomization table. A one-minute pause was taken between each measurement.
Repeatability was evaluated by comparing the three consecutive measurements performed by
technician A. Reproducibility was determined by comparing the first measurement by
technician A with the measurement performed by technician B. Mean CorVis ST measured
values obtained from the three measurements by technician A were used to compare the
differences between the virgin and post-PRK eyes groups, as well as for the correlation
analysis.
7.4 Data Analysis
7.4.1 Visual Acuity Analysis Visual acuity was measured using a Snellen chart with a decimal scale and converted to
logMAR for analysis. The mean CDVA and UDVA were converted back to Snellen for the
calculation of efficacy and safety indexes. The efficacy index was the ratio between the mean
postoperative UDVA at the end of the follow-up and the mean preoperative CDVA. The
safety index was defined as the ratio between the mean postoperative CDVA and the mean
preoperative CDVA. The predictability was evaluated by calculating the number of eyes
having an achieved spherical equivalent refraction change or vector analysis indices within
±0.50 D and ±1.00 D of the attempted correction.533
7.4.2 Vector Analysis

77
To determine the efficacy of astigmatic correction, vector analysis was performed using an
established method of Alpins.534, 535 We calculated the target-induced astigmatism (TIA) and
surgically induced astigmatism (SIA). The TIA represents the intended astigmatic change,
which is the vectorial difference between the target postoperative cylinder vector, usually 0,
and preoperative cylinder vector. The SIA is defined as the vectorial difference between the
postoperative and preoperative astigmatism. The difference vector (DV) is the vectorial
difference between the TIA and SIA, and represents the remaining uncorrected (difference)
vector. Magnitude of error (ME) demonstrates the arithmetic difference between the
magnitude of the SIA and TIA, whereas the angle of error (AE) is the angle difference
between the SIA and TIA (positive or negative if the SIA is counter-clockwise or clockwise
to the TIA, respectively). The correction index is the ratio of magnitude of SIA and TIA, and
is preferably 1.0; values larger than 1.0 mean that an overcorrection occurred and values
lower than 1.0 mean that an under-correction occurred. The index of success (IOS) is given as
the ratio of DV to the TIA. In an ideal case, in which all preoperative refractive astigmatism is
corrected, the DV or IOS should be zero, or analogously, the remaining uncorrected
astigmatism should be zero, which is the goal of the treatment. Coefficient of adjustment
(CA), calculated by dividing TIA by SIA, is the coefficient required to adjust future
astigmatism treatment magnitudes (TIA). Its value is preferably 1.0 and is the inverse of the
CI. The geometric mean correction index and CA were derived by taking the mean of the
individual logarithmic values, followed by the antilog of this calculated mean value.
The ocular residual astigmatism (ORA) was determined as the vector difference
between the preoperative refractive astigmatism at the corneal plane using a vertex distance of
12 mm and the anterior corneal topographic astigmatism (obtained by aconic fitting within
central 3.5 mm, and use of corneal refractive index of 1.376) obtained by Precisio
topo/tomographer.
7.4.3 Statistical Analysis Statistical analyses were performed using IBM SPSS Statistics (IBM Corp., Armonk, NY).
The Shapiro-Wilk test was used to test the normality of the data distribution. Independent
sample t-test or Mann-Whitney U test was used to compare two groups, whereas paired t-test
or Wilcoxon signed rank test was used to compare paired samples. In study 7, for the
parameters that showed significant differences, univariate analysis of covariance (ANCOVA)
was applied to adjust for selected covariates (age, CCT measured by the CorVis ST, and mean

78
simulated keratometry value measured by OPD Scan II) to control for potentially confounding
factors. In study 2, a linear mixed model was employed to compare the measurements at
different postoperative times. Pearson or Spearman correlation coefficient was applied to seek
possible correlations between different parameters. In all analyses, p < 0.05 was considered
statistically significant.
In study 7, MedCalc software 11.4.2 (MedCalc Software, Ostend, Belgium) was used
to calculate the within-subject standard deviation (Sw), within-subject coefficient of variation
(COV), and intraclass correlation coefficient (ICC) to assess the intraobserver repeatability
and interobserver reproducibility.

79
8. SUMMARY OF RESULTS 8.1 Paper I In paper I, we compared the surface ablation treatments with wavefront optimized and
custom-Q ablations for myopia and astigmatism. Preoperative and 3-month postoperative Q-
values, higher order aberrations, low contrast visual acuity, and classic outcome parameters
were analyzed.
The wavefront optimized ablation group comprised of 46 eyes of 23 patients with a
mean SE of -3.64 D (range: -1.15 to -8.25 D). Mean Q-value changed from -0.33
preoperatively to 0.06 postoperatively. The custom-Q ablation group comprised of 42 eyes of
21 patients with a mean SE of -3.24 D (range: -1.47 to -8.00 D). Their mean Q-value changed
from -0.36 preoperatively to -0.03 postoperatively. A statistically significant difference in
postoperative change in Q-values (P=0.049) between the two groups was noted, but there was
no such difference in higher order aberrations, low contrast visual acuity, or classic outcome
parameters.
8.2 Paper II In paper II, we retrospectively analyzed the postoperative corneal epithelial and stromal
thickness profile changes in 46 left eyes of 46 patients treated with PRK for myopia. Corneal
and epithelial thickness maps within the central 6 mm were obtained by anterior segment
spectral-domain optical coherence tomography preoperatively and at 1, 3, and 6 months
postoperatively. Stromal thickness was calculated by subtracting the epithelial thickness from
the total corneal thickness. Correlations between postoperative thickness changes and the
amount of correction, treatment zone, and preoperative epithelial thickness were analyzed.
Compared to preoperative values, the central 2 mm and the paracentral 2 to 5 mm zone
epithelium was 5.20±3.43 and 5.72±3.30 µm thicker, respectively, at 3 months
postoperatively (p < 0.05). No significant difference was detected between 3 and 6 months
postoperatively. The stromal thickness did not change between 1 and 6 months
postoperatively. The spherical equivalent (SE) changed from -2.82±1.54 D preoperatively to -
0.06±0.42 D at 1 month postoperatively, and remained stable thereafter.
8.3 Paper III

80
In paper III, we evaluated corneal epithelial remodelling after transepithelial TGCA followed
by CXL in the treatment of keratoconus. This study retrospectively analyzed the epithelial
thickness distribution changes in 53 keratoconic eyes of 44 patients. Manifest refraction,
maximum (Kmax) and minimum (Kmin) keratometry obtained by Placido topography, corneal
irregularity index (IRI) measured by Scheimpflug topography, and the epithelial thickness
profile over the central 5-mm zone obtained by anterior-segment spectral domain optical
coherence tomography (SD-OCT) were evaluated preoperatively and at 1–3, 3–6, and >6
months postoperatively.
The epithelial thickness at the preoperatively thinnest area (Minarea) was 48.8±4.4 µm,
correlating negatively with Kmax (r=-0.310, p<0.05) and IRI (r=-0.362, p< 0.05).
Improvements in corrected distance visual acuity, decreased refractive astigmatism, Kmax,
Kmin, and IRI were registered after the treatment (p< 0.05). At > 6 months postoperatively,
epithelial thickening of 5.9±5.1 µm was registered at the respective area. No statistically
significant change in the epithelial thickness was detected in other sectors, leading to a
decrease in epithelial thickness difference between Minarea and the rest of the paracentre areas
by 5.6±4.4 µm.
8.4 Paper IV Paper IV investigated the transepithelial TGCA in the treatment of low to moderate myopic
astigmatism using a 1 KHz excimer laser. In this study, 117 consecutive eyes available for
evaluation 12 months after surgery were included. Pre- and post-operative visual and
refractive data as well as post-operative pain and haze were analyzed.
The mean pre-operative SE and the mean cylinder were: –3.22 D ± 1.54 (range –0.63
to –7.25 D) and –0.77 D ± 0.65 (range 0 to –4.50 D), respectively. At 12 months after
surgery: no eyes lost ≥ 2 lines of CDVA. Safety and efficacy indexes were 1.27 and 1.09,
respectively. Uncorrected distant visual acuity was ≥ 20/20 in 96.6% of the eyes. Manifest
refraction spherical equivalent was within ± 0.5 D of the desired refraction in 93.2% of the
eyes. Average root mean square (RMS) wavefront error measured at central 6 mm, increased
from 0.38 pre-operatively to 0.47 μm post-operatively. Refractive stability was achieved and
sustained 1 month after surgery. No visually significant haze was registered during the
observation period. Post-operative pain was reported in 4.5% of patients.
8.5 Paper V

81
Paper V analyzed the outcomes of treatment of astigmatism ≥ 2.0 diopters (D) with
transepithelial TGCA. In this study we retrospectively analyzed a series of 206 eyes, divided
into two groups: myopic astigmatism (153 eyes) and mixed astigmatism (53 eyes). Efficacy,
safety and predictability were evaluated, and vector analysis of cylindrical correction was
performed.
The median preoperative spherical equivalent (SE) was -2.63D and -0.63D for the
myopic and mixed astigmatism groups, respectively, with a median cylinder -2.50D.
Postoperative uncorrected distance visual acuity (UDVA) was ≥ 20/20 in 92% and 83% of
eyes in the myopic and mixed astigmatism groups, respectively; the corresponding efficacy
indices were 1.00 and 0.96 and residual astigmatism ≤ 0.50D was present in 82.4% and 56.7%
of myopic and mixed astigmatism eyes respectively. The arithmetic mean magnitude of the
difference vector (DV) was 0.38D (myopic) and 0.65D (mixed). DV magnitude was
positively correlated with the magnitude of target induced astigmatism (TIA) in both groups.
The geometric mean coefficient of adjustment index was 1.04 and 1.19, representing under-
correction of 4% and 19%, in the myopic and mixed astigmatism group, respectively.
8.6 Paper VI Paper VI evaluated the efficacy and safety of transepithelial TGCA in the treatment of
visually disturbing irregular astigmatism and/or scattering caused by LASIK-flap/interface
complications. In this study, 17 eyes of 16 patients with LASIK flap/interface complications
and central residual stromal thickness ≥ 300 microns were treated with transepithelial TGCA.
The laser regularized the irregular corneal surface and in the same continuous process ablated
the flap/interface pathology that caused the irregularity and/or scattering. UDVA, CDVA,
refraction, corneal irregularity, ocular HOAs, and visual symptoms were analyzed.
At 15.9±11.0 months postoperatively, mean UDVA increased from 20/87 to 20/25.
Mean CDVA increased from 20/28 to 20/19 (P<0.001), with 64.7% of the eyes gaining two
lines of CDVA or more. The mean corneal irregularity index decreased from 25.82 to 20.36
microns (P= 0.009). The mean root-mean-square (RMS) of total HOAs decreased from 1.30
to 0.49 (P=0.042), while RMS of the odd-order (3rd and 5th) and even order (4th and 6th)
HOAs decreased from 0.85 to 0.38 (P= 0.001) and from 0.43 to 0.24 (P= 0.036), respectively.
All patients claimed their visual symptoms to be better (8 eyes) or cured (9 eyes). Corneal
regularization and removal of the underlying flap/interface pathology by cTEN ablation
appears to be a simple and effective treatment for LASIK-flap/interface complications
82
associated with visually disturbing irregular astigmatism and/or scattering in cases with
sufficient residual stromal thickness.
8.7 Paper VII Paper VII investigated the measurement reliability of CorVis ST, a dynamic Scheimpflug
analyser, in virgin and post-photorefractive keratectomy (PRK) eyes and compared the results
between these two groups. Forty virgin eyes and 42 post-PRK eyes underwent CorVis ST
measurements performed by two technicians. Repeatability was evaluated by comparing three
consecutive measurements by technician A. Reproducibility was determined by comparing
the first measurement by technician A with one performed by technician B. Intraobserver and
interobserver intraclass correlation coefficients (ICCs) were calculated. Univariate analysis of
covariance (ANCOVA) was used to compare measured parameters between virgin and post-
PRK eyes.
The intraocular pressure IOP, CCT and 1st applanation time demonstrated good
intraobserver repeatability and interobserver reproducibility (ICC 0.90) in virgin and post-
PRK eyes. The deformation amplitude showed a good or close to good repeatability and
reproducibility in both groups (ICC 0.88). The CCT correlated positively with 1st
applanation time (r= 0.437 and 0.483, respectively, p<0.05) and negatively with deformation
amplitude (r=-0.384 and -0.375, respectively, p<0.05) in both groups. Compared to post-PRK
eyes, virgin eyes showed longer 1st applanation time (7.29±0.21 vs. 6.96±0.17 ms, p<0.05)
and lower deformation amplitude (1.06±0.07 vs. 1.17±0.08 mm, p<0.05).
8.8 Paper VIII Paper VIII evaluated the efficacy and safety of epithelium-on corneal collagen cross-linking
(CXL) using a multifactorial approach to achieve proper stromal riboflavin saturation in 61
eyes with progressive keratoconus treated with epithelium-on CXL. Chemical epithelial
penetration enhancement (benzalkonium chloride-containing local medication and hypotonic
riboflavin solution), mechanical disruption of the superficial epithelium, and prolongation of
the riboflavin-induction time until verification of stromal saturation were used prior to the
UVA irradiation. Uncorrected and corrected distance visual acuity (UDVA, CDVA),
refraction, corneal topography, and aberrometry were evaluated at baseline and at 1, 3, 6, and
12 months postoperative.

83
At 12-months, UDVA and CDVA improved significantly. None of the eyes lost lines
of CDVA, while 27.4% of the eyes gained 2 or more lines. Mean spherical equivalent
decreased by 0.74 D, and mean cylindrical reduction was 1.15 D. Irregularity index and
asymmetry from Scheimpflug-based topography and Max-K at the location of cone from
Placido-based topography showed a significant decrease. Higher-order-aberration data
demonstrated a slight reduction in odd-order aberrations S3, 5, 7 (P=0.04). Postoperative pain
without other complications was recorded.
8.9 Paper IX Paper IX evaluated the combination of transepithelial TGCA and CXL in a single procedure
for the treatment of keratectasia. Twelve eyes of 12 patients with keratectasia were treated
with topography-guided custom ablation and CXL. Topography-guided custom ablation was
performed using a transepithelial technique with the iVIS Suite 1 kHz flying spot excimer
laser. Collagen cross-linking was performed immediately after topography-guided custom
ablation, according to standard protocol. Postoperative follow-up examinations were
performed at 1, 3, 6, and 12 months. Uncorrected visual acuity (UDVA), best spectacle-
corrected visual acuity (CDVA), refractive change, corneal topography, and pachymetry were
analyzed pre- and postoperatively.
Mean UDVA increased from 20/1000 preoperatively to 20/125 12 months
postoperatively. Mean CDVA increased from 20/57 to 20/35, with no loss of lines of visual
acuity. Mean astigmatism was reduced from 5.40±2.13 diopters (D) to 2.70±1.44 D, and
keratometric asymmetry decreased from 6.38±1.02 D to 2.76±0.73 D. Only minor changes in
posterior corneal surface elevation and stability of refraction were found, confirming that no
progression of ectasia occurred during the observation time.

84
9. GENERAL DISCUSSION 9.1 Rationale for Transepithelial Topography-Guided Custom
Ablation in Treatment of Irregular Astigmatism
9.1.1 Custom Ablation Corneal excimer laser surgery for correction of refractive errors has advanced significantly
since its introduction. It is reported that conventional excimer laser keratorefractive
procedures induce an increase in spherical-like and coma-like HOAs, mainly due to the
modification of corneal asphericity/inadequate optical zone size and optical decentration,
respectively.536-538 The ablation profile can have a significant impact on postoperative
outcome. Application of modern wavefront and topography technologies in corneal refractive
surgery offers opportunities for better optical quality and visual performance.539
9.1.1.1 Aspheric ablation profile It is currently known that for most eyes a negative (prolate) corneal asphericity is required to
balance the positive (oblate) asphericity of the crystalline lens to achieve minimal spherical
aberration. However, the conventional (non-aspheric) treatments for myopia result in an
oblate shift of the cornea,540 which disturbs this balance. Furthermore, this shift seems to be
directly correlated with the amount of correction.541 Among the HOAs induced by corneal
refractive surgery, spherical aberration caused by the change in corneal asphericity after laser
ablation seems to be the most prevalent.542-545 Good control of spherical aberration and a
physiological postoperative corneal shape may be achieved with aspheric laser ablation
profile design.546 Modern refractive ablation design, with considerations to control
asphericity, reduces this oblate shift, which typically become progressively less effective
towards high degrees of myopic treatment.541 In study 1, we compared the wavefront
optimized treatment and the custom-Q treatment employed by WaveLight ALLEGRETTO
(Wave-Light AG, Erlangen, Germany) laser. The wavefront optimized ablation has an
aspheric profile in which the amount of asphericity is not adjustable (and is the default
treatment type on that platform). The custom-Q ablation is also an aspheric ablation; however,
it allows the surgeon to define the intended Q-shift (postoperative Q-value minus preoperative
Q-value) by specifying a desired asphericity target. The custom-Q treatment uses only
preoperative mean corneal asphericity data in addition to refractive data. It does not attempt to
achieve a given asphericity at all points within the optical zone because no preoperative local

85
asphericity values are taken into account in programming of the ablation; it aims only to
change the mean asphericity by symmetrically adjusting the number of mid-peripheral laser
pulses.
Our results showed almost universal oblate Q-shift in both groups. The shift was less
in the custom-Q group, especially for higher degrees of myopia. However, the difference
between groups was just marginally statistically significant (P=0.049) and did not result in
any significant difference in postoperative spherical aberration or low contrast visual acuity.
A combination of factors such as the decrease in effective radiant exposure to laser energy
from the corneal center towards the periphery154 (due to inclination of corneal surface);
reflection losses according to Fresnel’s law,154, 547 and the corneal biomechanical response154,
538, 548 seem to be responsible for the oblate shift. The first two factors are addressed by
aspheric ablations that feature a correction matrix, which compensates for the reduced laser
ablation efficacy in the mid-peripheral cornea.549 Ablation profiles used in both groups in our
study are compensated for by such a correction matrix549 and, therefore, the residual oblate
shift that our results show is probably, or at least partially, due to a biomechanical response of
the cornea in agreement with study the by Koller et al.154, 550
Because we treated only virgin eyes with good preoperative contrast sensitivity and a
low preoperative level of HOAs, our aim was to eliminate the patient’s spherocylindrical error
without disturbing the remainder of the corneal optics significantly. Koller et al.550 used the
same laser platform and found a much larger increase in the 3rd order HOAs (from
0.181±0.072 µm before surgery to 0.296±0.115 µm after surgery) in eyes treated with
custom-Q ablation, compared to wavefront-guided treatments (from 0.182±0.094 µm before
surgery to 0.192±0.088 µm after surgery). Tran and Shah551 compared WaveLight wavefront
optimize treatments and LADARVision4000 (Alcon Laboratories Inc., Ft Worth, Tex)
wavefront-guided treatments and found significantly more induced 3rd HOAs with the
former. The 3rd order HOAs in both groups changed only insignificantly (from 0.163±0.081
µm before surgery to 0.191±0.092 µm after surgery in the wavefront optimized group and
from 0.182±0.092 µm before surgery to 0.193±0.085 µm after surgery in the custom-Q
group). Hence, our results in both groups were more comparable to Koller et al.550 and Tran
and Shah’s551 wavefront-guided treatments than with their wavefront optimized treatments.
The reason for this may be our centration of the ablation on the corneal vertex. Our total RMS
HOAs, spherical aberration, and the 3rd order HOAs increased very little and resulted in well-
preserved low contrast visual acuity under light and dark conditions, with and without glare (a
finding comparable to the study by Koller et al.550), and a statistically significant correlation
86
between the postoperative Q-values and low contrast visual acuity has not been found. Tuan
and Chernyak552 also did not find such a correlation and concluded that “an oblate cornea is as
likely to produce high-quality vision as a prolate one.” Other explanations may be that low
contrast visual acuity is a subjective measurement dependent on a number of interrelated
factors and the low quality of postoperative asphericity data.
The non-significant difference in postoperative Q-value or spherical aberration or low
contrast visual acuity between the two groups may be caused either by the insufficient
measurement reliability of our asphericity and wavefront aberrometry, or by a small influence
of the achieved Q-value changes on the spherical aberration and low contrast visual acuity. It
is uncertain whether more prolate Q-targets would further diminish or eliminate the remaining
oblate shift found in our custom-Q treatments. We are limited to what we can achieve by the
Q-target adjustment, especially if we bear in mind that part of the oblate shift most likely
occurs due to biomechanical response of the cornea, which may need to be counteracted by a
different approach. However, with the custom-Q treatments we have a new possibility to
better control the oblate shift. Hopefully, in the future, it will be possible to achieve specific
Q-targets resulting in minimal spherical aberration.
9.1.1.2 Topography-guided custom ablation Topography-guided custom ablation uses the patient’s corneal topography as the starting
point. Corneal topography measures the corneal surface irregularities that represent the
substrate for the vast majority of ocular aberrations; therefore, using this information for
programming of the treatment is the most direct approach. The TGCA smoothens the anterior
corneal surface irregularities and changes the anterior corneal curvature to treat the anterior
corneal HOAs and the refractive error of the eye at the same time. In cases with highly
aberrated corneal optics, as after PKP and where corneal irregularities and/or media opacity
prevent reliable wavefront analysis, TGCA is the only refractive surgery choice.542, 553 In
paper 4 and 5, we investigated the effect of TGCA in treatment of myopia and astigmatism in
healthy eyes.
In study 4, all eyes were within ±1.0 D of emmetropia, 94% of eyes were within ±0.5
D of emmetropia and 97% of eyes had refractive astigmatism less than or equal to 0.5 D at 12
months post-operatively. Postoperative UDVA of at least 20/20 was achieved in 96.6% of the
eyes. No eyes lost ≥ two lines of CDVA. In study 5, a postoperative UDVA of at least 20/20
was achieved in 92% and 83% of eyes treated for myopic and mixed astigmatism

87
respectively. No change or a gain of up to two lines of CDVA was observed in 97% (myopic
astigmatism) and 96% (mixed astigmatism) of eyes; no eye lost more than one line of CDVA.
The safety, efficacy, and predictability in our results are comparable with the best outcomes
of surface ablation in treatment of myopic astigmatism358, 359, 554-569 (Table 2) and corneal laser
refractive surgery for moderate to high astigmatism402, 546, 570-579 published in recent years
(Table 3).
The ablation profile can have a significant impact on postoperative outcome. Alpins580
recommended the use of vector planning to link preoperative topographic measurements into
the treatment plan with the refractive values. The topography-guided custom ablation pattern
used in this study was based on a resolution of the vectors of the manifest and the corneal
astigmatism as measured by topography and is in consistent with Alpins’s recommendations.
Vinciguerra et al.581 argued that creating a smooth transition (low dioptric gradient) between
the treated and untreated cornea might improve the outcomes of surgery for astigmatism. We
sought to achieve this by creating a customized transition that results in a continuously low
dioptric gradient towards the untreated cornea. A smooth transition zone may be the key to
low regression as it may prevent the counterproductive epithelial remodelling, which is
induced by non-smooth transitions.
Misalignment of the axis in astigmatic treatment results in under correction.582 It is
well known that the pupil centroid varies with pupil size, resulting in registration error that
may significantly affect the quality of laser surgery outcomes.583, 584 It follows that accurate
centration and control of the cyclotorsional movements of the eye are necessary to optimize
visual and refractive outcomes and reduce the induction of optical aberrations.584 The system
used in this study deals with the centroid shift by using an intra-operation laser illumination
adjustment to control pupil size and using x,y pupillary tracking for accurate centration during
the ablation procedure. The use of iris registration and dynamic cyclotorsional eye-tracking
has also been shown to improve the accuracy of astigmatism treatment.582 We observed small
absolute mean AEs (2.2 degrees and 3.7 degrees for myopic and mixed astigmatism groups
respectively) which is consistent with the closeness of the aggregate vector mean TIA (0.83D
x 172 and 0.89D x 173) and SIA (0.85D x 174 and 0.95D x 173) axes. Therefore, no
significant systematic error due to misaligned treatment was evident. However, at the
individual patient level, AE ranged from -14 degrees to 13 degrees in myopic astigmatic
correction, and from -22 degrees to 13 degrees in mixed astigmatic correction, which may
suggest variable factors at work, such as healing response.

88
Hyperopic and mixed astigmatism are technically demanding and difficult to
correct.546, 577 We observed a slight under-correction of astigmatism in both our groups, but
this was more evident in the mixed astigmatism group. Data indicating under-correction of
4% (myopic astigmatism) and 19% (mixed astigmatism) are corroborated by negative mean
MEs of -0.08D and -0.34D, and arithmetic mean DVs of 0.38D and 0.65D for the myopic and
mixed astigmatism groups, respectively. The DV is a useful vector measure of uncorrected
astigmatism. In our sample, DV magnitude was positively correlated with TIA and the DV
was larger in the mixed astigmatism group.
Furthermore, our studies showed minimal or no significant change in HOAs. Unlike
the custom-Q treatment which uses only preoperative mean corneal asphericity data, the
ablation procedure used in our TGCA minimizes the induction of spherical aberration by
adjusting the target value for asphericity according to the preoperative anterior corneal
curvature and the planned curvature change, as well as by compensating for the reduction in
radial efficiency of the laser towards the corneal periphery. We did not observe an increase in
coma-like HOAs in our study and this may also be attributed to the ablation design, which is
based on the existing centering and symmetry of the corneal optics measured by topography.
Some studies have demonstrated that visual outcomes of astigmatic correction are worse in
eyes with high ORA,585-587 but the predictability of astigmatic correction was similar for eyes
with high and low ORA in our study. Further investigation is warranted to determine whether
the topography-guided design is advantageous in this respect.
The TGCA performed with the iVIS platform is a safe, effective and predictable
treatment for myopia and for moderate to high astigmatism in healthy eyes. Outcomes could
be further improved by a better understanding of postoperative wound healing, postoperative
irregular epithelial thickening and corneal biomechanical changes.538, 588, 589
9.1.1.3 Epithelial remodelling The corneal epithelium protects the eye and plays an important role in maintaining corneal
transparency and optical quality.590 It has a rapid cell turnover and is highly reactive to
irregularities of the underlying stromal surface.196, 591, 592 The clinical application of corneal
epithelial thickness profile measurements is becoming important in the diagnosis of
keratoconus and especially so in corneal therapeutic refractive surgery.196, 593, 594 The
epithelial thickness has been studied using Artemis very high-frequency digital ultrasound
(ArcScan Inc., Morrison, Colo),595 confocal microscopy,596 optical coherence tomography,597
89
ultrasound,598 and optical pachymetry.599 However, apart from the studies applying
Artemis,595 the majority of other studies were solely based on central epithelial thickness
measurements. One of the recent applications of SD-OCT allows non-contact, in vivo three-
dimensional mapping of the corneal epithelial thickness.190, 600, 601 In the current project, we
used the RTVue 100 SD-OCT in evaluating epithelial thickness profile changes in healthy
myopic eyes treated with PRK (study 2), as well as in keratoconic eyes treated with combined
topography-guided transepithelial PRK and CXL (study 3).
The corneal epithelium in normal eyes is mostly evenly distributed, being only slightly
thicker inferiorly and nasally than superiorly and temporally.40, 588, 591, 600, 602 In study 2, the
preoperative average central epithelial thickness in myopic eyes was 54.79±3.71 µm, which is
within the range of previously reported values (from 48.3 to 58.4 µm).40, 591, 603-606 Similar to
the finding by Kanellopoulos et al.,600 we found the preoperative epithelium in male eyes to
be thicker than in female eyes. The non-uniform preoperative epithelial thickness profile,
characterized by thinner epithelium superiorly than inferiorly and temporally than nasally,
was also in accordance with other studies.40, 591, 595, 600, 602 Our results generally matched the
data obtained by SD-OCT,190, 591, 600, 602 while they differed from the measurements with
Artemis very high-frequency ultrasound in the following way: 1) We did not detect a
significant difference between central and paracentral epithelial thickness after annular
averaging, whereas the measurements with Artemis demonstrated 2.3 µm thinner epithelium
centrally (within 1.5 mm) than paracentrally (annulus between 3 and 3.4 mm);595 and 2) the
difference of 1.7±2.1 µm between superior and inferior paracentral epithelium in the current
study is considerably smaller than 5.3 to 5.9 µm, as reported by Reinstein et al.40, 595 The
variations may be caused by the differences in technology and measurement technique
(noncontact SD-OCT vs. saline immersion ultrasound). The SD-OCT measurements’ inability
to discriminate the tear film, and the central specular hyper refractive reflex, may affect the
detection of layer boundaries in the center due to the reduced signal to noise ratio. The
patient’s demographics may also contribute to the discrepancies. For example, Yang et al.607
reported that except for the central 2-mm sector and the inferiotemporal sector in the
paracentral area, corneal epithelial thickness was negatively correlated with age.
After the myopic treatment, the epithelial thickness in all the measured areas
continued to increase between 1 and 3 months after the surgery, whereas refractive stability
was achieved by 1 month. No correlation was found between the epithelial thickening and
postoperative refraction change. The epithelium may affect refraction due to its shape at the
air-tear film interface and because of its different refractive index compared to the stroma,608

90
but a uniform epithelial thickening (or thinning) would not appreciably change the curvature
of the corneal surface and refraction. The difference between central and paracentral epithelial
thickening in the current study was within 1 µm; therefore, it did not affect the postoperative
SimKmean, nor the manifest refraction. In eyes with refractive regression, pronounced
postoperative epithelial thickening or thinning occur,599, 609 after myopic and hyperopic
treatments, respectively, in addition to a large difference in the postoperative central and
paracentral epithelial thickness.
In agreement with previous findings,190, 595, 598, 610, 611 the postoperative epithelial
thickening in the current study correlated with the programmed SE correction and the
treatment zone. Our findings concur with those of Gauthier and associates610, 611 who
demonstrated that epithelial hyperplasia was greater with smaller zone sizes. Interestingly, we
found a significant negative correlation between the postoperative epithelial thickening and
the preoperative epithelial thickness. Our data demonstrated that the preoperatively thinnest
epithelium in the temporal superior region had the most pronounced postoperative thickening.
The preoperative superior-inferior epithelial thickness asymmetry was explained by eyelid
dynamics,40 and the effect of gravity upon tear film when measured with SD-OCT.600
However, the mechanism behind the negative correlation between epithelial thickening and
the preoperative epithelial thickness is unclear. One may speculate that the corneal flattening
due to myopic treatment results in a mismatch of anatomy between the eyelid and the cornea,
allowing the epithelium to fill the gap.
In eyes with irregular stromal surface due to corneal pathology, injury, or corneal
refractive surgery that results in non-physiologic stromal shape, the epithelium remodels, in
an attempt to establish a smoother anterior corneal surface.189 This process results in thinning
above the relatively elevated corneal area and thickening above the relatively depressed
regions. It is hypothesized that the magnitude of epithelial compensation is determined by the
curvature gradient.189, 612, 613 Keratconus is characterized by conical ectasia, and the epithelial
profile in keratoconus is reported to be doughnut-shaped with localized central thinning over
the apex of the cone, surrounded by an annulus of thickened epithelium around the cone.591,
614
In study 3, we found thinning of the epithelium in the temporal inferior area in
keratoconic eyes preoperatively, which is in accordance with other studies196, 591, 602, 614-616
Furthermore, we found that the epithelial thickness at Minarea correlated negatively with Kmax
and IRI, whereas the epithelial thickness difference between Minarea and ParaRest areas
correlated positively with these parameters. This means that in the keratoconic corneas, the
91
steeper and more irregular corneal shape is, the thinner the epithelium at the cone apex and
larger its variation from the surroundings will be, confirming the previously described
compensatory epithelial thickness changes.
After the combined treatment of transepithelial TGCA and CXL, the postoperative
epithelial thickness increase was limited to the areas where the thinnest epithelium was
located preoperatively, whereas the mean central and paracentral corneal thickness did not
show a statistically significant change. This is different from the findings in study 2, where
we demonstrated that 3 months after topography-guided PRK in treatment of myopia, the
epithelial thickness was increased centrally by 5.20±3.43 µm and paracentrally by 5.72±3.30
µm. The difference in epithelial remodelling between our two studies may be attributed to the
different starting points (regular vs. irregular), the additional CXL procedure performed after
the topography guided PRK, or to the different epithelial healing pattern in keratoconic eyes.
Kanellopoulos and Asimellis617 investigated the epithelial thickness profile changes after high
myopic femtosecond laser LASIK with or without concurrent high-fluence CXL (UVA
fluence of 30 mW/cm2 for a total of 80 seconds). The comparison of matched myopic
correction subgroups treated for myopia over -7 D indicated significantly less thickening of
the epithelium paracentrally in eyes treated with concurrent CXL, indicating that the
application of CXL might play a role in preventing postoperative epithelial thickening which
is commonly found in normal virgin eyes.190, 588
In line with study 2, where preoperatively thinner epithelium correlated to more
thickening postoperatively after topography-guided PRK in the treatment of myopia in normal
eyes, our data in study 3 showed postoperative epithelial thickening in the areas with
preoperatively thinned epithelium at the cone location. Hence, the thickening correlated
negatively with the preoperative thickness values in both studies. Reinstein et al.612 advocated
that the amount of epithelial thickening is determined by the rate of change of the curvature of
the stromal surface. This is in agreement with our findings that the area with preoperatively
thinner epithelium due to the local “bulging” of the anterior stroma increased in thickness
after the smoothening of the “bulge”. This smoothening is achieved by the effect of the
topography-guided ablation (as shown by decreased Kmax and IRI), which transfers to a
decrease in the rate of change of the stromal curvature.
The limitations of the studies are the inability of the RTVue 100 to measure corneal
and epithelial thickness outside the central 6-mm diameter of the cornea, and a lack of longer
follow-up data. Limitations of the current SD-OCT technology (limited axial resolution and
no ability for tear film discrimination) may also influence the validity of our analysis. Higher

92
axial resolution equipment with a better ability for discrimination of the tear film would be
beneficial. Future studies with longer follow-up time, particularly pertaining to changes in
epithelial thickness profile extending beyond the 6 mm diameter, are warranted. Still, the
values presented in our results are in accordance with the earlier findings obtained by VHF
ultrasound technology,40 which features higher resolution, as well as with the findings of the
related research with OCT instrumentation.190, 600
9.1.1.4 Transepithelial TGCA As described above, in eyes with irregular stromal surface, the epithelial remodelling
compensates to some degree for the irregular astigmatism, meaning that the irregularity we
see and measure on topography is only part of the stromal irregularity, implying a mismatch
between the epithelial and the stromal surfaces. Therefore, a topography-guided ablation
based on the preoperative measurements of the epithelial surface applied to the stroma after
removal of the epithelium can only correct the irregularity that has not been compensated by
the epithelium. It also means that as a consequence of epithelial remodelling, mechanical or
alcohol epithelial removal used with traditional surface ablation techniques (ASA, LASEK,
Epi-LASIK) will reveal an irregular stromal surface that does not match the preoperative
corneal topography (Figure 11). This may represent a source of potentially significant
ablation error when topography-guided surface ablation is used. To circumvent this issue, we
use a transepithelial approach in which manual epithelial removal is replaced by adding a
lamellar component to the refractive ablation.
The lamellar part is aimed at removal of the epithelium and the simultaneous
preservation of its smoothening effect, achieved by its previous remodelling. With this
approach, the epithelium and anterior stroma protruding into the lamellar ablation depth are
uniformly ablated across the treatment diameter (Figure 13). The depth of the lamellar part
can be decided by using the information from the preoperative epithelial thickness map
obtained by OCT, while the ‘refractive’ ablation map is produced on the basis of Scheimpflug
topography. The sum of the two has to be no less than the epithelial thickness at any point
throughout the area of the treatment, to ensure that the post-ablation surface would be beneath
the thickest point of the epithelium. As a result, no epithelium rested at the post-ablation
surface, and the minimal use of stromal tissue will be achieved at the same time. Based on
similar reasoning, Renstein et al.193 used transepithelial phototherapeutic keratectomy (PTK)
to regularize the irregular corneal stromal surface.

93
Figure 13. Schematic drawing of the ablation plan of the topography-guided transepithelial ablation in
keratoconic eyes. The green layer represents the epithelium. The top and bottom dashed lines represent the
epithelial surface and the desired postoperative surface. The spaces between the top and middle dashed lines
represent the lamellar part of the ablation, and the space between the middle and bottom dashed lines represents
the refractive part of the ablation. The lamellar part of the ablation in the area of the cone consists of both the
epithelium and stroma, due to the epithelial thinning over the cone.
In integrated transepithelial treatment, total ablation volume far exceeds stromal
ablation volume, typically by a factor of 3 to 6; it is therefore necessary to use a high-
frequency excimer laser to achieve short ablation times in order to prevent stromal
dehydration effects.618 With the iRES 1KHz laser, full thickness epithelial removal can be
performed in only 16 s, whilst a myopic ablation for 6 D (6.5 mm optical zone and 7.5 mm
total ablation zone) requires 15 s.
With conventional flying-spot lasers, there is a linear increase in the number of pulses
per mm2 per sec (local frequency), as the ablation area decreases towards the end of the
treatment, causing an increased thermal effect and increased plume production that would
culminate in a decreased ablation effect. This is traditionally compensated for by empirical
nomogram adjustments. In contrast, the laser used in this study maintains a local frequency of
4Hz, i.e. the laser beam will always hit the same spot in the treated area four times per
second.568 Because it produces a low, constant and even delivery of energy across the ablation
area, the unwanted thermal effects due to the high frequency are avoided. This is essential to
achieving a smooth ablation surface, which is important for the prevention of postoperative
haze.619

94
To apply transepithelial concept to treat refractive errors with high precision, the
compatibility of ablation rates between the epithelium and the stroma must be achieved. As
the laser used in the cases reported here was specially designed for transepithelial ablation it
optimizes the fluence, shot pattern and frequency to minimize the difference in ablation rate
between the epithelium and the stroma. This approach is different from that used in another
laser platform (Schwind Amaris, Schwind eye-tech-solutions GmbH and Co. KG), which
attempts to compensate for the ablation rate difference by employing a non-modifiable
nomogram of ablating approximately 55µm epithelium at the center and 65µm at the
periphery (4.0mm radially from the center), presumably based on population measurements of
epithelial thickness.620
Using transepithelial approach, the de-epithelialization area fits exactly the edge of the
refractive part of the ablation, thus generates less corneal trauma compare to mechanical
epithelial removal, potentially resulting in faster and less painful re-epithelialization. The idea
of transepithelial laser treatment appeals to patients because it is much quicker and more
comfortable than traditional excimer laser surgery. The main appeal of this procedure to the
surgeon is its perceived lack of serious complications as well as ease and speed of
performance.

95
Aut
hor,
year
Su
rgic
al
tech
niqu
e
Follo
w-u
p
(mon
ths)
Eyes
SI
EI
Pred
icta
bilit
y
±
0.50
D
± .1
.0 D
M
MC
H
aze
Epi.
rem
oval
Man
che56
4 ,
2011
WF-
guid
ed
PRK
12
34
1.
15
1.02
91
%
97%
n/
a no
haz
e A
moi
ls b
rush
Gam
bato
558 ,
2011
WF-
optim
ized
PRK
12
303
1.
05
1.05
99
%
n/a
Abl
. dep
. ≥ 8
0 µm
gr
ade ≤
1 20
% e
than
ol
Miff
lin56
5 ,
2012
Cus
tom
PR
K
12
40
1.
23
1.15
89
%
94%
n/
a no
t sig
nific
ant
n/a
Stan
dard
PR
K
12
40
1.
19
1.06
86
%
97%
n/
a no
t sig
nific
ant
n/a
Sia56
7 , 201
2 St
anda
rd P
RK
12
29
8
1.29
0.
67
83%
10
0%
n/a
not s
igni
fican
t A
moi
ls b
rush
Asl
anid
es35
9 ,
2012
WF-
optim
ized
PRK
12
60
n/
a 0.
99
n/a
n/a
Abl
. dep
. ≥ 7
5 µm
no
t sig
nific
ant
20%
eth
anol
Cel
ik35
8 , 201
4 W
F-op
timiz
ed
PRK
12
84
1.
00
1.00
n/
a n/
a n/
a gr
ade
0.5
to 2
in
47%
eye
s
Blu
nt sp
atul
a
Asl
anid
es55
5 ,
2015
WF-
optim
ized
PRK
12
29
n/
a 0.
95
85.7
%
89.3
%
all e
yes
no
20%
eth
anol
Has
hem
i560 ,
2015
WF-
optim
ized
PRK
6 30
1.00
0.
89
n/a
n/a
all e
yes
n/a
Mec
hani
cal
scra
ping
Scha
llhor
n566 ,
2015
WF-
guid
ed
PRK
6 66
2
1.02
0.
95
92.1
%
98.9
%
Abl
. dep
. ≥ 7
0 µm
n/
a 20
% e
than
ol
Gha
raee
559 ,
2015
Stan
dard
PR
K
6 25
W
ith e
ye-tr
acki
ng
1.00
0.
99
n/a
n/a
all e
yes
n/a
n/a
Stan
dard
PR
K
6 25
W
ithou
t eye
-
track
ing
1.00
0.
99
n/a
n/a
all e
yes
n/a
n/a
Kal
uzny
562 ,
WF-
optim
ized
3
103
n/
a n/
a 10
0%
100%
al
l eye
s gr
ade≤
1 in
20
% e
than
ol

96
2016
R
PK
8.89
% e
yes
Ang
554 , 2
016
Stan
dard
PR
K
3 34
7
1.09
0.
88
96.5
%
99.7
%
Abl
. dep
. ≥65
µm
or >
1 cy
linde
r
grad
e≤2
in
46.1
% e
yes
20%
eth
anol
Koc
amis
563 ,
2016
Stan
dard
PR
K
42.3
22
1.21
1.
08
n/a
n/a
<-6D
SE
corr
ectio
n
grad
e 0.
5 in
18%
eye
s
20%
eth
anol
Has
hem
i561 ,
2016
WF-
optim
ized
PRK
60
145
1.
04
1.02
89
%
96%
al
l eye
s no
t sig
nific
ant
20%
eth
anol
Tran
sepi
thel
ial P
RK
Gha
dhfa
n569 ,
2007
Stan
dard
T-
PRK
8.9
37
Low
to m
oder
ate
myo
pia
n/a
0.93
95
%
n/a
n/a
not s
igni
fican
t PT
K
Stan
dard
T-
PRK
8.9
22
Hig
h m
yopi
a n/
a 0.
84
95%
n/
a n/
a no
t sig
nific
ant
PTK
WF:
Wav
efro
nt; T
-PR
K: T
rans
epith
elia
l PR
K; S
I: Sa
fety
Inde
x= p
reop
erat
ive
CD
VA
/pos
tope
rativ
e C
DV
A; E
I: Ef
ficac
y In
dex
= po
stop
erat
ive
UD
VA
/pre
oper
ativ
e C
DV
A; M
MC
: Mito
myc
in C
; Abl
. dep
.= a
blat
ion
dept
h.

