Embed Size (px)
Citation preview

Malignant tumors of nasopharyngeal epitheliumdiffer clinically depending on the course of diseaseand applied therapy. They are presented in rega-rd to the sex, age, smoking habits, alcohol usageand nutrition factors. Various studies already sho-wed various etiological-causal links with Epstein-Barr virus (EBV). This leads to diversity of vari-
ous morphological and histological types of diseasesbelonging to various classifications. In this work wepresented 60 diagnosed and treated cases with malig-nant tumor of nasopharyngeal epithelium in the Insti-tute for Otorynolaringology and maxillofacial surgeryof Clinical Center of Serbia. All of them were pato-his-tologicaly examined and 24 of them received serologi-cal examination in regard to the concept of associationbetween malignant epithelial tumour and EBV. An im-portant correlation between histopathology and serol-ogy was found. Finally, the terminology used by WHO classification isnot optimal for further histological determination ofnasopharyngeal malignancy; therefore we recommendthe French classification of C. Micheaua.
Key words: malignant, epithelial, tumours, nasopharynx
INTRODUCTION
Morphology of undifferentiated nasopharyngeal carci-noma is characteristic, though there are arguments
on grouping the undifferentiated carcinomas showingloose or "compact, fibrous" configuration as compa-
red to the carcinoma groups of syncytial look of richlymphatic infiltration (UCNT). Other tumours show squa-mous, glandular or neuroendocrine differentiation. Sincethere is great vagueness about the term to be used with re-gard to squamocellular, low differentiated or sometimesunkeratinizing carcinoma, there is also vagueness with re-gard to the implementation of therapy, which, accordingto the most recent understanding, differs greatly for thesetwo types of tumour. The morphological tumour charac-
teristics include also the variants of its stroma and cell in-filtration variants. Differential diagnosis UCNT includesboth benign and malignant lymphoid lesion and any tu-mour with subtle differentiation1. The known histologicaldivisions are in everyday practice in the world, of whichthe most important are the classifying of epypharynx loca-lization neoplasmas, showing new etiopatogenetic entiti-es. The most important classi-fying are WHO classifying2
the French Micheau classi-fying3 and the German classi-fying by Krueger and associates4.
The main drawback of the once very modern WHO cla-ssifying was the difficulty in distinguishing the type 2 tu-mour, id est, the unkeratinizing, the so-called NKC fromthe type 3, id est, the undifferentiated carcinoma of naso-pharyngeal type, that is, UCNT. Shanmugaratnam withhis associates used this classifying on a large number ofNPC in Singapore but failed to find correlation betweenthe histology and distribution of age, sex, HLA antigens,cells immunologic status. Together with his associates, heconcluded at that time: "The three subtypes of tumours,according to the WHO classifying, most probably are thevariant of a very homogeneous group of neoplasmas inSingapore population".
Neel, Pearson and Taylor5 came to similar conclusionsresear-ching correlation of histology and EBV serologyon NPC patients.
The clinical value of histological classifying is basedupon capability to foresee answers to treatment and possi-bility to compare the obtained results. There is reliableevidence that squamocellular carcinoma (SCC) should beclassified separately because of relative radioresistenceand bad prognosis5-7. WHO classifying2 divides these tu-mours into unkeratinizing carcinomas NKC (not showingeither squamous or glandular differentiation) and undiffe-rentiated carcinoma UCNT. This division of undifferenti-ated carcinomas seems not to have therapeutic and prog-nostic significance. The two types of tumour are not final.Some authors pointed to the differences in prognosis be-tween UCNT and compact type, such as WHO classifying
.........................................
New viewpoint to histological classification ofmalignant epithelial tumours of nasopharynx
S. Sto{i}–Divjak1, V Kanjuh2, V. Djuki}1, A. Ra~i}1,
V. Ne{i}1, D. Basari}3
1I nstitute for Otolaringology and Maxillofacial Surgery,Clinical Centre of Serbia, Belgrade2Serbian Academy of Sciences and Arts3Institute for Digestive System Diseases, Clinical Centre ofSerbia, Belgrade
/STRU^NI RAD 616.321-006-091.8
rezi
me

unkeratinizing carcinoma. It seems that better prognosis iswith the first tumour type as compared to the second one8-12.
