Embed Size (px)
Citation preview

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 1/59
Facial trauma
DR : RAMI ELIAS SAAB
CONSULTANT OF ORAL &
MAXILLOFACIAL SURGERY

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 2/59
The term facial trauma means any injury to the face orupper jaw bone. Facial traumas include injuries to the
skin covering, underlying skeleton, neck,ear, nasal
(sinuses), orbital socket, or oral lining, as well as the
teeth and dental structures. Sometimes these types of
injuries are called maxillofacial injury. Facial trauma is
often recognized by lacerations (breaks in the skin);
bruising around the eyes, widening of the distance
between the eyes (which may indicate injury to the
bones between the eye sockets); movement of theupper jaw when the head is stabilized (which may
indicate a fracture in this area); and abnormal
sensations on the cheek.
What is facial trauma?

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 3/59
Photo at time of
admission in
emergency
department, showing
extent of injuries
After reconstructive...
skin covering
3D
Ct /scan

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 4/59
Classification of Injury
Contusion
Abrasion
Accidental Tattoo
Retained Foreign Bodies
Puncture Wounds
Simple Laceration
Avulsion (flap)
Avulsion (complete)

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 5/59
Contusions Abrasion
Accidental Tattoo
Avulsion
puncture wound looss of tissue

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 6/59
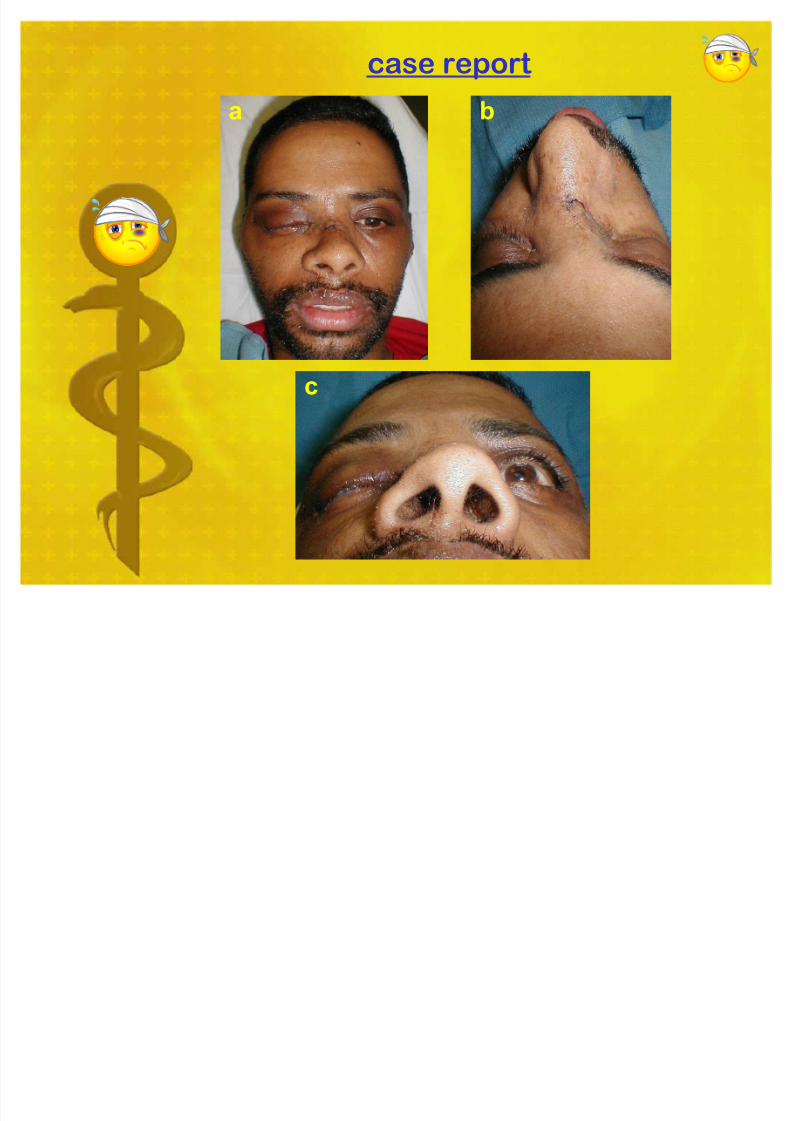
case report
a b
a b
c

