Embed Size (px)
Citation preview
CONTRACEPTION IN CONTRACEPTION IN EXTREME EXTREME REPRODUCTIVE AGEREPRODUCTIVE AGEDR DAHLIA ABD MALIK, O&G SPECIALIST, SGHDR DAHLIA ABD MALIK, O&G SPECIALIST, SGH
CONTRACEPTION IN EXTREME CONTRACEPTION IN EXTREME REPRODUCTIVE AGEREPRODUCTIVE AGE
ADOLESCENTADOLESCENT
PERIMENOPAUSAL PERIMENOPAUSAL
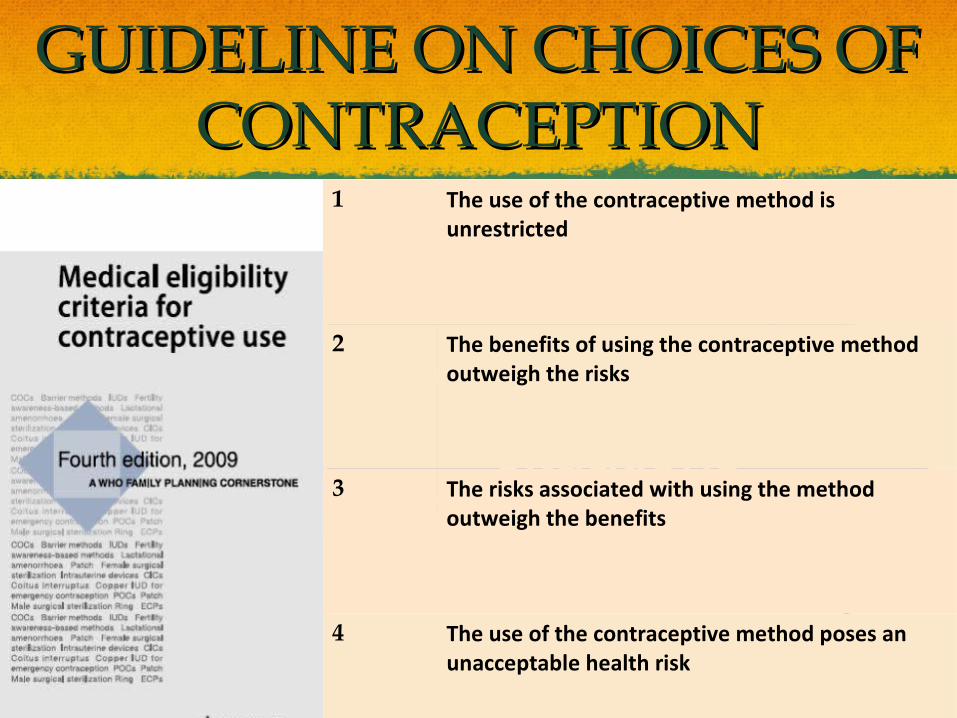
GUIDELINE ON CHOICES OF GUIDELINE ON CHOICES OF CONTRACEPTIONCONTRACEPTION
1 The use of the contraceptive method is unrestricted
2 The benefits of using the contraceptive method outweigh the risks
3 The risks associated with using the method outweigh the benefits
4 The use of the contraceptive method poses an unacceptable health risk