97
Tab
le 3
. Lite
ratu
re R
evie
w o
f Stu
dies
Pre
sent
ing
Res
ults
of L
aser
Cor
neal
Ref
ract
ive
Surg
ery
for
Mod
erat
e to
Hig
h A
stig
mat
ism
Cor
rect
ion
Pr
eope
rativ
e Po
stop
erat
ive
Aut
hor,
year
Su
rger
y (p
latfo
rm)
Follo
w-u
p
(mon
ths)
Eyes
Sp
here
(D)
Cyl
inde
r (D
) C
ylin
der (
D)
UD
VA≥
20/4
0
UD
VA≥
20/2
0
Cyl
inde
r
≤ 0.
5 D
Cyl
inde
r
≤ 1.
0 D
SE w
ithin
±0.5
D
SE w
ithin
±1.0
D
Arb
elae
z573 , 2
009
LASI
K (A
mar
is)
6 50
3.54
±0.8
5
(-4.
75, -
2.00
)
0.50
±0.2
6
(-1.
25, 0
.00)
100%
84
%
76%
94
%
78%
Abo
lhas
sani
570 ,
2009
LASI
K (N
IDEK
EC
-
5000
)
30
34
-0.1
25±0
.50
(-0.
75, +
0.75
)
-4.7
3±0.
89
(-7.
00, -
4.00
)
-0.2
9±0.
47
(-1.
50, 0
.00)
97.1
%
23.5
%
70.6
%
94.1
%
Igar
ashi
576 , 2
012
LASI
K (T
echn
olas
217z
)
12
48
-5.1
0±2.
11
(-10
.75,
-1.5
0)
-2.7
4±0.
99
(-6.
00, -
2.00
)
-0.6
3±0.
63
(-2.
50, 0
.00)
Has
egaw
a575 ,
2012
LASI
K (M
EL-8
0)
12
30
-2.2
6±2.
39
-3.6
6±0.
44
-0.6
8±0.
52
53.3
%
83.3
%
Kat
z578 , 2
013
LASI
K
(Alle
gret
to 2
00/4
00)
2-6
57
-1.8
9±1.
72
(-6.
75, 0
)
-3.8
6±0.
57
(-5.
75, -
3.25
)
-1.2
3±0.
51
(-3.
75, 0
.00)
91.2
%
12%
54
%
67%
93%
PRK
(A
llegr
etto
200/
400)
57
-2
.82±
2.06
(-6.
75, 0
.00)
3.81
±0.6
3
(-5.
75, -
3.25
)
-1.2
9±0.
67
(-2.
50, -
0.25
)
77.2
%
21%
39%
54
%
86%
Alio
572 , 2
013
LASI
K (A
mar
is)
6 37
-2
.72±
1.93
(-8.
00, -
0.25
)
-3.6
1±0.
58
(-5.
25, -
3.00
)
-0.4
5±0.
38
(-1.
25, 0
.00)
94%
61
%
67%
93
%
87%
97
%
Alio
571 , 2
013
LASI
K (A
mar
is)
3 52
2.
41±1
.26
(0.2
5, 5
.00)
-3.8
9±0.
70
(-5.
25, -
3.00
)
-1.1
1±0.
67
(-3.
50, 0
.00)
85%
26.9
%
65.3
%
Ivar
sen57
7 , 201
3 LA
SIK
(MEL
-80)
3
46
-3.1
0±2.
60
(-10
.00,
0.0
0)
-3.9
2±0.
82
(-6.
00, -
2.75
)
-1.0
0±0.
50
(-2.
25, -
0.25
)
94.4
%
25%
87%
98
%
52
3.
50±2
.30
(0.0
0, 8
.75)
-4.4
2±1.
10
(-6.
50, -
2.00
)
-1.4
0±0.
90
(-4.
50, 0
.00)
86.4
%
13.6
%
71%
90
%

98
Boh
ac54
6 , 201
4 LA
SIK
(Alle
gret
to 4
00)
12
127
-2.8
0±2.
01
(-8.
50, 0
.00)
-3.3
0±1.
00
(-7.
50, -
2.00
)
-0.5
5±0.
46
(-2.
25, 0
.00)
48%
61
2.
72±1
.79
(0.2
5, 7
.00)
-3.8
4±1.
21
(-6.
50, -
2.00
)
-0.8
5±0.
41
(-2.
00, 0
.00)
28%
LASI
K (A
mar
is 7
50S)
119
-2.4
4±2.
17
(-7.
50, 0
.00)
-3.2
1±0.
87
(-6.
50, -
2.00
)
-0.4
3±0.
36
(-1.
50, 0
.00)
54%
11
1 3.
11±1
.57
(0.5
0, 7
.50)
-3.6
6±1.
16
(-7.
00, -
2.00
)
-0.5
8±0.
38
(-1.
50, 0
.00)
42%
Ivar
sen40
2 , 201
4 SM
ILE
(Vis
umax
) 3
106
-4.3
0±2.
66
(-9.
50, -
0.25
)
-3.2
2±0.
67
(-5.
75, -
2.50
)
-0.7
9±0.
58
(-2.
75, 0
)
89%
39
.6%
77
%
97%
Frin
gs57
4 , 201
4 LA
SEK
(Mel
80)
6
82
-3.9
8±2.
28
(-10
.00,
0.0
0)
-2.5
0±0.
82
(-5.
00, 0
.00)
-0.2
7±0.
41
(-1.
50, 0
.00)
76%
89
%
Scha
llhor
n579 ,
2015
LASI
K
(Vis
x S4
IR)
3 61
1 -2
.79±
2.32
(-9.
75, 0
.00)
-2.7
6±0.
81
(-6.
00, -
2.00
)
-0.3
7±0.
38
(-2.
00, 0
.00)
83
.8%
79
.1%
95
.7%
90
.3%
99
.2%
Cur
rent
stud
y Tr
ans P
RK
(iV
IS)
≥ 6
153
-1.5
8±1.
42
(-6.
50, 0
.00)
-2.6
7±0.
77
(-5.
75, -
2.00
)
-0.3
9±0.
32
(-1.
50, 0
.00)
99%
92
%
82.4
%
97.4
%
83.7
%
99.3
%
53
0.
83±0
.54
(0.2
5, 2
.25)
-2.8
2±0.
79
(-5.
25, -
2.00
)
-0.6
5±0.
46
(-1.
75, 0
.00)
98%
83
%
56.7
%
84.9
%
79.2
%
94.3
%

99
9.2 Effect of Transepithelial TGCA in the Treatment of Irregular
Astigmatism In study 6, we analyzed the transepithelial TGCA technique in 17 eyes of 16 patients with
visually disturbing irregular astigmatism and/or scattering in LASIK flap/interface
complications. The concept was: 1) to regularize the cornea and treat the irregular
astigmatism and 2) to ablate the underlying anatomical substrate and remove a potential
source for scattering.
In addition to the successful treatment of optical irregularities, our study generally
showed good refractive outcomes as well, even though the treatment of regular sphere and
cylinder was our secondary aim. Already in 2000, Alessio and colleagues621 published a study
where basically the same concept as in ours was applied by using an early version of CIPTA
software for the TGCA planning in the treatment of irregular astigmatism. The outcomes
showed good safety, while the efficacy and predictability were below the level of the current
results, which can be explained by far the more advanced hardware technology and
continuous refinement of the software that occurred in the years between the two projects.
Two of the eyes in our study were not aimed for emetropia; one due to a lack of
available corneal tissue, and the other in order to achieve isometropia. Five eyes still needed
enhancement to treat the residual refractive error, which may be attributed to: First, error in
planning of the spherocylindrical correction due to the influence of HOAs on the measured
amount of the preoperative sphere and cylinder;622 and second, epithelial remodelling, which
occurs after the current treatment, affecting the final refractive outcome. Thus, a more precise
preoperative refraction measurement and better knowledge and control of the postoperative
epithelial healing/remodelling process may improve the refractive outcome.
9.3 Combined Treatment of Transepithelial TGCA and CXL in
Treatment of Keratoconus
9.3.1 Corneal Biomechanics in Virgin and Post-PRK Eyes Corneal refractive laser ablation in virgin eyes weakens the cornea mechanically due to tissue
removal, leading to a deterioration in corneal biomechanical strength.623 Biomechanical
changes may also affect the refractive outcome.624 Moreover, biomechanical weakening after
corneal refractive laser treatment may potentially induce iatrogenic keratectasia.625 Therefore,

100
knowledge of corneal biomechanical properties is important in predicting clinical outcomes626
and in identifying cases with high risk for postoperative keratectasia after corneal refractive
surgery. In study 7, we tested the hypothesis that the CorVis ST performs reliable
measurements in both virgin and post-refractive surgery eyes. The secondary purpose was to
test the hypothesis that the measurements can reveal differences in biomechanical properties
between these two groups.
Similar to the studies performed by Nemeth et al.282 and Hon et al.,275 we found
that the following parameters had the best repeatability in both groups: CCT, IOP, 1st
applanation time, and deformation amplitude. Our study also presented good repeatability for
2nd applanation time. In addition, the ICCs in the current study were generally higher than in
the mentioned studies for most of the parameters measured. The differences between the
studies may be attributed to different patient populations and software versions. For example,
in the study by Nemeth et al., the mean age was 61.24±15.72 years (95% CI: 57.62 to 64.86
years), while the population in the current study was much younger. In the study by Hon et
al., the software did not offer values for the radius of curvature and peak distance. When
comparing reproducibility, Hon et al. found a statistically significant difference in the CCT
measurement between the two sessions. However, the intersession difference was calculated
by comparing the examinations performed in the morning (9:00–10:99 am) and afternoon
(3:99–5:99 pm) by the same observer. This time difference may have affected the
reproducibility evaluation, as corneal thickness demonstrates diurnal variation.627 The other
parameters measured with the CorVis ST did not show satisfactory reliability. The ICCs
varied between the virgin and post-PRK eyes.
It is conceivable that the cornea would be more difficult to deform and would deform
less in eyes with a greater CCT. In line with other studies,275, 284 we revealed a negative
correlation between CCT and deformation amplitude in both groups. In addition, the CCT
correlated positively with 1st applanation time and radius of curvature in both virgin and post-
PRK eyes. However, correlations between CCT and 1st applanation velocity, 2nd applanation
time, length, and velocity were only found in post-PRK eyes. This may imply that CCT in
normal virgin eyes does not introduce much variation to some of the CorVis ST parameters,
while affecting those measurements in biomechanically compromised corneas. The MRSE in
our virgin-eyes group demonstrated correlation with some of the parameters measured by
CorVis ST. This may need to be taken into consideration if a database of “healthy corneas” is
built for the purpose of identifying biomechanically weaker corneas.

101
The IOP measured with the CorVis ST was significantly lower in the post-PRK eye
group compared to the virgin-eye group, while the historical preoperative data (IOP measured
by Icare, CCT, and corneal curvature) of the post-PRK group showed no significant
difference compared to the respective data in the virgin-eye group. The CorVis ST
measurements in our post-PRK group were performed a minimum of two months
postoperatively, by which time the patients had discontinued the use of local steroids for at
least three weeks, to exclude a possible pharmacological effect on their IOP. Some studies
have demonstrated that IOP measured with the CorVis ST is more reliable compared to
Goldmann applanation tonometry (GAT) and Topcon noncontact tonometry in virgin eyes
(Topcon CT-80A Computerized Tonometer; Topcon, Tokyo, Japan).628 Still, in the version of
CorVis ST used in this study, IOP is calculated based on the timing of the 1st applanation
event and is not adjusted for corneal biomechanical properties. Both CCT and corneal
biomechanical properties can affect IOP measurements, with the latter suggested to be more
influential.629 The difference in the CorVis ST measured IOP between the groups was most
likely caused by changes in corneal biomechanical properties and CCT after PRK.
Interestingly, before being adjusted for age, CCT, and simK, the CorVis ST
parameters that demonstrated differences between the virgin and post-PRK eyes (1st
applanation time, 1st applanation velocity, 2nd applanation time, 2nd applanation velocity,
deformation amplitude and radius of curvature) were the same parameters as those showing
differences between normal eyes and keratoconus eyes in the study conducted by Ali et al.276
It seems that these parameters may be of value in evaluating corneal biomechanical
properties.
The earlier start of the apex indentation (shorter 1st applanation time) and greater
deformation amplitude in post-PRK eyes indicates a lower resistance to deformation due to a
decrease in corneal stiffness.292, 630 Shen et al.288 compared corneal deformation parameters
after femtosecond laser small incision lenticule extraction (SMILE), laser-assisted sub-
epithelial keratomileusis (LASEK), and femtosecond laser-assisted LASIK (FS-LASIK).
They found greater deformation amplitude and shorter 1st applanation time in the FS-LASIK
group compared to the LASEK group. However, those parameters did not differ significantly
between the SMILE and LASEK groups, or between SMILE and FS-LASIK groups. This
indicates that corneal refractive surgery alters the stiffness of the cornea to different degrees
with respect to different surgical approaches.
In the current study, the CorVis ST measurements in virgin- and post-PRK eyes were
taken from two groups of unrelated populations. Pre- and postoperative comparison of the
102
same population would have been better suited to evaluate changes in the biomechanical
properties caused by the surgery. We attempted to compensate for this by applying age, CCT,
and simK as covariates to adjust for potential confounding factors. For the sake of this
discussion, we also introduced a separate group of 28 eyes of 16 patients who underwent PRK
for myopic astigmatism (mean preoperative MRSE: -3.35±1.98 D, mean postoperative time
9.21±5.09 months) with both pre- and postoperative CorVis ST measurements. The pre- and
postoperative CorVis ST measurements of CCT and IOP in that group [547.53±28.89 µm vs.
460.32±48.57 µm (p<0.05), and 15.00±1.48 mmHg vs. 13.48±1.24 mmHg (p<0.001),
respectively] were similar to the differences found in the virgin and post-PRK eyes in the
current study. Comparable similarity was also found for the 1st applanation time [7.37±0.23 vs.
7.14±0.20 ms (p<0.001)], 2nd applanation time (21.39±0.32 vs. 21.57±0.25 ms (p<0.05),
radius of curvature [7.76±0.83 vs. 6.55±0.66 mm (p<0.001)] and deformation amplitude
[1.03±0.08 vs. 1.10±0.08 mm, (p<0.05)]. Still, a separate study measuring pre- and post-PRK
parameters with a larger population is warranted.
9.3.2 CXL in Treatment of Keratectasia Corneal collagen crosslinking is a minimally invasive procedure for treating keratoconus and
iatrogenic keratectasia by increasing the biomechanical stability of the corneal stroma.438-442
The corneal epithelium with its tight junctions and hydrophobic character is the most
important barrier to the penetration of hydrophilic macromolecules like riboflavin.453 Thus,
with the “standard protocol” (“epithelium-off” CXL), the removal of the corneal epithelium
before the application of riboflavin is considered crucial to enable sufficient intrastromal
diffusion of riboflavin.443, 454, 455 To avoid potential complications occurring due to epithelial
removal, such as delayed re-epithelialization, keratitis, or severe pain, modifications of the
technique with the epithelium kept intact (“epithelium-on” CXL) have been developed.459, 464,
472, 631 The safety and efficacy of different CXL protocols have been documented by various
studies.472, 632-635 In study 8, a multifactorial approach was utilized to enhance the riboflavin
penetration by employing: 1) BAC-containing local medication; 2) hypotonic riboflavin
solution without dextran; 3) increased riboflavin solution concentration; 4) mechanical
disruption of the superficial epithelium (micro-abrasions); and 5) prolongation of the
riboflavin-induction time until objective verification of the stromal saturation is confirmed.
Epithelial permeability can be enhanced by the application of several tensioactive
substances including BAC and gentamycin at concentrations normally used in industrial

103
preparations.636 Such pharmacological enhancements, which are commonly used in
epithelium-on CXL,459 were included in our protocol. On the basis of previous studies
reporting increased epithelial riboflavin permeability using hypotonic solution compared to
isotonic solution,637, 638 hypotonic solution was applied in our protocol. Furthermore, we
avoided the use of riboflavin solution with dextran due to its high viscosity, which inhibits
penetration through the epithelium.639 Hypotonic riboflavin was originally used with
epithelium-off CXL protocol to induce significant edema in corneas thinner than 400 μm.638
However, the swelling of the corneas with intact epithelium seem to be of a considerably
lower degree. In our study, only around 10 microns of swelling was recorded in a subgroup of
29 eyes, presenting respective mean pachymetry of 450.50±42.90 and 471.65±41.43 μm
before and after the corneal saturation with the 0.5% hypotonic riboflavin solution. Even
though the clinical safety of CXL with hypotonic riboflavin solution has been documented,640
issues with the corneal endothelial cell toxicity were considered because of the decreased UV-
protective effect with hypotonic riboflavin due to the decrease of UV-absorption coefficient
from ≈ 53 cm-1 for 0.1 % isotonic Riboflavin solution, to ≈ 42 cm-1 for 0.1 % hypotonic
riboflavin solution.640 To compensate for this, the concentration of riboflavin in the
hypoosmolar solution may be increased to enhance UVA absorption476 and hence decrease the
UV-radiation at the endothelial level. In our study, a hypotonic riboflavin concentration of 0.5%
was applied. A secondary benefit of the increased concentration was the presumably
increased availability of the riboflavin molecules to penetrate the epithelium and saturate the
stroma. In a subgroup analysis of 21 eyes by the use of pre- and postoperative specular
microscopy with Konan CellCheck XL (Konan Medical, Irvine, CA), the endothelial count
decreased insignificantly, from 2738±188 cells/mm2 to 2608±311 cells/mm2.
Our protocol also employed mechanical scarification of the epithelial surface by the
creation of micro-abrasions caused by the movement of a merocel sponge over the corneal
surface with patient blinking. The amount of such micro-abrasions could obviously not be
standardized and varied between cases. This may be the reason for a relatively large variation
in saturation time (mentioned in the next paragraph).
Finally, in addition to the chemical and mechanical enhancements, our protocol
demanded a slit-lamp verification of the stromal saturation before the UVA-radiation (Figure
12). Our clinical observations showed that riboflavin saturation was achieved after 25-45
minutes, so that a commonly used set induction time of e.g. 30 minutes, would in many cases
lead to insufficient riboflavin concentration in the stroma.

104
Our visual and refractive outcomes were comparable to other published CXL studies.
In the current study, there were no cases with a loss of ≥ 2 lines of CDVA, endothelial cell
count did not change significantly, and there were no infections or other types of keratitis.
Most of the patients reported pain peaking 4-6 hours after the treatment despite the
mostly preserved epithelium. This may be explained by actinic-keratoconjunctivitis-like
reaction caused by the UV-exposure during the treatment and by the micro-abrasions caused
on purpose, to enhance riboflavin penetration.
Corneal topography change in curvature has often been used to evaluate the effect of
CXL.464, 641, 642 In our study, the maximum-K value and DSI (differential sector index)
decreased significantly on the OPD II, Placido-based topography, as did the posterior
elevation, irregularity index and asymmetry on the Precisio, Scheimpflug-based topography.
However, our mean-K did not decrease in contrast to most other studies. In most of our cases,
in addition to the Max-K decrease, a moderate increase in steepness on the opposite side of
the cone occurred, resulting in only a minor decrease of the mean-K, but more symmetrical
corneal optics, decreased higher-order-aberrations, and improved vision. We hypothesize that
this may be a consequence of a possibly heavier riboflavin load in the inferior corneal stroma
due to the sitting position and blinking during the riboflavin induction, leading to a locally
increased cross-linking effect. This theory warrants further study and may be a small step in
the direction of “customized” CXL.
Detection of the demarcation line468 after CXL has been considered proof of the
efficacy and the measure of the depth of the corneal cross-linking. Although the precise
nature and significance of the demarcation line (increased optical density) in relation to the
cross-linking process are uncertain, it may be consequent to the keratocyte apoptosis and their
subsequent repopulation.643 Keratocyte apoptosis has to a lesser extent been demonstrated
after epithelium-on CXL.466 Filipello´s epithelium-on CXL with 0.1% isotonic riboflavin
solution showed that the demarcation line two weeks postoperatively was located
approximately 100 μm from the corneal epithelium.464 In 24 eyes treated with the current
protocol that could be evaluated by RTVue (Optovue Inc., Fremont, CA) AS-OCT (anterior
segment optical coherence tomography), the mean demarcation line was located at the depth
of 316.92±49.16 μm (range 260 to 367) from the surface, which is close to the observations
after epithelium-off CXL.
Epithelial absorption/filtering of the UVA light that could potentially lead to lesser
energy delivered to riboflavin-saturated stroma, has also been stated as an argument against
the use of epithelium-on CXL. Different studies offer a variety of evaluation backgrounds of
105
this matter. A study performed by Baiocci et al.453 claimed that human corneal epithelium and
the underlying basement membrane naturally absorbs 30% to 33% of UVA radiation (400 to
350 nm), while other studies showed that the epithelial UV absorption occurs only with
wavelengths lower than 310 nm.501, 644, 645 We may assume that the UV-absorption of the
riboflavin within the epithelium is probably low (since the epithelial cells are hydrophobic
and do not absorb riboflavin) and that the epithelial interstitial space is of negligible volume
to allow riboflavin to accumulate and contribute to UV-absorption. In addition, our protocol
included washing off the riboflavin from the corneal surface before the UVA-radiation in
order to minimize the UV-energy loss due to its possible absorption by riboflavin.
Our retrospective study showed that epithelium-on CXL using our novel protocol
appeared to be effective and safe in treating progressive keratoconus. The improvements in
visual, refractive and topographic parameters indicated that epithelium-on CXL had a
sufficient effect to halt the progression of keratoconus and improve the corneal shape.
However, CXL is an oxygen-dependent process646 and the intact epithelium might represent
an additional barrier to oxygen molecules and could be the reason for lower efficacy in
corneal flattening compared to the epithelium-on CXL. At present, the literature on
transepithelial CXL reports an evident morphologic impact of epi-on that is approximately a
third of that of epi-off in vitro and in vivo, without uniformity of protocols. The epi-on CXL
was around 70-80% less effective in terms of biomechanical strength than standard epi-off
CXL.88, 466 A randomized controlled trial is warranted to verify that the effect of the current
approach is comparable with the standard epithelium-off CXL. Furthermore, the combination
of different enhancers, osmolality and concentration of riboflavin should be explored to
further improve the procedure.
9.3.3 Combination of Transepithelial TGCA and CXL in Treatment of
Keratectasia A study with ten-year results demonstrated that CXL was effective in treating progressive
keratoconus, achieving long-term stabilization of the condition.634 However, the CXL does
not directly address the patient´s refractive error. The spherocylindrical change that it
achieves is limited. Our study 6 has shown that the topography-guided custom ablation is a
suitable treatment for regularizing visually disturbing irregular astigmatism in non-ectatic
corneas with sufficient thickness. However, laser ablation is commonly considered
contraindicated in unstable corneas with keratectasia because of the danger of worsening of

106
the corneal structural stability and its consequences, caused by tissue removal. Topography-
guided custom ablation and CXL combines the benefits of both treatments with the potential
for creating a safe and stable optical improvement of the irregular keratectatic cornea in a less
invasive fashion. The concept was first introduced by Kanelloloulos and Binder.647 In that
study, the laser ablation was performed 12 months after CXL. Ablation performed after CXL
may however cause a reduction in corneal strength in the ablation area by removal of the
superficial (supposedly the most strengthened) part of the CXL-treated tissue. In our studies 3
and 9, we performed the procedure in a reverse order by applying CXL immediately after
topography-guided custom ablation to strengthen the stroma, before the ectatic process had a
chance to progress.
Our studies showed relatively good safety, efficacy, and predictability of the combined
treatment, which was confirmed by improvement in CDVA and corneal regularity. The
advantages of performing cTEN and CXL within the same surgical session may include the
fact that laser ablation does not interfere with the cornea where the CXL takes place, while
CXL of the ablated stroma depletes keratocytes of the anterior cornea, thus reducing the
possibility of postoperative haze. Similar results have been reported by other studies.521, 523
Generally, patients undergoing this dual procedure experience an increase in uncorrected
visual acuity and improved corneal irregularity and resistance. However, the procedure is not
free from complications. Guell et al.648 recently reported a late onset, persistent, deep stromal
haze alteration in contact with the endothelium after the combined procedure. The focal haze
improved with a corticoid-based treatment; however, the haze clearly affected visual acuity.
The authors therefore advocated that a longer follow-up study that includes data from more
cases was necessary to determine whether this combination should be a standard approach.
Alessio and colleagues649 performed a long-term confocal microscopy evaluation of corneas
up to 48 months after the treatment by the combined procedure. They showed permanently
decreased keratocyte density in the anterior stroma, while the other corneal structures mostly
reached their preoperative characteristics six months after treatment. A prospective clinical
study by the same authors compared two eyes of 17 patients, with progressive keratoconus,
where the best eye was treated by only CXL, and the fellow eye received CXL treatment after
previous corneal regularization by transepithelial TGCA.518 They showed that the combined
procedure increased vision, reduced corneal aberrations and stabilized corneas, while CXL
alone stabilized and flattened corneas with no significant visual impact. A recently published
study by Kontadakis and colleagues650 came to a similar conclusion in a long-term
comparative study. Their simultaneous transepithelial PRK followed by CXL offered

107
significantly improved vision to treated patients with keratoconus in comparison with CXL
alone, while similar results regarding postoperative stability were achieved.
9.4 Ethics All studies were performed in accordance with the Declaration of Helsinki. All examinations
mentioned in the current project are part of the clinic´s standard routine examinations. The
approvals from The Regional Ethics Committee (REC) were obtained. The use of data for
retrospective studies was reported to the Norwegian Data Protection Authority. Informed
consent for the anonymous use of data for analysis and publication was obtained from study
subjects.
10. FUTURE PERSPECTIVES 10.1 Corneal Biomechanical Property Measurement with the
CorVis ST The CorVis ST’s direct view of corneal deformation may offer information that promises to
yield clinically relevant parameters correlated with corneal biomechanical properties.
However, more work needs to be done to explore the optimal parameters representing the
corneal biomechanical strength.
10.2 Stromal Surface Topography-Guided Custom Ablation Our study shows that transepithelial TGCA is effective in the treatment of corneal irregular
astigmatism. Stromal surface topography-guided ablation by incorporating the epithelial
thickness profile into the corneal topography might offer advantages over the current
transepithelial TGCA.
11. CONCLUSIONS 11.1 General Conclusion Topography-guided customized corneal ablation is safe and effective in optical regularization
in eyes with irregular astigmatism, while CXL is the first causative therapy that achieves
biomechanical stabilization in keratoconus. The combination of topography-guided treatment

108
with CXL is a promising therapy for keratoconus and corneal keratectasia to achieve both
goals and decrease the need for corneal transplantation.
11.2 Conclusions of the individual papers
Paper I We concluded that Custom-Q ablation resulted in a mean postoperative
asphericity that was closer to preoperative compared to wavefront optimized
ablation, whereas the other outcome parameters showed no statistically
significant differences.
Paper II We conclude there was a trend towards greater epithelial thickening with a
larger amount of programmed SE correction, smaller treatment zone, and
thinner preoperative epithelium. No correlation between epithelial thickness
change and postoperative change in refraction was detected.
Paper III We concluded that a significant epithelial thickness profile change occurred
after treatment, with an increase in thickness in the preoperatively thinnest
area. The thickness remained largely unchanged in the other areas, resulting in
a more even epithelial thickness distribution, which may be attributed to
regularized postoperative corneal stromal shape.
Paper IV We concluded that one-step transepithelial topography-guided treatment for
low to moderate myopia and astigmatism performed with a 1 KHz laser
provided safe, effective, predictable and stable results with low pain and no
visually significant haze.
Paper V We concluded that transepithelial TGCA appeared to be a safe, effective, and
predictable treatment for moderate to high astigmatism.
Paper VI We concluded that corneal regularization and removal of the underlying flap or
interface pathology by transepithelial TGCA appeared to be an effective
treatment for LASIK flap or interface complications associated with visually

109
disturbing irregular astigmatism and light scattering in cases with sufficient
residual stromal thickness.
Paper VII We concluded that CorVis ST demonstrated reliable measurements for CCT,
IOP, and 1st applanation time, as well as relatively reliable measurement for
deformation amplitude in both virgin and post-PRK eyes. There were
differences in 1st applanation time and deformation amplitude between virgin
and post-PRK eyes, which may reflect corneal biomechanical changes
occurring after surgery in the latter.
Paper VIII We concluded that epithelium-on CXL with our novel protocol appeared to be
safe and effective in the treatment of progressive keratoconus.
Paper IX We concluded that the combination of topography-guided custom ablation and
CXL improved patients’ visual, refractive, and topography outcomes and
halted the progression of keratectasia within the observation period of 12
months. This method may postpone or eliminate the need for corneal
transplantation in suitable cases with keratectasia.

110
12. ERRATA Page 4, line 29: Combination with
Page 4, line 31: .. the Study
Page 4, line 32: Aims of the
Page 6, line 6: with the
Page 10, line 4: laser-assisted
Page 14, line 32: high astigmatism
Page 22, line 32: Gullstrand´s eye model
Page 24, line 2: Gullstrand´s eye model
Page 104, line 14: deleted “Figure 6”
Page 104, line 30, deleted “Figure 7”

111
13. REFERENCES 1. Mishima S, Gasset A, Klyce SD, Jr., Baum JL. Determination of tear volume and tear
flow. Invest Ophthalmol 1966;5:264-276. 2. Dartt DA. Regulation of mucin and fluid secretion by conjunctival epithelial cells.
Prog Retin Eye Res 2002;21:555-576. 3. Holly FJ, Lemp MA. Tear physiology and dry eyes. Surv Ophthalmol 1977;22:69-87. 4. Dursun D, Monroy D, Knighton R, et al. The effects of experimental tear film removal
on corneal surface regularity and barrier function. Ophthalmology 2000;107:1754-1760.
5. Hanna C, O'Brien JE. Cell production and migration in the epithelial layer of the cornea. Arch Ophthalmol 1960;64:536-539.
6. Doane MG. Blinking and the mechanics of the lacrimal drainage system. Ophthalmology 1981;88:844-851.
7. Stern ME, Beuerman RW, Fox RI, Gao J, Mircheff AK, Pflugfelder SC. The pathology of dry eye: the interaction between the ocular surface and lacrimal glands. Cornea 1998;17:584-589.
8. Paulsen FP, Schaudig U, Thale AB. Drainage of tears: impact on the ocular surface and lacrimal system. Ocul Surf 2003;1:180-191.
9. Klyce SD, Beuerman R. Structures and functions of the cornea. New York: Churchill Livingstone; 1988.
10. Rolando M, Zierhut M. The ocular surface and tear film and their dysfunction in dry eye disease. Surv Ophthalmol 2001;45 Suppl 2:S203-210.
11. Kaido M, Matsumoto Y, Shigeno Y, Ishida R, Dogru M, Tsubota K. Corneal fluorescein staining correlates with visual function in dry eye patients. Invest Ophthalmol Vis Sci 2011;52:9516-9522.
12. Liu H, Thibos L, Begley CG, Bradley A. Measurement of the time course of optical quality and visual deterioration during tear break-up. Invest Ophthalmol Vis Sci 2010;51:3318-3326.
13. The definition and classification of dry eye disease: report of the Definition and Classification Subcommittee of the International Dry Eye WorkShop (2007). Ocul Surf 2007;5:75-92.
14. Bron AJ, Tomlinson A, Foulks GN, et al. Rethinking dry eye disease: a perspective on clinical implications. Ocul Surf 2014;12:S1-31.
15. Albietz JM, Lenton LM. Management of the ocular surface and tear film before, during, and after laser in situ keratomileusis. J Refract Surg 2004;20:62-71.
16. Labbe A, Alalwani H, Van Went C, Brasnu E, Georgescu D, Baudouin C. The relationship between subbasal nerve morphology and corneal sensation in ocular surface disease. Invest Ophthalmol Vis Sci 2012;53:4926-4931.
17. Levinson BA, Rapuano CJ, Cohen EJ, Hammersmith KM, Ayres BD, Laibson PR. Referrals to the Wills Eye Institute Cornea Service after laser in situ keratomileusis: reasons for patient dissatisfaction. J Cataract Refract Surg 2008;34:32-39.
18. Golas L, Manche EE. Dry eye after laser in situ keratomileusis with femtosecond laser and mechanical keratome. J Cataract Refract Surg 2011;37:1476-1480.
19. Murakami Y, Manche EE. Prospective, randomized comparison of self-reported postoperative dry eye and visual fluctuation in LASIK and photorefractive keratectomy. Ophthalmology 2012;119:2220-2224.
20. Pflugfelder SC, Solomon A, Stern ME. The diagnosis and management of dry eye: a twenty-five-year review. Cornea 2000;19:644-649.

112
21. Mian SI, Li AY, Dutta S, Musch DC, Shtein RM. Dry eyes and corneal sensation after laser in situ keratomileusis with femtosecond laser flap creation Effect of hinge position, hinge angle, and flap thickness. J Cataract Refract Surg 2009;35:2092-2098.
22. Vestergaard A, Ivarsen AR, Asp S, Hjortdal JO. Small-incision lenticule extraction for moderate to high myopia: Predictability, safety, and patient satisfaction. J Cataract Refract Surg 2012;38:2003-2010.
23. Sugar A, Rapuano CJ, Culbertson WW, et al. Laser in situ keratomileusis for myopia and astigmatism: safety and efficacy: a report by the American Academy of Ophthalmology. Ophthalmology 2002;109:175-187.
24. Ambrosio R, Jr., Tervo T, Wilson SE. LASIK-associated dry eye and neurotrophic epitheliopathy: pathophysiology and strategies for prevention and treatment. J Refract Surg 2008;24:396-407.
25. Behrens A, Doyle JJ, Stern L, et al. Dysfunctional tear syndrome: a Delphi approach to treatment recommendations. Cornea 2006;25:900-907.
26. Berry S, Mangione CM, Lindblad AS, McDonnell PJ. Development of the National Eye Institute refractive error correction quality of life questionnaire: focus groups. Ophthalmology 2003;110:2285-2291.
27. Mertzanis P, Abetz L, Rajagopalan K, et al. The relative burden of dry eye in patients' lives: comparisons to a U.S. normative sample. Invest Ophthalmol Vis Sci 2005;46:46-50.
28. Bailey MD, Mitchell GL, Dhaliwal DK, Boxer Wachler BS, Zadnik K. Patient satisfaction and visual symptoms after laser in situ keratomileusis. Ophthalmology 2003;110:1371-1378.
29. Albietz JM, Lenton LM, McLennan SG. Chronic dry eye and regression after laser in situ keratomileusis for myopia. J Cataract Refract Surg 2004;30:675-684.
30. Toda I. LASIK and dry eye. Compr Ophthalmol Update 2007;8:79-85; discussion 87-79.
31. Torricelli AA, Santhiago MR, Wilson SE. Topical cyclosporine a treatment in corneal refractive surgery and patients with dry eye. J Refract Surg 2014;30:558-564.
32. Garcia-Zalisnak D, Nash D, Yeu E. Ocular surface diseases and corneal refractive surgery. Curr Opin Ophthalmol 2014;25:264-269.
33. Mori Y, Nejima R, Masuda A, et al. Effect of diquafosol tetrasodium eye drop for persistent dry eye after laser in situ keratomileusis. Cornea 2014;33:659-662.
34. Alfawaz AM, Algehedan S, Jastaneiah SS, Al-Mansouri S, Mousa A, Al-Assiri A. Efficacy of punctal occlusion in management of dry eyes after laser in situ keratomileusis for myopia. Curr Eye Res 2014;39:257-262.
35. Khalil MB, Latkany RA, Speaker MG, Yu G. Effect of punctal plugs in patients with low refractive errors considering refractive surgery. J Refract Surg 2007;23:467-471.
36. DelMonte DW, Kim T. Anatomy and physiology of the cornea. J Cataract Refract Surg 2011;37:588-598.
37. Riordan-Eva P, Cunningham ETJ. Vaughan & Asbury's General Ophthalmology, 18th Edition 18 ed: McGraw-Hill Professional; 18 edition (June 7, 2011); 2011:504.
38. Dua HS, Faraj LA, Said DG, Gray T, Lowe J. Human corneal anatomy redefined: a novel pre-Descemet's layer (Dua's layer). Ophthalmology 2013;120:1778-1785.
39. Ehlers N. Some comparative studies on the mammalian corneal epithelium. Acta Ophthalmol (Copenh) 1970;48:821-828.
40. Reinstein DZ, Archer TJ, Gobbe M, Silverman RH, Coleman DJ. Epithelial thickness in the normal cornea: three-dimensional display with Artemis very high-frequency digital ultrasound. J Refract Surg 2008;24:571-581.

113
41. Friend J KK. Physiology of the conjunctiva: metabolism and biochemistry. In: Cornea. Scientific foundations and clinical practice. (Eds.Smolin G, Thoft R). Boston: Little, Brown and Company, 1987; 2: 16-38.
42. Beuerman RW, Pedroza L. Ultrastructure of the human cornea. Microsc Res Tech 1996;33:320-335.
43. Majo F, Rochat A, Nicolas M, Jaoude GA, Barrandon Y. Oligopotent stem cells are distributed throughout the mammalian ocular surface. Nature 2008;456:250-254.
44. Davanger M, Evensen A. Role of the pericorneal papillary structure in renewal of corneal epithelium. Nature 1971;229:560-561.
45. Schermer A, Galvin S, Sun TT. Differentiation-related expression of a major 64K corneal keratin in vivo and in culture suggests limbal location of corneal epithelial stem cells. J Cell Biol 1986;103:49-62.
46. Pfister RR. The normal surface of corneal epithelium: a scanning electron microscopic study. Invest Ophthalmol 1973;12:654-668.
47. Wang J, Fonn D, Simpson TL, Jones L. Precorneal and pre- and postlens tear film thickness measured indirectly with optical coherence tomography. Invest Ophthalmol Vis Sci 2003;44:2524-2528.
48. Klyce SD. Electrical profiles in the corneal epithelium. J Physiol 1972;226:407-429. 49. Pajoohesh-Ganji A, Stepp MA. In search of markers for the stem cells of the corneal
epithelium. Biol Cell 2005;97:265-276. 50. Wagoner MD. Chemical injuries of the eye: current concepts in pathophysiology and
therapy. Surv Ophthalmol 1997;41:275-313. 51. Green H. The keratinocyte as differentiated cell type. Harvey Lect 1980;74:101-139. 52. Thoft RA, Friend J. Biochemical transformation of regenerating ocular surface
epithelium. Invest Ophthalmol Vis Sci 1977;16:14-20. 53. Sharma A, Coles WH. Kinetics of corneal epithelial maintenance and graft loss. A
population balance model. Invest Ophthalmol Vis Sci 1989;30:1962-1971. 54. Zieske JD. Perpetuation of stem cells in the eye. Eye (Lond) 1994;8 ( Pt 2):163-169. 55. Beebe DC, Masters BR. Cell lineage and the differentiation of corneal epithelial cells.
Invest Ophthalmol Vis Sci 1996;37:1815-1825. 56. Welge-Lussen U, May CA, Neubauer AS, Priglinger S. Role of tissue growth factors
in aqueous humor homeostasis. Curr Opin Ophthalmol 2001;12:94-99. 57. West-Mays JA, Dwivedi DJ. The keratocyte: corneal stromal cell with variable repair
phenotypes. Int J Biochem Cell Biol 2006;38:1625-1631. 58. Komai Y, Ushiki T. The three-dimensional organization of collagen fibrils in the
human cornea and sclera. Invest Ophthalmol Vis Sci 1991;32:2244-2258. 59. Abahussin M, Hayes S, Knox Cartwright NE, et al. 3D collagen orientation study of
the human cornea using X-ray diffraction and femtosecond laser technology. Invest Ophthalmol Vis Sci 2009;50:5159-5164.
60. Aghamohammadzadeh H, Newton RH, Meek KM. X-ray scattering used to map the preferred collagen orientation in the human cornea and limbus. Structure 2004;12:249-256.
61. Morishige N, Shin-Gyou-Uchi R, Azumi H, et al. Quantitative analysis of collagen lamellae in the normal and keratoconic human cornea by second harmonic generation imaging microscopy. Invest Ophthalmol Vis Sci 2014;55:8377-8385.
62. Maurice DM. The structure and transparency of the cornea. J Physiol 1957;136:263-286.
63. Meek KM, Boote C. The organization of collagen in the corneal stroma. Exp Eye Res 2004;78:503-512.