OBJECTIVE
We wanted to clear up vagueness concerning the recog-nition of histological classifying of nasopharyngeal tu-mours in our surroundings, on the basis of morphologicaldifferences that are in accordance with the clinical and se-rological parameters of our surveyed patients, in compli-ance with the new cognitions in the literature in the world.
MATERIAL AND METHODS
Pathohistological specimens of 60 patients, with malig-nant epithelial nasopharyngeal tumour diagnosed andtreated during the period 1989-1998 in Belgrade, dyed he-matoxylin-eosin (HE) were examined. Simultaneously 24of them were prospectively chosen for serological and his-tological examinations in the Institute Gustave Roussy inParis, where methods of immuno–fluorescent dyeing wasapplied. Serum of the same number of volunteering blooddonors was used as the control group for serological ex-amination. The serum preparations of 24 prospectivelyfollowed up patients, the tumour specimen of which hadbeen examined in Paris, were serologically examined forthe presence of Epstein-Barr virus (EBV) antibodies. Anoriginal method of immuno-fluorescence was used, whichpositivity means detection of two antigen groups of virusEpstein Barr: EA test discovering antibody presence in thepatient’s serum on virus EA (early antigen) as well as testVCA (virus capsid antigen). Test discover, through indi-rect immuno-fluorescence with different titres of the pa-tient serum, the antibodies specific for structural antigensof the viral capsid EB. The most powerful immuno-fluo-rescence, obtained in a series of different serum titres ofthe surveyed patient and behaving as a geometric progres-sion, is taken for statistical processing. Logarithmic valuesof the serum titres are statistically processed by use of themethod of one factor analysis of variance13.
RESULTS
Undifferentiated carcinoma of nasopharingeal type hasreticular architecture (structure), stratified arrangement ofsyncytial luminous cells with vesicular nucleus. Usuallypresent is, more or less shown, lympho–plasmocyte infil-tration.
Tumour more frequently has a reticular than syncytiallook. The walls of the cells are difficult to differentiate(Figure 1). Tumour cells are arranged in irregular and dif-ferently defined masses and bands, which could be seen inthe same tumour. The cells themselves do not producemucin. Pin-like tumour cells with hyperchromatic nucle-uses dominate (Figure 2). When the lymphoid stroma isso thick partially to hide carcinoma cells, there are differ-ential diagnostic difficulties as compared to other malig-nant tumours, primarily the lymphomas, this being thereason in the past to utilize most frequently for this tu-mour the term lymphoepithelioma. Dependent on the den-sity of lymphocyte infiltrates, lymphoepitheliomas could
FIG. 1. PRIMARY NPC. TUMOUR CELLS ARE ARRANGED IN IR-REGULAR AND DIFFERENTLY DEFINED MASSES ANDBONDS WHICH COULD BE SEEN IN THE SAME TUMOUR.THE CELLS THEMSELVES NOT PRODUCE MUCIN. PINK-LIKE TUMOUR CELLS WITH HYPERHROMATIC NUCLE-USES DOMINAT . HE, x80.
FIG. 2. DOMINEERING CARCINOMA FIELD MADE OF SEEM-INGLY SYNCYTIAL LUMINOUS CELLS WITH VESICULARNUCLEUS, UCNT. BORDER TOWARDS LYMPHO–PLASMO-CYTE STROMA RATHER VAGUE. HE, 260.
70 S. Stosic-Divjak et al. ACI Vol. LII

be divided into two subtypes: "Regaud" and "Schminke".Type "Rigaud" possesses little islands of undifferentiatedcells of typical morphologic cohesive groups surroundedby lymphocyte infiltrates. Type "Schminke" shows expli-cit lymphocyte infiltration and could be considered a lym-phoma (Figure 3).
