Embed Size (px)
Citation preview
Alimenti e salute
dalla nascita alletagrave anziana
Prevenire e curare
con la giusta alimentazione
Comune di Genzano di
Roma
Sala delle Armi
Palazzo Sforza Cesarini
27 Settembre 2014
La corretta dieta per la gestante Dott Grazia Carroni - ginecologa
La corretta alimentazione in gravidanza atta
ad agevolare le fisiologiche modificazioni
gravidiche al fine di prevenirne le
complicanze (aborto parto pretermine
diabete preeclampsia etc) crea le basi per
un adeguato sviluppo del feto presupposto
indispensabile a garantire uno stato di
buona salute nel nascituro sia nellrsquoimmediato
periodo neonatale che nella vita adulta
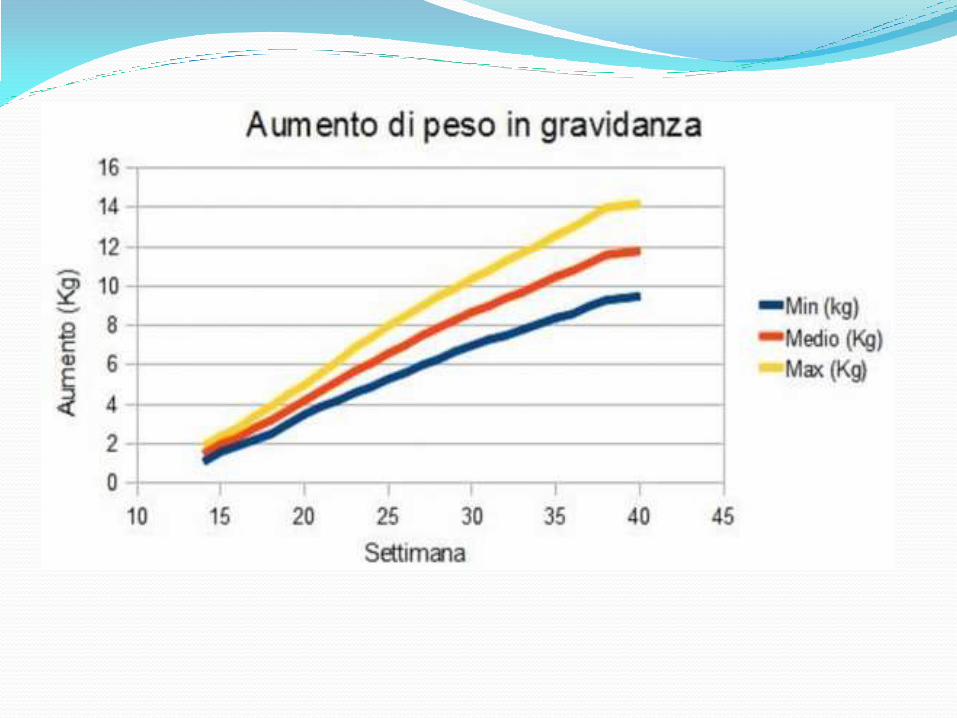
laumento del peso corporeo durante la
prima metagrave della gravidanza egrave dovuto
allaumento dei tessuti di riserva mentre
successivamente egrave rappresentato dal
prodotto del concepimento
Varia comunque a seconda delletagrave della
paritagrave e della costituzione corporea
In gravidanza crsquoegrave un aumento di richiesta di
energia necessaria per la sintesi dei nuovi
tessuti sia del prodotto del concepimento
che degli organi materni (utero mammelle
grasso) per lattivitagrave metabolica della unitagrave
feto placentare e per il normale lavoro della
gestante
La richiesta giornaliera di calorie egrave di circa
2100 2200 e 2300 kcal al di nei trimestri 1
2 e 3deg
Componenti che determinano lrsquoaumento i peso in gravidanza
Il regime dietetico deve considerare le condizioni nutrizionali
al momento del concepimento e il bisogno alimentare attuale
e remoto
Lalimentazione inadeguata si ripercuote negativamente sullevoluzione della gravidanza e sullaccrescimento fetale Una riduzione dellapporto quantitativo ma ancor piugrave di quello qualitativo puograve esitare in
bullneonato di insufficiente peso alla nascita con sviluppo osseo e dentale insufficiente bullcomplicazioni della gestazione quali parto pretermine distocia del travaglio
bulldifficoltagrave nellallattamento lalimentazione ipercalorica puograve d altro canto determinare
bullgestosi bulldisturbi digestivi bulldiabete gestazionale bullmacrosomia fetale con possibile conseguente distocia da sproporzione fetopelvica
EQUILIBRIO GLICEMICO = IG CG
durante tutta la gravidanza egrave importante
mantenere lequilibrio glicemico
costante ed adeguato apporto proteico
adeguata introduzione di liquidi
adeguato apporto di vitamine e sali
le modificazioni in senso diabetogeno del
metabolismo degli zuccheri in senso
chetogenico del metabolismo dei grassi e la
necessita di incrementare la quota proteica
giornaliera consigliano
bull5 pasti al di
bullcarboidrati ad ogni pasto
bullolio vergine doliva
bullsemi
bullesclusione degli zuccheri raffinati
bullproteine ad ogni pasto
esempio di colazione
frullato di
2 cucchiai di yogurth
2 cucchiai di olio di lino
12 banana
12 succo di limone
1 cucchiaio di riso integrale
1 cucchiaio di miele
2 cucchiaini di semi oleosi
Lalimentazione deve apportare una adeguata
quantitagrave di colesterolo utile nella produzione
attraverso il pregnenolone del progesterone uova
uova di pesce acciughe crostacei e molluschi
alimenti ricchi di omega 3 pesce azzurro almeno tre
volte alla settimana
Lapporto di folati indispensabili per la prevenzione
in questa epoca delle patologie del tubo neurale puograve
essere assicurato con le verdure e la frutta (kiwi
fragole arance) il Calcio puograve essere introdotto con
semi di sesamo e formaggio caprino
I TRIMESTRE
Modificazioni materne embriogenesi e placentazione
II TRIMESTRE
IN QUESTO PERIODO egrave MOLTO IMPORTANTE ATTIVARE LA
TIROIDE ATTRAVERSO LrsquoASSUNZIONE DI SELENIO