114
64. Hamada R, Giraud JP, Graf B, Pouliquen Y. [Analytical and statistical study of the lamellae, keratocytes and collagen fibrils of the central region of the normal human cornea. (Light and electron microscopy)]. Arch Ophtalmol Rev Gen Ophtalmol 1972;32:563-570.
65. Radner W, Zehetmayer M, Aufreiter R, Mallinger R. Interlacing and cross-angle distribution of collagen lamellae in the human cornea. Cornea 1998;17:537-543.
66. Jester JV, Winkler M, Jester BE, Nien C, Chai D, Brown DJ. Evaluating corneal collagen organization using high-resolution nonlinear optical macroscopy. Eye Contact Lens 2010;36:260-264.
67. Winkler M, Chai D, Kriling S, et al. Nonlinear optical macroscopic assessment of 3-D corneal collagen organization and axial biomechanics. Invest Ophthalmol Vis Sci 2011;52:8818-8827.
68. Kamma-Lorger CS, Boote C, Hayes S, et al. Collagen and mature elastic fibre organisation as a function of depth in the human cornea and limbus. J Struct Biol 2010;169:424-430.
69. Muller LJ, Pels E, Vrensen GF. The specific architecture of the anterior stroma accounts for maintenance of corneal curvature. Br J Ophthalmol 2001;85:437-443.
70. Petsche SJ, Chernyak D, Martiz J, Levenston ME, Pinsky PM. Depth-dependent transverse shear properties of the human corneal stroma. Invest Ophthalmol Vis Sci 2012;53:873-880.
71. Randleman JB, Dawson DG, Grossniklaus HE, McCarey BE, Edelhauser HF. Depth-dependent cohesive tensile strength in human donor corneas: implications for refractive surgery. J Refract Surg 2008;24:S85-89.
72. Boote C, Dennis S, Huang Y, Quantock AJ, Meek KM. Lamellar orientation in human cornea in relation to mechanical properties. J Struct Biol 2005;149:1-6.
73. Daxer A, Fratzl P. Collagen fibril orientation in the human corneal stroma and its implication in keratoconus. Invest Ophthalmol Vis Sci 1997;38:121-129.
74. Boote C, Dennis S, Newton RH, Puri H, Meek KM. Collagen fibrils appear more closely packed in the prepupillary cornea: optical and biomechanical implications. Invest Ophthalmol Vis Sci 2003;44:2941-2948.
75. Jester JV, Moller-Pedersen T, Huang J, et al. The cellular basis of corneal transparency: evidence for 'corneal crystallins'. J Cell Sci 1999;112 ( Pt 5):613-622.
76. Bourne WM, Nelson LR, Hodge DO. Central corneal endothelial cell changes over a ten-year period. Invest Ophthalmol Vis Sci 1997;38:779-782.
77. Tanaka E, Aoyama J, Tanaka M, et al. The proteoglycan contents of the temporomandibular joint disc influence its dynamic viscoelastic properties. J Biomed Mater Res A 2003;65:386-392.
78. Glass DH, Roberts CJ, Litsky AS, Weber PA. A viscoelastic biomechanical model of the cornea describing the effect of viscosity and elasticity on hysteresis. Invest Ophthalmol Vis Sci 2008;49:3919-3926.
79. Maurice DM, Monroe F. Cohesive strength of corneal lamellae. Exp Eye Res 1990;50:59-63.
80. Richoz O, Kling S, Zandi S, Hammer A, Spoerl E, Hafezi F. A constant-force technique to measure corneal biomechanical changes after collagen cross-linking. PLoS One 2014;9:e105095.
81. Hjortdal JO. Regional elastic performance of the human cornea. J Biomech 1996;29:931-942.
82. Torricelli AA, Ford MR, Singh V, Santhiago MR, Dupps WJ, Jr., Wilson SE. BAC-EDTA transepithelial riboflavin-UVA crosslinking has greater biomechanical

115
stiffening effect than standard epithelium-off in rabbit corneas. Exp Eye Res 2014;125:114-117.
83. Wang H, Prendiville PL, McDonnell PJ, Chang WV. An ultrasonic technique for the measurement of the elastic moduli of human cornea. J Biomech 1996;29:1633-1636.
84. Touboul D, Gennisson JL, Nguyen TM, et al. Supersonic shear wave elastography for the in vivo evaluation of transepithelial corneal collagen cross-linking. Invest Ophthalmol Vis Sci 2014;55:1976-1984.
85. Luce DA. Determining in vivo biomechanical properties of the cornea with an ocular response analyzer. J Cataract Refract Surg 2005;31:156-162.
86. Shah S, Laiquzzaman M, Bhojwani R, Mantry S, Cunliffe I. Assessment of the biomechanical properties of the cornea with the ocular response analyzer in normal and keratoconic eyes. Invest Ophthalmol Vis Sci 2007;48:3026-3031.
87. Moreno-Montanes J, Maldonado MJ, Garcia N, Mendiluce L, Garcia-Gomez PJ, Segui-Gomez M. Reproducibility and clinical relevance of the ocular response analyzer in nonoperated eyes: corneal biomechanical and tonometric implications. Invest Ophthalmol Vis Sci 2008;49:968-974.
88. Scarcelli G, Kling S, Quijano E, Pineda R, Marcos S, Yun SH. Brillouin microscopy of collagen crosslinking: noncontact depth-dependent analysis of corneal elastic modulus. Invest Ophthalmol Vis Sci 2013;54:1418-1425.
89. Scarcelli G, Besner S, Pineda R, Yun SH. Biomechanical characterization of keratoconus corneas ex vivo with Brillouin microscopy. Invest Ophthalmol Vis Sci 2014;55:4490-4495.
90. Lombardo M, Lombardo G, Carbone G, De Santo MP, Barberi R, Serrao S. Biomechanics of the anterior human corneal tissue investigated with atomic force microscopy. Invest Ophthalmol Vis Sci 2012;53:1050-1057.
91. Last JA, Thomasy SM, Croasdale CR, Russell P, Murphy CJ. Compliance profile of the human cornea as measured by atomic force microscopy. Micron 2012;43:1293-1298.
92. Dias JM, Ziebarth NM. Anterior and posterior corneal stroma elasticity assessed using nanoindentation. Exp Eye Res 2013;115:41-46.
93. Dawson DG, Grossniklaus HE, McCarey BE, Edelhauser HF. Biomechanical and wound healing characteristics of corneas after excimer laser keratorefractive surgery: is there a difference between advanced surface ablation and sub-Bowman's keratomileusis? J Refract Surg 2008;24:S90-96.
94. Malik NS, Moss SJ, Ahmed N, Furth AJ, Wall RS, Meek KM. Ageing of the human corneal stroma: structural and biochemical changes. Biochim Biophys Acta 1992;1138:222-228.
95. Daxer A, Misof K, Grabner B, Ettl A, Fratzl P. Collagen fibrils in the human corneal stroma: structure and aging. Invest Ophthalmol Vis Sci 1998;39:644-648.
96. Sady C, Khosrof S, Nagaraj R. Advanced Maillard reaction and crosslinking of corneal collagen in diabetes. Biochem Biophys Res Commun 1995;214:793-797.
97. Akhtar S, Bron AJ, Salvi SM, Hawksworth NR, Tuft SJ, Meek KM. Ultrastructural analysis of collagen fibrils and proteoglycans in keratoconus. Acta Ophthalmol 2008;86:764-772.
98. Meek KM, Tuft SJ, Huang Y, et al. Changes in collagen orientation and distribution in keratoconus corneas. Invest Ophthalmol Vis Sci 2005;46:1948-1956.
99. Hayes S, Boote C, Tuft SJ, Quantock AJ, Meek KM. A study of corneal thickness, shape and collagen organisation in keratoconus using videokeratography and X-ray scattering techniques. Exp Eye Res 2007;84:423-434.

116
100. Morishige N, Wahlert AJ, Kenney MC, et al. Second-harmonic imaging microscopy of normal human and keratoconus cornea. Invest Ophthalmol Vis Sci 2007;48:1087-1094.
101. Uzbek AK, Kamburoglu G, Mahmoud AM, Roberts CJ. Change in biomechanical parameters after flap creation using the Intralase femtosecond laser and subsequent excimer laser ablation. Curr Eye Res 2011;36:614-619.
102. Kamiya K, Shimizu K, Ohmoto F. Comparison of the changes in corneal biomechanical properties after photorefractive keratectomy and laser in situ keratomileusis. Cornea 2009;28:765-769.
103. Hayes S, Kamma-Lorger CS, Boote C, et al. The effect of riboflavin/UVA collagen cross-linking therapy on the structure and hydrodynamic behaviour of the ungulate and rabbit corneal stroma. PLoS One 2013;8:e52860.
104. Pan CW, Ramamurthy D, Saw SM. Worldwide prevalence and risk factors for myopia. Ophthalmic Physiol Opt 2012;32:3-16.
105. Lee YY, Lo CT, Sheu SJ, Lin JL. What factors are associated with myopia in young adults? A survey study in Taiwan Military Conscripts. Invest Ophthalmol Vis Sci 2013;54:1026-1033.
106. Mirshahi A, Ponto KA, Hoehn R, et al. Myopia and level of education: results from the Gutenberg Health Study. Ophthalmology 2014;121:2047-2052.
107. Midelfart A, Aamo B, Sjohaug KA, Dysthe BE. Myopia among medical students in Norway. Acta Ophthalmol (Copenh) 1992;70:317-322.
108. Midelfart A. [Myopia--a disease or a physiological defect?]. Tidsskr Nor Laegeforen 1991;111:3635-3637.
109. Midelfart A, Kinge B, Midelfart S, Lydersen S. Prevalence of refractive errors in young and middle-aged adults in Norway. Acta Ophthalmol Scand 2002;80:501-505.
110. Carlson N. Optometry: Daniel Kurtz; 1983. 111. Kiely PM SG, Carney LG. The mean shape of the human cornea. Opt Acta
1982;29:1027-1040. 112. Atchison D SG. Refractive components: cornea and lens. In: Atchison D SG (ed),
Optics of the Human Eye. Edinburgh, United Kingdom: Butterworth-Heinemann; 2003:11-20.
113. Guirao A, Porter J, Williams DR, Cox IG. Calculated impact of higher-order monochromatic aberrations on retinal image quality in a population of human eyes. J Opt Soc Am A Opt Image Sci Vis 2002;19:620-628.
114. McCormick GJ, Porter J, Cox IG, MacRae S. Higher-order aberrations in eyes with irregular corneas after laser refractive surgery. Ophthalmology 2005;112:1699-1709.
115. Wang M. Irregular Astigmatism: Diagnosis and Treatment: Slack Incorporated; 1st edition 2007:320.
116. Binder PS. Optical problems following refractive surgery. Ophthalmology 1986;93:739-745.
117. Mahajan VN. Zernike Circle Polynomials and Optical Aberrations of Systems with Circular Pupils. Applied Optics 1994;33:8121-8124.
118. D. M. Optical Shop Testing. New York: Wiley-Interscience, New York, NY ; 1912:792. 119. Griffiths M, Zahner K, Collins M, Carney L. Masking of irregular corneal topography
with contact lenses. CLAO J 1998;24:76-81. 120. Kanpolat A, Ciftci OU. The use of rigid gas permeable contact lenses in scarred
corneas. Clao j 1995;21:64-66. 121. Jupiter DG, Katz HR. Management of irregular astigmatism with rigid gas permeable
contact lenses. CLAO J 2000;26:14-17.

117
122. Yanai R, Ueda K, Nishida T. Retrospective analysis of vision correction and lens tolerance in keratoconus patients prescribed a contact lens with dual aspherical curves. Eye Contact Lens 2010;36:86-89.
123. A. K, O.U. C. The use of rigid gas permeable contact lenses in scarred corneas. . CLAO J. 1995;64-66. 124. Durrie DS, Schumer DJ, Cavanaugh TB. Holmium:YAG laser thermokeratoplasty for
hyperopia. J Refract Corneal Surg 1994;10:S277-280. 125. Thompson VM, Seiler T, Durrie DS, Cavanaugh TB. Holmium:YAG laser
thermokeratoplasty for hyperopia and astigmatism: an overview. Refract Corneal Surg 1993;9:S134-137.
126. Moreira H, Campos M, Sawusch MR, McDonnell JM, Sand B, McDonnell PJ. Holmium laser thermokeratoplasty. Ophthalmology 1993;100:752-761.
127. Hennekes R. Holmium:YAG laser thermokeratoplasty for correction of astigmatism. J Refract Surg 1995;11:S358-360.
128. Asbell PA, Maloney RK, Davidorf J, Hersh P, McDonald M, Manche E. Conductive keratoplasty for the correction of hyperopia. Trans Am Ophthalmol Soc 2001;99:79-84; discussion 84-77.
129. Kato N, Toda I, Kawakita T, Sakai C, Tsubota K. Topography-guided conductive keratoplasty: treatment for advanced keratoconus. Am J Ophthalmol 2010;150:481-489.e481.
130. Celik U, Alagoz N, Yildirim Y, et al. New method of microwave thermokeratoplasty to correct myopia in 33 eyes: one-year results. J Cataract Refract Surg 2013;39:225-233.
131. Vega-Estrada A, Alio JL, Plaza Puche AB, Marshall J. Outcomes of a new microwave procedure followed by accelerated cross-linking for the treatment of keratoconus: a pilot study. J Refract Surg 2012;28:787-793.
132. Schanzlin DJ, Asbell PA, Burris TE, Durrie DS. The intrastromal corneal ring segments. Phase II results for the correction of myopia. Ophthalmology 1997;104:1067-1078.
133. Burris TE. Intrastromal corneal ring technology: results and indications. Curr Opin Ophthalmol 1998;9:9-14.
134. Rabinowitz YS. Intacs for keratoconus. Curr Opin Ophthalmol 2007;18:279-283. 135. Kubaloglu A, Sari ES, Cinar Y, et al. Comparison of mechanical and femtosecond
laser tunnel creation for intrastromal corneal ring segment implantation in keratoconus: prospective randomized clinical trial. J Cataract Refract Surg 2010;36:1556-1561.
136. Kubaloglu A, Sari ES, Cinar Y, Koytak A, Kurnaz E, Ozerturk Y. Intrastromal corneal ring segment implantation for the treatment of keratoconus. Cornea 2011;30:11-17.
137. Sogutlu E, Pinero DP, Kubaloglu A, Alio JL, Cinar Y. Elevation changes of central posterior corneal surface after intracorneal ring segment implantation in keratoconus. Cornea 2012;31:387-395.
138. Pinero DP, Alio JL, El Kady B, et al. Refractive and aberrometric outcomes of intracorneal ring segments for keratoconus: mechanical versus femtosecond-assisted procedures. Ophthalmology 2009;116:1675-1687.
139. Rabinowitz YS, Li X, Ignacio TS, Maguen E. INTACS inserts using the femtosecond laser compared to the mechanical spreader in the treatment of keratoconus. J Refract Surg 2006;22:764-771.
140. Ertan A, Colin J. Intracorneal rings for keratoconus and keratectasia. J Cataract Refract Surg 2007;33:1303-1314.

118
141. Ferreira TB, Guell JL, Manero F. Combined intracorneal ring segments and iris-fixated phakic intraocular lens for keratoconus refractive and visual improvement. J Refract Surg 2014;30:336-341.
142. Park J, Gritz DC. Evolution in the use of intrastromal corneal ring segments for corneal ectasia. Curr Opin Ophthalmol 2013;24:296-301.
143. Torquetti L, Berbel RF, Ferrara P. Long-term follow-up of intrastromal corneal ring segments in keratoconus. J Cataract Refract Surg 2009;35:1768-1773.
144. Vega-Estrada A, Alio JL, Brenner LF, Burguera N. Outcomes of intrastromal corneal ring segments for treatment of keratoconus: five-year follow-up analysis. J Cataract Refract Surg 2013;39:1234-1240.
145. Vega-Estrada A, Alio JL, Plaza-Puche AB. Keratoconus progression after intrastromal corneal ring segment implantation in young patients: Five-year follow-up. J Cataract Refract Surg 2015;41:1145-1152.
146. Rozema JJ, Van Dyck DE, Tassignon MJ. Clinical comparison of 6 aberrometers. Part 1: Technical specifications. J Cataract Refract Surg 2005;31:1114-1127.
147. Molebny VV, Panagopoulou SI, Molebny SV, Wakil YS, Pallikaris IG. Principles of ray tracing aberrometry. J Refract Surg 2000;16:S572-575.
148. MacRae S, Fujieda M. Slit skiascopic-guided ablation using the Nidek laser. J Refract Surg 2000;16:S576-580.
149. Thibos LN. Principles of Hartmann-Shack aberrometry. J Refract Surg 2000;16:S563-565.
150. Mrochen M, Kaemmerer M, Mierdel P, Krinke HE, Seiler T. Principles of Tscherning aberrometry. J Refract Surg 2000;16:S570-571.
151. He JC, Burns SA, Marcos S. Monochromatic aberrations in the accommodated human eye. Vision Res 2000;40:41-48.
152. McLellan JS, Marcos S, Burns SA. Age-related changes in monochromatic wave aberrations of the human eye. Invest Ophthalmol Vis Sci 2001;42:1390-1395.
153. Seitz B, Behrens A, Langenbucher A. Corneal topography. Curr Opin Ophthalmol 1997;8:8-24.
154. Corneal topography. American Academy of Ophthalmology. Ophthalmology 1999;106:1628-1638.
155. Schlegel Z, Hoang-Xuan T, Gatinel D. Comparison of and correlation between anterior and posterior corneal elevation maps in normal eyes and keratoconus-suspect eyes. J Cataract Refract Surg 2008;34:789-795.
156. Lim L, Wei RH, Chan WK, Tan DT. Evaluation of keratoconus in Asians: role of Orbscan II and Tomey TMS-2 corneal topography. Am J Ophthalmol 2007;143:390-400.
157. Saad A, Gatinel D. Topographic and tomographic properties of forme fruste keratoconus corneas. Invest Ophthalmol Vis Sci 2010;51:5546-5555.
158. Oliveira CM, Ribeiro C, Franco S. Corneal imaging with slit-scanning and Scheimpflug imaging techniques. Clin Exp Optom 2011;94:33-42.
159. Drews RC. DEPTH OF FIELD IN SLIT LAMP PHOTOGRAPHY. AN OPTICAL SOLUTION USING THE SCHEIMPFLUG PRINCIPLE. Ophthalmologica 1964;148:143-150.
160. Hashemi H, Mehravaran S. Day to Day Clinically Relevant Corneal Elevation, Thickness, and Curvature Parameters Using the Orbscan II Scanning Slit Topographer and the Pentacam Scheimpflug Imaging Device. Middle East Afr J Ophthalmol 2010;17:44-55.

119
161. Stefano VS, Melo Junior LA, Mallmann F, Schor P. Interchangeability between Placido disc and Scheimpflug system: quantitative and qualitative analysis. Arq Bras Oftalmol 2010;73:363-366.
162. Oliveira CM, Ferreira A, Franco S. Wavefront analysis and Zernike polynomial decomposition for evaluation of corneal optical quality. J Cataract Refract Surg 2012;38:343-356.
163. Chen M, Yoon G. Posterior corneal aberrations and their compensation effects on anterior corneal aberrations in keratoconic eyes. Invest Ophthalmol Vis Sci 2008;49:5645-5652.
164. Pinero DP, Alio JL, Barraquer RI, Michael R, Jimenez R. Corneal biomechanics, refraction, and corneal aberrometry in keratoconus: an integrated study. Invest Ophthalmol Vis Sci 2010;51:1948-1955.
165. Pinero DP, Alio JL, Aleson A, Escaf M, Miranda M. Pentacam posterior and anterior corneal aberrations in normal and keratoconic eyes. Clin Exp Optom 2009;92:297-303.
166. Alio JL, Shabayek MH. Corneal higher order aberrations: a method to grade keratoconus. J Refract Surg 2006;22:539-545.
167. Gobbe M, Guillon M. Corneal wavefront aberration measurements to detect keratoconus patients. Cont Lens Anterior Eye 2005;28:57-66.
168. Barbero S, Marcos S, Merayo-Lloves J, Moreno-Barriuso E. Validation of the estimation of corneal aberrations from videokeratography in keratoconus. J Refract Surg 2002;18:263-270.
169. Buhren J, Kuhne C, Kohnen T. Defining subclinical keratoconus using corneal first-surface higher-order aberrations. Am J Ophthalmol 2007;143:381-389.
170. Rabinowitz YS. Keratoconus. Surv Ophthalmol 1998;42:297-319. 171. Wilson SE, Lin DT, Klyce SD. Corneal topography of keratoconus. Cornea
1991;10:2-8. 172. Demirbas NH, Pflugfelder SC. Topographic pattern and apex location of keratoconus
on elevation topography maps. Cornea 1998;17:476-484. 173. Sahin A, Yildirim N, Basmak H. Two-year interval changes in Orbscan II topography
in eyes with keratoconus. J Cataract Refract Surg 2008;34:1295-1299. 174. Kanellopoulos AJ, Asimellis G. Revisiting keratoconus diagnosis and progression
classification based on evaluation of corneal asymmetry indices, derived from Scheimpflug imaging in keratoconic and suspect cases. Clin Ophthalmol 2013;7:1539-1548.
175. Ambrosio R, Jr., Caiado AL, Guerra FP, et al. Novel pachymetric parameters based on corneal tomography for diagnosing keratoconus. J Refract Surg 2011;27:753-758.
176. Rao SN, Raviv T, Majmudar PA, Epstein RJ. Role of Orbscan II in screening keratoconus suspects before refractive corneal surgery. Ophthalmology 2002;109:1642-1646.
177. Ramos JL, Li Y, Huang D. Clinical and research applications of anterior segment optical coherence tomography - a review. Clin Experiment Ophthalmol 2009;37:81-89.
178. Doors M, Berendschot TT, de Brabander J, Webers CA, Nuijts RM. Value of optical coherence tomography for anterior segment surgery. J Cataract Refract Surg 2010;36:1213-1229.
179. Rosas Salaroli CH, Li Y, Zhang X, et al. Repeatability of laser in situ keratomileusis flap thickness measurement by Fourier-domain optical coherence tomography. J Cataract Refract Surg 2011;37:649-654.
120
180. Li Y, Meisler DM, Tang M, et al. Keratoconus diagnosis with optical coherence tomography pachymetry mapping. Ophthalmology 2008;115:2159-2166.
181. Mohamed S, Lee GK, Rao SK, et al. Repeatability and reproducibility of pachymetric mapping with Visante anterior segment-optical coherence tomography. Invest Ophthalmol Vis Sci 2007;48:5499-5504.
182. Kanellopoulos AJ, Asimellis G. OCT-derived comparison of corneal thickness distribution and asymmetry differences between normal and keratoconic eyes. Cornea 2014;33:1274-1281.
183. Nakagawa T, Maeda N, Higashiura R, Hori Y, Inoue T, Nishida K. Corneal topographic analysis in patients with keratoconus using 3-dimensional anterior segment optical coherence tomography. J Cataract Refract Surg 2011;37:1871-1878.
184. Aptel F, Chiquet C, Gimbert A, et al. Anterior segment biometry using spectral-domain optical coherence tomography. J Refract Surg 2014;30:354-360.
185. Nakakura S, Mori E, Nagatomi N, Tabuchi H, Kiuchi Y. Comparison of anterior chamber depth measurements by 3-dimensional optical coherence tomography, partial coherence interferometry biometry, Scheimpflug rotating camera imaging, and ultrasound biomicroscopy. J Cataract Refract Surg 2012;38:1207-1213.
186. Gora M, Karnowski K, Szkulmowski M, et al. Ultra high-speed swept source OCT imaging of the anterior segment of human eye at 200 kHz with adjustable imaging range. Opt Express 2009;17:14880-14894.
187. Khurana RN, Li Y, Tang M, Lai MM, Huang D. High-speed optical coherence tomography of corneal opacities. Ophthalmology 2007;114:1278-1285.
188. Boscia F, La Tegola MG, Alessio G, Sborgia C. Accuracy of Orbscan optical pachymetry in corneas with haze. J Cataract Refract Surg 2002;28:253-258.
189. Reinstein DZ, Archer TJ, Gobbe M. Rate of change of curvature of the corneal stromal surface drives epithelial compensatory changes and remodeling. J Refract Surg 2014;30:799-802.
190. Kanellopoulos AJ, Asimellis G. Longitudinal postoperative lasik epithelial thickness profile changes in correlation with degree of myopia correction. J Refract Surg 2014;30:166-171.
191. Reinstein DZ, Archer TJ, Gobbe M, Silverman RH, Coleman DJ. Epithelial thickness after hyperopic LASIK: three-dimensional display with Artemis very high-frequency digital ultrasound. J Refract Surg 2010;26:555-564.
192. Reinstein DZ, Gobbe M, Archer TJ, Couch D, Bloom B. Epithelial, stromal, and corneal pachymetry changes during orthokeratology. Optom Vis Sci 2009;86:E1006-1014.
193. Reinstein DZ, Archer TJ, Dickeson ZI, Gobbe M. Transepithelial phototherapeutic keratectomy protocol for treating irregular astigmatism based on population epithelial thickness measurements by artemis very high-frequency digital ultrasound. J Refract Surg 2014;30:380-387.
194. Zhou W, Stojanovic A. Comparison of corneal epithelial and stromal thickness distributions between eyes with keratoconus and healthy eyes with corneal astigmatism >/= 2.0 D. PLoS One 2014;9:e85994.
195. Kanellopoulos AJ, Asimellis G. OCT corneal epithelial topographic asymmetry as a sensitive diagnostic tool for early and advancing keratoconus. Clin Ophthalmol 2014;8:2277-2287.
196. Reinstein DZ, Archer TJ, Gobbe M. Corneal epithelial thickness profile in the diagnosis of keratoconus. J Refract Surg 2009;25:604-610.
121
197. Guthoff RF, Baudouin C, Stave J. Atlas of Confocal Laser Scanning In-vivo Microscopy in Ophthalmology- Principles and Applications in Diagnostic and Therapeutic Ophthalmology. Leipzig, Germany: Springer; 2006.
198. Kobayashi A, Sugiyama K. In vivo corneal confocal microscopic findings of palisades of Vogt and its underlying limbal stroma. Cornea 2005;24:435-437.
199. Kobayashi A, Yokogawa H, Sugiyama K. In vivo laser confocal microscopy of Bowman's layer of the cornea. Ophthalmology 2006;113:2203-2208.
200. Patel DV, Ku JY, Johnson R, McGhee CN. Laser scanning in vivo confocal microscopy and quantitative aesthesiometry reveal decreased corneal innervation and sensation in keratoconus. Eye (Lond) 2009;23:586-592.
201. Oliveira-Soto L, Efron N. Morphology of corneal nerves using confocal microscopy. Cornea 2001;20:374-384.
202. Klingler KN, McLaren JW, Bourne WM, Patel SV. Corneal endothelial cell changes 5 years after laser in situ keratomileusis: femtosecond laser versus mechanical microkeratome. J Cataract Refract Surg 2012;38:2125-2130.
203. Patel SV, Erie JC, McLaren JW, Bourne WM. Confocal microscopy changes in epithelial and stromal thickness up to 7 years after LASIK and photorefractive keratectomy for myopia. J Refract Surg 2007;23:385-392.
204. Ivarsen A, Fledelius W, Hjortdal JO. Three-year changes in epithelial and stromal thickness after PRK or LASIK for high myopia. Invest Ophthalmol Vis Sci 2009;50:2061-2066.
205. Kobayashi A, Sugiyama K, Huang AJ. In vivo confocal microscopy in patients with central cloudy dystrophy of Francois. Arch Ophthalmol 2004;122:1676-1679.
206. Patel S, McLaren J, Hodge D, Bourne W. Normal human keratocyte density and corneal thickness measurement by using confocal microscopy in vivo. Invest Ophthalmol Vis Sci 2001;42:333-339.
207. Sengor T, Kurna SA, Altun A, Irkec M, Aki SF, Aksoy S. Contact Lens-Related Acanthamoeba Keratitis and Accompanying Dacryoadenitis. Eye Contact Lens 2015.
208. Niederer RL, Perumal D, Sherwin T, McGhee CN. Laser scanning in vivo confocal microscopy reveals reduced innervation and reduction in cell density in all layers of the keratoconic cornea. Invest Ophthalmol Vis Sci 2008;49:2964-2970.
209. Kobayashi A, Yokogawa H, Yamazaki N, Masaki T, Sugiyama K. In vivo laser confocal microscopy after Descemet's membrane endothelial keratoplasty. Ophthalmology 2013;120:923-930.
210. Sindt CW, Grout TK, Critser DB, Kern JR, Meadows DL. Dendritic immune cell densities in the central cornea associated with soft contact lens types and lens care solution types: a pilot study. Clin Ophthalmol 2012;6:511-519.
211. Lum E, Golebiowski B, Swarbrick HA. Mapping the corneal sub-basal nerve plexus in orthokeratology lens wear using in vivo laser scanning confocal microscopy. Invest Ophthalmol Vis Sci 2012;53:1803-1809.
212. Dupps WJ, Jr., Wilson SE. Biomechanics and wound healing in the cornea. Exp Eye Res 2006;83:709-720.
213. Mohan RR, Mohan RR, Kim WJ, Wilson SE. Modulation of TNF-alpha-induced apoptosis in corneal fibroblasts by transcription factor NF-kappaB. Invest Ophthalmol Vis Sci 2000;41:1327-1336.
214. Tuominen IS, Tervo TM, Teppo AM, Valle TU, Gronhagen-Riska C, Vesaluoma MH. Human tear fluid PDGF-BB, TNF-alpha and TGF-beta1 vs corneal haze and regeneration of corneal epithelium and subbasal nerve plexus after PRK. Exp Eye Res 2001;72:631-641.

122
215. Wilson SE, Chen L, Mohan RR, Liang Q, Liu J. Expression of HGF, KGF, EGF and receptor messenger RNAs following corneal epithelial wounding. Exp Eye Res 1999;68:377-397.
216. Wilson SE, He YG, Weng J, et al. Epithelial injury induces keratocyte apoptosis: hypothesized role for the interleukin-1 system in the modulation of corneal tissue organization and wound healing. Exp Eye Res 1996;62:325-327.
217. Nunomura W, Takakuwa Y, Tokimitsu R, Krauss SW, Kawashima M, Mohandas N. Regulation of CD44-protein 4.1 interaction by Ca2+ and calmodulin. Implications for modulation of CD44-ankyrin interaction. J Biol Chem 1997;272:30322-30328.
218. Wilson SE, Li Q, Weng J, et al. The Fas-Fas ligand system and other modulators of apoptosis in the cornea. Invest Ophthalmol Vis Sci 1996;37:1582-1592.
219. Leonardi A, Tavolato M, Curnow SJ, Fregona IA, Violato D, Alio JL. Cytokine and chemokine levels in tears and in corneal fibroblast cultures before and after excimer laser treatment. J Cataract Refract Surg 2009;35:240-247.
220. Farah SG, Azar DT, Gurdal C, Wong J. Laser in situ keratomileusis: literature review of a developing technique. J Cataract Refract Surg 1998;24:989-1006.
221. Hersh PS, Brint SF, Maloney RK, et al. Photorefractive keratectomy versus laser in situ keratomileusis for moderate to high myopia. A randomized prospective study. Ophthalmology 1998;105:1512-1522, discussion 1522-1513.
222. McLaren JW, Bourne WM, Patel SV. Standardization of corneal haze measurement in confocal microscopy. Invest Ophthalmol Vis Sci 2010;51:5610-5616.
223. Moller-Pedersen T, Vogel M, Li HF, Petroll WM, Cavanagh HD, Jester JV. Quantification of stromal thinning, epithelial thickness, and corneal haze after photorefractive keratectomy using in vivo confocal microscopy. Ophthalmology 1997;104:360-368.
224. Marchini G, Mastropasqua L, Pedrotti E, Nubile M, Ciancaglini M, Sbabo A. Deep lamellar keratoplasty by intracorneal dissection: a prospective clinical and confocal microscopic study. Ophthalmology 2006;113:1289-1300.
225. Wei S, Wang Y. Comparison of corneal sensitivity between FS-LASIK and femtosecond lenticule extraction (ReLEx flex) or small-incision lenticule extraction (ReLEx smile) for myopic eyes. Graefes Arch Clin Exp Ophthalmol 2013;251:1645-1654.
226. Cruzat A, Pavan-Langston D, Hamrah P. In vivo confocal microscopy of corneal nerves: analysis and clinical correlation. Semin Ophthalmol 2010;25:171-177.
227. Lee SJ, Kim JK, Seo KY, Kim EK, Lee HK. Comparison of corneal nerve regeneration and sensitivity between LASIK and laser epithelial keratomileusis (LASEK). Am J Ophthalmol 2006;141:1009-1015.
228. Erie JC, McLaren JW, Hodge DO, Bourne WM. Recovery of corneal subbasal nerve density after PRK and LASIK. Am J Ophthalmol 2005;140:1059-1064.
229. Hillenaar T, Weenen C, Wubbels RJ, Remeijer L. Endothelial involvement in herpes simplex virus keratitis: an in vivo confocal microscopy study. Ophthalmology 2009;116:2077-2086 e2071-2072.
230. Kotecha A. What biomechanical properties of the cornea are relevant for the clinician? Surv Ophthalmol 2007;52 Suppl 2:S109-114.
231. Gatinel D, Chaabouni S, Adam PA, Munck J, Puech M, Hoang-Xuan T. Corneal hysteresis, resistance factor, topography, and pachymetry after corneal lamellar flap. J Refract Surg 2007;23:76-84.
232. Kopito R, Gaujoux T, Montard R, et al. Reproducibility of viscoelastic property and intraocular pressure measurements obtained with the Ocular Response Analyzer. Acta Ophthalmol 2011;89:e225-230.

123
233. Oncel B, Dinc UA, Gorgun E, Yalvac BI. Diurnal variation of corneal biomechanics and intraocular pressure in normal subjects. Eur J Ophthalmol 2009;19:798-803.
234. Lam AK, Chen D, Tse J. The usefulness of waveform score from the ocular response analyzer. Optom Vis Sci 2010;87:195-199.
235. Vestergaard AH, Grauslund J, Ivarsen AR, Hjortdal JO. Central corneal sublayer pachymetry and biomechanical properties after refractive femtosecond lenticule extraction. J Refract Surg 2014;30:102-108.
236. Touboul D, Roberts C, Kerautret J, et al. Correlations between corneal hysteresis, intraocular pressure, and corneal central pachymetry. J Cataract Refract Surg 2008;34:616-622.
237. Schweitzer C, Roberts CJ, Mahmoud AM, Colin J, Maurice-Tison S, Kerautret J. Screening of forme fruste keratoconus with the ocular response analyzer. Invest Ophthalmol Vis Sci 2010;51:2403-2410.
238. Kida T, Liu JH, Weinreb RN. Effects of aging on corneal biomechanical properties and their impact on 24-hour measurement of intraocular pressure. Am J Ophthalmol 2008;146:567-572.
239. Kamiya K, Shimizu K, Ohmoto F. Effect of aging on corneal biomechanical parameters using the ocular response analyzer. J Refract Surg 2009;25:888-893.
240. Strobbe E, Cellini M, Barbaresi U, Campos EC. Influence of age and gender on corneal biomechanical properties in a healthy Italian population. Cornea 2014;33:968-972.
241. Sullivan-Mee M, Katiyar S, Pensyl D, Halverson KD, Qualls C. Relative importance of factors affecting corneal hysteresis measurement. Optom Vis Sci 2012;89:E803-811.
242. Leite MT, Alencar LM, Gore C, et al. Comparison of corneal biomechanical properties between healthy blacks and whites using the Ocular Response Analyzer. Am J Ophthalmol 2010;150:163-168 e161.
243. Haseltine SJ, Pae J, Ehrlich JR, Shammas M, Radcliffe NM. Variation in corneal hysteresis and central corneal thickness among black, hispanic and white subjects. Acta Ophthalmol 2012;90:e626-631.
244. Kida T, Liu JH, Weinreb RN. Effect of 24-hour corneal biomechanical changes on intraocular pressure measurement. Invest Ophthalmol Vis Sci 2006;47:4422-4426.
245. Kotecha A, Crabb DP, Spratt A, Garway-Heath DF. The relationship between diurnal variations in intraocular pressure measurements and central corneal thickness and corneal hysteresis. Invest Ophthalmol Vis Sci 2009;50:4229-4236.
246. Shen M, Wang J, Qu J, et al. Diurnal variation of ocular hysteresis, corneal thickness, and intraocular pressure. Optom Vis Sci 2008;85:1185-1192.
247. Abitbol O, Bouden J, Doan S, Hoang-Xuan T, Gatinel D. Corneal hysteresis measured with the Ocular Response Analyzer in normal and glaucomatous eyes. Acta Ophthalmol 2010;88:116-119.
248. Hager A, Wegscheider K, Wiegand W. Changes of extracellular matrix of the cornea in diabetes mellitus. Graefes Arch Clin Exp Ophthalmol 2009;247:1369-1374.
249. Goldich Y, Barkana Y, Gerber Y, et al. Effect of diabetes mellitus on biomechanical parameters of the cornea. J Cataract Refract Surg 2009;35:715-719.
250. Castro DP, Prata TS, Lima VC, Biteli LG, de Moraes CG, Paranhos A, Jr. Corneal viscoelasticity differences between diabetic and nondiabetic glaucomatous patients. J Glaucoma 2010;19:341-343.
251. Kotecha A, Oddone F, Sinapis C, et al. Corneal biomechanical characteristics in patients with diabetes mellitus. J Cataract Refract Surg 2010;36:1822-1828.

124
252. Sahin A, Bayer A, Ozge G, Mumcuoglu T. Corneal biomechanical changes in diabetes mellitus and their influence on intraocular pressure measurements. Invest Ophthalmol Vis Sci 2009;50:4597-4604.
253. Perez-Rico C, Gutierrez-Ortiz C, Gonzalez-Mesa A, Zandueta AM, Moreno-Salgueiro A, Germain F. Effect of diabetes mellitus on Corvis ST measurement process. Acta Ophthalmol 2014.
254. Wong YZ, Lam AK. The Roles of Cornea and Axial Length in Corneal Hysteresis among Emmetropes and High Myopes: A Pilot Study. Curr Eye Res 2014;1-8.
255. Altan C, Demirel B, Azman E, et al. Biomechanical properties of axially myopic cornea. Eur J Ophthalmol 2012;22 Suppl 7:S24-28.
256. Plakitsi A, O'Donnell C, Miranda MA, Charman WN, Radhakrishnan H. Corneal biomechanical properties measured with the Ocular Response Analyser in a myopic population. Ophthalmic Physiol Opt 2011;31:404-412.
257. Shen M, Fan F, Xue A, Wang J, Zhou X, Lu F. Biomechanical properties of the cornea in high myopia. Vision Res 2008;48:2167-2171.
258. Lim L, Cheung N, Gazzard G, Chan YH, Wong TY, Saw SM. Corneal biomechanical properties and retinal vascular caliber in children. Invest Ophthalmol Vis Sci 2009;50:121-125.
259. Bueno-Gimeno I, Espana-Gregori E, Gene-Sampedro A, Lanzagorta-Aresti A, Pinero-Llorens DP. Relationship among corneal biomechanics, refractive error, and axial length. Optom Vis Sci 2014;91:507-513.
260. Kamiya K, Hagishima M, Fujimura F, Shimizu K. Factors affecting corneal hysteresis in normal eyes. Graefes Arch Clin Exp Ophthalmol 2008;246:1491-1494.
261. Mikielewicz M, Kotliar K, Barraquer RI, Michael R. Air-pulse corneal applanation signal curve parameters for the characterisation of keratoconus. Br J Ophthalmol 2011;95:793-798.
262. Saad A, Lteif Y, Azan E, Gatinel D. Biomechanical properties of keratoconus suspect eyes. Invest Ophthalmol Vis Sci 2010;51:2912-2916.
263. Fontes BM, Ambrosio R, Jr., Velarde GC, Nose W. Ocular response analyzer measurements in keratoconus with normal central corneal thickness compared with matched normal control eyes. J Refract Surg 2011;27:209-215.
264. Shah S, Laiquzzaman M. Comparison of corneal biomechanics in pre and post-refractive surgery and keratoconic eyes by Ocular Response Analyser. Cont Lens Anterior Eye 2009;32:129-132; quiz 151.
265. Kirwan C, O'Keefe M. Corneal hysteresis using the Reichert ocular response analyser: findings pre- and post-LASIK and LASEK. Acta Ophthalmol 2008;86:215-218.
266. Ortiz D, Pinero D, Shabayek MH, Arnalich-Montiel F, Alio JL. Corneal biomechanical properties in normal, post-laser in situ keratomileusis, and keratoconic eyes. J Cataract Refract Surg 2007;33:1371-1375.
267. Pepose JS, Feigenbaum SK, Qazi MA, Sanderson JP, Roberts CJ. Changes in corneal biomechanics and intraocular pressure following LASIK using static, dynamic, and noncontact tonometry. Am J Ophthalmol 2007;143:39-47.
268. Zarei-Ghanavati S, Ramirez-Miranda A, Yu F, Hamilton DR. Corneal deformation signal waveform analysis in keratoconic versus post-femtosecond laser in situ keratomileusis eyes after statistical correction for potentially confounding factors. J Cataract Refract Surg 2012;38:607-614.
269. Terai N, Raiskup F, Haustein M, Pillunat LE, Spoerl E. Identification of biomechanical properties of the cornea: the ocular response analyzer. Curr Eye Res 2012;37:553-562.

