Embed Size (px)
Citation preview

831
CONTROL OF ALDOSTERONE EXCRETIONBY CHANGES IN VOLUME OF BODY-FLUID
ALEX F. MULLERM.D.
ANNE M. RIONDELIng. chem.
RENÉ S. MACHM.D.
From the Department of Medicine in the University of Geneva,Clinique Therapeutique, Hôpital Cantonal
VASOPRESSIN, a long-acting extract of the posterior lobeof the pituitary gland, administered to normallyhydrated people for three days, produces acute retentionof water, and the resulting abnormal increase of the
body-fluid evokes, by homceostasis, renal loss of sodiumand chloride (Leaf et al. 1953). The urinary excretionof sodium has also been increased by acutely overloadinghealthy people with water (Stewart and Rourke 1942)and by giving an infusion of hypotonic saline solution(Strauss et al. 1952).According to Leaf et al. (1953) this loss of electrolyte
can be prevented by administering either corticotrophinor a low-sodium diet. Since the latter stimulates the
urinary excretion of aldosterone, it seems reasonable toassume that the increased renal excretion of sodiumwhich follows the increase of body-fluid may be due todiminished production of aldosterone, and that the
striking retention of sodium after vasopressin has beenwithheld might be secondary to increased secretion ofaldosterone by the suprarenal cortex.
Methods
The subject studied was a healthy man, aged 32, maintainedon a constant low-sodium diet and a fluid intake of 2000-2500ml. a day. After an initial control period posterior-pituitaryextract was administered intramuscularly as vasopressintannate in oil every twelve hours.Urine was collected every twelve or twenty-four hours, from
7 A.M. and analysed for sodium in a flame-photometer. The
urinary 17-hydroxyeorticoids were determined according toa modification of Reddy’s method (Hertoghe et al. 1955).Aldosterone was analysed chromatographically after acidifica-tion of the urine at pH 1 for twenty-four hours (method dofNeher and Wettstein [19.35]).*
Results
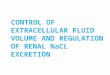
The accompanying figure shows the typical response ofa healthy person to vasopressin tannate over two and ahalf days, as described by Leaf et al. (1953). Theretention of water as the antidiuretic effect of vasopressinis seen in the abrupt decrease in volume of the urineand the corresponding increase in body-weight. As
expected, on the second and, especially, the third daysof administration of vasopressin the urinary sodiumincreased. Though the appearance of increased excretionof electrolytes was delayed, making a direct action of
vasopressin on sodium very unlikely, there was an
immediate decrease in the urinarv excretion of aldosteronefollowing the retention of water and the abnormal increaseof body-fluid. It is therefore highly probable that thisdecreased urinary excretion of aldosterone, as a directconsequence of increase of body-fluid, caused secondarilythe delayed renal loss of sodium.The withholding of vasopressin was followed by a
large water diuresis and a, loss of body-weiglit. This
significant diminution of body-fluid took place pari passuwith an increased urinary excretion of aldosterone. Thelatter was the immediate cause of the pronouncedretention of sodium three days after vasopressin hadbeen withheld. The fact that the urinary excretion ofaldosterone remained high for several days s can be
explained by the body-fluid volume expressed as body-weight being below the level found at the beginningof the study.*We wish to thank Dr. A. Wettstein and Dr. R. Neher for their
valuable help in setting up this method in our laboratory.
During the whole of this investigation the amountof urinary 17-hydroxycorticoids did not show anysignificant change.
Discussion
Leaf et al. (1953) interpreted the renal loss of sodiumresulting from retention of water as a homceostaticresponse to abnormal increase of body-fluid. That thisincreased urinary excretion of electrolytes in man is adirect effect of decreased production of aldosterone is
suggested by the results of the present study. The
sequence of events after the administration of vasopressinis as follows : (1) retention of water; (2) decrease ofsecretion of aldosterone as a hoiiiofostatic response toincrease of body-fluid ; and (3) increase in urinaryexcretion of sodium as a direct consequence of thediminution of aldosterone.
