Embed Size (px)
Citation preview
1

Contents
2
Introduction Page 4
Financial Management Page 6
QiPP Month 12 Page 7
Board Assurance and Risk Register Page 8
Performance Standards Page 19
Quality Assurance –CQRG Summaries Page 22
Quality Alerts Page 29
Serious Incidents and Never Events Page 30
Integrated Children and Young People Page 31
Integrated Adults Elective, Urgent Care and Cancer Page 43
Integrated Adults Older People Page 45
Integrated Adults Long Term Conditions and Medicines Optimisation Page 50
Integrated Mental Health Page 54
Learning Disabilities Page 62
Staying Healthy Page 65
Primary Care Development Page 71

Contents
3
Enablers
• Digital Page 71
• Business Intelligence Page 76
• Estates Page 78
• Organisational Development Page 79
• Equalities Page 80
• Involvement Page 81
• Workforce Page 82
• PALS Page 83
• Freedom of Information Page 84
Acronyms Page 85

4
Assura
nce
NHS Lambeth CCG agreed our Strategic Vision "Healthier Together" in November 2013, informed by the views of local people, stakeholders andpartners developed through the Big Lambeth Health Debate. 2018/19 is the final year of our CCG 5 Year Strategic Plan, and has been developed in thecontext of responding to the financial and performance challenges we face. One of the key strategic aims of the year ahead will be to meet thesechallenges, deliver our strategic aims, and to work with partners to shape and develop our next 5 year health strategy covering the period 2019 – 2024.
Through Lambeth Together, NHS Lambeth CCG and Lambeth Council, and with representatives from the Lambeth Patient Participation Groups andour partners, we will be building upon these existing relationships and continue our conversations on the next steps towards integration anddeveloping alliances that encompass all health and care activity in Lambeth as a fully Integrated Care System to address the challenges we face.
The strategic direction for the NHS as a whole has been set out by NHS England the Five Year Forward View (FYFV) in October 2014 and oversuccessive years the themes within it have been expanded and refreshed. We continue to commit to delivering the required outcomes of the FYFVrecognising that this is something that we can achieve by working with our key commissioner and provider partners including a broad range oforganisations across the NHS, independent and voluntary sector, as well as our Local Authority colleagues in public health and social care, and also thewider council.
We recognise that there are areas where we can only be delivering effectively by collective action of a wider group and there is added value to workingtogether at a south east London partnership and sometimes London scale. We continue to work in partnership with Bexley, Bromley, Greenwich,Lewisham and Southwark CCGs, our STP, NHS England, local authorities, local providers and other key stakeholders to deliver ‘Our Healthier South EastLondon’ a five-year Strategy for health and integrated care services across South East London. The South East London Sustainability andTransformation Plan forms an important roadmap for the future development and sustainability of the South East London health and care economy.
At a London wide level, NHS England (London), London’s 32 clinical commissioning groups (CCGs), boroughs, the Greater London Authority (GLA) andPublic Health England London (PHE London) considered the Five Year Forward View and Better Health for London. Together, they have ratified acollective vision to improve the lives of Londoners. Lambeth CCG is also committed to delivering on the London wide plan for Transforming PrimaryCare.
Local Care Networks (LCNs) are being developed to support everyone across south east London. Each borough is developing its own LCNs to respondto the different needs and characteristics of its community, with the details of how they work decided locally. Across Lambeth the LCNs involve healthand social care providers, voluntary sector services and local people working together to address all of someone’s issues. This includes self-care, widerinformal family, carer and community support, and broader issues affecting people’s health and wellbeing. Our aim is to move towards a system thatjoins up care, harnesses local community assets, and works with service users, families and carers to meet all their needs, whether physical,psychological or social.
At a local Lambeth level, in our “Healthier Together” Five Year Strategy 2014 to 2019 we clearly identify and articulate our vision for the future ofhealth and care in Lambeth.
We will increasingly work closely with Lambeth Council, and recognise the resource constraints within locality authority, particularly in social care, andthe challenges and priorities identified through the Joint Strategic Needs Assessment that inform our approach to reducing health inequalities forLambeth people.
Introduction

5
Assura
nce
Strategic Context

6
Director Christine Caton
Management Lead Sabera Ebrahim
The CCG is required by statute to meet certain financial duties to ensure that public funds are used appropriately. CCGs are required not to
exceed the revenue (administration and programme) and capital resource limits in any one year and to have cash balances of no greater than
1.25% of the monthly drawdown.
NHS Lambeth reported a surplus of £1,290K at the end of the year. This is 292k above our planned surplus. The CCG is reporting an
underspend position on Running Costs at month 12, living within the £22.50 per head Running Cost allowance for 2018/19.
Lambeth CCG’s cash balance at bank at the end of March was £232k. The national target of keeping the closing cash within 1.25% of cash
drawdown was met in March.
Susta
inabili
ty
Financial Management Sustainability
Performance DutyAnnual
Target
Performance
for the Year
Rag
Rating
Achieve Planned in year Surplus £988k £1,290k
Achieve Planned Historic Surplus £12,097k £12,097k
Revenue Expenditure does not EXCEED
Revenue Allowance£569.220m £567.930m
Capital Expenditure does not EXCEED
Capital Allowance£187k £186k
Capital Resource use on specified
matters does not exceed the allowanceN/A N/A
Revenue resource use on specified
matters does not exceed the allowanceN/A N/A
Revenue administration resource use
does not exceed the allowance£7.751m £6.957m

QIPP Analysis by Delivery Area
In 2018/19, QIPP plans totals £19,513k. The CCG had an original unidentified QIPP of £2.256m at the start of the year, and we are now
reporting delivery of this following other identified non recurrent savings
Susta
inabili
ty
7
Financial Management - QIPP Month 12 Sustainability
Annual Plan
LAMBETH CCG QIPP 2018-19
QIPP
Programme YTD Plan YTD Actual YTD Variance
QIPP
Delivered Variance
£'000 £'000 £'000 £'000 £'000 £'000
Acute 7,491 6,867 6,867 0 7,491 0
Mental Health 2,298 2,107 2,107 0 2,298 0
Prescribing 2,090 1,916 1,916 0 2,090 0
Primary Care 2,603 2,386 2,386 0 2,603 0
Continuing Health Care 401 368 368 0 401 0
Corporate & Communit Care 2,074 1,901 1,901 0 2,074 0
Running Cost 300 275 275 0 300 0
Qther QIPP Schemes (previously unidentified) 2,256 2,068 2,068 0 2,256 0
Total QIPP Savings 19,513 17,887 17,887 0 19,513 0
Forecast OutturnYear to Date

8
The NHS Lambeth CCG Board Assurance Framework (BAF) is included in this report, along with a Heat Map showing the number of risks at each score
for all risks recorded on Lambeth CCG’s Risk Register not just those scoring 12 or above. The BAF and supporting Risk Register are living documents,
updated regularly.
Leaders
hip
Risk Register Leadership
Risk Matrix Impact
Likelihood 1 Negligible 2 Minor 3 Moderate 4 Major 5 Catastrophic 5 4x4=16 2A1 Delivery of Medicines Optimisation Scheme
4x4=16 2M Community Nursing Vacancy Level
4x4=16 6C1 IT Service Delivery
4x4=16 7C QIPP delivery risk
4x4=16 7D Financial Planning Risk
5 3x4=12 2A Community Nursing Service Improvement Plan
3x4=12 3Q Alliance service transformation
3x4=12 3R Psychiatric bed demand
3x4=12 5ACPCC Sustainability of Federations
3x4=12 8E Premises needs at Crown Dale
9 4x3=12 6Q BCP Risk - loss of telecoms
4x3=12 6S BCP Risk - loss of utilities
4x3=12 6T BCP Risk - internet fraud
4x3=12 8B Lower Marsh Lease
4x3=12 8A Premises needs at Waterloo Health Centre
4x3=12 8C Premises needs at Nine Elms
4x3=12 6G1 Telephony offer to general practice
4x3=12 6I1 Building security and IG risk
4x3=12 6J1 NEL engagement with CCG IG process
Zero Tolernance Risks
2x5=10 1A Safeguarding children (Zero Tolerance Risk)
2x4=8 2B Safeguarding Adults
1 Rare
1x1=1 1x2=2
4x5=20
5 Almost Certain
1x5=5 2x5=10 3x5=15 4x5=20 5x5=20
4 Likely
4x1=4 4x2=8 4x3=12 4x4=16
3x5=15
2 Unlikely
2x1=2 2x2=4 2x3=6 2x4=8
3 Possible
3x1=3 3x2=6 3x3=9 3x4=12
1x3=3 1x4=4
Risks scoring 12 and above
1x5=5
2x5=10
6 3
5121
2 59
12

9
A summary of the NHS Lambeth CCG Board Assurance Framework (BAF) is included along with a Heat Map showing the number of risks at
each score for all risks recorded on Lambeth CCG’s Risk Register not just those scoring 12 or above. The BAF and supporting Risk Register
are living documents, updated regularly. The summary BAF tracks progress of risk scores over the previous 12 months. The full BAF is
included as an appendix to this report.
Three new risks have been added to the BAF:
2A1 ‘Risk that Non-Delivery of the Medicines Optimisation Scheme 2019-20 will impact on achievement of QIPP savings, CCG financial balance,
patients not receiving evidence based cost effective medicines
7C ‘There is a risk that the CCG will not deliver 100% QIPP in 2019/20. This will contribute to the in-year and underlying financial pressure for the
CCG’
7D ‘There is a risk that activity related expenditure is greater than budget in 2019/20 and that the current shortfall on the delegated primary care
budgets cannot be resolved’
The following risks have been removed from the BAF, as these are now being monitored at the SEL Integrated Governance and
Performance Committee and the SEL BAF will be available to IGC to review:
2U ‘Likely risk that acute trusts will not achieve improvement trajectories to meet 95% A&E target’
2V ‘Likely risk that the CCG will not achieve the improvement trajectory for meeting the access to cancer treatment as measured by the standard
for 62 days from GP referral to treatment impacting on the CCG quality premium and assurance framework’
2X ‘Risk that the number of long waiters (waiting more than 52 weeks) is not half (or less than) the level at March 2019 than it was at March 2018
resulting in long waits for patients’
2Y ‘Risk that the CCG is not able to maintain the PTL size at March 18 levels (The PTL size is the total number of patients on the waiting list)
increasing the challenge of trying to effectively manage care for patients waiting for elective appointments or treatment’
Other risks removed from the BAF:
2Z ‘Risk that Non-Delivery of the Medicines Optimisation Scheme 2018-19 will impact on achievement of QIPP savings, CCG financial balance,
patients not receiving evidence based cost effective medicines’. This has been re-framed for 2019/20 and replaced with risk 2A1.
5AFPCC ‘Risk that the allocation for NHS Lambeth CCG’s delegated primary care commissioning is not sufficient to meet forecast 2018/19
budgets’. This risk relates to the 2018/19 budgets so has been removed. The risk for 2019/20 is being assessed.
6M ‘There is a risk CCG data held on the incident management system is not securely protected due to gaps in the contract held with software
provider, resulting in a potential breach of data and loss of public confidence in the CCG’. IG review concluded that the GDPR addendum did not
have gaps relating to information governance. Issue to be resolved relates to indemnity and will be managed at directorate level.
7A ‘Possible risk that current planning and strategic approach is not sufficiently robust to manage pressures and deliver sustainable financial
position in the context of lower levels of growth in the period to 2020/21’ – this risk has been re-framed for 2019/20 and replaced by risk 7D.
7B ‘Risk of failure to deliver QIPP and acute over performance leading to CCG risk on financial sustainability‘ - this risk has been re-framed for
2019/20 and replaced by risk 7C.
There are currently 21 risks rated 12 or above (excluding Safeguarding Children and Adults risks).
Leaders
hip
CCG Board Assurance Framework Leadership

10
Leaders
hip
CCG Board Assurance Framework Summary Leadership
UPDATED May 2019
Ap
ril
Ma
y
Ju
ne
Ju
ly
Au
g
Se
pt
Oc
t
No
v
De
c
Ja
n
Fe
b
Ma
r
Ap
ril
Ma
y
Director of
Integrated
Commissioning
Children
1A
Zero Tolerance Risk - Risk of failure to safeguard children and identify
and respond appropriately to abuse 5 10 10 10 10 10 10 10 10 10 10 10 10 10 10
2A
Possible risk to service quality and safety of community nursing due to
failure to implement the Service Improvement Plan for Community
Nursing8 12 12 12 12 12 12 12 12 12 12 12 12 12 12
2BZero Tolerance Risk - Risk of failure to safeguard adults and identify
and respond appropriately to abuse 8 8 8 8 8 8 8 8 8 8 8 8 8 8 8
2MLikely risk service delivery due to vacancies in community nursing
resulting in inability to provide quality safe community nursing 16 16 16 16 16 16 16 16 16 16 16 16 16 16 16
2A1
Risk that Non-Delivery of the Medicines Optimisation Scheme 2019-20
will impact on achievement of QIPP savings, CCG financial balance,
patients not receiving evidence based cost effective medicines12 16
Corporate Objective 1.2: Quality,
Safety & Effectiveness - To
improve the quality and safety of
local services
ASSURANCE FRAMEWORK 2019/20 – PROGRESS
SUMMARY
Strategic AimExecutive
Lead
Risk
Register
Ref
Director of
Integrated
Commissioning
Adults
Target
Risk
Score
and
Direction
of Travel
Principal Risk (Obstacle to achievement of Strategic Aim)
2018 Monthly Progress 2019

11
Leaders
hip
CCG Board Assurance Framework Summary Leadership
UPDATED May 2019
Ap
ril
Ma
y
Ju
ne
Ju
ly
Au
g
Se
pt
Oc
t
No
v
De
c
Ja
n
Fe
b
Ma
r
Ap
ril
Ma
y
7C
There is a risk that the CCG will not delivery 100% QIPP in 2019/20. This
will contribute to the in-year and underlying financial pressure for the
CCG 8 16
7D
There is a risk that activity related expenditure is greater than budget in
2019/20 and that the current shortfall on the delegated primary care
budgets cannot be resolved8 16
Director of
Primary Care
Development
5ACPCC
There is a risk to the sustainability of the Lambeth GP Federations due
lack of capacity to deliver on contracts, resulting in a risk of the CCG
having to step in to manage and impacting on QIPP6 12 12 12
ASSURANCE FRAMEWORK 2019/20 – PROGRESS
SUMMARY
Strategic Aim
Corprate Objective 2.2:
Sustainable Delivery &
Governance - To ensure good
governance, financial stability of
the local health economy, VfM and
the delivery of statutory
responsibilities
Principal Risk (Obstacle to achievement of Strategic Aim)
Target
Risk
Score
and
Direction
of Travel
Executive
Lead
Chief Financial
Officer
Risk
Register
Ref
2018 Monthly Progress 2019

12
Leaders
hip
CCG Board Assurance Framework Summary Leadership
UPDATED May 2019
Ap
ril
Ma
y
Ju
ne
Ju
ly
Au
g
Se
pt
Se
pt
No
v
De
c
Ja
n
Fe
b
Ma
r
Ap
ril
Ma
y
6Q
Business Continuity Management Plan Risk - significant failure of the
major utility infrastructure as a medium risk which would mean a
widespread loss of the telecoms network for over a 24 hr period.
12 12 12 12 12 12 12 12 12 12 12 12 12 12 12
6S
Business Continuity Management Plan Risk - risk of a significant failure
of the major utility infrastructure as a medium risk resulting in a
widespread loss of the water, gas, electricity12 12 12 12 12 12 12 12 12 12 12 12 12 12 12
6T
Business Continuity Management Plan risk - risk that staff targeted by
internet fraudsters to gain access to secure servers, resulting in potential
major data breach/loss of secure patient data9 12 12 12 12 12 12 12 12 12 12 12 12 12 12
6I1
Risk of unauthorised access to personal confidential data due to poor
building security resulting in a data breach and potential financial
penalties6 12 12 12
6J1
Risk of incomplete assurance regarding information security due to lack
of engagement by NEL CSU ICT department in the information
governance processes in the CCG, resulting in potential risk to IT
systems and non-compliance with Data Security and Protection Toolkit.6 12 12 12
Strategic Aim
Corprate Objective 2.2:
Sustainable Delivery &
Governance - To ensure good
governance, financial stability of
the local health economy, VfM and
the delivery of statutory
responsibilities
Target
Risk
Score
and
Direction
of Travel
Executive
Lead
Risk
Register
Ref
Principal Risk (Obstacle to achievement of Strategic Aim)
ASSURANCE FRAMEWORK 2019/20 – PROGRESS
SUMMARY
2018 Monthly Progress 2019
Director of
Governance
and
Development

13
Leaders
hip
CCG Board Assurance Framework Summary Leadership
UPDATED May 2019
Ap
ril
Ma
y
Ju
ne
Ju
ly
Au
g
Se
pt
Se
pt
No
v
De
c
Ja
n
Fe
b
Ma
r
Ap
ril
Ma
y
3Q
Risk that the service transformation plans through the Alliance contract
fail to deliver planned improvements and savings resulting in financial
loss and lack of improved outcomes8 12 12 12 12 12 12 12 12 12 12 12 12 12
3R
Risk that demand for acute psychiatric beds is not reduced resulting in
poor outcomes for delayed transfers of care and negative financial
impact8 12 12 12 12 12 12 12 12 12 12 12 12 12
8ARisk of possible failure to plan for future premises needs - Waterloo
Health Centre Lease ends 20214 12 12 12 12 12 12 12
8C
Risk of possible failure to plan for future premises needs. Nine Elms
Vauxhall Business case does not adequately prepare for the influx of
residents up to 2021
4 12 12 12 12 12 12 12 12 12 12 12 12 12 12
8ERisk of possible failure to plan for future premises needs at Crown Dale
4 12 12 12 12 12 12 12 12 12
6C1
Likely risk of deteriorating IT service to Lambeth CCG and Lambeth
GP’s resulting in services being unable to operate effectively and safely8 16 16 16 16 16 16 16 16 16 16 16 16 16 16
6G1Risk to future Telephony offering to GP practices from NEL CSU after
migration to HSCN Network, resulting in lack of service2 12 12 12
Chief Financial
Officer8B
Risk of possible failure to plan for future premises needs when Lower
Marsh Lease ends 20174 12 12 12 12 12 12 12 12 12 12 12 12 12 12
Corporate Objective 3.1: System
Transformation - Commission
Proactive care focused on
prevention and early detection of
illness; Improve outcomes for
Lambeth patients, achieve better
value, integrated care through
transformation programmes in
partnership
Strategic AimExecutive
Lead
Risk
Register
Ref
Principal Risk (Obstacle to achievement of Strategic Aim)
Target
Risk
Score
and
Direction
of Travel
2018 Monthly Progress 2019
Director of
Governance
and
Development
Corporate Objective 3.2 System
Transformation - To ensure the
CCG’s commissioning resource
and organisational capability are
effectively aligned to deliver its
objectives
ASSURANCE FRAMEWORK 2019/20 – PROGRESS
SUMMARY
Chief Financial
Officer
Director of
Integrated
Commissioning
Adults

