-
In previous chapters we have given many examples of the role
played by the human microbiota in maintaining human health and
well-being. These include influencing tissue development,
controlling the induction and maturation of an effective immune
system, excluding exogenous pathogens, contributing to our
nutritional needs, contributing to our energy requirements and
detoxifying potentially dangerous constituents of our diet. We have
also indicated the downside of having a microbiota—the ability of
some of our symbionts to turn on us and cause disease. Since the
formulation of the germ theory of disease, determining the
involvement of microbes in human disease has been one of the main
driving forces of the science of microbiology. It is not
surprising, therefore, that modern-day microbiologists should also
show a keen interest in the disease potential of our microbial
symbionts. However, we have moved on from the notion that an
infectious disease is a simple equation involving the presence of a
particular organism and the onset of disease. While there are
certainly many examples (Bacillus anthracis, Yersinia pestis,
Mycobacterium tuberculosis) of the ability of highly pathogenic
microbes from the external environment (including other animals) to
cause disease in otherwise healthy individuals, our relationship
with our indigenous microbiota from the point of view of disease is
more complex. Some members of our microbiota, known as pathobionts
(for example N. meningitidis, Strep. pyogenes, Strep. pneumoniae,
H. influenzae, and Staph. aureus), are recognized as having
considerable disease-causing potential, but other species are less
threatening and only cause disease when our defense systems are
compromised in some way. We now find that the idea of labeling
particular species as being commensal, opportunistic, or pathogenic
is less helpful as it is too microbe-centered and fails to give
sufficient weight to the status of the host in determining the
outcome of any host–microbe interaction. Nevertheless, it is useful
to have some assessment of the relative risks of disease posed by
individual symbionts and for this
MICROBIAL COMMUNITY DISRUPTION—A ROLE IN OTHER HUMAN
DISEASES?
10
Text in red signifies a resource with a webpage that is given in
full at the end of the chapter
In this chapter:
• The microbiota–gut–brain axis in health and disease
• Microbiota and behavior
• Microbiota and neurodegenerative diseases
• Microbiota and autism spectrum disorders
• Microbiota and cancer
• Microbiota and diabetes
• Microbiota and rheumatoid arthritis
Copyright Taylor & Francis Group. Do Not Distribute.
-
Chapter 10: Microbial Community Disruption—A Role in Other Human
Diseases?428
purpose, a reasonable approach is to use the classification
system of the American Biological Safety Association which groups
organisms on the basis of their infection risk. Of the bacteria
isolated from humans: 94% belong to Risk Group 1 (defined as having
no or low individual and community risk), which includes microbes
that are unlikely to cause disease in humans; 5% belong to risk
Group 2 (defined as having a moderate risk to individuals and a low
community risk)—this includes microbes that could cause disease in
individuals but are unlikely to spread into the community; and 1%
belong to risk Group 3 (defined as having a high individual risk
but low community risk)—this includes bacteria that could cause
severe or lethal human infections and could be a serious hazard to
health-care workers. None of the human isolates are assigned to
risk group 4—defined as having a high individual risk and community
risk, for which no effective treatment or prophylaxis exists.
However, we are moving away from the idea that a disease is
always caused by individual species and are now aware of diseases
due to microbial consortia (polymicrobial infections). Disease may
also be a consequence of some change in the composition of the
community at a particular body site so that it is no longer in a
state of harmony with its host—the community is said to be
dysbiotic. However, it has to be pointed out that in many cases it
has not yet been established whether the dysbiosis observed at a
body site during the course of a particular disease is a cause or a
consequence of that disease. In many cases all we can really say is
that there is an association between the disease and the observed
dysbiosis. However, correlation does not necessarily equate to
causation. A causative relationship can only be established by
unraveling the mechanisms by which a microbial community shift
results in the pathology characteristic of that disease.
At this moment in time, research into the human microbiota and
its contribution to health and disease is a very exciting field
that is attracting considerable attention from researchers, the
media, and the general public. The availability of relatively cheap
and rapid methods for determining the composition of the various
communities that reside on our bodies has facilitated a large
number of research projects that focus on the possible roles of our
symbionts in a variety of human conditions. In this chapter, we
will examine some of the recent suggestions of such associations.
It must be remembered, however, that many of these claims are based
on only a limited number of investigations involving very small
numbers of individuals. They imply some very exciting
possibilities, but many may turn out to be unsupported by more
extensive investigation.
Is there a microbiota–gut–brain axis?The most recent of these
new ideas suggests an involvement of the gut microbiota in various
conditions related to the functioning of the central nervous system
(CNS). The gut has an extensive neuronal network, known as the
enteric nervous system (ENS), which is so large that it has been
referred to as our second brain. It has long been known that the
CNS and gut influence one another by a variety of neural,
endocrine, nutrient, and immunological signals and this has been
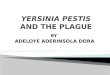
termed the gut–brain axis. What is now being proposed is that this
should be extended to include the gut microbiota so that we have a
microbiota–gut–brain axis (Figure 10.1). The core feature of this
concept is that there is a bi-directional interaction involving
diverse mechanisms.
There are a number of pathways in the microbiota–gut–brain axis
that enable bi-directional communication between the microbiota and
the CNS. Firstly, the microbiota is known to stimulate the release
of various cytokines and chemokines. These not only affect the
composition of the microbiota but can also alter the integrity of
the gut epithelium, interact with the CNS via neuronal receptors
and can enter the systemic circulation where they can induce a
variety of immune responses. Secondly, some members of the
Copyright Taylor & Francis Group. Do Not Distribute.
-
429Does the Gut Microbiota Influence Human Behavior?
microbiota are able to produce neuroactive substances such as
catecholamines, histamine, γ-aminobutyric acid, serotonin, and
SCFAs. These compounds can influence the CNS by interacting with
neuronal receptors in the GIT or in the brain following their
absorption into the bloodstream and crossing the blood–brain
barrier (BBB). Thirdly, the gut microbiota can alter the
permeability of the BBB thereby affecting the uptake of various
immune mediators and microbial metabolites facilitating their
interaction with the brain. Finally, the nerves of the ENS have
been shown to express a number of Toll-like receptors (TLRs),
including TLR2, 3, 4, and 7, which enable direct stimulation of the
CNS by microbes and their components. The CNS can, of course,
affect the GIT in a number of ways. By means of the vagus nerve it
controls the mechanical mixing of food in the stomach, coordinates
muscle contractions to propel food along the rest of the GIT,
maintains the correct environment within different sections of the
gut to enable digestive enzymes to function optimally, and controls
glandular secretion. All of these actions will, of course, affect
the composition of the gut microbiota. In addition, some of the
compounds produced by the CNS such as catecholamines have been
shown to influence bacterial growth and the production of virulence
factors.
