Embed Size (px)
Citation preview

ORIGINAL ARTICLE Psychology and counselling
The longitudinal impact of partnercoping in couples following 5 yearsof unsuccessful fertility treatmentsB.D. Peterson1,5, M. Pirritano2, U. Christensen3, J. Boivin4,J. Block1, and L. Schmidt3
1Department of Psychology, Chapman University, One University Drive, Orange, CA 92866, USA 2Orange County Health CareAgency Medical Services Initiative, USA 3Department of Social Medicine, Institute of Public Health, University of Copenhagen, ØsterFarimagsgade 5, PO Box 2099, DK-1014 Copenhagen K, Denmark 4School of Psychology, Cardiff University, Psychology Building, Park Place,Cardiff, Wales, UK
5Correspondence address. Tel: þ1-714-744-7915; Fax: þ1-714-997-6780; E-mail: [email protected]
background: Because there is a lack of longitudinal research examining the impact of partner coping in couples experiencing infertility,we know very little about the long-term nature of coping with infertility and how partner coping strategies impact personal, marital and socialdistress.
methods: Participants were Danish men and women about to start a cycle of assisted reproduction treatment who were followed for a 5year period of unsuccessful treatments. Multilevel modeling using the actor–partner interdependence model was used to examine the coupleas the unit of analysis.
results: Active and passive avoidance coping strategies were significantly related to increased personal, marital and social distress at theindividual and partner level. Meaning-based coping strategies were related to decreases in a woman’s individual distress and her partner’smarital distress.
conclusions: Partner coping strategies have a significant impact on the other member of the couple over time in men and womenundergoing infertility treatments over a 5 year period. Physicians and mental health professionals can educate men and women regarding theineffectiveness of avoidance coping strategies as well as the beneficial nature of finding new meaning and life goals while experiencing thestress of infertility.
Key words: longitudinal / infertility stress / coping / couples / APIM
IntroductionCoping with the stress of infertility is a topic that has received con-siderable attention from researchers, physicians and mental healthprofessionals over the past several decades (Peterson et al., 2006a;Schmidt et al., 2005a). When a couple experiences infertility, theyencounter changes in their familial, social and personal relationships(Newton et al., 1999). In addition, couples may re-examine theirneed to be biological parents and question long-held beliefs andassumptions about their identity. The aggregate weight of these unex-pected strains can produce infertility-related stress in one or bothpartners (Newton et al., 1999). How the couple responds to thesestressors has implications for both individuals and the couple.
In order to adequately respond to stress, couples use coping strat-egies, or behavioral or emotional efforts used to manage change and
regain control of their lives (Lazarus and Folkman, 1984). Men andwomen cope with infertility in different ways with women consistentlyreporting increased use of coping strategies when compared with men(Jordan and Revenson, 1999). A meta-analysis of studies examiningspecific gender differences in coping with infertility found that, whencompared with their partners, women used more escape-avoidancecoping, engaged in more social support seeking and used more posi-tive reappraisal coping (Jordan and Revenson, 1999). A more recentstudy examining relative coping found that women referred for IVFtreatment coped using proportionately greater amounts ofescape-avoidance, confrontive coping, accepting responsibility andsocial support seeking, whereas men used greater amounts of distan-cing, self-controlling coping and planful problem-solving (Petersonet al., 2006a). Similar gender differences and the increased reportingof coping behaviors in women were also found in a meta-analysis
& The Author 2009. Published by Oxford University Press on behalf of the European Society of Human Reproduction and Embryology. All rights reserved.For Permissions, please email: [email protected]
Human Reproduction, Vol.24, No.7 pp. 1656–1664, 2009
Advanced Access publication on March 15, 2009 doi:10.1093/humrep/dep061
by Agnes H
orvath Hajdu on F
ebruary 9, 2011hum
rep.oxfordjournals.orgD
ownloaded from

examining men and women coping with other life stressors includingwork, caregiving and chronic illness (Tamres et al., 2002).
Over the past decade, there has been an increased emphasis onstudying the relational nature of coping with infertility using the coupleas the unit of analysis. These analyses provide a more complete andaccurate picture of the impact of coping. By examining the couple asthe unit of analysis, researchers can understand the impact that onepartner’s coping has on the other. These studies have consistentlyfound that partner coping is related to individual distress and thatpartner coping impacts men and women in different ways, and theyhave significantly added to the infertility literature base (Stanton et al.,1992; Levin et al., 1997; Mikulincer et al., 1998; Peterson et al., 2003,2006b, 2008). Dyadic analyses have also been used to highlight import-ant relational dynamics and coping patterns in couples dealing withchronic illness such as cancer (Berg and Upchurch, 2007).
Although the number of studies examining the impact of partnercoping has increased, there have been very few studies that haveexamined this issue longitudinally. Berghuis and Stanton (2002) exam-ined the longitudinal impact of coping and depressive symptoms incouples following a failed insemination attempt. They found thatboth individual and partner coping were significantly related to dis-tress. Specifically, avoidant coping used prior to insemination pre-dicted increased distress after a failed insemination attempt,whereas approach-oriented coping was predictive of a more favorableadjustment. They also found that women who were low inemotional-approach coping benefited from their partner’s use of it.Other longitudinal studies not specifically related to coping, butwithin the infertility literature, have found that: anxiety and depressionincreased in women 6 months following failed treatments (Verhaaket al., 2005), infertility-stress had direct and indirect effects on treat-ment outcome (Boivin and Schmidt, 2005), couple relationshipswere strong and stable 1 year following failed IVF treatments (Sydsjoet al., 2005), and couples successfully adjusted to infertility 3 years fol-lowing failed treatments (Daniluk, 2001; Daniluk and Tench, 2007).