Better
Care
/Better
Health
Current Performance• March 2019 performance was 85.4% . This is a slight
deterioration from performance reported in February 2019.
• There were no trolley breaches in March 2019.
Drivers • Increased Attendances: Trust had 6.4% increase in ED attendances in March 2019 compared to March 2018. Most of the increase is from Majors,
Resus and paediatrics. • Staffing Gaps: Medical staffing gaps and a range of rota issues in both adults and paediatrics continued to impact performance in March leading to
difficulties keeping on top of surges of arrivals. • Flow/Beds issues: There has been improvement in the availability of general medical beds, with very few medical outliers compared to previous
years. However, increases in acuity have put pressure on ITU and HDU beds.
Performance – A&E GSTT Better Care/Better Health
14
Actions• A new governance structure is being implemented for the weekly A&E board, with each work stream focused on ED patient pathways and to ensuring
delivery of planned actions. The new structure will operate on a 4-week rolling programme: Week 1- Specialty pathways, Week 2 - A&E department (on the clock), Week 3 - Emergency floor (off the clock) and Week 4 - Oversight Group. Regular review of each work stream will support the achievement of the ED performance recovery plan.
• The new model of Ambulatory Emergency Care (AEC) & Medical Assessment Unit has been reviewed, together with NHS Elect, to review patients streaming to AEC and a process map has been completed, setting out the pathway between initial assessment and AEC, highlighting areas of delay in the pathway. This will be followed by; the establishment of escalation actions between ED and the AEC at times of surge in the ED, establishing a directory of all ambulatory pathways available in the trust to ensure everyone is aware of all services they can access, review of the Glasgow admission prediction score by completing an audit of patients who have been admitted to the admissions ward and reviewing portering support between ED and AEC to support earlier transfer of patients to AEC.
• A Majors Working Group has been set up to manage challenging performance in majors due to a sustained increase in attendances. The group is focussing on internal discharge and transfer processes. The group agreed to review the escalation protocol by ED SMT and the informatics team to refresh escalation triggers and actions as well as refresh the trust’s inter-professional standards, to improve specialty response times to the emergency floor and improve the flow of specialty patients.
• GP redirect: Business case will be written between GSTT and the GP hub to request an extension by Lambeth CCG and review of progress against this will be reported at next meeting.
• There are plans for the team to consider capacity in line with the BEST tool, review of nursing, review of administrative support and the consideration of introducing a new clinical fellow model which would support a higher rate of weekend working in line with the increase in attendances.
• Paediatrics staffing will be supported with the introduction of specialty roles to support emergency flow, including an extra plastics registrar and a surgical flow coordinator. There are plans for a staffing review of both the nursing and administrative establishment to match capacity to the increased demand.
• Flow/Beds: Flow to be supported by a refresh of the trust’s inter-professional standards, in order to improve specialty response times to the emergency floor and improve the flow of specialty patients.
Guy's & St Thomas' (GSTT) Jan-19 Feb-19 Mar-19
A&E Actual 87.5% 86.1% 85.4%
A&E National Target 95.0% 95.0% 95.0%
75%
80%
85%
90%
95%
100%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Guy's & St Thomas' (GSTT) - A&E Actual
Actual Trajectory A&E 4hr National Target Last Year

Drivers
Denmark Hill (DH)
• Poor patient flow through the system is impacting performance on both sites.
• Higher acuity patients seen with increased admission rates. • High staff turnover with increased number of vacancies across
medical and nursing staffing (PRUH).
Performance – A&E KCH Better Care/Better Health
Better
Care
/Better
Health
15
Actions• Hunter Healthcare working with the Trust to focus on driving flow on
both sites as key enabler to all aspects of the recovery programme.• On-going implementation of A&E Recovery plan. The plan has been
shared with NHSI and approved by the Trust Board• ECIST providing on-going support on clinical cultural change across
both sites.• Senior leadership team reviewing recruitment and retention
strategy.
Denmark Hill (DH)• London Ambulance Assessment Area (LASAA) opened on 21
December which the Trust state has helped significantly improve ambulance handover times.
• Stranded patient review in place for all specialties and increase in hours for the transfer team on-site from 10:00-22:00 to allow for early transfers from ED to support patient flow.
• Daily ED rhythm embedded via 2 hourly huddles (24/7) and daily breach review meeting.
• Streaming review underway supported by Hunter Healthcare.• Medical model for same day emergency care – plans being
developed for stand alone area • Adverts have been placed for 7x band 8a Emergency Nurse
Practitioner vacancies.• Joint weekly clinical meetings commenced between the Trust and
Hurley Group (UCC provider).• Re-provision of the seated ADU space due to be complete in May
which will provide an approved ‘clock stop’ area for patients.
75%
80%
85%
90%
95%
100%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
King's College (KCH) - A&E Actual
Actual Trajectory A&E 4hr National Target Last Year
0
5
10
15
20
25
30
35
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
King's College (KCH) - A&E Trolley Waits
Actual Last Year
King's Col lege (KCH) Jan-19 Feb-19 Mar-19
A&E Actual 80.3% 79.4% 81.5%
A&E National Target 95.0% 95.0% 95.0%

DriversGSTT• GP referrals remained higher than planned • Further increase in number of 40+ week waiters from 530 in February 2019 to
649 in March 2019. • High growth in PTL size and backlog of patients• Clinical/theatre capacity constraints in some specialities• Staff capacity issues in GMS and cleft servicesKCH• Shortfall in Bariatric operating capacity at the Trust• Capacity challenges on the Colorectal pathways
ActionsGSTT • An additional consultant has been recruited and will spend 40% of his
time doing cleft. Service is putting together a business case to recruit a highly specialised maxillofacial consultant and also drafting a business case to recruit a 5th consultant.
• Introduction of “Elective Weekly Rhythm” for operational management with associated KPIs to measure success / compliance.
• Establishment of a task and finish focus group to ensure operational grip and control of elective performance in each service, setting clear expectations of processes, performance management, roles and responsibilities and escalation.
• Transformation of outpatient processes which includes standardising processes, training and establishing a data quality dashboard to enable directorates to monitor the quality of their administrative processes.
• Acceleration of theatre build plans, incl. Queen Mary Hospital and Pain day case capacity - 2019/20 and St Thomas’s Main theatre capacity.
• Trust currently doing some work around validation of PTL and quality data improvement.
• Improvements in Waiting List Management processes have been implemented, through a range of initiatives as reported in previous Integrated Reports.
KCH• The focus of the Trust is delivering the planned reduction in long
waiting patients and therefore the current actions below will supportdelivery of this ambition:
• The Trust has secured additional capacity through outsourcing forchallenged specialties including Bariatrics, Colorectal andOrthopaedics.
• The Trust continues on-going validation of the PTL across the two sites.The validation work is also expected to identify patients who do notqualify for inclusion onto the inpatient list due to factors such as notbeing fit or eligible for surgery . This is expected to reduce the numberof long waiters.
• Continued direct oversight by senior management of theatrescheduling function for specialties with longest 52 week waiters; this isto ensure that patients are treated in a chronological order whereclinically appropriate.
• A new Trust wide governance system was launched in March which willfurther develop and embed over the coming months.
• Care Group PTL reviews in place supported by the RTT PerformanceManager.
• Weekly PTL meetings established on DH site led by the Chief OperatingOfficer. Meetings setup for PRUH site led by Deputy DirectorOperations for Planned Care.
• Clinical harm review process in place for all patients who breach 52weeks.
Performance – RTT Better Care/Better Health
Better
Care
/Better
Health
16
75%
80%
85%
90%
95%
100%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
NHS Lambeth CCG - RTT Incomplete Actual
Actual Trajectory RTT National Target Last Year
0
20
40
60
80
100
120
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
NHS Lambeth CCG - RTT 52 week waits
Actual Trajectory Last Year
10,000
12,000
14,000
16,000
18,000
20,000
22,000
24,000
26,000
28,000
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
NHS Lambeth CCG - RTT Incomplete Pathways
Actual Trajectory

Current Performance
In March 2019 there were 7 cancer 62 day breaches for NHS Lambeth CCG. The breaches were attributed to the following providers: Guy's And St Thomas' NHS Foundation Trust (5.5), King's College Hospital NHS Foundation Trust (0.5), St George's University Hospitals NHS Foundation Trust (1). The breach reasons reported were: Complex diagnostic pathway (2), Health Care Provider initiated delay (2), Patient choice (2), Treatment delayed for medical reasons (1).
Drivers• October – February 2019 deteriorating performance position at LGT. However, over the same period, performance at KCH has improved.• Urology/Prostate Pathway - Demand for 2WW still remains challenging. There has been a national step change in demand for this service over the course of 2018/19. Finding workforce at District
General Hospitals is an on-going challenge with PRUH in particular struggling in this area. • Diagnostic capacity and equipment - Demand has also impacted on the diagnostic phase of the pathway and aging diagnostic equipment particularly for CT, which requires replacement. CT Scanner
broken down at DH in August 2018.• Workforce - Challenge to recruit to short term posts due to ongoing turnover and sickness in key tumour sites• PTL and Backlog size – The system recognises that PTL and backlog size is currently too large, particularly at LGT.• Increased demand within SEL and from non SEL CCGs. • Delay in completing agreed actions at providers has pushed back expected performance improvement timelines.• Provider management capacity issues – Particularly at LGT operational grip has been a challenge due to management change and lost capacity.Actions (System wide)• SEL 2019/20 recovery plan and trajectories agreed. Completed 2018/19 actions moving into BAU. Trajectory for SEL to be above 85% from March 2020. Bilateral review meetings scheduled in May to
review risks and mitigations in local plans.• Diagnostic capacity and equipment - ACN funded outsourcing continuing into 2019/20 with SEL Diagnostic fund specifically for CT and MRI. • Network projects – long term plan to move to SEL network models for Urology and Dermatology. Network management lead recruited in January 2019. • Increased Oncology workforce – Further additional Oncology clinicians at GSTT to be recruited in 19/20 to reduce treatment times for Inter trust transfer patients. Further Oncology workforce review to
be conducted by ACN.• SEL system awarded circa £3.8 million of Cancer transformation funding for 19/20. Spend has been agreed for key projects and will be monitored through the ACN.• Move to 100% utilisation of 1 stop and STT pathways (Breast, Lower GI, Lung, Gynae, upper GI)• Reviewing joint appointment for Breast Radiologists between LGT and KCH.
Performance – Cancer Better Care/Better Health
17
Better
Care
/Better
Health
70%
75%
80%
85%
90%
95%
100%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
NHS Lambeth CCG - Cancer 2ww Actual
Actual Cancer 2ww National Target Last Year
50%
55%
60%
65%
70%
75%
80%
85%
90%
95%
100%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
NHS Lambeth CCG - Cancer 62 Day Actual
Actual Trajectory Cancer 62 day National Target Last Year

Performance – Diagnostics Better Care/Better Health
18
Better
Care
/Better
Health
Drivers• PRUH Endoscopy – historic increase in total demand (resulting in a backlog) coupled with utilising endoscopy capacity to support emergency pressures.• PRUH Echocardiography - capacity delivered at weekends was paused during October due to staffing constraints linked to a lack available agency back fills.• DH Cardiac Echocardiography: previous months staff sickness (impacting in hours and ability to cover weekend lists) and high inpatient demand.• DH Dexa Scanner – 15 breaches in March, many arising from patient choice (declining offers at Orpington and GSTT).GSTT• MRI - Increase in MRI demand and complexity of scan requested i.e. high demand for whole body and MRI Pelvis. • Endoscopy - Increase in endoscopy breaches due to: (1) inadequate levels of booking staff, (2) backlog of patients related to the eRS issue and (3) increase in colonoscopy & gastroscopy demand.• Echocardiography - Increase in backlog from 16 patients in February to 138 patients in March due to increase in demand.ActionsEchocardiography (both sites)
• DH - Additional temporary staff secured from mid January and continuing for April and May.
• Additional lists being undertaken during weekends.• Daily monitoring of waiting list by Principal Cardiac Physiologist Manager.
DH Dexa Scanner• New scanner installed and fully operational but Trust expects similar level of breaches during April (15) before compliance from May onwards.GSTTMRI• Undertaking a detailed review of referral demand for high level referring teams within GSTT and those referring patients for the complex/long scans, to better understand reasons behind this
with a view to reducing this internal demand. • Trust plan outsourcing contract with Alliance to provide additional capacity in the short term.• Undertaking a review into costings/feasibility for using scanning time on the KCL scanners based at GSTT in the medium term.• Fixed MRI capacity at weekends (8am-8pm) planned from February 2019.• Development of a full business case for the future purchase of 2 additional MRI scanners over the next 2 years. This MRI strategy/plan was presented and approved by the Trust Management
Executive (TME) in February.Endoscopy• Endoscopy breaches are all related to an eRS/admin issue which has now been resolved and all patients booked into this clinic have now been given an appointment.• Endoscopy service is currently out to advert for a third booking clerk for improvements in administration processes with timely scheduling of appointments, regular validation and also modelling
their demand and capacity.Echocardiography• Trust planned to use Evan Jones ward for inpatient scanning to improve capacity.• Service also planned to use another room in Guy’s to create an additional 124 slots and will be going live soon.• Saturday list – Service currently doing 3 lists per day and in process of implementing an extra 2 lists that will create 20 extra slots.• Business case put forward to procure additional 2 Echo machines to increase capacity.
NHS Lambeth CCG Jan-19 Feb-19 Mar-19
Diagnostic Actual 5.3% 2.6% 3.0%
Diagnostic National Target 1.0% 1.0% 1.0%
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
NHS Lambeth CCG - Diagnostic Actual
Actual Diagnostic National Target Last Year

Assurance : Performance Standards Acute standards Better Care/Better Health
Performance Measure Standa
rd
2018/19
Oct
-18
Nov
-18
Dec
-18
Jan
-19
Feb-
19
Mar
-19 Outturn
RTT Incomplete
pathway
92% 84.9
7%
84.27
%
83.5% 83.99% 84.5% 83.8% 83.8%
Diagnostic Waits >6
weeks
<1% 0.87
%
1.11% 2.52% 5.35% 97.3% 96.9% 1.8%
A&E waits (GSTFT) 95% 86.7
%
86.7% 81.64% 84.11% 82.78%
Cancer 2 weeks (GP
referral)
93% 93.1
8%
93.03
%
95.23% 93.02% 93.4% 94.6% 93.77%
Cancer 2 weeks (breast
symptoms)
93% 93.1
0%
93.02
%
95.12% 93.02% 97% 100% 92.86%
Cancer 31 days (first
definitive)
96% 95.9
2%
96.43
%
97.5% 95.18% 100% 100% 97.43%
Cancer 31 days
(subsequent - surgery)
94% 92.3
1%
100% 100% 92.86% 94.74% 100% 93.06%
Cancer 31 days
(subsequent - drug)
98% 94.5
9%
100% 96.15% 97.87% 100% 100% 98.21%
Cancer 31 days
(subsequent -
radiotherapy)
94% 92.6
8%
95.12
%
96.43% 97.92% 97.3% 100% 96.54%
Cancer 62 days (GP
referral)
85% 85.1
9%
82.35
%
87.81% 76.19% 85.45% 86.27% 83.89%
Cancer 62 days
(referral NHS
screening)
90% 40
%
75% 100% 100% 66.67% 75% 76.92%
Mixed Sex
Accommodation
0 0 7 3 2 3 3 24
19
Better
Care
/Better
Health

Performance Measure Operating
Standard
2018/19
Oct
-18
Nov
-18
Dec
-18
Jan
-19
Feb
-19
Mar
-19
Outturn
Proportion of people with depression
receiving for psychological therapy
19.2%
(4.75%
Rolling quarter
by Q4)
1.40% 1.50% 1.51% 1.81% 1.69% 1.4% 17.9%
4.9% (rolling
quarter)
Proportion who complete therapy who
are moving to recovery
50% 50.7% 44.1% 47.2% 52.80% 55.2% 52.1% 50.0%
Proportion of patients that finished a
course of treatment who received their
first treatment appointment within 6
weeks of referral
75% 94.2% 94.0% 94.2% 93.7% 94.4% 94.5% 94.5%
Proportion of patients that finished a
course of treatment who received their
first treatment appointment within 18
weeks of referral
95% 100% 100% 100% 100% 100% 100% 100%
Dementia diagnosis rate 67% 76.5% 76.7% 76.2% 75.5% 75.8% 80.1% 80.1%
Early intervention in psychosis 50% 56% 60% 71% 70% 66.8%
20
Better
Care
/Better
Health
National Performance Standards Non-Acute Better
Care/Better Health