Does the gut microbiota influence human behavior?A number of
studies have investigated the possible involvement of the gut
microbiota in the regulation of animal behavior. The behavior of
germ-free animals has been found to differ in several respects from
that of conventionally raised animals and it has also been shown
that restoration of their microbiota, or the administration of
probiotics, can reverse these differences. Furthermore,
administration of probiotics can also affect the behavior of
conventionally raised animals. The results of some of these studies
are summarized in Table 10.1.
Healthystatus
• Normal gutmicrobiota
• Healthy levels ofinflammatory cellsand/or mediators
• Normal brainfunction
Healthy CNSfunction
Healthy gutfunction
Abnormal CNSfunction
Abnormal gutfunction
Increased gutpermability
• Intestinal dysbiosis
• Altered levels of LPS,inflammatory cellsand/or mediators
• Alterations in brainfunction
Figure 10.1. The microbiota–gut–brain axis in health and
disease. (From van Hemert S et al. (2014). Front Neurol 5:241.
doi: 10.3389/fneur.2014.00241. Published under CC BY 4.0.)
Table 10.1. Studies of the effects of the indigenous microbiota
on animal behavior.
TREATMENT BEHAVIORAL EFFECTSAdministration of Bif. breve, Bif.
longum, Lactobacillus helveticus or L. rhamnosus to normal,
conventionally reared mice
Reduced anxiety-like behavior
Colonization of germ-free mice with gut microbiota of normal
mice
Increased exploratory behavior
Administration of Bif. infantis to germ-free rats
Reversed the reduced familiar social recognition observed in the
germ-free animals
Administration of Bif. infantis to germ-free mice
Reversed the increased stress response seen in the germ-free
animals
Re-colonization of germ-free mice with gut microbiota
Reversed the increased social avoidance seen in the germ-free
animals
Copyright Taylor & Francis Group. Do Not Distribute.
-
Chapter 10: Microbial Community Disruption—A Role in Other Human
Diseases?430
A limited number of studies in humans have also reported
probiotic-induced behavioral changes and the results of such
studies are summarized in Table 10.2.
Whether or not the probiotics themselves, or changes (if any)
induced in the gut microbiota by probiotic consumption, were
responsible for the observed behavioral changes remains to be
established. It is important to bear in mind that the number of
studies carried out so far is small and that these have not
involved large numbers of participants.
Does the microbiota play in role in neurodegenerative
diseases?Parkinson’s disease (PD) is the second most common
neurodegenerative disorder of aging, and is projected to affect
nearly 10 million people by 2030. A diagnostic feature of PD is the
presence of neuronal inclusions termed Lewy bodies (Figure 10.2)
which contain aggregates of α-synuclein and these are responsible
for the neurological symptoms of the disease. α-synuclein filaments
may also be deposited in some of the neurites (axons or dendrons)
of the neurons of affected individuals—these are known as Lewy
neurites (see Figure 10.2).
It is thought that the aggregates result from oxidative injury
but the source of this is not known. It has been suggested that the
GIT is a major site and source of oxidative stress in neuronal
tissue because it is the largest interface between neural tissue
and the environment, it has an extensive neuronal network, and this
network is in close proximity to the gut microbiota which contains
products, such as lipopolysaccharide (LPS), capable of inducing
oxidative stress. PD subjects have been shown to have significantly
greater intestinal permeability than controls, have increased
levels of mucosa-associated E. coli (Figure 10.3), and increased
concentrations of LPS-binding protein, which is indicative of
exposure to high levels of LPS. It has been suggested that LPS, a
well-known inducer of pro-inflammatory modulators, stimulates the
enteric immune system to promote local oxidative stress which
results in α-synuclein misfolding, aggregation and subsequent
neuronal damage in the ENS.
Recently, it has also been shown that PD is accompanied by a
dysbiosis of the gut microbiota in which there are elevated
proportions of a number of
Table 10.2. Effects of probiotic administration on human
behavior.
TREATMENTNUMBER AND TYPE OF SUBJECTS BEHAVIORAL EFFECTS
Daily consumption for 30 days of L. helveticus and Bif.
longum
Healthy volunteers; 26 test and 29 controls
Displayed reduced levels of depression and anger–hostility
compared to controls
Daily consumption for 3 weeks of L. helveticus fermented
milk
29 elderly subjects Significant improvement in sleep efficiency
and decreased number of wakening episodes
Daily consumption for 3 weeks of a milk containing L.
casei
Healthy volunteers; 62 test, 62 controls
Improved the mood of those whose mood was initially poor
Daily consumption for 2 months of L. casei
19 test subjects with chronic fatigue syndrome, 16 controls
Significant decrease in anxiety symptoms compared to controls;
significant increase in proportions of Lactobacillus and
Bifidobacterium in feces of test subjects
Daily consumption for 4 weeks of a probiotic containing Bif.
bifidum, Bif. lactis, L. acidophilus, L. brevis, L. casei, L.
salivarius, and L. lactis
Healthy volunteers; 20 test, 20 controls
Reduced aggressive and ruminative thoughts associated with sad
mood
Copyright Taylor & Francis Group. Do Not Distribute.
-
431Does the Microbiota Play in Role in Neurodegenerative
Diseases?
taxa including Ruminococcaceae and Clostridiales incertae sedis
IV but decreased proportions of Prevotellaceae (Figure 10.4). At
least two other studies have also confirmed a decreased proportion
of Prevotellaceae in the gut microbiota.