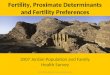
Although there have been a number of studies in the infertility lit-erature using longitudinal designs, there is a need for more studiesexamining the longitudinal impact of partner coping on individual dis-tress in couples experiencing infertility. Such studies are valuablebecause they assess the interactions between partners to see if anindividual’s stress levels can be accounted for by a partner’s copingstrategies. A new method of data analysis called the actor–partnerinterdependence model (APIM; Kenny et al., 2006; Fig. 1) can be effec-tive in analyzing data from such studies. The APIM allows for the sim-ultaneous estimation of actor effects (individual effects) and partnereffects (the effects of another closely associated person) to sharedstressors in dyads, thus providing a more complete picture of howcoping is related to stress in couples. In the infertility literature, tworecent studies have used the APIM in their data analysis: Petersonet al. (2008) used the same sample as the present study to examinethe partner effect of coping with infertility prior to undergoing inferti-lity treatment and Benyamini et al. (in press) studied how perceptionsof infertility are related to psychological adjustment in men andwomen. A body of research that uses the APIM, to examine theimpact of one partner’s coping on the stress of the other partner, isalso accumulating outside of the infertility literature (Butterfield andLewis, 2002; Rayens and Svavarsdottir, 2003; Cook and Kenny,2005; Rogers et al., 2005).
In the current study, we have examined the longitudinal impact ofpartner coping in men and women undergoing fertility treatmentsand link our results to previously established baseline findings, byusing the APIM (Peterson et al., 2008). We examined the impact offour types of coping [active-avoidance strategies (e.g. avoiding preg-nant women or children); active-confronting strategies (e.g. showingfeelings, asking others for advice); passive-avoidance strategies (e.g.hoping for a miracle) and meaning-based strategies (e.g. growing asa person in a good way; finding other goals in life)] on personal,marital and social distress in men and women experiencing failed fer-tility treatments over a 5 year time period.
Materials and Methods
SettingDenmark provides a tax-financed, comprehensive health-care system withequal, free and easy access to high-quality assisted reproductive technol-ogy (ART). In 2002, 6.2% of the national birth cohort was composed ofchildren conceived with some kind of assisted reproduction (NyboeAndersen and Erb, 2006), and in 2007, this proportion increased to8.0% (www.fertilitetsselskab.dk, 20th October 2008).
This study is part of The Copenhagen Multi-centre Psychosocial Inferti-lity (COMPI) Research Programme (Schmidt et al., 2003; Schmidt, 2006),which is a prospective longitudinal cohort study on a large population ofinfertile couples in fertility treatment initiated in Year 2000. The studywas approved by the Danish Data Protection Agency and was assessedby the Scientific Ethical Committee of Copenhagen and FrederiksbergMunicipalities who had no objections. The COMPI cohort comprised con-secutively all new couples initiating fertility treatment with intrauterineinsemination (IUI), in vitro fertilization (IVF) or intracytoplasmic sperminjection (ICSI) in four large public hospital-based tertiary fertility clinicsand one large private clinic in Denmark from 1 January 2000 to 1August 2001.
ProcedureAll new couples entering one of the five fertility clinics for the first timereceived a sealed envelope immediately before their first treatmentattempt (T1). The envelope contained information about the study, abaseline questionnaire, a form for declaration of non-participation in thestudy and a stamped, pre-addressed return envelope for each spouse.The baseline questionnaires were returned to the last author (L.S.) whowas not employed at any of the fertility clinics. The non-respondersreceived up to two written reminders. In total, 2812 fertility patients
Figure 1 General model of actor and partner effects of copingstrategy on distress.
Longitudinal impact of partner coping strategies 1657
by Agnes H
orvath Hajdu on F
ebruary 9, 2011hum
rep.oxfordjournals.orgD
ownloaded from

(1406 couples) received a baseline questionnaire for each partner and80.0% (n ¼ 2250) participated (1169 women, 83.1%; 1081 men,76.9%). Non-participants were significantly older, and female non-participants were more likely to have tubal occlusion. Among malenon-participants, more were about to start ICSI treatment (for a detailednon-participants analyses, see Schmidt et al., 2003; Schmidt, 2006). Intotal, 44 participants were lost by 1 year follow-up (T2) (38 participantswhose identity was not registered at T1, 4 participants whose addresscould not be traced, 1 participant who had died and 1 who sufferedfrom a severe brain injury). In total, 2206 participants received the 1year follow-up questionnaire and 1934 (87.7%) responded (1025women, 89.4%; 909 men, 85.8%). There were no significant differencesbetween the 1 year follow-up participants and non-participants amongeither women or men according to the baseline (T1) values of theCOMPI Fertility Problem Stress Scales or the COMPI Coping StrategyScales. At 5 year follow-up (T3), 72 were lost to follow-up (56 whoseaddress could not be traced, 16 who had died or whose partner haddied). In total, 2134 received the 5 year follow-up questionnaire and1481 (69.4%) responded (834 women, 75.0%; 647 men, 63.3%) afterup to two written reminders.
MeasuresThe COMPI fertility problem stress scalesFertility-related stress was measured using 14 items concerned with thestrains related to infertility produced in the personal, social and maritaldomains, as previous research has shown that infertility taps into thesedifferent arenas (Schmidt, 1996; Greil, 1997; Tjørnhøj-Thomsen, 2005).Seven of these items were taken from The Fertility Problem Stress Inven-tory (Abbey et al., 1991), as this instrument covers all three domains; theremaining seven items were developed from The Psychosocial InfertilityInterview Study (Schmidt, 1996). The items were developed in relationto the three domains (Schmidt et al., 2003). Afterwards, the items werefactor analyzed to produce a set of parsimonious factors, and strain inrelation to the three different domains was confirmed.