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 7/59

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 8/59
Special regional considerations
All injuries need to be copiously irrigated and have allforeign bodies removed. Simple linear lacerations withgood hemostasis can be closed with staples. Close moreextensive lacerations, lacerations with profuse bleeding,or large avulsions of the nonabsorbable suturesencompassing all layers of the scalp. This methodusually achieves good hemostasis.
Lacerations
8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 9/59
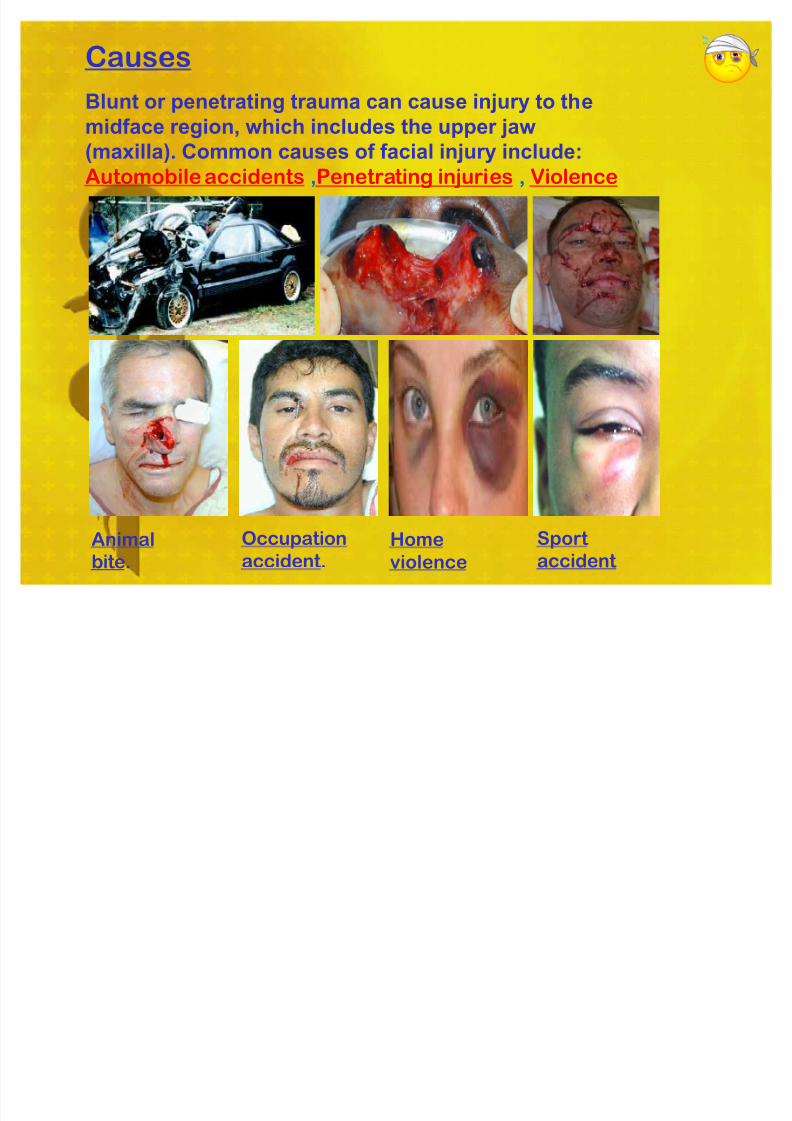
Blunt or penetrating trauma can cause injury to the
midface region, which includes the upper jaw
(maxilla). Common causes of facial injury include:
Automobile accidents ,Penetrating injuries , Violence
Causes
Occupation
accident.Animal
bite.
Home
violence
Sport
accident

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 10/59
Gunshot wound sustained injury to
t he Face, Closure / Tracheostomy
Facial X-Ray
Gunshot wound sustained injury to t he Face

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 11/59
pat hological truma.
a b
c

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 12/59
Exams and Tests
The doctor will perform a physical exam, which may show:
.Bleeding from the nose, ear, eyes, or mout h, or nasal obstruction
.Bruising around the eyes or widening of the distance between the
eyes, which may mean injury to the bones between the eye sockets
.Lacerations (breaks in t he skin)
The following may suggest bone fractures:
.Abnormal sensations on the cheek and irregularities that can be felt
.An upper jaw that moves when the head is still
.A CT scan of the head may be done .