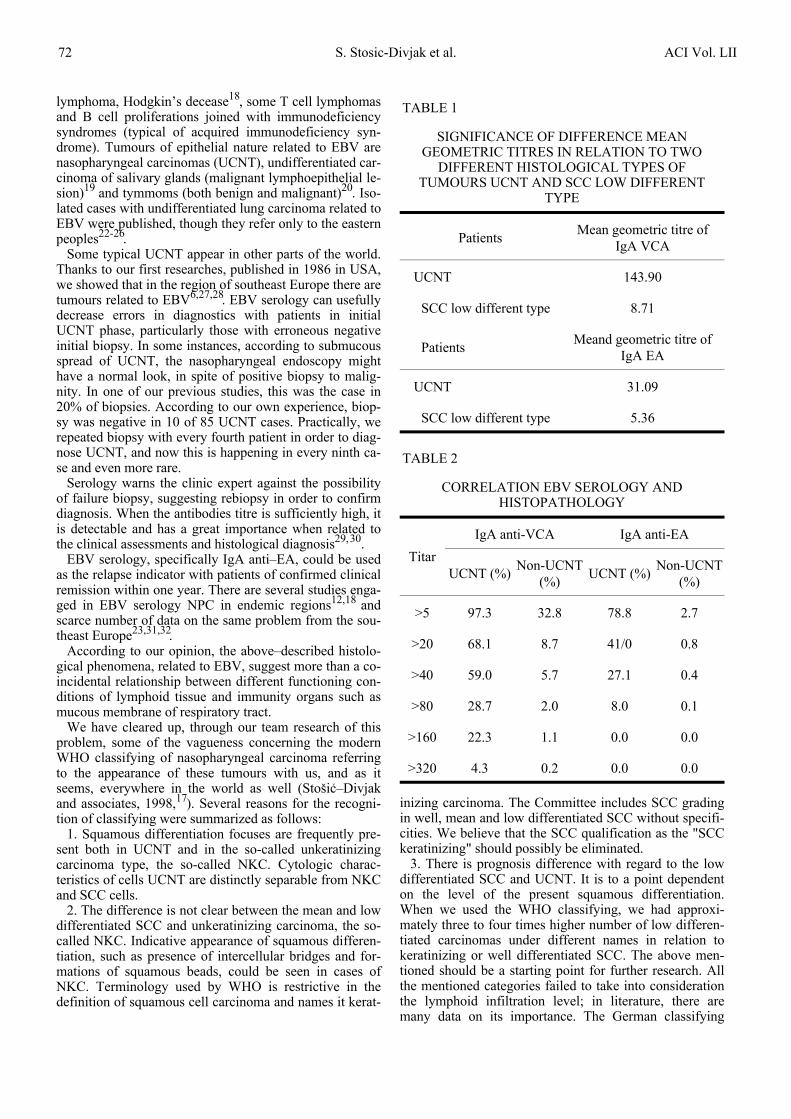
Important diagnostic feature in HE specimen is the iden-tification of cytoplasmatic ties between tumour cells (Fig-ure 4). In prognostic sense, there is no practical significan-ce of making distinction between the two undifferentiatedcarcinomas. The term lymphoepithelium generally is ac-cepted as inadequate as well as that the lymphocyte infil-tration is reactive and not neoplastic. (Table 1)
Titre anti-IgA VCA of antibody considerably is higherin the patient’s serum with UCNT and amounts to 143.9as compared to the patients with squamocellular tumourtype, which could be confused on a light microscope forundifferentiated tumour type, and amounts to 8.71. Statis-tically is highly important that the titre anti EA antibodyfrom the class IgA of a patient with UCNT is higher ascompared to the titre of a patient with SCC lower differ-entiated tumour form. (Table 2)
Correlation of EBV serology with the appearance ofNPC and non-NPC, is shown in the Table 2. While theIgA anti–VCA antibodies were found with 97.3% of NPCpatients, it was found as well with 32.8% of other, non-NPC surveyed patients. They belonged in most cases tonon-neoplastic conditions.
Specificity of serologic testing EBV grows with titre in-crease, while its sensitivity is reduced with titre decrease.Since sensitivity of IgA anti–EA is smaller, and specific-ity of the same antibodies greater as compared to IgAanti–VCA, we obtain in less than 3% of non–NPC patientcases a detectable titre IgA anti–EA. Test efficacy is cal-culated within the term of confident capability correctly todiagnose NPC. Maximum test efficacy is 0.88 for IgAanti–VCA at titre of 40 and amounts to 0.94 for IgA anti–EA at titre of 5.