Alzheimer’s Disease (AD) is an irreversible, progressive brain
disorder that involves the loss of cognitive functions and usually
first appears in those who are over the age of 65 years. It is the
most common cause of dementia among older adults and affects more
than 46 million people worldwide—this is estimated to increase to
131.5 million by 2050. A number of studies have implied a link
between the oral microbiota and AD. Oral bacteria and species
closely related to those found in the oral cavity have been found
at a higher frequency postmortem in the brains of patients with AD
than in those of patients who did not have AD. The most frequently
detected species are various spirochetes belonging to the genus
Treponema—T. denticola, T. pectinovorum (Figure 10.5), T.
vincenti, T. amylovorum, T. maltophilum, T. medium, and T.
socranskii—which are found in elevated proportions in the dysbiotic
subgingival microbiota associated with periodontitis.
Furthermore, epidemiological studies have shown a link between
poor cognitive performance and tooth loss, and tooth loss has been
associated with an increased risk of both dementia and cognitive
decline. However, a confounding factor is that dementia and
cognitive impairment are likely to result in poor oral hygiene
(resulting in eventual tooth loss) in patients suffering from these
conditions, which means that oral dysbiosis could be a consequence,
rather than a cause, of AD. In a longitudinal study of the serum
levels of antibodies against a range of oral bacteria in elderly
individuals, high levels of antibodies to A. naeslundii were found
to be associated with a high risk of AD while high levels of
antibodies to Eub. nodatum were associated with a low risk of AD. A
lower level of Fusobacteriaceae and a
(A) (B)
(C) (D)
Figure 10.2. Photomicrograph of two regions of the midbrain in a
patient with Parkin-son’s disease showing Lewy bodies and Lewy
neurites. The left-hand and right- hand panels are from
different regions of the midbrain. The presence of Lewy
bodies and neurites (red/brown-stained structures) has been
revealed by immunohistochemical staining using monoclonal
antibodies to α-synuclein. Top panels (A and B) show a ×60
magnification of the Lewy bodies. The bottom panels (C and D) are
×20 magnification images that show rounded Lewy bodies of various
sizes as well as Lewy neurites (filamentous structures). (Courtesy
of Suraj Rajan published under CC BY-SA 3.0.)
(A)
(B)
(C)
Figure 10.3. Immunohistochemical staining of intestinal biopsies
for E. coli (brown-staining regions). (A, B) Representative images
from a patient with Parkinson’s disease at magnifica-tions of ×10
and ×40, respectively. (C) A healthy control subject at a
magnification of ×40. Staining intensity is far greater in the case
of the patient with Parkinson’s disease. (From Forsyth CB
et al. (2011). PLOS ONE 6:e28032.
doi:10.1371/journal.pone.0028032. Published under CC BY 4.0.)
Copyright Taylor & Francis Group. Do Not Distribute.
-
Chapter 10: Microbial Community Disruption—A Role in Other Human
Diseases?432
higher level of Prevotellaceae have been reported in the
subgingival plaque of a small group of patients with dementia
compared with healthy controls.
Multiple sclerosis (MS) is a condition that can affect the brain
and/or the spinal cord and results in a wide range of possible
symptoms including fatigue and problems with vision, movement,
sensation, or balance. It is a life-long condition and affects
approximately 2.5 million people worldwide. Animal studies have
suggested a role for the gut microbiota in MS but few studies have
been carried out in humans. MS patients have been found to have
lower levels of Faec. prausinitzii (Figure 10.6) in their feces
compared with healthy controls. Faec. prausinitzii is a well-known
producer of butyrate, which has anti-inflammatory properties, and
the low levels of butyrate in Faecalibacterium-deficient MS
patients may contribute to the condition. Interestingly,
administration of vitamin D, which is frequently used in the
treatment of MS, resulted in increased levels of Faec.
prausinitzii. Another study found that MS patients have high levels
of Meth. smithii in their feces, but low levels of the
butyrate-producing organisms Butyricimonas and Lachnospiraceae. A
number of other studies found a reduction in Bacteroidetes and
Firmicutes in the feces of MS patients and these are important in
the production of butyrate and other SCFAs.
Is the gut microbiota involved in autism
spectrum disorders?Autism spectrum disorders (ASDs) are a
group of conditions characterized by a range of behavioral,
communication, and social disorders. Asperger’s
0 5 10 15 20 25 30 35 40
Prevotellaceae
Lactobacillaceae
Verrucomicrobiaceae
Bradyrhizobiaceae
Clostridiales incertae sedis IV
Ruminococcaceae
Proportion of sequences (%)
ControlPatients
Figure 10.4. Fecal microbiota of 72 patients with Parkinson’s
disease and 72 healthy controls as determined by 16S rRNA gene
sequencing. The figures show the proportions of sequences of those
taxa that showed a significant difference between patients and
controls.
10 µm
Figure 10.5. Section from an 84-year-old female subject with
Alzheimer’s disease showing the presence of Treponema pectinov-orum
(arrows) stained dark blue following immunostaining using
antibodies against the organism. (From Riviere GR et al.
(2002). Oral Microbiol Immunol 17:113–118. Copyright Wiley-VCH
Verlag GmbH & Co. KGaA. Reproduced with permission.)
(A) (B)
Figure 10.6. Faec. prausnitzii. (A) Scanning elec-tron
micrograph showing long bacilli (approxi-mately 2 µm) with rounded
ends and a number of characteristic budlike protrusions from the
cell wall (arrowed). (B) Higher magnification image showing the
budding more clearly. ([B] Reprinted from Miguel S et al. Curr
Opin Microbiol 16:255–261, doi:10.1016/j.mib.2013.06.003, Copyright
2013, with permission from Elsevier.)
Copyright Taylor & Francis Group. Do Not Distribute.
-
433Is the Microbiota Involved in Some Cancers?
syndrome is one well-known example of an ASD. They affect
approximately 1% of the population—males are four times more likely
to be affected than females. Studies of children with ASDs have
found that between 24% and 70% have some disturbance of the GIT
such as diarrhea, constipation, bloating, or abdominal pain. These
findings have prompted researchers to investigate a possible link
between the microbiota of the GIT and ASDs. A number of studies
have shown that the gut microbiota of children with ASDs differs
from that of healthy controls but there is little agreement between
these studies with regard to the nature of the dysbiosis (Table
10.3). A possible confounding factor is that children with
ASDs are often fussy eaters and may not have a balanced diet and
this could also affect the composition of the gut microbiota.