The (i) Marital stress subscale (four items) assessed the extent to whichinfertility had produced strain on the marital and sexual relationships (e.g.‘infertility has caused thoughts about divorce’). The (ii) Social stress sub-scale (four items) assessed the stress infertility had produced on socialrelations with family, friends and workmates (e.g. ‘infertility has causedstress in my relationships with family and friends’). The (iii) Personalstress subscale (six items) tapped into the stress infertility had producedon the person’s life and on mental and physical health (e.g. ‘it is verystressful for me to deal with this fertility problem’). The response keyfor the subscales personal stress, social stress and two items frommarital stress was a four-point scale from (1) none at all to (4) a greatdeal. The response key for the remaining two items from marital stresswas a five-point Likert response key from (1) strongly disagree to (5)strongly agree. Items from the different subscales were summed toproduce total scores. Higher scores indicated more marital, social and per-sonal stress. See Table I for means and standard deviations (SD).
The COMPI coping strategy scalesAs recommended by Folkman and Lazarus (1988) and Costa et al. (1996),we developed a coping questionnaire specifically aimed at measuringcoping strategies in relation to a specific stressor: infertility. This 29-itemquestionnaire was developed using three sources: (i) items wereadapted from the 66-item Ways of Coping Questionnaire (WOCQ), aprocess-oriented measure of coping derived from Lazarus’ and Folkman’stransactional model of stress (Lazarus and Folkman, 1984; Folkman andLazarus, 1988); (ii) Folkman’s (1997) later revision of the coping modelwith the inclusion of the new concept, meaning-based coping; and (iii)
items developed from a qualitative interview study (Schmidt, 1996).Items for the coping questionnaire were selected from WOCQ only ifthis specific way of coping was clearly revealed in the qualitative interviewtranscripts (Schmidt, 1996). In total, 18 items were selected fromWOCQ, and seven of these were re-formulated to focus on the specificstressor of infertility. Further, we developed 11 items based on the resultsfrom the interview study. These 29 items covered a wide range ofresponses the participants may have engaged in when dealing with the fer-tility problem.
The items were categorized into four subscales based on their concep-tual content: (i) active-avoidance strategies (e.g. avoiding pregnant womenor children); (ii) active-confronting strategies (e.g. showing feelings, askothers for advice); (iii) passive-avoidance strategies (e.g. hoping for amiracle); and (iv) meaning-based coping (e.g. growing as a person in agood way, finding other goals in life) (Schmidt et al., 2005b). The responsekey was (1) not used, (2) used somewhat, (3) used quite a bit and (4) useda great deal. The subscales comprised items that were significantly inter-correlated. Ten of the 29 items did not fit the scales, and we excludedthem from the analyses. On the final measure, active-avoidance copingwas covered by four items, active-confronting by seven items,passive-avoidance by three items and meaning-based coping by fiveitems. Only when the participants had answered at least half of theitems in a subscale did we include their response for that subscale. A con-firmatory factor analysis showed goodness-of-fit-index (GFI) ¼ 0.88 forthe entire model. When subscales were removed from the model oneat a time, the GFIs were .0.91.
Data analysisThe analyses were longitudinal, following couples across three waves ofdata collection: baseline, 1 and 5 years. Dyadic growth curve modelswere created using multilevel modeling techniques (Kenny et al., 2006;Kashy and Donnellan, 2008). In order to conduct the analyses, the datawere structured so that each line contained data for one individual atone time point, with a variable included that defined the couple (i.e.dyad), a variable that identified the individual and a variable that codedfor time. In growth curve modeling, the decision of which time pointshould be coded zero is not arbitrary because it affects the interpretationof later results (Singer and Willet, 2003). For the current analyses, thebaseline time point was coded as zero as the starting point where thecouple initiated a treatment period. Multilevel analyses, which involvemore than one regression model calculated at different levels of anested design, were conducted. In the current set of analyses, the
.................... .................... ....................
........................................................................................
Table I Male and female mean distress at baseline, 1and 5 years
Baseline 1 year 5 years
Mean SD Mean SD Mean SD
Personal distress
Male 5.38 0.31 5.15 0.11 4.64 0.31
Female 8.44 0.34 8.28 0.14 7.73 0.36
Marital distress
Male 4.22 0.25 4.24 0.09 5.31 0.27
Female 4.48 0.23 4.46 0.10 5.63 0.25
Social distress
Male 1.67 0.17 1.69 0.16 1.81 0.19
Female 2.36 0.17 2.42 0.16 2.64 0.18
1658 Peterson et al.
by Agnes H
orvath Hajdu on F
ebruary 9, 2011hum
rep.oxfordjournals.orgD
ownloaded from

individual level was nested within the couple level. Multilevel analyses esti-mate the model independently at each of these levels. Because multiplemodels are constructed at each level of the nested design, the analysisis able to use all available data without having to use listwise deletionacross the entire analysis. Because of this, when data were available foronly one partner, they were included in the individual level analyses, butnot the couple level analyses.
The design of the analysis is very similar to a multiple regression withone dependent variable and a set of predictor (or independent) variables.The dependent variables in the current study were three different types ofinfertility-related stress (personal, marital and social), and the independentvariables were the four coping strategies and time. Interaction effects withtime were also examined for the gender, actor and partner effects. Multi-level analyses were conducted for each combination of dependent andindependent variables, resulting in 12 analyses. These analyses provideunstandardized estimates of path coefficients for actor and partnereffects. Analyses were also conducted to determine if there were signifi-cant differences in the strength of the actor and partner effects.
One of the principal challenges in running the multilevel dyadic growthmodels that sets them apart from cross-sectional models is the increase inparameter estimates that are possible (i.e. more random effects are avail-able to be included in the models), and the resulting difficulty in findingmodels that will actually run. To discover the best model, analyses wererun starting with the saturated model (the model including all possiblerandom effects) and gradually refining them until the optimal modelemerged. In some instances, models designed only to estimate the var-iance of components were run. This served as a diagnostic tool for deter-mining if there was in fact any unexplained variance to be estimated inparticular variables. If it was determined that there was not any unex-plained variance in an independent variable to be estimated by themodel (a situation that inevitably results in the model’s inability to con-verge), that variable was fixed in subsequent models.