Performance
Measure
Operating
Standard
2018/19
Oct
-18
Nov
-18
Dec
-18
Jan
-19
Feb
-19
Mar
-19 Outturn
Extended access
(evening and
weekends) at GP
services
100% 100% 100% 100% 100% 100% 100% 100%
Clostridium difficile
(C.Diff) cases
TBC 4 2 2 3 3 4 39
MRSA bacteraemia 0 0 0 2 0 0 1 5
21
Better
Care
/Better
Health
National Performance Standards Better Care/Better Health

Quality Assurance – GSTT CQRG March 2019 Leadership
22
Leaders
hip
Domain Indicator Unit Year Apr May June Jul Aug Sep Oct Nov Dec Jan Feb Mar Target
2018-19 2 0 2 2 1 3 1 1 3 2 5 1
2017-18 1 4 7 2 5 2 0 1 3 3 2 5
2018-19 2 3 3 3 3 0 3 3 0 4 3 2
2017-18 2 1 4 2 3 3 0 1 4 6 1 1
2018-19 1 2 2 1 5 3 2 0 0 no data 0 1
2017-18 2 2 1 5 0 3 1 4 1 4 1 5
2018-19 2 3 6 9 3 7 7 4 3 3 5 6
2017-18 2 2 3 3 4 3 3 8 5 5 3 4
2018-19 70 60 43 44 45 42 32 26 36 48 52 39
2017-18 35 33 28 40 38 44 49 50 50 51 34 46
2018-19 1 0 0 1 1 1 1 3 0 0 0 1
2017-18 0 0 2 0 2 3 1 0 1 0 1 0
2018-19 71.4 71.4 72 72 72 70 70 70 69.8 69.8 70.2 70.2
2017-18 72 72 73 73 76 76.5 72.5 71.3 71.3 72.8 72.8 73.4
2018-19 2 1 0 4 1 1 1 3 0 4 2 3
2017-18 2 1 2 5 3 3 3 2 2 1 3 0
2018-19 0 0 0 0 0 0 1 0 1 0 1 0
2017-18 0 2 2 0 1 0 0 0 0 0 0 0
2018-19 84.56% 83.91% 84.37% 84.56% 84.29% 83.54% 83.57% no data 83.97% 84.94% 84.69% no data
2017-18 80.44% 81.03% 82.05% 82.18% 82.57% 83.47% 82.45% 83.21% 82.77% 82.28% 82.39% 83.3%
2018-19 85.37% 83.72% 84.64% 85.53% 84.42% 83.45% 84.40% 84.46% 84.10% 86.22% no data 86.09%
2017-18 85.19% 85.30% 85.13% 83.81% 83.04% 83.04% 84.29% 83.94% 83.89% 83.94% 82.90% 84.99%
2018-19 79.75% 81.07% 81.34% 82.79% 82.81% 79.34% 77.89% 77.15% 77.18% 81.00% no data 83.02%
2017-18 82.23% 83.00% 82.49% 82.40% 82.40% 82.04% 78.42% 80.58% 80.44% 80.58% 80.04% 79.28%
2018-19 80.00% no data no data no data
2017-18 77.00% 77.00% no data no data
2018-19 94.00% no data no data no data
2017-18 93.00% 93.90% no data no data
2018-19 11.10% no data no data no data
2017-18 8.80% 10.02% no data no data
2018-19 10.90% 10.80% 10.90% 10.87% 9.80% 9.00% 9.40% 10.30% 10.52% 10.10% 10.40% 13.90%
2017-18 11.20% 11.53% 11.70% 11.90% 11.87% 11.00% 10.40% 10.10% 10.16% 10.40% 9.80% 10.30%
2018-19 84% 83.80% 84.30% 85.24% 85.60% 85.00% 85.20% 85.20% 85.20% 85.80% 86.50% 87.10%
2017-18 84.00% 84.24% 84.00% 84.34% 84.02% 84.00% 84.02% 84.00% 83.67% 83.70% 83.60% 84.60%
2018-19 114 126 110 125 140 120 147 129 126 133 136 144
2017-1892 114 113 117 118 81 94 133 95 118 97 100Pa
tien
t
Expe
ri
ence
Complaints opened in Month Number not spec
Staff Vacancy rate % <10%
Mandatory training compliance % >95%
Wel
l - le
d
Staff FFT - recommended as a place to work %
Safe
Incidents resulting in severe harm (STEIS) Number not spec
Incidents resulting in moderate harm (STEIS) Number
80%
80%
MRSA - number of cases (Trust -attributable) Number 0
Safeguarding % Adults Level 2 % 80%
Summary Hospital -level Mortality Indicator (SHMI) Ratio
Number 0
Staff FFT - recommended for care or treatment %
Staff FFT - Response rate %
Safeguarding % Children Level 2 %
Safeguarding % Children Level 3 %
>70%
>80%
not spec
Data source: Trust scorecards and performance reports as reported to CQRG
not spec
Patient falls with moderate or severe harm Number not spec
Pressure ulcer acquisitions (grade 2 and above) Number <5
<90
C-Difficile acquisitions (Trust attributed) Number <4pm
Admissions with pressure ulcers (grade 2 and above) Cases not spec
Never Events declared

The information provided in this section is a summary of discussions at CQRG meetings in March and April 2019. This meeting is attended by
senior Trust representatives, including the Medical and Nursing Directors, Clinical Commissioners and Directors of Quality from Lambeth and
Southwark Clinical Commissioning Groups (CCGs).
Key issues discussed at the March and April CQRG meetings:
Dental Services update on actions from never events - checklist developed and audit confirmed this is in use; Guidelines including Standard
Operating Procedures (SOPs) completed and shared with staff; presentation completed for dental nurses and will be part of training and audit
meetings; training packages to include videos for students around situational awareness; pictures of ‘how to use the checklist’ to be placed on
walls as visual aids.
Astley Cooper CQC Action Plan update: developing a resilience programme looking at teaching staff about mentoring and coaching in
conjunction with the Trust coaching lead; Matron appointed with sole area of responsibility for Astley Cooper and oversight of quality
improvement; regular team meetings; additional Band 2 staff approved in response to ‘speaking up’ survey; Psychology staff support regular
debriefs to facilitate discussion and teaching; Patients in custody policy approved.
Falls: main learning from falls relate to delirium, enhanced care and equipment. Forward plan to link learning within existing teams such as
delirium and pressure ulcers teams. Reduction in number of falls in Acute Medicine and Cardiovascular over the past year. Triangulating falls
data, other data and aspects of quality of care and focusing improvement work on particular areas such as haematology and oncology, transplant,
renal and urology. Plan to review and improve pathway for patients’ with dementia and delirium linked to on-going work around vulnerable adults,
mental health and older adults. The Trust is part of the NHSI collaborative enhanced care out of which has emerged a project around
identification of enhanced carers. Future plans to work even closer with the community.
Pressure ulcers: learning themes include identification of patients at risk of pressure ulcers, repositioning of patients, the utilisation of the risk
assessment tool and replacing of equipment. New beds procured and staff trained in Critical Care as well as new NG tube devices introduced and
a change in practice in placement of NG tubes. Closer working relationships in place with Southwark services and care agencies, providing
direction in the management of pressure ulcers.
Workforce: retention a key focus for the Trust People Strategy. PDR rates have improved. Mandatory training is at 86% a noted positive score
with some areas offering online training to allow for flexibility and ease of learning. Staff survey results very positive for the fourth year running.
Targeted intervention is in place and is currently working with ‘Timewise’ to assist with promoting flexible working.
Cancer: referrals for psychology post diagnosis seen within a week if urgent and no more than six weeks if non-urgent. CNSs complete holistic
needs assessments in all patients at different points of the pathway - patients referred to Dimbleby team if in-depth psychological assessment
needed. Recovery package includes - holistic needs assessments and care planning, health and wellbeing event, treatment summary and cancer
care review. Progressing with introduction of navigators who ensure care plans sent to GPs in a timely manner.
Quality Assurance – GSTT Quality Overview April 2019 Leadership
23
Leaders
hip

Quality Assurance – KCH Denmark Hill March 2019 Leadership
Leaders
hip
24
Domain Indicator Unit Year Apr May June Jul Aug Sep Oct Nov Dec Jan Feb Mar Target
Number 2018-19 10 17 15 9 12 14 6 9 9 10 10 4
2017-18 4 12 3 6 7 4 10 12 12 9 9 5
Number 2018-19 1 1 2 1 4 1 0 1 2 1 1 1
2017-18 2 0 3 4 3 0 2 0 3 0 0 2
Number 2018-19 1 1 2 0 2 3 0 1 1 2 3 2
2017-18 1 3 0 0 0 0 1 1 3 3 0 0
Number 2018-19 2 1 1 1 1 4 1 0 0 2 0 0
2017-18 2 0 0 2 0 0 1 1 0 0 0 2
Number 2018-19 0 3 0 1 0 3 0 1 0 0 0 0
2017-18 0 0 1 0 0 1 0 0 0 1 2 2
Index 2018-19 no data no data no data no data no data no data no data no data no data no data no data no data
2017-18 89.8 89.5 88.5 86.1 84.1 84.5 83.3 82 84.7 no data no data no data
Cases YTD 2018-19 6 2 6 10 7 7 4 5 4 3 8 7
2017-18 4 8 17 23 26 29 32 36 43 51 58 62
Cases YTD 2018-19 0 0 0 0 1 1 0 1 1 1 0 1
2017-18 1 1 1 2 2 2 2 3 3 3 3 3
% 2018-19 81.89% 82.89% 84.74% 83.10% 80.95% 83.77% 83.15% 83.33% 84.14% no data 85.50% no data
2017-18 71.80% 73.60% no data no data 94.01% 92.45% 91.80% 73.92% 75.00% 75.66% 75.63% 79.50%
% 2018-19 78.08% 78.60% 79.34% 78.34% 75.72% 78.62% 78.16% 78.85% 79.8% no data 79.21% no data
2017-18 68.5% 69.03% no data no data 75.70% 75.28% 75.96% 75.01% 76% 76.55% 77.02% 75.53%
% 2018-19 78.58% 74.90% 76.01% 77.79% 69.86% 73.34% 78.05% 80.76% 81.18% no data 79.94% no data
2017-18 72.40% 73% no data no data 76.18% 71.24% 72.64% 71.33% 72.68% 69.88% 72.42% 80.07%
%2018-19
55.00% no data no data no data
2017-18 58.00% 57% no data no data
%2018-19
80.00% no data no data no data
2017-18 84.00% 82.0% no data no data
%2018-19
15.00% no data no data no data
2017-18 18.10% 18.4% no data no data
% 2018-19 9.53% 9.46% 9.75% 9.69% 9.69% 10.33% 10.11% 10.31% 10.03% 10.35% 11.25% no data
2017-18 no data 11.92% 12.00% 12.49% 12.16% 11.99% 10.34% 9.79% 9.68% 9.06% 8.51% 8.44%
% 2018-19 no data no data no data no data no data 78.6% 81.77% no data 81.96% 82.35% no data 81.94%
2017-18 76% 76% 75% no data 82% no data no data no data no data no data no data no data
Number of complaints Number 2018-19 52 52 54 66 53 43 58 61 39 55 58 62
2017-18 46 55 41 51 38 45 64 60 53 61 59 54
Number 2018-19 29 33 19 33 35 26 26 29 23 25 12 25
2017-18 25 31 35 28 29 29 27 53 31 43 36 37
Statutory & Mandatory Training
Safeguarding % Children Level 3 80%
80
Pati
ent
expe
rien
ce
45
Complaints response >25 working days 0
Wel
l - le
d
Staff FFT recommended as a place to work
Trust wide not spec
Staff FFT recommended for care or
treatment Trust wide
not spec
Staff FFT response rate Trust wide not spec
Vacancy rate
52
Safeguarding % Adults Level 2 80%
Safeguarding % Children Level 2 80%
MRSA number of cases 0
Data source: Trust scorecards and performance reports as reported to CQRG
Safe
Total Serious incidents reported 0
Falls (moderate) <3
Falls (major) not spec
Hospital Acquired Pressure Ulcers- Grade 3
or Grade 4 not spec
Never Events declared 0
SHMI (National External) <100
C-Difficile
5-8%

The information provided in this section is a summary of discussions at CQRG meeting in March and April 2019. This meeting is attended by
senior Trust representatives, including the Medical and Nursing Directors, Clinical Commissioners and Directors of Quality from Lambeth and
Southwark Clinical Commissioning Groups (CCGs).
Key issues discussed at the March and April CQRG meetings regarding Denmark Hill:
Patient Safety: assurance regarding supervision of locum consultants - work undertaken around Trust and local induction with new E-learning
packages developed. The aim is to ensure that safe practice is embedded. Every area has a Clinical Lead, Clinical Director and a Divisional
Medical Director to supervise all consultants in their group and look to address any issues that arise.
Commissioners asked for an update on DH frailty assessment unit. The Trust commented that the frailty assessment unit has recruited two Band
7 nurses, and have secured funding from the Friends of Kings charitable fund to create a friendlier dementia environment. This work will
commence in May.
Flu Vaccination update: overarching increase in uptake of 14.8% compared to the prior year. The Trust was awarded the most improved flu
campaign nationally. Keys to success included commencing the flu campaign early, applying an MDT approach and the use of Peer Vaccinators.
Next year’s campaign to include increasing the number of doctors being peer vaccinators.
Cost Improvement Plans – plans for 2019/20 in early stages. The 19/20 programme contains three elements, Financial Improvement Plan (FIP’s),
Service Improvement Plans (SIPs) and Vacancy factors. There is now an internal team running the programme. Better collaborations and
alignment of processes have been developed taking into consideration the impact of quality, data protection and staffing on the Quality Impact
Assessment submissions. The new process completion of a QIA form within divisions and all schemes are submitted to the panel for
consideration. Once approved by the panel, any monitoring or areas that require tracking particularly to understand cumulative effect are identified
then the governance team register and agree further measures for monitoring.
Cancer services - Macmillan have funded two CNSs (one on each site), a programme manager and project manager with remits to drive the work
around ‘Living with beyond Cancer’ agenda. Further developments include a psychology team starting this month who will undertake a scoping
exercise of the work required going forward. It was noted that only 20% of BAME users accessed the MISC (Macmillan Information & Support
Centre) at DH between March and November 2018, an acknowledged under representation of this population group. Cancer patient literature
across London indicate that the elderly and BAME patents generally do not seek information. The Trust has been approached by charity ‘Bonded
Thru Cancer’ to set up support group targeting BAME population and are submitting a bid to Macmillan for Care Navigators to support patient
pathways.
Lost to follow up - of the 250k pathways initially identified 130k have been closed the remaining 120k have been put into six cohort categories of
which the ‘Active monitoring in the last 6 months’ sub cohort has been sampled, findings to be interrogated. Work has also commenced sampling
on ‘RTT LFT Active monitoring’ as these are considered the highest risk. Numbers relate to patients identified in 2014 and not new patients. To
date patient tracking is reviewed in a different way with better ways of identifying patients within the system that are potentially ‘lost to follow up’.
Quality Assurance – KCH CQRG April 2019 Leadership
25
Leaders
hip

The information provided in this section is a summary of discussions at CQRG meeting in March and April 2019. This meeting is attended by
senior Trust representatives, including the Medical and Nursing Directors, Clinical Commissioners and Directors of Quality from Lambeth
Clinical Commissioning Group.
Key issues discussed at the March and April CQRG meeting:
Staff Survey: 10 key areas reflected in the report. Of the 10, three areas reflect ‘average’ as a result. Results not as the expected standard considering
work undertaken on staff engagement and there is a need to do more work around the engagement score and staffing. Diversity and inclusion strategy
in place. The Trust has launched a disability and health morbidity staff group. The Trust has also put in place base values improvement around trust
culture, and is exploring instant messaging and improving on communication. Working on a clinical strategy and open seminars for staff have been
held to improve clinical engagement.
Complaints: response rate remains low at 69% for 25 days and 22% for 40 days. A number of actions are in place to address this. The Team will be
appointing a Head of Patient Experience & Partnership to manage the service as well as restructuring the team and working on positives such as how
deadlines have been met and what responses should have gone out; this piece of work has started.
GP alerts: three GP alerts were noted relating to rapid access chest pain clinic. The Trust is to ensure there is a clear way of booking into this and that
this is on the eRS system. NICE Guidelines for urgent referrals is five working days and at the moment the Trust is doing this in one month.
Mortality report: moving on with this work and the monitoring of death reviews is more robust. Major improvement is on DNA CPR data. The trust is
engaged on a major project to reflect what the learning is.
CQC action plan update: paper around the ‘Must dos and Should dos’ reflected significant progress made. In addition, there were six outstanding
actions discussed and rag rated as one red and five amber. These actions will be included in the Trust Quality Improvement Plan.
Serious incident learning: following an SI which was a failure to escalate a deteriorating patient, the development of an outreach team was part of the
action plan to address the issues identified. As part as business planning, the Trust have a service development in place and an outreach team.
Infection Control: - two cases of C.difficile reported within 28 days on General Intensive Care Unit (GICU). Direct cross infection not indicated,
cleaning scores good for the period and in both cases, antimicrobial prescribing was found to be justified and appropriate.
Water safety: IPCT continue to work closely with Estates and the Authorised Engineer Water to establish a revised Water Safety Plan. A revised form
to be used to identify low use outlets is being developed. This will be launched during April 2019 to re-establish the Trust wide position for little used
outlets, in order to ensure an appropriate flushing regime is in place. An operational Water Safety Group has been established to oversee this process
and for review and revision of guidance for cleaning of clinical hand wash basins.
Quality Assurance – St Georges CQRG April 2019 Leadership
26
Leaders
hip

The information provided in this section is a summary of discussions at CQRG meeting in March and April 2019. This meeting is attended by
senior Trust representatives, including the Medical and Nursing Directors, Clinical Commissioners and Directors of Quality from Lambeth,
Southwark, Lewisham and Croydon Clinical Commissioning Groups (CCGs).
Key issues discussed at the March and April CQRG meetings:
Flu Vaccination: Trust improved significantly in its rate of vaccination in the 2017-18 campaign and had built on this in the 2018-19 campaign. SLaM
will be working across SLP for the next flu campaign, as the vaccination target has increased for 2019-20.
CQC action plan update: CQC inspection has taken place. Improvement warning notice issued in August 2018 for Acute/PICU pathways has been
lifted on 17th April and that no further action is to be taken by CQC. governance within/across the Trust had undergone significant structural and
process improvements in response to the notice and was now compliant and robust in this regard on a sustainable basis. The new Quality and
Performance reporting was highlighted as a very notable improvement in support of these changes. Flow continues to be an issue, MADE events
have made some difference. Ongoing challenges - to move from red to green into standard process of escalating, allowing the Trust to identify
barriers via MADE process, and fully bringing MADE processes into business as usual operations.
Safer staffing/workforce: nursing agency usage had decreased from 10.38% (2016-17), to 8.37% (2017-18) to 7.57% (YTD). Trust has decreased
its turnover by more than 1% in nine months. Recruiting is an issue, particularly in Croydon and recruitment of good ward managers is difficult.
Discussed a concerted campaign to address this and the importance of harnessing and developing, retaining talented new staff via
leadership/culture and induction/training/support for students and new starters.
Cost Improvement Plans - end of year assurance review completed to assess delivery against CIPs and a review of the QIAs undertaken in 2018-
19. Learning was presented via quality impact and risk themes at borough / operational level. The process for QIAs for Trust CIPs has been in
place for 18 months and is fully embedded, including regular meetings with PMO. A range quality metrics is used to monitor progress. The 2019-20
QIA assurance process is under way – an assurance paper will be provided in due course.
Performance report
Response times (number of days) to complaints were reducing. The restructure into operational directorates was designed to better address this
and that this was a key factor behind the reported data.
QUESTT scores expected to show a downward trend in light of the response and improvements made following the recent CQC inspections in
subsequent quarterly reports – not only because of the improvements made in response to CQC but also that a number of wards rated red would
reduce in risk rating as a result of recent recruitment exercises and appointments.
Mandatory training compliance has slipped - this was mainly due to newly registered nurses and impact of lots of new starters at this time of year
(approximately 100 between Sept-Nov each year) which often results in lower compliance scores than at other points in the year. The Trust’s
learning and development team is working to find a way of spreading the training across the year.
Quality Assurance – SLAM CQRG April 2019 Leadership
27
Leaders
hip

Quality Assurance – Primary Care CQRG Leadership
28
Leaders
hip
The next CQRG meeting is scheduled in June and will be reported in the next IGPR.

