Embed Size (px)
Citation preview

CONSIDERATIONS IN DESIGNING ACUTE GVHD PREVENTION TRIALS:
Patient Selection, Concomitant Treatments, S l i d A i E d iSelecting and Assessing Endpoints
CENTER FOR INTERNATIONAL BLOODAND MARROW TRANSPLANT RESEARCH

Potential conflicts/disclosures
Research support for BMT CTN trials: R h E i Li d M k ARoche, Easai, Ligand, Merck, Amgen, Supergen, Therakos, Pfizer
Research support for CIBMTR studies:Research support for CIBMTR studies:Otsuka, Amgen, Fujisawa
Analysis of Fujisawa clinical trial data done inAnalysis of Fujisawa clinical trial data done in collaboration with industry investigators; all other analyses conducted with no knowledge or input form industry supporters
ISSUES IN DESIGNING GVHD PREVENTION TRIALS
Heterogeneity of patients Heterogeneity of preparative regimensHeterogeneity of preparative regimensHeterogeneity in GVHD assessment and treatment philosophiestreatment philosophiesMultiple competing risks
ISSUES IN DESIGNING GVHD PREVENTION TRIALS
Heterogeneity of patientsHeterogeneity of preparative regimensHeterogeneity of preparative regimensHeterogeneity in GVHD assessment and treatment philosophiestreatment philosophiesMultiple competing risks