Results
Sample characteristicsIn total, 1169 women and 1081 men who were members of consecu-tively referred couples undergoing fertility treatments completed thebaseline questionnaires (T1). At the 1 year follow-up (T2), therewere 552 males and 592 females who still had no child. At the 5year follow-up (T3), there were 133 males and 201 females whohad not had achieved parenthood either after a treatment-relatedpregnancy, a spontaneous conception or adoption, or a current preg-nancy and who were still partnered with the same partner at inclusion(samples at each time point contained an unequal number of men andwomen because when data were available for both partners, theywere included in the couples analysis, whereas when data were avail-able for only one partner, they were included in the individual levelanalyses but not in the couple level analyses).
At baseline, participants had been infertile for �4 years [women4.1 years (SD ¼ 2.3); men 4.1 years (SD ¼ 2.2)] and 57.8% hadbeen in fertility treatment (most frequently IUI) prior to inclusion inCOMPI. Men were also significantly older than women, with a meanage of 34.4 versus 32.0 years, respectively (t ¼ 17.6, P , 0.001). At5 years, couples had been trying to have a child for an average of9.1 years. Men continued to be significantly older than women, witha mean age of 40.1 versus 37.4 years, respectively (t ¼ 4.4, P ,
0.001). Couples reported receiving an average of 4.3 fertility
treatments over the 5 year period. For those still trying to have chil-dren at 5 years, 35.3% of men and 32.8% of women attributed theinfertility to men, whereas 41.8% of women and 41.4% of men attrib-uted the infertility to women. In terms of social position, 25% of par-ticipants were from a high social position (professionals, executivesand medium level white collar employees), 52% were from amedium social position (low level white collar employees and skilledworkers) and 23% were from a low social position (unskilled and semi-skilled workers and participants receiving social benefits).
Baseline models and longitudinaldistress levelsTable I presents the mean levels of personal, marital and social distressat the three time points. Table II presents the findings from the base-line models that were used to determine the growth curve for sub-sequent analyses that would include covariates. The baseline modelsprovide an estimate of the mean for males and females as well asan estimate of the slope of the growth curve. The significant meansindicate that these means were significantly different from zero. Thesignificant negative slope for males and females on personal distressindicates that personal distress decreased across the 5 years of thestudy. Social distress did not change significantly during the studyperiod. The significant positive slope for males and females formarital distress indicates that marital distress increased across the5 years of the study. Significant gender differences indicate thatwomen had higher scores on personal and social distress than menat baseline and 5 years. The significant time effects for personal dis-tress and marital distress simply reiterate the significant male andfemale slopes. The lack of significant gender by time interactions indi-cates that the slope of the growth curves did not significantly differ formales and females.
Multilevel model: significant actorand partner effectsFigure 1 provides a visual depiction of the general model of actor andpartner effects and their influence on male and female distress. Whena significant female partner effect is found, it indicates the existence ofa relationship between a male partner’s coping strategy and the femalepartner’s personal, social or marital distress. Similarly, when
........................................................................................
Table II Two-intercept and interaction growth modelsfor personal, martial and social distress
Personaldistress
Martialdistress
Socialdistress
Male mean 5.23*** 3.93*** 1.63***
Female mean 8.44*** 4.09*** 2.39***
Male slope 20.23*** 0.27*** 0.04
Female slope 20.19** 0.33*** 0.09
Gender 1.60*** 0.15** 0.45***
Time 20.22*** 0.30*** 0.07**
Gender bytime
0.01 0.00 0.03
***P , 0.001; **P , 0.01.
Longitudinal impact of partner coping strategies 1659
by Agnes H
orvath Hajdu on F
ebruary 9, 2011hum
rep.oxfordjournals.orgD
ownloaded from

a significant male partner effect is found, it highlights the relationshipbetween a female partner’s coping strategy and the male partner’sdistress.
Table III presents the significant actor and partner effects for eachcoping strategy by personal, marital and social distress over time.Unstandardized beta coefficients (b) are reported. Comparisons ofthe relative contribution of independent variables can be made sinceall variables are measured on the same response scale.
Active-avoidance copingFor active-avoidance, there were significant actor effects on personal,marital and social distress. The positive actor effects for men andwomen indicate that greater use of active-avoidance predictedgreater personal, marital and social distress across time for bothmen and women. There were also significant partner effects formales and females on personal and social distress, indicating that apartner’s use of increased active-avoidance coping was related toincreases in his or her partner’s levels of personal and social distress.This was also true for marital distress, but only for women: theincreased use of active-avoidance in men increased levels of maritaldistress in women. There was one interaction between time andthe female actor effect. Follow-up ordinary least squares (OLS)regression analyses showed that over time, the actor effect forwomen was strengthened. This indicates that over time, the relation-ship between the use of the active-avoidance coping strategy andgreater social distress increased. No other interactions betweeneither partner or actor effects with time were significant, indicatingthat the strength of all other actor and partner effects remained con-stant across time.
Active-confronting copingFor active-confronting, there was a significant actor effect for socialdistress and an actor by time effect for men and marital distress.There was also a significant male partner effect for marital distressand a male partner by time effect for marital distress. Follow-upOLS regression analyses indicated that for the actor effect, therewas a significant increase in the strength of the effect at 5 years.Thus, for the partner effect, a female’s increased use of active-confronting coping strategies was related to increased male marital dis-tress over time.
Passive-avoidance copingFor personal distress, there was a significant actor effect for men andwomen and a significant partner effect for women. There were alsosignificant interactions between time and the actor effect forwomen; this indicated an increase in the strength of the femaleactor effect over time. For marital distress, there was a significantactor effect for men and a significant partner effect for females, indicat-ing that a male’s use of passive avoidance was related to his own andhis partner’s increased marital distress. For social distress, there weresignificant actor effects for men and significant interactions betweenthe actor and partner effects over time for women, meaning thatwith an increased actor effect for women, there was a concomitantdecrease in the partner effect.
Meaning-based copingFor personal distress, there was a significant negative actor effect forfemales, indicating that the increased use of meaning-based copingwas related to decreased personal distress. There was, however, aninteraction between the gender and the actor effects, indicating thatalthough the increased use of meaning-based coping decreasedfemale personal distress, for males this was not the case. There wasno effect of meaning-based coping on the personal distress of men.