Componente delle selenoproteine ha effetti immunomodulatori e
svolge un ruolo chiave nel metabolismo degli ormoni tiroidei nella
famiglia delle deiodinasi Il suo deficit egrave responsabile del cretinismo
edematoso endemico
Fonti naturali di selenio sono le frattaglie pesce molluschi carne
latte lievito di birra pasta riso funghi noci
La seleneproteina detta GPx ( glutatione perossidasi) egrave un potente
regolatore della sintesi degli ormoni tiroidei e protegge dal danno
ossidativo
II TRIMESTRE
Tra le deiodinasi la D3 egrave particolarmente localizzate nelle cellule del
cervello fegato fetale placenta e pelle Protegge il concepito dalla
eccessiva esposizione agli ormoni tiroidei
Lipotiroidismo subclinico si associa a distacco di placenta parto
pretermine e aborto (Casey 2005) e al rischio di sviluppo nel post
partum di tiroidite autoimmune e di sviluppo cognitivo subottimale nella
prole (Papi e coll 2007) Dose giornaliera selenio egrave 60 microgrammi
Le richieste fetali impongono di introdurre con la dieta anche agenti
antiossidanti vit C vit E betacarotene
III TRIMESTRE
In questo periodo della gestazione il notevole
accrescimento ponderale fetale e le variazione in senso
procoagulatorio dei parametri ematici consigliano di
ridurre i carboidrati di aumentare le proteine di origine
vegetale e di favorire la funzione renale
Si evitino funghi e asparagi e si limitino ananas kiwi
salvia per la loro azione sulla coagulazione
NAUSEA ED EMESI GRAVIDICA
Dobbiamo ridurre i carboidrati evitare dolci e liquidi limitare le proteine
Nella dieta sono utili
verdure amare
limone
zenzero
aceto
Per stabilizzare lambiente gastrico bisogna alcalinizzarlo
Migliorare la funzione epatica evitando fritti limitando gli ortaggi gialli
(carotenoidi) e le crucifere (per lo zolfo)
dare carboidrati facili senza glutine
coleretici e colagoghi tipo zucchine marinate con aglio menta e aceto
fragole kiwi papaya (aiuta a digerire ed egrave drenante ricca di K) e avocado
LA MINACCIA DABORTO
Dobbiamo fornire lorganismo di
Magnesio fonti sono germe di grano fagioli ceci cereali integrali riso
avena banane kiwi uva mais
Antiossidanti antinfiammatori ottenere lequilibrio glicemico omega 3 e
fibre Possiamo consigliare olio di semi di lino noci e frutta fresca uova
tonno e pesce spada Per lacido lipoico patate broccoli spinaci fegato
cuore carni rosse
ALIMENTAZIONE ED AMNIOCENTESI
evitare le contrazioni con alimenti ricchi di Mg e K riso patate
fagiolini zucchine banane
favorire la funzione epatica in senso procoagulante uova fegato
pomodori fragole peperonicarote zucca soiabrassicacee e
formaggio fuso
evitare le infezioni aglio zenzero cipolla prezzemolo chiodi di
garofano limone per la loro funzione immunostimolante
PREVENZIONE DELLE INFEZIONI GRAVIDICHE
Ligiene degli alimenti egrave fondamentale per la
prevenzione della toxoplasmosi
Bisogna mantenere un buon equilibrio glicemico e
seguire una dieta ricca di fibre e di antiossidanti quali
cipolla olio di oliva curcuma mirtilli riso integrale
frutta secca zenzero e aglio
IMPORTANZA DELLA COTTURA DEI
CIBI PER OTTENERE IL MIGLIOR
RISULTATO SOTTO IL PROFILO DELLA
DIGERIBILITA E DELLA QUALITA
PREVENZIONE DELLA GESTOSI
Consigliabile introdurre con la dieta pochi zuccheri molte
proteine (molto pesce e latte poche carni rosse) alimenti a
basso indice glicemico e verdure ricche di acqua come
fragole patate cipolle e cicoria
Per diminuire le resistenze vascolari e i grassi circolanti egrave
utile assumere prezzemolo ananas finocchio cipolla melone
aglio e fragole
Per migliorare la funzione cuore-reni sono utili legumi frutta
secca miele cereali integrali rucola vongole e uova
Iodine deficiency in pregnant women living in the South East