SURVIVAL AFTER HEMATOPOIETIC STEM CELLSURVIVAL AFTER HEMATOPOIETIC STEM CELL TRANSPLANTS, 1998-2003
80
100
ILIT
Y, %
60
80
HLA-identical sib (N = 14,473)
PRO
BA
B
40Unrelated (N = 5,358)
0
20 Autotransplant (N = 23,857)
YEARS0 1 2 3 4 5
ENT04_2.ppt
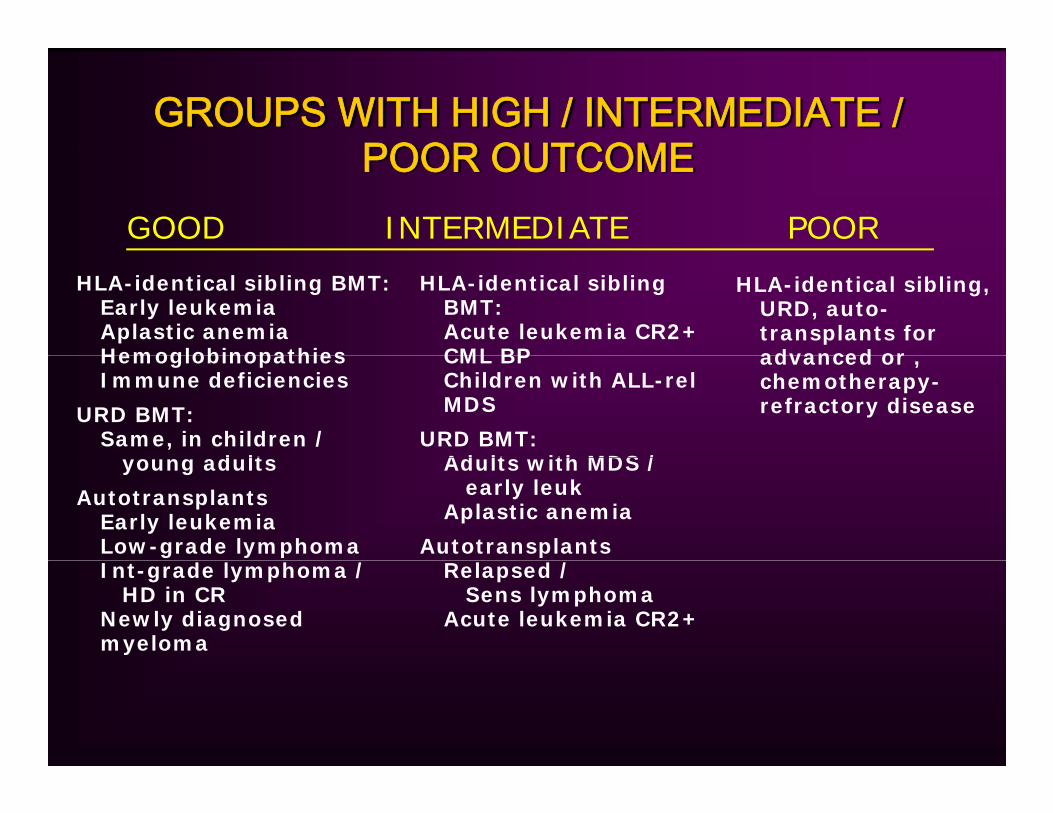
GROUPS WITH HIGH / INTERMEDIATE / POOR OUTCOMEPOOR OUTCOME
GOOD INTERMEDIATE POOR
HLA-identical sibling BMT:Early leukemiaAplastic anemiaHemoglobinopathies
HLA-identical sibling BMT:Acute leukemia CR2+CML BP
HLA-identical sibling, URD, auto-transplants for advanced or Hemoglobinopathies
Immune deficiencies
URD BMT:Same, in children /
d lt
CML BPChildren with ALL-relMDS
URD BMT:Ad lt ith MDS /
advanced or , chemotherapy-refractory disease
young adults
AutotransplantsEarly leukemiaLow-grade lymphoma
Adults with MDS / early leuk
Aplastic anemia
AutotransplantsInt-grade lymphoma /
HD in CRNewly diagnosed myeloma
Relapsed / Sens lymphoma
Acute leukemia CR2+
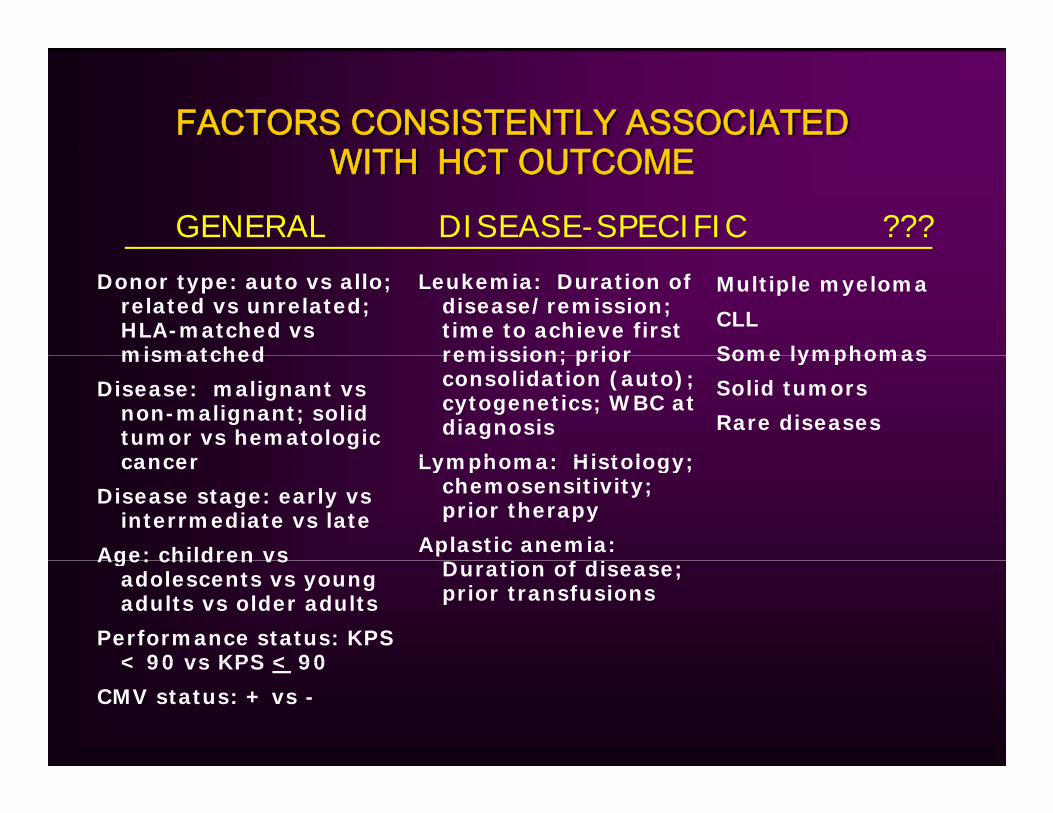
FACTORS CONSISTENTLY ASSOCIATED WITH HCT OUTCOMEWITH HCT OUTCOME
GENERAL DISEASE-SPECIFIC ???
Donor type: auto vs allo; related vs unrelated; HLA-matched vs mismatched
Leukemia: Duration of disease/remission; time to achieve first remission; prior
Multiple myeloma
CLL
Some lymphomasmismatched
Disease: malignant vs non-malignant; solid tumor vs hematologic cancer
remission; prior consolidation (auto); cytogenetics; WBC at diagnosis
Lymphoma: Histology;
Some lymphomas
Solid tumors
Rare diseases
cancer
Disease stage: early vs interrmediate vs late
Age: children vs
Lymphoma: Histology; chemosensitivity; prior therapy
Aplastic anemia: i f di
Age: children vs adolescents vs young adults vs older adults
Performance status: KPS < 90 vs KPS < 90
Duration of disease; prior transfusions
< 90 vs KPS < 90
CMV status: + vs -
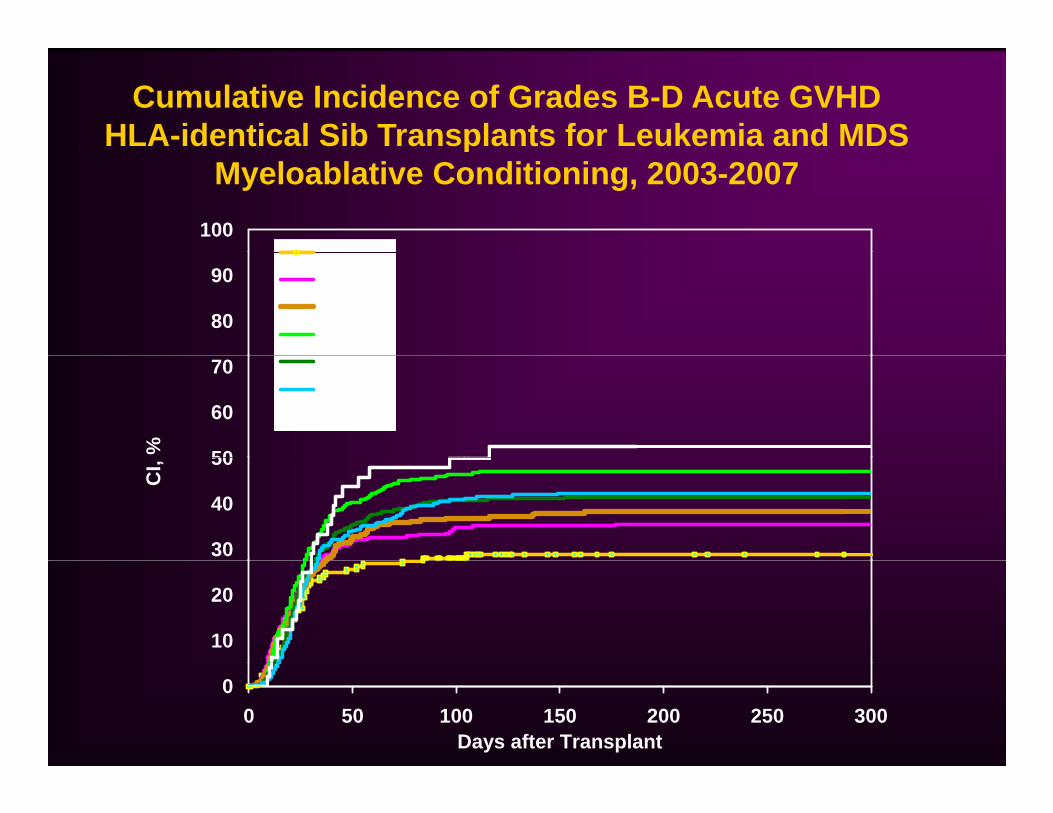
Cumulative Incidence of Grades B-D Acute GVHDHLA-identical Sib Transplants for Leukemia and MDS
1000 9 y
pMyeloablative Conditioning, 2003-2007
80
900-9 y10 - 19 y20-29 y30-39 y
50
60
70
%
40- 49 y50- 59 y>60 y
30
40
50
CI,
10
20
00 50 100 150 200 250 300
Days after Transplant
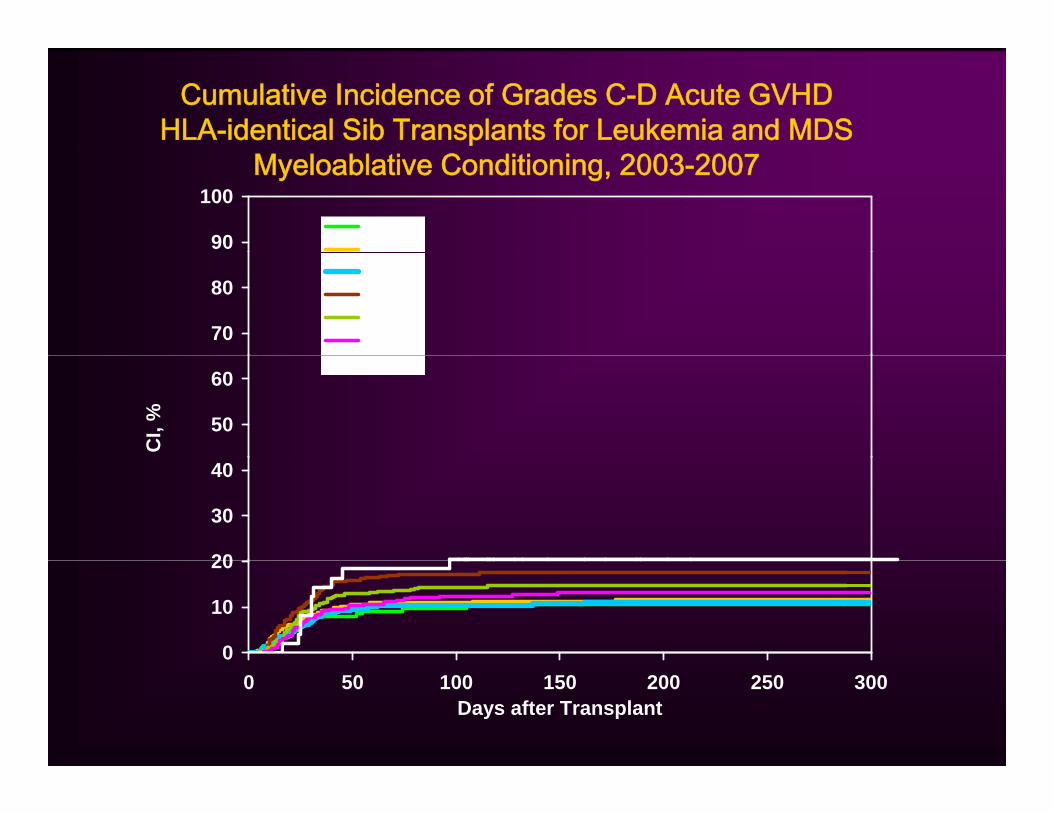
Cumulative Incidence of Grades C-D Acute GVHDHLA-identical Sib Transplants for Leukemia and MDS
90
1000-9 y10 - 19 y
Myeloablative Conditioning, 2003-2007
70
80
10 19 y20-29 y30-39 y40- 49 y50- 59 y
50
60
CI,
%
>60 y
20
30
40
0
10
20
0 50 100 150 200 250 300Days after Transplant