125
270. Kerautret J, Colin J, Touboul D, Roberts C. Biomechanical characteristics of the ectatic cornea. J Cataract Refract Surg 2008;34:510-513.
271. Hallahan KM, Sinha Roy A, Ambrosio R, Jr., Salomao M, Dupps WJ, Jr. Discriminant value of custom ocular response analyzer waveform derivatives in keratoconus. Ophthalmology 2014;121:459-468.
272. Greenstein SA, Fry KL, Hersh PS. In vivo biomechanical changes after corneal collagen cross-linking for keratoconus and corneal ectasia: 1-year analysis of a randomized, controlled, clinical trial. Cornea 2012;31:21-25.
273. Goldich Y, Marcovich AL, Barkana Y, et al. Clinical and corneal biomechanical changes after collagen cross-linking with riboflavin and UV irradiation in patients with progressive keratoconus: results after 2 years of follow-up. Cornea 2012;31:609-614.
274. Spoerl E, Terai N, Scholz F, Raiskup F, Pillunat LE. Detection of biomechanical changes after corneal cross-linking using Ocular Response Analyzer software. J Refract Surg 2011;27:452-457.
275. Hon Y, Lam AK. Corneal deformation measurement using Scheimpflug noncontact tonometry. Optom Vis Sci 2013;90:e1-8.
276. Ali NQ, Patel DV, McGhee CN. Biomechanical responses of healthy and keratoconic corneas measured using a non contact Scheimpflug tonometer. Investigative Ophthalmology and Visual Science 2014.
277. Chen X, Stojanovic A, Hua Y, et al. Reliability of corneal dynamic scheimpflug analyser measurements in virgin and post-PRK eyes. PLoS One 2014;9:e109577.
278. Hong J, Xu J, Wei A, et al. A New Tonometer--The Corvis ST Tonometer: Clinical Comparison with Noncontact and Goldmann Applanation Tonometers. Investigative Ophthalmology and Visual Science 2013;54:659-665.
279. Lanza M, Iaccarino S, Cennamo M, Irregolare C, Romano V, Carnevale UA. Comparison between Corvis and other tonometers in healthy eyes. Cont Lens Anterior Eye 2014.
280. Bak-Nielsen S, Pedersen IB, Ivarsen A, Hjortdal J. Repeatability, reproducibility, and age dependency of dynamic Scheimpflug-based pneumotonometer and its correlation with a dynamic bidirectional pneumotonometry device. Cornea 2015;34:71-77.
281. Kling S, Marcos S. Contributing factors to corneal deformation in air puff measurements. Invest Ophthalmol Vis Sci 2013;54:5078-5085.
282. Nemeth G, Hassan Z, Csutak A, Szalai E, Berta A, Modis L, Jr. Repeatability of ocular biomechanical data measurements with a Scheimpflug-based noncontact device on normal corneas. J Refract Surg 2013;29:558-563.
283. Valbon BF, Ambrosio R, Jr., Fontes BM, Alves MR. Effects of age on corneal deformation by non-contact tonometry integrated with an ultra-high-speed (UHS) Scheimpflug camera. Arq Bras Oftalmol 2013;76:229-232.
284. Leung CK, Ye C, Weinreb RN. An ultra-high-speed Scheimpflug camera for evaluation of corneal deformation response and its impact on IOP measurement. Investigative Ophthalmology and Visual Science 2013;54:2885-2892.
285. Hassan Z, Modis L, Jr., Szalai E, Berta A, Nemeth G. Examination of ocular biomechanics with a new Scheimpflug technology after corneal refractive surgery. Cont Lens Anterior Eye 2014;37:337-341.
286. Shen Y, Zhao J, Yao P, et al. Changes in corneal deformation parameters after lenticule creation and extraction during small incision lenticule extraction (SMILE) procedure. PLoS One 2014;9:e103893.

126
287. Mastropasqua L, Calienno R, Lanzini M, et al. Evaluation of corneal biomechanical properties modification after small incision lenticule extraction using Scheimpflug-based noncontact tonometer. Biomed Res Int 2014;2014:290619.
288. Shen Y, Chen Z, Knorz MC, Li M, Zhao J, Zhou X. Comparison of Corneal Deformation Parameters After SMILE, LASEK, and Femtosecond Laser-Assisted LASIK. J Refract Surg 2014;30:310-318.
289. Bak-Nielsen S, Pedersen IB, Ivarsen A, Hjortdal J. Dynamic Scheimpflug-based assessment of keratoconus and the effects of corneal cross-linking. J Refract Surg 2014;30:408-414.
290. Lanza M, Cennamo M, Iaccarino S, et al. Evaluation of corneal deformation analyzed with Scheimpflug based device in healthy eyes and diseased ones. Biomed Res Int 2014;2014:748671.
291. Tian L, Ko MW, Wang LK, et al. Assessment of ocular biomechanics using dynamic ultra high-speed Scheimpflug imaging in keratoconic and normal eyes. J Refract Surg 2014;30:785-791.
292. Kling S, Marcos S. Contributing factors to corneal deformation in air puff measurements. Investigative Ophthalmology and Visual Science 2013;54:5078-5085.
293. Metzler KM, Mahmoud AM, Liu J, Roberts CJ. Deformation response of paired donor corneas to an air puff: intact whole globe versus mounted corneoscleral rim. Journal of Cataract and Refractive Surgery 2014;40:888-896.
294. Dorronsoro C, Pascual D, Perez-Merino P, Kling S, Marcos S. Dynamic OCT measurement of corneal deformation by an air puff in normal and cross-linked corneas. Biomed Opt Express 2012;3:473-487.
295. Nahas A, Bauer M, Roux S, Boccara AC. 3D static elastography at the micrometer scale using Full Field OCT. Biomed Opt Express 2013;4:2138-2149.
296. Wang S, Larin KV. Noncontact depth-resolved micro-scale optical coherence elastography of the cornea. Biomed Opt Express 2014;5:3807-3821.
297. Scarcelli G, Pineda R, Yun SH. Brillouin optical microscopy for corneal biomechanics. Invest Ophthalmol Vis Sci 2012;53:185-190.
298. Scarcelli G, Yun SH. Confocal Brillouin microscopy for three-dimensional mechanical imaging. Nat Photonics 2007;2:39-43.
299. Scarcelli G, Kim P, Yun SH. In vivo measurement of age-related stiffening in the crystalline lens by Brillouin optical microscopy. Biophys J 2011;101:1539-1545.
300. Scarcelli G, Yun SH. In vivo Brillouin optical microscopy of the human eye. Opt Express 2012;20:9197-9202.
301. Li X, Rabinowitz YS, Rasheed K, Yang H. Longitudinal study of the normal eyes in unilateral keratoconus patients. Ophthalmology 2004;111:440-446.
302. Klyce SD. Chasing the suspect: keratoconus. Br J Ophthalmol 2009;93:845-847. 303. Kennedy RH, Bourne WM, Dyer JA. A 48-year clinical and epidemiologic study of
keratoconus. Am J Ophthalmol 1986;101:267-273. 304. Pearson AR, Soneji B, Sarvananthan N, Sandford-Smith JH. Does ethnic origin
influence the incidence or severity of keratoconus? Eye (Lond) 2000;14 ( Pt 4):625-628.
305. Nielsen K, Hjortdal J, Aagaard Nohr E, Ehlers N. Incidence and prevalence of keratoconus in Denmark. Acta Ophthalmol Scand 2007;85:890-892.
306. Georgiou T, Funnell CL, Cassels-Brown A, O'Conor R. Influence of ethnic origin on the incidence of keratoconus and associated atopic disease in Asians and white patients. Eye (Lond) 2004;18:379-383.
307. Rahi A, Davies P, Ruben M, Lobascher D, Menon J. Keratoconus and coexisting atopic disease. Br J Ophthalmol 1977;61:761-764.

127
308. Totan Y, Hepsen IF, Cekic O, Gunduz A, Aydin E. Incidence of keratoconus in subjects with vernal keratoconjunctivitis: a videokeratographic study. Ophthalmology 2001;108:824-827.
309. Balasubramanian SA, Pye DC, Willcox MD. Effects of eye rubbing on the levels of protease, protease activity and cytokines in tears: relevance in keratoconus. Clin Exp Optom 2013;96:214-218.
310. Culbertson WW, Tseng SC. Corneal disorders in floppy eyelid syndrome. Cornea 1994;13:33-42.
311. Shapiro MB, France TD. The ocular features of Down's syndrome. Am J Ophthalmol 1985;99:659-663.
312. Robertson I. Keratoconus and the Ehlers-Danlos syndrome: a new aspect of keratoconus. Med J Aust 1975;1:571-573.
313. Woodward EG, Morris MT. Joint hypermobility in keratoconus. Ophthalmic Physiol Opt 1990;10:360-362.
314. Abu-Amero KK, Al-Muammar AM, Kondkar AA. Genetics of keratoconus: where do we stand? J Ophthalmol 2014;2014:641708.
315. Gomes JA, Tan D, Rapuano CJ, et al. Global consensus on keratoconus and ectatic diseases. Cornea 2015;34:359-369.
316. Chan CC, Squissato V. Keratoconus and crosslinking: pharmacokinetic considerations. Expert Opin Drug Metab Toxicol 2013;9:1613-1624.
317. Collier SA, Madigan MC, Penfold PL. Expression of membrane-type 1 matrix metalloproteinase (MT1-MMP) and MMP-2 in normal and keratoconus corneas. Curr Eye Res 2000;21:662-668.
318. Lema I, Duran JA. Inflammatory molecules in the tears of patients with keratoconus. Ophthalmology 2005;112:654-659.
319. Mackiewicz Z, Maatta M, Stenman M, Konttinen L, Tervo T, Konttinen YT. Collagenolytic proteinases in keratoconus. Cornea 2006;25:603-610.
320. Zhou L, Sawaguchi S, Twining SS, Sugar J, Feder RS, Yue BY. Expression of degradative enzymes and protease inhibitors in corneas with keratoconus. Invest Ophthalmol Vis Sci 1998;39:1117-1124.
321. Jun AS, Cope L, Speck C, et al. Subnormal cytokine profile in the tear fluid of keratoconus patients. PLoS One 2011;6:e16437.
322. Kim WJ, Rabinowitz YS, Meisler DM, Wilson SE. Keratocyte apoptosis associated with keratoconus. Exp Eye Res 1999;69:475-481.
323. Critchfield JW, Calandra AJ, Nesburn AB, Kenney MC. Keratoconus: I. Biochemical studies. Exp Eye Res 1988;46:953-963.
324. Yue BY, Sugar J, Benveniste K. Heterogeneity in keratoconus: possible biochemical basis. Proc Soc Exp Biol Med 1984;175:336-341.
325. Kao WW, Vergnes JP, Ebert J, Sundar-Raj CV, Brown SI. Increased collagenase and gelatinase activities in keratoconus. Biochem Biophys Res Commun 1982;107:929-936.
326. Andreassen TT, Simonsen AH, Oxlund H. Biomechanical properties of keratoconus and normal corneas. Exp Eye Res 1980;31:435-441.
327. Nash IS, Greene PR, Foster CS. Comparison of mechanical properties of keratoconus and normal corneas. Exp Eye Res 1982;35:413-424.
328. Edmund C. Corneal elasticity and ocular rigidity in normal and keratoconic eyes. Acta Ophthalmol (Copenh) 1988;66:134-140.
329. Krumeich JH, Daniel J. [Live epikeratophakia and deep lamellar keratoplasty for I-III stage-specific surgical treatment of keratoconus]. Klin Monbl Augenheilkd 1997;211:94-100.
128
330. Trokel SL, Srinivasan R, Braren B. Excimer laser surgery of the cornea. Am J Ophthalmol 1983;96:710-715.
331. Marshall J, Sliney DH. Endoexcimer laser intraocular ablative photodecomposition. Am J Ophthalmol 1986;101:130-131.
332. Shah S, Sheppard AL, Castle J, et al. Refractive outcomes of laser-assisted subepithelial keratectomy for myopia, hyperopia, and astigmatism using a 213 nm wavelength solid-state laser. J Cataract Refract Surg 2012;38:746-751.
333. Tsiklis NS, Kymionis GD, Kounis GA, Naoumidi, II, Pallikaris IG. Photorefractive keratectomy using solid state laser 213 nm and excimer laser 193 nm: a randomized, contralateral, comparative, experimental study. Invest Ophthalmol Vis Sci 2008;49:1415-1420.
334. Marshall J, Trokel SL, Rothery S, Krueger RR. Long-term healing of the central cornea after photorefractive keratectomy using an excimer laser. Ophthalmology 1988;95:1411-1421.
335. Munnerlyn CR, Koons SJ, Marshall J. Photorefractive keratectomy: a technique for laser refractive surgery. J Cataract Refract Surg 1988;14:46-52.
336. Seiler T, Bende T, Wollensak J, Trokel S. Excimer laser keratectomy for correction of astigmatism. Am J Ophthalmol 1988;105:117-124.
337. Alio JL, Muftuoglu O, Ortiz D, et al. Ten-year follow-up of photorefractive keratectomy for myopia of less than -6 diopters. Am J Ophthalmol 2008;145:29-36.
338. Rajan MS, O'Brart D, Jaycock P, Marshall J. Effects of ablation diameter on long-term refractive stability and corneal transparency after photorefractive keratectomy. Ophthalmology 2006;113:1798-1806.
339. Shalchi Z, O'Brart DP, McDonald RJ, Patel P, Archer TJ, Marshall J. Eighteen-year follow-up of excimer laser photorefractive keratectomy. J Cataract Refract Surg 2015;41:23-32.
340. de Benito-Llopis L, Alio JL, Ortiz D, Teus MA, Artola A. Ten-year follow-up of excimer laser surface ablation for myopia in thin corneas. Am J Ophthalmol 2009;147:768-773, 773.e761-762.
341. Ehlers N, Hjortdal JO. Excimer laser refractive keratectomy for high myopia. 6-month follow-up of patients treated bilaterally. Acta Ophthalmol (Copenh) 1992;70:578-586.
342. Gartry DS, Kerr Muir MG, Marshall J. Excimer laser photorefractive keratectomy. 18-month follow-up. Ophthalmology 1992;99:1209-1219.
343. Mohan RR, Hutcheon AE, Choi R, et al. Apoptosis, necrosis, proliferation, and myofibroblast generation in the stroma following LASIK and PRK. Exp Eye Res 2003;76:71-87.
344. Wilson SE, Mohan RR, Mohan RR, Ambrosio R, Jr., Hong J, Lee J. The corneal wound healing response: cytokine-mediated interaction of the epithelium, stroma, and inflammatory cells. Prog Retin Eye Res 2001;20:625-637.
345. McAlinden C, Skiadaresi E, Moore JE. Visual and refractive outcomes following myopic laser-assisted subepithelial keratectomy with a flying-spot excimer laser. J Cataract Refract Surg 2011;37:901-906.
346. Netto MV, Mohan RR, Sinha S, Sharma A, Dupps W, Wilson SE. Stromal haze, myofibroblasts, and surface irregularity after PRK. Exp Eye Res 2006;82:788-797.
347. Hashemi H, Taheri SM, Fotouhi A, Kheiltash A. Evaluation of the prophylactic use of mitomycin-C to inhibit haze formation after photorefractive keratectomy in high myopia: a prospective clinical study. BMC Ophthalmol 2004;4:12.
348. Rajan MS, O'Brart DP, Patmore A, Marshall J. Cellular effects of mitomycin-C on human corneas after photorefractive keratectomy. J Cataract Refract Surg 2006;32:1741-1747.

129
349. Faktorovich EG, Melwani K. Efficacy and safety of pain relief medications after photorefractive keratectomy: review of prospective randomized trials. J Cataract Refract Surg 2014;40:1716-1730.
350. Cherry PM, Tutton MK, Adhikary H, et al. The treatment of pain following photorefractive keratectomy. J Refract Corneal Surg 1994;10:S222-225.
351. Stramer BM, Zieske JD, Jung JC, Austin JS, Fini ME. Molecular mechanisms controlling the fibrotic repair phenotype in cornea: implications for surgical outcomes. Invest Ophthalmol Vis Sci 2003;44:4237-4246.
352. Taneri S, Zieske JD, Azar DT. Evolution, techniques, clinical outcomes, and pathophysiology of LASEK: review of the literature. Surv Ophthalmol 2004;49:576-602.
353. Herrmann WA, Hillenkamp J, Hufendiek K, et al. Epi-laser in situ keratomileusis: comparative evaluation of epithelial separation with 3 microkeratomes. J Cataract Refract Surg 2008;34:1761-1766.
354. Sia RK, Ryan DS, Edwards JD, Stutzman RD, Bower KS. The U.S. Army Surface Ablation Study: comparison of PRK, MMC-PRK, and LASEK in moderate to high myopia. J Refract Surg 2014;30:256-264.
355. Diakonis VF, Kankariya VP, Kounis G, et al. Contralateral-eye study of surface refractive treatments: clinical and confocal microscopy evaluation. J Cataract Refract Surg 2014;40:224-231.
356. Reynolds A, Moore JE, Naroo SA, Moore CB, Shah S. Excimer laser surface ablation - a review. Clin Experiment Ophthalmol 2010;38:168-182.
357. Korkmaz S, Bilgihan K, Sul S, Hondur A. A Clinical and Confocal Microscopic Comparison of Transepithelial PRK and LASEK for Myopia. J Ophthalmol 2014;2014:784185.
358. Celik U, Bozkurt E, Celik B, Demirok A, Yilmaz OF. Pain, wound healing and refractive comparison of mechanical and transepithelial debridement in photorefractive keratectomy for myopia: results of 1 year follow-up. Cont Lens Anterior Eye 2014;37:420-426.
359. Aslanides IM, Padroni S, Arba Mosquera S, Ioannides A, Mukherjee A. Comparison of single-step reverse transepithelial all-surface laser ablation (ASLA) to alcohol-assisted photorefractive keratectomy. Clin Ophthalmol 2012;6:973-980.
360. Pallikaris IG, Papatzanaki ME, Stathi EZ, Frenschock O, Georgiadis A. Laser in situ keratomileusis. Lasers Surg Med 1990;10:463-468.
361. Pallikaris IG, Papatzanaki ME, Siganos DS, Tsilimbaris MK. A corneal flap technique for laser in situ keratomileusis. Human studies. Arch Ophthalmol 1991;109:1699-1702.
362. Duffey RJ, Leaming D. U.S. trends in refractive surgery: 2001 International Society of Refractive Surgery Survey. J Refract Surg 2002;18:185-188.
363. Pallikaris IG, Siganos DS. Laser in situ keratomileusis to treat myopia: early experience. J Cataract Refract Surg 1997;23:39-49.
364. Pop M, Payette Y. Photorefractive keratectomy versus laser in situ keratomileusis: a control-matched study. Ophthalmology 2000;107:251-257.
365. Smadja D, Santhiago MR, Tellouck J, et al. Safety and efficacy of wavefront-guided myopic laser in situ keratomileusis using a new wavefront sensor technology: first 100 cases. J Cataract Refract Surg 2015;41:1588-1593.
366. Schallhorn SC, Venter JA, Hannan SJ, Hettinger KA. Outcomes of wavefront-guided laser in situ keratomileusis using a new-generation Hartmann-Shack aberrometer in patients with high myopia. J Cataract Refract Surg 2015;41:1810-1819.

130
367. Santos AM, Torricelli AA, Marino GK, et al. Femtosecond Laser-Assisted LASIK Flap Complications. J Refract Surg 2016;32:52-59.
368. Sarayba MA, Ignacio TS, Binder PS, Tran DB. Comparative study of stromal bed quality by using mechanical, IntraLase femtosecond laser 15- and 30-kHz microkeratomes. Cornea 2007;26:446-451.
369. Wang Y, Li J, Liu Y, Xie L. Intraocular straylight after thin-flap LASIK with a femtosecond laser versus a mechanical microkeratome. J Refract Surg 2013;29:534-539.
370. Lapid-Gortzak R, van der Meulen I, van der Linden JW, Nieuwendaal C, Mourits M, van den Berg T. Straylight measurements before and after removal of epithelial ingrowth. J Cataract Refract Surg 2009;35:1829-1832.
371. JK IJ, de Waard PW, van den Berg TJ, de Jong PT. The intraocular straylight function in 129 healthy volunteers; dependence on angle, age and pigmentation. Vision Res 1990;30:699-707.
372. Shaikh NM, Wee CE, Kaufman SC. The safety and efficacy of photorefractive keratectomy after laser in situ keratomileusis. J Refract Surg 2005;21:353-358.
373. Utz VM, Krueger RR. Management of irregular astigmatism following rotationally disoriented free cap after LASIK. J Refract Surg 2008;24:383-391.
374. Weisenthal RW, Salz J, Sugar A, et al. Photorefractive keratectomy for treatment of flap complications in laser in situ keratomileusis. Cornea 2003;22:399-404.
375. Abdulaal MR, Wehbe HA, Awwad ST. One-step transepithelial photorefractive keratectomy with mitomycin C as an early treatment for LASIK flap buttonhole formation. J Refract Surg 2015;31:48-52.
376. Chen X, Stojanovic A, Nitter TA. Topography-guided transepithelial surface ablation in treatment of recurrent epithelial ingrowths. J Refract Surg 2010;26:529-532.
377. Rush SW, Han DY, Rush RB. Optical coherence tomography-guided transepithelial phototherapeutic keratectomy for the treatment of anterior corneal scarring. Am J Ophthalmol 2013;156:1088-1094.
378. Soong HK, Malta JB. Femtosecond lasers in ophthalmology. Am J Ophthalmol 2009;147:189-197 e182.
379. Sekundo W, Kunert K, Russmann C, et al. First efficacy and safety study of femtosecond lenticule extraction for the correction of myopia: six-month results. J Cataract Refract Surg 2008;34:1513-1520.
380. Ang M, Mehta JS, Chan C, Htoon HM, Koh JC, Tan DT. Refractive lenticule extraction: transition and comparison of 3 surgical techniques. J Cataract Refract Surg 2014;40:1415-1424.
381. Gertnere J, Solomatin I, Sekundo W. Refractive lenticule extraction (ReLEx flex) and wavefront-optimized Femto-LASIK: comparison of contrast sensitivity and high-order aberrations at 1 year. Graefes Arch Clin Exp Ophthalmol 2013;251:1437-1442.
382. Kamiya K, Shimizu K, Igarashi A, Kobashi H, Komatsu M. Comparison of visual acuity, higher-order aberrations and corneal asphericity after refractive lenticule extraction and wavefront-guided laser-assisted in situ keratomileusis for myopia. Br J Ophthalmol 2013;97:968-975.
383. Vestergaard A, Ivarsen A, Asp S, Hjortdal JO. Femtosecond (FS) laser vision correction procedure for moderate to high myopia: a prospective study of ReLEx((R)) flex and comparison with a retrospective study of FS-laser in situ keratomileusis. Acta Ophthalmol 2013;91:355-362.
384. Vestergaard AH, Gronbech KT, Grauslund J, Ivarsen AR, Hjortdal JO. Subbasal nerve morphology, corneal sensation, and tear film evaluation after refractive femtosecond laser lenticule extraction. Graefes Arch Clin Exp Ophthalmol 2013;251:2591-2600.

131
385. Reinstein DZ, Archer TJ, Gobbe M, Johnson N. Accuracy and reproducibility of artemis central flap thickness and visual outcomes of LASIK with the Carl Zeiss Meditec VisuMax femtosecond laser and MEL 80 excimer laser platforms. J Refract Surg 2010;26:107-119.
386. Tay E, Li X, Chan C, Tan DT, Mehta JS. Refractive lenticule extraction flap and stromal bed morphology assessment with anterior segment optical coherence tomography. J Cataract Refract Surg 2012;38:1544-1551.
387. Lim DH, Keum JE, Ju WK, Lee JH, Chung TY, Chung ES. Prospective contralateral eye study to compare 80- and 120-mum flap LASIK using the VisuMax femtosecond laser. J Refract Surg 2013;29:462-468.
388. Kunert KS, Blum M, Duncker GI, Sietmann R, Heichel J. Surface quality of human corneal lenticules after femtosecond laser surgery for myopia comparing different laser parameters. Graefes Arch Clin Exp Ophthalmol 2011;249:1417-1424.
389. Riau AK, Angunawela RI, Chaurasia SS, Tan DT, Mehta JS. Effect of different femtosecond laser-firing patterns on collagen disruption during refractive lenticule extraction. J Cataract Refract Surg 2012;38:1467-1475.
390. Shah R, Shah S. Effect of scanning patterns on the results of femtosecond laser lenticule extraction refractive surgery. J Cataract Refract Surg 2011;37:1636-1647.
391. Hjortdal JO, Vestergaard AH, Ivarsen A, Ragunathan S, Asp S. Predictors for the outcome of small-incision lenticule extraction for Myopia. J Refract Surg 2012;28:865-871.
392. Sekundo W, Kunert KS, Blum M. Small incision corneal refractive surgery using the small incision lenticule extraction (SMILE) procedure for the correction of myopia and myopic astigmatism: results of a 6 month prospective study. Br J Ophthalmol 2011;95:335-339.
393. Kim WS, Jo JM. Corneal hydration affects ablation during laser in situ keratomileusis surgery. Cornea 2001;20:394-397.
394. Patel S, Alio JL, Artola A. Changes in the refractive index of the human corneal stroma during laser in situ keratomileusis. Effects of exposure time and method used to create the flap. J Cataract Refract Surg 2008;34:1077-1082.
395. Patel S, Alio JL, Perez-Santonja JJ. Refractive index change in bovine and human corneal stroma before and after lasik: a study of untreated and re-treated corneas implicating stromal hydration. Invest Ophthalmol Vis Sci 2004;45:3523-3530.
396. Agca A, Demirok A, Cankaya KI, et al. Comparison of visual acuity and higher-order aberrations after femtosecond lenticule extraction and small-incision lenticule extraction. Cont Lens Anterior Eye 2014;37:292-296.
397. Ganesh S, Gupta R. Comparison of visual and refractive outcomes following femtosecond laser- assisted lasik with smile in patients with myopia or myopic astigmatism. J Refract Surg 2014;30:590-596.
398. Lin F, Xu Y, Yang Y. Comparison of the visual results after SMILE and femtosecond laser-assisted LASIK for myopia. J Refract Surg 2014;30:248-254.
399. Agca A, Ozgurhan EB, Yildirim Y, et al. Corneal backscatter analysis by in vivo confocal microscopy: fellow eye comparison of small incision lenticule extraction and femtosecond laser-assisted LASIK. J Ophthalmol 2014;2014:265012.
400. Li M, Zhao J, Miao H, et al. Mild decentration measured by a Scheimpflug camera and its impact on visual quality following SMILE in the early learning curve. Invest Ophthalmol Vis Sci 2014;55:3886-3892.
401. Lazaridis A, Droutsas K, Sekundo W. Topographic analysis of the centration of the treatment zone after SMILE for myopia and comparison to FS-LASIK: subjective versus objective alignment. J Refract Surg 2014;30:680-686.

132
402. Ivarsen A, Hjortdal J. Correction of myopic astigmatism with small incision lenticule extraction. J Refract Surg 2014;30:240-247.
403. Kohlhaas M, Spoerl E, Schilde T, Unger G, Wittig C, Pillunat LE. Biomechanical evidence of the distribution of cross-links in corneas treated with riboflavin and ultraviolet A light. J Cataract Refract Surg 2006;32:279-283.
404. Sinha Roy A, Dupps WJ, Jr., Roberts CJ. Comparison of biomechanical effects of small-incision lenticule extraction and laser in situ keratomileusis: finite-element analysis. J Cataract Refract Surg 2014;40:971-980.
405. Reinstein DZ, Archer TJ, Randleman JB. Mathematical model to compare the relative tensile strength of the cornea after PRK, LASIK, and small incision lenticule extraction. J Refract Surg 2013;29:454-460.
406. Agca A, Ozgurhan EB, Demirok A, et al. Comparison of corneal hysteresis and corneal resistance factor after small incision lenticule extraction and femtosecond laser-assisted LASIK: a prospective fellow eye study. Cont Lens Anterior Eye 2014;37:77-80.
407. Kamiya K, Shimizu K, Igarashi A, Kobashi H, Sato N, Ishii R. Intraindividual comparison of changes in corneal biomechanical parameters after femtosecond lenticule extraction and small-incision lenticule extraction. J Cataract Refract Surg 2014;40:963-970.
408. Wang D, Liu M, Chen Y, et al. Differences in the corneal biomechanical changes after SMILE and LASIK. J Refract Surg 2014;30:702-707.
409. Wu D, Wang Y, Zhang L, Wei S, Tang X. Corneal biomechanical effects: small-incision lenticule extraction versus femtosecond laser-assisted laser in situ keratomileusis. J Cataract Refract Surg 2014;40:954-962.
410. Shtein RM. Post-LASIK dry eye. Expert Rev Ophthalmol 2011;6:575-582. 411. Calvillo MP, McLaren JW, Hodge DO, Bourne WM. Corneal reinnervation after
LASIK: prospective 3-year longitudinal study. Invest Ophthalmol Vis Sci 2004;45:3991-3996.
412. Mohamed-Noriega K, Riau AK, Lwin NC, Chaurasia SS, Tan DT, Mehta JS. Early corneal nerve damage and recovery following small incision lenticule extraction (SMILE) and laser in situ keratomileusis (LASIK). Invest Ophthalmol Vis Sci 2014;55:1823-1834.
413. Denoyer A, Landman E, Trinh L, Faure JF, Auclin F, Baudouin C. Dry Eye Disease after Refractive Surgery: Comparative Outcomes of Small Incision Lenticule Extraction versus LASIK. Ophthalmology 2014.
414. Ishii R, Shimizu K, Igarashi A, Kobashi H, Kamiya K. Influence of femtosecond lenticule extraction and small incision lenticule extraction on corneal nerve density and ocular surface: a 1-year prospective, confocal, microscopic study. J Refract Surg 2015;31:10-15.
415. Xu Y, Yang Y. Dry eye after small incision lenticule extraction and LASIK for myopia. J Refract Surg 2014;30:186-190.
416. Gao S, Li S, Liu L, et al. Early changes in ocular surface and tear inflammatory mediators after small-incision lenticule extraction and femtosecond laser-assisted laser in situ keratomileusis. PLoS One 2014;9:e107370.
417. Pradhan KR, Reinstein DZ, Carp GI, Archer TJ, Gobbe M, Gurung R. Femtosecond laser-assisted keyhole endokeratophakia: correction of hyperopia by implantation of an allogeneic lenticule obtained by SMILE from a myopic donor. J Refract Surg 2013;29:777-782.

133
418. Ganesh S, Brar S, Rao PA. Cryopreservation of extracted corneal lenticules after small incision lenticule extraction for potential use in human subjects. Cornea 2014;33:1355-1362.
419. Wong CW, Chan C, Tan D, Mehta JS. Incidence and management of suction loss in refractive lenticule extraction. J Cataract Refract Surg 2014;40:2002-2010.
420. Dong Z, Zhou X. Irregular astigmatism after femtosecond laser refractive lenticule extraction. J Cataract Refract Surg 2013;39:952-954.
421. Ivarsen A, Asp S, Hjortdal J. Safety and complications of more than 1500 small-incision lenticule extraction procedures. Ophthalmology 2014;121:822-828.
422. Ivarsen A, Hjortdal JO. Topography-guided photorefractive keratectomy for irregular astigmatism after small incision lenticule extraction. J Refract Surg 2014;30:429-432.
423. Donate D, Thaeron R. Preliminary Evidence of Successful Enhancement After a Primary SMILE Procedure With the Sub-Cap-Lenticule-Extraction Technique. J Refract Surg 2015;31:708-710.
424. Vazirani J, Basu S. Keratoconus: current perspectives. Clin Ophthalmol 2013;7:2019-2030.
425. Barnett M, Mannis MJ. Contact lenses in the management of keratoconus. Cornea 2011;30:1510-1516.
426. Zare MA, Hashemi H, Salari MR. Intracorneal ring segment implantation for the management of keratoconus: safety and efficacy. J Cataract Refract Surg 2007;33:1886-1891.
427. Shetty R, Kurian M, Anand D, Mhaske P, Narayana KM, Shetty BK. Intacs in advanced keratoconus. Cornea 2008;27:1022-1029.
428. Ertan A, Kamburoglu G. Intacs implantation using a femtosecond laser for management of keratoconus: Comparison of 306 cases in different stages. J Cataract Refract Surg 2008;34:1521-1526.
429. Ameerh MA, Hamad GI, Ababneh OH, Gharaibeh AM, Refai RM, Bdour MD. Ferrara ring segments implantation for treating keratoconus. Int J Ophthalmol 2012;5:586-590.
430. Sharif KW, Casey TA. Penetrating keratoplasty for keratoconus: complications and long-term success. Br J Ophthalmol 1991;75:142-146.
431. Buzard KA, Fundingsland BR. Corneal transplant for keratoconus: results in early and late disease. J Cataract Refract Surg 1997;23:398-406.
432. Olson RJ, Pingree M, Ridges R, Lundergan ML, Alldredge C, Jr., Clinch TE. Penetrating keratoplasty for keratoconus: a long-term review of results and complications. J Cataract Refract Surg 2000;26:987-991.
433. Javadi MA, Motlagh BF, Jafarinasab MR, et al. Outcomes of penetrating keratoplasty in keratoconus. Cornea 2005;24:941-946.
434. Mendes F, Schaumberg DA, Navon S, et al. Assessment of visual function after corneal transplantation: the quality of life and psychometric assessment after corneal transplantation (Q-PACT) study. Am J Ophthalmol 2003;135:785-793.
435. Karimian F, Feizi S. Deep anterior lamellar keratoplasty: indications, surgical techniques and complications. Middle East Afr J Ophthalmol 2010;17:28-37.
436. Reinhart WJ, Musch DC, Jacobs DS, Lee WB, Kaufman SC, Shtein RM. Deep anterior lamellar keratoplasty as an alternative to penetrating keratoplasty a report by the american academy of ophthalmology. Ophthalmology 2011;118:209-218.
437. Shimmura S, Tsubota K. Deep anterior lamellar keratoplasty. Curr Opin Ophthalmol 2006;17:349-355.
438. Spoerl E, Wollensak G, Dittert DD, Seiler T. Thermomechanical behavior of collagen-cross-linked porcine cornea. Ophthalmologica. Journal international d'ophtalmologie.

134
International journal of ophthalmology. Zeitschrift fur Augenheilkunde 2004;218:136-140.
439. Spoerl E, Wollensak G, Seiler T. Increased resistance of crosslinked cornea against enzymatic digestion. Current eye research 2004;29:35-40.
440. Sporl E, Huhle M, Kasper M, Seiler T. [Increased rigidity of the cornea caused by intrastromal cross-linking]. Der Ophthalmologe : Zeitschrift der Deutschen Ophthalmologischen Gesellschaft 1997;94:902-906.
441. Wollensak G, Spoerl E, Seiler T. Stress-strain measurements of human and porcine corneas after riboflavin-ultraviolet-A-induced cross-linking. J Cataract Refract Surg 2003;29:1780-1785.
442. Wollensak G, Spoerl E, Seiler T. Riboflavin/ultraviolet-a-induced collagen crosslinking for the treatment of keratoconus. Am J Ophthalmol 2003;135:620-627.
443. Kohlhaas M, Spoerl E, Schilde T, Unger G, Wittig C, Pillunat LE. Biomechanical evidence of the distribution of cross-links in corneas treated with riboflavin and ultraviolet A light. Journal of cataract and refractive surgery 2006;32:279-283.
444. Spoerl E, Huhle M, Seiler T. Induction of cross-links in corneal tissue. Exp Eye Res 1998;66:97-103.
445. Wollensak G, Redl B. Gel electrophoretic analysis of corneal collagen after photodynamic cross-linking treatment. Cornea 2008;27:353-356.
446. Fadlallah A, Dirani A, Chelala E, Antonios R, Cherfan G, Jarade E. Non-topography-guided PRK combined with CXL for the correction of refractive errors in patients with early stage keratoconus. J Refract Surg 2014;30:688-693.
447. Legare ME, Iovieno A, Yeung SN, et al. Intacs with or without same-day corneal collagen cross-linking to treat corneal ectasia. Can J Ophthalmol 2013;48:173-178.
448. Kamaev P, Friedman MD, Sherr E, Muller D. Photochemical kinetics of corneal cross-linking with riboflavin. Invest Ophthalmol Vis Sci 2012;53:2360-2367.
449. Seiler T, Huhle S, Spoerl E, Kunath H. Manifest diabetes and keratoconus: a retrospective case-control study. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie 2000;238:822-825.
450. Wollensak G, Spoerl E, Seiler T. Riboflavin/ultraviolet-a-induced collagen crosslinking for the treatment of keratoconus. American journal of ophthalmology 2003;135:620-627.
451. Zhang Y, Conrad AH, Conrad GW. Effects of ultraviolet-A and riboflavin on the interaction of collagen and proteoglycans during corneal cross-linking. The Journal of biological chemistry 2011;286:13011-13022.
452. Wollensak G, Spoerl E, Wilsch M, Seiler T. Endothelial cell damage after riboflavin-ultraviolet-A treatment in the rabbit. Journal of cataract and refractive surgery 2003;29:1786-1790.
453. Baiocchi S, Mazzotta C, Cerretani D, Caporossi T, Caporossi A. Corneal crosslinking: riboflavin concentration in corneal stroma exposed with and without epithelium. Journal of cataract and refractive surgery 2009;35:893-899.
454. Spoerl E, Mrochen M, Sliney D, Trokel S, Seiler T. Safety of UVA-riboflavin cross-linking of the cornea. Cornea 2007;26:385-389.
455. Sporl E, Raiskup-Wolf F, Pillunat LE. [Biophysical principles of collagen cross-linking]. Klinische Monatsblatter fur Augenheilkunde 2008;225:131-137.
456. Wollensak G. Crosslinking treatment of progressive keratoconus: new hope. Current opinion in ophthalmology 2006;17:356-360.
457. Spoerl E, Hoyer A, Pillunat LE, Raiskup F. Corneal cross-linking and safety issues. The open ophthalmology journal 2011;5:14-16.

135
458. Al Marzouky M.M. E-SHI, Pinelli R. Tensioactive-mediated Transepithelial Corneal Cross-linking – First Laboratory Report. European Ophthalmic Review 2009;3:3.
459. Boxer Wachler BS, Pinelli R, Ertan A, Chan CC. Safety and efficacy of transepithelial crosslinking (C3-R/CXL). Journal of cataract and refractive surgery 2010;36:186-188; author reply 188-189.
460. Chang SW, Chi RF, Wu CC, Su MJ. Benzalkonium chloride and gentamicin cause a leak in corneal epithelial cell membrane. Exp Eye Res 2000;71:3-10.
461. Majumdar S, Hippalgaonkar K, Repka MA. Effect of chitosan, benzalkonium chloride and ethylenediaminetetraacetic acid on permeation of acyclovir across isolated rabbit cornea. Int J Pharm 2008;348:175-178.
462. Koppen C, Wouters K, Mathysen D, Rozema J, Tassignon MJ. Refractive and topographic results of benzalkonium chloride-assisted transepithelial crosslinking. J Cataract Refract Surg 2012;38:1000-1005.
463. Soeters N, Wisse RP, Godefrooij DA, Imhof SM, Tahzib NG. Transepithelial versus epithelium-off corneal cross-linking for the treatment of progressive keratoconus: a randomized controlled trial. Am J Ophthalmol 2015;159:821-828 e823.
464. Filippello M, Stagni E, O'Brart D. Transepithelial corneal collagen crosslinking: bilateral study. J Cataract Refract Surg 2012;38:283-291.
465. Leccisotti A, Islam T. Transepithelial corneal collagen cross-linking in keratoconus. Journal of refractive surgery 2010;26:942-948.
466. Wollensak G, Iomdina E. Biomechanical and histological changes after corneal crosslinking with and without epithelial debridement. Journal of cataract and refractive surgery 2009;35:540-546.
467. Wollensak G, Sporl E, Reber F, Pillunat L, Funk R. Corneal endothelial cytotoxicity of riboflavin/UVA treatment in vitro. Ophthalmic Res 2003;35:324-328.
468. Seiler T, Hafezi F. Corneal cross-linking-induced stromal demarcation line. Cornea 2006;25:1057-1059.
469. Dai E, Gunderson CA. Pediatric central corneal thickness variation among major ethnic populations. J AAPOS 2006;10:22-25.
470. Haider KM, Mickler C, Oliver D, Moya FJ, Cruz OA, Davitt BV. Age and racial variation in central corneal thickness of preschool and school-aged children. J Pediatr Ophthalmol Strabismus 2008;45:227-233.
471. Raiskup F, Spoerl E. Corneal Cross-linking with Hypo-osmolar Riboflavin Solution in Thin Keratoconic Corneas. American journal of ophthalmology 2011;152:28-32 e21.
472. Bikbova G, Bikbov M. Transepithelial corneal collagen cross-linking by iontophoresis of riboflavin. Acta Ophthalmol 2014;92:e30-34.
473. Kymionis GD, Diakonis VF, Coskunseven E, Jankov M, Yoo SH, Pallikaris IG. Customized pachymetric guided epithelial debridement for corneal collagen cross linking. BMC Ophthalmol 2009;9:10.
474. Jacob S, Kumar DA, Agarwal A, Basu S, Sinha P, Agarwal A. Contact lens-assisted collagen cross-linking (CACXL): A new technique for cross-linking thin corneas. J Refract Surg 2014;30:366-372.
475. Kymionis GD, Portaliou DM, Diakonis VF, Kounis GA, Panagopoulou SI, Grentzelos MA. Corneal collagen cross-linking with riboflavin and ultraviolet-A irradiation in patients with thin corneas. Am J Ophthalmol 2012;153:24-28.
476. Wollensak G, Aurich H, Wirbelauer C, Sel S. Significance of the riboflavin film in corneal collagen crosslinking. J Cataract Refract Surg 2010;36:114-120.
477. Dohlman CH, Hedbys BO, Mishima S. The swelling pressure of the corneal stroma. Invest Ophthalmol 1962;1:158-162.