A number of metabolomic studies of children with ASD have been
carried out and these have usually involved determining the
metabolites present in urine or blood. The main findings are:
• ASD children have increased urinary concentrations of tartaric
acid (2, 3-dihydroxybutanedioic acid), d-mannitol, hippurate,
phenyacetylglu-tamine, 3-hydroxybenzoic acid, and
p-hydroxyphenylacetic acid.
• In ASD children there is a decrease in the conversion of
tryptophan to melatonin.
• A number of metabolites associated with tricarboxylic acid
cycle (citric acid, succinic acid, cis-acotinic acid, and
β-hydroxybutyric acid) are altered in ASD patients, suggesting that
mitochondrial dysfunction may be a crucial risk factor for
autism.
Investigations of the possible role of the microbiota in ASDs
are still at a very early stage and the absence of a consensus on
the nature of the dysbiosis accompanying the condition has hindered
progress and makes it difficult to postulate on the underlying
mechanisms involved in the pathology of the condition.
Is the microbiota involved in some cancers?The role of Hel.
pylori in gastric cancer and lymphomas is well established (see
Chapter 9) but a number of studies have found a correlation between
dysbiosis and cancer at other body sites and these are summarized
in Table 10.4.
The cross-sectional nature of the studies summarized in Table
10.4 limits their value and, furthermore, most of them involved
only small numbers of subjects. There is a need for much larger,
longitudinal studies. The evidence for an involvement of the human
microbiota in cancer is strongest in the case of colorectal cancer
although the mechanisms involved have not been elucidated.
Table 10.3. Studies of the fecal microbiota of children with
ASDs.
NATURE OF STUDYOBSERVED DYSBIOSIS IN THE FECAL MICROBIOTA
19 children with ASD and 20 healthy controls
Lower abundance of Prevotella, Coprococcus, and unclassified
Veillonellaceae in ASD subjects
51 children with ASD and 53 healthy controls
No difference between patients and controls
33 children with ASD and 15 healthy controls
Increased proportions of Desulfovibrio, Parabacteroides, and
Bacteroides; decreased proportions of Turicibacter, Clostridium,
Weissella, Anaerofilum, Ruminococcus, Streptococcus, and Dialister
in ASD subjects
13 children with ASD and 8 healthy controls
Increased proportions of Clostridium and Ruminococcus in ASD
subjects
20 children with ASD and 10 healthy controls
Increased proportions of Clostridium, Alistipes, Akkermansia,
Caloramator, and Sarcina; decrease in Prevotella, Eubacterium
siraeum, and Bifidobacterium
Copyright Taylor & Francis Group. Do Not Distribute.
-
Chapter 10: Microbial Community Disruption—A Role in Other Human
Diseases?434
Is the gut microbiota involved in Type I diabetes?Type 1
diabetes mellitus (DM) is a chronic immune-mediated disease
characterized by the loss of insulin-producing β cells in the
pancreas. Insulin is a hormone that controls the concentration of
glucose in the blood and a deficiency results in high blood glucose
levels—hyperglycemia. The disease affects between 20 and 40 million
people worldwide. DM can develop at any age but usually appears
before the age of 40, especially in childhood and is the most
common type of diabetes found in children. Patients with DM must
receive daily injections of insulin.
The few studies that have been carried out to date indicate that
the intestinal microbiota of individuals with DM is different to
that of healthy individuals, and most studies have reported
increased proportions of Bacteroidetes (Table 10.5).
Once again, as in many examples of dysbioses, it remains to be
established whether the observed changes in the composition of the
gut microbiota are a cause or consequence of DM.
Is the gut microbiota involved in Type 2 diabetes?Type 2
diabetes (T2D) is a metabolic disorder in which the pancreas does
not produce sufficient insulin and/or the body’s cells fail to
react to the
Table 10.4. Studies reporting an association between cancer and
dysbiosis.
CONDITION NUMBER OF SUBJECTS INVOLVED MAIN FINDINGSEsophageal
cancer 142 subjects with esophageal squamous dysplasia
and 191 withoutDecreased microbial richness (in terms of the
number of bacterial genera) in the esophageal microbiota of
patients with esophageal squamous dysplasia, which is a precursor
to esophageal squamous cell carcinoma
Pancreatic cancer 10 subjects with pancreatic cancer and 10
healthy controls
Proportions of Neisseria elongata and Strep. mitis were
significantly decreased in the saliva of patients with pancreatic
cancer relative to healthy controls
Lung cancer 8 subjects with lung cancer and 8 healthy controls
Proportions of Granulicatella, Abiotrophia, and Streptococcus in
sputum were increased in patients compared with controls
Colorectal cancer 7 different studies involving 291 patients
with colorectal cancer and 386 healthy controls
High prevalence and levels of Fusobacterium and Porphyromonas,
and lower levels of Ruminococcus in the feces of patients compared
with controls
Breast cancer 48 postmenopausal women with breast cancer and 48
controls
Lower community diversity in the gut microbiota of patients
compared with controls
Table 10.5. Examples of studies comparing the fecal microbiota
of patients with Type I diabetes with that of healthy controls.
STUDY PARTICIPANTS MAIN FINDINGS18 patients and 18 controls •
Reduced abundance of lactate-producing bacteria
and butyrate-producing bacteria in the patients• Decreased
abundance of two dominant
Bifidobacterium species and an increased abundance of
Bacteroides in the patients
21 patients and eight controls • Patients had an increased
abundance of Bacteroides, whereas controls had a higher abundance
of Prevotella
28 patients and 27 controls • Patients had increased microbial
diversity and a reduced fraction of butyrate-producing species
within Clostridium clusters IX and XIVa
16 patients and 16 controls • In patients the Firmicutes to
Bacteroidetes ratio was decreased
• Patients had increased proportions of Clostridium,
Bacteroides, and Veillonella and a decrease in Lactobacillus,
Bifidobacterium, the Blautia coccoides–Eub. rectale group, and
Prevotella
Copyright Taylor & Francis Group. Do Not Distribute.