DISCUSSION
Pathohistological specimens of 60 patients with malig-nant epithelial nasopharyngeal tumour were examined si-multaneously and 24 of them were prospectively chosenfor serological and histological examinations in the Insti-tute Gustave Roussy in Paris, where methods of immuno–fluorescent dyeing was applied.
After examination of 24 patohistological specimens ofNPC patients from different parts of southeastern Europe,it is confirmed that two main groups of malignant epi-thelial tumours exist in nasopharynx: SCC and UCNT3, 14.Patients with squamous cell carcinoma (SCC) had lowanti EBV titres, etiopatogenetically are associated withconsummation of alcohol and tobacco, react much worseto radio and chemotherapy, have lower rates of five yearlife span. The same correlations were obtained in researchmade by the authors Anderson–Anvret, Saltiel–Berdahand Resta when using Micheau’s classifying on two basictumour types SCC and UCNT15-21. According to presentday understanding, numerous tumours are connected withEBV. Encompassed here are lymphomas such as Burkitt
FIG. 3. PRIMARY UCNT, THE SO-CALLED SCHMINKE TYPE. TU-MOUR OF LOOSE ARCHITECTURE, WITH DISPERSIVECELLS IN A DENSE LYMPHOID INFILTRATE NEARLYMASKING THEM. HE, 400.
FIG. 4. PRIMARY UCNT. TUMOUR OF DIFFUSIVE ARCHITEC-TURE CONSISTING OF LUMINOUS CELLS MIXED WITHLYMPHOID ELEMENTS, CONSEQUENTLY REMINDINGVERY MUCH OF NHL. GIEMSA, 400.
Br. 3 New viewpoint to histological classification of malignant 71epithelial tumours of nasopharynx
lymphoma, Hodgkin’s decease18, some T cell lymphomasand B cell proliferations joined with immunodeficiencysyndromes (typical of acquired immunodeficiency syn-drome). Tumours of epithelial nature related to EBV arenasopharyngeal carcinomas (UCNT), undifferentiated car-cinoma of salivary glands (malignant lymphoepithelial le-sion)19 and tymmoms (both benign and malignant)20. Iso-lated cases with undifferentiated lung carcinoma related toEBV were published, though they refer only to the easternpeoples22-26.
Some typical UCNT appear in other parts of the world.Thanks to our first researches, published in 1986 in USA,we showed that in the region of southeast Europe there aretumours related to EBV6,27,28. EBV serology can usefullydecrease errors in diagnostics with patients in initialUCNT phase, particularly those with erroneous negativeinitial biopsy. In some instances, according to submucousspread of UCNT, the nasopharyngeal endoscopy mighthave a normal look, in spite of positive biopsy to malig-nity. In one of our previous studies, this was the case in20% of biopsies. According to our own experience, biop-sy was negative in 10 of 85 UCNT cases. Practically, werepeated biopsy with every fourth patient in order to diag-nose UCNT, and now this is happening in every ninth ca-se and even more rare.
Serology warns the clinic expert against the possibilityof failure biopsy, suggesting rebiopsy in order to confirmdiagnosis. When the antibodies titre is sufficiently high, itis detectable and has a great importance when related tothe clinical assessments and histological diagnosis29, 30.
EBV serology, specifically IgA anti–EA, could be usedas the relapse indicator with patients of confirmed clinicalremission within one year. There are several studies enga-ged in EBV serology NPC in endemic regions12,18 andscarce number of data on the same problem from the sou-theast Europe23,31,32.
According to our opinion, the above–described histolo-gical phenomena, related to EBV, suggest more than a co-incidental relationship between different functioning con-ditions of lymphoid tissue and immunity organs such asmucous membrane of respiratory tract.
We have cleared up, through our team research of thisproblem, some of the vagueness concerning the modernWHO classifying of nasopharyngeal carcinoma referringto the appearance of these tumours with us, and as itseems, everywhere in the world as well (Sto{i}–Divjakand associates, 1998,17). Several reasons for the recogni-tion of classifying were summarized as follows:
1. Squamous differentiation focuses are frequently pre-sent both in UCNT and in the so-called unkeratinizingcarcinoma type, the so-called NKC. Cytologic charac-teristics of cells UCNT are distinctly separable from NKCand SCC cells.