CONTRACEPTION IN CONTRACEPTION IN ADOLESCENTADOLESCENT
1. CAN OVULATION OCCUR 1. CAN OVULATION OCCUR DURING ADOLESCENCE?DURING ADOLESCENCE?
2. CAN PREGNANCY OCCUR 2. CAN PREGNANCY OCCUR DURING ADOLESCENCE?DURING ADOLESCENCE?
3. WHAT IS THE ADOLESCENT 3. WHAT IS THE ADOLESCENT FERTILITY RATE?FERTILITY RATE?
4. WHY IS THE PROVISION OF 4. WHY IS THE PROVISION OF CONTRACEPTION CONTRACEPTION IMPORTANT FOR IMPORTANT FOR ADOLESCENTS?ADOLESCENTS?
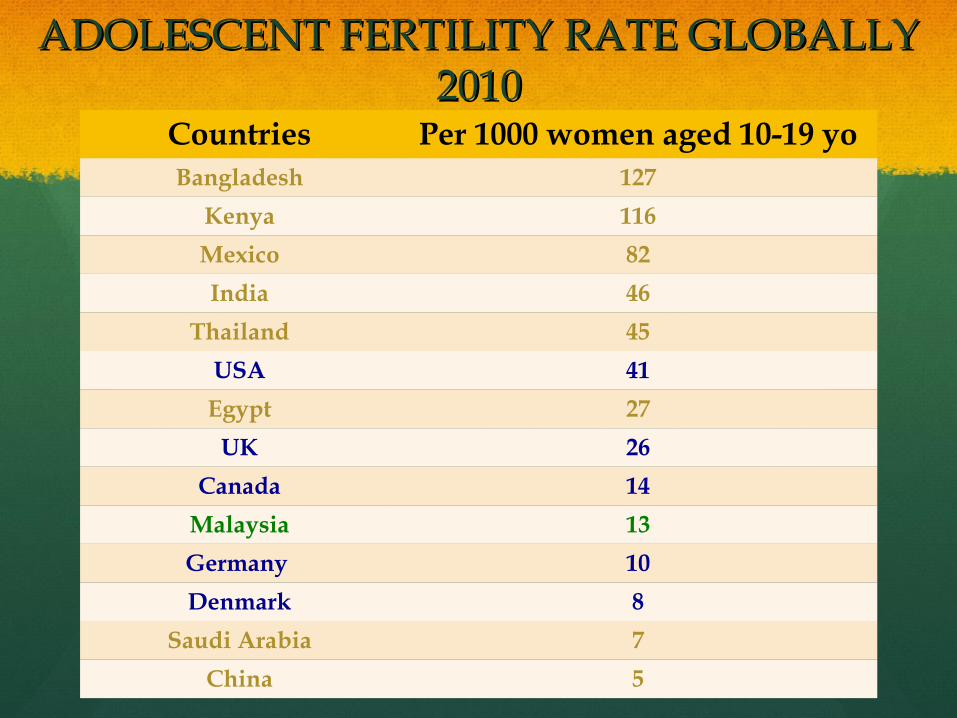
ADOLESCENT FERTILITY RATE GLOBALLY ADOLESCENT FERTILITY RATE GLOBALLY 20102010
Countries Per 1000 women aged 10-19 yoBangladesh 127
Kenya 116
Mexico 82
India 46
Thailand 45
USA 41
Egypt 27
UK 26
Canada 14
Malaysia 13
Germany 10
Denmark 8
Saudi Arabia 7
China 5

Consequences(of(unprotected(adolescent(sexual(intercourse((
Community)
Family)
Adolescent))$$$
Unprotected$adolescent$sexual$
intercourse$
Unwanted pregnancies STIs
Drop out of school Social outcast
Unsafe abortions Psychological problems
Shame Increased financial burden
Increased social and financial burden Baby abandonment
Increased health and safety concerns for baby
stigma
HIV and AIDs
Poverty