For marital distress, there was a significant female actor effect and asignificant male partner effect, indicating that a female’s use ofmeaning-based coping was related to a decrease in both her andher partner’s marital distress. There was also a significant positivemale actor effect for social distress indicating that for men, greateruse of meaning-based coping strategies was related to increasedsocial distress.
DiscussionThe current study highlights the impact of partner coping strategies onpersonal, marital and social distress in a sample of men and womenundergoing unsuccessful fertility treatments over a 5 year period.Given the lack of longitudinal studies examining the impact ofpartner coping on infertility distress, it is difficult to make direct com-parisons to findings of previous studies (Berghuis and Stanton, 2002).However, key findings from this study confirm that active and passiveavoidance coping are consistently associated with poorer personaloutcomes for the individual and their partner, and that meaning-basedcoping strategies are more beneficial for women than for men at boththe individual and the partner levels. These findings can benefit bothphysicians and mental health professionals by underscoring theimportance of coping over time, but also by addressing the significantlong-term impact of one partner’s coping on his or her partner’sinfertility-related distress.
When examining distress levels over time, women reported greateramounts of personal distress when compared with men, yet personaldistress decreased significantly for both men and women over time atsimilar rates. This is consistent with a wide range of studies indicatingthat women report greater amounts of infertility-related distress whencompared with men (Slade et al., 1997; Newton et al., 1999). This islikely due to the fact that the experience of infertility is so closelylinked to the female identity, and because the female’s body is themain focus of fertility treatment (Morrow et al., 1995; Petersonet al., 2007). The longitudinal model was valuable, in that it allowedus to see that over time, both male and female personal distresslevels decreased at similar rates. This finding supports a previousstudy which found that adaptation of men and women to failed fertilitytreatments was similar, and that couples report less distress over time,potentially because they have more psychological space to respond tothe life transition (Daniluk and Tench, 2007). The results are also con-sistent with a recent systematic review among women in IVF treat-ment showing that the long-term prognosis for people undergoingtreatment was generally positive with ,25% of women showing subor clinical levels of anxiety or depression (Verhaak et al., 2007a).
Time also predicted a significant increase in marital distress for bothmen and women. As with personal distress, there were no significantgender differences over time, highlighting the reciprocal nature of the
1660 Peterson et al.
by Agnes H
orvath Hajdu on F
ebruary 9, 2011hum
rep.oxfordjournals.orgD
ownloaded from

.............................................................................................................................................................................................
Table III Actor and partner effects of coping style on distress over time
Personal distress Martial distress Social distress
Active-avoidance
Actor effects
Male 0.79*** 0.39*** 0.38***
Female 0.89*** 0.30*** 0.30***
Actor effect by gender 0.05 20.05 20.04
Male actor effect by time 0.01 20.02 0.00
Female actor effect by time 0.04 0.03 0.05**
Partner effects
Male 0.23*** 0.09 0.08*
Female 0.44*** 0.21*** 0.23***
Partner effect by gender 0.10* 0.06 0.07**
Male partner effect by time 20.03 0.04* 0.00
Female partner effect by time 20.02 0.03 20.03
Active-confronting
Actor effects
Male 0.03 20.02 0.06*
Female 0.00 0.02 0.04
Actor effect by gender 20.01 0.02 20.01
Male actor effect by time 0.02 0.04** 0.00
Female actor effect by time 0.00 0.00 20.02
Partner effects
Male 0.00 0.07* 20.02
Female 0.02 0.01 0.01
Partner effect by gender 0.01 20.03 0.01
Male partner effect by time 0.02 20.03* 20.01
Female partner effect by time 20.02 0.01 20.02
Passive-avoidance
Actor effects
Male 0.35*** 0.19*** 0.16***
Female 0.28*** 0.08 0.05
Actor effect by gender 20.03 20.06 20.05
Male actor effect by time 0.02 0.00 20.01
Female actor effect by time 0.07* 0.04 0.04*
Partner effects
Male 0.10 20.06 20.05
Female 0.21** 0.11* 0.08
Partner effect by gender 0.06 0.08 0.06
Male partner effect by time 0.00 0.03 0.01
Female partner effect by time 20.02 0.00 20.05*
Meaning-based
Actor effects
Male 0.01 0.01 0.09**
Female 20.23*** 20.12** 20.02
Actor effect by gender 20.12** 20.07* 20.06*
Male actor effect by time 0.02 0.02 0.00
Female actor effect by time 0.02 0.02 0.00
Continued
Longitudinal impact of partner coping strategies 1661
by Agnes H
orvath Hajdu on F
ebruary 9, 2011hum
rep.oxfordjournals.orgD
ownloaded from

marital relationship in experiencing the stress of infertility. It is import-ant to note that our study did not specifically measure marital adjust-ment or satisfaction, but rather marital distress (e.g. stress placed onthe marriage, stress on sexual relations). Therefore, it is difficult togeneralize findings on marital distress to other studies examining theconstruct of marital adjustment. Although a large number of studiesshow that marital adjustment is strong in men and women experien-cing infertility before and after treatments (Schmidt et al., 2005c;Sydsjo et al., 2005), some studies have shown that time can play arole in decreasing satisfaction. For example, Berg and Wilson (1991)found in a cross-sectional study that marital satisfaction was strongfor couples during the first 2 years of treatments, but significantlylower in the third year, proposing that advanced stages of infertilityand treatments not only take a toll on the individual, but also uponthe couple. Holter et al. (2006) studied the short-term psychologicalimpact of IVF treatment and found that at the time of treatment, acouple’s relationship was strengthened because of the treatmentprocess, but that further treatments might cause problems in therelationship. This may be due to a couple’s reliance on one anotherfor emotional support throughout the treatment process, which mayerode over time. In our study, increased marital distress could haveto do with men and women’s differing desires in treatment continu-ance. In a study of 45 couples experiencing failed IVF treatment,Sydsjo et al. (2005) found that nearly three-quarters of womenwanted to undergo further IVF treatments, whereas the majority ofmen did not intend to. Although the current study did not examinethis construct directly, gender differences regarding desired continu-ance or cessation of treatment may play a role in the increase ofmarital distress over time.