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 13/59
Diffirent types of x-rays

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 14/59
Clinical signs & symptoms
Traumatic telecanthus
Normal intercanthal distance = 33-34 mm>35 mm may indicate NOE disruption
.Damage to lacrimal apparatus => (epiphora)
.CSF leak

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 15/59
Battle SignRacoon sign
train sign

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 16/59
.Depression or angulation
.Periorbital ecchymosis
.Epistaxis
.Tenderness
.Crepitus.Septal deviation
.Septal hematoma
.Rule out septal hematoma.Remove clots with suction
.incise and drain if present to prevent septal
necrosis
.Closed reduction for simple fractures
.Open reduction for severelydisplaced fractures
Nasal Fractures
Treatment
clinical observation

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 17/59
This pictures shows a septal
hematoma on both sides of thenose. The black arrows point to
the lining of the septum that is
ballooned up by underlying blood
Control epistaxis.
Drain septal hematomas.Refer patients to ENT as outpatient
This clinical photograph
shows septal hematoma.

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 18/59
Clinical photograph shows delayed
drainage of septal hematoma resulting in
infection. This patient did not present tothe emergency room until 1 week
following sustaining nasal trauma
Traumatic telecanthus secondary
to nasoorbitoethmoid fracture.Intercanthal distance is( 39 mm).
Postoperative view of patient, demonstrating
normal intercanthal distance (33 mm) after resuspension of the medial canthal ligament
and fixation of the nasoorbitoethmoid
component.

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 19/59
Nasal-Orbital-Et hmoid Fractures
.Epistaxis.
.Severe periorbital edema &
Ecchymosis.
.Subconjunctival hemorrhage.
.Comminuted With posterior displacement.
.Widened nasal bridge.
.Splaying of nasal complex.
Nasalh
emorrh
age.Epistat
.Foley cathe
.Nasal packing
.Merocel sponge
.Nasopharyngeal ballon

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 20/59
Why is facial trauma different in children t han adults?
Facial trauma can range between minor injury to
disfigurement that lasts a lifetime. The face is critical in
communicating with others, so it is important to get the
best treatment possible. Pediatric facial trauma differs
from adult injury because the face is not fully formed and
future growth will be a factor in how the child heals and
recovers. (Certain types of trauma may cause a delay in
t he growt h or furt her complicate recover) . Difficult
cases require physicians with great skill to make a repair that will grow with your child.

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 21/59
trauma
Pediatric facial
Certain
types of
trauma may
cause a
delay in t hegrowt h or
furt her
complicate
recovery
a b c
d e f