WHO WILL BENEFIT FROM WHO WILL BENEFIT FROM CONTRACEPTIVE ADVICES?CONTRACEPTIVE ADVICES?
A married adolescent who will benefit from spacing her A married adolescent who will benefit from spacing her pregnancies in terms of her health and care for her infantpregnancies in terms of her health and care for her infant
A sexually active adolescent with high-risk behaviorA sexually active adolescent with high-risk behavior
An adolescent who has been sexually assaultedAn adolescent who has been sexually assaulted
An adolescent following a wanted or unwanted An adolescent following a wanted or unwanted pregnancy regardless of her pregnancy outcomepregnancy regardless of her pregnancy outcome
An intellectually disabled adolescent at risk of abuseAn intellectually disabled adolescent at risk of abuse
A sexually active active adolescent with a chronic A sexually active active adolescent with a chronic medical conditionmedical condition
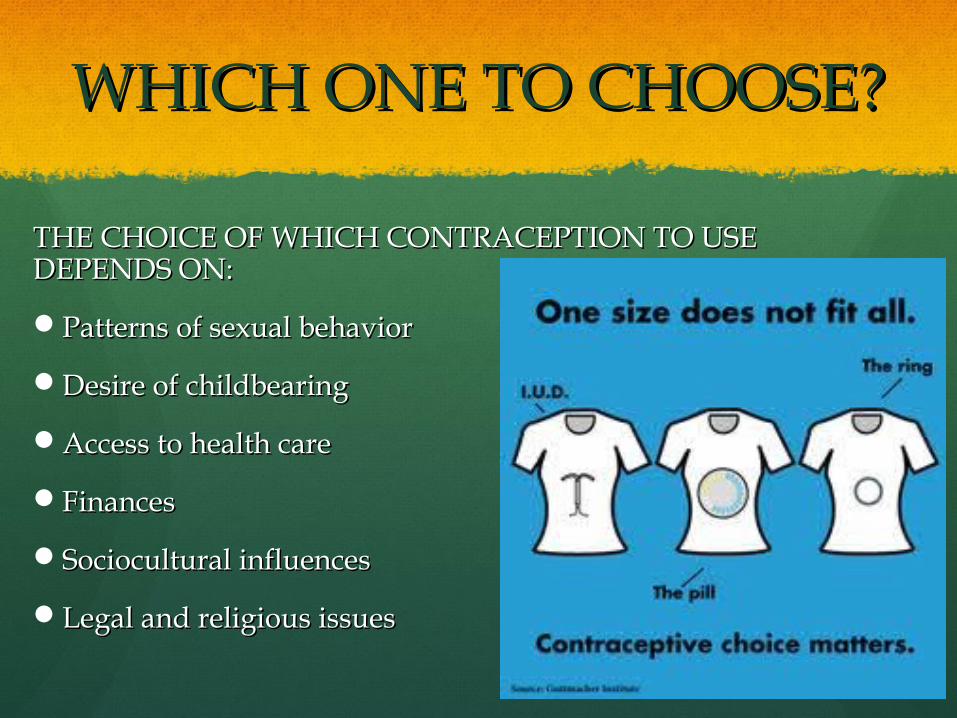
WHICH ONE TO CHOOSE?WHICH ONE TO CHOOSE?
THE CHOICE OF WHICH CONTRACEPTION TO USE THE CHOICE OF WHICH CONTRACEPTION TO USE DEPENDS ON:DEPENDS ON:
Patterns of sexual behaviorPatterns of sexual behavior
Desire of childbearingDesire of childbearing
Access to health careAccess to health care
FinancesFinances
Sociocultural influencesSociocultural influences
Legal and religious issuesLegal and religious issues

WHEN CONSIDERING WHEN CONSIDERING CONTRACEPTION FOR ADOLESCENTS...CONTRACEPTION FOR ADOLESCENTS...
Be aware of local laws and practicesBe aware of local laws and practices
DocumentationDocumentation
Encourage parental involvementEncourage parental involvement
Abstinence and also secondary abstinence should Abstinence and also secondary abstinence should always be emphasizedalways be emphasized
Condoms are important to prevent both unwanted Condoms are important to prevent both unwanted pregnancies and STIspregnancies and STIs
Education and reinforcementEducation and reinforcement

OPTIONSOPTIONS

CONTRACEPTIVE METHODS
WHO Age-specific Medical Eligibility Criteria
Strengths Weaknesses
Barrier 1 Offers protection from STIEasily available
Less protection against pregnancyCoital-relatedReliant on user
COC Unrestricted from menarche1
Highly effectiveOther non-contraceptive benefit
No protection against STIReliant on userMinor side-effectsHave to attend clinical service
POP Unrestricted from menarche1
Effective No protection against STIReliant on userMenstrual side-effects

CONTRACEPTIVE METHODS
WHO Age-specific Medical Eligibility Criteria
Strengths Weaknesses
Injectables 2 Easier complianceMore privateNot coitally-related
No protection against STIMenstrual side-effectsWeight gainDelay return of fertility
Implanon 1 Easier complianceMore privateNot coitally-related
No protection against STIAmenorrhea – may be unacceptableMinor operative procedure
Patch 1 Easier complianceMore privateNot coitally-related
No protection against STIReliant on usersPatch detachment

CONTRACEPTIVE METHODS
WHO Age-specific Medical Eligibility Criteria
Strengths Weaknesses
Intra-uterine system (Mirena)
2Restricted in an individual with high-risk of STI - 3
Highly effective protectionNot-coitally dependentReduces dysmenorrhea
No protection against STIAmenorrheaVE and invasive procedure requiredDifficult insertion in nulliparous
IUCD 2Restricted in an individual with high-risk of STI - 3
Highly effective protectionNot-coitally dependentReduces dysmenorrhea
Increased menstrual bleeding and painNo protection against STIVE and invasive procedure requiredDifficult insertion in nulliparous