The longitudinal model also allowed us to examine the long-termimpact of various coping strategies, and the impact these coping strat-egies have on infertility-related distress. When examining the impact ofpartner coping on distress over time, active-avoidance coping,passive-avoidance coping and meaning-based coping produced note-worthy results. In our baseline analysis, we found that active-avoidancecoping strategies had significant actor and partner effects on personal,marital and social distress (Peterson et al., 2008). In the current study,the actor effects for males and females on each type of distress aresignificant, indicating that a male or female’s use of active-avoidancecoping predicted higher levels of individual distress over time, and sup-porting previous studies showing that active-avoidance coping isrelated to increased individual distress (Peterson et al., 2006a).
When examining partner effects, a partner’s use of active avoidancewas related to increased personal and social distress in men andwomen, and increased marital distress in women over time. In theirlongitudinal study of partner coping over time, Berghuis and Stanton(2002) also found that a partner’s avoidant coping strategies wererelated to greater distress. Contrary to what couples attempt toachieve, namely relief from the stress through actively avoiding situ-ations and reminders of infertility, the findings from this study clearlyshow that using active-avoidance coping strategies over time doesnot ultimately help one’s level of personal distress, neither at the indi-vidual nor at the partner level. Physicians and mental health pro-fessionals can help men and women reduce their levels ofactive-avoidance coping by educating patients regarding the paradox-ical nature of this ineffective coping strategy, specifically that themore they avoid the stressor, the greater distress both they andtheir partner are likely to report.
The findings related to passive avoidance varied greatly from base-line to Year 5. At baseline, there were no significant partner effects forpassive-avoidance coping (Peterson et al., 2008). At that time, wehypothesized that the non-significant impact of the partner effectwas likely due to the unexpressed nature of the coping strategy, andthat because of this, partners may not be aware of one another’suse of passive avoidance. In the current study, there was a maleactor effect for passive avoidance on personal, marital and social dis-tress, and a female actor effect for personal distress. There was also afemale partner effect for personal and marital distress. This findingshowed that men’s use of passive-avoidance coping strategies (e.g.relying on a miracle and feeling the only thing they could do aboutinfertility was wait) was linked with increased personal, marital andsocial distress for themselves, and increased personal and marital dis-tress for their partners. One possible explanation for this is that aman’s use of passive avoidance over time goes against the typicalmale role of problem-solver, and although he is taking actionthrough treatments, his coping strategy lacks belief that his actionswill make a difference. A meta-analysis on the association of copingto physical and psychological health outcomes based in studies usingeither the Lazarus and Folkman Revised WOCQ or Vitiliano’s Waysof Coping Checklist showed that wishful thinking was inversely associ-ated with psychological well-being (Penley et al., 2002). The measure-ment of wishful thinking is overlapping with our subscale forpassive-avoidance coping and the meta-analysis and hence supportsour results among a population of infertile people.
.............................................................................................................................................................................................
Table III Continued
Personal distress Martial distress Social distress
Partner effects
Male 20.06 20.08* 0.00
Female 0.02 20.01 0.03
Partner effect by gender 0.04 0.04 0.02
Male partner effect by time 20.02 0.01 20.02
Female partner effect by time 0.00 0.02 0.00
***P , 0.001; **P , 0.01; *P , 0.05.
1662 Peterson et al.
by Agnes H
orvath Hajdu on F
ebruary 9, 2011hum
rep.oxfordjournals.orgD
ownloaded from

The impact of meaning-based coping over time was also note-worthy. When a woman used this strategy, it had a beneficial effecton her personal and marital distress, and also on her partner’smarital distress. This is a significant finding because it is rare to findcoping strategies that are significantly related to decreased distress(Jordan and Revenson, 1999). This finding is even more importantgiven the earlier findings that marital distress increases over time.When a woman engages in meaning-based coping, she reports thatthe experience of infertility helped her grow as a person, find othergoals in life and ultimately think about infertility in a positive light. Inother words, women in these couples may more successfully integratethe experience of infertility into their identity—a crucial developmen-tal task when coping with this life transition (Peterson et al., 2007).Further, when Folkman (1997) introduced the concept of meaning-based coping, she stressed that meaning-based coping sustained thecoping process by generating positive emotions. The decreasedmarital distress may be related to a woman’s expanded focus onother life activities, which removes some of the shared burdens thatinfertility places on her and her partner and that lead to increasedmarital distress over time. Women who found new life goals followingtreatments also reported less anxiety and depressive symptoms(Verhaak et al., 2007b). Meaning-based coping has also been shownto be effective for couples in adapting to other life stressors includingcoping with experience of breast cancer (Skerrett, 1998). As couplesredefine and work through the complexities of this difficult life stres-sor, they have increased opportunities to develop new forms of com-munication, jointly solve problems and increase their levels ofinterpersonal intimacy (Skerrett, 1998).
Men and women should be aware of the positive impact ofmeaning-based coping, while also being aware that it may take timeto implement this coping strategy. Gender differences in the pacingand timing of treatment may be related to men and women’s unwill-ingness to redefine the stress of infertility at the beginning of treatment(Peterson et al., 2008). Also men and women in the COMPI cohorthave different reasons for seeking treatment and significantly moremen than women have sought treatment for their partner’s sake(Schmidt et al., 2003). It may take time to experience the benefitsof meaning-based coping because they may only come when aperson has addressed the many complicated questions and stressorspresented through the infertility experience (e.g. why did thishappen to me, will my family and social relationships ever be thesame and what new activities will make life more meaningful?).Although the benefit of this coping strategy is obvious for women, itis important to note it cannot be rushed and may be a long-termprocess.