2. The difference is not clear between the mean and lowdifferentiated SCC and unkeratinizing carcinoma, the so-called NKC. Indicative appearance of squamous differen-tiation, such as presence of intercellular bridges and for-mations of squamous beads, could be seen in cases ofNKC. Terminology used by WHO is restrictive in thedefinition of squamous cell carcinoma and names it kerat-
inizing carcinoma. The Committee includes SCC gradingin well, mean and low differentiated SCC without specifi-cities. We believe that the SCC qualification as the "SCCkeratinizing" should possibly be eliminated.
3. There is prognosis difference with regard to the lowdifferentiated SCC and UCNT. It is to a point dependenton the level of the present squamous differentiation.When we used the WHO classifying, we had approxi-mately three to four times higher number of low differen-tiated carcinomas under different names in relation tokeratinizing or well differentiated SCC. The above men-tioned should be a starting point for further research. Allthe mentioned categories failed to take into considerationthe lymphoid infiltration level; in literature, there aremany data on its importance. The German classifying
TABLE 1
SIGNIFICANCE OF DIFFERENCE MEANGEOMETRIC TITRES IN RELATION TO TWO
DIFFERENT HISTOLOGICAL TYPES OFTUMOURS UCNT AND SCC LOW DIFFERENT
TYPE
PatientsMean geometric titre of
IgA VCA
UCNT 143.90
SCC low different type 8.71
PatientsMeand geometric titre of
IgA EA
UCNT 31.09
SCC low different type 5.36
TABLE 2
CORRELATION EBV SEROLOGY ANDHISTOPATHOLOGY
Titar
IgA anti-VCA IgA anti-EA
UCNT (%)Non-UCNT
(%)UCNT (%)
Non-UCNT(%)
>5 97.3 32.8 78.8 2.7
>20 68.1 8.7 41/0 0.8
>40 59.0 5.7 27.1 0.4
>80 28.7 2.0 8.0 0.1
>160 22.3 1.1 0.0 0.0
>320 4.3 0.2 0.0 0.0
72 S. Stosic-Divjak et al. ACI Vol. LII

gives absolutely a great significance to the lymphoid infil-tration level. We have studied it and reached certain con-clusions, but further research is compulsory to be ableclinically to explain it and prognostically to be applied33-37.
UCNT has expression of different cytokeratins, same assome of the lymphoma. Tumour cells react to the most ofthe commercial preparations of anticytokeratin antibodies,such as AEL, PKK 1 or CAM 5.2, while AE 3 is less re-active25. Antibodies against keratin of high molecularweight and its unmanifested antigenic components couldbe used for the study of the squamous differentiation levelof these tumours. Epithelial membrane antigen (EMA) isfrequently positive, while the carcinoma–embryonal anti-gen (CEA) is only sometimes positive. S–100 protein isnegative in tumour cells, though, however, were found S–100 protein–positive dendritic cells38,39, interdigital reti-culum cells and Langerhans’s cells. The common leuco-cytic antigen (LCA) is usually negative in tumour cells,but it is positive in lymphoid and reactive T–cells40-44.
CONCLUSION
Undifferentiated carcinoma of nasopharyngeal type(UCNT) is a carcinoma of syncytial look, id est, of vaguecell walls, of vesicular nucleuses with prominent eosino-phil core and intercellular bridges in less than 10% of tu-mour cells; Well–differentiated SCC carcinoma, wherekeratinization encompasses more than 10% of the tumour;
Mean differentiated SCC carcinoma where keratiniza-tion exists in less than 10% of the tumour surface and in-tercellular bridges are more frequent than 10% of the tu-mour surface; Low differentiated SCC is a carcinoma ofloose structure, id est, of separated cell walls, where kerat-inization and intercellular bridges exist in less than 10 %of the tumour, without evidence of glandular differentia-tion. All the surveyed patients with the UCNT tumour hadsignificantly higher anti EBV titres. From our experiencein biopsy repetitions, particularly in cases of performedEBV serology, UCNT was always confirmed. Our find-ings are in compliance with, that is, they confirm, the so-called, French classifying by C. Micheau.
