Embed Size (px)
Citation preview

Contraceptive 326
Dr.HazarDr.Hazar

ObjectivesObjectives List the drugs and mechanisms used to attenuate
the actions of sex hormones.Ex. Gonadotrophines releasing hormones ;agonists
&antagonists.
Understand the Types ,MOA,S.E ,uses & C.I. of the hormonal contraceptive drugs.
Understand the Types ,MOA,S.E ,uses & C.I. of the fertility drugs.

Gonadotrophines releasing hormones agonists &antagonists.
1.danazol &danazol analogues1.danazol &danazol analogues 2.gonadorelines analogues2.gonadorelines analogues 3.fertility drugs3.fertility drugs
1.danazol &danazol analogues1.danazol &danazol analogues
Danazol 1.Gonadotropin inhibitor with
antiestrogen ,progestational and androgenic properties
2.synthetic version of the male hormone testosterone2.synthetic version of the male hormone testosterone
3.inhibits the release of FSH and LH by the pituitary 3.inhibits the release of FSH and LH by the pituitary glandgland
4.decreases estrogen levels similar to menopause, stops 4.decreases estrogen levels similar to menopause, stops ovulationovulation
5.shrink abnormal implants5.shrink abnormal implants


Danazol
Indications:
1.Endometriosis
2. Mammary dysplasia (fibrocystic breast nodularity)
3. Menorrhagia ;(but not contraception).
4.Gynaecomastia.

Danazol
Side effects androgenic effects (deepening of the voice, of the voice,
abnormal hair growth, reduced breast size, abnormal hair growth, reduced breast size, water retention, water retention, acne, weight gain ;nearly weight gain ;nearly all gain weight between 8-10 lbs.all gain weight between 8-10 lbs.)
hypoestrogenic reactions (flushing, sweating, vaginal dryness, irritation)
amenorrhea irregular vaginal bleeding, muscle cramps

Danazol analogues
1-Gestrinone is danazol agonist
Ditto action –danazol
Used only in Endometriosis
2-2-CetrorelixCetrorelix-LHRH antagonist -LHRH antagonist ↓↓FSH &LH FSH &LH used in infertility.used in infertility.
3-3-GanirelixGanirelix-ditto-ditto

2.Gonadorelines analogues
Continuos use
1.1. ↓↓ Gonadotropines Receptors and sensitivity in the Pituitary ; Down regulation
2.2. ↓ ↓ LH,FSH ;estrogen level ↓LH,FSH ;estrogen level ↓
3.3. No ovulationNo ovulation
4.4. ↓ ↓ endometriumendometrium

Treatment
Endometriosis Polycystic ovarian Disease Prostate Cancer Precocious Puberty Breast Cancer

2.Gonadorelines analogues
Pulsatile use1. Activation of natural Gonadotropines
pituitary Receptors to stimulate release of FSH and LH
Indication
Induction of ovulation invitro fertilization

Types of Gonadorelines analogues

GnRH Analogues
NafarelinNafarelin-nasal spray approved in 1990-nasal spray approved in 1990
-200x>potent than natural LHRH-200x>potent than natural LHRH
-relieves symptoms and shrinks implant or stops -them from -relieves symptoms and shrinks implant or stops -them from growinggrowing
-puts body into menopausal like state-puts body into menopausal like state
-side effects:-side effects:
hot flashes; vaginal dryness; lighter, lesshot flashes; vaginal dryness; lighter, less
frequentor no menstruation; headaches; nasal irritationfrequentor no menstruation; headaches; nasal irritation
-should not be used in women who are pregnant, breast -should not be used in women who are pregnant, breast feeding, or have undiagnosed vaginal bleedingfeeding, or have undiagnosed vaginal bleeding

Goserelin
· Made specifically for treatment of endometriosis in 1990
· by decreasing the amount of estrogen in the body, the body is induced into a menopausal state
· may be administered by a subcutaneous implant which is placed in the abdominal wall

Types of GnRH analogues+uses
Types EndometriEndometriosisosis
Prostate Prostate cancercancer IVFIVF Breast Breast
cancercancer
BuserelBuserelinin
++ ++
NafarelNafarelinin
++ ++
LeuprolLeuprolinin
++ ++
TriptorolTriptorolinin
++ ++
GoserelGoserelinin
++ ++ ++ ++

ContraceptivesContraceptives

Objectives 1. Understand the mechanisms by which oral
contraceptives prevent ovulation.
2. Know the potential adverse effects & containdication of oral contraceptive therapy .
3. Become familiar with the other type of contrceptives ( non oral ) REF 1. Katzung's. 2. Rang & Dale 3. Goodman and Gilman

Types of Oral Contraceptives Types of preparations
1. Combinations - contain an estrogen and a progestin given continuously for three weeks (most widely used).
a. High dose estrogen ≥ 0.05 mg (first generation)
b. Low dose estrogen < 0.05 mg, usually 0.02 - 0.035 (second generation)
c. Low dose estrogen with a lesser androgenic progestin (third generation)


2.Sequential Products2.Sequential Products
a. monophasic a. monophasic
b. biphasic b. biphasic
c. triphasicc. triphasic



Monophasic OC


3. Minipills-progestin only (block 3. Minipills-progestin only (block ovulation, slowing GnRH pulse ovulation, slowing GnRH pulse generation generation decreased LH surge) decreased LH surge)
For female with:For female with:
Venous thromboembolism , smoker, Venous thromboembolism , smoker, DM, HT, migrain & lactation.DM, HT, migrain & lactation.