Cumulative Incidence of Grades B-D Acute GVHDUnrelated Donor Transplants for Leukemia and MDS
90
1000-9 y10 19 y
pMyeloablative Conditioning, 2003-2007
70
80
90 10 - 19 y20-29 y30-39 y40- 49 y50- 59 y
50
60
I, %
50 59 y>60 y
30
40
CI
10
20
00 50 100 150 200 250 300
Days after Transplant
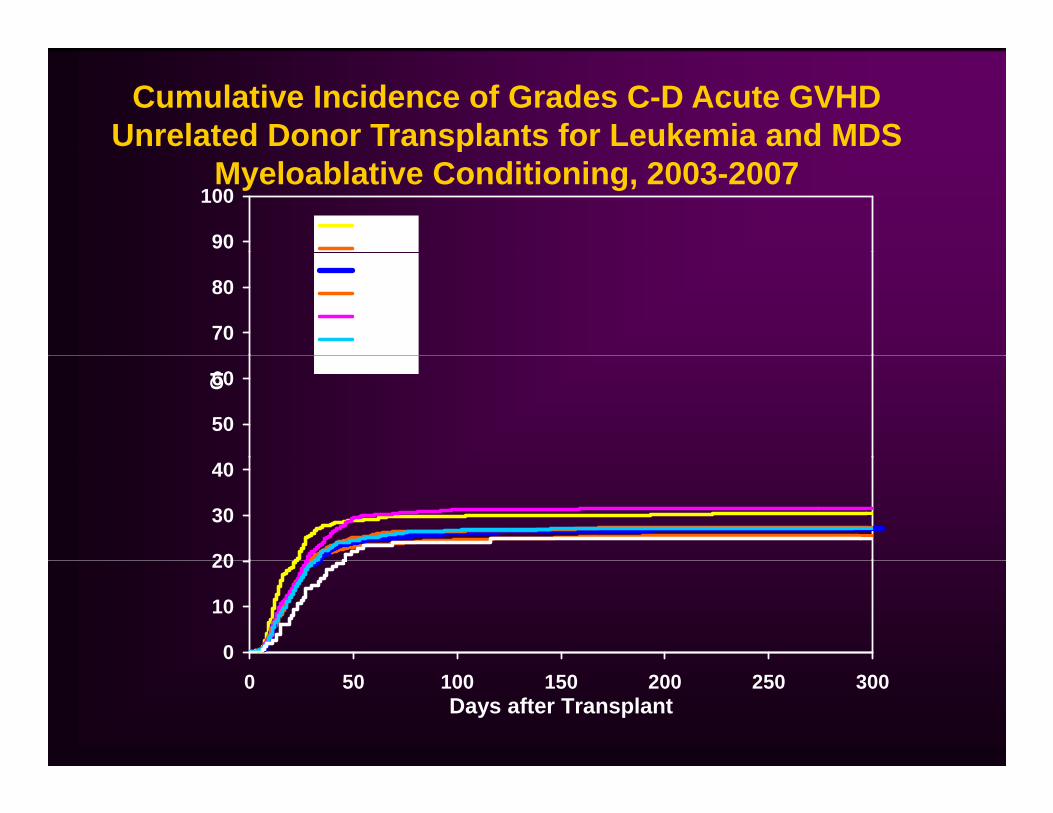
Cumulative Incidence of Grades C-D Acute GVHDUnrelated Donor Transplants for Leukemia and MDS
90
1000-9 y10 - 19 y
pMyeloablative Conditioning, 2003-2007
70
80
10 19 y20-29 y30-39 y40- 49 y50- 59 y
50
60CI
>60 y
20
30
40
0
10
20
0 50 100 150 200 250 300Days after Transplant