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 22/59
Treatments
Surgery is needed if the person cannot function normally
or if there is significant deformity.
.Control bleeding
.Create a clear airway
.Fix broken bone segments with titanium plates
and screws
.Leave the fewest scars possible
.Rule out other injuries
.Treat the fracture
.Treatment should be immediate, as long as the
person is stable and there a no neck fractures
or life-t hreatening injuries
The goal of treatment is to:
8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 23/59
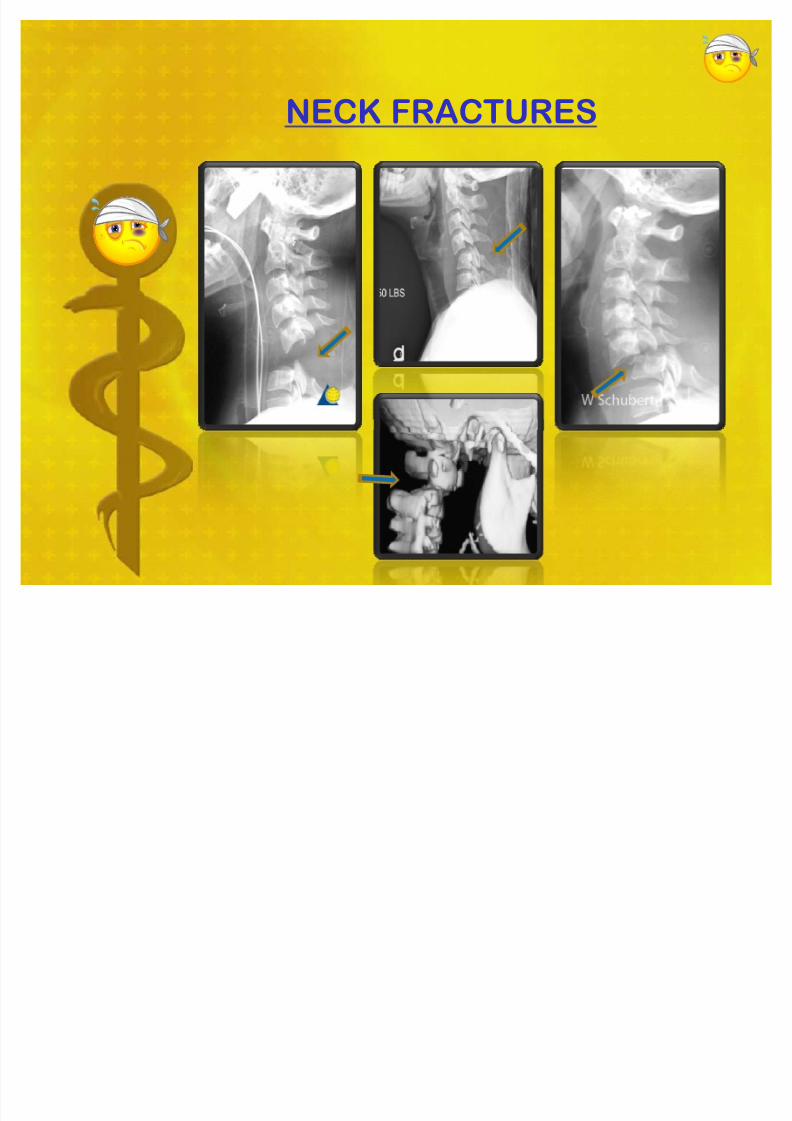
NECK FRACTURES
8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 24/59
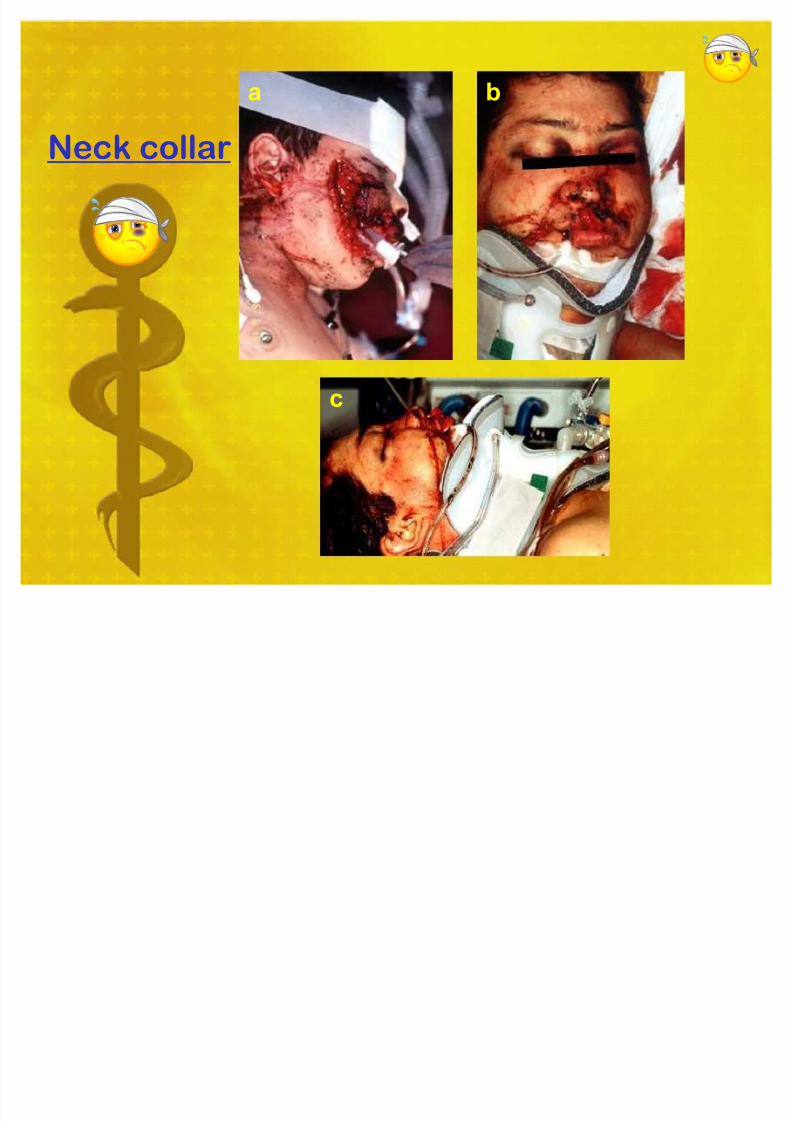
Neck collar
a b
c