29
Quality Assurance – Quality Alerts Update Leadership
Director Una Dalton
Management Lead Pippa Pritchard
Chart 1 Q4 Quality Alerts regarding GSTFT by Category Chart 2 Q4 Total Number of Quality Alerts
reported by Lambeth and Southwark GPs reported to Lambeth CCG by Provider of Concern
Source: QUIC (Lambeth CCG) and Southwark CCG Datix
The majority of Quality Alerts for GSTT related to Diagnostic imaging, Gastroenterology, District Nursing, and A&E. The most
quality alerts received were in relation to communication, clinical care and results.
Alerts about Lambeth general practices: GSTFT reported 12 quality alerts regarding eight general practices in Lambeth.
These mostly related to referral. KCH reported five quality alerts regarding five general practices in Lambeth. These also
related to referrals. Assura
nce

Director Una Dalton
Management Lead Pippa Pritchard
In Quarter 4 2018/19, a total of 50 serious incidents were reported to the CCG via STEIS requiring investigation. KCH, SLaM and LAS
SI’s relate to Lambeth patients or services only. The Lambeth CCG SI was reported on behalf of a general practice. One SI was de-
escalated and it is possible that SIs reported during this period may be de-escalated at a later date if found not to meet the criteria
following further investigation.
The Serious Incident (SI) Framework requires serious incident investigation reports to be submitted to the CCG within 60 working days of
reporting on STEIS. Overall, 90% of reports from GSTFT and 0% from SLaM due for submission within the quarter were submitted on
time. The SI Framework allows the CCG 20 calendar days to evaluate a submitted SI investigation report. NHS Lambeth CCG evaluated
56% of submitted SI reports within the stated timeframe; a proportion of these were evaluated by NHSE as commissioners.
Never Events: One never event was reported by GSTFT in Q4: wrong site surgery.
Quality Assurance – Serious Incidents and Never Events Leadership
30
Leaders
hip
Category GSTT KCHLambeth
CCG LAS SLaM Total
Surgical/invasive procedure incident meeting SI criteria 8 0 0 0 0 8
Treatment delay meeting SI criteria 6 1 0 1 0 8
Apparent/actual/suspected self-inflicted harm meeting SI criteria 0 0 0 0 7 7
Diagnostic incident incl delay meeting SI criteria 6 0 0 0 0 6
Medication incident meeting SI criteria 4 0 0 0 0 4
Maternity/obstetric incident meeting SI criteria: baby 3 0 0 0 0 3
Apparent/actual/suspected homicide meeting SI criteria 0 0 0 0 2 2
Confidential information leak/IG breach meeting SI criteria 2 0 0 0 0 2
Pending review 1 0 0 0 1 2
Pressure ulcer meeting SI criteria 1 1 0 0 0 2
Blood product/transfusion incident meeting meeting SI criteria 1 0 0 0 0 1
Environmental incident meeting SI criteria 1 0 0 0 0 1
Major incident/EPRR/suspension of services 0 0 1 0 0 1
Screening issues meeting SI criteria 0 1 0 0 0 1
Slips/trips/falls meeting SI criteria 0 1 0 0 0 1
Sub-optimal care of the deteriorating patient meeting SI criteria 1 0 0 0 0 1
Total 34 4 1 1 10 50

Programme Director Tony Parker (Acting Director Children’s Commissioning)
Programme Clinical Lead Dr Nandini Mukhopadhyay
Programme Management lead Daniel Stoten
Key Aims 2018/19
• Deliver on our Children and Young People’s Plan for Lambeth. This
includes work on A Better Start, Maternity, Early Help, CAMHs,
children with disabilities and special educational needs, looked after
children and more.
• Continued support of delivery of the Children & Young People’s Health
Partnership programme of work, including consideration for extending
practice across the whole borough.
• Work with Primary Care Commissioning colleagues to align elements
of the Children, Young People and Maternity Programme, CYPHP and
LEAP to the Local Care Networks/federated GP model.
• Continued support of the delivery of LEAP across 4 wards
• Strengthening governance around immunisation and support GPs to
deliver neonate Hep B and MMR school catch up through monitoring
and awareness.
Key achievements 2018/19
• Our plan was launched in March 2018, so we remain in implementation phase of our programme.
• Lambeth Made has been making significant headway over the first quarter of 19/20, with our Social
Enterprise Academy partnership launched and the beginning of our new programme with LDN
Apprenticeships, aiming to recruit 100 Lambeth CYP into high quality apprenticeships within 2 years.
Alongside this our charter for business and project ‘toolkit’ are in the final stages of development.
• Within our Early Help programme, the Early Help Toolkit has been finalised and hard copies are being
distributed amongst partners. The pilot evaluation will be completed by the end of May and shared as part of
the Early Help consultation process and with informal cabinet. The Team Manager has set up a Tulse Hill
Youth Forum to work with young people to inform the commissioning and delivery of services in the area,
while we are also currently devising a roll out plan for the North and South East of the borough.
• Community Safety have agreed to fund an additional Community Practice Lead within Early Help to support
the roll out of the new approach to Early Help in Angell Town and Coldhabour. Finally, the Early Help
Restructure will be launching in June, with the EQIA going to the Equalities Steering Group for Approval at
the end of May.
• Our consultation on children’s centre redesign closed in early 2019; papers have been through Cabinet
where recommendations were agreed. There has been a change to the initially proposed model (in
Streatham), which requires further consultation – this will be open until late June. The Cabinet decision was
called-in but has been through scrutiny and will progress with recommendations.
• We continue to work with colleagues in Children’s Social Care on the next steps of it’s improvement journey,
as well as continuing to support the preparation for the Special Educational Needs and Disabilities (SEND)
inspection. We are chairing the Commissioning and Engagement working group and playing a key role in all
of the other projects.
• Around Youth and Play, following a review, a decision has been taken to end the contract with Young
Lambeth Cooperative (YLC) in October 2019. This is due to a number of reasons including financial
instability, feedback from frontline VCS organisations and partners, and efficiencies and future direction.
Project and comms plans are being developed for the next 6 months, including tender/procurement
exercises, and working closely with the YLC on exit strategies and effective transition. The elements of the
contract will continue in 4 separate parts – commissioning of frontline provision (coming back in house to the
council), brokerage service, Youth Council and Young Mayor programme, and Infrastructure and
sustainability support to the VCS.
• Our Serious Youth Violence Strategy Group is now meeting, includes numerous strands of work beneath
including Education, Early Help and Families, and Interventions and Response. The Task and Finish groups
meet regularly and feed back to the main Strategy group.
• Funding of £500k for the short term has been allocated to pieces of work including mental health support in
the Tulse Hill area particularly, youth work with a trauma informed approach, and community engagement
worker. Public Health have conducted an evidence review of the interventions related to early help and
families that have been effective in supporting a reduction in violence. This will inform the longer term
intervention work to be commissioned. The critical incident response plan is being developed, ensuring all
elements are included: emotional and mental health support, staff support for organisations, parental
support, alternative ‘positive activities’ provision for young people available.
Integrated Children and Young People (including Maternity) Better Care
31
Inte
gra
ted C
hild
ren &
Young P
eople
Pro
gra
mm
e u
pdate
32
Programme Risks
Lambeth fails to meet its statutory responsibility to provide every looked
after child a health assessment within 20 days of referral and that each
health assessment is reviewed within 6 months for under 5yr olds and 12
months for over 5
Failure to reduce waiting time from referral to first treatment for the
CAMHS Early Intervention Team resulting in poorer outcomes and
increased escalation to Tier 3-4 services.
Immunisation performance
Actions taken
• Working group underway with colleagues in GSTT and LBL to ensure
improved performance, to reduce ‘batching’ of referrals.
• Clear pathways developed and briefing sessions for key teams in train
• Slight improvement in performance according to most recent data
• This risk remains mitigated, but we are once again seeing an increase
in waiting times. Teams are very stretched and demand is very, very
high.
• Our new Kooth online offer launched in February; we have taken on
the mental health first aid training contract (delivered by The Training
Effect), and our redesigned SLAM service (as mentioned in the bullet
point below), using the Mental Health Investment Standard money, will
develop a lighter-touch version of the model we had put in our bid.
• Our access target remains a risk. This is partially due to Kooth’s
reporting being currently at South East London, not individual CCG
level; but also due to capacity within SLAM. Commissioners are due to
arrange extraordinary contract management meetings as required to
ensure this improves; we do have a risk around property and are the
redesign goes live in July.
• We are also working with SLAM to redesign the Lambeth service, to
implement an assessment and triage team: this will take referrals,
assess, and deliver low level mental health interventions, CBT etc.
There are also plans to share specialisms across SLaM teams.
• Lambeth CCG is working with it’s partners in Public Health to ensure
we have a joined-up action plan to improve our local performance
regarding immunisations.
• A meeting took place on 21st May to review the existing action plan
and ensure actions are being taken. This action plan will be revised
and updated by week commencing 10th June.

33
Integrated Children and Young People (including Maternity) Better Care
Dashboard update
The red, amber, green (RAG) rating status of the 42 indicators on the dashboard following the latest data update is currently:
• 9 rated green• 9 rated amber• 14 rated red• 10 not rated
There have been five changes in the distribution of red, amber and green (RAG) ratings since the March report. Four of these represent improvements, whilst the other one reflects a deterioration. These are as follows:
• Percentage of children and young people 2-18 years on the asthma register that have had a high quality and personalised Asthma UK Asthma Plan within the last 12 months – red to green.
• Percentage of children and young people 2-18yrs on the asthma register who have an Asthma UK asthma plan within the last 12 months have also had an annual review in the last 12 months – red to amber.
• Percentage of children and young people 2-18yrs without an asthma diagnosis who have been issued with ≥ 4 SABA prescriptions in the last 12months have had a review as per the Pan London Asthma Care Standards – amber to green.
• Average waiting time from referral to 1st assessment Community CAMHS (weeks) – red to green.• Care leavers in employment, education and training – amber to red.
The net effect of these changes is that there are two less red RAG rated indicators on the dashboard than appeared in March..
Since the previous report, there have been updates to the data for twenty-three of the indicators on the dashboard. More details are given below.

34
Integrated Children and Young People (including Maternity) Better Care
Percentage of women that were smokers at time of delivery
Admissions of babies under 14 days
Percentage of children aged 5 with one or more obviously decayed, missing (due to decay) and filled teeth
Percentage of children and young people 2-18 years on the asthma register that have had a high quality and personalised Asthma UK Asthma Plan within
the last 12 months
Percentage of children and young people 2-18yrs without an asthma diagnosis who have been issued with ≥ 4 SABA prescriptions in the last 12 months have
had a review as per the Pan London Asthma Care Standards
Percentage of unplanned hospitalisations for children and young people with asthma, diabetes and epilepsy
Percentage of all paediatric (0-18) admissions due to asthma
Average waiting time from referral to 1st assessment Community CAMHS (weeks)
Average waiting time from referral to 1st assessment CLAMHS (weeks)
Rate of stillbirths for all maternal ages occurring in the respective calendar years per 1,000 births.
The number of stillbirths and deaths under 28 days, per 1,000 live births and stillbirths
Rate of deaths in infants aged under 1 year per 1,000 live births
Child (aged 1 to 17) mortality rate per 100,000 of population
Percentage of all live births at term with low birth weight
Percentage of eligible children who have received 3 doses of DTaP/IPV/Hib vaccine by their second birthday
Percentage of children and young people 2-18yrs on the asthma register who have an Asthma UK asthma plan within the last 12 months have also had an
annual review in the last 12 months
Permanent exclusion rate (primary & secondary) pupils with an EHCP
Permanent exclusion rate (primary & secondary) pupils with SEN support

35
Integrated Children and Young People (including Maternity) Better Care
Percentage of eligible children who have received one dose of MMR vaccine on or after their 1st birthday and anytime up to their 2nd birthday
Rate of hospital admissions for dental caries amongst children aged 0-4 years per 100,000 of population
Prevalence of obesity among children in Year 6 (aged 10-11 years)
A&E attendance (aged <18 years), rate per 1,000 population
Percentage of pupils identified as having a SEN
Early Years Foundation Stage Profile (EYFSP) - good level of development, those on SEN support
Key Stage 2 Reading Writing and Maths (RWM), expected standard or higher for those with an EHCP
Attainment 8 for those with an EHCP
Percentage qualified to level 2 including in maths and English by age 19 for those with an EHCP
Percentage of SEN aged 16 to 17 in education and training
Average waiting time from referral to 1st assessment Early Intervention Team (weeks)
Percentage of looked after children who have an initial health assessment within 20 days of becoming looked after
Percentage of children that have been looked after continuously for 12 months that have had an annual health assessment
Care leavers in employment, education and training

36
Integrated Children and Young People (including Maternity) Better Care
CQC Maternity services survey - Labour & birth -GSTT
CQC Maternity services survey - Labour & birth –Kings College
CQC Maternity services survey - Staff during labour & birth - GSTT
CQC Maternity services survey - Staff during labour & birth – Kings College
CQC Maternity services survey - Care in hospital after birth - GSTT
CQC Maternity services survey - Care in hospital after birth – Kings College
Progress 8 for those with an EHCP
Percentage of children with diagnosable MH conditions able to access community MH services in year
Number of children on a Child Protection Plan (CPP)
Number of children in need during the year (under 18 years)
Not rated (10):

37
Integrated Children and Young People (including Maternity) Better Care
INDICATOR UPDATE COMMENTARY
Since the previous report, twenty-three indicators have been updated with new data. Where this has affected an indicator which was previously red RAG rated or where the indicator has become red rated as a result of the new data, the change is as follows:
Percentage of children and young people 2-18 years on the
asthma register that have had a high quality and personalised
Asthma UK Asthma Plan within the last 12 months – red to
green
This indicator was previously red RAG rated on the basis that
coverage fell well below the CCG target of 85%. Latest data for
the end of March 2019 shows the year end position as 90.6%, a
considerable increase having been achieved in the final quarter.
This is likely to reflect the focus put on this area through
individual practice improvement plans and the task force
approach adopted by the GP Federations, which included
support from dedicated Service Improvement Facilitators.
Percentage of children and young people 2-18yrs on the asthma
register who have an Asthma UK asthma plan within the last 12
months have also had an annual review in the last 12 months
With the addition of year end data 2018-19, this indicator shows
coverage to be at 96.7%, just over 3% short of the CCG annual
target of 100%. On this basis it attracts an amber RAG rating, an
improvement on the previous red. It is likely that this
improvement can be ascribed to the effort put in as described
above in respect of asthma plan indicator.
Average waiting time from referral to 1st assessment
Community CAMHS (weeks)
Despite a rise in the average wait time over the first three
quarters of 2018-19, it fell in quarter four from 23.0 to 15.5
weeks and thereby came back within the 18 week target. Hence
the previous red RAG rating changed to green. This is
encouraging in the face of reported increases in average wait
times for other SLAM services, in particular for the neuro-
development team.
Care leavers in employment, education and training – amber to
red
Having previously been at 55% and within 5% of the local target
of 60%, with the addition of final quarter data, this indicator fell
back to 45% and so loses it’s amber RAG, rating to be replaced
by red.