-
435Are the Oral and Gut Microbiotas Involved in Rheumatoid
Arthritis?
insulin produced. Although there is a genetic predisposition to
T2D, it is caused mainly by obesity and lack of exercise. The
incidence of T2D has more than doubled since 1980, with over 382
million affected individuals worldwide, in conjunction with an
increase in obesity rates and the spread of a Western
lifestyle.
A number of studies have reported an association between T2D and
dysbiosis of the fecal microbiota (Table 10.6).
The results of these and other studies generally agree that in
the fecal microbiota of patients with T2D there is a reduction in
the proportions of members of the Firmicutes (mainly Clostridium,
Eub. rectale, Faec. prausnitzii, Roseburia, and Akkermansia
muciniphila) and an enrichment in the Betaproteobacteria,
Desulfovibrio, and some lactobacilli. Furthermore, the proportions
of Betaproteobacteria positively correlates with blood glucose
levels in patients with T2D. Butyrate, an important metabolite of
many Firmicutes, is known to play a role in regulating human
mitochondrial function, energy generation, glucose metabolism, and
lipid metabolism. Changes in butyrate concentrations in the GIT as
a result of dysbiosis may, therefore, be a contributing factor in
T2D and obesity.
Are the oral and gut microbiotas involved in rheumatoid
arthritis?Rheumatoid arthritis (RA) is a chronic, inflammatory
autoimmune disease that results in painful and swollen
joints—usually in the hands, wrists, and feet. It affects
approximately 1% of the population but over 30% of individuals are
over the age of 65 years. It is characterized by the presence of
specific autoantibodies—rheumatoid factor and anti-citrullinated
protein antibodies (ACPAs). Studies have investigated the possible
involvement of both the gut and oral microbiotas in RA.
The results obtained from studies of the gut microbiota show
little agreement. Some studies have reported an increased diversity
in the fecal microbiota of patients with RA while others found a
decrease in diversity. There are reports of decreased levels of
Bifidobacterium and Bacteroides as well as increased proportions of
Collinsella, Eggerthella, Prev. copri, and Faecalibacterium.
In contrast, there is considerable evidence in support of an
association between RA and dysbiosis of the oral microbiota. The
involvement of the oral microbiota, particularly the microbiota
that is associated with periodontitis, in RA has been studied for
many years. Both periodontitis and RA have several features in
common: they are chronic inflammatory
Table 10.6. Examples of studies comparing the fecal microbiota
of patients with Type 2 diabetes with that
of healthy controls.
PARTICIPANTS MAIN FINDINGS173 patients with T2D and 173 controls
Compared with controls, patients had:
• Moderate degree of dysbiosis• Decrease in the abundance of
some butyrate-producing bacteria• Increase in various opportunistic
pathogens
18 patients with T2D and 18 controls Compared with controls,
patients had:• Lower abundance of Firmicutes• Higher proportion of
Bacteroidetes• Higher proportion of Proteobacteria
53 women with T2D and 43 controls Compared with controls,
patients had:• Increased proportions of L. gasseri, L. salivarius,
L. antri, Lactobacillus oris, Cl. clostridioforme, and
Strep. mutans• Decreased proportions of Clostridium
thermocellum, Clostridium botulinum, and Clostridium
beijerinkii
50 women with T2D and 50 controls Compared with controls,
patients had:• Increased proportions of L. reuteri and other
Lactobacillus spp.• Decreased proportions of Cl. coccoides group,
Atopobium cluster, and Prevotella
Copyright Taylor & Francis Group. Do Not Distribute.
-
Chapter 10: Microbial Community Disruption—A Role in Other Human
Diseases?436
conditions; they are characterized by high levels of cytokines,
matrix-metalloproteinases, neutrophil-derived mediators, and
oxidative stress; and they have a number of contributory factors in
common such as smoking and low socio-economic status. Many studies
have shown that there is a high incidence of periodontitis in
patients with RA. Furthermore, in a recent review and meta-analysis
of 17 studies involving 153,492 participants the authors concluded
that there was a significant association between RA and
periodontitis. There is also evidence that treatment of
periodontitis is accompanied by a reduction in the symptoms of RA.
However, a confounding factor is that patients with arthritis of
the hands and/or wrists have a reduced ability to clean their
teeth properly and this could eventually result in periodontitis,
that is, periodontitis is a consequence, rather than a
cause, of RA.
The etiology of RA involves an autoimmune response to
citrullinated proteins and the presence of antibodies
(anti-citrullinated protein antibodies—ACPAs) is diagnostic of the
condition. Citrullinated proteins result from the action of
peptidyl-arginine-deiminases (PADs) that convert peptidyl-arginine
residues to peptidyl-citrulline on various proteins including
α-enolase, keratin, fibrinogen, fibronectin, collagen, and
vimentin. The loss of tolerance to these new epitopes results in
the production of ACPAs and this auto-immune response results in
the chronic inflammation characteristic of RA. One of the organisms
whose proportions increase during the dysbiosis accompanying
periodontitis is Por. gingivalis (Figure 10.7). This bacterium is
the only species known to produce a PAD and has been shown to
citrullinate fibrinogen, enolase, vimentin, and collagen. There is
also evidence that some of the oral organisms in the dysbiotic
community associated with periodontitis can directly cause damage
to the joints in RA. DNA belonging to a number of bacterial species
has been found in the synovial fluid of patients with RA including
Por. gingivalis, Eub. saburreum, Parvimonas micra (formerly
Peptostreptococcus micros), A. israelii, Selenomonas noxia, P.
acnes, Camp. showae, Tan. forsythia, Cap. sputigena, Lep. buccalis,
and Prev. intermedia.
KEY CONCEPTS• Dysbiosis is associated with a number of human
diseases.
• In many cases it has not been established whether the
dysbiosis associated with a disease is a cause of that disease or a
consequence of it.
BIBLIOGRAPHY
Human microbiota and disease—generalAlthani AA, Marei HE, Hamdi
WS et al. (2016). Human microbiome
and its association with health and diseases. J Cell Physiol
231: 1688–1694.
Boers SA, Jansen R & Hays JP (2016). Suddenly everyone is a
micro-biota specialist. Clin Microbiol Infect 22:581–582.