4. Morning-After Pill (administer 4. Morning-After Pill (administer within 72 hrs of coitus, continue within 72 hrs of coitus, continue 2x for 5 days)2x for 5 days)

Emergency Emergency contraceptivescontraceptives
drugs used for the prevention of drugs used for the prevention of pregnancy following unprotected pregnancy following unprotected intercourse or a known or suspected intercourse or a known or suspected contraceptive failurecontraceptive failure
to be effective these must be taken within 72 to be effective these must be taken within 72 hours of intercoursehours of intercourse
two products are available:two products are available: Plan B: 0.75 mg Plan B: 0.75 mg levonorgestrellevonorgestrel Preven: 0.25 mg Preven: 0.25 mg levonorgestrel levonorgestrel and 0.05 mg and 0.05 mg ethinyl ethinyl
estradiol estradiol (this product includes a pregnancy test kit)(this product includes a pregnancy test kit)


Mechanism of Action
Combination Inhibition of ovulation via continuous negative feedback
on hypothalamic-hypophyseal axis (LH/FSH suppressed, no LH surge)
Progesterone decreases the frequency of GnRH pulses Changes in the Endometrium Thickens cervical mucus- difficult sperm penetration Changes in the Fallopian Tube Prevent follicular maturation

M.O.A Progestins alone
1.There is variable suppression of FSH, LH and ovulation. Menstruation may occur with irregular cycles.
2. Altered endometrial structure may prevent implantation and heavy cervical mucus may prevent sperm penetration.
3. Continuous use lends itself to long-acting preparations - intramuscular, subcutaneous, or intrauterine depots (medroxyprogesterone acetate, levonorgestrel).

NamesNames
Combinations Estrogens: Ethinyl estradiol ,Mestranol Progestins : levonorgestrel , Norethindrone Progestins-only Levonorgestrel , norethindrone,
ethynodiol diacetate

Morning-After
DiethylstilbestrolDiethylstilbestrol Norethindrone Ethinyl estradiol + levonorgestrel Postcoital IUD contain Cu (best)

Other oral preparations:
Ethinyl estradiol + norethindrone
Ethinyl estradiol + ethynodiol diacetate
Ethinyl estradiol + norethynodrel Ethinyl estradiol +
levonorgestrel

Adverse effects
Estrogen-related
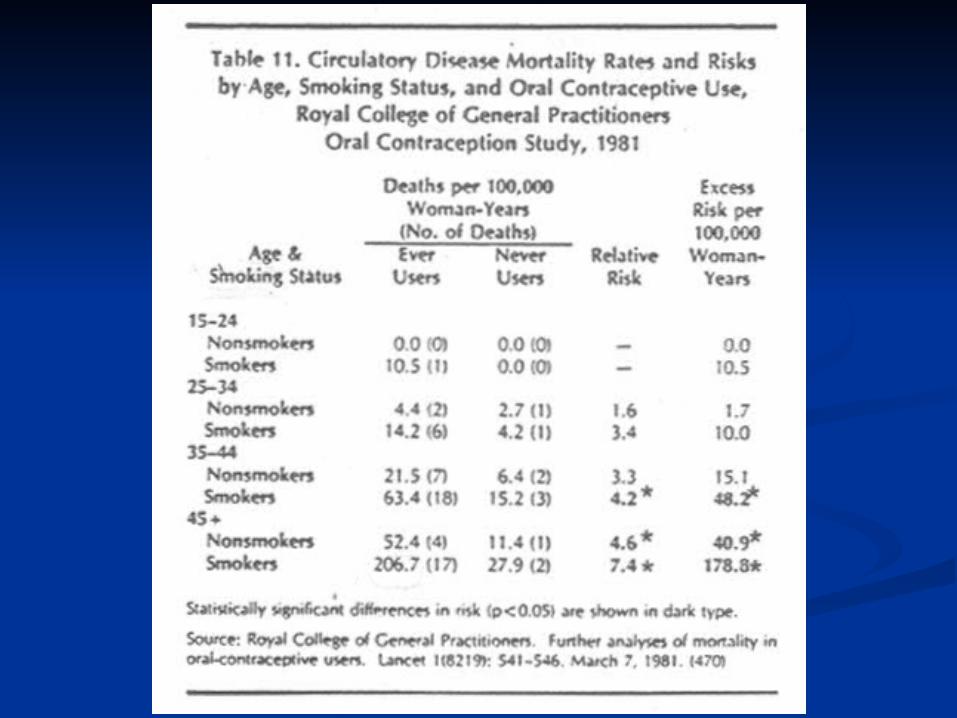
1.Cardiovcascular Disease a. Deep vein thrombosis b. Thromboembolism
Thromboembolic disorders due to effects on Thromboembolic disorders due to effects on clotting factors and platelet aggregation clotting factors and platelet aggregation properties; myocardial infarction; strokeproperties; myocardial infarction; stroke