38
Integrated Children and Young People (including Maternity) Better Care
Other changes can be noted as below:
Percentage of children and young people 2-18yrs
without an asthma diagnosis who have been issued
with ≥ 4 SABA prescriptions in the last 12 months have
had a review as per the Pan London Asthma Care
Standards.
With the addition of final quarter 2018-19 data, this percentage moved up to 72.9% and so exceeds
the CCG target of 50% and thereby attracts a green RAG rating. It had previously been amber rated.
The indicator is a close relative of the other two asthma-related indicators (YL2 and YL3) and all three
saw a final quarter upward surge.
CQC Maternity services survey indicators (BS1-3) There are no target expectations for these indicators, and they therefore do not have a RAG-rating.
There are similarities between the results achieved by the two local Hospital Trusts in that both GSTT
and Kings College saw a decline of 1% from 89% to 88% in the patient rating of their experience of
labour and birth. Similarly, both saw a 1% decline with regard to the care offered by staff during labour
and birth, although Kings College’s rating is 1% higher than GSTT’s. Both Trusts enjoyed rating
increases of 2% from 73% to 75% in respect of care in hospital after birth.
Percentage of women that were smokers at time of
delivery.
The addition of data for the third quarter of 2018-19 brings the yearly average for this indicator to
3.7%. This remains below the national target of 6% and so remains green RAG rated.
Rate of stillbirths for all maternal ages occurring in the
respective calendar years per 1,000 births.
Data for the two year average for the period 2015-17 has recently been published and shows the rate
of stillbirths for all maternal ages to be 4.6 for Lambeth. This represents an increase of 0.4 compared
with the previous two year period but nevertheless this indicator remains amber RAG rated.
Child (aged 1 to 17) mortality rate per 100,000 of
population
Data for the two year average for the period 2015-17 has recently been published and shows
Lambeth’s child mortality rate per 100,000 of population to be 10.1. This is a fall of 3.3 since 2014-16
and is the second successive fall. This latest value attracts an amber RAG rating and the indicator has
moved to below the England average of 11.2.
Percentage of all live births at term with low birth weight The latest (2017) percentage of all live births at term with low birth weight was 2.4%. This is the lowest
figure in the last five years and a fall of 0.4% compared to the previous year. Although below the
England average, this indicator continues to merit an amber RAG rating.
Percentage of unplanned hospitalisations for children
and young people with asthma, diabetes and epilepsy
And
Percentage of all paediatric (0-18) admissions due to
asthma
The addition of final quarter data for these two indicators brought the 2018-19 yearly averages to 2.7%
and 1.9%. Although these figures represent increases of 0.1% and 0.2% respectively, both indicators
remain below their stated targets of 3.6% and 2.3% and so continue to merit green RAG ratings.

39
Integrated Children and Young People (including Maternity) Better Care
Average waiting time from referral to 1st assessment
Early Intervention Team (weeks)
And
Average waiting time from referral to 1st assessment
CLAMHS (weeks)
Despite the good news noted above about the final quarter decline in the average wait times from
referral to first assessment with the community CAMHs team, the average wait for these two other
services rose in the same period, by more than 10 weeks for the Early Intervention team and by
almost seven for Children Looked After. The wait for the former is now over 41 weeks and rose
steadily throughout 2018-9, whilst the latter, whilst initially stable for the majority of the year, suddenly
almost doubled in the final quarter. Unsurprisingly the wait time from first assessment to Early
Intervention continues to attract a red RAG rating but the CLAMHS wait is still green rated as less than
18 weeks. There is however a danger of the 18 week target being breached if the current trend
continues.
Number of children on a Child Protection Plan (CPP) Between December 2018 and February 2019, this rose from 238 to 262. Although this is a rise of 24, it
was higher earlier in the year and topped 300 in March 2018.
Number of children in need during the year (under 18
years)
Between December 2018 and February 2019, this fell from 1469 to 1442, a fall of 27. Although the
number was lower earlier in the year, the latest figure is 39 less than that at the start of 2018-19.
Percentage of looked after children who have an initial
health assessment within 20 days of becoming looked
after.
The final quarter percentage of 57% represents an improvement for this indicator, which has risen
from 31% at the start of 2018-19. Still 18% below the statutory target of 75%, this indicator remains
red RAG rated.
Percentage of children that have been looked after
continuously for 12 months that have had an annual
health assessment
The final quarter percentage for this indicator was 77% and red RAG rated as it falls below the
statutory target of 90%. Coverage of health assessments appears to have remained fairly static
throughout the 2018-19 year, varying between 68% and 78%.

Integrated Children and Young People (including Maternity) Better Care
40
Inte
gra
ted C
hild
ren &
Young P
eople
Pro
gra
mm
e u
pdate
This was presented at the Children and Young People’s programme Board on the 21 March 2019.

Integrated Children and Young People (including Maternity) Better Care
41
Inte
gra
ted C
hild
ren &
Young P
eople
Pro
gra
mm
e u
pdate

CYP mental health: performance position and trend Better Care
42
Inte
gra
ted C
hild
ren &
Young P
eople
Pro
gra
mm
e u
pdate
Context
• The 2018-19 planning requirement is that 32 % of Children and Young People estimated to have mental health needs are assessed. And there is a 5 year ambition to achieve 35% annually
• This relates to children and young people having at least two sessions in the year. Once each person has had those two sessions, then they are not counted again for the year.
• The current performance position for South East London CCGs in 2018/19 is 28.3% against a target of 32%.This is based on year to date performance forecasted to the end of the year with some assumptions about the delivery of planned stretch actions in-year as set-out in the graphs.
• SEL has delivered an assurance return to NHSE, detailing which of it’s CCGs expect to deliver the CYP target. Bromley and Southwark have stated they expect to achieve the target by year end. Greenwich and Lambeth have stated they are not forecasting to achieve, while Bexley and Lewisham have expressed concern around the risk to achievement. Lambeth is working with Kooth for digital mental health support.
Programme Director Moira McGrath
Programme Clinical Lead Dr. Martin Godfrey (Elective and Cancer), Harpal Harrar (Urgent Care)
Programme Management lead Sara White / Kelly Hudson
Integrated Adults: Elective, Urgent Care and Cancer Better Care
43
Inte
gra
ted A
dults P
rogra
mm
e u
pdate
Key Aims 2018/19
Elective
• Reduce variation and levels of inappropriate GP initiated outpatient
referrals
• Conduct pathway review of specific specialties to consider alternative
provision in the community, referral triage, GP education and training to
support appropriateness of secondary care outpatient appointments
• Pilot a tier 3 weight management service
• Ensure effective and efficient use of specific diagnostic testing within care
pathways
• Increase utilisation of e-referrals (ERS) across Lambeth to agreed
trajectories
• Procure a community ultrasound service using new specification
Cancer
• Increase screening uptake/coverage and earlier detection of cancer
supported by General Practice education and training.
• Improve the early treatment of patients with cancer through improvement
in the 62 day wait cancer performance
Urgent Care
• Support A&E performance with redirection initiatives, system approaches
to managing emergency demand and public communications of
alternatives to A&E
• Implement a high intensity user service to support patients who
frequently attend A&E or dial 999, helping patients identify alternative
services to better meet their needs
• Recommissioning of Integrated Urgent Care service (formerly 111)
Key achievements 2018/19
Elective• Practice Visits summary report actions completed. GB agreed next round of
practice visits to start from September onwards once PCN’s are established.
• Community services for dermatology to be piloted with GST in Lambeth from
summer 2019
• Tier 3 weight management pilot is operational. High referrals in to the pilot
from Lambeth GPs, with 127 starters. Six month data is being collated to feed
into the pilot.
• The CCG & Trust monthly meetings continue to discuss and take action on e-
RS issues. Such as missing referral letters, GP Practices are contacted and
offered support and training.
• Community diagnostics service being scoped aiming to go to procurement
during 2019/20, subject to approval.
• The new MECS & Optometry Triage service across 5 CCG’s will start from
July 2019 with Primary Ophthalmic Solutions Ltd. Eye group meetings
continue to prepare for the start of the service.
Cancer:
• The GP Text messaging pilot for cervical screening , feedback is we are doing
great. The average for London is 84% and Lambeth is average of 93%.
• Lambeth cancer working group continue with GP Practice visits and have
started follow up visits to some practices.
• Planning further cancer health events as part of the Cancer recovery package
joint health event with Lambeth and Southwark. Next meeting is in May and
will invite participants interested in being involved in the event.
Urgent CareThe commencement of the on-site GP Hub at St Thomas’ ED has supported the
Urgent Care Centre (UCC) and the 4 hour target. This initiative has increased
access to primary care out of hours (18:00-22:00 weekdays and 12:00-17:00
weekends and BH) during times that ED have identified they face pressure but
did not have access to primary care. A request has been put in by the Trust to
extend the service by 1 more month (till May 2019) to support with the two Bank
Holidays and also allow time to do a ‘needs audit’

Integrated Adults: Elective, Urgent Care and Cancer Better Care
44
Inte
gra
ted A
dults P
rogra
mm
e u
pdate
Key risks on risk register
Urgent Care:
Likely risk that acute trusts will not achieve improvement trajectories to
meet the 95% A&E target
Cancer:
Likely risk that the CCG will not achieve the improvement trajectory for
meeting the access to cancer treatment as measured by the standard for
62 days from GP referral to treatment impacting on the CCG quality
premium and assurance framework
Long waiters (Referral to Treatment Times):
The risk that the number of long waiters (waiting more than 52 weeks) is
not half (or less than) the level at March 2019 than it was at March 2018
resulting in long waits for patients
Patient Treatment List (PTL):
Risk that the CCG is not able to maintain the PTL size at March 18 levels
(The PTL size is the total number of patients on the waiting list) increasing
the challenge of trying to effectively manage care for patients waiting for
elective appointments or treatment.
Actions taken
Urgent Care:
No current actions as no gaps in controls or assurances identified.
Cancer:
No current actions as no gaps or assurances identified.
Long waiters:
No current actions as no gaps or assurances identified.
Patient Treatment List (PTL):
Although there is no RTT plan beyond long waiting patients for KCH, the
ICDT and Regulators have accepted that addressing these patients is the
priority, but will continue to review RTT performance by specialty and
address any issues as they arise.

Programme Director Moira McGrath
Programme Clinical Lead Lead Member for Adult Social Care
Di AitkenCllrs Ed Davie
Programme Management lead Liz Clegg (AD, Older People),
Key Aims 2018/19
• To ensure further integration of health and social care,
including delivery of priorities set out in the two year
Better Care Fund Plan
• Build on Lambeth’s high performance in relation to
identifying individuals with dementia by increasing the
support available to individuals with dementia and their
families
• To continue to deliver the priorities for continuing health
care (CHC) including local and SEL sector QIPP plans,
discharge to assess and to implement the new revised
CHC framework.
• Ensure that patients have the best experience possible
at the end of life
• A sustainable and engaged social care market.
Key achievements 2018/19
The number of older people who are supported to remain at home continues to increase. Increase in the
number of people benefitting from reablement and remaining at home 91 days after rehabilitation/reablement
with fewer older people going into long term care.
Performance on dementia diagnosis remains well above national target achieving 80% in March 2019
Continuing care – Lambeth CCG met performance on continuing care discharge to assess for the year with
91% of CHC assessments took place in the community (target 85%) and 82% of assessments took place
within 28 days (target 80%). Sector wide Choice and Equity Policy finalised. Sector wide specialist care home
contract went live in January 2019.
Support to social care market in 2018/19 continued with joint working between GSTT, the Health Innovation
Network and commissioners. This includes the Community Medicines Project, Nursing Home Leadership
Programme, development of @home pathways for nursing homes, falls programmes and home care Yellow
Bag initiative.
Work continues on the development of community support provision closely aligned to development of LCNs
and neighbourhoods. Commissioners continued to engage with social care providers to ensure business
continuity in light of potential impact of Brexit.
Intensive support has also been provided for three nursing homes in the borough where there have been
concerns about quality of care. Fairlie House Nursing Home has been rated ‘outstanding’ by CQC following
inspection in December 2018
New care and support contracts were awarded for Lingham Court and Charleston House Extracare.
Transfer of Care Leadership Group in place and work plan agreed. Review of 7/7 working undertaken, Excess
Bed Day (EBD) Schemes in place funded by top slice of winter funding and EBD targets achieved .
Lambeth CCG continues to be an active member of the Lambeth Advance Care Planning Consortium. The
consortium has submitted a bid to the Big Lottery Fund to develop ACP champions and resources to roll out
ACP across the borough. Further information available at
www.healthwatchlambeth.org.uk/advancecareplanning
Five safeguarding masterclasses held, audit of primary care of safeguarding awareness and policies
undertaken and MCA checklist and flow chart developed
Project Smith roll out continues and evaluation commenced. – now operating in 11 wards. Over 100
community connectors have been trained, 63 are ‘actively connecting’
Integrated Adults: Older Adults (inc Committee in Common & joint arrangement with Lambeth Council) Better Care
45
Inte
gra
ted A
dults P
rogra
mm
e u
pdate

Key risks on risk register
Meeting the target set via Better Care Fund (BCF) to reduce delayed
transfers of care within the local system and associated impact on length
of stay.
Actions taken
Continued work streams to implement each of the High Impact Changes with
three HIC moving to ‘mature’ status in Q4.
Review and update of Choice Protocol as part of 8 High Impact
Changes. Review in March 2019.
Continued work to refine D2A pathway, as part of 8 High Impact – to be
reviewed March 2019
Recovery plan in place and intensive quality and safety monitoring by
commissioners following CQC inspections and Requires Improvement ratings
for a number of care homes. Suspensions in place for new placements for one
of the Lambeth Council block contract care homes.
Established use of trusted assessor (TA) role with one Council block contract
home, and GSTT/KCH.
Integrated Adults: Older Adults (inc Committee in Common & joint arrangement with Lambeth Council) Better Care
46
Inte
gra
ted A
dults P
rogra
mm
e u
pdate

2018/19 Delayed Transfers of Care (DTOC)
The Better Care Fund (BCF) was announced by the Government in the June 2013 spending round, to ensure a transformation in integrated health and social
care. BCF creates a local single pooled budget to support CCGs and local authorities to work more closely together around people, placing their well-being
as the focus of health and care services. BCF is managed via Committee in Common, devolved from Lambeth Health and Wellbeing Board. Performance
metrics are as follows:
The trajectory is based on number of delayed days. A revised trajectory for 2018/19 has been agreed, and reflected in the chart
above.
Validated DTOC data is released six weeks after month end and can then be compared with the DTOC trajectory outlined above. However to better
understand a more up-to-date picture of the processes supporting discharge at our local acute Trusts (Guy’s and St Thomas’ (GSTT), King’s College
Hospital (KCH), and South London and Maudsley (SLaM)), commissioners have oversight of operational discussions.
DTOC remains on the risk register (refer previous page). DTOC for January 2019 is above trajectory. The main reasons for the delay in transfer are
patient/family choice, and available beds in care homes. Transfer of Care Leadership Group currently reviewing Choice Policy for improved management
of patient/family choice; and ongoing quality issues in the care home block contract being intensively managed by commissioners and adult social care –
refer overleaf for all actions.
Integrated Adults: Older Adults Better Care Fund Better Care
47
Inte
gra
ted A
dults P
rogra
mm
e u
pdate

Non-elective admissions (NEA)Reablement – people remaining at home 3 months
following treatment
Permanent admissions to residential care homes
Integrated Adults: Older Adults Better Care Fund Better Care
48
Inte
gra
ted A
dults P
rogra
mm
e u
pdate

Integrated Adults: Personal Health Budgets Better Care
49
Inte
gra
ted A
dults P
rogra
mm
e u
pdate
The below table sets out each CCGs forecast position against its annual target for PHBs. It also includes a comparative position against the total cohort identified as potentially eligible for a PHB. The data shows CCG forecast year end position based on maintaining the run-rate delivered in the last month. For Bexley this omits the one-off impact of 60 wheelchair PHBs delivered in M9. It should be noted that year end-trajectories vary betweenCCGs in terms of phasing, so Greenwich have a stretching Q4 and Southwark benefit from flatter phasing.
Original cohort to set plans (i.e. total
opportunity)Q4 target Q4 forecast
Q4 forecast vs 18/19 PHB target
Q4 forecast vs total opportunity
NHS Bexley CCG 381 190 270 142% 71%
NHS Bromley CCG 553 347 247 71% 45%
NHS Greenwich CCG 343 296 198 67% 58%
NHS Lambeth CCG 533 170 74 44% 14%
NHS Lewisham CCG 443 150 79 53% 18%
NHS Southwark CCG 421 179 182 102% 43%
SEL CCG Total 2674 1332 1181 79% 39%