EFFECTS OF CONTRACEPTION EFFECTS OF CONTRACEPTION ON ADOLESCENTSON ADOLESCENTS
Concerns about side effects and health risk Concerns about side effects and health risk discontinuation discontinuation
Weight gainWeight gain
Menstrual changesMenstrual changes
Mood changes and depressionMood changes and depression
Bone mineral densityBone mineral density
CVS effectsCVS effects
CancerCancer
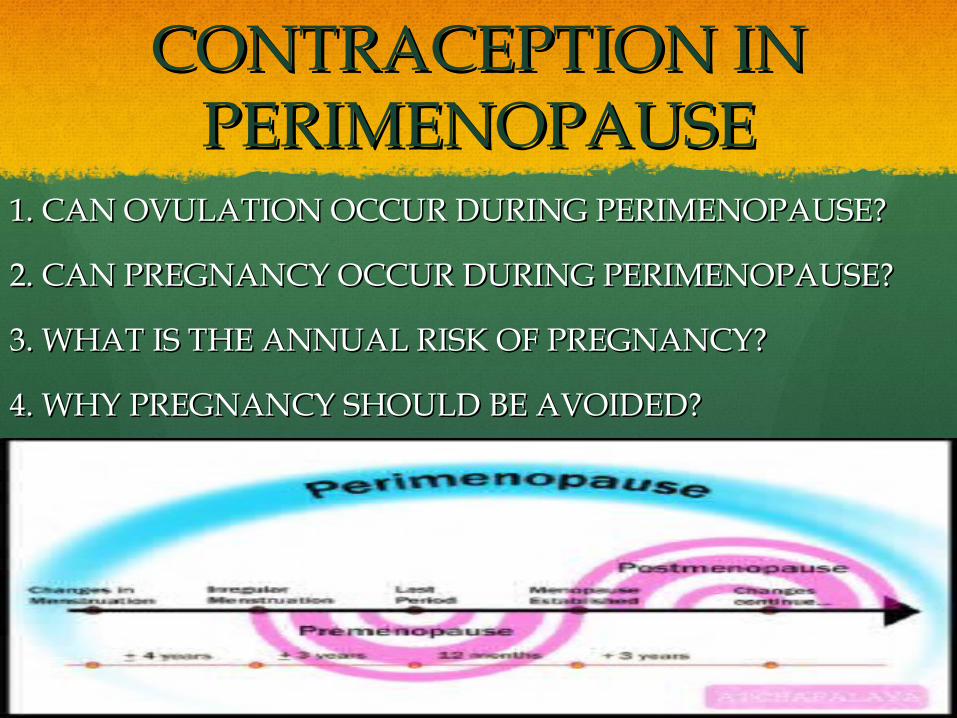
CONTRACEPTION IN CONTRACEPTION IN PERIMENOPAUSEPERIMENOPAUSE
1. CAN OVULATION OCCUR DURING PERIMENOPAUSE?1. CAN OVULATION OCCUR DURING PERIMENOPAUSE?
2. CAN PREGNANCY OCCUR DURING PERIMENOPAUSE?2. CAN PREGNANCY OCCUR DURING PERIMENOPAUSE?
3. WHAT IS THE ANNUAL RISK OF PREGNANCY?3. WHAT IS THE ANNUAL RISK OF PREGNANCY?
4. WHY PREGNANCY SHOULD BE AVOIDED?4. WHY PREGNANCY SHOULD BE AVOIDED?