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 25/59
Patients generally do very well with proper treatment. Thepatient should gently be told that they will probably look
different than they did before their injury, and that additional
surgeries may be needed 6-12 months later.
Prognosis
General complications include, but are not limited to:
.Bleeding
.Facial asymmetry
.Infection
.Neurologic complications
Possible Complications
When to contact a medical professional
Go to the emergency room or call the local emergency
number if you have a severe injury to your face.

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 26/59
MAXILLARY FRACTURES
(Low Maxillary) (Pyramidal) (Craniofacial Dysjunction)
Rene Le Fort : French surgeon (1869-1951)

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 27/59
Prevalence of mid-face fracturesFracture TypeFracture Type PrevalencePrevalence
ZygomaticomaxillaryZygomaticomaxillary complex (tripodcomplex (tripod
fracture) fracture)40 %40 %
LeFort LeFort
II 15 %15 %
IIII 10 %10 %
IIIIII 10 %10 %
ZygomaticZygomatic arch
arch 1
0 %1
0 %Alveolar process of maxillaAlveolar process of maxilla 5 %5 %
Smash fracturesSmash fractures 5 %5 %
Ot herOt her 5 %5 %

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 28/59
ZYGOMATICOMAXILLARY & ORBITAL FRACTURES

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 29/59
MUSCLE ENTRAPMENT
This child presented with diplopia following blunt
trauma to the right eye. On exam, he was unable to
move his right eyeball up on upward gaze.

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 30/59
The facial skeleton is one of the most complex arrangements of
curving bony surfaces in the body. Today, facial imaging is most
successfully performed with CT.
a b
C d e

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 31/59
CT: Blowout Fracture of Orbit
A: Orbital blowout fracture with displacement of thefloor (arrow), distortion of the inferior rectus, andherniation of orbital fat through defect. Arrowheadindicates medial fracture.
B: Note opacified left anterior ethmoid air cells anddisplaced medial orbital fracture (arrowheads).
A B

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 32/59
Isolated injuries to teeth are quite common and mayrequire the expertise of various dental specialists.
Because of the specific needs of the dental
structures, certain actions and precautions should
be taken if a child has received an injury to his or
her teeth or surrounding dental structures.
If a tooth is ³ knocked out ´, it should be placed
in salt water or milk. The sooner the tooth is re-
inserted into the dental socket, the better chance it
will survive. Therefore, the patient should see a
dentist or oral surgeon as soon as possible.
Never attempt to ³ wipe t he toot h off ´ since
remnants of the ligament which hold the tooth in the
jaw are attached and are vital to the success of
replanting the tooth
Injuries to t he teet h and surrounding dental structures style

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 33/59
Panfacial fracture showing
characteristic anterior open
bite deformity which iscommonly associated with
Le Fort fractures. Multiple
dentoalveolar injuries are
present.
Clinical photographs show palatal
displacement of an alveolar
fracture comprising right central
and lateral maxillary incisors.

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 34/59
case report
Dentoalveolar #
a b
c

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 35/59
Clinical photographs showing extrusion of the coronal fragment
Intraoral films will show the root fracture usually diagonal and
located in the apical, middle, or cervical third of the root, or
combinations of these (middle cervical).