50
Programme Director Moira McGrath, Director of Integrated Commissioning (Older People)
Programme Clinical Lead Dr Azhar Saleem
Programme Management lead Vanessa Burgess
IAF Indicators 107a, 123a, 123b, 123d, 123e
Key aims
NHS Lambeth CCGs Primary Care Prescribing Medicines Optimisation Plan for
2018/19 seeks to embed improvements to the repeat prescribing process to improve
access to medicines and reduce wasted or unwanted medicines. We will work in
partnership to design pathways and support shared decision making with people
around their medicines to promote adherence, enable self care and the best value and
outcomes from medicines. By commissioning medicines across pathways with patient
orientated outcomes we intend to improve quality and length of life for people.
Working to a programme plan:
•Ensure advice and support is given to prescribers across Lambeth to ensure that
clinically appropriate cost effective medicines are prescribed.
•Maximise opportunities of patent expiry.
•Continue to support and implement the national antibiotic stewardship agenda.
•Work with secondary and primary care to ensure clear information on medicines is
shared as patients move between the different care settings and that a common
formulary is used across the health economy.
•Work with patients prescribers and pharmacies to ensure that medicines are only
dispensed when required and that patients understand why they are taking their
therapy and to tell healthcare professionals if they are unsure about taking their
prescribed treatment.
•Work with patients and prescribers to support self care and guiding patients to access
the appropriate healthcare setting for their current needs.
Key achievements 2018/19
• Engagement and communications of MOS with Medicines Clinical Leads / CCG Clinicians,
Federations and Local Care Networks, Practice Managers Forum, Practice Nurse Forum, Non-
medical prescriber’s forum, Lambeth Locum group, GP Trainee group and practice
pharmacists’ network, Lambeth Community Pharmacy, Access Hubs, etc.
• Encourage regular practice and peer discussion of prescribing budget position/ MOS through
practice/ locality meetings.
• All annual practice medicines optimisation visits to be completed by Q2 to encourage early
implementation. Identification of overspending practices revisited in-year.
• Fully integrate medicines initiatives into long term conditions pathways. Maximising adoption
through primary care, acute and community pharmacists and protected learning events
• Continue engagement with PPGs. Encourage practices to consult with PPGs regarding any
improvements to prescribing policies e.g. self-care and repeat prescribing.
• Consultation on revised terms of reference for the Borough Prescribing Committee and explore
potential of a joint CCG and council remit. Involve the public in medicines initiatives and use of
citizen engagement forums such as the Patient Participation Network to request feedback on
approaches.
• Increase numbers of GP practices employing ‘practice pharmacists’ to escalate delivery. Target
is to aim for 50% population coverage in 2018/19. 92% coverage achieved.
• Adoption of Area Prescribing Committee developed treatment pathways, shared care
guidelines, new medicines recommendations and NHS England directives to manage place in
therapy of drugs, associated costs and medicines which should not routinely be prescribed.
Collaborative approach to delivery with acute & community sector pharmacists to continue.
• Optimise Rx (prescribing decision support) software in operation to speed up adoption of local
and national prescribing recommendations. DXS and CCG intranet to encourage awareness.
• Engagement of community pharmacists via the LPC, development of CEPN-funded educational
training.
• Sector awareness of collaborative training of community pharmacies and general practice
model on ‘Reducing Medicines Waste’. Include coordination of public campaign of ‘pharmacy
bags’, posters and digital material.
• Area Prescribing Committee horizon scanning process and best practice implementation via
membership of LPP medicines workstream and PresQIPP.
• Local implementation of the NHSE Medicines Optimisation In Care Homes programme to
embed a network of good practice across South East London and to support the existing GSTT
Community Care Homes Support team medicines function.
• Lambeth Diabetes Improvement Program (run by DICT and AT Learning) has supported
practices to increase the average percentage of 8 Care Processes recorded to 74.6% (11.9%
annual improvement) and the average percentage of patients achieving the 3 Treatments
Targets (BP, HbA1c and total cholesterol) to 43.3% (3.5% annual improvement) for patients
with type 2 diabetes at the end of 2018-19
• Updated the Lambeth and Southwark Sexually Transmitted Infections quick reference
treatment guideline for primary care
Integrated Adults: Older Adults Long Term Conditions & Medicines Optimisation
50
Inte
gra
ted A
dults P
rogra
mm
e u
pdate

Key risks on risk register• Non-Delivery of the Medicines Optimisation Scheme 2018-19 will
impact on achievement of QIPP savings, CCG financial balance,
patients not receiving evidence based cost effective medicines
• Two-thirds of Lambeth practices currently do not employ practice
pharmacists
• Implementation plan on NHS England Guidance of ‘Items which
should not routinely be prescribed in primary care’ is required. Key
items described, namely, dosulepin, trimiprimine, lidocaine patches
and co-proxamol require significant SLAM engagement and SEL
APC wide implementation.
• Lack of awareness in wider population of the medicines waste
initiative.
• Cost pressures from new medicines launched in 18/19, growth
seen particularly in diabetes medicines and devices. Inability to
control unstable nationally agreed prices of a number of generic
medicines.
• Implications of Brexit on medicines prices and usage are as yet
unclear – may lead to instability of prices and over-ordering of
medicines by the public in Q4.
Actions taken (April 2018- March 2019)• Completed all three launch events for Medicines Optimisation Scheme 2018-19, further engagement and
communication to other groups/ forums ongoing, resources and materials to support delivery of Medicines
Optimisation Scheme 2018-19 uploaded to intranet site and all annual practice medicines optimisation visits
completed.
• 2018/19 Q3 Prescribing Dashboard disseminated to practices
• 2019/20 Medicines Optimisation Scheme and resources developed
• Refreshing / preparing OptimiseRx messages to support: 2019-20 plans around medicines optimisation,
CVD, respiratory, mental health. Collaborative working with Southwark CCG continuesDeveloped
implementation guidance on the NHS use of Freestyle Libre across London via South East London Area
Prescribing Committee.
• The BHF Hypertension Detection Project services have undertaken 345 blood pressure checks and found
60 people with potential hypertension. 5 people have been detected with severely high BP requiring urgent
review in 24 hours.
• Working jointly with Lambeth Council in commissioning prevention services as a key part of early
intervention or harm reduction in long term conditions pathways.
• Practice pharmacists now approx. 30 pharmacists (25 WTE) working in 38/42 practices, covering 92% of the
population; CCG meds team, Federations and CEPN aiding implementation.
• Working with primary care and Federations to develop PCN offer around pharmacist workforce for 2019-20
• Lambeth Pharmacist Network launched and monthly training and professional peer-led supervision in place
• Providing strategic input to the SEL Community Pharmacy Education and Training programme and
integrated junior pharmacist Vocational Training Scheme (HEE funded).
• Published/ disseminated South East London Area Prescribing Committee (SEL APC) guidance: see website
for detail
• Supporting SEL working group to implement mental health and pain drugs aspects of NHSE guidance
‘drugs not to be routinely prescribed in primary care’
• Facilitating SEL Task Group on harmonising non-biologic immunomodulatory drug guidelines
• 2019/20 Immunomodulatory (formerly known as DMARDs) Scheme developed
• Successfully ran reducing medicines waste advertising campaign across Lambeth
• Implementing delivery plan for NHS England Diabetes Transformation and Care: 3 Treatment Targets (3TT)
and Structured Education Improvement Programme. Diabetes Book and Learn service for diabetes
structured education has launched. Diabetes Intermediate Care Team/AT Learning launched the diabetes
quality improvement programme for 3TT and 8 Care Process. Diabetes Service Review completed.
• Reviewed demand and capacity for diabetes prevention courses. Updated the Healthier You referral
pathway to include discussion and referral of people at risk of diabetes with HbA1c 42-43 mmol/mol to
healthier you and the Lambeth Local Authority Your Health webpage.
• Obtained approval and disseminated the Lambeth Diabetes Foot Care Pathway.
• Supported GPDF contract monitoring and contract refresh for 2018/19.
• LTC and Medicines Commissioning Intentions developed for 2019/20.
• Actively participating in SEL STP ‘integrated pharmacy and medicines optimisation’ development by
contributing to the leadership group and medicines optimisation and workforce streams.
• Delivered successful cardio-respiratory PLT with 87 attendees from 40/43 practices. 97% found the event
useful, rating the sessions ‘good’ or ‘excellent’.
• Working with the Local authority and the stop smoking service to improve patient’s access to medicines
used for smoking cessation
• Supporting primary care team in preparing 2019/20 LNDF and premium specifications, and LTP/GP contract
implementation from medicines and LTC perspective.
51
Inte
gra
ted A
dults P
rogra
mm
e u
pdate
Integrated Adults: Older Adults Long Term Conditions & Medicines Optimisation

52
Inte
gra
ted A
dults P
rogra
mm
e u
pdate
Integrated Adults: Older Adults Long Term Conditions & Medicines Optimisation
NHS England Antibiotic Quality Premium Monitoring Dashboard (12 month rolling data)
Overall the prescribing budget was overspent at Month 11 by £513,612 (-1.6% see finance report).
The North Locality is overspent by 1.0%, the South East is underspent by 0.1% and the South West overspent by 3.3%
Spend per ASTRO-PU (data available quarterly)
2018/19 Spend per APUAchievement
ThresholdCCG average
No of practices achieving
threshold (out of 42)
Q1 2018/19 <£7.75 £7.49 29
Q2 2018/19 <£7.75 £7.41 29
Q3 2018/19 <£7.75 £7.23 29
Q4 2018/19 <£7.75
Antimicrobial Stewardship - Quality Premium indicators
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18
Antibacterial items/STAR PU13
Target Value by end of 2018/19 to be equal to or less than 0.965:
0.675 0.669 0.662 0.657 0.649 0.642
Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
0.641 0.633 0.626 0.621
Reduction in the number of trimethoprim items prescribed to patients aged 70 years or greater
Target value by the end of 2018/19 to be equal to or greater than -30% (reduction over the quarter)
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18
-30% -33% -35% -35% -36% -38%
Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
38% 40% 43% 43% 44%

53
Inte
gra
ted A
dults P
rogra
mm
e u
pdate
Integrated Adults: Older Adults Long Term Conditions & Medicines Optimisation
* The utility of ScriptSwitch is cost/growth avoidance
Medicines Optimisation Schemes 2018/19
Description SourceCurrent spend Lambeth
(17/18)
2018/19 Full Year Lambeth QIPP
ValueQIPP M1 M2 M3 M4 M5 M6 M7 M8 M9 M10 M11 M12 Total
SEL Collaborative QIPP
1. Stoma Care To be confirmed To be confirmed
Projected saving £0 £0 £0 £0 £0 £0 £0 £0 £0 £0 £0 £0 £0
Actual savings N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A
2. Reduce Medicines Waste in Repeat requesting of Prescriptions OtherApplicable to all
prescribing spend (£34,895,203)
£574,000
Projected savings £47,834 £47,834 £47,834 £47,834 £47,834 £47,834 £47,834 £47,834 £47,834 £47,834 £47,834 £47,834 £574,008
Actual savings £47,834 £47,834 £47,834 £47,834 £47,834 £47,834 £47,834 £47,834 £47,834 £47,834 £47,834 £47,834 £574,008
Lambeth CCG Medicines Optimisation Scheme 2018/19
M1 M2 M3 M4 M5 M6 M7 M8 M9 M10 M11 M12 Total
3. Primary Care Prescribing
EPACT
£956,000
Projected saving £85,667 £85,667 £85,667 £85,667 £85,667 £85,667 £85,667 £85,667 £85,667 £85,667 £85,667 £85,667 £1,028,004
Actual savings £86,592 £65,709 £105,709 £78,506 £98,918 £120,635 £64,707 £119,529 £119,506 £83,389 £139,467Data not available
£1,082,667
*OptimiseRX
Projected saving £24,000 £24,000 £24,000 £24,000 £24,000 £24,000 £24,000 £24,000 £24,000 £24,000 £24,000 £24,000 £288,000
Actual savings £24,439 £25,940 £24,313 £23,440 £21,142 £19,769 £20,108 £19,236 £19,659 £19,659 £19,555 £20,935 £258,195
5. Adherence support for older adults (medication review and care home support)
Other To be confirmed £200,000
Projected saving £16,667 £16,667 £16,667 £16,667 £16,667 £16,667 £16,667 £16,667 £16,667 £16,667 £16,667 £16,667 £200,004
Actual savings £16,667 £16,667 £16,667 £16,667 £16,667 £16,667 £16,667 £16,667 £16,667 £16,667 £16,667 £16,667 £200,004
£1,730,000 Cumulative savings £175,532 £331,682 £526,204 £692,651 £877,212 £1,082,117 £1,231,434 £1,434,699 £1,638,365 £1,808,163 £2,031,686 £2,117,122

Programme Director Moira McGrath, Director of Integrated Commissioning (Older People)
Programme Clinical Lead Dr Harpal Harrar
Programme Management lead Denis O’Rourke, Assistant Director
IAF Indicators 107a, 123a, 123b, 123d, 123e
Key Aims 2018/19
Deliver key service transformation programmes including new community
service offer (Living Well Centres) from October 2019 and new crisis service
offer from July 2019 ;
Deliver key financial and performance (LWNA, LBL, 5YFV) targets and
shadow run the LWNA outcomes framework from 1 October 2019.
Play an active role in opportunities for collaboration across SEL (including
the South London Partnership) and within Lambeth build strong links with the
PCNs and with the NBC delivery alliance.
Key achievements 2018/19 February 2019
Multi agency project groups are developing service redesign proposals
in relation to the four major transformation work streams : acute
pathway ; crisis and urgent care ; IPSA Plus and the development of
Living Well Centres which will encompass the “front end” and “focused
support”. A phased programme of service change will come into effect
from July 2019.
The Evening Sanctuary provided by Mosaic Club House has been
extended from 5 to 7 nights as part of the LWNA’s commitment to
improving crisis support.
A draft employment and vocational support strategy has been
developed following engagement with a wide range of stakeholders,
including service users. This is being finalised for circulation July 2019.
An Alliance workforce strategy has been developed, due for
implementation from July 2019. .
54
Inte
gra
ted A
dults P
rogra
mm
e u
pdate
Integrated Adults - Mental Health Better Care

Key risks on risk register
Risk that the service transformation plans through the Alliance contract
fail to deliver planned improvements and savings resulting in financial
loss and lack of improved outcomes.
Risk that demand for acute psychiatric beds is not reduced resulting in
poor outcomes for delayed transfers of care and negative financial
impact.
Actions taken
Service transformation plans (including savings) for acute in patient beds ;
Community; crisis care and placements (IPSA plus) and the development
of three Living Well Centres have all been developed via multi agency,
stakeholder project groups that have produced fully costed proposals.
These were all agreed and signed off by the LWNA ALT and programmed
for implementation over 2019/20.
Acute OBDs - new 6 bed step forward (alternative to in patient beds)
service is now fully utilised contributing to whole system plans to reduce
overall bed occupancy levels alongside plans to reduce the number of
long stay (super stranded) patients who have spent 200 plus days on the
wards.
An IPSA plus workshop is being held on 28 June 2019 in order to focus
on key challenges in relation to the high demand for placements.
Integrated Adults - Mental Health Better Care
55
Inte
gra
ted A
dults P
rogra
mm
e u
pdate

• IAPT 6 weeks NHS Lambeth CCG has performed consistently well against the target for the proportion of Lambeth patients finishing a
course of treatment receiving their first appointment within six weeks of referral. The 75% target has been exceeded for the last two years,
with average monthly performance at 95%.
• IAPT 18 weeks NHS Lambeth CCG has consistently met this target achieving 100% for every month for the last two years.
• IAPT in recovery Recovery rates have improved over the last couple of months with performance exceeding the 50% standard.
• Proportion of people receiving therapy The target for people with depression who are referred for and access psychological therapy is
19.2% for 2018/19 or a Q4 position of 4.75%. Performance in this area has improved with the last rolling quarter exceeding the 4.75%
requirement at 4.98%.
• Early Intervention in psychosis The target is for 50% of patients to access early intervention treatment within 2 weeks. Lambeth CCG has
exceeded the target througout 2018/19.
• Dementia Diagnosis Rate From April 2017, NHS England has changed the way it calculates the dementia prevalence. It is using the total
number of people registered on a GP Practice list as the baseline for the population of that borough, rather than using the ONS data as it
previously did. The CCG is still well above the standard and is still treating the same number of people. Current monthly performance as at
March is 80.1%. This is an increase of 6% on previously reported monthly data.
Performance – Mental Health Better Care/Better Health
56
Better
Care
/Better
Health

Integrated Adults - Mental Health Better Care
57
Inte
gra
ted A
dults P
rogra
mm
e u
pdate

Integrated Adults - Mental Health Better Care
58
Inte
gra
ted A
dults P
rogra
mm
e u
pdate

Integrated Adults - Mental Health Better Care
59
Inte
gra
ted A
dults P
rogra
mm
e u
pdate

Integrated Adults - Mental Health Better Care
60
Inte
gra
ted A
dults P
rogra
mm
e u
pdate

The Integrated Adults Programme dashboard is updated every two months (given the nature of the key performance indicators. The dash board was last
reviewed by the IGC in April, focussing on cancer services as a deep dive chapter. The next update will be provided in August 2019.
Integrated Adults – Programme Dashboard Better Care
61
Inte
gra
ted A
dults P
rogra
mm
e u
pdate

Programme Director Ruth Hutt
Programme Clinical Lead Dr Martin Godfrey
Programme Management lead Laval Lebon
IAF Indicators 124a, 124b
Key Aims 2018/19
• Develop a joint commissioning strategy with the council for adults with
a learning disability
• Improve take up of annual health checks for adults with a learning
disability
• Improve recording of people with a learning disability on GP register
• Reduction in inpatient numbers within CCG and NHSE Specialised
Commissioning Transforming Care cohort in line with intended
trajectory if possible
• Development of multi disciplinary team for overseeing Transforming
Care casework
• Developing appropriate community support/placements for
Transforming Care cohort to support inpatient reductions
• Playing a full role within the SEL TCP partnership and ensure that the
CCG is fully compliant with required reporting
• Ensuring improved pathways, with appropriate clinical input, for
Transforming Care clients
• Organise autism awareness training for GPs and practice staff
• Improve cancer screening rates for adults with a learning disability
• Ensure LD Mortality Review process is well managed and appropriate
learning is shared/acted upon.
Key achievements 2018/19
• Number of Transforming Care patients in CCG beds was 10 as of
March 19
• Additional PBS Practitioner being recruited to work with our
Transforming Care caseworker
• We did not meet our KPIs around CTRs in March for our inpatients
due a last minute cancellation by a clinical reviewer for 1 CTR.
Therefore professionals meeting held in place
• Monthly Multi Disciplinary Team meetings to discuss Transforming
Care client son the at risk register
• We are working with a provider to develop a local Supported Living
and crisis service and are refreshing service model, following
feedback from NHSE.
• The Learning Disability Task Force worked to ensure accurate
recording of people with a Learning Disability on GP register
• At the end of March 2018/19, we reported 75% for AHCs and care
plans 72%, an improvement of 4% over last years performance and
achievement of the national LD target
• There was low take up from GP practices on LD cancer screening
programme.
• Autism awareness training delivered to GPs and practice staff
• The LeDeR Steering Group continued to meet to identify some of the
key themes emanating from the reviews which have so far been
completed in Lambeth.
Inte
gra
ted A
dults P
rogra
mm
e u
pdate
62
Integrated Adults – Learning Disabilities Better Care