of the UK the influence of diet and nutritional supplements
on iodine status Bath SC Walter A Taylor A Wright J Rayman MP Author information
Iodine is a key component of the thyroid hormones which are crucial for brain development
Adequate intake of iodine in pregnancy is important as in utero deficiency may have lifelong
consequences for the offspring Data on the iodine status of UK pregnant women are sparse
and there are no such data for pregnant women in the South East of the UK A total of 100
pregnant women were recruited to a cross-sectional study carried out at the Royal Surrey
County Hospital Guildford at their first-trimester visit for an ultrasound scan The participants
provided a spot-urine sample (for the measurement of urinary iodine concentration (UIC) and
creatinine concentration) and 24 h iodine excretion was estimated from the urinary
iodinecreatinine ratio Women completed a general questionnaire and a FFQ The median UIC
(85middot3 μgl) indicated that the group was iodine deficient by World Health Organisation criteria
The median values of the iodinecreatinine ratio (122middot9 μgg) and of the estimated 24 h iodine
excretion (151middot2 μgd) were also suggestive of iodine deficiency UIC was significantly higher in
women taking an iodine-containing prenatal supplement (n 42) than in those not taking such a
supplement (Plt 0middot001) In the adjusted analyses milk intake maternal age and iodine-
containing prenatal supplement use were positively associated with the estimated 24 h urinary
iodine excretion Our finding of iodine deficiency in these women gives cause for concern We
suggest that women of childbearing age and pregnant women should be given advice on how to
improve their iodine status through dietary means A national survey of iodine status in UK
pregnant women is required
Maternal and in utero determinants of type 2 diabetes risk in the
young Bruce KD Abstract
The global prevalence of diabetes mellitus has reached epidemic proportions In 2010 it was estimated
that 64 of the adult population (285 million) have diabetes In recent years the incidence of type 2
diabetes (T2D) a condition traditionally associated with aging has been steadily increasing among
younger individuals It is now a well-established notion that the early-life period is a critical window of
development and that influences during this period can developmentally prime the metabolic status of the
adult This review discusses the role of maternal and in utero influences on the developmental priming of
T2D risk Both human epidemiological studies and experimental animal models are beginning to
demonstrate that early dietary challenges can accelerate the onset of age-associated metabolic
disturbances including insulin resistance T2D obesity hypertension and cardiovascular disease These
findings show that poor maternal nutrition can prime a prediabetes phenotype often manifest as insulin
resistance by very early stages of life Thus the maternal diet is a critical determinant of premature T2D
risk While the mechanisms that link early nutrition to age-associated metabolic decline are currently
unclear preliminary findings suggest perturbations in a number of processes involved in cellular aging
such as changes in longevity-associated Sirtuin activity epigenetic regulation of key metabolic genes and
mitochondrial dysfunction Preliminary studies show that pharmacological interventions in utero and dietary
supplementation in early postnatal life may alleviate insulin resistance and reduce T2D risk However
further studies are warranted to fully understand the relationship between the early environment and long-