Cumulative Incidence of Grades B-D Acute GVHDHLA-identical Sib Transplants for Leukemia, MDS, SAA
100
Conventional Conditioning, 2003-2007
70
80
90
SAA (n=51)
AML, ALL, CML, MDS (n=2279)
50
60
70
I, %
30
40
C
10
20
00 10 20 30 40 50 60 70 80 90 100
Days after Transplant
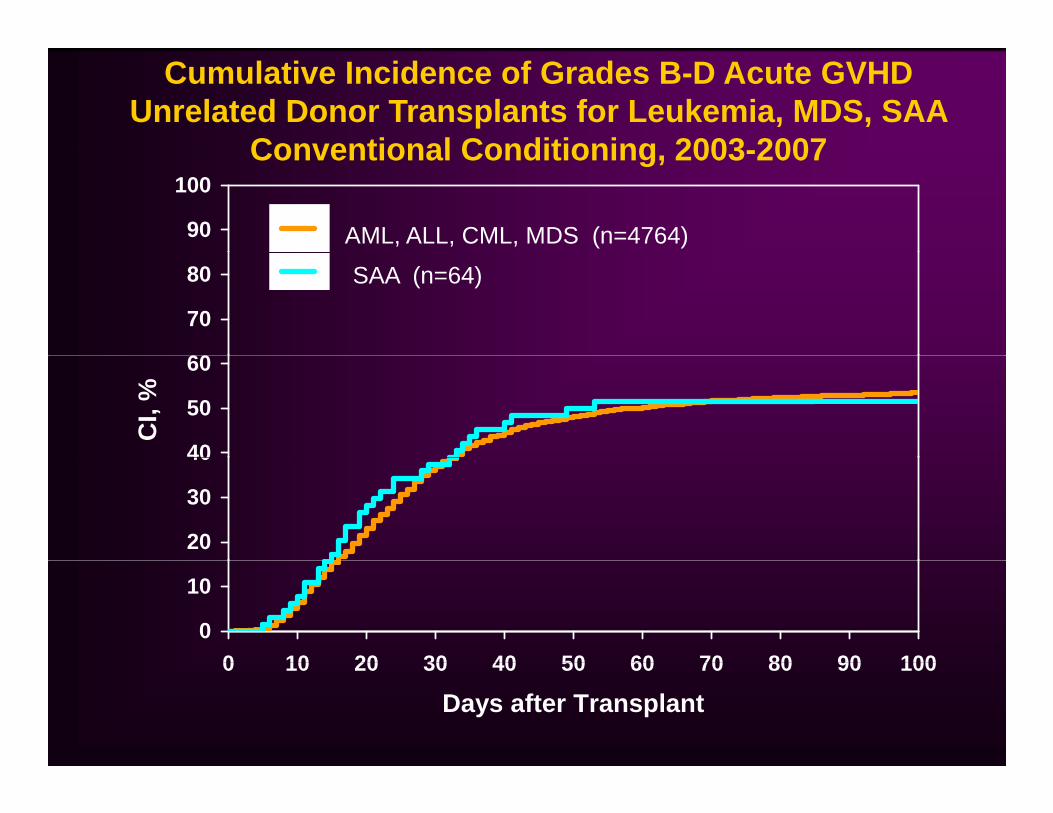
Cumulative Incidence of Grades B-D Acute GVHDUnrelated Donor Transplants for Leukemia, MDS, SAA
Conventional Conditioning 2003-2007
90
100
AML, ALL, CML, MDS (n=4764)
Conventional Conditioning, 2003-2007
60
70
80 SAA (n=64)
40
50
60
CI,
%
20
30
40
0
10
0 10 20 30 40 50 60 70 80 90 1000 10 20 30 40 50 60 70 80 90 100
Days after Transplant

PROGNOSTIC FACTORS FOR AGVHD in 1 960 adults receiving HLA-identical sib transplants1,960 adults receiving HLA identical sib transplants
Factor RR
Age 40y vs Younger (only for BM grafts) 1.43
PBSC vs BM Graft (only for young patients) 1.44SC s G a t (o y o you g pat e ts) 1.44
White/Black vs Hispanic/Asian 1.54
CML vs Acute Leukemia 1.35
KPS <90 vs 90-100 1.27
CyTBI vs BuCy 1.40
D/R CMV -/- vs not 1 20D/R CMV -/- vs not 1.20