Bullman S, Meyerson M & Kostic AD (2017). Emerging con cepts
and technologies for the discovery of microorganisms involved in
human disease. Annu Rev Pathol 12:217–244.
Clemente JC, Manasson J, Scher JU (2018). The role of the gut
micro-biome in systemic inflammatory disease. BMJ 360:j5145. doi:
10.1136/bmj.j5145.
El-Jurdi N & Ghannoum MA (2017). The mycobiome: impact on
health and disease states. Microbiol Spectr 5(3). doi:
10.1128/microbiolspec.FUNK-0045-2016.
Gilbert JA, Quinn RA, Debelius J et al. (2016).
Microbiome-wide association studies link dynamic microbial
consortia to disease. Nature 535:94–103.
Limon JJ, Skalski JH, Underhill DM (2017). Commensal fungi in
health and disease. Cell Host Microbe 22:156–165.
Kashyap PC, Chia N, Nelson H et al. (2017). Microbiome at
the fron-tier of personalized medicine. Mayo Clin Proc 92:
1855–1864.
Logan AC, Jacka FN & Prescott SL (2016). Immune-microbiota
inter-actions: dysbiosis as a global health issue. Curr Allergy
Asthma Rep 16:13.
Selber-Hnatiw S, Rukundo B, Ahmadi M et al. (2017). Human
gut microbiota: toward an ecology of disease. Front Microbiol 8:
1265–6.
Weiss GA & Hennet T (2017). Mechanisms and consequences of
intestinal dysbiosis. Cell Mol Life Sci 74:2959–2977.
2 µm
Figure 10.7. Scanning electron micrograph of Por. gingivalis.
(From Zhu Y et al. (2013) PLOS ONE 8: e71727.
doi:10.1371/journal.pone.0071. Published under CC BY 4.0.)
Copyright Taylor & Francis Group. Do Not Distribute.
-
437Bibliography
Wu H, Tremaroli V & Bäckhed F (2015). Linking microbiota to
human diseases: a systems biology perspective. Trends Endocrinol
Metab 26:758–770.
Young VB (2017). The role of the microbiome in human health and
disease: an introduction for clinicians. BMJ 356:j831 doi:
https://doi.org/10.1136/bmj.j831.
Microbiota–gut–brain axisBauer KC, Huus KE & Finlay BB
(2016). Microbes and the mind:
emerging hallmarks of the gut microbiota-brain axis. Cell
Micro-biol 18:632–644.
Bharwani A & Forsythe P (2016). The gut microbiota and the
CNS: an old story with a new beginning. In The Human Microbiota and
Chronic Disease: dysbiosis as a Cause of Human Pathology (Nibali L
& Henderson B eds). John Wiley & Sons, Hoboken, NJ, pp.
409–430.
El Aidy S, Stilling R, Dinan TG & Cryan JF (2016).
Microbiome to brain: unravelling the multidirectional axes of
communication. Adv Exp Med Biol 874:301–336.
Forsythe P, Bienenstock J & Kunze WA (2014). Vagal pathways
for microbiome-brain-gut axis communication. Adv Exp Med Biol
817:115–133.
Fung TC, Olson CA & Hsiao EY (2017). Interactions between
the microbiota, immune and nervous systems in health and disease.
Nat Neurosci 20:145–155.
Lyte M (2013). Microbial endocrinology in the
microbiome-gut-brain axis: how bacterial production and utilization
of neurochemicals influence behavior. PLoS Pathog 9: e1003726.
Sandhu KV, Sherwin E, Schellekens H et al. (2017). Feeding
the microbiota-gut-brain axis: diet, microbiome, and
neuropsychi-atry. Transl Res 179:223–244.
Sherwin E, Rea K, Dinan TG & Cryan JF (2016). A gut
(microbiome) feeling about the brain. Curr Opin Gastroenterol
32:96–102.
Tillisch K & Labus JS (2014). Neuroimaging the
microbiome-gut-brain axis. Adv Exp Med Biol 817:405–416.
van de Wouw M, Schellekens H, Dinan TG & Cryan JF (2017).
Microbiota- gut-brain axis: modulator of host metabolism and
appetite. J Nutr 147:727–745.
Westfall S, Lomis N, Kahouli I et al. (2017). Microbiome,
probiotics and neurodegenerative diseases: deciphering the gut
brain axis. Cell Mol Life Sci 74:3769–3787.
Wiley NC, Dinan TG, Ross RP et al. (2017). The
microbiota-gut-brain axis as a key regulator of neural function and
the stress response: implications for human and animal health. J
Anim Sci 95:3225–3246.
Microbiota and behaviorClarke G, O’Mahony SM, Dinan TG &
Cryan JF (2014). Priming for
health: gut microbiota acquired in early life regulates
physi-ology, brain and behaviour. Acta Paediatr 103: 812–819.
Dinan TG & Cryan JF (2015). The impact of gut microbiota on
brain and behaviour: implications for psychiatry. Curr Opin Clin
Nutr Metab Care 18:552–528.
Dinan TG & Cryan JF (2016). Mood by microbe: towards
clinical translation. Genome Med 8:36.
Farmer AD, Randall HA & Aziz Q (2014). It’s a gut feeling:
how the gut microbiota affects the state of mind. J Physiol
592: 2981–2988.
Flowers SA & Ellingrod VL (2015). The microbiome in mental
health: Potential contribution of gut microbiota in disease and
pharmacotherapy management. Pharmacotherapy 35:910–916.
Karakuła-Juchnowicz H, Pankowicz H, Juchnowicz D et al.
(2017). Intestinal microbiota—a key to understanding the
pathophysi-ology of anorexia nervosa? Psychiatr Pol 51:859–870.
Panduro A, Rivera-Iñiguez I, Sepulveda-Villegas M et al.
(2017). Genes, emotions and gut microbiota: the next frontier for
the gastroenterologist. World J Gastroenterol 23:3030–3042.
Parashar A & Udayabanu M (2016). Gut microbiota regulates
key modulators of social behavior. Eur Neuropsychopharmacol
26:78–91.