term effects on metabolism Such mechanistic insights will facilitate strategic interventions that prevent
accelerated metabolic decline and the premature onset of T2D in the current and future generations
Counteracting oxidative stress in pregnancy through modulation
of maternal micronutrients and omega-3 fatty acids DSouza V1 Chavan-Gautam P Joshi S Abstract
During pregnancy oxidative stress has been implicated in the pathophysiology of
preeclampsia and preterm birth leading to poor birth outcome Hyperhomocysteinemia
caused as a consequence of altered micronutrients like folic acid and vitamin B12 is
associated with increased production of reactive oxygen species that generate oxidative
stress These micronutrients are important determinants of methyl donor s-adenosyl
methionine while phospholipids are important methyl acceptors in the one-carbon
metabolic cycle A series of our studies in women during pregnancy have demonstrated
altered levels of these micronutrients and the negative association of docosahexaenoic
acid with homocysteine Various strategies to counteract oxidative stress
during pregnancy such as antioxidant therapy have been examined and found to be
inconsistent In this review we focus on the role of oxidative stress in pregnancy and
discuss the possibility of ameliorating it through modulation of maternal micronutrients
and omega 3 fatty acids especially docosahexaenoic acid We propose for the first time
that manipulation of one-carbon metabolism by maternal diet could be a potential
mechanism to counteract oxidative stress through homocysteine lowering effects and
help in reducing the risk for adverse pregnancyoutcomes
The influence of a low glycemic index dietary intervention on maternal
dietary intake glycemic index and gestational weight gain
during pregnancy a randomized controlled trial McGowan CA Walsh JM Byrne J Curran S McAuliffe FM1 Abstract
BACKGROUND Maternal diet is known to impact pregnancy outcome Following a low glycemic index (GI) diet during pregnancy has been shown
to improve maternal glycemia and reduce infant birthweight and may be associated with a higher fibre intake We assessed the
impact of a low GI dietary intervention on maternal GI nutritional intake and gestational weight gain (GWG) during pregnancy Compliance and acceptability of the low GIdiet was also examined METHOD Eight hundred women were randomised in early pregnancy to receive low GI and healthy eating dietary advice or to receive
standard maternity care The intervention group received dietary advice at a group education session before 22 weeks gestation
All women completed a 3 day food diary during each trimester of pregnancy Two hundred and thirty five women from the intervention arm and 285 women from the control arm returned complete 3x3d FDs and were included in the present analysis RESULTS Maternal GI was significantly reduced in the intervention group at trimester 2 and 3 The numbers of women within the lowest
quartile of GI increased from 37 in trimester 1 to 52 in trimester 3 (Pthinspltthinsp0001) among the intervention group The intervention
group had significantly lower energy intake (Pthinspltthinsp005) higher protein ( TE) (Pthinspltthinsp001) and higher dietary fibre intake (Pthinspltthinsp001)
post intervention Consumption of food groups with known high GI values were significantly reduced among the intervention group Women in the intervention low GI group were less likely to exceed the Institute of Medicines GWG goals CONCLUSION A dietary intervention in early pregnancy had a positive influence on maternal GI food and nutrient intakes and GWG Following