Withholding the vasopressin reverses the process :(1) a large water diuresis causes a loss of weight ; (2) thediminution of body-fluid stimulates the production ofaldosterone ; and (3) pronounced renal retention ofsodium.The significant variations in the amount of aldosterone
excreted, in spite of a constant amount of 17-hydroxy-corticoids excreted throughout the whole study, stronglysuggest an adaptive mechanism which, independent ofany effect of corticotrophin and acting through somevolume of body-fluid, regulates the secretion of aldos-terone in favour of homceostasis. In a recent similar
experiment (A. F. Muller and A. M. Riondel, unpublished),however, exogenous corticotrophin was found to influencethe excretion of aldosterone. The " rebound " produc-tion of aldosterone after vasopressin has been withheldwas much increased and hastened by an injection of
corticotrophin twelve hours after the last dose of vaso-
Effect of vasopressin on body-weight, volume of urine, and urinaryexcretion of sodium, 17-hydroxycorticoids, and aldosterone. The
relatively high values of aldosterone are due to the constant low-sodium diet with its effect on the volume of the body-fluid.

832
pressin. Other experiments (Falbriard et al. 1955)indicated that the secretion of aldosterone was possiblystimulated by corticotrophin.
Conclusion
Our experiment demonstrates a homceostatic mecha-nism affecting the secretion of aldosterone as a con-
sequence of changes in the volume of body-fluid. This
regulation seems to be independent of the pituitary-adrenal system. Liddle et al. (1955) note a diminutionof the sodium-retaining factor in the urine of dogs andman after the administration of vasopressin, and theysuspect that it is not the serum-sodium level but thevolume of the body-fluid that influences the secretion ofaldosterone. Apart from this homceostatic regulation ofthe production of aldosterone by some volume of body-fluid, the production of aldosterone probably also dependson corticotrophin. Studies are now in process to establishwhich fluid compartment may be involved in thishomoeostatic regulation of aldosterone.
SummaryEvidence is presented that the urinary excretion of
aldosterone is controlled by some volume of the body -fluid.This homeeostatic regulation of the secretion of
aldosterone is independent of the secretion of cortico-
trophin, but corticotrophin nevertheless can also influencethe secretion of aldosterone independently.
REFERENCES
Falbriard, A., Muller, A. F., Neher, R., Mach, R. S. (1955) Schweiz.med. Wschr. 85, 1218.
Hertoghe, J., Crabbé, J., Duckert-Maulbetsch. A., Muller. A. F.(1955) Acta endocr., Copenhagen, 20, 139.
Leaf, A., Bartter, F. C., Santos, R. F., Wrong, O. (1953) J. clin,Invest. 32, 868.
Liddle, G. W., Bartter, F. C., Duncan, L. E. jun., Barber, J K.,Dolea, C. (1955) Ibid. 34, 949.
Neher, R., Wettstcin, A. (1955) Acta endocr., Copenhagen, 18. 386.Stewart, J. D., Rourke, G. M. (1942) J. clin. Invest. 21, 197.Strauss, M. B., Davis. R. K., Rosenhaum, J. D., Rossmeisl, E. C.
(1952) Ibid. 31, 80.
INGUINAL ENDOMETRIOSIS
THOMAS L. DORMANDYM.B. Lond., B.ès Sc. Geneva
LIEUTENANT, R.A.M.C.; LATE SURGICAL REGISTRAR,HACKNEY HOSPITAL, LONDON
IN 3 patients seen within five months in the surgicaloutpatient department of the Hackney General Hospitala fairly confident clinical diagnosis of inguinal endometri-osis was confirmed.
This rare condition was first reported by Cullen in1896. Thirty years later Polster, in a collective review ofover 1000 cases of endometriosis, found 34 inguinal lesions,including intraperitoiieal and the apparently less commonextraperitoneal deposits.