Key risks on risk register
• Discharging these individuals, with very complex care needs, into
CCG-commissioned inpatient beds (from those commissioned by NHS
England) or into the community will lead to financial pressures on
CCGs and councils.
• Financial, reputational and community safety risk of moving forensic
patients from out of area inpatients units to south London, as part of
specialised commissioning’s New Care Models Programme.
• The South East London TCP not meeting its inpatient trajectory.
• Not realising the wider, quality benefits of the Transforming Care
agenda.
• Absence of clarity about funding flows between NHSE and CCGs (and
about how the TCP partnership will share these funds when received)
creating financial risk/lack of control.
Actions taken
• Lambeth inpatients identified and funding bodies clarified.
• Transforming Care caseworker monitors of all Lambeth inpatients and
plans in place to discharge to community placements for those who
are ready for discharge.
• New multi-disciplinary team in place to better sustain placements in
the community, ensure timely case reviews and support discharges.
• Transforming Care Steering Group monitors Lambeth inpatients,
performance and associated finance.
• SEL Transforming Care programme team monitors Lambeth
performance closely. Weekly calls and casework meetings happening
at SEL level.
• Quarterly SEL TCP surgeries to discuss care pathway for Specialised
Commissioning patients
63
Integrated Adults – Learning Disabilities Better Care
Inte
gra
ted A
dults P
rogra
mm
e u
pdate

• NHS Lambeth CCG performance for the % of health checks carried out over the last 12 months is 75% and the number of plans in place is
71%. This is excellent progress and exceeds 2017/18 performance.
Learning Disability – Health Checks and Plans Better Care
64
Inte
gra
ted A
dults P
rogra
mm
e u
pdate

Programme Director Ruth Hutt
Programme Clinical Lead Dr Raj Mitra
Lead member for Lambeth Council Councillor Edward Davie and Councillor Jacqui Dyer
Key Aims 2018/19
• Support the Health and Wellbeing Board to take a strategic and
evidence base approach to decision making and prioritisation in
health improvement to improve population health and wellbeing and
reduce health inequalities.
• Enable partners to deliver evidence based and needs led health
improvement.
• Provide strategic direction and support to the Lambeth Together
development, particularly around population health outcomes.
• Support the effective implementation of the Health and Wellbeing
Strategy
• Continue to enable the effective delivery of key health improvement
programmes led by Lambeth on behalf of other boroughs, such as
the LSL Sexual Health , London HIV Prevention and Elton John
AIDS Foundation (EJAF) Social Impact Bond Programmes
• Support the embedding of Health in all Policies across the local
authority and partner organisations
• Ensure the effective commissioning of health improvement services
(sexual health, substance misuse, smoking cessation, weight
management, NHS Health Checks) that deliver optimal outcomes
and value for money.
• Support the key aims and delivery of Black Thrive.
• Support the development and coordination of the JSNA.
• Facilitate the promotion of key messages promoting health and
preventing ill health with partners such as immunisations and AMR
awareness
Key Achievements 2018/19
• Lambeth Health and Wellbeing 2018/9 Implementation
Plan delivered and reported
• Lambeth Together Task and Finish group developing draft strategy,
to be published in the summer.
• Successful local delivery of national vegetable campaign, about
13,000 KS2 children engaged
• Ran the first of a series of workshops to support the ‘Health in All
Policies’ approach. Focus of the workshop was Environment and
Public Protection.
Staying Healthy Better Care
65
Sta
ying H
ealthy

Key risks as identified on the risk register Actions taken
Increase (widening) in health inequalities as a result of austerity, cuts to public
services and prevention services.
Working with Lambeth Together partners to make best use of
resources and assets across the system, including local
communities.
Services rationalised and targeted at those most in need /
recommissioned in context of reduced budgets
Financial impact of Pre-exposure Prophylaxis for HIV (PReP)Impact trial
Lambeth have pushed London boroughs to seek concessions
including use of online screening rather than clinic based, to
reduce costs, and sought to lobby for a fully funded solution to
commissioning PrEP within the lifetime of the trial.
NHS Health Checks delivery may not have desired impact on identified risk
groups, including take-up by those most at risk
One-year review of risk stratification tool and overall Health Check
programme to assess impact and develop local action plan; initial
findings will be available by end of April 2019, including process
mapping and NHS Health Check Quality Assurance Framework
benchmarking to help guide recommendations.
Increase in drug related deaths
Extensive provision of "Take Home Naloxone" - Naloxone is an
essential life-saving medication that counteracts the effect of
opioids and is used to reverse opioid overdose.
Local Dug Information System established to receive and assess
risk based on intelligence about dangerous drugs and determine
appropriate response. Key messages can be disseminated via the
Professional Information Network (PIN)
Localised measles outbreak
Supporting CCG to improve record of vaccination uptake,
supporting CCG to improve quality of the service delivery
Implementing Make every Contact Count
Facilitating the delivery of a borough-wide immunisations action
plan, which includes support to primary care and call/recall.
66
Sta
ying H
ealthy
Staying Healthy Better Care

Key risks as identified on the risk register Actions taken
Increase in drug related deaths / Fentanyl Provision of "Take Home Naloxone" - Naloxone is an essential life-saving medication that counteracts the effect of opioids and is used to reverse opioid overdose.
Local Dug Information System established to receive and assess risk based on intelligence about dangerous drugs and determine appropriate response. Key messages can be disseminated via the Professional Information Network (PIN)
Lack of preparedness to respond to pandemic flu Flu pandemic flu plan being revised, checklist for preparedness in local authority being finalized. Update of response framework due to be completed within next months. Pandemic flu plan to be presented at the June LBRF
Send final preparedness checklist to each relevant departments in local authority
Localised measles outbreak Supporting CCG to improve record of vaccination uptake, supporting CCG to improve quality of the service delivery
Implementing Make every Contact Count
Facilitating the delivery of a borough-wide immunisations action plan, which includes support to primary care and call/recall.
Increased frequency of bacterial infection in PWID and transmission of resistant bacterial infection
Joint project with SL HPA, Inclusion team (community services GSTT), LSHTM to raise awareness of bacterial infection in PWID
Improve hygiene (individual and environment) in hostels, and training for hostel workers.
Update of the epidemiology planned for Q1 2019
Staying Healthy Better Care
67
Sta
ying H
ealthy

Staying Healthy Better Care
68
Sta
ying H
ealthy
Notes – updates from last report
Under 18 Conceptions changed from Amber to Red, and is Improving (long-term trend).
Please note: Smoking Prevalence (routine and manual) has changed in 2019/20 to Smoking Prevalence (socioeconomic gap). Lambeth is currently
ranked in the top quintile nationally.

Staying Healthy Better Care
69
Sta
ying H
ealthy
Sexual Health Testing and Treatment
Total spend 2018/19 (M11 Forecast Estimates)
Block Contracts £3,600,108 | Out-of-Borough Activity £3,453,415 | SHL e-
Service £553,272 | TOTAL £7,606,795
In March 2019, e-service activity for our residents averaged 83 kits ordered per
day, with 49 ordered directly from the SHL website and the remaining
(34) through clinic and NHS trust websites.
Our local integrated sexual health clinics have channel shifted patients with no
symptoms of STIs at greater rates than other London trusts. Additionally, in-clinic
activity has not declined at other London trusts at the same rates as it has
at GSTT + KCH. Lambeth has seen high demand for tests and our e-
service affordability limits were exceeded for the year by January.
Sexual Health Outcomes (latest data for all indicators is 2017)
STI testing rate (exc chlamydia, aged <25) / 100,000
• 59,480 per 100,000 residents compared to 63,399 in 2016, trend is
improving.
There was a slight decrease in testing between 2016 and 2017 (6%). Lambeth is
still testing more of our residents for STIs than any other local authority in
England.
New HIV diagnosis rate / 100,000 aged 15+
• 42.2 per 100,000 residents compared to 105.5 in 2016, trend is improving.
Between 2016 and 2017, Lambeth saw a huge decrease in new HIV diagnoses,
from 105.5 to 42.2 per 100,000. Factors contributing to this drop
include increases in access to PrEP through private purchase and the PrEP
Impact Trial, and an increase in the frequency of STI testing.
Total prescribed LARC excluding injections rate / 1,000 (Female)
• 47.1 per 1,000 female residents compared to 41.4 in 2016, statistical trend
cannot be calculated but numbers have increased
Lambeth now prescribes LARC at similar rates to England. This is likely due to
the high activity at our integrated sexual health services.
Under 18s conception rate / 1,000 (Female, <18 yrs)
• 24.0 compared to 22.8 in 2016, overall trend is improving.
Since 2002, Lambeth has seen a big decrease in conceptions in under-18s, from
97.8 in 2002 to 24.0 per 1,000 in 2017. The 2017 increase is an absolute
number of 7 more pregnancies.
Substance MisuseIn 2018/19, Lambeth's drug and alcohol services engaged 937 opiate
clients, 326 non-opiate clients, and 336 alcohol clients in treatment.
• 7.1% opiate users successfully completed treatment in
2018/19, compared to 6.4% in 2017/18. AMBER, outside top quartile for
comparator local authorities and trend is improving.
Latest performance has Lambeth just outside the top quartile of similar local
authorities, needing just five more successful completions in year to achieve this.
Opiate care pathway has been reviewed with stronger focus on recovery
support.
• 53.1% alcohol clients successfully completed treatment in
2018/19, compared to 47.5% in 2017/18. GREEN, above national average
(38%) and trend is improving.
Latest data indicates that Lambeth continues to achieve higher than national
performance for alcohol successful completions.
Review of alcohol care pathway undertaken. The new care pathway is a success
and is now fully embedded and established, enabling quicker access
to treatment including detox.

Staying Healthy Better Care
70
Sta
ying H
ealthy
NHS Health Checks
Public health is accountable for delivery of the local NHS Health
Checks programme.
• In 2018/19 Lambeth sent 14,493 invites and 3,557 attended
for a Health Check, compared to 13,286 and 3,802 respectively in
2017/18.
• Lambeth continues to overperform in terms of offers but did not meet
target to increase uptake by 3%.
Public Health are working with Lambeth GP Federations to address the
performance, including implementation of an
improvement plan which has had some positive impacts on performance
for Q3 and Q4.
A review of the delivery of our NHS Health Check programme is
also underway to look at both broader commissioning strategy
and process, outcomes and impact, to be completed by the
end of Q1 2019/20. Recommendations will be used to inform in-
year improvement, future commissioning and operational strategy.
Smoking Cessation
Lambeth implemented a redesigned targeted smoking service,
providing quality support on a reduced budget in 2018-19. Specialist
support is delivered by the GSTT Smoking Cessation Team with open
access support provided through community pharmacies.
• GSTT Specialist Stop Smoking service had 300 people set quit
dates and 159 (53%) successful quits in 2018/19, compared to 254
and 157 (57%) respectively in 2017/18.
• Fourteen pharmacies are commissioned to deliver stop smoking
advice. In 2018-19, 363 people set a quit date and 147
(40%) successfully quit, compared to 521 and 216 (41%) respectively
in 2017/18.
Improved GSTT performance was offset by reduced pharmacy activity
(due to delayed pharmacy mobilisation linked to acquisition of
competency requirements). Now addressed and performance should
improve for 2019-20.
Steering group has been established to oversee delivery of the overall
community smoking service in Lambeth and review Year 1 performance.
Performance targets based on 2018/19 baseline are being agreed with
providers as part of this process.
Negotiations are also ongoing to streamline access to pharmacological
support for patients accessing the GSTT specialist service.

Programme Director Andrew Parker, Director of Primary Care Development
Programme Clinical Lead Dr. Martin Godfrey, Governing Body lead for Primary Care
Programme Lead Garry Money, Assistant Director of Primary Care
IAF indicators 128c, 128d
Key Aims 2018/19
Develop General Practice to work at scale;
Make primary care a more attractive place to work;
Primary Care Commissioning;
Develop new way of working to reduce variation in Primary Care;
Give people in Lambeth the opportunity for their voices to be heard;
Primary Care to be better configured to deliver an increased range of
services to patients;
Ensure primary care is an integral part of current and future plans for
unscheduled care - e.g. harnessing the full potential of extended access
hubs, SELDOC and 111;
Develop enhanced Primary Care Access in Lambeth;
Planned care – support the Peer Review work stream, and increased
usage of ERS;
Utilise the community pharmacy network & other community services to
improve outcomes for patients through integrated care and by improving
safety, access and focussing on prevention:
Key achievements
The new premium specification negotiated via the PMS Review is now
contractually signed up to by all PMS and GMS practices (the latter via a
Local Enhanced Service), and 1 APMS practice. Following complex
negotiations, a paper will go for decision to the June PCCWG regarding
assessment of performance for Jan 18-Mar 19 and changes for 2019/20.
The next meeting with the LMC is on 02/07/19.
Negotiations are ongoing with the other 5 APMS practices to agree how
the new premium specification will be delivered by them and ensure
whole population coverage through ‘equalisation’. The CCG is continuing
individual negotiation meetings with each Practice, jointly with the SELCA
PC Team and Londonwide LMCs. Following progress with each of these,
a paper will go for decision to the June PCCWG.
Appointment utilisation at the Extended Access Hubs is now amongst the
highest in London at over 90%.
The CCG has continued investment in a number of areas to support
delivery of the GP Forward View, including Resilience, Care Navigation
and Online Consultations
Work is underway to support the development of Primary Care Networks,
in accordance with the recent 5 Year GP Contract settlement. This work
builds upon previous work around the SCF pilots and LCNs. There are 9
proposed PCNs in Lambeth, and each is now providing further detail of
their Extended Hours arrangements from 01/07/19.
Practice support and engagement visits are continuing quarterly
The CCG wrote to all Practices regarding contractual changes for
2019/20, including the reversion to a practice-level GP Delivery
Framework, necessitated by funding changes associated with PCNs. This
will be combined with the Medicines Optimisation and Immunomodulatory
Drugs Schemes for 2019/20 only. Final specifications should be agreed
and issued following a paper being taken to the June PCCWG for
decision.
A review has recently been completed of Interpreting & Translation
Services commissioned for Practices across Lambeth, Southwark, and
Lewisham. This involved a significant engagement project with patients
and staff, and will be used to inform the development of commissioning
options.
Primary Care Development Better Care
71
Prim
ary
Care
Develo
pm
ent
Primary Care Development Better Care
Key risks as identified on the risk register:
Risk that the allocation for NHS Lambeth CCGs delegated primary are
commissioning is not sufficient to meet forecast 2019/20 budgets
There is a risk to the sustainability of the Lambeth GP Federations due to lack of
capacity to deliver on contracts.
There is a risk that failure to achieve equalisation of the PMS Commissioning
Intentions across GMS and APMS practices will impact on whole population
coverage of primary care delivery such as care co-ordination
Risk that poor performance of Capita in managing the Performer list, and
administration of pension statements and payments to GPs will impact upon the
delivery of services to patients, resulting in delays in GP start dates, a diminution
in access and problems closing annual accounts.
Actions taken
New risk for 2019/20 – currently being assessed so that it can be added to the Risk
Register, with appropriate updating of key mitigating actions.
This had been being mitigated through contract monitoring meetings to
demonstrate contracts are being delivered, and board-to-board meetings. The
Federations presented an annual report on their contracts at the PCCC in public on
12/9/18. In addition the CCG held a meeting to review the Federations’ audited
accounts and new 2 Year Business Plan on 25/10/18. The CCG’s commissioning
intentions gave assurance on contracts for 2019/20, with discussions ongoing
about the CCG’s wider Alliance propositions and the need for the Federations to
diversify income sources.
The development of Primary Care Networks (PCNs) has meant much of the
income derived from CCG contracts has now switched to PCNs – this has
therefore increased the risk to Federation stability. Discussions are ongoing
between Practices and Federations about what services may be offered and
purchased.
Federations launched PCN support offer to practices on 2nd May - CCG awaiting
outcome of local discussions within the new PCN's.
All PMS and GMS Practices have signed up to the new premium specification. One
APMS practice was equalised from 1st April 2018, leaving five further practices to
be equalised. Negotiations with these Practices are complex due to historical
anomalies and significant financial gaps. A number of further meetings have taken
place between the CCG, Practices, LMC and SELCA PC Team.
A paper will brought to the Primary care Working Group on 12 June 2019 with a
substantive update on all contract negotiations. This paper is likely to include some
decisions to be taken by the CCG as the delegated commissioner, including
equalisation of Streatham Place Surgery.
Overall performance across service lines by Capita is reported as poor by Lambeth
GP Practices, as elsewhere.
Discussed removing risk at PCCWG - awaiting implementation of audit
recommendations for a SEL wide risk register, then remove from CCG risk register.
Primary Care Development Better Care
72
Prim
ary
Care
Develo
pm
ent

Practice Information Support Packs Month 12 (March 2019) Managing the demand for outpatient appointments throughout 2018/19 has been a huge
challenge across South East London and London as a whole. NHS Lambeth CCG was reported to be the highest referring CCG in South East London and
the 3rd highest in London. In 2018/19, after a series of work streams and an extensive and worthwhile period of data validation, the GP referrals outturn was
9% higher than the previous year. This growth is similar to previous years, but significantly higher than our sustainability plan of 0.8% and higher than our
registered population growth, of 2.4% over this period. Further work is required in order to reduce demand to sustainable levels in line with our CCG-led
acute QIPP targets for 2019/20. Over the next few weeks the CCG will be looking at what the sustainability plan might be for 2019/20.
Data source: Monthly Referral Data direct from Trusts (not MAR, which is reported through the contracts). The activity is GP referral data
received by the acute trusts and does not relate to whether an outpatient attendances took place or not.
Demand Management – GP Referrals Better Care/Better Health
73
Better
Care
/Better
Health
North Locality South East Locality South West Locality

Primary Care Development - GP Information Report Better Care
74
Prim
ary
Care
Develo
pm
ent
• The next updated GP Information Report will be presented at the PCCWG on the 12 June 2019. It will then be available in this
report in August 2019.