The COMPI scales used in this study have not yet been validated inlarge-scale psychometric studies. However, the measures wereadopted from existing scales and developed after in-depth qualitativeinterviews with Danish fertility patients. In addition, both measureswere stressor specific to infertility and were not instruments measur-ing general stress and coping. Future research studies which examinethe process of change in couples and the stages of coping with inferti-lity are increasingly necessary to better understand this issue.
We are hopeful that this study will lead to future research examin-ing the impact of coping within the greater social context of infertility.Previous research on the psychosocial factors associated with infertilityhas found several gender differences in how men and women respond
to infertility. These differences include men and women’s differencesfor seeking treatment, gender differences in communication andcoping strategies, differences in depression and anxiety levels followingtreatments, and the impact of infertility on men and women’s identi-ties. These factors are embedded within the social context in whichwe live and the roles and responsibilities related to childbearing andchildcare may differ greatly for men and women (e.g. thedual-bread-winner society, differences in maternal/paternal leave,differences in role expectation of motherhood and fatherhood).Future studies which explore how infertility, gender and their respect-ive consequences are interwoven in cultural and societal expectationswould be valuable.
In conclusion, this longitudinal analysis supports baseline findingsand also adds to the existing knowledge regarding the impact ofcoping with infertility over time. It is clear that active- andpassive-avoidance coping strategies are related to increased distressover time at the individual and partner levels. In addition, awoman’s use of meaning-based coping benefits her and her partner’smarriage over time, particularly at a time when their marital relation-ship may be under duress. This study helps illustrate that partnercoping strategies are related to distress over time, and this knowledgecan benefit physicians and mental health professionals who workdirectly with couples coping with the stress of infertility.
AcknowledgementsThis study is part of The Copenhagen Multi-Centre Psychosocial Infer-tility Research Program (COMPI) initiated by Dr Lone Schmidt, Uni-versity of Copenhagen, 2000. The programme is a collaborationbetween the public fertility clinics at Braedstrup Hospital; Herlev Uni-versity Hospital; Copenhagen University Hospital, Rigshospitalet;Odense University Hospital.
FundingThis study has received support from the Danish Health InsuranceFund (J. nr. 11/097-97), the Else and Mogens Wedell-WedellsborgsFund, the manager E. Danielsen and Wife’s Fund, the merchant L.F.Foghts Fund, the Jacob Madsen and Wife Olga Madsen’s Fund, andthe engineer K.A. Rohde and Wife’s Fund.
ReferencesAbbey A, Andrews FM, Halman LJ. Gender’s role in responses to
infertility. Psychol Women Q 1991;15:295–316.Benyamini Y, Gozlan M, Kokia E. Women’s and men’s perceptions of
infertility and their associations with psychological adjustment: adyadic approach. Br J Health Psychol 2009;14:1–16.
Berg BJ, Wilson JF. Psychological functioning across stages of treatment forinfertility. J Behav Med 1991;14:11–26.
Berg CA, Upchurch R. A developmental-contextual model of couplescoping with chronic illness across the adult life span. Psychol Bull 2007;133:920–954.
Berghuis JP, Stanton AL. Adjustment to a dyadic stressor: a longitudinalstudy of coping and depressive symptoms in infertile couples over aninsemination attempt. J Consult Clin Psychol 2002;70:433–438.
Boivin J, Schmidt L. Infertility-related stress in men and women predictstreatment outcome 1 year later. Fertil Steril 2005;83:1745–1752.
Longitudinal impact of partner coping strategies 1663
by Agnes H
orvath Hajdu on F
ebruary 9, 2011hum
rep.oxfordjournals.orgD
ownloaded from

Butterfield RM, Lewis MA. Health-related social influence: a socialecological perspective on tactic use. J Soc Personal Relationships 2002;19:505–526.
Cook WL, Kenny DA. The actor–partner interdependence model: amodel of bi-directional effects in developmental studies. Int J BehavDev 2005;29:101–109.
Costa PT, Somerfield MR, McCraee RR. Personality and coping: areconceptualization. In: Zeidner M, Endler NS (eds). Handbook ofCoping. Theory, Research, Applications. New York, NY: John Wiley &Sons, Inc., 1996, 44–61.
Daniluk JC. Reconstructing their lives: a longitudinal, qualitative analysis ofthe transition to biological childlessness for infertile couples. J Couns Dev2001;79:439–450.
Daniluk JC, Tench E. Long-term adjustment to infertile couples followingunsuccessful medical intervention. J Couns Dev 2007;85:89–100.
Folkman S. Positive psychological states and coping with severe stress. SocSci Med 1997;45:1207–1221.
Folkman S, Lazarus RS. Manual for the Ways of Coping Questionnaire. PaloAlto, CA: Consulting Psychologists Press, 1988.
Greil AL. Infertility and psychological distress: a critical review of theliterature. Soc Sci Med 1997;45:1679–1704.
Holter H, Anderheim L, Bergh C, Moller A. First IVF treatment-short-term impact on psychological well-being and the maritalrelationship. Hum Reprod 2006;12:3295–3302.
Jordan C, Revenson TA. Gender differences in coping with infertility: ameta-analysis. J Behav Med 1999;22:341–358.
Kashy DA, Donnellan MB. Comparing MLM and SEM approaches toanalyzing developmental dyadic data: growth curve models of hostilityin families. In: Card NE, Selig JP, Little T (eds). Modeling Dyadic andInterdependent Data in the Developmental and Behavioral Sciences.New York, NY: Routledge, 2008, 165–190.
Kenny DA, Kashy DA, Cook WL. Dyadic Data Analysis. New York, NY:The Guilford Press, 2006.
Lazarus RS, Folkman S. Stress, Appraisal, and Coping. New York, NY:Springer, 1984.
Levin JB, Sher TG, Theodos V. The effect of intracouple copingconcordance on psychological and marital distress in infertilitypatients. J Clin Psychol Med 1997;4:361–372.