Does This Really Matter?Does This Really Matter?
Ratanatharathorn et al. (Blood, 1998): FK506+MTX vs. CSA+MTX in HLA-FK506 MTX vs. CSA MTX in HLAidentical sibling BM transplants (n=329)Stratified on patient age (<40 vs. >=40) and donor/recipient sex match
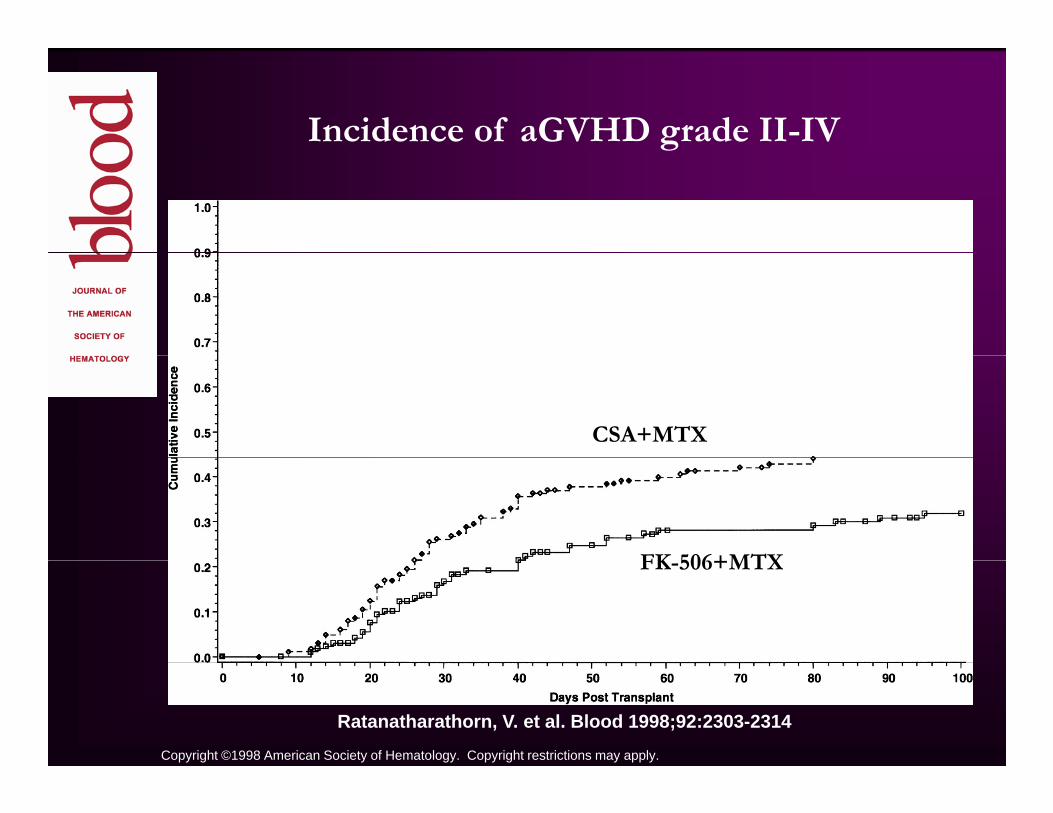
Incidence of aGVHD grade II-IVg
CSA+MTX
FK 506+MTXFK-506+MTX
Copyright ©1998 American Society of Hematology. Copyright restrictions may apply.
Ratanatharathorn, V. et al. Blood 1998;92:2303-2314

Overall Survival
CSA+MTX
FK-506+MTX
W i l f FK 506 d i l GVHD i id
Copyright ©1998 American Society of Hematology. Copyright restrictions may apply.
Ratanatharathorn, V. et al. Blood 1998;92:2303-2314
Worse survival for FK-506 group despite lower aGVHD incidence