a low GI diet may be particularly beneficial for women at risk of exceeding the GWG goals for pregnancy

La corretta alimentazione in gravidanza atta
ad agevolare le fisiologiche modificazioni
gravidiche al fine di prevenirne le
complicanze (aborto parto pretermine
diabete preeclampsia etc) crea le basi per
un adeguato sviluppo del feto presupposto
indispensabile a garantire uno stato di
buona salute nel nascituro sia nellrsquoimmediato
periodo neonatale che nella vita adulta
laumento del peso corporeo durante la
prima metagrave della gravidanza egrave dovuto
allaumento dei tessuti di riserva mentre
successivamente egrave rappresentato dal
prodotto del concepimento
Varia comunque a seconda delletagrave della
paritagrave e della costituzione corporea
In gravidanza crsquoegrave un aumento di richiesta di
energia necessaria per la sintesi dei nuovi
tessuti sia del prodotto del concepimento
che degli organi materni (utero mammelle
grasso) per lattivitagrave metabolica della unitagrave
feto placentare e per il normale lavoro della
gestante
La richiesta giornaliera di calorie egrave di circa
2100 2200 e 2300 kcal al di nei trimestri 1
2 e 3deg
Componenti che determinano lrsquoaumento i peso in gravidanza
Il regime dietetico deve considerare le condizioni nutrizionali
al momento del concepimento e il bisogno alimentare attuale
e remoto
Lalimentazione inadeguata si ripercuote negativamente sullevoluzione della gravidanza e sullaccrescimento fetale Una riduzione dellapporto quantitativo ma ancor piugrave di quello qualitativo puograve esitare in
bullneonato di insufficiente peso alla nascita con sviluppo osseo e dentale insufficiente bullcomplicazioni della gestazione quali parto pretermine distocia del travaglio
bulldifficoltagrave nellallattamento lalimentazione ipercalorica puograve d altro canto determinare
bullgestosi bulldisturbi digestivi bulldiabete gestazionale bullmacrosomia fetale con possibile conseguente distocia da sproporzione fetopelvica
EQUILIBRIO GLICEMICO = IG CG
durante tutta la gravidanza egrave importante
mantenere lequilibrio glicemico
costante ed adeguato apporto proteico
adeguata introduzione di liquidi
adeguato apporto di vitamine e sali
le modificazioni in senso diabetogeno del
metabolismo degli zuccheri in senso
chetogenico del metabolismo dei grassi e la
necessita di incrementare la quota proteica
giornaliera consigliano
bull5 pasti al di
bullcarboidrati ad ogni pasto
bullolio vergine doliva
bullsemi
bullesclusione degli zuccheri raffinati
bullproteine ad ogni pasto
esempio di colazione
frullato di
2 cucchiai di yogurth
2 cucchiai di olio di lino
12 banana
12 succo di limone
1 cucchiaio di riso integrale
1 cucchiaio di miele
2 cucchiaini di semi oleosi
Lalimentazione deve apportare una adeguata
quantitagrave di colesterolo utile nella produzione
attraverso il pregnenolone del progesterone uova
uova di pesce acciughe crostacei e molluschi
alimenti ricchi di omega 3 pesce azzurro almeno tre
volte alla settimana
Lapporto di folati indispensabili per la prevenzione
in questa epoca delle patologie del tubo neurale puograve
essere assicurato con le verdure e la frutta (kiwi
fragole arance) il Calcio puograve essere introdotto con
semi di sesamo e formaggio caprino
I TRIMESTRE
Modificazioni materne embriogenesi e placentazione
II TRIMESTRE
IN QUESTO PERIODO egrave MOLTO IMPORTANTE ATTIVARE LA
TIROIDE ATTRAVERSO LrsquoASSUNZIONE DI SELENIO
Componente delle selenoproteine ha effetti immunomodulatori e
svolge un ruolo chiave nel metabolismo degli ormoni tiroidei nella
famiglia delle deiodinasi Il suo deficit egrave responsabile del cretinismo
edematoso endemico
Fonti naturali di selenio sono le frattaglie pesce molluschi carne