Mikulincer M, Horesh N, Levy-Shiff R, Manovich R. The contribution ofadult attachment style to the adjustment to infertility. Br J Med Psychol1998;71:265–280.
Morrow KA, Thoreson RW, Penney LL. Predictors of psychological distressamong infertility clinic patients. J Consult Clin Psychol 1995;63:163–167.
Newton CR, Sherrard MA, Glavac I. The fertility problem inventory:measuring perceived infertility-related stress. Fertil Steril 1999;72:54–62.
Nyboe Andersen A, Erb K. Register data on assisted reproductivetechnology (ART) in Europe including a detailed description of ART inDenmark. Int J Androl 2006;29:12–16.
Penley JA, Tomoka J, Wiebe JS. The association of coping to physical andpsychological health outcomes: a meta-analytic review. J Behav Med2002;25:551–603.
Peterson BD, Newton CR, Rosen KH. Examining congruence betweenpartners’ perceived infertility-related stress and its relationship to maritaladjustment and depression in infertile couples. Fam Process 2003;42:59–71.
Peterson BD, Newton CR, Rosen KH, Skaggs GE. Gender differences inhow men and women referred with in vitro fertilization cope withinfertility stress. Hum Reprod 2006a;21:2443–2449.
Peterson BD, Newton CR, Rosen KH, Schulman RS. Coping processes ofcouples experiencing infertility. Fam Relations 2006b;55:227–239.
Peterson BD, Gold L, Feingold T. The experience and influence ofinfertility: considerations for mental health counselors. Fam J 2007;15:251–257.
Peterson BD, Pirritano M, Christensen U, Schmidt L. The impact of partnercoping in couples experiencing infertility. Hum Reprod 2008;23:1128–1137.
Rayens MK, Svavarsdottir EK. A new methodological approach in nursingresearch: an actor, partner, and interaction effect model for familyoutcomes. Res Nurs Health 2003;26:409–419.
Rogers WS, Bidwell J, Wilson L. Perception of and satisfaction withrelationship power, sex, and attachment styles: a couples levelanalysis. J Fam Violence 2005;20:241–251.
Schmidt L. Psykosociale konsekvenser af infertilitet og behandling[Psychosocial consequences of infertility and treatment, in Danish],PhD-thesis. Copenhagen, Denmark: FADL’s Publishers, 1996.
Schmidt L. Infertility and assisted reproduction in Denmark: epidemiologyand psychosocial consequences, Medical Dissertation. Dan Med Bull2006;53:390–417. http://www.danmedbul.dk/Dmb_2006/0406/0406-disputatser/DMB3808.htm.
Schmidt L, Holstein BE, Boivin J, Sangren H, Tjørnhøj-Thomsen T,Blaabjerg J, Hald F, Nyboe Andersen A, Rasmussen PE. Patients’attitudes to medical and psychosocial aspects of care in fertility clinics:findings from the Copenhagen Multi-centre Psychosocial Infertility(COMPI) Research Programme. Hum Reprod 2003;18:628–637.
Schmidt L, Holstein BE, Christensen U, Boivin J. Communication andcoping as predictors of fertility problem stress: cohort study of 816participants who did not achieve a delivery after 12 months of fertilitytreatment. Hum Reprod 2005a;20:3248–3256.
Schmidt L, Christensen U, Holstein BE. The social epidemiology of copingwith infertility. Hum Reprod 2005b;20:1044–1052.
Schmidt L, Holstein BE, Christensen U, Boivin J. Does infertility causemarital benefit? An epidemiological study of 2250 women and men infertility treatment. Pat Educ Couns 2005c;59:244–251.
Singer JD, Willet JB. Applied Longitudinal Data Analysis: Modeling Change andEvent Occurrence. New York, NY: Oxford University Press, 2003.
Skerrett K. Couple adjustment to the experience of breast cancer. Fam SysHealth 1998;16:281–298.
Slade P, Emery J, Liberman BA. A prospective, longitudinal study ofemotions and relationships in in-vitro fertilization treatment. HumReprod 1997;12:183–190.
Stanton AL, Tennen H, Affleck G, Mendola R. Coping and adjustment toinfertility. J Soc Clin Psychol 1992;11:1–13.
Sydsjo G, Ekholm K, Wadsby M, Kjellberg S, Sydsjo A. Relationships incouples after failed IVF treatment: a prospective follow-up study. HumReprod 2005;20:1952–1957.
Tamres LK, Janicki D, Helgeson VS. Sex differences in coping behavior: ameta-analytic review and an examination of relative coping. Pers SocPsychol Rev 2002;6:2–30.
Tjørnhøj-Thomsen T. Close encounters with infertility and procreativetechnology. In: Jenkins J, Jessen H, Steffen V. (eds). ManagingUncertainty. Ethnographic Studies of Illness, Risk and the Struggle for Control.Copenhagen, Denmark: Museum Tusculanum Press, University ofCopenhagen, 2005, 71–91.
Verhaak CM, Smeenk JMJ, van Minnen A, Kremer JAM, Kraaimaat FW. Alongitudinal, prospective study on emotional adjustment before, duringand after consecutive fertility treatment cycles. Hum Reprod 2005;20:2253–2260.
Verhaak CM, Smeenk JMJ, Evers AWM, Kremer JAM, Kraaimaat FW,Braat DDM. Women’s emotional adjustment to IVF: a systematicreview of 25 years of research. Hum Reprod Update 2007a;13:27–36.
Verhaak CM, Smeenk JM, Nahuis MJ, Kremer JA, Braat DD. Long-termpsychological adjustment to IVF/ICSI treatment in women. HumReprod 2007b;22:305–308.
Submitted on November 4, 2008; resubmitted on February 3, 2009; accepted onFebruary 6, 2009
1664 Peterson et al.
by Agnes H
orvath Hajdu on F
ebruary 9, 2011hum
rep.oxfordjournals.orgD
ownloaded from