Figure 5.
CSA+MTX (n=48)Advanced Di
FK-506+MTX (n=68)
Disease
Ratanatharathorn V et alRatanatharathorn, V. et al. Blood 1998;92:2303-2314
E lEarly Disease
Copyright ©1998 American Society of Hematology. Copyright restrictions may apply.
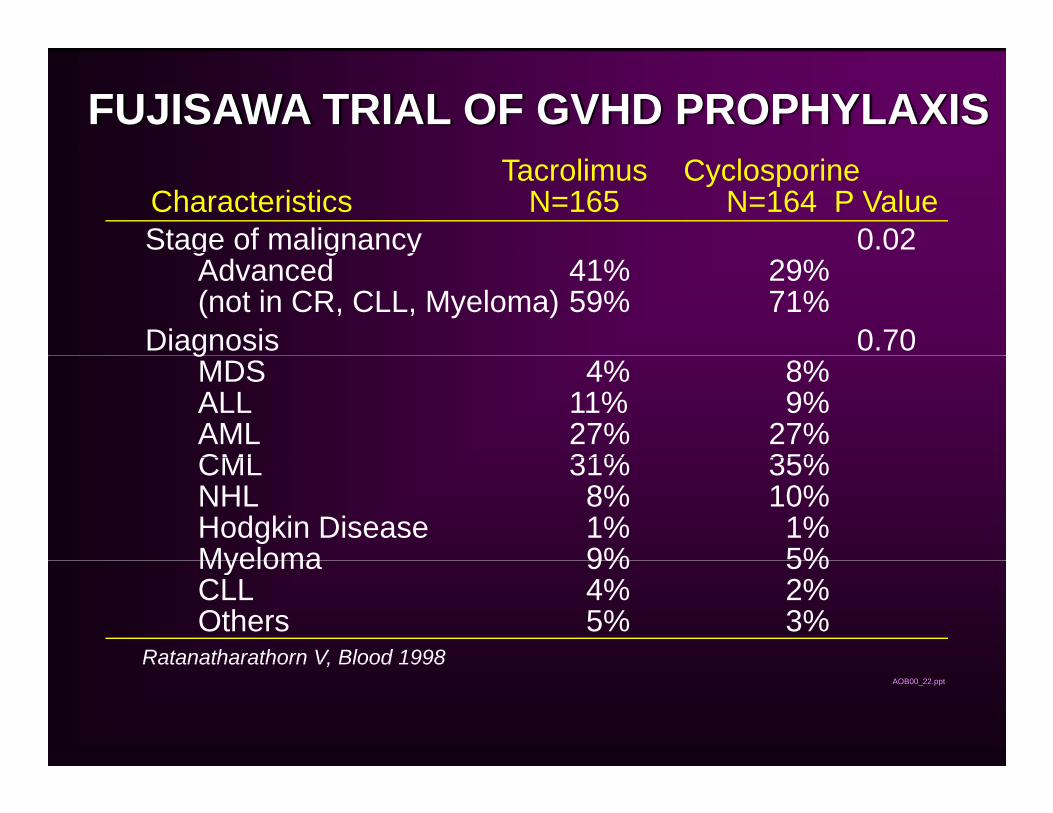
FUJISAWA TRIAL OF GVHD PROPHYLAXIS
Stage of malignancy 0.02
Tacrolimus CyclosporineCharacteristics N=165 N=164 P Value
g g yAdvanced 41% 29%(not in CR, CLL, Myeloma) 59% 71%
Diagnosis 0.70gMDS 4% 8%ALL 11% 9%AML 27% 27%CML 31% 35%CML 31% 35%NHL 8% 10%Hodgkin Disease 1% 1%Myeloma 9% 5%Myeloma 9% 5%CLL 4% 2%Others 5% 3%
Ratanatharathorn V, Blood 1998AOB00_22.ppt
Ratanatharathorn V, Blood 1998
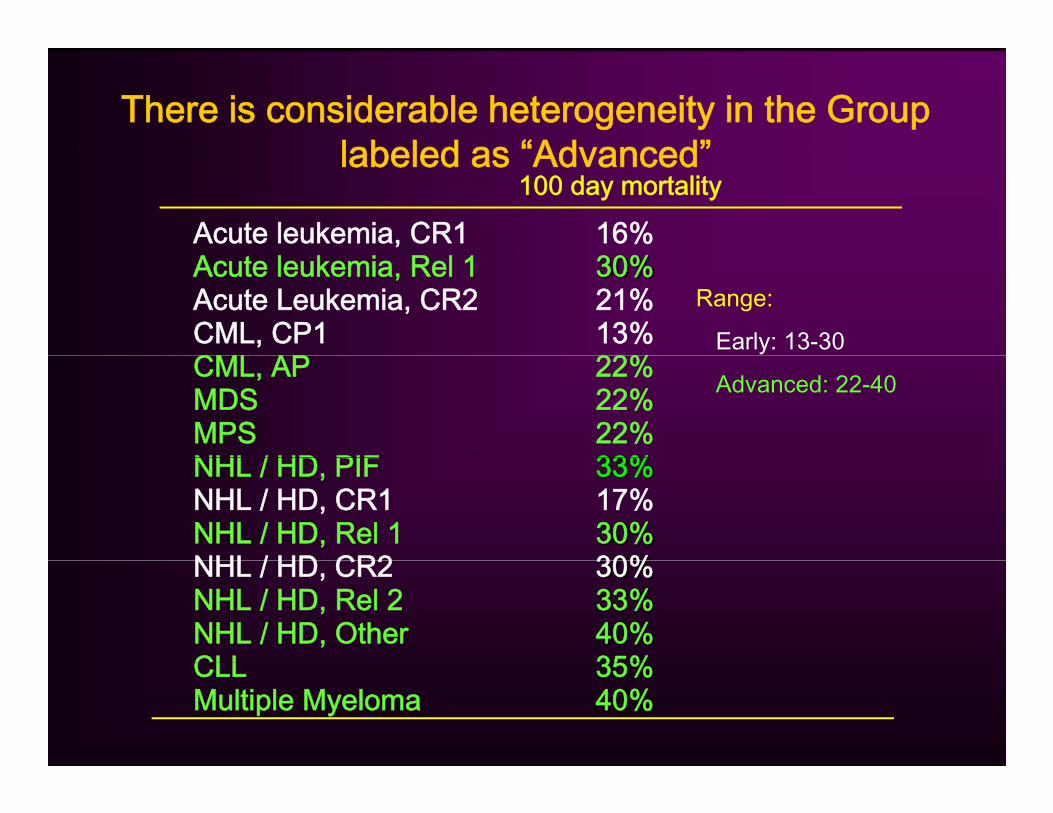
There is considerable heterogeneity in the Group labeled as “Advanced”labeled as Advanced
Acute leukemia, CR1 16%100 day mortality
Acute leukemia, Rel 1 30%Acute Leukemia, CR2 21%CML, CP1 13%C 22%
Range:
Early: 13-30CML, AP 22%MDS 22%MPS 22%NHL / HD PIF 33%
Advanced: 22-40
NHL / HD, PIF 33%NHL / HD, CR1 17%NHL / HD, Rel 1 30%NHL / HD CR2 30%NHL / HD, CR2 30%NHL / HD, Rel 2 33%NHL / HD, Other 40%CLL 35%CLL 35%Multiple Myeloma 40%
Further investigation into whether imbalance gin prognostic factors led to survival difference
Comparison of matched IBMTR controls for advanced disease patients in abovefor advanced disease patients in above trial (n=116 )Matched on diagnosis, pre-tx disease status, age (within 5 years)Controls received CSA+MTX
Horowitz et al, BBMT, 1999)
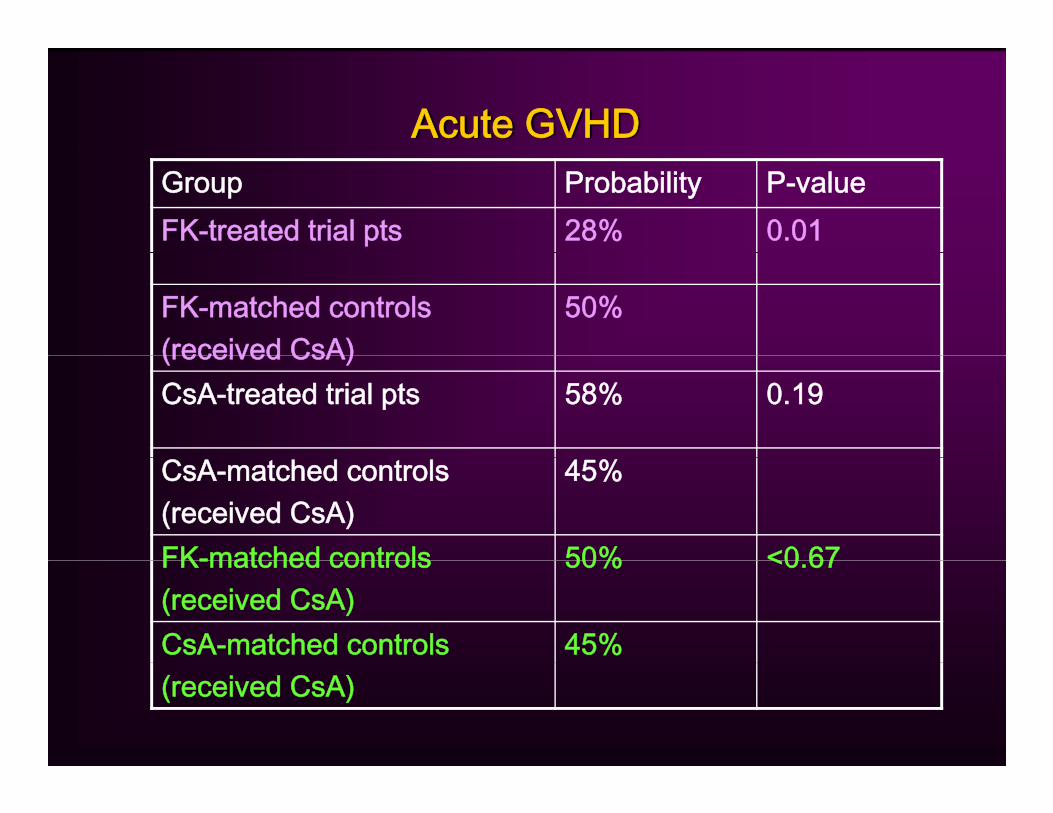
Acute GVHDGroup Probability P-valueFK-treated trial pts 28% 0.01
FK-matched controls(received CsA)
50%(received CsA)CsA-treated trial pts 58% 0.19
CsA-matched controls(received CsA)
45%
FK-matched controls 50% <0 67FK-matched controls(received CsA)
50% <0.67
CsA-matched controls 45%(received CsA)