REZIME
Maligni epitelni tumori nazofarinksa se o~igledno med-jusobno razlikuju klini~ki po toku bolesti zavisno od pri-menjene terapije, zastupljeni su razli~ito u odnosu na: poli uzrast, na navike pu{enja i konzumiranja alkohola; za-tim na navike uzimanja razli~itih namirnica u ishrani.Mnogobrojnim studijama u svetu pokazano je da postojerazli~ite etiolo{ko-kauzalne veze sa infekcijom EpsteinBarr-ovim virusom (EBV) {to direktno za posledicu imamorfolo{ko-histolo{ki razli~ite tipove bolesti koji se svrs-tavaju u razli~ite klasifikacije. U ovom radu je prikazano60 dijagnostikovanih i le~enih bolesnika sa malignimepitelnim tumorom nazofarinksa u Institutu za otorinolar-ingologiju i maksilofacijalnu hirurgiju Klini~kog centraSrbije. Svi ispitanici sa nazofarinksnim karcinomom(NPC) su obradjeni patohistolo{ki, a davdeset~etvoro jeobradjeno i serolo{ki prema konceptu povezanosti malig-
nih epitelnih neoplazmi sa EB. Nadjeno je da postoji zna-~ajna korelacija serologije i histopatologije.
Kona~no, po{to terminologija koju koristi WHO klasifi-kacija nije optimalna za dalja histolo{ka tipiziranja nazo-farinksnih maligniteta, mi preporu~ujemo prihvatljivijuFrancusku klasifikaciju C. Micheaua.
Klju~ne re~i: maligni, epitelijalni, tumor, epifarinks
REFERENCES
1. McGuire LJ, Lee JCK.. The histopathologic diagnosisof nasopharyngeal carcinoma. Ear Nose and Throat Jour-nal. 1990;69(2):229-36.
2. Shanmugaratnam K, Sobin L. Histological Typing ofUpper Respiratory Tract Tumors. In: International Histo-logical Typing of Tumors. Geneva: WHO, 1978;19:32.
3. Micheau C. et al. Practical Value of Classifying NPCinto two major microscopical types. In: Grundman E.,Krueger GRF, Ablashi DV, eds. Nasopharyngeal Carci-noma, Cancer Campaign Vol. 5. Stuttgart: Gustav FisherVerlag, 1981:51.
4. Krueger GRF, Kottaridis SD, Wolf H, Ablashi DV.Histological types of Nasopharyngeal Carcinoma as com-pared to EBV serology. Anticancer Research 1981;1:187-94.
5. Neel HB, Pearson GR, Taylor WE. Antibodies to theEBV in patients with NPC and in comparison group. AmJ Otol Rinol Laryngol 1984;93:477-82.
6. Stosic S, Marinkovic J, Spalajkovic M, Krejovic B,De-The G. Geographical distribution, clinical, pathologi-cal and virological data on NPC in Yugoslavia. In: SecondInternational Symposium EBV and Associated MalignantDisease. Florida 1986., 2
7. Stosic-Divjak S, Krejovic B, De-The G et al. Evalu-ation of different therapeutical approaches in NPC pa-tients in Belgrade. In: Sixth international Symposium onEpstein-Barr Virus and associated Diseases. New York1994:216.
8. Hsu HC, Chen CL, Hsu MM, Lynn TC, Tu SM,Huang SC. Pathology of nasopharyngeal carcinoma. Pro-posal of a new histologic classification correlated withprognosis. Cancer 1987;59:945-51.
9. Vera-Sempere FI, Burgos IS, Bothela MS, Morera S.Immunohistochemical expression of Bcl-2 oncoprotein inEBV associated nasopharyngeal carcinoma correlated tohistological type and survival. Histol Histopathol1997;12(1):9-18.
10. Mills SE, Fechner RE.. "Undifferentiated" neo-plasms of the sinonasal region: Differential diagnosisbased on clinical, light microscopic, immunohistochemi-cal, and ultrastructural features. Sem Diag Oathol1989;6:316-28.
11. Sidagis J, Ueno K, Tokunaga M, Ohyama M, EizuruY. Molecular epidemiology of Epstein-Barr virus (EBV)in EBV-related malignancies. Int J Cancer 1997;72(1):72-6.
12. Yu MC, Garabrant GH, Huang TB, Henderson BE.Occupational and other non-dietary risk factors for naso-pharyngeal carcinoma in Guangzhou, China. Int J Cancer1990;45:1033-9.