MATERNAL DEATH BY MATERNAL DEATH BY AGE GROUPAGE GROUP
AGE 2001 2002 2003 2004 2005
15-19 3.0 - 3.3 1.6 4.8
20-24 10.0 11.4 8.2 14.7 8.8
25-29 24.1 22.2 19.6 21.2 24.8
30-34 26.5 20.6 32.0 27.6 24.8
35-39 21.1 28.2 21.3 25.2 23.2
40-44 11.8 16.0 131.1 8.9 12.0
45-49 3.5 1.5 2.5 0.8 1.6
Report on the Confidential enquires into Maternal Deaths in Malaysia ( 2001-2005)
WHICH ONE TO CHOOSE?WHICH ONE TO CHOOSE?
THE CHOICE OF WHICH CONTRACEPTION TO THE CHOICE OF WHICH CONTRACEPTION TO USE DEPENDS ON:USE DEPENDS ON:
Age-specific medical conditionsAge-specific medical conditions
Desire of childbearingDesire of childbearing
Access to health careAccess to health care
Sexual functionSexual function
Menstrual dysfunctionMenstrual dysfunction
OPTIONSOPTIONS

CONTRACEPTIVE METHODS
WHO Age-specific Medical Eligibility Criteria
Strengths Weaknesses
Barrier 1 More proficientFailure rates fall with increasing ageProtection from STI
Hypersensitivity to latexNon-hormonal – no benefits to those with menstrual problems and climacteric
Hormonal COCs 2Cautious in CVS disease, VTE, breast cancer
Non-smokers – no increased risk in CVS disease.50% reduced risk of endometrial & ovarian cancer (after 3 years usage and continues till 15 years after discontinuation.Symptomatic improvement of vasomotor symptoms.
Small risk of ischemic stroke (but not haemorrhagic stroke).Risk of VTE.24% risk of breast ca > 40yo.
CONTRACEPTIVE METHODS
WHO Age-specific Medical Eligibility Criteria
Strengths Weaknesses
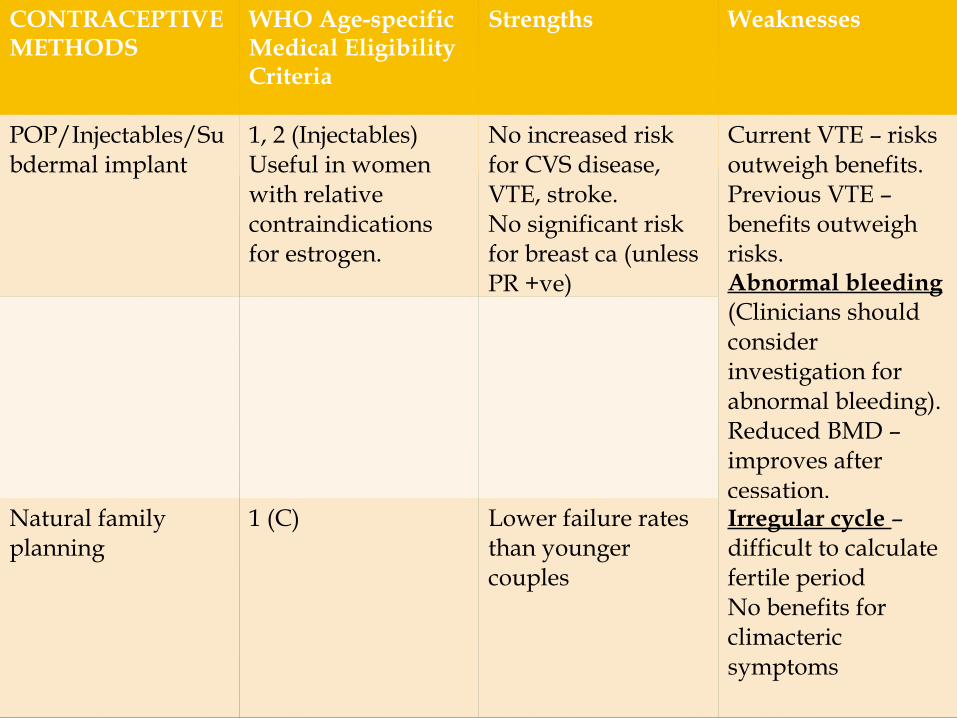
POP/Injectables/Subdermal implant
1, 2 (Injectables)Useful in women with relative contraindications for estrogen.
No increased risk for CVS disease, VTE, stroke.No significant risk for breast ca (unless PR +ve)
Current VTE – risks outweigh benefits.Previous VTE – benefits outweigh risks.Abnormal bleeding (Clinicians should consider investigation for abnormal bleeding).Reduced BMD – improves after cessation.
Natural family planning
1 (C) Lower failure rates than younger couples