There was no inguinal localisation in a number of laterseries (Pumphrey 1937, Moss 1939, Dreyfuss 1940, Colcock andLamphier 1950) ; but a very unusual case was included inSanders’s survey (1943) : a patient who bled from a sinusopening in the groin, during her periods. Masson (1945)reviewing 2686 recorded cases of endometriosis, affecting 4365sites, found no example of inguinal endometrioma though henoted 2 cases with deposits in femoral hernial sacs. Fallonet al. (1950) found 1 in 400 cases of external endometriosisand Scott and Te Linde (1950) 4 in 514 cases.
In 1954 Daro et al. wrote :" In a survey of the 3250 cases of external endometriosis
reported during the past 17 years, there were only 26 (0-8%)in which the condition was localised in the round ligament,and only 13 (0-4%) in which it was definitely demonstratedto be in the extraperitoneal part."This bears out Counsellor’s statement (1948), that con-trary to what the close anatomical relationship betweenpelvic organs and inguinal canal would lead one to expect,the latter is one of the rarest sites of endometriosis.
Fig. I-Operative exposure of the inguinal endometrioma in case I.The canal of Nuck has been opened.
Among individual cases described in clinical detail are thoseof Cullen (1920), Sampson (1925), Dickinson (1939), Lyall(1945). Mazza (1949), Rubinstein and Kurzon (1952), Daroet al. (1954), and Labry and de Mourgues (1954).
Case-reportsTIIE FIRST CASE
A, aged 3S. was referred to the outpatient departmentwith " recurrent inguinal lymphadenitis." She gave a fifteen
years’ history of a painful lump in her right groin whichregularly increased in size two or three days before her periods.At the same time the pain and tenderness became more intense.She had already had two courses of’ injections-one from herown doctor, and one in the casualty department at anotherhospital-but neither had benefited her more than temporarily.
During her most recent menstrual period the pain in hergroin had kept her confined to bed for seven days and hadreduced her to exhaustion.
Apart from the inguinal pain she had never suffered fromany form of menstrual discomfort, intermenstrual bleeding,vaginal discharge, backache, or dyspareunia. During the pastten months she had noticed a lengthening of the intermenstrualperiod and a diminishing loss. Her general health was excellent.
She had one son, aged 17, whose delivery had been normal.Three years after his birth she was operated on for a righttubal pregnancy. Three years after this she had a miscarriage.Exall/inationA lower right paramedian abdominal incision was soundly
healed and not tender. There was moderate tenderness anddiffuse induration over the right external inguinal ring, butno redness, subcutaneous oedema, or enlarged lymph-nodes.A faint but definite cough impulse was present in both groins.Rectal and vaginal examination were negative. The diagnosisof endometriosis of the canal of Nuck was made.
OperationThrough an inguinal skin-crease incision a grey mass of
fibrous consistence, the size of a cherry, was displayed. It
overlapped the external ring and was densely adherent to theexternal oblique aponeurosis, the emerging round ligament,and the fat of the abdominal fascia. The inguinal canalcontained an empty indirect hernial sac which reached thefibrous mass and was inseparable from it. On opening the sacthe glistening peritoneal surface appeared intact (fig. 1).The sac was divided and its proximal end closed. In separatingand removing the distal part, together with the fibrous noduleand round ligament, small cysts were entered, and dark fluidescaped. The internal ring was obliterated, the inguinalcanal reinforced with floss nylon darn, the external obliqueaponeurosis sutured, and the skin closed with drainage.Follow-upThe patient made an uneventful recovery. Since her
discharge she has had several menstrual periods withoutrecurrence of symptoms.

















![Aldosterone and dopamine receptors in the kidney: Sites for ...Aldosterone and dopamine receptors 625 with the aldosterone receptor, when measured in vitro [21, 23] (Funder and Adam,](https://img.dokumen.tips/doc/110x75/608977add019a330f10765d3/aldosterone-and-dopamine-receptors-in-the-kidney-sites-for-aldosterone-and.jpg)