Director Una Dalton
Clinical lead Dr Adrian McLachlan
Management lead Una Dalton
Key Aims 2018/19
• Support implementation of the GP Forward View.
• Deliver a high quality IM&T service to General Practice.
• Work closely with the other CCGs in the South East London Digital
Footprint.
• Develop Lambeth DataNet into a valued business intelligence resource
for all stakeholders in the service.
• Work with corporate IM&T delivery partner to provide an excellent
corporate IM&T service
• Support Programmes to deliver improved patient care.
Key achievements 2018/19
• A number of digital projects are underway in terms of local implementation
of the GP Forward View including piloting on line access and calling in
screens.
• The remediation plan with NEL CSU has been agreed and the
management of this is ongoing.
• We continue to work with SEL partners on the development of SEL wide
issues – a key project to take forward in the second quarter of this year
will be the implementation of HSCN, the replacement of the N3 network,
currently have 3 live practices on the HSCN network.
• We have appointed an interim head of IT/Digital to support this work.
• The DTG group has been refreshed with revised membership and terms
of reference. The group will meet bi monthly to drive forward our IT
agenda and will look to provide support to our five programmes of work on
IT/Digital issues.
• Communications: refreshing and updating website page and FAQ. This
will include links to research findings and summaries of key projects
undertaken using primary care data, eg Multiple Long Term Conditions.
• Lambeth DataNet 3: working with GSTT and NEL CSU to expand
DataNet to include hospital acute and adult community data, which will
enrich the research questions we can ask of DataNet.
• CCG successfully bid for funding to be a Digital Accelerator, this work will
define the digital first encounter which could be on-line, video or sign
posting to an appointment with a GP and built on the basis of providing
unscheduled care between 8 – 8. The App would provide a standardised
approach into services.
Key risks as on the risk register
• Risk of NELCSU failing to deliver
• Current Practice Telephony offering from NEL CSU will cease to work
or be of the required standard set by NHSD after migration to the
HSCN Network.
Actions taken
• We continue to work closely with NEL colleagues on the delivery of a
remediation plan. A remediation plan is in the process of being agreed to
bring the service to a satisfactory level.
• Currently working on different options for an alternative Telephony
solution for practices who take their telephony services from NEL CSU.
Enabler - Digital Services Sustainability
75
Enable
r D
igital S
erv
ices

Director Christine Caton (Performance) Andrew Parker (Business Intelligence)
Clinical lead Dr Adrian McLachlan
Management lead Brian Reynolds
Key Aims 2018/19
• Refresh Programme dashboards to reflect 2018/19 priorities as
required
• Develop and enhance the monthly Practice Information Packs
• Consolidation and reduction of performance reporting internally
• Active engagement in collaborative working with London-Wide BI
programme and South East London information and performance
Key achievements 2018/19
• The Primary Care Dashboard has been updated and will be presented at
the Primary Care Commissioning Work group meeting on the 12 June
2019. The dashboard focuses on Quality and Enablers as a deep dive
chapter and will be reported to the IGC in August in line with the agreed
timetable.
• The month 12 (March) Practice Information Support Packs went out to
practices on the 24 May. The packs included monthly progress against 5
Premium Specification indicators. These are Atrial Fibrillation, Bowel
Screening, Diabetes, Flu and HIV. The packs are intended to help
highlight and assist discussions at a practice and locality level about the
opportunities and challenges across the system, and how to learn and
best respond to them.
• The monthly Finance and QIPP Performance Report has been
streamlined and aligned with the Integrated Governance Performance
Report.
• Participating in the south east London Assurance Working Group which is
looking at the development of at scale assurance processes, and
identification of efficiencies and best practice within CCGs.
Enabler – Business Intelligence Sustainability
76
Enable
r B
usin
ess Inte
lligence

Director Christine Caton
Clinical lead Dr Adrian McLachlan
Management lead Malcolm Brydon
Key Aims 2018 / 2019
• To ensure that the Lambeth estate is mapped and monitored on an on-going
basis and to ensure appropriate dialogue is in place to manage the estate
• To improve estates utilisation and reduce void costs, working with partners to
make best use of all estate to deliver value for money
• To prioritise investment and review and aim to secure sources of investment
• Respond to population increases as a result of housing development
• Ensure the needs of the Local Care Networks as part of Lambeth Together
delivery alliances are delivered from an estates perspective
• Ensure that clinical and non-clinical space is used effectively
• Make appropriate use of Section 106/Community Interest Levy (CIL)
Contributions
• Ensure projects involving development link into the Lambeth Digital Roadmap
• Access further funding to undertake feasibility studies / option appraisals
across key Primary Care Premises.
• Deliver funded projects scheduled to complete in the 2019 / 2020 Financial
Year
• Develop and consolidate plans to deliver STPW4 Capital Projects
Key achievements 2018 / 2019
• Phase 1 of Clapham Park achieved Practical Completion on the 13 May 2019.
CIL funding is approved for Phase 2 and the construction work for Phase 2 is the
due to start in June 2019. It is expected that Phase 2 will be delivered by the end
December 2019.
• The One Public Estate Brixton Health Hub Project was completed in September
2018. An action plan has been agreed for implementation by partners
• The 2019/20 Local Improvement Grant Bid was submitted in July 2018 for 17
practices for approximately £1m. We have yet to be advised of the full extent of
approved funding.
• For Gracefield Gardens, discussions successfully concluded with the General
Practices participating in the Project. The FBC is scheduled for submission in
August 2019 which will release the ETTF funding for the project with practical
completion for Phase 1 expected by April 2020. We are seeking to align Phase 1
(ETTF) and the NHS Wave 4 Capital funded Phase 2 as far as possible to enable
a single contract to be let for both phases. The priority is to deliver Phase 2 at the
earliest opportunity to enable SLaM service to re-locate from Station House.
• The application for NHS Wave 4 capital for Baldry Gardens was approved in
December 2018. This will enable the relocation of the Streatham Common Group
Practice to Baldry Gardens. The delivery of the Project is expected on or before
March 2020. This is however, subject to addressing issues including the
agreement of a planning application.
• Akerman Health Centre is a NHS Wave 4 capital scheme and part of the SEL
STP portfolio bid to improve utilisation and clinical capacity within LIFT buildings.
Through the ‘Re-Imagining Akerman’ project we are engaging with local
stakeholders and this will help inform the Business Case submission. The
consultation exercise “Re-imaging Akerman” is complete and design work is
being progressed to deliver the outcomes of the Consultation and to optimise the
clinical space.
• The Nine Elms Vauxhall (NEV) scheme involves Lambeth and Wandsworth
CCGs and councils to address the expected significant population growth in the
area. It is intended clinical capacity will be increased in three practices in
Lambeth. Some delays have been identified in the submission of the FBC
planned for May 2019, including the Wandsworth component of the Project. The
Project Board has recommended that the Lambeth scheme will deliver by the end
March 2020
Enabler – Estates Sustainability
77
Enable
r E
sta
tes

Director Christine Caton
Clinical lead Dr Adrian McLachlan
Management lead Malcolm Brydon
Enabler – Estates Sustainability
78
Enable
r E
sta
tes
Key risks as on the risk register
• Finalisation of Lower Marsh lease.
• Crowndale – solution for development of the site needs to be identified.
• Grantham / Beckett House and Lambeth Walk Health Centre –
solutions for the development and future sustainability for these sites
needs to be identified
• As a general principle, all of the projects and developments listed
opposite all carry a degree of risk in both timing and delivery and we will
update on project specific issues as they arise.
Actions taken
• The Business Case being developed for the CCG Governing Body to
consider options to re-locate from Lower Marsh has been deferred as
staffing requirements are likely to change because of the proposed SEL
and borough re-organisations.
• A high level options appraisal for Crown Dale has been produced and is
under review with funding options being actively explored. We are working
closely with NHSPS, the landlord, to agree exact space requirements to
inform more detailed work.
• The CCG has approved funding for feasibility studies for North Lambeth
Practices and Crown Dale.
Director Una Dalton
Management Lead Lucy Day / Janie Conlin
Governing Body Lead Dr Adrian McLachlan
Key Aims 2018/19
The people within our programmes will be enabled to further develop effective
behaviours to best support delivery
• Clinical leadership (particularly the clinical network) will be harnessed as a
valuable asset to effective member engagement and leadership
succession planning
• Behaviours that demonstrate the value of listening will be actively used
• Resilience and readiness will be built within the local commissioning
system – starting with staff, leadership and membership
• CCG staff will demonstrate competent system leadership in order to
influence local system development
Key achievements to June 2019
• OD expertise to support the Lambeth Together Culture and Ways
of Working work stream in order to develop a collaborative OD
offer to the system
• OD advice to the SEL CCG system reform organisational change
• Development of suite of offers to support staff in response to staff
survey findings and in anticipation of organisational change
including lunchtime sessions; buddying; training; coaching and
mentoring
• Successful leadership of local participation in national CCG 360
stakeholder survey followed by analysis and reporting results
• Sponsorship of external consulting resource to support leadership
and resilience of AD group
• Design and launch of team coaching programme for children’s
commissioning team to support the further development of
integrated commissioning with LBL
• Development of draft proposal to review practice based
pharmacists including recommendations on how best to approach
employing a shared clinical resource
• Refresh and launch of 2019/20 appraisal process for CCG staff
• Review of CCG participation in the national NHS staff survey
process and recommendation at SEL for coming year
Enabler – Organisational Development Leadership
79
Enable
r O
rganis
ational D
evelo
pm
ent

Director Una Dalton
Management Lead Valerie Richards
Key Aims 2018/19
Strategy refresh
• Refresh CCG equalities strategy for 2019/20 setting new equalities
objectives and developing associated plans
Data use
• Ensure CCG has clear and measurable equalities objectives and targets
• Ensure appropriate data focus to enable consideration of equalities in
CQRG/Trust meetings
• Robust use of data in equality analysis for programme plans
Engaging diverse voices
• Implement WRES
• Complete equality analysis of any new/refreshed policies
• Leadership – ensure inclusive recruitment procedures and processes
• Produce statutory compliance reports as required
• Ongoing support to the development of Lambeth Together, integration with
Lambeth Council and collaborative work across SEL CCGs.
Key achievements 2018/19
• New Involving People Strategy agreed this year – identifying ‘focus’
and ‘diversity’ as engagement priorities – action plan includes
reviewing role descriptions and recruitment to ‘Patient and Public
Voice’ (PPV) roles and targeted engagement plans for CCG
priorities
• Detailed WRES briefings for GB and members of Engagement,
Equalities and Communications Committee, looking at Trust data
(which CCG WRES scoring is based on)
• Equalities and Engagement Committee was assured of WRES
compliance by GStT via CQRG in November 2018.
• NEL has provided equalities/engagement support to cover the one-
year secondment of the Head of Engagement/Equalities
• Equality Objectives for 2019/2020 refreshed taking into
consideration NHS England 10 year plan (March 2019)
• Health Inequalities objectives for 2019/2020 refreshed taking into
consideration NHS England 10 year plan (March 2019)
• NEL has provided WRES / A Model Employer update for EEC
(March 2019)
• NEL has provided WDES (Workforce Disability Equality Standard)
update for EEC (March 2019)
• Contribution Black Thrive Partners inequality measures dashboard
80
Enable
r E
qualit
y
Enabler – Equality Leadership

Director Una Dalton
Management Lead Antonia Knifton
• Key Aims• Involve people in governance
• Involvement in commissioning plans
• Involvement in annual reports
• Promote and publicise involvement
• Systematically assess, plan and act to involve people across all areas of
CCG responsibility
• Feed back and evaluate
• Implement assurance and improvement systems
• Involvement to advance equality and reduce inequalities
• Support for involvement
• Hold providers to account for involvement
Engaging effectively with residents
• Comply with public duty to engage
• Ensure engagement is planned and delivered with equalities and diversity
goals integrated at all levels
• Develop representative engagement structures and channels that include
all Lambeth residents
• Ongoing support to the development of Lambeth Together, integration with
Lambeth Council and collaborative work across SEL CCGs
• Continue to work closely with local NHS Trusts
• Continue to develop close working relationships with community and
voluntary sector involvement professionals.
• Principles for engagement updated and incorporated into new Involving
People Strategy
• PPV roles for Lambeth defined in Recognition Policy
• CCG Committee members in PPV roles included in mandatory training
(conflict of interest)
• Business Plan 2019-20 identifies priority areas for engagement by
programme
• Refreshed content on ‘Get involved’ pages of website including feedback to
patients and public; use of website and social media and Healthwatch
channels to share information promote feedback and involve people in
current projects.
• SEL engagement leads Network continues
• SEL Stakeholder Reference Group continues, with participation from CCG
lay member and also chair, in addition to engagement lead; work to re-
engage SEL Healthwatch organisations more systematically in SRG
underway with SEL comms and engagement team
• Website used to feed back on engagement eg Living Well Network, NHS
prescriptions
• EEC meetings scheduled for 2019-20; agreed minutes are included in
Governing Body papers; assurance preparation continued
• Ongoing support to programmes
• Engagement lead reaching out to Healthwatch and community
organisations
• Regular meetings and close working established with STP engagement
lead, Southwark engagement lead and LSSP team.
• Engagement planning for 2019/2020 will be refreshed to take into
consideration NHS England Long Term Plan (March 2019)
• NEL has provided engagement support to cover the one-year secondment
of the Head of Engagement/Equalities
Enabler – Involvement Leadership
Enable
r In
volv
em
ent
81

Director Una Dalton
Management Lead Charles Beardsley
Enabler – Workforce
Enable
r W
ork
forc
e
82
NHS Lambeth CCG’s Human Resources services are provided by the NEL and the organisation’s named Business Partner is Charles Beardsley, providing
support to managers and staff within the CCG. Payroll, resourcing, workforce and pensions services are provided by NEL’s in-house team.
• Staff in Post As of the 31st March 2019 the CCG’s
headcount was 74 with an FTE of 69.07. Over the
past 12 months, staffing numbers have remained
stable, with only slight fluctuation.
• Staff Turnover The yearly rolling average turnover
for March 2019 was 13.30%.
• Starters There was 1 starter in March 2019.
• Leavers There was 1 leaver in March 2019.
• Sickness The average sickness absence rate
for February 2019 was 2.2%, well below the
peak of 5.10% in August 2018.
• The long term absence percentage for February
2019 remains at zero, which is significant and a
marked decline from the peak of 4.35% in March
2018. Short term absence also remains low.
There were only 16 days total absence in
February 2019 compared to 118 days total
absence in March 2018.
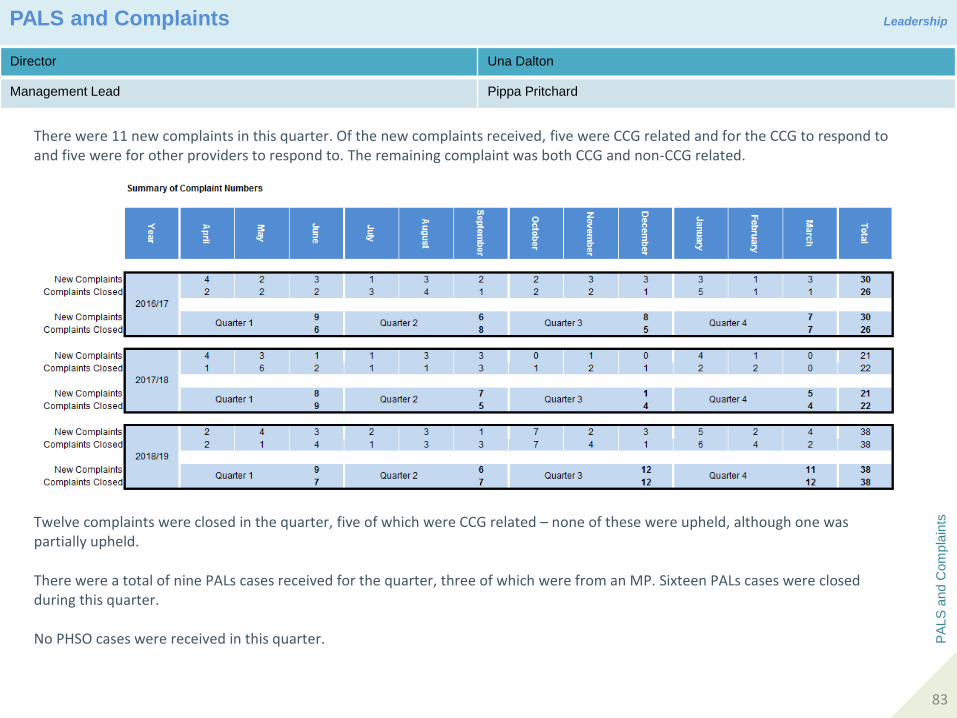
Director Una Dalton
Management Lead Pippa Pritchard
PALS and Complaints Leadership
PA
LS
and C
om
pla
ints
83
There were 11 new complaints in this quarter. Of the new complaints received, five were CCG related and for the CCG to respond to and five were for other providers to respond to. The remaining complaint was both CCG and non-CCG related.
Twelve complaints were closed in the quarter, five of which were CCG related – none of these were upheld, although one was partially upheld. There were a total of nine PALs cases received for the quarter, three of which were from an MP. Sixteen PALs cases were closed during this quarter. No PHSO cases were received in this quarter.

Director Una Dalton
Management Lead Pippa Pritchard
Freedom of Information Leadership
Fre
edom
of In
form
ation
84
The CCG saw an increase of 11% in the number of requests received in quarter 3. This follows on from a 91% increase in quarter 2and a 20% increase in quarter 1. This gives a total increase year to date of 40%
The CCG achieved 100% compliance in quarter 3 and quarter 2. This far exceeds current best practice guidance set out by the Information Commissioners Officer of 90%

Acronyms
Acro
nym
s
85

Acro
nym
s
86
Acronyms





