• Nausea, vomiting • Edema (weight gain, breast engorgement) due to salt and
water retention • Headaches, dizziness • Hypertension resulting from salt and water retention and
increased hepatic secretion of angiotensinogen • Breakthrough bleeding • Urinary tract infection • Folic acid deficiency • Increased serum triglycerides • Dysmennorrhea • Ocular changes • Chloasma • Gall bladder disease related to increased cholesterol
precipitation due to a decrease in bile flow

• Decreased glucose tolerance via lowered sensitivity to insulin; possibly related to estrogen-stimulated release of insulin-antagonistic hormones (e.g., GH, T3+4, cortisol).
• Carcinogenesis a. breast b. endometrial c. ovarian d. cervical e. hepatic

Progestin-related
Depression - possibly related to increased MAO activity
Headaches Loss of hair and/or hirsutism, acne-
associated with 19-norsteroids Yeast infections

Contraindications to Oral Contraceptive Use
Current or past history of deep vein thrombosis, stroke, coronary artery disease, or hypertension
Cancer of the breast Strong family history of the above Active liver disease Heavy cigarette smoking Stroke - smokers
over 35

Types of non oral contrceptives
1.Barrier-condom1.Barrier-condom 2.Devices-IUD 2.Devices-IUD – (levonorgestrel,Cu),Cap.,Cap. 3.Spermicidal-Nonoxinol (creams and gels).3.Spermicidal-Nonoxinol (creams and gels). 4.Injections4.Injections
Monthly injectable – medroxyprogesterone1/12Norethisterone 8/525.Vaginal ring - ethinyl estradiol + etonorgestrel6.Patch - ethinyl estradiol + norelgestromin7. Levonorgestrel implantsLevonorgestrel implants . .

Levonorgestrel Levonorgestrel Intrauterine Device Intrauterine Device
Releases 20 µg Releases 20 µg levonorgestrelevonorgestrel each dayl each day Indicated for contraceptionIndicated for contraception 80%–90% reduction in menstrual blood loss 80%–90% reduction in menstrual blood loss
(not associated with copper-T IUD)(not associated with copper-T IUD) Also effective in treating menorrhagia, Also effective in treating menorrhagia,
endometriosisendometriosis Use up to 5 yearsUse up to 5 years Side effects: breakthrough bleeding, Side effects: breakthrough bleeding,
ovarian cysts, acneovarian cysts, acne Cost effectiveCost effective
.

LevonorgestrelLevonorgestrel-releasing intra uterine system -releasing intra uterine system Progesterone releasing IUDProgesterone releasing IUDSuperior to oral progesterones reduces MBL by Superior to oral progesterones reduces MBL by
96%96%64% women cancelled hysterectomy compared to 64% women cancelled hysterectomy compared to
14% on14% onmedical treatment, effective contraceptivemedical treatment, effective contraceptiveSuppresses development of endometrium but does Suppresses development of endometrium but does
not not suppress ovulation suppress ovulation Effective for 5 yearsEffective for 5 years90% women menorrhagia cured in 3 months90% women menorrhagia cured in 3 months




Infertility

Ovulatory Dysfunction Ovulatory Dysfunction
Causes of ovulatory dysfunction:Causes of ovulatory dysfunction: polycystic ovary syndromepolycystic ovary syndrome hypothalamic anovulationhypothalamic anovulation hyperprolactinemiahyperprolactinemia premature and age-related ovarian premature and age-related ovarian
failurefailure luteal phase defectluteal phase defect

Polycystic Ovarian Polycystic Ovarian SyndromeSyndrome
Oligomenorrhea/amenorrhea and Oligomenorrhea/amenorrhea and hyperandrogenismhyperandrogenism
Prevalence: 5%. Among women Prevalence: 5%. Among women with O.D., 70% have PCOS.with O.D., 70% have PCOS.
Clinical evidence: hirsutism, acne, Clinical evidence: hirsutism, acne, obesityobesity
Lab evidence: elevated Lab evidence: elevated testosterone, elevated DHEA-S.testosterone, elevated DHEA-S.

PCOS: Treatment PCOS: Treatment ApproachApproach
Weight loss if BMI>30 Clomiphene to induce ovulation If DHEA-S >2, clomiphene + glucocorticoid
(dexamethasone) If clomiphene alone unsuccessful, try metformin +
clomiphene.

Endometriosis Medical Medical TreatmentsTreatments
Oral ContraceptivesOral Contraceptives ProgestinsProgestins Danazol D.O.C NSAIDsNSAIDs GnRH analoguesGnRH analogues