136
478. Maurice DM, Giardini AA. Swelling of the cornea in vivo after the destruction of its limiting layers. The British journal of ophthalmology 1951;35:791-797.
479. Hafezi F, Mrochen M, Iseli HP, Seiler T. Collagen crosslinking with ultraviolet-A and hypoosmolar riboflavin solution in thin corneas. Journal of Cataract and Refractive Surgery 2009;35:621-624.
480. Wu H, Luo S, Dong N, Lin Z, Liu Z, Shang X. [The clinical study of corneal cross-linking with hypo-osmolar riboflavin solution in thin keratoconic corneas]. Zhonghua Yan Ke Za Zhi 2014;50:681-686.
481. Raiskup F, Hoyer A, Spoerl E. Permanent corneal haze after riboflavin-UVA-induced cross-linking in keratoconus. Journal of refractive surgery 2009;25:S824-828.
482. Gu SF, Fan ZS, Wang LH, et al. A short-term study of corneal collagen cross-linking with hypo-osmolar riboflavin solution in keratoconic corneas. Int J Ophthalmol 2015;8:94-97.
483. Hafezi F. Limitation of collagen cross-linking with hypoosmolar riboflavin solution: failure in an extremely thin cornea. Cornea 2011;30:917-919.
484. Kaya V, Utine CA, Yilmaz OF. Intraoperative corneal thickness measurements during corneal collagen cross-linking with hypoosmolar riboflavin solution in thin corneas. Cornea 2012;31:486-490.
485. Soeters N, Tahzib NG. Standard and hypoosmolar corneal cross-linking in various pachymetry groups. Optom Vis Sci 2015;92:329-336.
486. Soeters N, van Bussel E, van der Valk R, Van der Lelij A, Tahzib NG. Effect of the eyelid speculum on pachymetry during corneal collagen crosslinking in keratoconus patients. J Cataract Refract Surg 2014;40:575-581.
487. Iwata S, Lemp MA, Holly FJ, Dohlman CH. Evaporation rate of water from the precorneal tear film and cornea in the rabbit. Invest Ophthalmol 1969;8:613-619.
488. Holopainen JM, Krootila K. Transient corneal thinning in eyes undergoing corneal cross-linking. Am J Ophthalmol 2011;152:533-536.
489. Tahzib NG, Van der Lelij A. Pachymetry during Cross-linking. Ophthalmology 2010;117:2041, 2041 e2041; author reply 2041-2042.
490. Schmidinger G, Pachala M, Prager F. Pachymetry changes during corneal crosslinking: effect of closed eyelids and hypotonic riboflavin solution. J Cataract Refract Surg 2013;39:1179-1183.
491. Muller LJ, Pels E, Vrensen GF. The effects of organ-culture on the density of keratocytes and collagen fibers in human corneas. Cornea 2001;20:86-95.
492. Ahearne M, Yang Y, Then KY, Liu KK. Non-destructive mechanical characterisation of UVA/riboflavin crosslinked collagen hydrogels. Br J Ophthalmol 2008;92:268-271.
493. Spadea L, Mencucci R. Transepithelial corneal collagen cross-linking in ultrathin keratoconic corneas. Clin Ophthalmol 2012;6:1785-1792.
494. Wollensak G, Iomdina E. Biomechanical and histological changes after corneal crosslinking with and without epithelial debridement. J Cataract Refract Surg 2009;35:540-546.
495. Zhang ZY, Zhang XR. Efficacy and safety of transepithelial corneal collagen crosslinking. J Cataract Refract Surg 2012;38:1304; author reply 1304-1305.
496. Bonnel S, Berguiga M, De Rivoyre B, et al. Demarcation line evaluation of iontophoresis-assisted transepithelial corneal collagen cross-linking for keratoconus. J Refract Surg 2015;31:36-40.
497. Buzzonetti L, Petrocelli G. Transepithelial corneal cross-linking in pediatric patients: early results. J Refract Surg 2012;28:763-767.

137
498. Kaya V, Utine CA, Yilmaz OF. Efficacy of corneal collagen cross-linking using a custom epithelial debridement technique in thin corneas: a confocal microscopy study. J Refract Surg 2011;27:444-450.
499. Mazzotta C, Ramovecchi V. Customized epithelial debridement for thin ectatic corneas undergoing corneal cross-linking: epithelial island cross-linking technique. Clin Ophthalmol 2014;8:1337-1343.
500. Samaras K, O'Brart D P, Doutch J, Hayes S, Marshall J, Meek KM. Effect of epithelial retention and removal on riboflavin absorption in porcine corneas. Journal of Refractive Surgery 2009;25:771-775.
501. Kolozsvari L, Nogradi A, Hopp B, Bor Z. UV absorbance of the human cornea in the 240- to 400-nm range. Invest Ophthalmol Vis Sci 2002;43:2165-2168.
502. Iseli HP, Popp M, Seiler T, Spoerl E, Mrochen M. Laboratory measurement of the absorption coefficient of riboflavin for ultraviolet light (365 nm). J Refract Surg 2011;27:195-201.
503. Ozgurhan EB, Akcay BI, Kurt T, Yildirim Y, Demirok A. Accelerated Corneal Collagen Cross-Linking in Thin Keratoconic Corneas. J Refract Surg 2015;31:386-390.
504. Mazzotta C, Traversi C, Caragiuli S, Rechichi M. Pulsed vs continuous light accelerated corneal collagen crosslinking: in vivo qualitative investigation by confocal microscopy and corneal OCT. Eye (Lond) 2014;28:1179-1183.
505. Muller D KP, Friedman MD, Sherr E, Eddington W. Accelerated UVA-RF corneal cross-linking through pulsed UVA illumination and oxygen rich environments. 2013.
506. Rechichi M MA, Mazzotta C. . Intraop in-vivo OCT pachymetric mapping during epi-off pulsed accellerated high fluence corneal collagen cross-linking with dextran free riboflavin. . 2013.
507. Labiris G, Giarmoukakis A, Sideroudi H, Gkika M, Fanariotis M, Kozobolis V. Impact of keratoconus, cross-linking and cross-linking combined with photorefractive keratectomy on self-reported quality of life. Cornea 2012;31:734-739.
508. Chen X, Stojanovic A, Zhou W, Utheim TP, Stojanovic F, Wang Q. Transepithelial, Topography-guided Ablation in the Treatment of Visual Disturbances in LASIK Flap or Interface Complications. J Refract Surg 2012;28:120-126.
509. Randleman JB. Post-laser in-situ keratomileusis ectasia: current understanding and future directions. Curr Opin Ophthalmol 2006;17:406-412.
510. Chelala E, Rami HE, Dirani A, Fadlallah A, Fakhoury O, Warrak E. Photorefractive keratectomy in patients with mild to moderate stable keratoconus: a five-year prospective follow-up study. Clin Ophthalmol 2013;7:1923-1928.
511. Cennamo G, Intravaja A, Boccuzzi D, Marotta G, Cennamo G. Treatment of keratoconus by topography-guided customized photorefractive keratectomy: two-year follow-up study. J Refract Surg 2008;24:145-149.
512. Kasparova EA, Kasparov AA. Six-year experience with excimer laser surgery for primary keratoconus in Russia. J Refract Surg 2003;19:S250-254.
513. Alpins N, Stamatelatos G. Customized photoastigmatic refractive keratectomy using combined topographic and refractive data for myopia and astigmatism in eyes with forme fruste and mild keratoconus. J Cataract Refract Surg 2007;33:591-602.
514. Guedj M, Saad A, Audureau E, Gatinel D. Photorefractive keratectomy in patients with suspected keratoconus: five-year follow-up. J Cataract Refract Surg 2013;39:66-73.
515. Koller T, Iseli HP, Donitzky C, Ing D, Papadopoulos N, Seiler T. Topography-guided surface ablation for forme fruste keratoconus. Ophthalmology 2006;113:2198-2202.

138
516. Khochtali S, Colin J, Touboul D, Binder PS. Does photorefractive keratectomy affect keratoconus progression? J Refract Surg 2010;26:925-926.
517. Kanellopoulos AJ. Comparison of sequential vs same-day simultaneous collagen cross-linking and topography-guided PRK for treatment of keratoconus. J Refract Surg 2009;25:S812-818.
518. Alessio G, L'Abbate M, Sborgia C, La Tegola MG. Photorefractive keratectomy followed by cross-linking versus cross-linking alone for management of progressive keratoconus: two-year follow-up. Am J Ophthalmol 2013;155:54-65 e51.
519. Sakla H, Altroudi W, Munoz G, Albarran-Diego C. Simultaneous topography-guided partial photorefractive keratectomy and corneal collagen crosslinking for keratoconus. J Cataract Refract Surg 2014;40:1430-1438.
520. Kymionis GD, Diakonis VF, Kalyvianaki M, et al. One-year follow-up of corneal confocal microscopy after corneal cross-linking in patients with post laser in situ keratosmileusis ectasia and keratoconus. Am J Ophthalmol 2009;147:774-778, 778 e771.
521. Kymionis GD, Kontadakis GA, Kounis GA, et al. Simultaneous topography-guided PRK followed by corneal collagen cross-linking for keratoconus. J Refract Surg 2009;25:S807-811.
522. Mukherjee AN, Selimis V, Aslanides I. Transepithelial photorefractive keratectomy with crosslinking for keratoconus. Open Ophthalmol J 2013;7:63-68.
523. Krueger RR, Kanellopoulos AJ. Stability of simultaneous topography-guided photorefractive keratectomy and riboflavin/UVA cross-linking for progressive keratoconus: case reports. J Refract Surg 2010;26:S827-832.
524. Kymionis GD, Portaliou DM, Kounis GA, Limnopoulou AN, Kontadakis GA, Grentzelos MA. Simultaneous topography-guided photorefractive keratectomy followed by corneal collagen cross-linking for keratoconus. Am J Ophthalmol 2011;152:748-755.
525. Kremer I, Aizenman I, Lichter H, Shayer S, Levinger S. Simultaneous wavefront-guided photorefractive keratectomy and corneal collagen crosslinking after intrastromal corneal ring segment implantation for keratoconus. J Cataract Refract Surg 2012;38:1802-1807.
526. Tuwairqi WS, Sinjab MM. Safety and efficacy of simultaneous corneal collagen cross-linking with topography-guided PRK in managing low-grade keratoconus: 1-year follow-up. J Refract Surg 2012;28:341-345.
527. Kymionis GD, Karavitaki AE, Kounis GA, Portaliou DM, Yoo SH, Pallikaris IG. Management of pellucid marginal corneal degeneration with simultaneous customized photorefractive keratectomy and collagen crosslinking. J Cataract Refract Surg 2009;35:1298-1301.
528. Kymionis GD, Portaliou DM, Diakonis VF, et al. Management of post laser in situ keratomileusis ectasia with simultaneous topography guided photorefractive keratectomy and collagen cross-linking. Open Ophthalmol J 2011;5:11-13.
529. Spadea L, Paroli M. Simultaneous topography-guided PRK followed by corneal collagen cross-linking after lamellar keratoplasty for keratoconus. Clin Ophthalmol 2012;6:1793-1800.
530. Al-Tuwairqi W, Sinjab MM. Intracorneal ring segments implantation followed by same-day topography-guided PRK and corneal collagen CXL in low to moderate keratoconus. J Refract Surg 2013;29:59-63.
531. Iovieno A, Legare ME, Rootman DB, Yeung SN, Kim P, Rootman DS. Intracorneal ring segments implantation followed by same-day photorefractive keratectomy and corneal collagen cross-linking in keratoconus. J Refract Surg 2011;27:915-918.

139
532. Li Y, Tang M, Zhang X, Salaroli CH, Ramos JL, Huang D. Pachymetric mapping with Fourier-domain optical coherence tomography. J Cataract Refract Surg 2010;36:826-831.
533. Eydelman MB, Drum B, Holladay J, et al. Standardized analyses of correction of astigmatism by laser systems that reshape the cornea. J Refract Surg 2006;22:81-95.
534. Alpins NA. A new method of analyzing vectors for changes in astigmatism. J Cataract Refract Surg 1993;19:524-533.
535. Alpins N. Astigmatism analysis by the Alpins method. J Cataract Refract Surg 2001;27:31-49.
536. Hersh PS, Fry K, Blaker JW. Spherical aberration after laser in situ keratomileusis and photorefractive keratectomy. Clinical results and theoretical models of etiology. J Cataract Refract Surg 2003;29:2096-2104.
537. Mrochen M, Kaemmerer M, Mierdel P, Seiler T. Increased higher-order optical aberrations after laser refractive surgery: a problem of subclinical decentration. J Cataract Refract Surg 2001;27:362-369.
538. Roberts C. The cornea is not a piece of plastic. J Refract Surg 2000;16:407-413. 539. Stulting RD, Fant BS, Group TCS. Results of topography-guided laser in situ
keratomileusis custom ablation treatment with a refractive excimer laser. J Cataract Refract Surg 2016;42:11-18.
540. Anera RG, Jimenez JR, Jimenez del Barco L, Bermudez J, Hita E. Changes in corneal asphericity after laser in situ keratomileusis. J Cataract Refract Surg 2003;29:762-768.
541. Marcos S, Cano D, Barbero S. Increase in corneal asphericity after standard laser in situ keratomileusis for myopia is not inherent to the Munnerlyn algorithm. J Refract Surg 2003;19:S592-596.
542. Kanellopoulos AJ. Topography-guided custom retreatments in 27 symptomatic eyes. J Refract Surg 2005;21:S513-518.
543. Yoon G, Macrae S, Williams DR, Cox IG. Causes of spherical aberration induced by laser refractive surgery. J Cataract Refract Surg 2005;31:127-135.
544. Calossi A. Corneal asphericity and spherical aberration. J Refract Surg 2007;23:505-514.
545. Kwon Y, Bott S. Postsurgery corneal asphericity and spherical aberration due to ablation efficiency reduction and corneal remodelling in refractive surgeries. Eye (Lond) 2009;23:1845-1850.
546. Bohac M, Biscevic A, Koncarevic M, Anticic M, Gabric N, Patel S. Comparison of Wavelight Allegretto Eye-Q and Schwind Amaris 750S excimer laser in treatment of high astigmatism. Graefes Arch Clin Exp Ophthalmol 2014;252:1679-1686.
547. Ginis HS, Katsanevaki VJ, Pallikaris IG. Influence of ablation parameters on refractive changes after phototherapeutic keratectomy. J Refract Surg 2003;19:443-448.
548. Roberts C. Biomechanics of the cornea and wavefront-guided laser refractive surgery. J Refract Surg 2002;18:S589-592.
549. Mrochen M, Donitzky C, Wullner C, Loffler J. Wavefront-optimized ablation profiles: theoretical background. J Cataract Refract Surg 2004;30:775-785.
550. Koller T, Iseli HP, Hafezi F, Mrochen M, Seiler T. Q-factor customized ablation profile for the correction of myopic astigmatism. J Cataract Refract Surg 2006;32:584-589.
551. Tran DB, Shah V. Higher order aberrations comparison in fellow eyes following intraLase LASIK with wavelight allegretto and customcornea LADArvision4000 systems. J Refract Surg 2006;22:S961-964.

140
552. Tuan KM, Chernyak D. Corneal asphericity and visual function after wavefront-guided LASIK. Optom Vis Sci 2006;83:605-610.
553. Krueger RR. Corneal topography vs ocular wavefront sensing in the retreatment of highly aberrated post surgical eyes. J Refract Surg 2006;22:328-330.
554. Ang BC, Foo RC, Lim EW, et al. Risk factors for early-onset corneal haze after photorefractive keratectomy in an Asian population: Outcomes from the Singapore Armed Forces Corneal Refractive Surgery Programme 2006 to 2013. J Cataract Refract Surg 2016;42:710-716.
555. Aslanides IM, Georgoudis PN, Selimis VD, Mukherjee AN. Single-step transepithelial ASLA (SCHWIND) with mitomycin-C for the correction of high myopia: long term follow-up. Clin Ophthalmol 2015;9:33-41.
556. Buzzonetti L, Petrocelli G, Laborante A, et al. A new transepithelial phototherapeutic keratectomy mode using the NIDEK CXIII excimer laser. J Refract Surg 2009;25:S122-124.
557. Fadlallah A, Fahed D, Khalil K, et al. Transepithelial photorefractive keratectomy: clinical results. J Cataract Refract Surg 2011;37:1852-1857.
558. Gambato C, Catania AG, Vujosevic S, Midena E. Wavefront-optimized surface ablation with the Allegretto Wave Eye-Q excimer laser platform: 12-month visual and refractive results. J Refract Surg 2011;27:792-795.
559. Gharaee H, Ghanavati SZ, Rad SS, Omidtabrizi A, Naseri H. Effectiveness of Technolas torsional eye tracking system on visual outcomes after photorefractive keratectomy. J Curr Ophthalmol 2015;27:82-86.
560. Hashemi H, Miraftab M, Ghaffari R, Asgari S. Femtosecond-Assisted LASIK Versus PRK: Comparison of 6-Month Visual Acuity and Quality Outcome for High Myopia. Eye Contact Lens 2015.
561. Hashemi M, Amiri MA, Tabatabaee M, Ayatollahi A. The results of photorefractive keratectomy with Mitomycin-C in myopia correction after 5 years. Pak J Med Sci 2016;32:225-228.
562. Kaluzny BJ, Cieslinska I, Mosquera SA, Verma S. Single-Step Transepithelial PRK vs Alcohol-Assisted PRK in Myopia and Compound Myopic Astigmatism Correction. Medicine (Baltimore) 2016;95:e1993.
563. Kocamis SI, Cakmak HB, Gerceker S, Cagil N. Long-Term Clinical Outcomes of Myopic Patients Having Thin Residual Corneal Thickness after Excimer Laser Surface Ablation. Semin Ophthalmol 2016;0.
564. Manche EE, Haw WW. Wavefront-guided laser in situ keratomileusis (Lasik) versus wavefront-guided photorefractive keratectomy (Prk): a prospective randomized eye-to-eye comparison (an American Ophthalmological Society thesis). Trans Am Ophthalmol Soc 2011;109:201-220.
565. Mifflin MD, Hatch BB, Sikder S, Bell J, Kurz CJ, Moshirfar M. Custom vs conventional PRK: a prospective, randomized, contralateral eye comparison of postoperative visual function. J Refract Surg 2012;28:127-132.
566. Schallhorn SC, Venter JA, Hannan SJ, Hettinger KA. Wavefront-Guided Photorefractive Keratectomy with the Use of a New Hartmann-Shack Aberrometer in Patients with Myopia and Compound Myopic Astigmatism. J Ophthalmol 2015;2015:514837.
567. Sia RK, Coe CD, Edwards JD, Ryan DS, Bower KS. Visual outcomes after Epi-LASIK and PRK for low and moderate myopia. J Refract Surg 2012;28:65-71.
568. Stojanovic A, Chen S, Chen X, et al. One-step transepithelial topography-guided ablation in the treatment of myopic astigmatism. PLoS One 2013;8:e66618.

141
569. Ghadhfan F, Al-Rajhi A, Wagoner MD. Laser in situ keratomileusis versus surface ablation: visual outcomes and complications. J Cataract Refract Surg 2007;33:2041-2048.
570. Abolhassani A, Shojaei A, Baradaran-Rafiee AR, Eslani M, Elahi B, Noorizadeh F. Vector analysis of cross cylinder LASIK with the NIDEK EC-5000 excimer laser for high astigmatism. J Refract Surg 2009;25:1075-1082.
571. Alio JL, Pachkoria K, El Aswad A, Plaza-Puche AB. Laser-assisted in situ keratomileusis in high mixed astigmatism with optimized, fast-repetition and cyclotorsion control excimer laser. Am J Ophthalmol 2013;155:829-836.
572. Alio JL, Plaza-Puche AB, Martinez LM, Torky M, Brenner LF. Laser in situ keratomileusis using optimized aspheric profiles and cyclotorsion control to treat compound myopic astigmatism with high cylinder. J Cataract Refract Surg 2013;39:28-35.
573. Arbelaez MC, Vidal C, Arba-Mosquera S. Excimer laser correction of moderate to high astigmatism with a non-wavefront-guided aberration-free ablation profile: Six-month results. J Cataract Refract Surg 2009;35:1789-1798.
574. Frings A, Vidic B, El-Shabrawi Y, Ardjomand N. Laser-assisted subepithelial keratomileusis with mitomycin C for myopic astigmatism >/=2.00 diopters using a Zeiss MEL 80 Excimer. Int Ophthalmol 2014;34:225-233.
575. Hasegawa A, Kojima T, Isogai N, Tamaoki A, Nakamura T, Ichikawa K. Astigmatism correction: Laser in situ keratomileusis versus posterior chamber collagen copolymer toric phakic intraocular lens implantation. J Cataract Refract Surg 2012;38:574-581.
576. Igarashi A, Kamiya K, Shimizu K, Komatsu M. Time course of refractive and corneal astigmatism after laser in situ keratomileusis for moderate to high astigmatism. J Cataract Refract Surg 2012;38:1408-1413.
577. Ivarsen A, Naeser K, Hjortdal J. Laser in situ keratomileusis for high astigmatism in myopic and hyperopic eyes. J Cataract Refract Surg 2013;39:74-80.
578. Katz T, Wagenfeld L, Galambos P, Darrelmann BG, Richard G, Linke SJ. LASIK versus photorefractive keratectomy for high myopic (> 3 diopter) astigmatism. J Refract Surg 2013;29:824-831.
579. Schallhorn SC, Venter JA, Hannan SJ, Hettinger KA. Clinical outcomes of wavefront-guided laser in situ keratomileusis to treat moderate-to-high astigmatism. Clin Ophthalmol 2015;9:1291-1298.
580. Alpins NA. New method of targeting vectors to treat astigmatism. J Cataract Refract Surg 1997;23:65-75.
581. Vinciguerra P, Sborgia M, Epstein D, Azzolini M, MacRae S. Photorefractive keratectomy to correct myopic or hyperopic astigmatism with a cross-cylinder ablation. J Refract Surg 1999;15:S183-185.
582. Hori-Komai Y, Sakai C, Toda I, Ito M, Yamamoto T, Tsubota K. Detection of cyclotorsional rotation during excimer laser ablation in LASIK. J Refract Surg 2007;23:911-915.
583. Porter J, Yoon G, Lozano D, et al. Aberrations induced in wavefront-guided laser refractive surgery due to shifts between natural and dilated pupil center locations. J Cataract Refract Surg 2006;32:21-32.
584. Wang L, Koch DD. Residual higher-order aberrations caused by clinically measured cyclotorsional misalignment or decentration during wavefront-guided excimer laser corneal ablation. J Cataract Refract Surg 2008;34:2057-2062.
585. Qian Y, Huang J, Chu R, Zhou X, Olszewski E. Influence of intraocular astigmatism on the correction of myopic astigmatism by laser-assisted subepithelial keratectomy. J Cataract Refract Surg 2014;40:558-563.

142
586. Qian YS, Huang J, Liu R, et al. Influence of internal optical astigmatism on the correction of myopic astigmatism by LASIK. J Refract Surg 2011;27:863-868.
587. Archer TJ, Reinstein DZ, Pinero DP, Gobbe M, Carp GI. Comparison of the predictability of refractive cylinder correction by laser in situ keratomileusis in eyes with low or high ocular residual astigmatism. J Cataract Refract Surg 2015;41:1383-1392.
588. Chen X, Stojanovic A, Liu Y, Chen Y, Zhou Y, Utheim TP. Postoperative Changes in Corneal Epithelial and Stromal Thickness Profiles After Photorefractive Keratectomy in Treatment of Myopia. J Refract Surg 2015;31:446-453.
589. Azar DT, Chang JH, Han KY. Wound healing after keratorefractive surgery: review of biological and optical considerations. Cornea 2012;31 Suppl 1:S9-19.
590. Zagon IS, Sassani JW, Ruth TB, McLaughlin PJ. Epithelial adhesion complexes and organ culture of the human cornea. Brain Res 2001;900:205-213.
591. Li Y, Tan O, Brass R, Weiss JL, Huang D. Corneal epithelial thickness mapping by Fourier-domain optical coherence tomography in normal and keratoconic eyes. Ophthalmology 2012;119:2425-2433.
592. Silverman RH, Urs R, Roychoudhury A, Archer TJ, Gobbe M, Reinstein DZ. Epithelial remodeling as basis for machine-based identification of keratoconus. Invest Ophthalmol Vis Sci 2014;55:1580-1587.
593. Reinstein DZ, Gobbe M, Archer TJ, Couch D. Epithelial thickness profile as a method to evaluate the effectiveness of collagen cross-linking treatment after corneal ectasia. J Refract Surg 2011;27:356-363.
594. Reinstein DZ, Gobbe M, Archer TJ, Youssefi G, Sutton HF. Stromal surface topography-guided custom ablation as a repair tool for corneal irregular astigmatism. J Refract Surg 2015;31:54-59.
595. Reinstein DZ, Archer TJ, Gobbe M. Change in epithelial thickness profile 24 hours and longitudinally for 1 year after myopic LASIK: three-dimensional display with Artemis very high-frequency digital ultrasound. J Refract Surg 2012;28:195-201.
596. Erie JC, Patel SV, McLaren JW, et al. Effect of myopic laser in situ keratomileusis on epithelial and stromal thickness: a confocal microscopy study. Ophthalmology 2002;109:1447-1452.
597. Wang J, Thomas J, Cox I, Rollins A. Noncontact measurements of central corneal epithelial and flap thickness after laser in situ keratomileusis. Invest Ophthalmol Vis Sci 2004;45:1812-1816.
598. Spadea L, Fasciani R, Necozione S, Balestrazzi E. Role of the corneal epithelium in refractive changes following laser in situ keratomileusis for high myopia. J Refract Surg 2000;16:133-139.
599. Gauthier CA, Holden BA, Epstein D, Tengroth B, Fagerholm P, Hamberg-Nystrom H. Role of epithelial hyperplasia in regression following photorefractive keratectomy. Br J Ophthalmol 1996;80:545-548.
600. Kanellopoulos AJ, Asimellis G. In vivo three-dimensional corneal epithelium imaging in normal eyes by anterior-segment optical coherence tomography: a clinical reference study. Cornea 2013;32:1493-1498.
601. Kanellopoulos AJ, Asimellis G. Corneal epithelial remodeling following cataract surgery: three-dimensional investigation with anterior-segment optical coherence tomography. J Refract Surg 2014;30:348-353.
602. Rocha KM, Perez-Straziota CE, Stulting RD, Randleman JB. SD-OCT analysis of regional epithelial thickness profiles in keratoconus, postoperative corneal ectasia, and normal eyes. J Refract Surg 2013;29:173-179.

143
603. Kanellopoulos AJ, Asimellis G. In vivo 3-dimensional corneal epithelial thickness mapping as an indicator of dry eye: preliminary clinical assessment. Am J Ophthalmol 2014;157:63-68 e62.
604. Francoz M, Karamoko I, Baudouin C, Labbe A. Ocular surface epithelial thickness evaluation with spectral-domain optical coherence tomography. Invest Ophthalmol Vis Sci 2011;52:9116-9123.
605. Feng Y, Simpson TL. Corneal, limbal, and conjunctival epithelial thickness from optical coherence tomography. Optom Vis Sci 2008;85:E880-883.
606. Du C, Wang J, Cui L, Shen M, Yuan Y. Vertical and horizontal corneal epithelial thickness profiles determined by ultrahigh resolution optical coherence tomography. Cornea 2012;31:1036-1043.
607. Yang Y, Hong J, Deng SX, Xu J. Age-related changes in human corneal epithelial thickness measured with anterior segment optical coherence tomography. Invest Ophthalmol Vis Sci 2014;55:5032-5038.
608. Radford SW, Lim R, Salmon JF. Comparison of Orbscan and ultrasound pachymetry in the measurement of central corneal thickness. Eye (Lond) 2004;18:434-436.
609. Lohmann CP, Reischl U, Marshall J. Regression and epithelial hyperplasia after myopic photorefractive keratectomy in a human cornea. J Cataract Refract Surg 1999;25:712-715.
610. Gauthier CA, Holden BA, Epstein D, Tengroth B, Fagerholm P, Hamberg-Nystrom H. Factors affecting epithelial hyperplasia after photorefractive keratectomy. J Cataract Refract Surg 1997;23:1042-1050.
611. Gauthier CA, Epstein D, Holden BA, et al. Epithelial alterations following photorefractive keratectomy for myopia. J Refract Surg 1995;11:113-118.
612. Reinstein DZ, Archer TJ, Gobbe M. Refractive and topographic errors in topography-guided ablation produced by epithelial compensation predicted by 3D Artemis VHF digital ultrasound stromal and epithelial thickness mapping. J Refract Surg 2012;28:657-663.
613. Vinciguerra P, Azzolini C, Vinciguerra R. Corneal curvature gradient determines corneal healing process and epithelial behavior. J Refract Surg 2015;31:281-282.
614. Reinstein DZ, Gobbe M, Archer TJ, Silverman RH, Coleman DJ. Epithelial, stromal, and total corneal thickness in keratoconus: three-dimensional display with artemis very-high frequency digital ultrasound. J Refract Surg 2010;26:259-271.
615. Haque S, Jones L, Simpson T. Thickness mapping of the cornea and epithelium using optical coherence tomography. Optom Vis Sci 2008;85:E963-976.
616. Zhao Y, Hong J, Wang F, et al. [The study of corneal epithelial change in keratoconic eyes with Fourier-domain optical coherence tomographic pachymetry]. Zhonghua Yan Ke Za Zhi 2014;50:665-670.
617. Kanellopoulos AJ, Asimellis G. Epithelial remodeling after femtosecond laser-assisted high myopic LASIK: comparison of stand-alone with LASIK combined with prophylactic high-fluence cross-linking. Cornea 2014;33:463-469.
618. Dougherty PJ, Wellish KL, Maloney RK. Excimer laser ablation rate and corneal hydration. Am J Ophthalmol 1994;118:169-176.
619. Vinciguerra P, Azzolini M, Radice P, Sborgia M, De Molfetta V. A method for examining surface and interface irregularities after photorefractive keratectomy and laser in situ keratomileusis: predictor of optical and functional outcomes. J Refract Surg 1998;14:S204-206.
620. Luger MH, Ewering T, Arba-Mosquera S. Consecutive myopia correction with transepithelial versus alcohol-assisted photorefractive keratectomy in contralateral eyes: one-year results. J Cataract Refract Surg 2012;38:1414-1423.

144
621. Alessio G, Boscia F, La Tegola MG, Sborgia C. Topography-driven photorefractive keratectomy: results of corneal interactive programmed topographic ablation software. Ophthalmology 2000;107:1578-1587.
622. Guirao A, Williams DR. A method to predict refractive errors from wave aberration data. Optom Vis Sci 2003;80:36-42.
623. Guirao A. Theoretical elastic response of the cornea to refractive surgery: risk factors for keratectasia. J Refract Surg 2005;21:176-185.
624. Roberts C. Biomechanical customization: the next generation of laser refractive surgery. Journal of Cataract and Refractive Surgery 2005;31:2-5.
625. Klein SR, Epstein RJ, Randleman JB, Stulting RD. Corneal ectasia after laser in situ keratomileusis in patients without apparent preoperative risk factors. Cornea 2006;25:388-403.
626. Roy AS, Dupps WJ, Jr. Effects of altered corneal stiffness on native and postoperative LASIK corneal biomechanical behavior: A whole-eye finite element analysis. J Refract Surg 2009;25:875-887.
627. Read SA, Collins MJ. Diurnal variation of corneal shape and thickness. Optom Vis Sci 2009;86:170-180.
628. Reznicek L, Muth D, Kampik A, Neubauer AS, Hirneiss C. Evaluation of a novel Scheimpflug-based non-contact tonometer in healthy subjects and patients with ocular hypertension and glaucoma. Br J Ophthalmol 2013;97:1410-1414.
629. Liu J, Roberts CJ. Influence of corneal biomechanical properties on intraocular pressure measurement: quantitative analysis. Journal of Cataract and Refractive Surgery 2005;31:146-155.
630. Han Z, Tao C, Zhou D, et al. Air puff induced corneal vibrations: theoretical simulations and clinical observations. J Refract Surg 2014;30:208-213.
631. Rechichi M, Daya S, Scorcia V, Meduri A, Scorcia G. Epithelial-disruption collagen crosslinking for keratoconus: one-year results. J Cataract Refract Surg 2013;39:1171-1178.
632. Caporossi A, Mazzotta C, Paradiso AL, Baiocchi S, Marigliani D, Caporossi T. Transepithelial corneal collagen crosslinking for progressive keratoconus: 24-month clinical results. J Cataract Refract Surg 2013;39:1157-1163.
633. Raiskup-Wolf F, Hoyer A, Spoerl E, Pillunat LE. Collagen crosslinking with riboflavin and ultraviolet-A light in keratoconus: long-term results. J Cataract Refract Surg 2008;34:796-801.
634. Raiskup F, Theuring A, Pillunat LE, Spoerl E. Corneal collagen crosslinking with riboflavin and ultraviolet-A light in progressive keratoconus: ten-year results. J Cataract Refract Surg 2015;41:41-46.
635. Kapasi M, Baath J, Mintsioulis G, Jackson WB, Baig K. Phototherapeutic keratectomy versus mechanical epithelial removal followed by corneal collagen crosslinking for keratoconus. Can J Ophthalmol 2012;47:344-347.
636. Cha SH, Lee JS, Oum BS, Kim CD. Corneal epithelial cellular dysfunction from benzalkonium chloride (BAC) in vitro. Clin Experiment Ophthalmol 2004;32:180-184.
637. Kissner A, Spoerl E, Jung R, Spekl K, Pillunat LE, Raiskup F. Pharmacological modification of the epithelial permeability by benzalkonium chloride in UVA/Riboflavin corneal collagen cross-linking. Curr Eye Res 2010;35:715-721.
638. Raiskup F, Spoerl E. Corneal cross-linking with hypo-osmolar riboflavin solution in thin keratoconic corneas. Am J Ophthalmol 2011;152:28-32 e21.

145
639. Meadows DL, Paugh JR, Joshi A, Mordaunt J. A novel method to evaluate residence time in humans using a nonpenetrating fluorescent tracer. Invest Ophthalmol Vis Sci 2002;43:1032-1039.
640. Hafezi F, Iseli HP. Pregnancy-related exacerbation of iatrogenic keratectasia despite corneal collagen crosslinking. J Cataract Refract Surg 2008;34:1219-1221.
641. Asri D, Touboul D, Fournie P, et al. Corneal collagen crosslinking in progressive keratoconus: multicenter results from the French National Reference Center for Keratoconus. J Cataract Refract Surg 2011;37:2137-2143.
642. Vinciguerra P, Albe E, Trazza S, et al. Refractive, topographic, tomographic, and aberrometric analysis of keratoconic eyes undergoing corneal cross-linking. Ophthalmology 2009;116:369-378.
643. Wollensak G, Iomdina E, Dittert DD, Herbst H. Wound healing in the rabbit cornea after corneal collagen cross-linking with riboflavin and UVA. Cornea 2007;26:600-605.
644. Ringvold A. Corneal epithelium and UV-protection of the eye. Acta Ophthalmol Scand 1998;76:149-153.
645. Podskochy A. Protective role of corneal epithelium against ultraviolet radiation damage. Acta Ophthalmol Scand 2004;82:714-717.
646. Richoz O, Hammer A, Tabibian D, Gatzioufas Z, Hafezi F. The Biomechanical Effect of Corneal Collagen Cross-Linking (CXL) With Riboflavin and UV-A is Oxygen Dependent. Transl Vis Sci Technol 2013;2:6.
647. Kanellopoulos AJ, Binder PS. Collagen cross-linking (CCL) with sequential topography-guided PRK: a temporizing alternative for keratoconus to penetrating keratoplasty. Cornea 2007;26:891-895.
648. Guell JL, Verdaguer P, Elies D, Gris O, Manero F. Late onset of a persistent, deep stromal scarring after PRK and corneal cross-linking in a patient with forme fruste keratoconus. J Refract Surg 2014;30:286-288.
649. Alessio G, L'Abbate M, Furino C, Sborgia C, La Tegola MG. Confocal microscopy analysis of corneal changes after photorefractive keratectomy plus cross-linking for keratoconus: 4-year follow-up. Am J Ophthalmol 2014;158:476-484.e471.
650. Kontadakis GA, Kankariya VP, Tsoulnaras K, Pallikaris AI, Plaka A, Kymionis GD. Long-Term Comparison of Simultaneous Topography-Guided Photorefractive Keratectomy Followed by Corneal Cross-linking versus Corneal Cross-linking Alone. Ophthalmology 2016.