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 36/59
The tooth is out of its socket, and
radiographic examination has
excluded intrusive luxation. The
patient frequently presents the
tooth exhibiting with varying
degree of contamination,
periodontal ligament injury, and/or
dryness, unless kept moist.
Inhaled toothSwallowed tooth

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 37/59
Frontal and palatal view of
left central maxillary incisor with lateral luxation. The
tooth is only attached to the
palatal mucosa, and it is
displaced in palatal direction.
Intraoral films will show the tooth
axially dislocated out of its socket
with partial or total loss of bony
attachment. In this case, there is atotal loss of periodontal attachment
to the bone, and the tooth is
retained solely by the palatal
mucosal attachment.

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 38/59
The left central maxillary incisor is intruded in half its crown
length in apical direction.
. X-ray shows the same patient case report

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 39/59
case report
a b c
d f e
3/mont h
later

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 40/59
case report
a b
c

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 41/59
case report
a b
c d

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 42/59
case report
a b
c d
8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 43/59
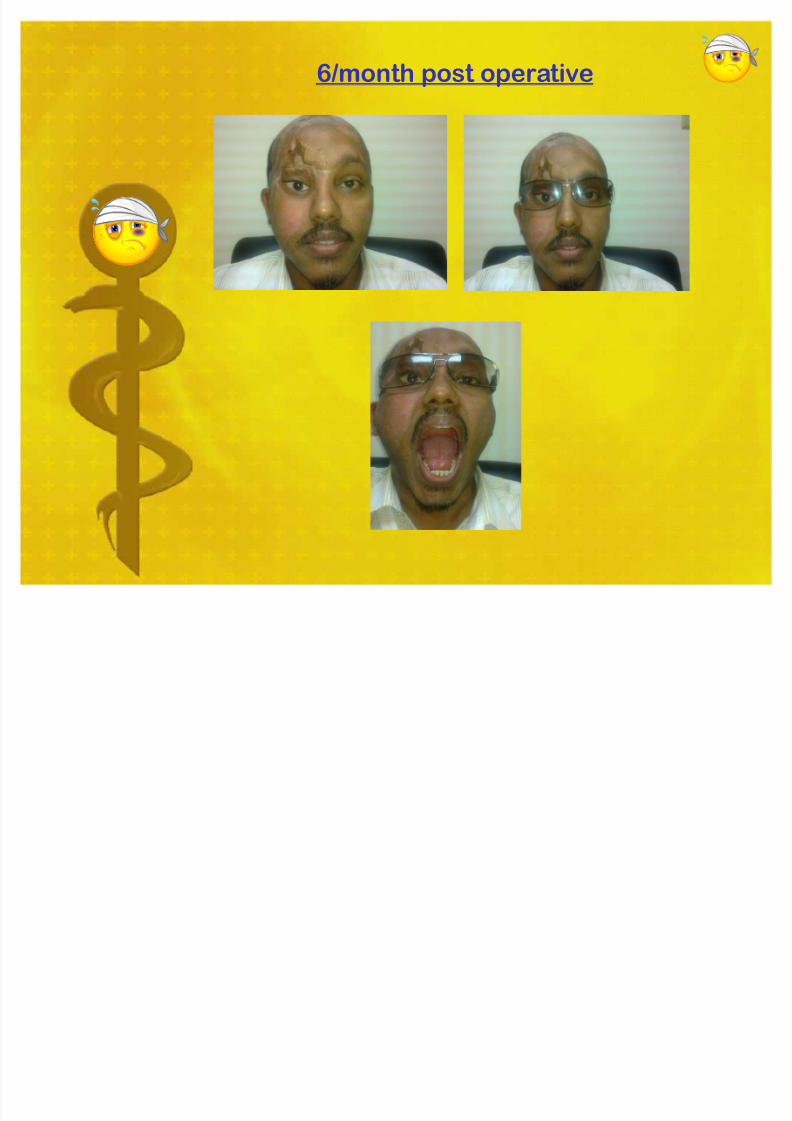
6/mont h post operative

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 44/59
case report
a b
dc

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 45/59
direct post operative
a b
c

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 46/59
One week
post operative
a b
c d

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 47/59
3 / week post operative
a b
c d

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 48/59
case report
a b c
d

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 49/59
a b c
d e f
Intraoperative vision
8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 50/59
case report
a b
c