Br. 3 New viewpoint to histological classification of malignant 73epithelial tumours of nasopharynx

13. De The G. Indirect imunofluorescent test for detect-ing EBV antibodies: anti VCA and anti EA. Lyon: IARC,1985.
14. De Vathaire F, Sancho-Garnier H, De The et al.Prognostic value of EBV markers in the clinical manage-ment of nasopharyngeal carcinoma (NPC): a multicenterfollow-up study. Int J Cancer 1988:42:176-81.
15. Stosic S. Undifferentiated nasopharyngeal carci-noma in south eastern Europe is also an Epstein-Barr vi-rus associated tumor. Journal of the Balkan Union of On-cology 1998;13(1):77- 80.
16. Sto{i}-Divjak S, Jovanovi} V, Stamenkovi} M, Jeli}S, Krejovi} B. Evaluacija rezultata le~enja bolesnika sakarcinomom nazofarinksne lokalizacije. Medicinska is-tra‘ivanja 1991;24(1-2):35-40.
17. Stosic-Divjak S, Krejovic B, Petrovic et al. Study ofzorubicin and zorubicin-cisplatin efects in EBV associatedcarcinoma of nasopharynx (UCNT) In: 8th InternationalSymposium of Tumor Associated Herpesviruses. Stock-holm 1998:94.
18. Kuo WR, Chang CS, Lee CP et al. Detection of theEBV in tumour tissue and perypheral blood by polym-erase chain reaction in patients with nasopharyngeal carci-noma. Kao-Hsiung-I-Hsueh-Tsa-Chih 1996:12(11):613-8.
19. Vera Sempere FJ, Burgos JS, Botella MS, CordobaJ, Gobernado M. Immunohistochemical expression of theEpstein-Barr virus-encoded latent membrane protein(LMP-1) in paraffin sections of EBV-associated naso-pharyngeal carcinoma in Spanish patients. Eur J Cancer BOral Oncol 1996;32(3):163-8.
20. Pallesen G, Hamilton-Dutoit SJ, Rowe M, Young LS. Expression of Epstein-Barr virus latent gene productsin tumor cells of Hodgkin’s disease. Lancet 1991; 337:320-2.
21. Huang DP, Ng HK, Ho YH, Chan KM. Epsten-Barrvirus associated undifferentiated carcinoma of the parotidgland. Histopathol 1988;13:509-17.
22. Inghirami G, Chilosi M, Knowles DM. Western thy-momas lack Epstein-Barr virus by Southern blottinganalysis and by polymerase chain reaction. Am J Pathol1990;136:1429-36.
23. Nakagawa H, Inomoto T, Rustgi AK. A CACCCbox-like cis-regulatory element of the Epstein-Barr virusED-L2 promoter interacts with a novel transcriptional fac-tor in tissue-specific squamous epithelia. J Biol Chem1997;272(26):1666-8.
24. Sto{i}-Divjak S, Krejovi} B, Stoji~i} G. Mogu}nostkori{}enja anti-EA anti EBV serolo{ke metode u dijag-nostici malignih tumora glave i vrata. In: Tumori glave ivrata i sredinjeg ‘iv~anog sustava. Savremena dostignu}ai stremljenja u dijagnostici i terapiji. JugoslavenskaAkademija znanosti i umjetnosti. Zagreb 1988:58-9.
25. Stosic-Divjak S, Krejovic B, Stojicic G. Report of aYugoslav nasopharyngeal carcinoma group. 14th WorldCongress of Otorhinolarynology Head and Neck Surgery.Madrid 1989:944.
26. Sto{i}-Divjak S. Klini~ki zna~aj odredjivanja titaraantitela na EBV i nekih op{tih imunolo{kih parametara umalignih epitelnih tumora nazofarinksa. Doktorska diser-tacija. Medicinski fakultet, Beograd 1986.
27. Yuen KW, Chew EC, Lee JCK. Studies of lectinbinding to the normal and neoplastic nasopharyngeal epi-thelium. In: Abstract of the 18th International Academy ofPathology. Buenos Aires 1990:13.