146
14. PAPERS



One-Step Transepithelial Topography-Guided Ablationin the Treatment of Myopic AstigmatismAleksandar Stojanovic1,2*, Shihao Chen3,4, Xiangjun Chen1, Filip Stojanovic5, Jia Zhang3,4, Ting Zhang3,
Tor Paaske Utheim1,6
1 SynsLaser Kirurgi, Oslo and Tromsø, Norway, 2 Eye Department, University Hospital North Norway, Tromsø, Norway, 3 School of Optometry and Ophthalmology and Eye
Hospital, Wenzhou Medical College, Wenzhou, Zhejiang, China, 4 Key Laboratory of Vision Science, Ministry of Health P.R. China, Wenzhou, Zhejiang, China, 5 Faculty of
Medicine, University of Tromsø, Tromsø, Norway, 6Department of Medical Biochemistry, Oslo University Hospital, Oslo, Norway
Abstract
Purpose: To evaluate one-step topography-guided transepithelial ablation in the treatment of low to moderate myopicastigmatism using a 1KHz excimer laser.
Methods: Retrospective study of 117 consecutive eyes available for evaluation 12 months after surgery. Pre- and post-operative visual and refractive data as well as post-operative pain and haze were analyzed. A novel technique integratingcustom refractive- and epithelial- ablation in a single uninterrupted procedure was used.
Results: The mean pre-operative spherical equivalent (SE) and the mean cylinder were: –3.22 diopters (D) 61.54 (SD) (range–0.63 to –7.25 D) and –0.77 D 60.65 (range 0 to –4.50 D), respectively. At 12 months after surgery: no eyes lost $2 lines ofcorrected distant visual acuity (CDVA). Safety and efficacy indexes were 1.27 and 1.09, respectively. Uncorrected distantvisual acuity (UDVA) was $20/20 in 96.6% of the eyes. Manifest refraction spherical equivalent was within 60.5 D of thedesired refraction in 93.2% of the eyes. Average root mean square (RMS) wavefront error measured at central 6 mm,increased from 0.38 pre-operatively to 0.47 mm post-operatively. Refractive stability was achieved and sustained 1 monthafter surgery. No visually significant haze was registered during the observation period. Post-operative pain was reported in4.5% of patients.
Conclusions: One-step transepithelial topography-guided treatment for low to moderate myopia and astigmatismperformed with a 1 KHz laser, provided safe, effective, predictable and stable results with low pain and no visuallysignificant haze.
Citation: Stojanovic A, Chen S, Chen X, Stojanovic F, Zhang J, et al. (2013) One-Step Transepithelial Topography-Guided Ablation in the Treatment of MyopicAstigmatism. PLoS ONE 8(6): e66618. doi:10.1371/journal.pone.0066618
Editor: Andreas Wedrich, Medical University Graz, Austria
Received December 27, 2012; Accepted May 8, 2013; Published June 17, 2013
Copyright: � 2013 Stojanovic et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permitsunrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Funding: This work was supported by SynsLaser Kirurgi AS, Tromsø, Norway and Norges forskningsrad, Oslo, Norway. The funders had no role in the studydesign, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing Interests: This study was funded by SynsLaser Kirurgi AS, Tromsø, together with Norges forskningsrad, Oslo, Norway. Authors AleksandarStojanovic, Xiangjun Chen, and Tor Paaske Utheim are employed by SynsLaser Kirurgi AS. This does not alter the authors’ adherence to all the PLOS ONE policeson sharing data and materials.
* E-mail: [email protected]
Introduction
Due to its lower impact on corneal biomechanical stability and
lower risk of dry eye[1,2] compared to LASIK, surface ablation is
often used in cases with thin corneas, recurrent erosion,
predisposition for trauma, or in patients who are anatomically or
psychologically unsuitable for use of microkeratome.[3] Post-
operative haze,[4–6] slow visual recovery[7,8] and post-operative
discomfort,[9,10] all inherent to the traditional photorefractive
keratectomy, are now better controlled with modern surface
ablation protocols. Smooth ablation achieved by small-Gaussian-
beam, high-frequency lasers, pre-operative use of mitomycin-C,
post-operative protection from UV-radiation and dietary supple-
mentation with vitamin-C have previously reduced the incidence
and severity of post-operative haze after surface ablation.[11–
14]_ENREF_10 Refinement of de-epithelialization techniques
and pre- and post-operative medication continues to decrease the
severity of post-operative discomfort[15] and to increase the speed
of visual recovery.[16,17] The current transepithelial topography-
guided ablation technique has been reported earlier for treatment
of irregular astigmatism.[18–20] To our knowledge, not only has
the combination of one-step transepithelial ablation, topography-
guided custom ablation and 1000 Hz-laser technology never been
published before, but there are few reports concerning any of the
mentioned technologies; transepithelial ablation,[21–23] topogra-
phy-guided ablation,[24–30] or use of 1000 Hz- laser[31,32] in
routine treatments of low to moderate myopia in virgin eyes.
Patients and MethodsThe present retrospective study comprises 117 consecutive eyes
of 61 patients (30 female, 31 male) who were available for
evaluation at $12 months after treatment for myopic astigmatism,
at SynsLaser Clinic in Tromsø, Norway. The mean age was
32.7169.7 years (range 18 to 61). Patients provided written,
PLOS ONE | www.plosone.org 1 June 2013 | Volume 8 | Issue 6 | e66618

informed consent and the study was approved by the regional
ethics committee ‘‘Regional komite for medisinsk og helsefaglig
forskningsetikk, Nord-Norge (REK Nord)’’- P REK NORD 55/
2009 Sikkerhet og effekt av refraktiv kirurgi med iVIS lasersystem:
en retrospektiv analyse av kliniske data. Inclusion criteria for
treatment were: age $18 years; no soft contact lens wear for 1
week (hard contact lens for 4 weeks) before the baseline
examination; SE between –0.5 and –10.00 diopters (D) with
#6.00 D of refractive astigmatism; stable refractive error (change
of SE #0.50 D) for $2 years; and CDVA of 20/25 or better.
Exclusion criteria were: eye pathology, including keratoconus or
keratoconus suspect (detected by corneal topo-/tomography);
previous eye surgery; glaucoma; diabetes; and systemic diseases
that could affect corneal wound healing (e.g. collagen vascular
diseases). Pre-operative examination included slit lamp biomicros-
copy, Scheimpflug-based corneal topo-/tomography (Precisio,
iVIS Technology, Taranto, Italy), visual acuity/subjective refrac-
tion (Nidek RT 2100 system, Nidek Co. Ltd., Aichi, Japan),
Placido-based corneal topography and wavefront aberrometry
(Nidek OPD II, Nidek Co. Ltd., Aichi, Japan), dynamic
pupilometry (pMetrics, iVIS Technology, Taranto, Italy), Gold-
mann applanation tonometry and central ultrasound pachymetry
(Corneo-Gage Plus, Sonogage Inc., Cleveland, Ohio).
The refraction, corneal anterior elevation and pachymetry maps
of patients, as well as their dynamic pupilometry data were
imported to ‘‘Corneal Interactive Programmed Topographic
Ablation’’ (CIPTA, iVIS Technology, Taranto, Italy) software to
generate a custom ablation plan within a treatment zone suggested
by the dynamic pupilometry. The pupilometer measures pupil size
and the speed of the pupillary reactions under various lighting
conditions adjusted for the patient’s ‘‘life-style’’. The result of the
examination produces so-called ‘‘ideal entrance pupil’’ size, to
which the distance of pupil decentration with respect to the visual
axis intercept is added, resulting in the default optical zone that
can be overwritten by the user. The CIPTA software uses
subjective refraction and corneal topography as the basis for
treatment of lower- and higher-order aberrations (HOAs),
respectively (the latter limited to HOAs originating from the
corneal surface). Since the treatments are calculated on the basis of
topography, the manifest cylinder is superimposed on the existing
toric surface. Hence the aimed regular aconic surface is a
resolution of the vectors of the manifest and the corneal
astigmatism. In the current study, the calculated post-operative
minimal corneal residual stromal thickness was set to $350 mm,
assuming the epithelial thickness of 65 mm. All treatments were
aimed toward achieving emmetropia and within the ablation
pattern the optic of the ablated lenticel were centered on the
corneal intercept of the visual axis.
Ascorbic acid (C-vitamin, Weifa, Norway) and EPA/DHA
(Omega-3, Nycomed, Norway) were both given 1000 mg daily 2
weeks before and 2 weeks after the surgery. Prednisolone
(Prednisolone, Nycomed, Asker, Norway) 40 mg tablet and
Alprazolam (Xanor, Pfizer Inc., New York, USA) 0.5 mg tablet
were given orally as a single dose 30 minutes before the surgery.
Diclophenac 0.1% (Voltaren, Novartis, Basel, Switzerland) and
ciprofloxacine 0.5% (Cilox, Alcon, Fort Worth, Texas) eye drops
were administered 15, 10 and 5 minutes before the surgery.
Proparacaine 0.5% (Alcaine, Alcon, Fort Worth, Texas), 2–3
drops, were applied before, and 1–2 additional drops after the
insertion of the eye speculum. Before the laser ablation, 10–15
drops of Balanced Salt Solution (BSS, Alcon, Fort Worth, Texas)
chilled to the freezing point, were applied, after which the corneal
surface was gently dried with a lint-free pre-shrunk Merocel until a
reflective homogeneous, dry epithelial surface was achieved. After
the cyclotorsional (iris and scleral vessels) and the pupil eye-
tracker-registration, the treatment was performed with a 0.6-mm
dual-flying-spot 1 KHz (26500 Hz) excimer laser (iRES, iVIS
Technology, Taranto, Italy) using the one-step custom transepi-
thelial ‘‘no-touch’’ (cTEN, iVIS Technology, Taranto, Italy)
ablation technique.
The cTEN-ablation consists of a refractive part, which reshapes
the corneal surface within the treatment zone into an aspheric
regular shape of desired curvature, and a lamellar part of 65 mm,
based on Reinsteins measurement which showed thickest epithe-
lium of 58.8 64.9 mm.[33] (Figure 1). These two parts are
summed and executed in a single uninterrupted ablation, lasting
typically 20–35s. With this approach, the de-epithelialized area
corresponds directly to the area of the custom ablation, so only an
absolutely necessary amount of epithelium is removed. The mean
targeted optical zone diameter was 6.3060.28 mm (range 6.0 to
7.6 mm) and the mean total ablation diameter was
7.7260.62 mm (range 7.0 to 9.9 mm).
At the end 1–2 non-preserved Chloramphenicol (Novartis,
Basel, Switzerland) eye drops were applied, followed by a bandage
contact lens (Acuvue Oaysis, Johnson & Johnson, USA). Dexa-
methasone with Chloramphenicol mixture (Spersadex med
Kloramfenikol, Novartis, Basel, Switzerland) eye drops QID were
used the first 2 weeks, and then replaced by a low potency steroid
Rimexolone 1% (Vexol, Alcon, Fort Worth, Texas) eye drops in
tapering doses for another 2–4 weeks. Refrigerated 0.2%
hyaluronic acid (Oxyal, SantenPharma, Solna, Sweden) was used
for lubrication and lavage purposes every 10 minutes the rest of
the day after the surgery and later as needed. Additionally, the
patients were supplied with ‘‘comfort drops’’, a single container
with 0.5 ml, 1% Tetracaine hydroxide (Tetrakain minims,
Chauvin, Kingston, England) in case of pain. All patients were
questioned regarding postoperative pain and the need for use of
‘‘comfort drops’’. _ENREF_22.
Bandage contact lens was removed from the cornea of patients
between post-operative days 3 to 7 and patients were observed at
1, 3, 6, and 12 months after surgery. Post-operative examinations
were similar to pre-operative examinations. Haze was defined as:
grade 0.5 - trace easily seen using a slit-lamp microscope; grade 1 –
trace that does not affect vision; grade 2 - dense patches affecting
Figure 1. Pre-operative corneal surface with the epithelium(green) (a), is reshaped into a regular aspheric surface ofdesired curvature (b) and the new surface is transferred belowthe epithelium (c) in a single non-interrupted ablation.doi:10.1371/journal.pone.0066618.g001
Transepithelial Topo-Guided Custom Ablation
PLOS ONE | www.plosone.org 2 June 2013 | Volume 8 | Issue 6 | e66618

vision; grade 3 - dense partially obscuring iris details; grade 4 -
dense haze completely obscuring iris details.
Statistical analysis was performed using SPSS 13.0. The initial
Snellen visual acuity was recorded using logMAR steps. Calcula-
tion of mean visual acuity was achieved via conversion from
Snellen to logMAR and back to Snellen. The outcomes were
reported according to the Standardized graphs and terms for
refractive surgery results.[34].
Results
AccountabilityAmong the 165 eyes of 86 patients treated for primary myopia
from September 21 to December 19, 2009, 117 eyes of 61 patients
(71%) were available for evaluation $12 months after surgery.
Among those, 104 (89%), 110 (94%), and 66 (56%) eyes were also
available for evaluation at 1, 3 and 6 months post-operatively,
respectively.
Baseline dataThe mean pre-operative UDVA and CDVA were 20/160
(range 20/1000 to 20/25) and 20/18.2 (range 20/20 to 20/13.3),
respectively. The mean pre-operative SE was –3.2261.54 D
(range –0.63 to –7.25 D) and the mean cylinder was –0.7760.65
D (range 0 to –4.50 D).
EfficacyCumulative UDVA at 6 and 12 months after surgery compared
to pre-operative CDVA are shown on Figure 2. Efficacy index was
0.91, 1.00, 1.09 and 1.09, at 1, 3, 6 and 12 months post-
operatively, respectively.
PredictabilityThe attempted versus achieved SE at 6 and 12 months post-
operatively are shown in Figure 3. All eyes were within 61.0 D of
emmetropia, 94% of eyes were within 60.5 D of emmetropia at
12 months and 97% of eyes had refractive astigmatism less or
equal to 0.5 D at 12 months post-operatively.
SafetyLoss and gain of lines of CDVA are shown in Figure 4. The
safety index was 1.27 for both 6 and 12 months.
Stability of refractionThe stability of refraction is shown on Figure 5. Post-operative
spherical equivalent refraction stability was reached at 1 month,
with no statistically significant difference between each two follow-
up points thereafter. Seven (10.6%) out of 66 eyes available for a 6
month follow-up control, regressed more than -0.50 D between 6
and 12 months post-operatively.
Higher order aberrationsPre-operative and 12-month post-operative average RMS of
total HOAs, coma-type- (S3+5+7) and spherical- (S4+6+8)aberrations are shown in table 1. RMS of total HOAs and
coma-type aberrations increased, while the spherical aberration
showed no statistically significant change.
Figure 2. Post-operative uncorrected visual acuity vs. pre-operative best spectacle-corrected visual acuity.doi:10.1371/journal.pone.0066618.g002
Figure 3. Attempted vs. achieved spherical equivalent refrac-tive change at 12 months postoperatively.doi:10.1371/journal.pone.0066618.g003
Transepithelial Topo-Guided Custom Ablation
PLOS ONE | www.plosone.org 3 June 2013 | Volume 8 | Issue 6 | e66618
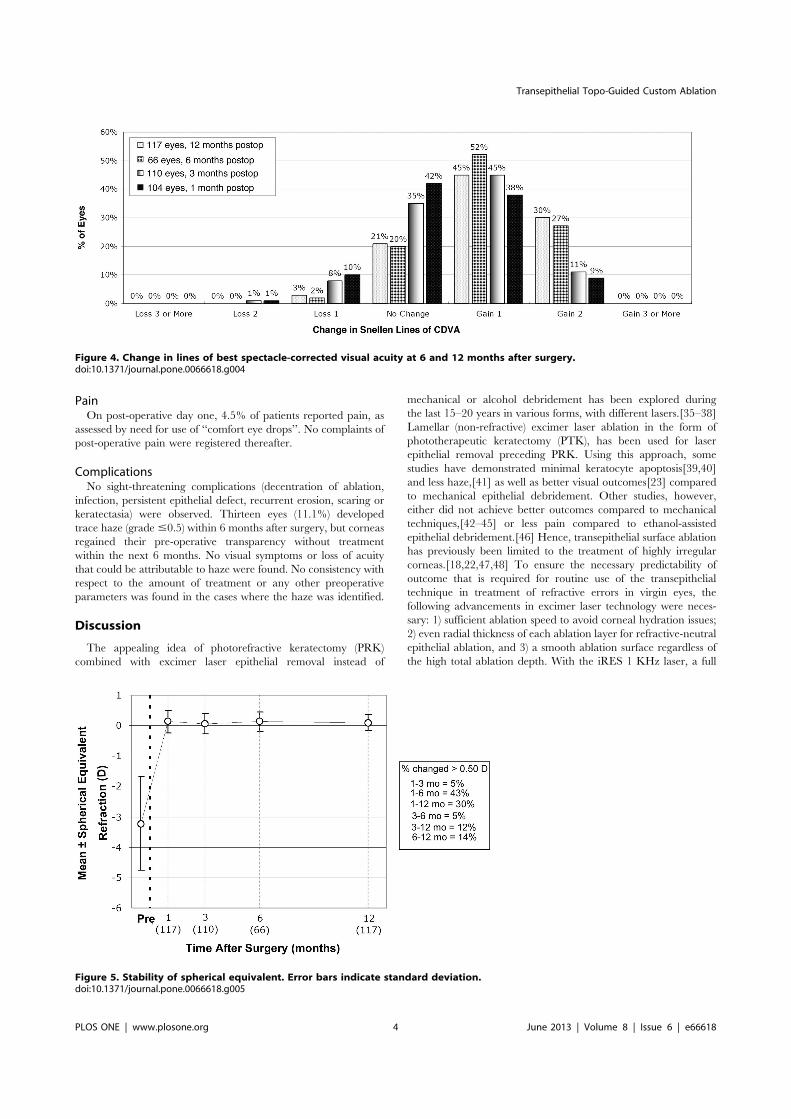
PainOn post-operative day one, 4.5% of patients reported pain, as
assessed by need for use of ‘‘comfort eye drops’’. No complaints of
post-operative pain were registered thereafter.
ComplicationsNo sight-threatening complications (decentration of ablation,
infection, persistent epithelial defect, recurrent erosion, scaring or
keratectasia) were observed. Thirteen eyes (11.1%) developed
trace haze (grade #0.5) within 6 months after surgery, but corneas
regained their pre-operative transparency without treatment
within the next 6 months. No visual symptoms or loss of acuity
that could be attributable to haze were found. No consistency with
respect to the amount of treatment or any other preoperative
parameters was found in the cases where the haze was identified.
Discussion
The appealing idea of photorefractive keratectomy (PRK)
combined with excimer laser epithelial removal instead of
mechanical or alcohol debridement has been explored during
the last 15–20 years in various forms, with different lasers.[35–38]
Lamellar (non-refractive) excimer laser ablation in the form of
phototherapeutic keratectomy (PTK), has been used for laser
epithelial removal preceding PRK. Using this approach, some
studies have demonstrated minimal keratocyte apoptosis[39,40]
and less haze,[41] as well as better visual outcomes[23] compared
to mechanical epithelial debridement. Other studies, however,
either did not achieve better outcomes compared to mechanical
techniques,[42–45] or less pain compared to ethanol-assisted
epithelial debridement.[46] Hence, transepithelial surface ablation
has previously been limited to the treatment of highly irregular
corneas.[18,22,47,48] To ensure the necessary predictability of
outcome that is required for routine use of the transepithelial
technique in treatment of refractive errors in virgin eyes, the
following advancements in excimer laser technology were neces-
sary: 1) sufficient ablation speed to avoid corneal hydration issues;
2) even radial thickness of each ablation layer for refractive-neutral
epithelial ablation, and 3) a smooth ablation surface regardless of
the high total ablation depth. With the iRES 1 KHz laser, a full
Figure 4. Change in lines of best spectacle-corrected visual acuity at 6 and 12 months after surgery.doi:10.1371/journal.pone.0066618.g004
Figure 5. Stability of spherical equivalent. Error bars indicate standard deviation.doi:10.1371/journal.pone.0066618.g005
Transepithelial Topo-Guided Custom Ablation
PLOS ONE | www.plosone.org 4 June 2013 | Volume 8 | Issue 6 | e66618
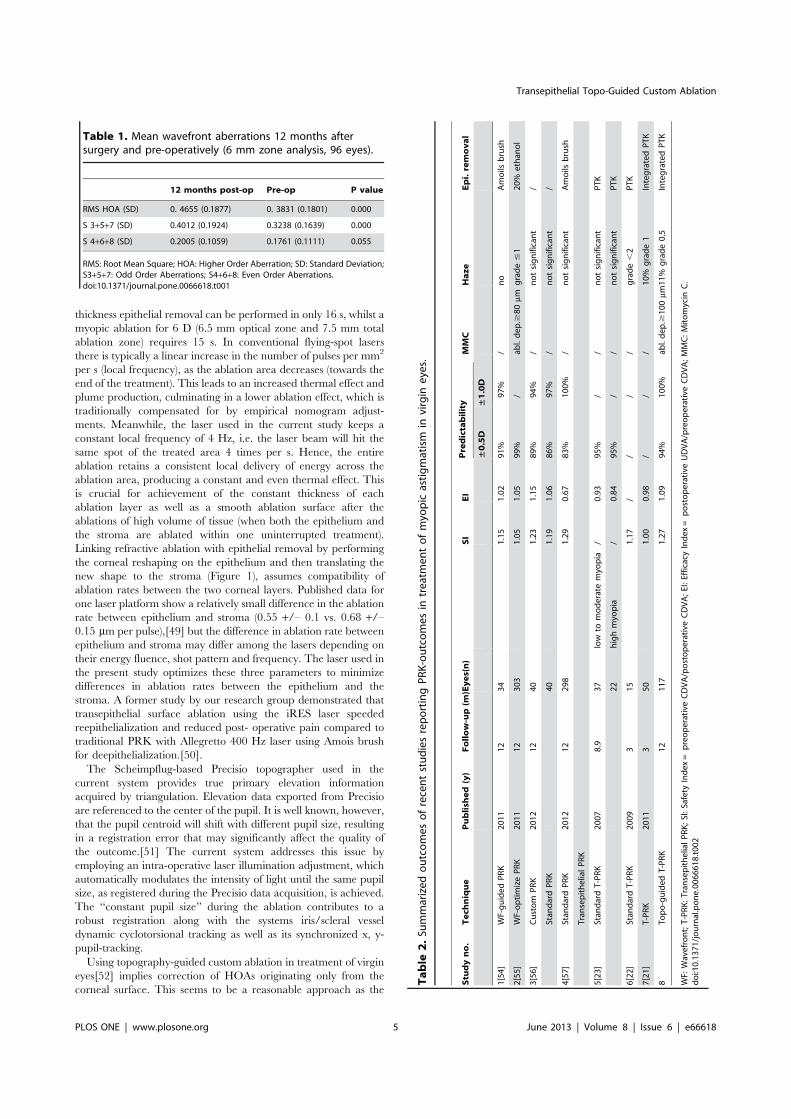
thickness epithelial removal can be performed in only 16 s, whilst a
myopic ablation for 6 D (6.5 mm optical zone and 7.5 mm total
ablation zone) requires 15 s. In conventional flying-spot lasers
there is typically a linear increase in the number of pulses per mm2
per s (local frequency), as the ablation area decreases (towards the
end of the treatment). This leads to an increased thermal effect and
plume production, culminating in a lower ablation effect, which is
traditionally compensated for by empirical nomogram adjust-
ments. Meanwhile, the laser used in the current study keeps a
constant local frequency of 4 Hz, i.e. the laser beam will hit the
same spot of the treated area 4 times per s. Hence, the entire
ablation retains a consistent local delivery of energy across the
ablation area, producing a constant and even thermal effect. This
is crucial for achievement of the constant thickness of each
ablation layer as well as a smooth ablation surface after the
ablations of high volume of tissue (when both the epithelium and
the stroma are ablated within one uninterrupted treatment).
Linking refractive ablation with epithelial removal by performing
the corneal reshaping on the epithelium and then translating the
new shape to the stroma (Figure 1), assumes compatibility of
ablation rates between the two corneal layers. Published data for
one laser platform show a relatively small difference in the ablation
rate between epithelium and stroma (0.55 +/– 0.1 vs. 0.68 +/–0.15 mm per pulse),[49] but the difference in ablation rate between
epithelium and stroma may differ among the lasers depending on
their energy fluence, shot pattern and frequency. The laser used in
the present study optimizes these three parameters to minimize
differences in ablation rates between the epithelium and the
stroma. A former study by our research group demonstrated that
transepithelial surface ablation using the iRES laser speeded
reepithelialization and reduced post- operative pain compared to
traditional PRK with Allegretto 400 Hz laser using Amois brush
for deepithelialization.[50].
The Scheimpflug-based Precisio topographer used in the
current system provides true primary elevation information
acquired by triangulation. Elevation data exported from Precisio
are referenced to the center of the pupil. It is well known, however,
that the pupil centroid will shift with different pupil size, resulting
in a registration error that may significantly affect the quality of
the outcome.[51] The current system addresses this issue by
employing an intra-operative laser illumination adjustment, which
automatically modulates the intensity of light until the same pupil
size, as registered during the Precisio data acquisition, is achieved.
The ‘‘constant pupil size’’ during the ablation contributes to a
robust registration along with the systems iris/scleral vessel
dynamic cyclotorsional tracking as well as its synchronized x, y-
pupil-tracking.
Using topography-guided custom ablation in treatment of virgin
eyes[52] implies correction of HOAs originating only from the
corneal surface. This seems to be a reasonable approach as the
Table 1. Mean wavefront aberrations 12 months aftersurgery and pre-operatively (6 mm zone analysis, 96 eyes).
12 months post-op Pre-op P value
RMS HOA (SD) 0. 4655 (0.1877) 0. 3831 (0.1801) 0.000
S 3+5+7 (SD) 0.4012 (0.1924) 0.3238 (0.1639) 0.000
S 4+6+8 (SD) 0.2005 (0.1059) 0.1761 (0.1111) 0.055
RMS: Root Mean Square; HOA: Higher Order Aberration; SD: Standard Deviation;S3+5+7: Odd Order Aberrations; S4+6+8: Even Order Aberrations.doi:10.1371/journal.pone.0066618.t001
Table
2.Su
mmarizedoutcomesofrecentstudiesreportingPRK-outcomesin
treatmentofmyo
pic
astigmatism
invirgin
eyes.
Stu
dyno.
Tech
nique
Publish
ed(y)
Follow-up(m
)Eyes(n)
SI
EI
Predictability
MMC
Haze
Epi.removal
±0.5D
±1.0D
1[54]
WF-guidedPRK
2011
12
34
1.15
1.02
91%
97%
/no
Amoils
brush
2[55]
WF-optimizePRK
2011
12
303
1.05
1.05
99%
/ab
l.dep.$
80mm
grade#1
20%
ethan
ol
3[56]
Custom
PRK
2012
12
40
1.23
1.15
89%
94%
/notsignifican
t/
Stan
dardPRK
40
1.19
1.06
86%
97%
/notsignifican
t/
4[57]
Stan
dardPRK
2012
12
298
1.29
0.67
83%
100%
/notsignifican
tAmoils
brush
TransepithelialPRK
5[23]
Stan
dardT-PRK
2007
8.9
37
low
tomoderate
myo
pia
/0.93
95%
//
notsignifican
tPTK
22
highmyo
pia
/0.84
95%
//
notsignifican
tPTK
6[22]
Stan
dardT-PRK
2009
315
1.17
//
//
grade,2
PTK
7[21]
T-PRK
2011
350
1.00
0.98
//
/10%
grade1
IntegratedPTK
8Topo-guidedT-PRK
12
117
1.27
1.09
94%
100%
abl.dep.$
100mm
11%
grade0.5
IntegratedPTK
WF:
Wavefront;T-PRK:TransepithelialPRK;SI:Safety
Index=
preoperative
CDVA/postoperative
CDVA;EI:Efficacy
Index=
postoperative
UDVA/preoperative
CDVA;MMC:Mitomycin
C.
doi:10.1371/journal.pone.0066618.t002
Transepithelial Topo-Guided Custom Ablation
PLOS ONE | www.plosone.org 5 June 2013 | Volume 8 | Issue 6 | e66618

corneal surface is responsible for the majority of light refraction in
the eye. Furthermore the corneal HOAs are static and hence more
appropriate as a target for treatment than the dynamic HOAs of
crystalline lens. In addition to correcting the corneal surface
HOAs, the current topography-guided ablation creates a custom-
ized transition that keeps a constant dioptric gradient towards the
untreated cornea, instead of employing commonly used fixed
transition zone diameter. This may lead to lower regression by
preventing any counterproductive epithelial remodeling.
Peer-reviewed publications from the recent five years reporting
the outcomes of PRK in treatment of myopic astigmatism in virgin
eyes are listed in table 2. The table shows that the safety, efficacy
and predictability in our study are comparable with the best
outcomes of the other studies, independent on the mode of
epithelial removal or the excimer laser used. Moreover, the table
shows only trace haze (grade #0.5). This also compares very
favorably with the other studies. There is only one publication[21]
reporting the outcomes using a similar approach to the current
one, with the epithelial removal integrated within a single ablation.
However, the treatments from that report were non-customized
and only the initial 3-month results in 50 eyes were analyzed.
One shortcoming of the transepithelial technique used in this
study is the epithelial thickness estimation (estimated to 65 mm by
default), instead of using the real measurement. This estimation
may lead to too deep ablation and waste of corneal tissue if the real
epithelial thickness is lower, or to shallower ablation and a smaller
optical/treatment zone than intended if the real epithelial
thickness is higher. A high-resolution corneal imaging technology,
that could be expected in the near future, is likely to provide the
necessary precision for measurement of epithelial thickness. This
may provide an epithelial thickness map usable for custom
ablation planning. In that event, an ablation plan consisting of an
epithelial and a stromal component would allow for accurate
compensation for any difference in laser ablation rates between
these two corneal tissues, further increasing the precision of the
procedure. This would address the issues of slightly irregular
ablation in eyes with non-uniform epithelial thickness,[33] as
described in our previous work.[53] Precise epithelial thickness
mapping would also be of great value in studying the influence of
different reepithelialization profiles on the refractive outcomes and
would supposedly be of great help in refining the ablation design.
The idea of one-step ‘‘no-touch’’ laser treatment appeals to the
patients because it is much quicker and more comfortable than
traditional excimer laser surgery. The main appeal of this
procedure to the surgeon is its perceived lack of serious
complications as well as ease and speed of performance.
In conclusion, the outcomes of this study suggest that
transepithelial topography- guided surface ablation, which inte-
grates epithelial debridement and refractive error correction into a
single custom ablation, is safe, effective, and predictable in
treatment of low to moderate myopic astigmatism.
Author Contributions
Conceived and designed the experiments: AS SC XC FS JZ TPU.
Performed the experiments: AS SC XC JZ TZ. Analyzed the data: AS SC
XC FS JZ TZ. Contributed reagents/materials/analysis tools: AS SC XC
FS JZ TZ TPU. Wrote the paper: AS SC XC FS JZ TPU.
References
1. Seiler T, Huhle S, Spoerl E, Kunath H (2000) Manifest diabetes and
keratoconus: a retrospective case-control study. Graefes Arch Clin Exp
Ophthalmol 238: 822–825.
2. Krueger RR, Mrochen M (2008) Introduction to the proceedings of the Third
International Congress of Corneal Cross-Linking. Journal of refractive surgery
24: S713–714.
3. Ambrosio R Jr, Wilson S (2003) LASIK vs LASEK vs PRK: advantages and
indications. Seminars in ophthalmology 18: 2–10.
4. Kolozsvari L, Nogradi A, Hopp B, Bor Z (2002) UV absorbance of the human
cornea in the 240- to 400-nm range. Invest Ophthalmol Vis Sci 43: 2165–2168.
5. Koller T, Mrochen M, Seiler T (2009) Complication and failure rates after
corneal crosslinking. J Cataract Refract Surg 35: 1358–1362.
6. Stojanovic A, Nitter TA (2001) Correlation between ultraviolet radiation level
and the incidence of late-onset corneal haze after photorefractive keratectomy.
Journal of cataract and refractive surgery 27: 404–410.
7. Shortt AJ, Allan BD (2006) Photorefractive keratectomy (PRK) versus laser-
assisted in-situ keratomileusis (LASIK) for myopia. Cochrane database of
systematic reviews: CD005135.
8. de Benito-Llopis L, Teus MA, Sanchez-Pina JM, Hernandez-Verdejo JL (2007)
Comparison between LASEK and LASIK for the correction of low myopia.
Journal of refractive surgery 23: 139–145.
9. O’Doherty M, Kirwan C, O’Keeffe M, O’Doherty J (2007) Postoperative pain
following epi-LASIK, LASEK, and PRK for myopia. Journal of refractive
surgery 23: 133–138.
10. Torres LF, Sancho C, Tan B, Padilla K, Schanzlin DJ, et al. (2007) Early
postoperative pain following Epi-LASIK and photorefractive keratectomy: a
prospective, comparative, bilateral study. Journal of refractive surgery 23: 126–
132.
11. Vinciguerra P, Azzolini M, Radice P, Sborgia M, De Molfetta V (1998) A
method for examining surface and interface irregularities after photorefractive
keratectomy and laser in situ keratomileusis: predictor of optical and functional
outcomes. Journal of refractive surgery 14: S204–206.
12. Argento C, Cosentino MJ, Ganly M (2006) Comparison of laser epithelial
keratomileusis with and without the use of mitomycin C. Journal of refractive
surgery 22: 782–786.
13. Caffi M (1966) [Histopathology of keratoconus]. Annali di ottalmologia e clinica
oculistica 92: 429–435.
14. Stojanovic A, Ringvold A, Nitter T (2003) Ascorbate prophylaxis for corneal
haze after photorefractive keratectomy. Journal of refractive surgery 19: 338–
343.
15. Faktorovich EG, Basbaum AI (2010) Effect of topical 0.5% morphine on
postoperative pain after photorefractive keratectomy. Journal of refractive
surgery 26: 934–941.
16. Autrata R, Rehurek J (2003) Laser-assisted subepithelial keratectomy for
myopia: two-year follow-up. J Cataract Refract Surg 29: 661–668.
17. Leccisotti A (2003) Laser-assisted subepithelial keratectomy (LASEK) without
alcohol versus photorefractive keratectomy (PRK). Eur J Ophthalmol 13: 676–
680.
18. Pedrotti E, Sbabo A, Marchini G (2006) Customized transepithelial photo-
refractive keratectomy for iatrogenic ametropia after penetrating or deep
lamellar keratoplasty. Journal of cataract and refractive surgery 32: 1288–1291.
19. Cusumano A, Coleman DJ, Silverman RH, Reinstein DZ, Rondeau MJ, et al.
(1998) Three-dimensional ultrasound imaging. Clinical applications. Ophthal-
mology 105: 300–306.
20. Chen X, Stojanovic A, Nitter TA (2010) Topography-guided transepithelial
surface ablation in treatment of recurrent epithelial ingrowths. Journal of
refractive surgery 26: 529–532.
21. Fadlallah A, Fahed D, Khalil K, Dunia I, Menassa J, et al. (2011) Transepithelial
photorefractive keratectomy: clinical results. J Cataract Refract Surg 37: 1852–
1857.
22. Buzzonetti L, Petrocelli G, Laborante A, Mazzilli E, Gaspari M, et al. (2009) A
new transepithelial phototherapeutic keratectomy mode using the NIDEK
CXIII excimer laser. J Refract Surg 25: S122–124.
23. Ghadhfan F, Al-Rajhi A, Wagoner MD (2007) Laser in situ keratomileusis versus
surface ablation: visual outcomes and complications. Journal of cataract and
refractive surgery 33: 2041–2048.
24. Waring G, Dougherty PJ, Chayet A, Fischer J, Fant B, et al. (2007)
Topographically guided LASIK for myopia using the Nidek CXII customized
aspheric treatment zone (CATz). Trans Am Ophthalmol Soc 105: 240–246;
discussion 247–248.
25. Kermani O, Schmiedt K, Oberheide U, Gerten G (2006) Topographic- and
wavefront-guided customized ablations with the NIDEK-EC5000CXII in
LASIK for myopia. J Refract Surg 22: 754–763.
26. Pop M, Bains HS (2005) Clinical outcomes of CATz versus OPDCAT. J Refract
Surg 21: S636–639.
27. Vinciguerra P, Albe E, Camesasca FI, Trazza S, Epstein D (2007) Wavefront-
versus topography-guided customized ablations with the NIDEK EC-5000 CX
II in surface ablation treatment: refractive and aberrometric outcomes. J Refract
Surg 23: S1029–1036.
28. El Awady HE, Ghanem AA, Saleh SM (2011) Wavefront-optimized ablation
versus topography-guided customized ablation in myopic LASIK: comparative
Transepithelial Topo-Guided Custom Ablation
PLOS ONE | www.plosone.org 6 June 2013 | Volume 8 | Issue 6 | e66618

study of higher order aberrations. Ophthalmic Surg Lasers Imaging 42: 314–
320.29. Falavarjani KG, Hashemi M, Modarres M, Sanjari MS, Darvish N, et al. (2011)
Topography-Guided vs Wavefront-Optimized Surface Ablation for Myopia
Using the WaveLight Platform: A Contralateral Eye Study. J Refract Surg 27:13–17.
30. Cummings AB, Mascharka N (2010) Outcomes after topography-based LASIKand LASEK with the wavelight oculyzer and topolyzer platforms. J Refract Surg
26: 478–485.
31. Khoramnia R, Salgado JP, Wuellner C, Donitzky C, Lohmann CP, et al. (2011)Safety, efficacy, predictability and stability of laser in situ keratomileusis (LASIK)
with a 1000-Hz scanning spot excimer laser. Acta Ophthalmol.32. Winkler von Mohrenfels C, Khoramnia R, Wullner C, Donitzky C, Salgado J, et
al. (2010) First clinical results of epithelial laser in situ keratomileusis with a1000 Hz excimer laser. J Cataract Refract Surg 36: 449–455.
33. Reinstein DZ, Archer TJ, Gobbe M, Silverman RH, Coleman DJ (2008)
Epithelial thickness in the normal cornea: three-dimensional display withArtemis very high-frequency digital ultrasound. Journal of refractive surgery 24:
571–581.34. Stulting RD, Dupps WJ Jr, Kohnen T, Mamalis N, Rosen ES, et al. (2011)
Standardized graphs and terms for refractive surgery results. Cornea 30: 945–
947.35. Phillips AF, McDonnell PJ (1997) Laser-induced fluorescence during photo-
refractive keratectomy: a method for controlling epithelial removal. Americanjournal of ophthalmology 123: 42–47.
36. Kim WJ, Shah S, Wilson SE (1998) Differences in keratocyte apoptosis followingtransepithelial and laser-scrape photorefractive keratectomy in rabbits. Journal
of refractive surgery 14: 526–533.
37. Kapadia MS, Wilson SE (1998) Transepithelial photorefractive keratectomy fortreatment of thin flaps or caps after complicated laser in situ keratomileusis.
American journal of ophthalmology 126: 827–829.38. Kapadia MS, Meisler DM, Wilson SE (1999) Epithelial removal with the
excimer laser (laser-scrape) in photorefractive keratectomy retreatment.
Ophthalmology 106: 29–34.39. Helena MC, Baerveldt F, Kim WJ, Wilson SE (1998) Keratocyte apoptosis after
corneal surgery. Investigative ophthalmology & visual science 39: 276–283.40. Bilgihan K, Bilgihan A, Adiguzel U, Sezer C, Yis O, et al. (2002) Keratocyte
apoptosis and corneal antioxidant enzyme activities after refractive cornealsurgery. Eye 16: 63–68.
41. Carr JD, Patel R, Hersh PS (1995) Management of late corneal haze following
photorefractive keratectomy. Journal of refractive surgery 11: S309–313.42. Clinch TE, Moshirfar M, Weis JR, Ahn CS, Hutchinson CB, et al. (1999)
Comparison of mechanical and transepithelial debridement during photore-fractive keratectomy. Ophthalmology 106: 483–489.
43. Gimbel HV, DeBroff BM, Beldavs RA, van Westenbrugge JA, Ferensowicz M
(1995) Comparison of laser and manual removal of corneal epithelium forphotorefractive keratectomy. Journal of refractive surgery 11: 36–41.
44. Lee JB, Seong GJ, Lee JH, Seo KY, Lee YG, et al. (2001) Comparison of laserepithelial keratomileusis and photorefractive keratectomy for low to moderate
myopia. Journal of cataract and refractive surgery 27: 565–570.
45. Lee HK, Lee KS, Kim JK, Kim HC, Seo KR, et al. (2005) Epithelial healing
and clinical outcomes in excimer laser photorefractive surgery following three
epithelial removal techniques: mechanical, alcohol, and excimer laser. American
journal of ophthalmology 139: 56–63.
46. Kanitkar KD, Camp J, Humble H, Shen DJ, Wang MX (2000) Pain after
epithelial removal by ethanol-assisted mechanical versus transepithelial excimer
laser debridement. Journal of refractive surgery 16: 519–522.
47. Alessio G, Boscia F, La Tegola MG, Sborgia C (2001) Topography-driven
excimer laser for the retreatment of decentralized myopic photorefractive
keratectomy. Ophthalmology 108: 1695–1703.
48. La Tegola MG, Alessio G, Sborgia C (2007) Topographic customized
photorefractive keratectomy for regular and irregular astigmatism after
penetrating keratoplasty using the LIGI CIPTA/LaserSight platform. Journal
of refractive surgery 23: 681–693.
49. Seiler T, Kriegerowski M, Schnoy N, Bende T (1990) Ablation rate of human
corneal epithelium and Bowman’s layer with the excimer laser (193 nm).
Refractive & corneal surgery 6: 99–102.
50. Chen X, Stojanovic A, Oeritsland H (2010) "Transepithelial Custom Ablation vs
PRK With Mechanical Epithelial Removal. Comparison of Postoperative Pain,
Re- epithelialization Speed and Early Visual Outcomes.". pp. presentated at the
XXVIII Congress of the European Society of Cataract and Refractive Surgeons,
Paris, France. Reference available at: http://escrs.org/publications/eurotimes/
11March/no-touch.pdf. Accessed September 25, 2011.
51. Porter J, Yoon G, Lozano D, Wolfing J, Tumbar R, et al. (2006) Aberrations
induced in wavefront-guided laser refractive surgery due to shifts between
natural and dilated pupil center locations. Journal of cataract and refractive
surgery 32: 21–32.
52. Falavarjani KG, Hashemi M, Modarres M, Sanjari MS, Darvish N, et al. (2011)
Topography-Guided vs Wavefront-Optimized Surface Ablation for Myopia
Using the WaveLight Platform: A Contralateral Eye Study. Journal of Refractive
Surgery 27: 13–17.
53. Chen X, Stojanovic A, Zhou W, Utheim TP, Stojanovic F, et al. (2012)
Transepithelial, Topography-guided Ablation in the Treatment of Visual
Disturbances in LASIK Flap or Interface Complications. J Refract Surg 28:
120–126.
54. Manche EE, Haw WW (2011) Wavefront-guided laser in situ keratomileusis
(Lasik) versus wavefront-guided photorefractive keratectomy (Prk): a prospective
randomized eye-to-eye comparison (an American Ophthalmological Society
thesis). Trans Am Ophthalmol Soc 109: 201–220.
55. Gambato C, Catania AG, Vujosevic S, Midena E (2011) Wavefront-optimized
surface ablation with the Allegretto Wave Eye-Q excimer laser platform: 12-
month visual and refractive results. J Refract Surg 27: 792–795.
56. Mifflin MD, Hatch BB, Sikder S, Bell J, Kurz CJ, et al. (2012) Custom vs
conventional PRK: a prospective, randomized, contralateral eye comparison of
postoperative visual function. J Refract Surg 28: 127–132.
57. Sia RK, Coe CD, Edwards JD, Ryan DS, Bower KS (2012) Visual outcomes
after Epi-LASIK and PRK for low and moderate myopia. J Refract Surg 28: 65–
71.
Transepithelial Topo-Guided Custom Ablation
PLOS ONE | www.plosone.org 7 June 2013 | Volume 8 | Issue 6 | e66618