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 51/59
Intraoperative vision
a b c
d e f f

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 52/59
Postoperative frontal view
of patient, demonstrating
good facial symmetry
Initial clinical presentationof a patient with panfacial
fracture
Large stellate upper liplaceration demonstrating
comminution of anterior
a b c
case report

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 53/59
Coronal access to nasal and
medial orbital components.
Fixation of zygoma and
zygomatic arch.
Fixation of nasoorbitoethmoid
component.
Comminuted zygomatic arch.
a b
c d
Intraoperative vision

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 54/59
case report
Pre operativerPost operative

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 55/59
6 / mont h postoperative
a
b
c
8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 56/59
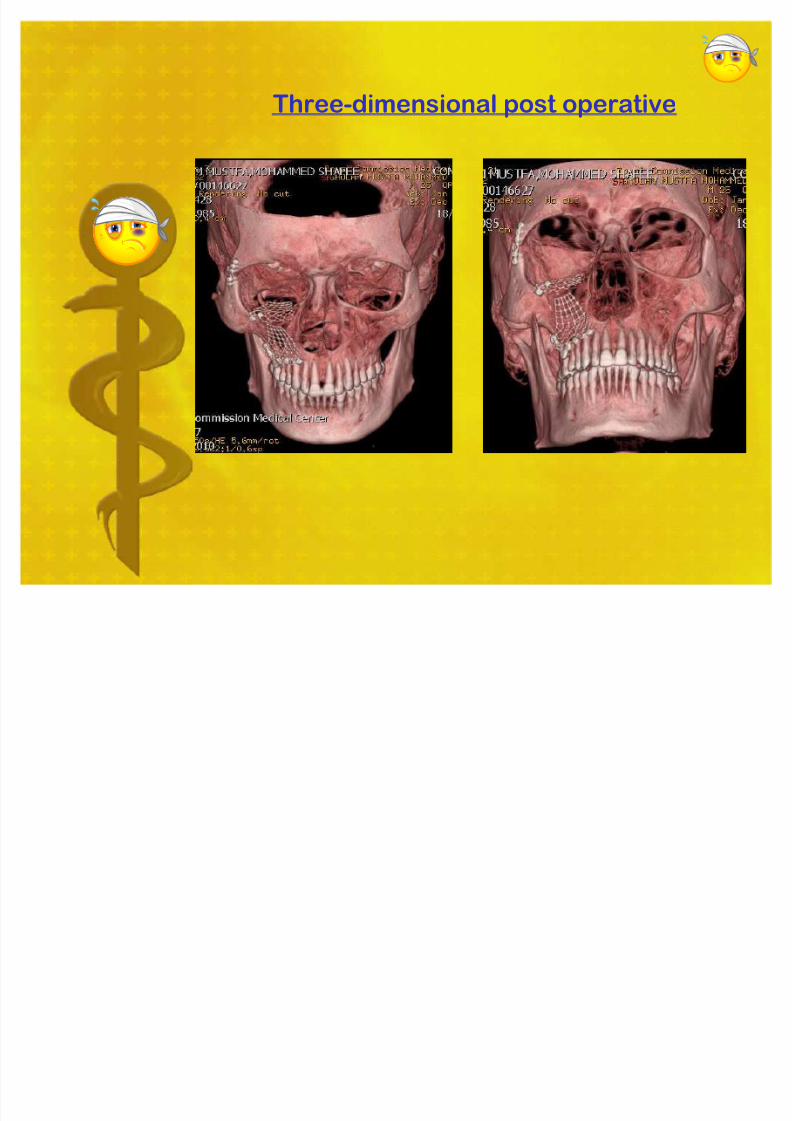
Three-dimensional post operative

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 57/59
case report

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 58/59
Facial trauma can range between minor injury
to disfigurement that lasts a lifetime. The face
is critical in communicating with others, so itis important to get the best treatment possible.
The End
Facial lacerations, oral trauma and dental
trauma are the most common injuries. The
majority of patients are dealt with ,without
admission or referral to another speciality.
Conclusions

8/3/2019 Copy of Facial Truma 11
http://slidepdf.com/reader/full/copy-of-facial-truma-11 59/59
THANK YOU
A I





