Rea K, Dinan TG & Cryan JF (2016). The microbiome: a key
regulator of stress and neuroinflammation. Neurobiol Stress
4:23–33.
Temko JE, Bouhlal S, Farokhnia M et al. (2017). The
microbiota, the gut and the brain in eating and alcohol use
disorders: a ’ménage à trois’? Alcohol Alcohol
52:403–413.
Vuong HE, Yano JM, Fung TC et al. (2017). The Microbiome
and Host Behavior. Annu Rev Neurosci 40:21–49.
Microbiota and neurodegenerative diseasesAlam MZ, Alam Q, Kamal
MA et al. (2014). A possible link of gut
microbiota alteration in type 2 diabetes and Alzheimer’s disease
pathogenicity: an update. CNS Neurol Disord Drug Targets 13:
383–390.
Alkasir R, Li J, Li X et al. (2017). Human gut microbiota:
the links with dementia development. Protein Cell 8:90–102.
Budhram A, Parvathy S, Kremenchutzky M & Silverman M (2017).
Breaking down the gut microbiome composition in multiple sclerosis.
Mult Scler 23:628–636.
Catanzaro R, Anzalone M, Calabrese F et al. (2015). The gut
micro-biota and its correlations with the central nervous system
disorders. Panminerva Med 57:127–143.
Friedland RP (2015). Mechanisms of molecular mimicry involving
the microbiota in neurodegeneration. J Alzheimers Dis
45:349–362.
Jiang C, Li G, Huang P et al. (2017). The gut microbiota
and alzheim-er’s disease. J Alzheimers Dis 58:1–15.
Joscelyn J & Kasper LH (2014). Digesting the emerging role
for the gut microbiome in central nervous system demyelination.
Mult Scler 20:1553–1559.
Marizzoni M, Provasi S, Cattaneo A et al. (2017).
Microbiota and neurodegenerative diseases. Curr Opin Neurol
30:630–638.
Mulak A & Bonaz B (2015). Brain-gut-microbiota axis in
Parkinson’s disease. World J Gastroenterol 21:10609–10620.
Parashar A & Udayabanu M (2017). Gut microbiota:
Implications in Parkinson’s disease. Parkinsonism Relat Disord
38:1–7.
Quigley EMM (2017). Microbiota-brain-gut axis and
neurodegen-erative diseases. Curr Neurol Neurosci Rep 17:94. doi:
10.1007/s11910-017-0802-6.
Scheperjans F (2016). Can microbiota research change our
under-standing of neurodegenerative diseases? Neurodegener Dis
Manag 6:81–85.
Scheperjans F, Pekkonen E, Kaakkola S & Auvinen P (2015).
Linking smoking, coffee, urate, and Parkinson’s disease—a role for
gut microbiota? J Parkinsons Dis 5:255–262.
Sharon G, Sampson TR, Geschwind DH & Mazmanian SK (2016).
The central nervous system and the gut microbiome. Cell
167:915–932.
Shoemark DK & Allen SJ (2015). The microbiome and disease:
reviewing the links between the oral microbiome, aging, and
Alzheimer’s disease. J Alzheimers Dis 43:725–738.
Tremlett H, Bauer KC, Appel-Cresswell S et al. (2017). The
gut micro -biome in human neurological disease: a review. Ann
Neurol 81: 369–382.
Wang Y & Kasper LH (2014). The role of microbiome in central
ner vous system disorders. Brain Behav Immun 38:1–12.
Copyright Taylor & Francis Group. Do Not Distribute.
https://doi.org/10.1136/bmj.j831
-
Chapter 10: Microbial Community Disruption—A Role in Other Human
Diseases?438
Microbiota and autism spectrum disordersDe Angelis M,
Francavilla R, Piccolo M et al. (2015). Autism spectrum
disorders and intestinal microbiota. Gut Microbes 6:207–213.Ding
HT, Taur Y, Walkup JT (2017). Gut microbiota and autism: key
concepts and findings. J Autism Dev Disord 47:480–489.Li Q &
Zhou JM (2016). The microbiota-gut-brain axis and its poten-
tial therapeutic role in autism spectrum disorder. Neuroscience
324:131–139.
Mulle JG, Sharp WG & Cubells JF (2013). The gut microbiome:
a new frontier in autism research. Curr Psychiatry Rep 15:337.
Reddy BL & Saier MH (2015). Autism and our intestinal
microbiota. J Mol Microbiol Biotechnol 25:51–55.
Rosenfeld CS (2015). Microbiome disturbances and autism
spec-trum disorders. Drug Metab Dispos 43:1557–1571.
Vuong HE & Hsiao EY (2017). Emerging roles for the gut
microbiome in autism spectrum disorder. Biol Psychiatry
81:411–423.
Yang Y, Tian J, Yang B (2018). Targeting gut microbiome: a novel
and potential therapy for autism. Life Sci 194:111–119
Microbiota and cancerBultman SJ (2016). The microbiome and its
potential as a cancer
preventive intervention. Semin Oncol 43:97–106.Erdman SE &
Poutahidis T (2015). Gut bacteria and cancer. Biochim
Biophys Acta 1856:86–90.Ertz-Archambault N, Keim P & Von
Hoff D (2017). Microbiome and
pancreatic cancer: a comprehensive topic review of literature.
World J Gastroenterol 23:1899–1908.
Francescone R & Vendramini-Costa DB (2016). Microbiome and
cancer. In The Human Microbiota and Chronic Disease:
dysbi-osis as a Cause of Human Pathology (Nibali L &
Henderson B eds). John Wiley & Sons, Hoboken, NJ,
pp. 371–390.
Garrett WS (2015). Cancer and the microbiota. Science 348:
80–86.
Gao R, Gao Z, Huang L & Qin H (2017). Gut microbiota and
colorectal cancer. Eur J Clin Microbiol Infect Dis 36:757–769.
Keku TO, Dulal S, Deveaux A et al. (2015). The
gastrointestinal micro-biota and colorectal cancer. Am J Physiol
Gastrointest Liver Physiol 308:G351–363.
Konstantinov SR (2017). Diet, microbiome, and colorectal cancer.
Best Pract Res Clin Gastroenterol 31:675–681.