Irregular cycle – difficult to calculate fertile periodNo benefits for climacteric symptoms
CONTRACEPTIVE METHODS
WHO Age-specific Medical Eligibility Criteria
Strengths Weaknesses
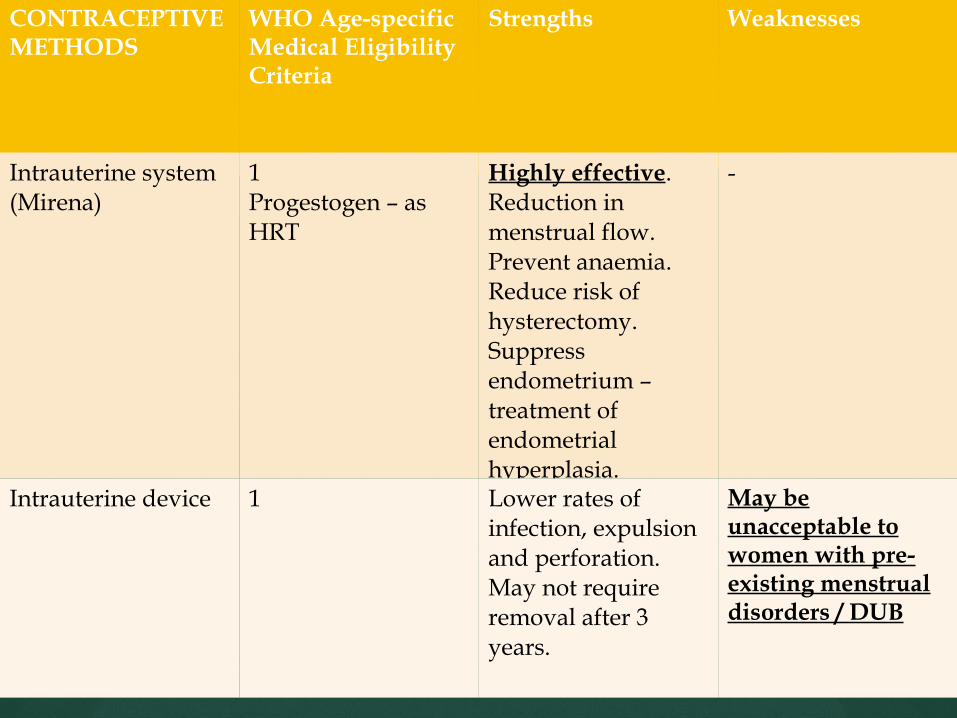
Intrauterine system (Mirena)
1Progestogen – as HRT
Highly effective.Reduction in menstrual flow.Prevent anaemia.Reduce risk of hysterectomy.Suppress endometrium – treatment of endometrial hyperplasia.
-
Intrauterine device 1 Lower rates of infection, expulsion and perforation.May not require removal after 3 years.
May be unacceptable to women with pre-existing menstrual disorders / DUB
CONTRACEPTION CONTRACEPTION & HRT& HRT
Contraception should be Contraception should be continued in women taking continued in women taking HRT who have not yet reached HRT who have not yet reached the menopause because the the menopause because the natural oestrogens contained natural oestrogens contained in HRT preparations are of in HRT preparations are of lower potency and dose than lower potency and dose than the synthetic oestrogen within the synthetic oestrogen within the COC and do not reliably the COC and do not reliably inhibit ovulation.inhibit ovulation.

WHEN TO STOP THE WHEN TO STOP THE CONTRACEPTION?CONTRACEPTION?
Continuation of contraception until 2 years of amenorrhea if the Continuation of contraception until 2 years of amenorrhea if the woman is aged <50 years as there may be a risk of ovulation, despite woman is aged <50 years as there may be a risk of ovulation, despite amenorrhea.amenorrhea.
The probability of menstruation (and possibly ovulation) after a year The probability of menstruation (and possibly ovulation) after a year of amenorrhea for women aged >45 years has been estimated by the of amenorrhea for women aged >45 years has been estimated by the WHO to be 2–10% .WHO to be 2–10% .
Women can be advised to stop contraception at the age of 55 years Women can be advised to stop contraception at the age of 55 years as most (95.9%) will be menopausal by this age.as most (95.9%) will be menopausal by this age.