Two-Year SurvivalGroup Probability P-valueFK-treated trial pts 27% 0.51
FK-matched controls(received CsA)
24%(received CsA)CsA-treated trial pts 42% 0.66
CsA-matched controls(received CsA)
45%
FK-matched controls 24% <0 01FK-matched controls(received CsA)
24% <0.01
CsA-matched controls 45%(received CsA)

ISSUES IN DESIGNING GVHD PREVENTION TRIALS
Heterogeneity of patients Heterogeneity of preparative regimensHeterogeneity of preparative regimensHeterogeneity in GVHD assessment and treatment philosophiestreatment philosophiesMultiple competing risks
Why Does Conditioning Regimen Matter?Why Does Conditioning Regimen Matter?
Affects GVHD risk and timing (myeloablative vs reduced intensity vs minimal intensity)Affects risk of other competing events (early morbidity and mortality)Variable interaction with treatments to be tested

PROGNOSTIC FACTORS FOR AGVHD in 1 960 adults receiving HLA-identical sib transplants1,960 adults receiving HLA identical sib transplants
Factor RR
Age 40y vs Younger (only for BM grafts) 1.43
PBSC vs BM Graft (only for young patients) 1 44PBSC vs BM Graft (only for young patients) 1.44
White/Black vs Hispanic/Asian 1.54
CML vs Acute Leukemia 1.35
KPS <90 vs 90-100 1.27
CyTBI vs BuCy 1.40
D/R CMV -/- vs not 1 20D/R CMV -/- vs not 1.20
Why Does Conditioning Regimen Matter?Why Does Conditioning Regimen Matter?
Affects GVHD risk and timing (myeloablative vs reduced intensity vs minimal intensity)Affects risk of other events (early morbidity and mortality)Variable interaction with treatments to be tested
BMT CTN 0402: FK+MTX vs FK+Sirolimus for GVHD Prophylaxis after HLA-id sib PBSCT
Endpoint – GVHD-free survivalMonitoring rules: mucositis and VODg
Stopped for excessive VODRisk found to be predominantly in patients receiving BuCy conditioningRe-opened with restriction to TBI-based
diti iconditioning

Why Does Conditioning Regimen Matter?Why Does Conditioning Regimen Matter?
Affects GVHD risk and timing (myeloablative vsAffects GVHD risk and timing (myeloablative vs reduced intensity vs minimal intensity)Affects risk of other events (early morbidity and ( y ymortality)Variable interaction with treatments to be testedBUT……….
Results of GVHD prophylaxis tested with a i l i f l dparticular regimen are often extrapolated to
other regimens without further evaluation
ISSUES IN DESIGNING GVHD PREVENTION TRIALS
Heterogeneity of patients Heterogeneity of preparative regimensHeterogeneity of preparative regimensHeterogeneity in GVHD assessment and treatment philosophiestreatment philosophiesMultiple competing risks

Interobserver Variability
Stratification on center helpful to address institutional differences in approach – but not individual differencesppBlinding
DesirableExpensiveDifficult (impossible?) when drug levels must be monitored or when therapies affect levels of other drugsp g
Independent observersExpensiveL i i ll diffi lLogistically difficult
Collection of primary data – allows computation of grade by predetermined algorithm, external reviewy p g

Treatment before reaching primary endpointTreatment before reaching primary endpoint
BMT CTN 0302: Treatment for Grades B-D AGVHDRequired enrollment within 24 hours of startingRequired enrollment within 24 hours of starting corticosteroids MANY patients ineligible because of corticosteroid therapy for Grade A AGVHD, including stage 1 skin only
– What we do is different from what we say we doPrevention trials that have Grade B-D or IV-IV AGVHD as anPrevention trials that have Grade B D or IV IV AGVHD as an endpoint may be compromised by treatments initiated for lesser degrees of GVHD
0402: Primary endpoint includes Grade II IV AGVHD or0402: Primary endpoint includes Grade II-IV AGVHD or treatment for Grade I GVHDStratification by center