Reliability of Corneal Dynamic Scheimpflug AnalyserMeasurements in Virgin and Post-PRK EyesXiangjun Chen1,2*, Aleksandar Stojanovic1,2,3, Yanjun Hua4,5, Jon Roger Eidet6, Di Hu5, Jingting Wang5,
Tor Paaske Utheim6,7
1 SynsLaser Kirurgi, Oslo and Tromsø, Norway, 2University of Oslo, Oslo, Norway, 3 Eye Department, University Hospital of North Norway, Tromsø, Norway, 4Department
of Ophthalmology, Taihe Hospital, Hubei Medical University, Hubei, China, 5 School of Ophthalmology and Optometry and Eye Hospital, Wenzhou Medical University,
Wenzhou, Zhejiang, China, 6Department of Medical Biochemistry, Oslo University Hospital, Oslo, Norway, 7 Institute of Oral Biology, Faculty of Dentistry, University of
Oslo, Oslo, Norway
Abstract
Purpose: To determine the measurement reliability of CorVis ST, a dynamic Scheimpflug analyser, in virgin and post-photorefractive keratectomy (PRK) eyes and compare the results between these two groups.
Methods: Forty virgin eyes and 42 post-PRK eyes underwent CorVis ST measurements performed by two technicians.Repeatability was evaluated by comparing three consecutive measurements by technician A. Reproducibility wasdetermined by comparing the first measurement by technician A with one performed by technician B. Intraobserver andinterobserver intraclass correlation coefficients (ICCs) were calculated. Univariate analysis of covariance (ANCOVA) was usedto compare measured parameters between virgin and post-PRK eyes.
Results: The intraocular pressure (IOP), central corneal thickness (CCT) and 1st applanation time demonstrated goodintraobserver repeatability and interobserver reproducibility (ICC§0.90) in virgin and post-PRK eyes. The deformationamplitude showed a good or close to good repeatability and reproducibility in both groups (ICC§0.88). The CCT correlatedpositively with 1st applanation time (r = 0.437 and 0.483, respectively, p,0.05) and negatively with deformation amplitude(r =20.384 and 20.375, respectively, p,0.05) in both groups. Compared to post-PRK eyes, virgin eyes showed longer 1stapplanation time (7.2960.21 vs. 6.9660.17 ms, p,0.05) and lower deformation amplitude (1.0660.07 vs. 1.1760.08 mm,p,0.05).
Conclusions: CorVis ST demonstrated reliable measurements for CCT, IOP, and 1st applanation time, as well as relativelyreliable measurement for deformation amplitude in both virgin and post-PRK eyes. There were differences in 1st applanationtime and deformation amplitude between virgin and post-PRK eyes, which may reflect corneal biomechanical changesoccurring after the surgery in the latter.
Citation: Chen X, Stojanovic A, Hua Y, Eidet JR, Hu D, et al. (2014) Reliability of Corneal Dynamic Scheimpflug Analyser Measurements in Virgin and Post-PRKEyes. PLoS ONE 9(10): e109577. doi:10.1371/journal.pone.0109577
Editor: Sanjoy Bhattacharya, Bascom Palmer Eye Institute, University of Miami School of Medicine;, United States of America
Received May 21, 2014; Accepted September 3, 2014; Published October 10, 2014
Copyright: � 2014 Chen et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permitsunrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Data Availability: The authors confirm that all data underlying the findings are fully available without restriction. All relevant data are within the paper.
Funding: The authors have no funding or support to report.
Competing Interests: The authors have declared that no competing interests exist.
* Email: [email protected]
Introduction
The cornea is a viscoelastic structure with quantifiable
biomechanical properties [1]. These properties are related to
corneal thickness, age, intraocular pressure (IOP), hydration, and
various pathologies [2–5]. The cornea’s biomechanical behaviour
is mostly dictated by the stroma, which encompasses 90% of the
total corneal thickness and has a greater mechanical stiffness than
the other corneal layers [6].
Corneal biomechanical failure is the basis of keratectatic
diseases [7] such as keratoconus and pellucid marginal degener-
ation. The ability to quantify corneal biomechanical failure
represents an important step towards better understanding and
treatment of keratectatic diseases. In addition, corneal refractive
laser ablation in virgin eyes weakens the cornea mechanically due
to tissue removal, leading to deterioration in corneal biomechan-
ical strength [8]. Biomechanical changes may also affect the
refractive outcome [9]. Moreover, biomechanical weakening after
corneal refractive laser treatment may potentially induce iatro-
genic keratectasia [10]. Therefore, knowledge of corneal biome-
chanical properties is important in predicting clinical outcomes
[11] and in identifying cases with high risk for postoperative
keratectasia after corneal refractive surgery.
Most of the earlier studies concerning corneal biomechanical
properties were performed in vitro [12–14]. The Ocular Response
Analyser (ORA, Reichert, Inc., Depew, NY) was the first device
available to evaluate in vivo corneal biomechanical response to an
air-puff [1]. It employs a quantitative electro-optical system to
monitor the pressures at which the cornea flattens inward and
outward by registering the corneal reflex of infrared light. The
PLOS ONE | www.plosone.org 1 October 2014 | Volume 9 | Issue 10 | e109577

recently introduced ultra-high-speed Scheimpflug video-imaging
device (CorVis ST; Oculus, Wetzlar, Germany) is the first
instrument allowing visualization and measurement of corneal
deformation in response to a standardized air-puff pressure. Data
evaluating the intraobserver repeatability and interobserver
reproducibility of measurements with this relatively new device
are scarce [15,16]. Furthermore, such studies as are available
concern only healthy virgin eyes. The main goal of the present
study was to test the hypothesis that the CorVis ST performs
reliable measurements in both virgin and post-refractive surgery
eyes. To our knowledge, this is the first study to evaluate the
repeatability and reproducibility of CorVis ST measurements in
post-refractive surgery eyes. The secondary purpose was to test the
hypothesis that the measurements can reveal differences in
biomechanical properties between these two groups.
CorVis STThe CorVis ST utilizes an ultraviolet free blue (455 nm
wavelength) light emitting diode (LED) and an ultra-high-speed
(4330 frames per second) Scheimpflug camera to record the
corneal deformation response to a high intensity air impulse. The
air impulse originates from a metered, symmetrical, and fixed
maximal internal pump generating a pressure of 25 kilopascal
[16]. When the eye is aligned and the Scheimpflug image is in
focus, the air puff gets released automatically and the cornea is
imaged during the deformation event. The air pulse (lasting
approximately 20 ms) forces the cornea inwards through
applanation until it achieves its highest concavity (concavity
phase). On its way back, the cornea undergoes a second
applanation before achieving its natural shape.
A total of approximately 140 images of the cornea’s two-
dimensional cross-section are collected. By software tracing of the
anterior and posterior corneal boundaries in individual image
frames, parameters describing the corneal deformation response
are automatically generated by the instrument. The CorVis ST
software version 1.00r30 rev. 771 was used in the current study.
With the Corvis ST the biomechanical response of the cornea is
characterized by three phases: 1st applanation, highest concavity,
and 2nd applanation. In addition to intraocular pressure (IOP) and
central corneal thickness (CCT) values, time (time to reach
applanation), length (the length of the flattened central cornea),
and velocity (the velocity of the corneal apex movement during
applanation) at the moment of both the 1st and 2nd applanation
events are recorded. The following characteristics at the point of
highest concavity are also presented: the highest concavity time,
the deformation amplitude, the distance between bending points
of the cornea (peak distance), and the concave radius of curvature.
(Figure 1.)
Patients and Methods
Forty candidates for laser refractive surgery (virgin-eye group:
28 males and 12 females) and 42 subjects treated for myopia and
astigmatism with photorefractive keratectomy (PRK) earlier (post-
PRK group: 23 males and 19 females) were recruited. The PRK
treatments were performed using topography-guided transepithe-
lial surface ablation with the iRES system (iRES, iVIS Technol-
ogy, Taranto, Italy) at SynsLaser Clinic in Tromsø, Norway,
12.69610.08 months (range: 2 to 48) prior to the current
examination. All participants received an extensive ophthalmic
examination including Placido-based topography (Nidek OPD
Scan II, Nidek Co. Ltd., Aichi, Japan), Scheimpflug topo/
tomography (Precisio, iVIS Technology, Taranto, Italy), slit-lamp
biomicroscopy and tonometry (Icare tonometer, Revenio Group
Corporation, Helsinki, Finland) to exclude corneal and other
ocular pathologies. The Regional Committee for Medical and
Health Research Ethics in Norway approved the study entitled
"2013/762 - Biomechanical cornea measurements by means of
CorVis ST". The research complied with the tenets of the
Declaration of Helsinki and written informed consent was
obtained from each participant before examination. Only the
data from the right eye of each participant was used for the present
study.
The CorVis ST measurements were performed three times by
technician A and one time by technician B. The measurement
sequence between the technicians was randomized using a
randomization table. A one-minute pause was given between
each measurement. Repeatability was evaluated by comparing the
three consecutive measurements performed by technician A.
Reproducibility was determined by comparing the first measure-
ment by technician A with the one performed by technician B.
Mean CorVis ST measured values obtained from the three
measurements by technician A were used to compare the
differences between the virgin and post-PRK eyes groups, as well
as for the correlation analysis.
Statistical AnalysisMedCalc software 11.4.2 (MedCalc Software, Ostend, Belgium)
and SPSS for Mac software (version 19. SPSS, Inc) were used for
statistical analysis. A p-value of less than 0.05 was considered
statistically significant. Descriptive statistical results were expressed
as mean 6 standard deviation (SD). The within-subject standard
deviation (Sw), within-subject coefficient of variation (COV), and
intraclass correlation coefficient (ICC) were determined to assess
the intraobserver repeatability. Interobserver Sw, COV, and ICC
were calculated to assess interobserver reproducibility. Indepen-
dent sample t-test was used to compare the CorVis measured
parameters in virgin and post-PRK eyes groups. For the
parameters that showed significant differences, univariate analysis
of covariance (ANCOVA) was then applied to adjust for selected
covariates (age, CCT measured by the CorVis ST, and mean
simulated keratometry (simK) value measured by OPD Scan II) to
control for potentially confounding factors. Pearson or Spearman
correlations were applied to examine the relationship between
CCT, manifest refraction spherical equivalent (MRSE) and the
deformation parameters.
Results
Patient DemographicsThe mean age of the participants at the time of the examination
was 27.669.0 (range, 18 to 48) and 31.866.7 years (range, 20 to
48) for the virgin-eye and post-PRK groups, respectively. In the
virgin-eye group, the values of central corneal thickness (CCT)
measured by Precisio, IOP measured by Icare rebound tonometer,
and mean simK measured by OPD Scan II were not significantly
different from the preoperative values of the post-PRK group
(Table 1). The mean manifest refraction spherical equivalent
(MRSE) in the virgin-eye and its preoperative value in the post-
PRK groups were 22.1562.28 D and 23.5261.93 D, respec-
tively. In the post-PRK group, the mean maximum ablation depth
was 66.71627.84 mm (range: 18 to 129).
Intraobserver Repeatability and InterobserverReproducibilityTables 2 and 3 present the intraobserver repeatability of the
CorVis ST measurements. In the virgin-eye group, the IOP, CCT,
1st applanation time, and 2nd applanation time demonstrated good
Corneal Dynamic Scheimpflug Analyzerin Virgin and Post-PRK Eyes
PLOS ONE | www.plosone.org 2 October 2014 | Volume 9 | Issue 10 | e109577

repeatability (ICC§0.92), followed by deformation amplitude
(ICC: 0.88), Radius of Curvature (ICC: 0.70), 2nd applanation
velocity (ICC: 0.65), and highest concavity time (ICC: 0.64). The
other parameters showed poor repeatability with large COVs and
low ICCs. In the post-PRK group, the IOP, CCT, 1st applanation
time, and deformation amplitude demonstrated good repeatability
(ICC§0.90), followed by 2nd applanation time (ICC: 0.89), 2ndapplanation velocity (ICC: 0.79), highest concavity time (ICC:
0.66), and radius of curvature (ICC: 0.63). The other parameters
showed poor repeatability with large COVs and low ICCs.
When comparing the interobserver reproducibility of the
CorVis ST parameters, the IOP, CCT, 1st applanation time,
and 2nd applanation time demonstrated good reproducibility
(ICC§0.91), followed by deformation amplitude (ICC: 0.88),
radius of curvature (ICC: 0.64) and 2nd applanation velocity (ICC:
0.59) in the virgin-eye group. In the post-PRK group, the IOP,
CCT, and 1st applanation time demonstrated good reproducibility
(ICC$0.90), followed by deformation amplitude (ICC: 0.88),
radius of curvature (ICC: 0.83), 2nd applanation time (ICC: 0.79),
highest concavity time (ICC: 0.63), 2nd applanation velocity (ICC:
Figure 1. The CorVis ST utilizes the Scheimpflug camera to record the dynamic procedure of the corneal response to an air puff. A)The 1st applanation is achieved. B) The cornea reaches its highest concavity. C) The 2nd applanation is achieved when the cornea rebounds to itsoriginal position from the highest concavity.doi:10.1371/journal.pone.0109577.g001
Table 1. Demographic Data of Participants.
Virgin eyes (n =40) Post-PRK eyes (n =42) p
Age, years 27.969.0 (18, 48) 31.866.9 (20, 48) 0.03
CCT (Precisio), mm 547.82626.78 preop 542.02630.68 postop 485.00640.10 0.30* 0.000*
IOP (Icare), mmHg 15.2062.57 preop 15.8163.29 postop 12.7162.77 0.46* 0.000*
MRSE, D 22.1562.28 preop 23.5261.93 postop 0.0160.48 0.03* 0.000*
Mean simK (OPD Scan II), D 43.4761.38 preop 43.8161.58 postop 40.8761.63 0.18* 0.000*
CCT = central corneal thickness; IOP = intraocular pressure; MRSE = manifest refraction spherical equivalent; simK = simulated karatometry.* p values were adjusted for age-difference.doi:10.1371/journal.pone.0109577.t001
Corneal Dynamic Scheimpflug Analyzerin Virgin and Post-PRK Eyes
PLOS ONE | www.plosone.org 3 October 2014 | Volume 9 | Issue 10 | e109577

0.60), and 2nd applanation length (ICC: 0.52), (Table 4 and 5).
The other parameters showed poor reproducibility.
The IOP, CCT, and 1st applanation time demonstrated good
intraobserver repeatability and interobserver reproducibility in
both groups. The 2nd applanation time had good repeatability and
reproducibility in the virgin eyes, with close to good repeatability
but not good reproducibility in post-PRK eyes. The deformation
amplitude showed a good or close to good repeatability and
reproducibility in both groups.
Comparison of the Measurements between Virgin-Eyeand Post-PRK GroupsDifferences in the CorVis ST measured parameters between the
virgin and post-PRK eyes are listed in Table 6. After adjustment
for age, CCT, and mean simK, the differences in the mean values
of IOP, 1st applanation time, 2nd applanation time, radius of
curvature, and deformation amplitude remained significant.
Compared to the virgin-eye group, the post-PRK group demon-
strated a shorter 1st applanation time, longer 2nd applanation time,
smaller radius of curvature, and larger deformation amplitude.
The CCT demonstrated a confounding effect in the above-
mentioned parameters (p,0.05 in all analyses), while age and
simK did not show statistically significant confounding effects (p.0.05 in all analyses).
Central corneal thickness measured with the CorVis ST
correlated to IOP, 1st applanation time, radius of curvature, and
deformation amplitude (r = 0.439, 0.437, 0.357, and 20.384,
respectively, p,0.05), without significant correlation to other
parameters in the virgin-eye group. In the post-PRK group, it
correlated to IOP, 1st applanation time, 1st applanation velocity, 2ndapplanation length, 2nd applanation velocity, radius of curvature,
and deformation amplitude (r = 0.482, 0.483, 0.401, 0.440, 0.395,
0.583, 20.375, respectively, p,0.05). The MRSE correlated to
IOP, 1st applanation time, and 2nd applanation time, without
significant correlation to other parameters in the virgin-eye group
Table 2. Intraobserver Repeatability of Parameters Obtained by Corvis in Virgin-Eye Group (n = 40).
Parameters Mean ± SD Sw 2.77Sw COV (%) ICC (95%CI)
IOP (mmHg) 14.4661.33 0.59 1.62 3.59 0.93 (0.89,0.96)
CCT (mm) 543.32625.08 5.34 12.56 0.69 0.99 (0.98,0.99)
1st appl. time (ms) 7.2960.21 0.09 0.24 1.09 0.94 (0.90,0.97)
1st appl. length (mm) 1.8360.18 0.29 0.81 13.94 0.10 (20.52,0.49)
1st appl. velocity (m/s) 0.1460.02 0.03 0.08 18.82 0.25 (20.26,0.57)
2nd appl. time (ms) 21.6560.34 0.17 0.48 0.71 0.92 (0.87,0.95)
2nd appl. length (mm) 1.8960.29 0.45 1.24 21.53 0.17 (20.39,0.53)
2nd appl. velocity (m/s) 20.3460.04 0.04 0.10 29.77 0.65 (0.42,0.80)
Highest concavity time (ms) 16.4060.37 0.37 1.02 2.02 0.64 (0.40,0.80)
Peak distance (mm) 4.3660.66 1.17 3.23 21.80 20.04 (20.74,0.41)
Radius of curvature (mm) 7.4960.60 0.55 1.51 6.31 0.70 (0.49,0.83)
Deformation amplitude (mm) 1.0660.07 0.04 0.11 3.34 0.88 (0.81,0.93)
SD = standard deviation, ICC = intraclass correlation coefficient, CI = confidence interval, Sw = within-subject standard deviation, COV = within-subject coefficient ofvariation, IOP = intraocular pressure, CCT = central corneal thickness.doi:10.1371/journal.pone.0109577.t002
Table 3. Intraobserver Repeatability of Parameters Obtained by Corvis in Post-PRK Group (n = 42).
Parameters Mean ± SD Sw 2.77Sw COV (%) ICC (95%CI)
IOP (mmHg) 12.3861.02 0.55 1.52 3.85 0.90 (0.84,0.94)
CCT (mm) 481.18642.45 8.16 22.61 2.29 0.99 (0.98,0.99)
1st appl. time (ms) 6.9660.17 0.09 0.25 1.11 0.91 (0.85,0.95)
1st appl. length (mm) 1.8260.22 0.36 0.99 17.65 0.08 (20.54,0.47)
1st appl. velocity (m/s) 0.1360.02 0.03 0.09 23.30 20.27 (21.14,0.28)
2nd appl. time (ms) 21.9660.31 0.18 0.49 0.69 0.89 (0.81,0.94)
2nd appl. length (mm) 1.7060.39 0.49 1.37 26.01 0.48 (0.12,0.70)
2nd appl. velocity (m/s) 20.4060.06 0.04 0.12 210.35 0.79 (0.65,0.88)
Highest concavity time (ms) 16.4860.35 0.41 1.15 2.12 0.66 (0.43,0.81)
Peak distance (mm) 4.5660.77 1.12 3.10 18.34 0.30 (20.18,0.60)
Radius of curvature (mm) 6.4360.66 0.70 1.94 6.76 0.63 (0.38,0.79)
Deformation amplitude (mm) 1.1760.08 0.04 0.12 3.16 0.92 (0.86,0.95)
SD = standard deviation, ICC = intraclass correlation coefficient, CI = confidence interval, Sw = within-subject standard deviation, COV = within-subject coefficient ofvariation, IOP = intraocular pressure, CCT = central corneal thickness.doi:10.1371/journal.pone.0109577.t003
Corneal Dynamic Scheimpflug Analyzerin Virgin and Post-PRK Eyes
PLOS ONE | www.plosone.org 4 October 2014 | Volume 9 | Issue 10 | e109577

(r =20.485, 20.492, and 0.420, respectively, p,0.05). The
postoperative MRSE was found to correlate only to radius of
curvature in the post-PRK group (r = 0.583, p,0.05).
Discussion
In vitro experiments [12,13] as well as theoretical mathematical
models [17,18] have demonstrated that the cornea exhibits both
elastic and viscoelastic properties. When loaded, the cornea shows
instantaneous deformation (purely elastic behaviour) followed by a
time-dependent deformation response (viscoelastic behaviour)
[19]. The ideal device for measuring corneal biomechanical
properties in vivo should be accurate, provide repeatable and
reproducible results, and be minimally invasive. In the current
study, the intraobserver repeatability and interobserver reproduc-
ibility of CorVis ST measurements in virgin eyes and post-PRK
eyes were investigated.
Similar to the studies performed by Nemeth et al. [16] and Hon
et al. [15], we found that the following parameters had the best
repeatability in both groups: CCT, IOP, 1st applanation time, and
deformation amplitude. The current study also presented good
repeatability for 2nd applanation time. In addition, the ICCs in the
current study were generally higher than in the mentioned studies
for most of the parameters measured. The differences between the
studies may be attributed to different patient populations and
software versions. For example, in the study by Nemeth et al., themean age was 61.24615.72 years (95% CI: 57.62 to 64.86 years),
while the population in the current study was much younger. In
the study by Hon et al., the software did not offer values for radius
of curvature and peak distance. When comparing reproducibility,
Hon et al. found a statistically significant difference in the CCT
measurement between the two sessions. However, the intersession
difference was calculated by comparing the examinations
performed in the morning (9:00–10:99 am) and afternoon (3:99–
5:99 pm) by the same observer. This time difference may have
Table 4. Interobserver Reproducibility of Parameters Obtained by Corvis in Virgin-Eye Group (n = 40).
Parameters Mean Difference ± SD Sw 2.77Sw COV (%) ICC (95%CI)
IOP (mmHg) 20.0160.82 0.58 1.60 3.25 0.92 (0.86,0.96)
CCT (mm) 21.4966.76 4.78 13.24 0.72 0.98 (0.97,0.99)
1st appl. time (ms) 0.0160.12 0.08 0.23 0.96 0.93 (0.88,0.96)
1st appl. length (mm) 20.0260.38 0.27 0.73 11.67 0.29 (20.35(0.63)
1st appl. velocity (m/s) (0.00560.05 0.03 0.09 19.10 0.08 ((0.75(0.51)
2nd appl. time (ms) (0.0160.24 0.17 0.47 0.61 0.91 (0.82(0.95)
2nd appl. length (mm) (0.1060.58 0.44 1.14 17.37 0.12 ((0.65(0.53)
2nd appl. velocity (m/s) (0.0160.06 0.04 0.11 (9.63 0.59 (0.25(0.78)
Highest concavity time (ms) (0.0260.54 0.38 1.06 1.81 0.47 (0.00(0.72)
Peak distance (mm) 0.1161.47 1.04 2.89 13.08 0.06 ((1.45(0.63)
Radius of curvature (mm) 0.0160.81 0.57 1.58 5.01 0.64 (0.31,0.81)
Deformation amplitude (mm) 20.00260.06 0.04 0.11 1.95 0.88 (0.78,0.94)
SD = standard deviation, ICC = intraclass correlation coefficient, CI = confidence interval, Sw = within-subject standard deviation, COV = within-subject coefficient ofvariation, IOP = intraocular pressure, CCT = central corneal thickness.doi:10.1371/journal.pone.0109577.t004
Table 5. Interobserver Reproducibility of Parameters Obtained by Corvis in Post-PRK Group (n = 42).
Parameters Mean Difference ± SD Sw 2.77Sw COV (%) ICC (95%CI)
IOP (mmHg) 20.1760.70 0.50 1.38 2.81 0.90 (0.81,0.95)
CCT (mm) 0.4365.05 3.57 9.89 0.58 1.00 (0.99,1.00)
1st appl. time (ms) 20.0260.11 0.08 0.23 0.84 0.90 (0.82,0.95)
1st appl. length (mm) 0.0860.46 0.32 0.90 14.45 0.27 (20.36,0.60)
1st appl. velocity (m/s) 20.0160.04 0.03 0.09 17.54 0.45 (20.03,0.70)
2nd appl. time (ms) 0.0460.28 0.20 0.55 0.64 0.79 (0.61,0.89)
2nd appl. length (mm) 20.1160.64 0.45 1.25 20.23 0.52 (0.12,0.74)
2nd appl. velocity (m/s) 0.0160.07 0.05 0.15 211.03 0.60 (0.26,0.78)
Highest concavity time (ms) 0.0560.49 0.35 0.97 1.54 0.63 (0.31,0.80)
Peak distance (mm) 0.00161.57 1.11 3.08 15.23 0.26 (20.39,0.61)
Radius of curvature (mm) 20.0660.49 0.35 0.97 4.27 0.83 (0.68,0.91)
Deformation amplitude (mm) 20.0260.15 0.04 0.12 3.89 0.88 (0.78,0.94)
SD = standard deviation, ICC = intraclass correlation coefficient, CI = confidence interval, Sw = within-subject standard deviation, COV = within-subject coefficient ofvariation, IOP = intraocular pressure, CCT = central corneal thickness.doi:10.1371/journal.pone.0109577.t005
Corneal Dynamic Scheimpflug Analyzerin Virgin and Post-PRK Eyes
PLOS ONE | www.plosone.org 5 October 2014 | Volume 9 | Issue 10 | e109577

affected the reproducibility evaluation, as corneal thickness
demonstrates diurnal variation [20]. The other parameters
measured with the CorVis ST did not show satisfactory reliability.
The ICCs varied between the virgin and post-PRK eyes.
It is conceivable that the cornea would be more difficult to
deform and would deform less in eyes with a greater CCT. In line
with other studies [15,21], we revealed a negative correlation
between CCT and deformation amplitude in both groups. In
addition, the CCT correlated positively with 1st applanation time
and radius of curvature in both virgin and post-PRK eyes.
However, correlations between CCT and 1st applanation velocity,
2nd applanation time, length, and velocity were only found in post-
PRK eyes. This may imply that CCT in normal virgin eyes does
not introduce much variation to some of the CorVis ST
parameters, while affecting those measurements in biomechani-
cally compromised corneas. The MRSE in our virgin-eyes group
demonstrated correlation with some of the parameters measured
by CorVis ST. This may need to be taken into consideration if a
database of ‘‘healthy corneas’’ is built for the purpose of identifying
biomechanically weaker corneas.
The IOP measured with the CorVis ST was significantly lower
in the post-PRK eye group compared to the virgin-eye group,
while the historical preoperative data (IOP measured by Icare,
CCT, and corneal curvature) of the post-PRK group showed no
significant difference compared to the respective data in the virgin-
eye group. The CorVis ST measurements in our post-PRK group
were performed a minimum of two months postoperatively, by
which time the patients had discontinued the use of local steroids
for at least three weeks, to exclude a possible pharmacological
effect on their IOP. Some studies have demonstrated that IOP
measured with the CorVis ST is more reliable compared to
Goldmann applanation tonometry (GAT) and Topcon noncontact
tonometry in virgin eyes (Topcon CT-80A Computerized
Tonometer; Topcon, Tokyo, Japan) [22]. Still, in the version of
CorVis ST used in this study, IOP is calculated based on the
timing of the 1st applanation event and is not adjusted for corneal
biomechanical properties. Both CCT and corneal biomechanical
properties can affect IOP measurements, with the latter suggested
to be more influential [18]. The difference in the CorVis ST
measured IOP between the groups was most likely caused by
changes in corneal biomechanical properties and CCT after PRK.
Interestingly, before being adjusted for age, CCT, and simK,
the CorVis ST parameters that demonstrated differences between
the virgin and post-PRK eyes (1st applanation time, 1st applana-
tion velocity, 2nd applanation time, 2nd applanation velocity,
deformation amplitude and radius of curvature) were the same
parameters as those showing differences between normal eyes and
keratoconus eyes in the study conducted by Ali et al. [23]. It seems
that these parameters may be of value in evaluating corneal
biomechanical properties.
The earlier start of the apex indentation (shorter 1st applanation
time) and greater deformation amplitude in post-PRK eyes
indicates a lower resistance to deformation due to a decrease in
corneal stiffness [24,25]. Shen et al. [26] compared corneal
deformation parameters after femtosecond laser small incision
lenticule extraction (SMILE), laser-assisted sub-epithelial kerato-
mileusis (LASEK), and femtosecond laser-assisted LASIK (FS-
LASIK). They found greater deformation amplitude and shorter
1st applanation time in the FS-LASIK group compared to the
LASEK group. However, those parameters did not differ
significantly between the SMILE and LASEK groups, or between
SMILE and FS-LASIK groups. This indicates that corneal
refractive surgery alters the stiffness of the cornea to different
degrees with respect to different surgical approaches.
In the current study the CorVis ST measurements in virgin- and
post-PRK eyes were taken from two groups of unrelated
populations. Pre- and postoperative comparison of the same
population would have been better suited to evaluate the changes
in biomechanical properties caused by the surgery. We attempted
to compensate for this by applying age, CCT, and simK as
covariates to adjust for potential confounding factors. For the sake
of this discussion we also introduced a separate group of 28 eyes of
Table 6. Comparison of The CorVis ST Measurments Between Virgin-Eye and Post-PRK Groups.
Virgin-eye (n =40) post-PRK (n =42) Difference (mean ± SE) p Adjusted p* Adjusted R2
IOP (mmHg) 14.4661.33 12.3861.02 2.0860.26 0.000 0.002 0.520
CCT (mm) 543.32 625.08 485.41639.00 57.9067.28 0.000
1st applanation
Time (ms) 7.2960.21 6.9660.17 0.3360.04 0.000 0.003 0.519
Length (mm) 1.8360.18 1.8160.22 0.0160.04 0.832
Velocity (m/s) 0.1460.02 0.1360.02 0.0160.00 0.010 0.614 0.160
2nd applanation
Time (ms) 21.6560.34 21.9660.31 20.3160.07 0.000 0.032 0.221
Length (mm) 1.8960.29 1.7060.39 0.1960.08 0.013 0.958 0.133
Velocity (m/s) 20.3460.04 20.4060.06 0.0760.01 0.000 0.053 0.372
Highest concavity
Time (ms) 16.4060.37 16.4860.41 20.0760.09 0.374
Peak distance 4.3660.66 4.5660.77 20.2060.16 0.216
Radius (mm) 7.4960.60 6.4360.66 1.0660.14 0.000 0.001 0.551
Deformationamplitude (mm)
1.0660.07 1.1760.08 20.1060.02 0.000 0.005 0.402
SE = standard error, IOP = intraocular pressure, CCT = central corneal thickness.p* values were adjusted for the effect of the age, CCT, mean simK difference between the virgin-eye and post-PRK groups.doi:10.1371/journal.pone.0109577.t006
Corneal Dynamic Scheimpflug Analyzerin Virgin and Post-PRK Eyes
PLOS ONE | www.plosone.org 6 October 2014 | Volume 9 | Issue 10 | e109577

16 patients who underwent PRK for myopic astigmatism (mean
preoperative MRSE: 23.3561.98 D, mean postoperative time
9.2165.09 months) with both pre- and postoperative CorVis ST
measurements. The pre- and postoperative CorVis ST measure-
ments of CCT and IOP in that group [547.53628.89 mm vs.
460.32648.57 mm (p,0.05), and 15.0061.48 mmHg vs.
13.4861.24 mmHg (p,0.001), respectively] were similar to the
differences found in the virgin and post-PRK eyes in the current
study. Comparable similarity was also found for the 1st applana-
tion time [7.3760.23 vs. 7.1460.20 ms (p,0.001)], 2nd applana-
tion time (21.3960.32 vs. 21.5760.25 ms (p,0.05), radius of
curvature [7.7660.83 vs. 6.5560.66 mm (p,0.001)] and defor-
mation amplitude [1.0360.08 vs. 1.1060.08 mm, (p,0.05)]. Still,
a separate study measuring pre- and post-PRK parameters with a
larger population is warranted.
The current study demonstrated that, in addition to measure-
ments of CCT and IOP, the CorVis ST showed relatively good
reliability in measurements of 1st applanation time and deforma-
tion amplitude in both virgin- and post-PRK eyes. The differences
in 1st applanation time and deformation amplitude between virgin
and post-PRK eyes may imply that the CorVis ST’s direct view of
the corneal deformation may offer information that promises to
yield clinically relevant parameters correlated with corneal
biomechanical properties.
Author Contributions
Conceived and designed the experiments: XC AS TPU. Performed the
experiments: DH JW. Analyzed the data: XC YH JRE. Contributed
reagents/materials/analysis tools: XC AS YH JRE. Wrote the paper: XC
AS YH JRE DH JW TPU.
References
1. Dupps WJ Jr (2005) Biomechanical modeling of corneal ectasia. J Refract Surg
21: 186–190.
2. Sullivan-Mee M, Billingsley SC, Patel AD, Halverson KD, Alldredge BR, et al.(2008) Ocular Response Analyzer in subjects with and without glaucoma.
Optometry and Vision Science 85: 463–470.3. del Buey MA, Cristobal JA, Ascaso FJ, Lavilla L, Lanchares E (2009)
Biomechanical properties of the cornea in Fuchs’ corneal dystrophy.Investigative Ophthalmology and Visual Science 50: 3199–3202.
4. Kida T, Liu JHK, Weinreb RN (2008) Effects of aging on corneal biomechanical
properties and their impact on 24-hour measurement of intraocular pressure.American Journal of Ophthalmology 146: 567–572.
5. Ortiz D, Pinero D, Shabayek MH, Arnalich-Montiel F, Alio JL (2007) Cornealbiomechanical properties in normal, post-laser in situ keratomileusis, and
keratoconic eyes. Journal of Cataract and Refractive Surgery 33: 1371–1375.
6. Elsheikh A, Alhasso D, Rama P (2008) Assessment of the epithelium’scontribution to corneal biomechanics. Experimental Eye Research 86: 445–451.
7. Roy AS, Shetty R, Kummelil MK (2013) Keratoconus: a biomechanicalperspective on loss of corneal stiffness. Indian J Ophthalmol 61: 392–393.
8. Guirao A (2005) Theoretical elastic response of the cornea to refractive surgery:risk factors for keratectasia. J Refract Surg 21: 176–185.
9. Roberts C (2005) Biomechanical customization: the next generation of laser
refractive surgery. Journal of Cataract and Refractive Surgery 31: 2–5.10. Klein SR, Epstein RJ, Randleman JB, Stulting RD (2006) Corneal ectasia after
laser in situ keratomileusis in patients without apparent preoperative risk factors.Cornea 25: 388–403.
11. Roy AS, Dupps WJ Jr (2009) Effects of altered corneal stiffness on native and
postoperative LASIK corneal biomechanical behavior: A whole-eye finiteelement analysis. J Refract Surg 25: 875–887.
12. Asejczyk-Widlicka M, Pierscionek BK (2008) The elasticity and rigidity of theouter coats of the eye. Br J Ophthalmol 92: 1415–1418.
13. Boyce BL, Grazier JM, Jones RE, Nguyen TD (2008) Full-field deformation of
bovine cornea under constrained inflation conditions. Biomaterials 29: 3896–3904.
14. Elsheikh A, Brown M, Alhasso D, Rama P, Campanelli M, et al. (2008)Experimental assessment of corneal anisotropy. J Refract Surg 24: 178–187.
15. Hon Y, Lam AK (2013) Corneal deformation measurement using Scheimpflug
noncontact tonometry. Optom Vis Sci 90: e1–8.
16. Nemeth G, Hassan Z, Csutak A, Szalai E, Berta A, et al. (2013) Repeatability of
ocular biomechanical data measurements with a Scheimpflug-based noncontact
device on normal corneas. J Refract Surg 29: 558–563.
17. Glass DH, Roberts CJ, Litsky AS, Weber PA (2008) A viscoelastic biomechanical
model of the cornea describing the effect of viscosity and elasticity on hysteresis.
Investigative Ophthalmology and Visual Science 49: 3919–3926.
18. Liu J, Roberts CJ (2005) Influence of corneal biomechanical properties on
intraocular pressure measurement: quantitative analysis. Journal of Cataract and
Refractive Surgery 31: 146–155.
19. Nash IS, Greene PR, Foster CS (1982) Comparison of mechanical properties of
keratoconus and normal corneas. Experimental Eye Research 35: 413–424.
20. Read SA, Collins MJ (2009) Diurnal variation of corneal shape and thickness.
Optom Vis Sci 86: 170–180.
21. Leung CK, Ye C, Weinreb RN (2013) An ultra-high-speed Scheimpflug camera
for evaluation of corneal deformation response and its impact on IOP
measurement. Investigative Ophthalmology and Visual Science 54: 2885–2892.
22. Reznicek L, Muth D, Kampik A, Neubauer AS, Hirneiss C (2013) Evaluation of
a novel Scheimpflug-based non-contact tonometer in healthy subjects and
patients with ocular hypertension and glaucoma. Br J Ophthalmol 97: 1410–
1414.
23. Ali NQ, Patel DV, McGhee CN (2014) Biomechanical responses of healthy and
keratoconic corneas measured using a non contact Scheimpflug tonometer.
Investigative Ophthalmology and Visual Science.
24. Han Z, Tao C, Zhou D, Sun Y, Zhou C, et al. (2014) Air puff induced corneal
vibrations: theoretical simulations and clinical observations. J Refract Surg 30:
208–213.
25. Kling S, Marcos S (2013) Contributing factors to corneal deformation in air puff
measurements. Investigative Ophthalmology and Visual Science 54: 5078–5085.
26. Shen Y, Chen Z, Knorz MC, Li M, Zhao J, et al. (2014) Comparison of Corneal
Deformation Parameters After SMILE, LASEK, and Femtosecond Laser-
Assisted LASIK. J Refract Surg 30: 310–318.
Corneal Dynamic Scheimpflug Analyzerin Virgin and Post-PRK Eyes
PLOS ONE | www.plosone.org 7 October 2014 | Volume 9 | Issue 10 | e109577




Hindawi Publishing CorporationJournal of OphthalmologyVolume 2012, Article ID 498435, 8 pagesdoi:10.1155/2012/498435
Research Article
Safety and Efficacy of Epithelium-On Corneal CollagenCross-Linking Using a Multifactorial Approach to Achieve ProperStromal Riboflavin Saturation
Aleksandar Stojanovic,1, 2 Xiangjun Chen,2 Nan Jin,3 Ting Zhang,3
Filip Stojanovic,4 Sten Raeder,5, 6 and Tor Paaske Utheim2, 7
1 Department of Ophthalmology, University Hospital of North Norway, Fløyvn. 32, Tromsdalen, 9020 Tromsø, Norway2 SynsLaser Kirurgi, 9008 Tromsø and 0159 Oslo, Norway3 School of Ophthalmology and Optometry and Eye Hospital, Wenzhou Medical College, Zhejiang, Wenzhou 325003, China4 University of Tromsø, 9037 Tromsø, Norway5 Department of Ophthalmology, Stavanger University Hospital, 4011 Stavanger, Norway6 Department of Clinical Medicine, University of Bergen, 5020 Bergen, Norway7 Department of Medical Biochemistry, Oslo University Hospital, 0424 Oslo, Norway
Correspondence should be addressed to Aleksandar Stojanovic, [email protected]
Received 3 February 2012; Accepted 10 June 2012
Academic Editor: Andrew G. Lee
Copyright © 2012 Aleksandar Stojanovic et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Purpose. To evaluate the efficacy and safety of epithelium-on corneal collagen cross-linking (CXL) using a multifactorialapproach to achieve proper stromal riboflavin saturation. Methods. This non-randomized retrospective study comprised 61 eyeswith progressive keratoconus treated with epithelium-on CXL. Chemical epithelial penetration enhancement (benzalkoniumchloride-containing local medication and hypotonic riboflavin solution), mechanical disruption of the superficial epithelium,and prolongation of the riboflavin-induction time until verification of stromal saturation were used before the UVA irradiation.Uncorrected and corrected distance visual acuity (UDVA, CDVA), refraction, corneal topography, and aberrometry were evaluatedat baseline and at 1, 3, 6, and 12 months postoperative. Results. At 12-month, UDVA and CDVA improved significantly. None ofthe eyes lost lines of CDVA, while 27.4% of the eyes gained 2 or more lines. Mean spherical equivalent decreased by 0.74 D, andmean cylindrical reduction was 1.15 D. Irregularity index and asymmetry from Scheimpflug-based topography and Max-K at thelocation of cone from Placido-based topography showed a significant decrease. Higher-order-aberration data demonstrated a slightreduction in odd-order aberrations S 3, 5,7 (P = 0.04). Postoperative pain without other complications was recorded. Conclusion.Epithelium-on CXL with our novel protocol appeared to be safe and effective in the treatment of progressive keratoconus.
1. Introduction
Corneal collagen cross-linking (CXL) is a low-invasive treat-ment aimed to improve biomechanical stability in eyes withkeratectasia [1–3]. A photodynamic reaction induced byphotosensitizing riboflavin and ultraviolet A (UVA) lightcauses an increase of the number of intra- and interfibrillarcovalent bonds and the corneal collagen resistance againstenzymatic degradation [4–6]. Increased stromal biomechan-ical strength and lamellar compaction lead to stabilized
corneal shape and better corneal symmetry, potentiallycausing an improvement in visual function [2, 7–9].
In CXL, riboflavin has a dual function acting both as aphotosensitizer inducing the physical collagen cross-linkingand as an absorber of the UVA irradiation, preventingdamage to deeper ocular structures [10, 11]. Proper cornealstromal saturation with riboflavin is therefore essential inCXL, and without its presence the UVA radiation may causethe collagen fibers to degrade rather than to facilitate cross-linking [12].