Lam SY, Yu J, Wong SH et al. (2017). The gastrointestinal
microbiota and its role in oncogenesis. Best Pract Res Clin
Gastroenterol 31: 607–618.
Manzat-Saplacan RM, Mircea PA, Balacescu L et al. (2015).
Can we change our microbiome to prevent colorectal cancer
develop-ment. Acta Oncol 54:1085–1095.
Marchesi JR, Adams DH, Fava F et al. (2016). The gut
microbiota and host health: a new clinical frontier. Gut
65:330–339.
Ohtani N (2015). Microbiome and cancer. Semin Immunopathol
37:65–72.
Rajagopala SV, Vashee S, Oldfield LM et al. (2017). The
human microbiome and cancer. Cancer Prev Res (Phila)
10:226–234.
Vogtmann E & Goedert JJ (2016). Epidemiologic studies of the
human microbiome and cancer. Br J Cancer 114:237–242.
Wang L & Ganly I (2014). The oral microbiome and oral
cancer. Clin Lab Med 34:711–719.
Zitvogel L, Daillére R, Roberti MP et al. (2017).
Anticancer effects of the microbiome and its products. Nat Rev
Microbiol 15: 465–478.
Zitvogel L, Galluzzi L, Viaud S et al. (2015). Cancer and
the gut microbiota: an unexpected link. Sci Transl Med
7(271):271ps1.
Microbiota and diabetesDelzenne NM, Cani PD, Everard A
et al. (2015). Gut microorgan-
isms as promising targets for the management of type 2 diabetes.
Diabetologia 58:2206–2217.
Fåk F (2016). The gut microbiota: a predisposing factor in
obesity, diabetes and atherosclerosis. In The Human Microbiota and
Chronic Disease: Dysbiosis as a Cause of Human Pathology (Nibali L
& Henderson B eds). John Wiley & Sons, Hoboken, NJ, pp.
351–359.
Gülden E, Wong FS & Wen L (2015). The gut microbiota and
Type 1 Diabetes. Clin Immunol 159:143–153.
Hartstra AV, Bouter KE, Bäckhed F & Nieuwdorp M (2015).
Insights into the role of the microbiome in obesity and type 2
diabetes. Diabetes Care 38:159–165.
Hu C, Wong FS & Wen L (2015). Type 1 diabetes and gut
micro-biota: Friend or foe? Pharmacol Res 98:9–15.
Hu Y, Wong FS & Wen L (2017). Antibiotics, gut microbiota,
envi-ronment in early life and type 1 diabetes. Pharmacol Res 119:
219–226.
Knip M & Siljander H (2016). The role of the intestinal
microbiota in type 1 diabetes mellitus. Nat Rev Endocrinol
12:154–167.
Knip M & Honkanen J (2017). Modulation of Type 1 Diabetes
Risk by the Intestinal Microbiome. Curr Diab Rep 17(11):105. doi:
10.1007/s11892-017-0933-9.
Lau E, Carvalho D, Pina-Vaz C et al. (2015). Beyond gut
microbiota: understanding obesity and type 2 diabetes. Hormones
(Athens) 14:358–369.
Needell JC & Zipris D (2016). The role of the intestinal
microbiome in Type 1 diabetes pathogenesis. Curr Diab Rep
16:89.
Park A & Zhao G (2018). Mining the virome for insights into
Type 1 diabetes. DNA Cell Biol 37:422–425.
Paun A, Yau C & Danska JS (2017). The Influence of the
microbiome on Type 1 diabetes. J Immunol 198:590–595.
Tai N, Wong FS & Wen L (2015). The role of gut microbiota in
the development of type 1, type 2 diabetes mellitus and obesity.
Rev Endocr Metab Disord 16:55–65.
van Olden C, Groen AK & Nieuwdorp M (2015). Role of
intestinal microbiome in lipid and glucose metabolism in diabetes
mellitus. Clin Ther 37:1172–1177.
Wen L & Duffy A (2017). Factors influencing the gut
microbiota, inflammation, and Type 2 diabetes. J Nutr
147:1468S–1475S.
Microbiota and rheumatoid arthritisAraújo VM, Melo IM & Lima
V (2015). Relationship between peri-
odontitis and rheumatoid arthritis: review of the literature.
Mediators Inflamm 2015:259074.
Brusca SB, Abramson SB & Scher JU (2014). Microbiome and
mucosal inflammation as extra-articular triggers for rheumatoid
arthritis and autoimmunity. Curr Opin Rheumatol 26:101–107.
Catrina AI, Deane KD & Scher JU (2016). Gene, environment,
microbiome and mucosal immune tolerance in rheumatoid arthritis.
Rheumatology (Oxford) 55:391–402.
Detert J (2016). Rheumatoid arthritis: the bacterial connection.
In The Human Microbiota and Chronic Disease: Dysbiosis as a Cause
of Human Pathology (Nibali L & Henderson B eds). John Wiley
& Sons, Hoboken, NJ, pp. 283–300.
Kang Y, Cai Y, Zhang X et al. (2017). Altered gut
microbiota in RA: implications for treatment. Z Rheumatol
76:451–457.
McLean MH, Dieguez D Jr, Miller LM & Young HA (2015). Does
the microbiota play a role in the pathogenesis of autoimmune
diseases? Gut 64:332–341.
Copyright Taylor & Francis Group. Do Not Distribute.
-
439Bibliography
Sandhya P, Danda D, Sharma D & Scaria V (2016). Does the
buck stop with the bugs?: an overview of microbial dysbiosis in
rheumatoid arthritis. Int J Rheum Dis 19:8–20.
Scher JU, Bretz WA & Abramson SB (2014). Periodontal disease
and subgingival microbiota as contributors for rheumatoid arthritis
pathogenesis: modifiable risk factors? Curr Opin Rheu-matol
26:424–429.
Van de Wiele T, Van Praet JT, Marzorati M et al. (2016).
How the microbiota shapes rheumatic diseases. Nat Rev Rheumatol
12:398–411.
WebsitesAmerican Biological Safety Association
http://www.absa.org/
riskgroups/
Copyright Taylor & Francis Group. Do Not Distribute.
http://www.absa.org/riskgroups/http://www.absa.org/riskgroups/