ISSUES IN DESIGNING GVHD PREVENTION TRIALS
Heterogeneity of patients Heterogeneity of preparative regimensHeterogeneity of preparative regimensHeterogeneity in GVHD assessment and treatment philosophiestreatment philosophiesMultiple competing risks
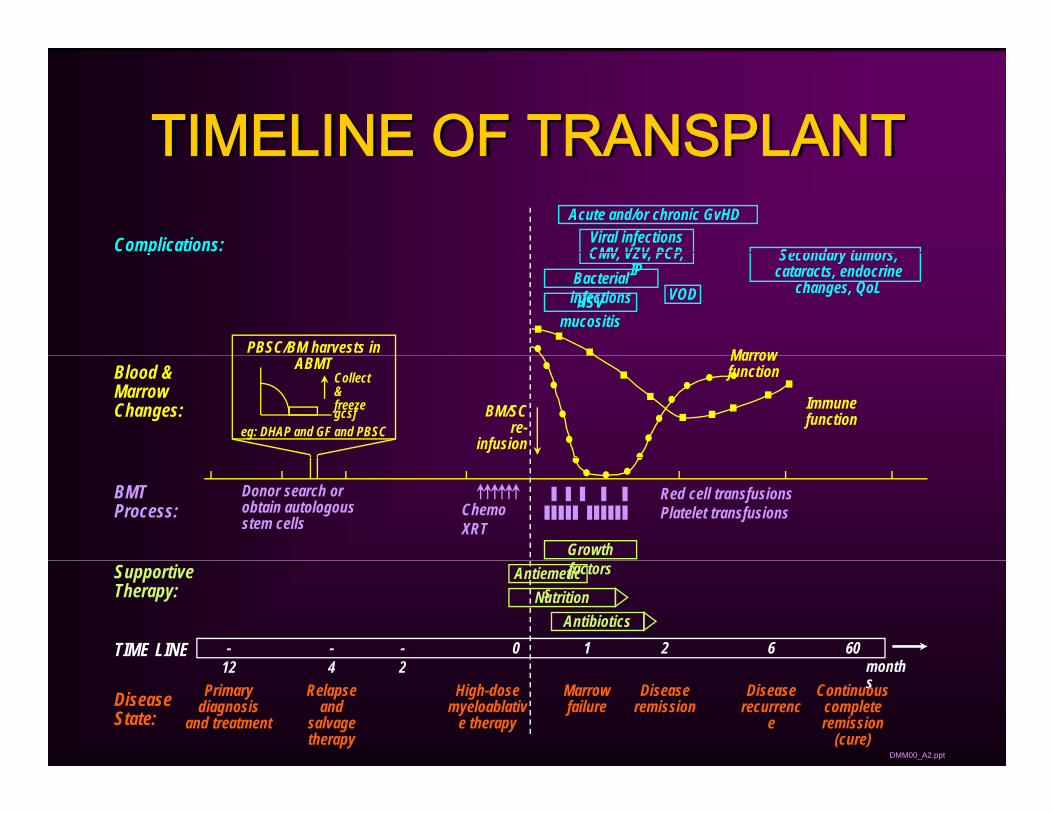
TIMELINE OF TRANSPLANTTIMELINE OF TRANSPLANTComplications: Secondary tumors
Acute and/or chronic GvHDViral infectionsCMV VZV PCPp
PBSC/BM harvests in
Secondary tumors, cataracts, endocrine
changes, QoL
CMV, VZV, PCP, IPBacterial
infectionsHSV mucositis
VOD
MarrowBlood & Marrow Changes:
ABMT
BM/SCre-
infusion
Marrow function
Immune function
eg: DHAP and GF and PBSC
Collect & freezegcsf
BMT Process:
Growth
Red cell transfusionsPlatelet transfusions
Donor search or obtain autologous stem cells
Chemo XRT
Supportive Therapy:
TIME LINE -12
-4
-2
0 1 2 6 60th
AntibioticsNutrition
Antiemetics
factors
DMM00_A2.ppt
12 4 2 monthsMarrow
failureDisease
remissionDisease
recurrence
Continuous complete remission
(cure)
High-dose myeloablativ
e therapy
Primary diagnosis
and treatment
Relapse and
salvage therapy
Disease State:
HOW DO COMPETING RISKS AFFECT ABILITY TO DO CLINICAL TRIALS IN HCT?DO CLINICAL TRIALS IN HCT?
Complicates the primary endpointComplicates the primary endpointHow do you treat patients who die before they have a chance to get the primary endpoint?have a chance to get the primary endpoint?May make final result unclear
Impairs ability to attribute toxicities to interventionImpairs ability to attribute toxicities to interventionMay lead to reporting many adverse events
May be increased by intervention even if GVHDMay be increased by intervention even if GVHD is decreased leading to overall adverse result
Impact of Competing Risks of Choice of EndpointImpact of Competing Risks of Choice of Endpoint
Acute GVHD – may be decreased at theAcute GVHD – may be decreased at the cost of increasing other toxicities
Need to ensure that the therapy doesNeed to ensure that the therapy does “no harm”, ie., unacceptable increases in adverse events, infections, non-, ,relapse mortality, recurrent malignancy
Survival – impacted by many things other than GVHD – unlikely to be able to show a benefit

Simulation Study using Multistate Models: What if AGVHD was decreased with NO impact on the rate of p
relapse or other causes of TRM?1459 patients with acute leukemia in CR1
Relapse TRM Survival
Real 17% 20% 65%
No AGVHD 18% 11% 72%
50% ↓ in AGVHD
17% 16% 69%

BMT CTN 0402: Composite Endpoint
Primary ObjectiveTo compare the rates of 114-day Grades II-IV acute
GVHD f i l b t t dGVHD-free survival between study arms
Rationale: Considers potential effects on both acuteRationale: Considers potential effects on both acute GVHD and TRM in primary endpoint
80% power to detect an increase in GVHD-free survival 114 days from randomization from 60 75%75%Sample size n = 312 patients

Summary
Transplant outcomes are influenced by many patient, disease and treatment factors – these must be considered for their
t ti l f di f l ti f GVHD ipotential confounding of evaluation of GVHD regimensThere is considerable variability in GVHD assessment and treatment approaches – blinding, stratification on center are importantGVHD is an important barrier to successful BMT outcome but not the only onethe only one
Improved survival requires better therapies to prevent GVHD AND to prevent and treat other transplant-related complications and disease recurrencecomplications and disease recurrenceA good GVHD prevention strategy must decrease GVHD without excessively increasing other causes of morbidity and mortality BUT cannot be expected to substantially improve survival by itself





