2 Journal of Ophthalmology
The “standard CXL protocol” described by Wollensakand colleagues includes removal of the corneal epitheliumin a diameter of 9 mm, followed by saturation of thecorneal stroma using 0.1% isotonic riboflavin solution in20% dextran [13]. This procedure is proved to be effectivein increasing corneal stiffness [13], stabilization of kera-toconus, and in some cases in improving the refractiveand topographic features [14, 15]. Even so, the epithelialremoval may lead to serious complications that includeinfection [16, 17], stromal haze [18], and corneal melting[19] in addition to severe pain and decrease in visionoccurring during the first days after the treatment. Toavoid such complications, Boxer Wachler et al. suggesteda modification of the technique by keeping the epitheliumintact (epithelium-on or transepithelial CXL) [20]. However,finding appropriate means of increasing corneal epithelialpermeability prior to riboflavin application was warrantedas riboflavin has a molecular weight of 338 Da, whereasthe corneal epithelium is impermeable to compounds witha molecular weight greater than 100 Da [21]. Accordingly,various approaches have been tried clinically and in thelaboratory to enhance the epithelial permeability beforethe riboflavin application. Chemical enhancers such asbenzalkonium chloride (BAC), ethylenediaminetetraaceticacid (EDTA), gentamycin, tetracaine, and 20% ethanol [22–25] were used, as well as partial grid-like pattern deepithelial-ization [22], excimer laser superficial epithelial removal [26],and the replacement of the isotonic by hypotonic riboflavinsolution [24, 27]. The results varied between the studies,but the majority of the aforementioned methods lead toincreased epithelial permeability for riboflavin.
In the current study, a multifactorial approach wasutilized to enhance the riboflavin penetration by employ-ing: (1) BAC-containing local medication; (2) hypotonicriboflavin solution without dextran; (3) increased riboflavinsolution concentration; (4) mechanical disruption of thesuperficial epithelium (microabrasions); (5) prolongation ofthe riboflavin-induction time until objective verification ofthe stromal saturation is confirmed. By such an approach,this nonrandomized retrospective study aimed to evaluatethe efficacy and safety of the epithelium-on CXL in treatmentof progressive keratoconus.
2. Patients and Methods
In this retrospective, interventional case series, we reviewedthe medical records of all patients with advanced progressivekeratoconus who had 12-month observation time afterthe epithelium-on CXL treatment using our multifactorialapproach. The treatment was performed at The Eye Depart-ment of the University Hospital North Norway, Tromsø, Nor-way, between September 15, 2009 and September 15, 2010.This study was approved by the regional ethics committeeand adhered to the official ethical regulations for clinicalresearch and the Tenets of the Declaration of Helsinki.Inclusion criteria included (1) documented progression ofkeratoconus during the last 12 months before treatment(increase of astigmatism or myopia by 1.00 D or increase in
average SimK by 1.50 D); (2) minimum corneal thicknessof no less than 400 μm at the thinnest point measuredby ultrasound pachymetry; (3) age ranging from 18 to45 years; (4) Amsler-Krumeich keratoconus classificationstage II to III. Exclusion criteria were: (1) history of herpesvirus keratitis; (2) severe dry eye; (3) concurrent cornealinfections; (4) previous ocular surgery; (5) hard contact lenswear ≤4 weeks before the baseline examination.
Pre- and postoperative assessments consisted of slitlamp biomicroscopy, Scheimpflug-based corneal topo-/tomography (Precisio, iVIS Technology, Taranto, Italy),Placido disk-based topography and wavefront aberrometry(OPD-Scan II, Nidek. Co., Ltd. Aichi, Japan), uncorrected(UDVA) and corrected (CDVA) distance visual acuities(Nidek RT 2100 system, Nidek Co. Ltd., Aichi, Japan),ultrasound pachymetry (Cornea-Gage Plus, Sonogage Inc.,Cleveland, Ohio), tonometry (Icare tonometer, RevenioGroup Corporation, Helsinki, Finland), and patients′ sub-jective evaluation of postoperative pain. The patients wereexamined at 1, 3, 6, and 12 months postoperative.
2.1. Surgical Technique. To reduce the risk for UV exposureof retroiridal eye structures, miosis was induced by applyingtwo drops of pilocarpine 2% (Pilokarpin, Ophtha AS, Nor-way). It was followed by the application of two drops of localanesthetic proparacaine 0.5% (Alcaine, Alcon Norway AS),two drops of local antibiotic gentamycin 0.3% (Garamycin,Schering-Plough AS, Norway) followed by proparacaineagain, one drop every minute for five minutes. All the dropswere preserved by BAC (0.001% for Pilokarpin, 0.005% forGaramycin and 0.01% for Alcaine), aiming to increase theepithelial permeability by chemically disrupting the tightjunction proteins. A round Merocel sponge (Medtronic,Inc., Minneapolis, MN) of 5 mm in diameter was insertedinto the conjunctival sac to provide a depot of riboflavin,and to produce microabrasions of the superficial epitheliallayers caused by friction upon patient’s blinking. Thereafter,two drops of proparacaine and two drops of 0.5% aqueousriboflavin solution without dextran (Vitamin B2; Streuli,Uznach, Switzerland) were applied alternating every 30seconds, until the riboflavin saturation was verified by theslit-lamp inspection of the cornea and by the determinationof the presence of riboflavin flare in the anterior chamber(Figure 1). Under the same examination the staining ofthe epithelial microabrasions was verified. The initial slit-lamp saturation evaluation was performed 25 minutes afterthe first application of riboflavin and repeated every fiveminutes until the saturation was confirmed. During thepremedication and riboflavin induction time the patient wasinstructed to blink normally between eye drop instillationand to remain in a comfortable sitting position. The Merocelsponge was then removed and corneal thickness measuredwith ultrasound pachymetry, at which point the patient wasplaced in supine position. Irrigation with isotonic balancedsalt solution (BSS) was performed before the UVA irradiationin order to avoid the shielding effect of riboflavin coveringthe epithelium. An eyelid speculum was then inserted, and aring-shaped Merocel shield k20-5021 (Katena Products, Inc.
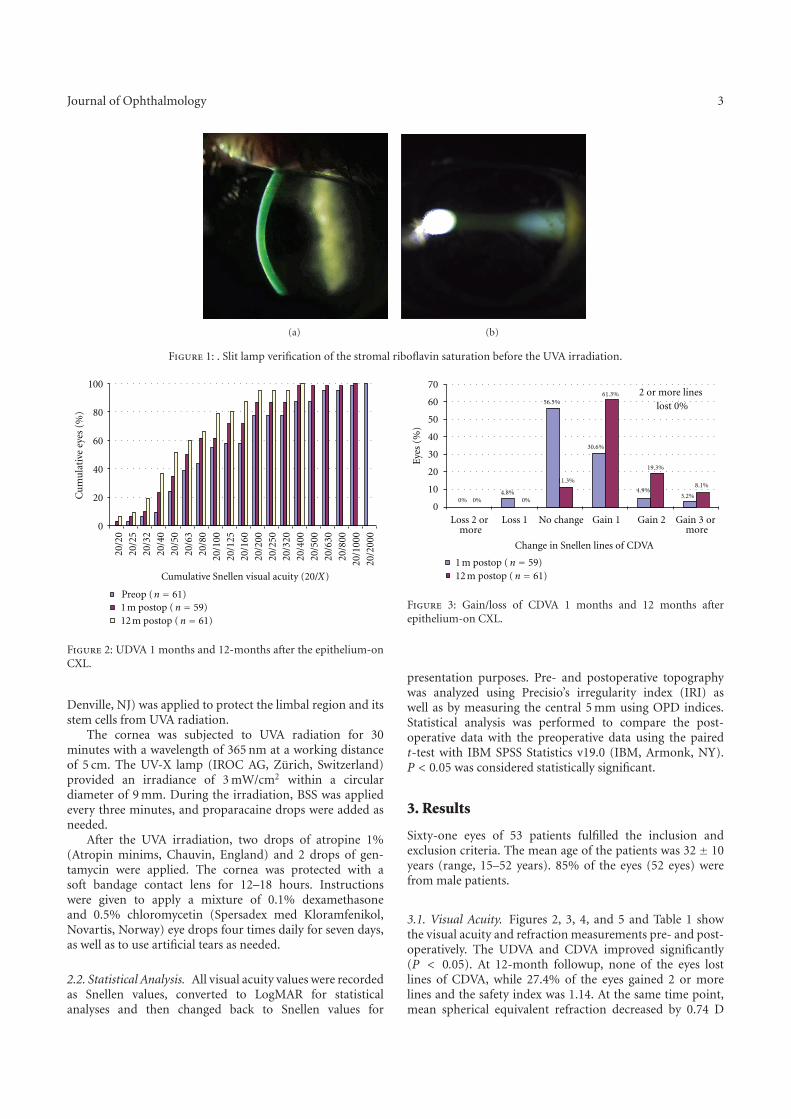
Journal of Ophthalmology 3
(a) (b)
Figure 1: . Slit lamp verification of the stromal riboflavin saturation before the UVA irradiation.
0
20
40
60
80
100
20/2
020
/25
20/3
220
/40
20/5
020
/63
20/8
020
/100
20/1
2520
/160
20/2
000
20/1
000
20/8
0020
/630
20/5
0020
/400
20/3
2020
/250
20/2
00
Cumulative Snellen visual acuity (20/X)
Cu
mu
lati
ve e
yes
(%)
12 m postop (n = 61)1 m postop (n = 59)Preop (n = 61)
Figure 2: UDVA 1 months and 12-months after the epithelium-onCXL.
Denville, NJ) was applied to protect the limbal region and itsstem cells from UVA radiation.
The cornea was subjected to UVA radiation for 30minutes with a wavelength of 365 nm at a working distanceof 5 cm. The UV-X lamp (IROC AG, Zurich, Switzerland)provided an irradiance of 3 mW/cm2 within a circulardiameter of 9 mm. During the irradiation, BSS was appliedevery three minutes, and proparacaine drops were added asneeded.
After the UVA irradiation, two drops of atropine 1%(Atropin minims, Chauvin, England) and 2 drops of gen-tamycin were applied. The cornea was protected with asoft bandage contact lens for 12–18 hours. Instructionswere given to apply a mixture of 0.1% dexamethasoneand 0.5% chloromycetin (Spersadex med Kloramfenikol,Novartis, Norway) eye drops four times daily for seven days,as well as to use artificial tears as needed.
2.2. Statistical Analysis. All visual acuity values were recordedas Snellen values, converted to LogMAR for statisticalanalyses and then changed back to Snellen values for
0
10
20
30
40
50
60
70
No changemore
Loss 2 or Loss 1 Gain 1 Gain 2more
Gain 3 or
Eye
s (%
)
Change in Snellen lines of CDVA
0% 0% 0%4.8%
56.5%
11.3%
30.6%
61.3%
4.9%
19.3%
3.2%
8.1%
2 or more lines lost 0%
12 m postop (n = 61)1 m postop (n = 59)
Figure 3: Gain/loss of CDVA 1 months and 12 months afterepithelium-on CXL.
presentation purposes. Pre- and postoperative topographywas analyzed using Precisio’s irregularity index (IRI) aswell as by measuring the central 5 mm using OPD indices.Statistical analysis was performed to compare the post-operative data with the preoperative data using the pairedt-test with IBM SPSS Statistics v19.0 (IBM, Armonk, NY).P < 0.05 was considered statistically significant.
3. Results
Sixty-one eyes of 53 patients fulfilled the inclusion andexclusion criteria. The mean age of the patients was 32 ± 10years (range, 15–52 years). 85% of the eyes (52 eyes) werefrom male patients.
3.1. Visual Acuity. Figures 2, 3, 4, and 5 and Table 1 showthe visual acuity and refraction measurements pre- and post-operatively. The UDVA and CDVA improved significantly(P < 0.05). At 12-month followup, none of the eyes lostlines of CDVA, while 27.4% of the eyes gained 2 or morelines and the safety index was 1.14. At the same time point,mean spherical equivalent refraction decreased by 0.74 D
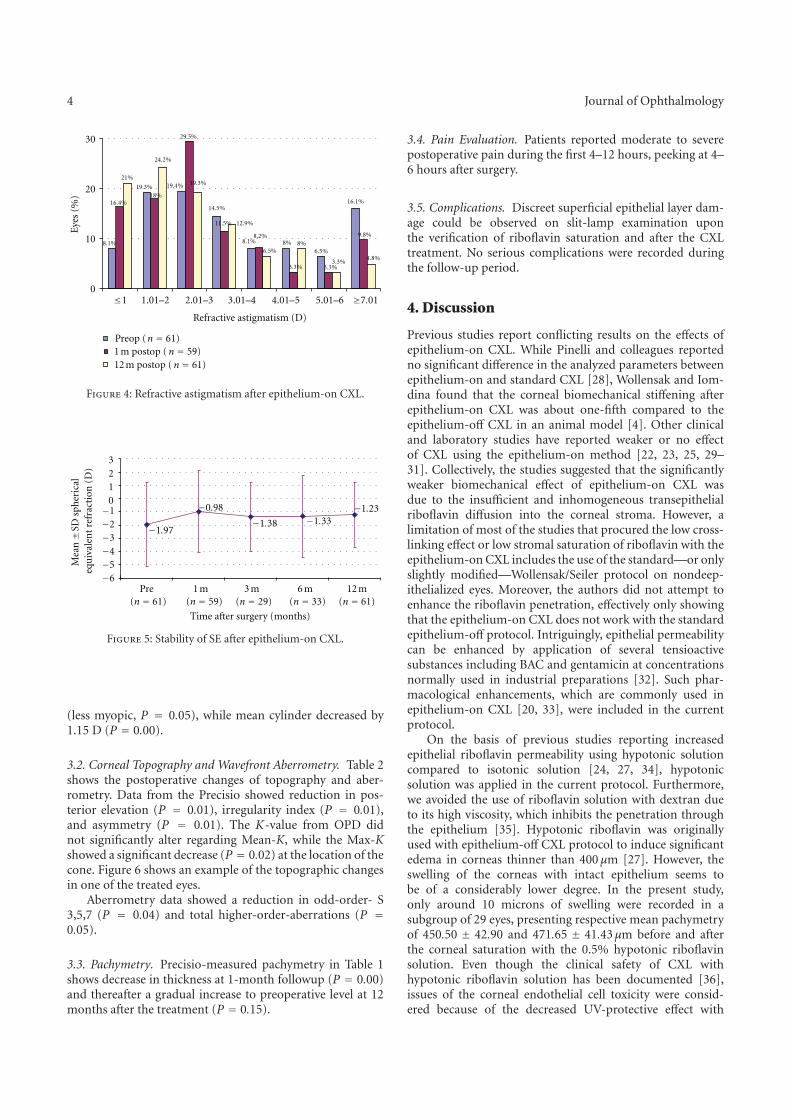
4 Journal of Ophthalmology
0
10
20
30
≤1 5.01–6 4.01–5 3.01–4 2.01–31.01–2 ≥7.01
Refractive astigmatism (D)
8.1%
16.4%
21%
19.3%18%
24.2%
19.4%
29.5%
19.3%
14.5%
11.5% 12.9%
8.1%8.2%
6.5%8%
3.3%
8%6.5%
3.3%3.3%
16.1%
9.8%
4.8%
Eye
s (%
)
12 m postop (n = 61)1 m postop (n = 59)Preop (n = 61)
Figure 4: Refractive astigmatism after epithelium-on CXL.
−6−5−4−3−2−1
0123
Pre(n = 61)
1 m(n = 59)
3 m(n = 29)
6 m(n = 33)
12 m(n = 61)
Mea
n±S
D s
pher
ical
equ
ival
ent
refr
acti
on (
D)
Time after surgery (months)
−1.97
−0.98
−1.38 −1.33−1.23
Figure 5: Stability of SE after epithelium-on CXL.
(less myopic, P = 0.05), while mean cylinder decreased by1.15 D (P = 0.00).
3.2. Corneal Topography and Wavefront Aberrometry. Table 2shows the postoperative changes of topography and aber-rometry. Data from the Precisio showed reduction in pos-terior elevation (P = 0.01), irregularity index (P = 0.01),and asymmetry (P = 0.01). The K-value from OPD didnot significantly alter regarding Mean-K, while the Max-Kshowed a significant decrease (P = 0.02) at the location of thecone. Figure 6 shows an example of the topographic changesin one of the treated eyes.
Aberrometry data showed a reduction in odd-order- S3,5,7 (P = 0.04) and total higher-order-aberrations (P =0.05).
3.3. Pachymetry. Precisio-measured pachymetry in Table 1shows decrease in thickness at 1-month followup (P = 0.00)and thereafter a gradual increase to preoperative level at 12months after the treatment (P = 0.15).
3.4. Pain Evaluation. Patients reported moderate to severepostoperative pain during the first 4–12 hours, peeking at 4–6 hours after surgery.
3.5. Complications. Discreet superficial epithelial layer dam-age could be observed on slit-lamp examination uponthe verification of riboflavin saturation and after the CXLtreatment. No serious complications were recorded duringthe follow-up period.
4. Discussion
Previous studies report conflicting results on the effects ofepithelium-on CXL. While Pinelli and colleagues reportedno significant difference in the analyzed parameters betweenepithelium-on and standard CXL [28], Wollensak and Iom-dina found that the corneal biomechanical stiffening afterepithelium-on CXL was about one-fifth compared to theepithelium-off CXL in an animal model [4]. Other clinicaland laboratory studies have reported weaker or no effectof CXL using the epithelium-on method [22, 23, 25, 29–31]. Collectively, the studies suggested that the significantlyweaker biomechanical effect of epithelium-on CXL wasdue to the insufficient and inhomogeneous transepithelialriboflavin diffusion into the corneal stroma. However, alimitation of most of the studies that procured the low cross-linking effect or low stromal saturation of riboflavin with theepithelium-on CXL includes the use of the standard—or onlyslightly modified—Wollensak/Seiler protocol on nondeep-ithelialized eyes. Moreover, the authors did not attempt toenhance the riboflavin penetration, effectively only showingthat the epithelium-on CXL does not work with the standardepithelium-off protocol. Intriguingly, epithelial permeabilitycan be enhanced by application of several tensioactivesubstances including BAC and gentamicin at concentrationsnormally used in industrial preparations [32]. Such phar-macological enhancements, which are commonly used inepithelium-on CXL [20, 33], were included in the currentprotocol.
On the basis of previous studies reporting increasedepithelial riboflavin permeability using hypotonic solutioncompared to isotonic solution [24, 27, 34], hypotonicsolution was applied in the current protocol. Furthermore,we avoided the use of riboflavin solution with dextran dueto its high viscosity, which inhibits the penetration throughthe epithelium [35]. Hypotonic riboflavin was originallyused with epithelium-off CXL protocol to induce significantedema in corneas thinner than 400 μm [27]. However, theswelling of the corneas with intact epithelium seems tobe of a considerably lower degree. In the present study,only around 10 microns of swelling were recorded in asubgroup of 29 eyes, presenting respective mean pachymetryof 450.50 ± 42.90 and 471.65 ± 41.43μm before and afterthe corneal saturation with the 0.5% hypotonic riboflavinsolution. Even though the clinical safety of CXL withhypotonic riboflavin solution has been documented [36],issues of the corneal endothelial cell toxicity were consid-ered because of the decreased UV-protective effect with

Journal of Ophthalmology 5
Table 1: Visual acuity, refraction, and corneal thickness changes during 1-year followup.
Parameter Preoperative (n = 61)Postoperative
1 Month (n = 59) 3 Months (n = 29) 6 Months (n = 33) 12 Months (n = 61)
VA (Snellen)
UDVA (20/133± 20/57)(20/95± 20/49)
(P = 0.00)(20/87± 20/44)
(P = 0.00)(20/80± 20/48)
(P = 0.00)(20/67± 20/42)
(P = 0.00)
CDVA (20/32± 20/33)(20/29± 20/30)
(P = 0.01)(20/28± 20/31)
(P = 0.00)(20/26± 20/30)
(P = 0.00)(20/24± 20/28)
(P = 0.00)
Refraction (D)
Sphere 0.05± 3.030.64± 3.14(P = 0.12)
0.44± 2.82(P = 0.55)
0.50± 2.92(P = 0.10)
0.21± 2.43(P = 0.61)
SE −1.97± 3.19−0.98± 3.09
(P = 0.00)−1.38± 2.58
(P = 0.03)−1.33± 3.11
(P = 0.01)−1.23± 2.46
(P = 0.05)
Cylinder −4.03± 2.53−3.27± 2.21
(P = 0.00)−3.65± 2.62
(P = 0.01)−3.66± 2.41
(P = 0.00)−2.88± 2.00
(P = 0.00)
CCT (μm) 451± 45425± 58
(P = 0.00;n = 21)436± 45
(P = 0.00;n = 31)441± 58
(P = 0.81;n = 26)460± 47
(P = 0.15;n = 50)
UDVA: uncorrected distance visual acuity; CDVA: corrected distance visual acuity; SE: spherical equivalent; CCT: central corneal thickness.
Table 2: Topographic changes during 1-year followup.
Parameter Preoperative (n = 61) 12 m postoperatively (n = 61)
Precisio
PE (μm) 71.56± 31.31 66.48± 28.81 (P = 0.01)
IRI (μm) 45.45± 22.60 42.18± 22.54 (P = 0.01)
Asym (D) 9.05± 5.50 8.12± 5.58 (P = 0.01)
OPD
Mean K (D) 46.97± 5.21 46.77± 5.31 (P = 0.06)
Max K (D) 55.55± 6.01 54.98± 5.78 (P = 0.02)
DSI 10.54± 5.30 9.71± 5.01 (P = 0.00)
S 3, 5, 7 1.40± 0.80 1.32± 0.80 (P = 0.04)
S 4, 6, 8 0.33± 0.21 0.34± 0.33 (P = 0.81)
Total HOA 4.80± 2.93 4.54± 2.72 (P = 0.05)
PE: posterior elevation; IRI: irregularity index; Asym: asymmetry within 5 mm zone; DSI: differential sector index; HOA: higher order aberration.
hypotonic riboflavin due to the decrease of UV absorptioncoefficient from ≈53 cm−1 for 0.1% isotonic Riboflavinsolution to ≈42 cm−1 for 0.1% hypotonic riboflavin solution[36]. To compensate for this, increasing the concentrationof riboflavin in the hypoosmolar solution may enhanceUVA absorption [37] and hence decrease the UV-radiationat the endothelial level. The current study addresses theendothelial safety as hypotonic riboflavin concentration of0.5% was applied. A secondary benefit of the increasedconcentration is the presumably increased availability of theriboflavin molecules to penetrate the epithelium and saturatethe stroma. In a subgroup analysis of 21 eyes performingpre- and postoperative specular microscopy using KonanCellCheck XL (Konan Medical, Irvine, CA), the endothelialcount decreased insignificantly (P = 0.09) from 2738 ±188 cells/mm2 to 2608± 311 cells/mm2.
The current protocol also employed mechanical scarifi-cation of the epithelial surface by creation of microabrasionscaused by movement of a Merocel sponge over the cornealsurface with patient’s blinking. The amount of such micro-abrasions could obviously not be standardized, and it varied
between cases. This may be the reason for a relativelylarge variation in saturation time (mentioned in the nextparagraph).
Finally, in addition to the chemical and mechanicalenhancements, the current protocol demanded a slit-lampverification of the stromal saturation before the UVAradiation (Figure 1). Our clinical observations showed thatriboflavin saturation was achieved after 25–45 minutes, sothat a commonly used set induction time of, for example, 30minutes would in many cases lead to insufficient riboflavinconcentration in the stroma.
Our visual and refractive outcomes were comparable toother published CXL studies. In the current study therewere no cases with a loss of ≥2 lines of CDVA, endothelialcell count did not change significantly, and there were noinfections or other types of keratitis.
Most of the patients reported pain peaking 4–6 hoursafter the treatment despite the mostly preserved epithelium.This may be explained by actinic-keratoconjunctivitis-likereaction caused by the UV exposure during the treatment
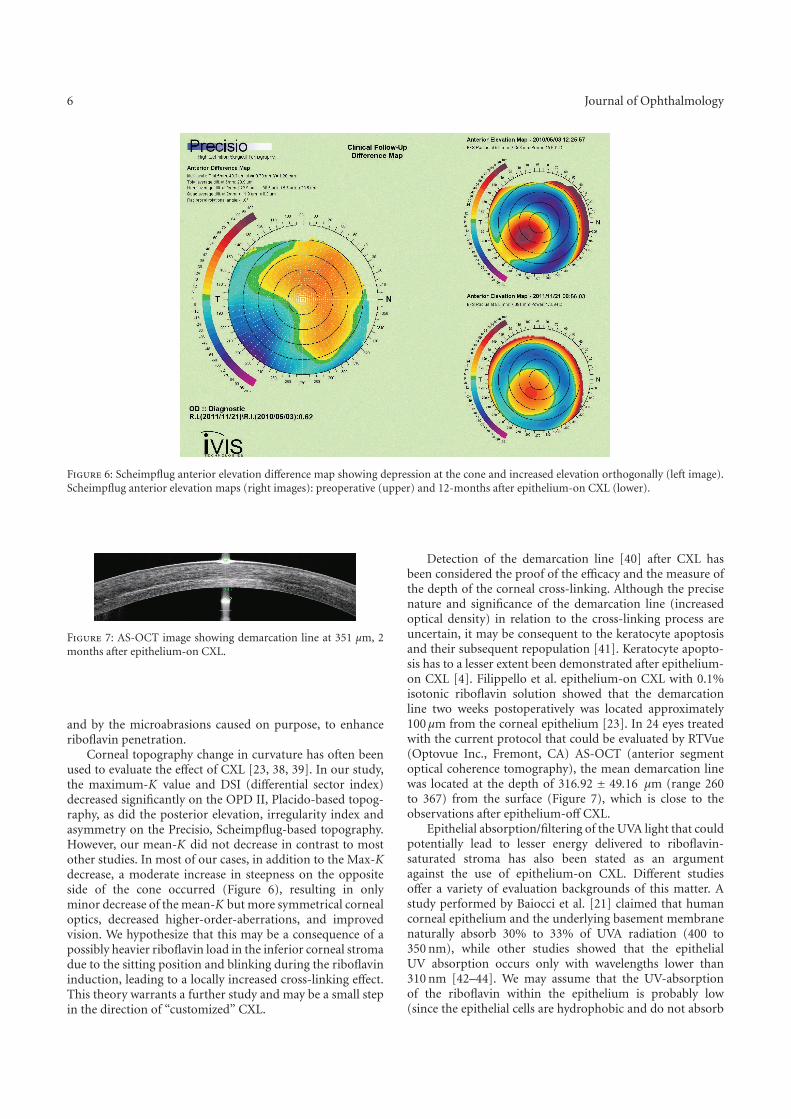
6 Journal of Ophthalmology
Figure 6: Scheimpflug anterior elevation difference map showing depression at the cone and increased elevation orthogonally (left image).Scheimpflug anterior elevation maps (right images): preoperative (upper) and 12-months after epithelium-on CXL (lower).
Figure 7: AS-OCT image showing demarcation line at 351 μm, 2months after epithelium-on CXL.
and by the microabrasions caused on purpose, to enhanceriboflavin penetration.
Corneal topography change in curvature has often beenused to evaluate the effect of CXL [23, 38, 39]. In our study,the maximum-K value and DSI (differential sector index)decreased significantly on the OPD II, Placido-based topog-raphy, as did the posterior elevation, irregularity index andasymmetry on the Precisio, Scheimpflug-based topography.However, our mean-K did not decrease in contrast to mostother studies. In most of our cases, in addition to the Max-Kdecrease, a moderate increase in steepness on the oppositeside of the cone occurred (Figure 6), resulting in onlyminor decrease of the mean-K but more symmetrical cornealoptics, decreased higher-order-aberrations, and improvedvision. We hypothesize that this may be a consequence of apossibly heavier riboflavin load in the inferior corneal stromadue to the sitting position and blinking during the riboflavininduction, leading to a locally increased cross-linking effect.This theory warrants a further study and may be a small stepin the direction of “customized” CXL.
Detection of the demarcation line [40] after CXL hasbeen considered the proof of the efficacy and the measure ofthe depth of the corneal cross-linking. Although the precisenature and significance of the demarcation line (increasedoptical density) in relation to the cross-linking process areuncertain, it may be consequent to the keratocyte apoptosisand their subsequent repopulation [41]. Keratocyte apopto-sis has to a lesser extent been demonstrated after epithelium-on CXL [4]. Filippello et al. epithelium-on CXL with 0.1%isotonic riboflavin solution showed that the demarcationline two weeks postoperatively was located approximately100 μm from the corneal epithelium [23]. In 24 eyes treatedwith the current protocol that could be evaluated by RTVue(Optovue Inc., Fremont, CA) AS-OCT (anterior segmentoptical coherence tomography), the mean demarcation linewas located at the depth of 316.92 ± 49.16 μm (range 260to 367) from the surface (Figure 7), which is close to theobservations after epithelium-off CXL.
Epithelial absorption/filtering of the UVA light that couldpotentially lead to lesser energy delivered to riboflavin-saturated stroma has also been stated as an argumentagainst the use of epithelium-on CXL. Different studiesoffer a variety of evaluation backgrounds of this matter. Astudy performed by Baiocci et al. [21] claimed that humancorneal epithelium and the underlying basement membranenaturally absorb 30% to 33% of UVA radiation (400 to350 nm), while other studies showed that the epithelialUV absorption occurs only with wavelengths lower than310 nm [42–44]. We may assume that the UV-absorptionof the riboflavin within the epithelium is probably low(since the epithelial cells are hydrophobic and do not absorb

Journal of Ophthalmology 7
riboflavin) and that the epithelial interstitial space is ofnegligible volume. The current protocol includes washingoff the riboflavin from the corneal surface before the UVA-radiation in order to minimize the UV-energy loss due to itspossible absorption by the riboflavin.
Finally, even if the epithelium-on CXL leads to ashallower cross-linking compared to the epithelium-off, thedensity of collagen fibers in corneal stroma is much higher inthe anterior portion where most of the collagen cross-linksoccur [40, 45].
5. Conclusion
This retrospective study showed that epithelium-on CXLusing our novel protocol appeared to be effective and safe intreating progressive keratoconus. The improvements in thevisual, refractive, and topographic parameters in our patientsindicate that epithelium-on CXL had sufficient effect to haltthe progression of keratoconus and improve the cornealshape. A randomized controlled trial is warranted to verifythat the effect of the current approach is comparable withthe standard epithelium-off CXL. Furthermore, the combi-nation of different enhancers, osmolality, and concentrationof riboflavin should be explored to further improve theprocedure.
Conflict of Interests
None of the authors has a commercial, proprietary, orfinancial interest in any material or procedure mentioned.
References
[1] L. Spadea, “Collagen crosslinking for ectasia following PRKperformed in excimer laser-assisted keratoplasty for kerato-conus,” European Journal of Ophthalmology, vol. 22, no. 2, pp.274–277, 2012.
[2] C. Mazzotta, A. Balestrazzi, C. Traversi et al., “Treatment ofprogressive keratoconus by riboflavin-UVA-induced cross-linking of corneal collagen: ultrastructural analysis by Hei-delberg Retinal Tomograph II in vivo confocal microscopy inhumans,” Cornea, vol. 26, no. 4, pp. 390–397, 2007.
[3] F. Hafezi, J. Kanellopoulos, R. Wiltfang, and T. Seiler, “Cornealcollagen crosslinking with riboflavin and ultraviolet A to treatinduced keratectasia after laser in situ keratomileusis,” Journalof Cataract & Refractive Surgery, vol. 33, no. 12, pp. 2035–2040,2007.
[4] G. Wollensak and E. Iomdina, “Biomechanical and histo-logical changes after corneal crosslinking with and withoutepithelial debridement,” Journal of Cataract & RefractiveSurgery, vol. 35, no. 3, pp. 540–546, 2009.
[5] G. Wollensak, M. Wilsch, E. Spoerl, and T. Seiler, “Collagenfiber diameter in the rabbit cornea after collagen crosslinkingby riboflavin/UVA,” Cornea, vol. 23, no. 5, pp. 503–507, 2004.
[6] E. Spoerl, G. Wollensak, and T. Seiler, “Increased resistance ofcrosslinked cornea against enzymatic digestion,” Current EyeResearch, vol. 29, no. 1, pp. 35–40, 2004.
[7] C. Mazzotta, C. Traversi, S. Baiocchi et al., “Corneal healingafter riboflavin ultraviolet-A collagen cross-linking deter-mined by confocal laser scanning microscopy in vivo: early and
late modifications,” American Journal of Ophthalmology, vol.146, no. 4, pp. 527–533, 2008.
[8] G. Wollensak and B. Redl, “Gel electrophoretic analysis ofcorneal collagen after photodynamic cross-linking treatment,”Cornea, vol. 27, no. 3, pp. 353–356, 2008.
[9] C. Mazzotta, T. Caporossi, R. Denaro et al., “Morphologicaland functional correlations in riboflavin UV A cornealcollagen cross-linking for keratoconus,” Acta Ophthalmologica,vol. 90, no. 3, pp. 259–265, 2012.
[10] G. Wollensak, E. Spoerl, M. Wilsch, and T. Seiler, “Endothelialcell damage after riboflavin-ultraviolet-A treatment in therabbit,” Journal of Cataract & Refractive Surgery, vol. 29, no.9, pp. 1786–1790, 2003.
[11] E. Spoerl, M. Mrochen, D. Sliney, S. Trokel, and T. Seiler,“Safety of UVA-riboflavin cross-linking of the cornea,” Cornea,vol. 26, no. 4, pp. 385–389, 2007.
[12] M. Ahearne, Y. Yang, K. Y. Then, and K. K. Liu, “Non-destructive mechanical characterisation of UVA/riboflavincrosslinked collagen hydrogels,” The British Journal of Oph-thalmology, vol. 92, no. 2, pp. 268–271, 2008.
[13] G. Wollensak, E. Spoerl, and T. Seiler, “Riboflavin/ultraviolet-A-induced collagen crosslinking for the treatment of kerato-conus,” American Journal of Ophthalmology, vol. 135, no. 5, pp.620–627, 2003.
[14] A. Caporossi, S. Baiocchi, C. Mazzotta, C. Traversi, and T.Caporossi, “Parasurgical therapy for keratoconus byriboflavin-ultraviolet type A rays induced cross-linking ofcorneal collagen: preliminary refractive results in an Italianstudy,” Journal of Cataract & Refractive Surgery, vol. 32, no. 5,pp. 837–845, 2006.
[15] D. S. Grewal, G. S. Brar, R. Jain, V. Sood, M. Singla, and S.P. S. Grewal, “Corneal collagen crosslinking using riboflavinand ultraviolet-A light for keratoconus: one-year analysisusing Scheimpflug imaging,” Journal of Cataract & RefractiveSurgery, vol. 35, no. 3, pp. 425–432, 2009.
[16] K. V. Zamora and J. J. Males, “Polymicrobial keratitis after acollagen cross-linking procedure with postoperative use of acontact lens: a case report,” Cornea, vol. 28, no. 4, pp. 474–476,2009.
[17] J. J. Perez-Santonja, A. Artola, J. Javaloy, J. L. Alio, and J. L.Abad, “Microbial keratitis after corneal collagen crosslinking,”Journal of Cataract & Refractive Surgery, vol. 35, no. 6, pp.1138–1140, 2009.
[18] C. Mazzotta, A. Balestrazzi, S. Baiocchi, C. Traversi, and A.Caporossi, “Stromal haze after combined riboflavin-UVAcorneal collagen cross-linking in keratoconus: in vivo confocalmicroscopic evaluation,” Clinical & Experimental Ophthalmol-ogy, vol. 35, no. 6, pp. 580–582, 2007.
[19] P. Eberwein, C. Auw-Hadrich, F. Birnbaum, P. C. Maier,and T. Reinhard, “Corneal melting after cross-linking anddeep lamellar keratoplasty in a keratokonus patient,” KlinischeMonatsblatter fur Augenheilkunde, vol. 225, no. 1, pp. 96–98,2008.
[20] B. S. Boxer Wachler, R. Pinelli, A. Ertan, and C. C. K.Chan, “Safety and efficacy of transepithelial crosslinking (C3-R/CXL),” Journal of Cataract & Refractive Surgery, vol. 36, no.1, pp. 186–189, 2010.
[21] S. Baiocchi, C. Mazzotta, D. Cerretani, T. Caporossi, and A.Caporossi, “Corneal crosslinking: riboflavin concentration incorneal stroma exposed with and without epithelium,” Journalof Cataract & Refractive Surgery, vol. 35, no. 5, pp. 893–899,2009.
[22] K. Samaras, D. P. O’Brart, J. Doutch, S. Hayes, J. Marshall,and K. M. Meek, “Effect of epithelial retention and removal on

8 Journal of Ophthalmology
riboflavin absorption in porcine corneas,” Journal of RefractiveSurgery, vol. 25, no. 9, pp. 771–775, 2009.
[23] M. Filippello, E. Stagni, and D. O’Brart, “Transepithelialcorneal collagen crosslinking: bilateral study,” Journal ofCataract & Refractive Surgery, vol. 38, no. 2, pp. 283–291, 2012.
[24] A. Kissner, E. Spoerl, R. Jung, K. Spekl, L. E. Pillunat, andF. Raiskup, “Pharmacological modification of the epithelialpermeability by benzalkonium chloride in UVA/Riboflavincorneal collagen cross-linking,” Current Eye Research, vol. 35,no. 8, pp. 715–721, 2010.
[25] S. Hayes, D. P. O’Brart, L. S. Lamdin et al., “Effect of completeepithelial debridement before riboflavin-ultraviolet-A cornealcollagen crosslinking therapy,” Journal of Cataract & RefractiveSurgery, vol. 34, no. 4, pp. 657–661, 2008.
[26] E. F. Bakke, A. Stojanovic, X. Chen, and L. Drolsum, “Penetra-tion of riboflavin and postoperative pain in corneal collagencrosslinking: excimer laser superficial versus mechanical full-thickness epithelial removal,” Journal of Cataract & RefractiveSurgery, vol. 35, no. 8, pp. 1363–1366, 2009.
[27] F. Raiskup and E. Spoerl, “Corneal cross-linking with hypo-osmolar riboflavin solution in thin keratoconic corneas,”American Journal of Ophthalmology, vol. 152, no. 1, pp. 28.e1–32.e1, 2011.
[28] R. Pinelli, M. M. Al Marzouky, and H. I. El-Shawaf,“Tensioactive-mediated transepithelial corneal cross-linking—first laboratory report,” European OphthalmicReview, vol. 3, no. 2, pp. 67–70, 2009.
[29] K. M. Bottos, J. L. Dreyfuss, C. V. S. Regatieri et al.,“Immunofluorescence confocal microscopy of porcinecorneas following collagen cross-linking treatment withriboflavin and ultraviolet A,” Journal of Refractive Surgery, vol.24, no. 7, pp. S715–S719, 2008.
[30] K. E. Samaras and D. B. Lake, “Corneal collagen cross linking(CXL): a review,” International Ophthalmology Clinics, vol. 50,no. 3, pp. 89–100, 2010.
[31] A. Leccisotti and T. Islam, “Transepithelial corneal collagencross-linking in keratoconus,” Journal of Refractive Surgery,vol. 26, no. 12, pp. 942–948, 2010.
[32] S. H. Cha, J. S. Lee, B. S. Oum, and C. D. Kim, “Cornealepithelial cellular dysfunction from benzalkonium chloride(BAC) in vitro,” Clinical & Experimental Ophthalmology, vol.32, no. 2, pp. 180–184, 2004.
[33] B. Boxer Wachler, “Corneal Collagen Crosslinking withRiboflavin. A new treatment to strengthen the cornea forkeratoectasia and keratoconus,” Cataract & Refractive SurgeryToday, vol. 1, pp. 73–74, 2005.
[34] F. Raiskup, R. Pinelli, and E. Spoerl, “Riboflavin osmolar mod-ification for transepithelial corneal cross-linking,” Current EyeResearch, vol. 37, no. 3, pp. 234–238, 2012.
[35] D. L. Meadows, J. R. Paugh, A. Joshi, and J. Mordaunt, “A novelmethod to evaluate residence time in humans using a non-penetrating fluorescent tracer,” Investigative Ophthalmology &Visual Science, vol. 43, no. 4, pp. 1032–1039, 2002.
[36] F. Hafezi, M. Mrochen, H. P. Iseli, and T. Seiler, “Collagencrosslinking with ultraviolet-A and hypoosmolar riboflavinsolution in thin corneas,” Journal of Cataract & RefractiveSurgery, vol. 35, no. 4, pp. 621–624, 2009.
[37] G. Wollensak, H. Aurich, C. Wirbelauer, and S. Sel, “Signifi-cance of the riboflavin film in corneal collagen crosslinking,”Journal of Cataract & Refractive Surgery, vol. 36, no. 1, pp. 114–120, 2010.
[38] D. Asri, D. Touboul, P. Fournie et al., “Corneal collagen cross-linking in progressive keratoconus: multicenter results fromthe French National Reference Center for Keratoconus,”
Journal of Cataract & Refractive Surgery, vol. 37, pp. 2137–2143, 2011.
[39] P. Vinciguerra, E. Albe, S. Trazza et al., “Refractive, topo-graphic, tomographic, and aberrometric analysis of kerato-conic eyes undergoing corneal cross-linking,” Ophthalmology,vol. 116, no. 3, pp. 369–378, 2009.
[40] T. Seiler and F. Hafezi, “Corneal cross-linking-induced stromaldemarcation line,” Cornea, vol. 25, no. 9, pp. 1057–1059, 2006.
[41] G. Wollensak, E. Iomdina, D. D. Dittert, and H. Herbst,“Wound healing in the rabbit cornea after corneal collagencross-linking with riboflavin and UVA,” Cornea, vol. 26, no.5, pp. 600–605, 2007.
[42] L. Kolozsvari, A. Nogradi, B. Hopp, and Z. Bor, “UVabsorbance of the human cornea in the 240- to 400-nm range,”Investigative Ophthalmology & Visual Science, vol. 43, no. 7, pp.2165–2168, 2002.
[43] A. Ringvold, “Corneal epithelium and UV-protection of theeye,” Acta Ophthalmologica Scandinavica, vol. 76, no. 2, pp.149–153, 1998.
[44] A. Podskochy, “Protective role of corneal epithelium againstultraviolet radiation damage,” Acta Ophthalmologica Scandi-navica, vol. 82, no. 6, pp. 714–717, 2004.
[45] G. Wollensak, E. Spoerl, and T. Seiler, “Stress-strain mea-surements of human and porcine corneas after riboflavin-ultraviolet-A-induced cross-linking,” Journal of Cataract &Refractive Surgery, vol. 29, no. 9, pp. 1780–1785, 2003.





