28. Weinig B, Hyams V, Heffner D. Nasopharyngealpapillary adenocarcinoma. A clinicopathologic study of alow-grade carcinoma. Am J Surg Pathol 1988;12:946-53.
29. Cooper JS, Scott C, Marcial V et al. The relationshipof nasopharyngeal carcinomas and second independentmalignancies based on the Radiation Therapy. Onsology.Group experience. Cancer 1991;67:1673-7.
30. Pallesen G, Hamilton-Dutoit SJ, Rowe M, YoungLS. Expression of Epstein-Barr virus latent gene productsin tumor cells of Hodgkin’s disease. Lancet 1991; 337:320-2.
31. Borisch Chappuis B, Nezelof C, Muller H, MullerHermelink HK. Different Epstein-Barr virus expression inlymphomas from immunocompromised and immunocom-petent patients. Am J Pathol 1990;136:751-8.
32. Hamilton-Dutoit SJ, Palesen G, Franzmann MB etal. AIDS related lymphoma. Histopathology, immunophe-notype, and association with Epstein-Barr virus as demon-strated by in situ nucleic acid hybridization. Am J Pathol1991;138:149-63.
33. Wolf BC, Martin AW, Neiman R et al. The detec-tion of Epstein-Barr virus in hairy cell leukemia cells byin situ hybridization. Am J Pathol 1990;136:717-23.
34. Stosic-Divjak S, Jelic S, Golubicic I, Pendjer I, Kre-jovic B. The role of markers in Ig A class of antibodies aspossible prognostic factor in nasopharyngeal carcinoma.Zdravstvena zatita Beograd 1997;17(Suppl l):183.
35. Sto{i}-Divjak S, Krejovi} B, Jovanovi} V. Detekcijanuklearne Epstein-Barr virus dezoksiribonukleinske kise-line u pacijenata sa nediferentovanim karcinomom nazo-farinksa. Acta Otorhinolaryngolog Serbica 1995;2:113-7.
36. Sham JST, Wei WI, Kwan WH, Chan CW, ChoiPHK, Choy D. Fibreoptic endoscopic examination and bi-opsy in determining the extent of nasopharyngeal carci-noma. Cancer 1989;64:1838-42.
37. Costello F, Mason BR, Collins RJ, Kearsley JH. Aclinical and flow cytometric analysis of patients with na-sopharyngeal cancer. Cancer 1990;66:1789-95.
38. Buson P, Braham K, Clausse B, Tursz T. Constitu-tive expression of HLA class II antigens on EBV positivemalignant cells from nasopharyngeal carcinoma: possibleinvolvement in T-cell infiltration. Cancer Detect Prev1988;12:363-8.
39. Hsu M.M. Loval infiltration of T-lymphocytesusbsets as a prognostic indicator in patients with naso-pharyngeal carcinoma. Ear Nose Throat J 1990;69:543-7.
40. Herait P, Ganem G, Lipinski M et al. Lymphocytesubsets in tumour of patients with undifferentiated naso-pharyngeal carcinoma: presence of lymphocytes with thephenotype of activated T cells. Br J Cancer 1987;55:135-9.
41. Roth SL, Krueger GF, Bertram G, Sack H. 1990.Carcinoma of the nasopharynx. The significance of lym-phocytic infiltration. Acta Oncol 1990;29:897-901.
74 S. Stosic-Divjak et al. ACI Vol. LII

42. Hsu MM, Hsu HC, Lui LT. Local immune reactionin nasopharyngea carcinoma with special reference to itsprognostic evaluation. Head Neck 1989;11:505-10.
43. Kanjuh V, Kne‘evi} M, Eri} , Ostoji} M, BeleslinB. Conceptions about cancer genetics and immortality ofcancer cells in 2000. Arch Oncol Sremska Kamenica2001;9(Suppl 1):3-4.
44. Micheau C, Boussen H, Klijanienko J, Cvitkovic E,Stosic S, Eshweege F. Bone marrow biopsies in patientswith undifferentiated carcinoma of nasopharyngeal type(UCNT), a report of 56 cases. Cancer 1987;60:2459-64.
Br. 3 New viewpoint to histological classification of malignant 75epithelial tumours of nasopharynx





