latte lievito di birra pasta riso funghi noci
La seleneproteina detta GPx ( glutatione perossidasi) egrave un potente
regolatore della sintesi degli ormoni tiroidei e protegge dal danno
ossidativo
II TRIMESTRE
Tra le deiodinasi la D3 egrave particolarmente localizzate nelle cellule del
cervello fegato fetale placenta e pelle Protegge il concepito dalla
eccessiva esposizione agli ormoni tiroidei
Lipotiroidismo subclinico si associa a distacco di placenta parto
pretermine e aborto (Casey 2005) e al rischio di sviluppo nel post
partum di tiroidite autoimmune e di sviluppo cognitivo subottimale nella
prole (Papi e coll 2007) Dose giornaliera selenio egrave 60 microgrammi
Le richieste fetali impongono di introdurre con la dieta anche agenti
antiossidanti vit C vit E betacarotene
III TRIMESTRE
In questo periodo della gestazione il notevole
accrescimento ponderale fetale e le variazione in senso
procoagulatorio dei parametri ematici consigliano di
ridurre i carboidrati di aumentare le proteine di origine
vegetale e di favorire la funzione renale
Si evitino funghi e asparagi e si limitino ananas kiwi
salvia per la loro azione sulla coagulazione
NAUSEA ED EMESI GRAVIDICA
Dobbiamo ridurre i carboidrati evitare dolci e liquidi limitare le proteine
Nella dieta sono utili
verdure amare
limone
zenzero
aceto
Per stabilizzare lambiente gastrico bisogna alcalinizzarlo
Migliorare la funzione epatica evitando fritti limitando gli ortaggi gialli
(carotenoidi) e le crucifere (per lo zolfo)
dare carboidrati facili senza glutine
coleretici e colagoghi tipo zucchine marinate con aglio menta e aceto
fragole kiwi papaya (aiuta a digerire ed egrave drenante ricca di K) e avocado
LA MINACCIA DABORTO
Dobbiamo fornire lorganismo di
Magnesio fonti sono germe di grano fagioli ceci cereali integrali riso
avena banane kiwi uva mais
Antiossidanti antinfiammatori ottenere lequilibrio glicemico omega 3 e
fibre Possiamo consigliare olio di semi di lino noci e frutta fresca uova
tonno e pesce spada Per lacido lipoico patate broccoli spinaci fegato
cuore carni rosse
ALIMENTAZIONE ED AMNIOCENTESI
evitare le contrazioni con alimenti ricchi di Mg e K riso patate
fagiolini zucchine banane
favorire la funzione epatica in senso procoagulante uova fegato
pomodori fragole peperonicarote zucca soiabrassicacee e
formaggio fuso
evitare le infezioni aglio zenzero cipolla prezzemolo chiodi di
garofano limone per la loro funzione immunostimolante
PREVENZIONE DELLE INFEZIONI GRAVIDICHE
Ligiene degli alimenti egrave fondamentale per la
prevenzione della toxoplasmosi
Bisogna mantenere un buon equilibrio glicemico e
seguire una dieta ricca di fibre e di antiossidanti quali
cipolla olio di oliva curcuma mirtilli riso integrale
frutta secca zenzero e aglio
IMPORTANZA DELLA COTTURA DEI
CIBI PER OTTENERE IL MIGLIOR
RISULTATO SOTTO IL PROFILO DELLA
DIGERIBILITA E DELLA QUALITA
PREVENZIONE DELLA GESTOSI
Consigliabile introdurre con la dieta pochi zuccheri molte
proteine (molto pesce e latte poche carni rosse) alimenti a
basso indice glicemico e verdure ricche di acqua come
fragole patate cipolle e cicoria
Per diminuire le resistenze vascolari e i grassi circolanti egrave
utile assumere prezzemolo ananas finocchio cipolla melone
aglio e fragole
Per migliorare la funzione cuore-reni sono utili legumi frutta
secca miele cereali integrali rucola vongole e uova
Iodine deficiency in pregnant women living in the South East
of the UK the influence of diet and nutritional supplements
on iodine status Bath SC Walter A Taylor A Wright J Rayman MP Author information
Iodine is a key component of the thyroid hormones which are crucial for brain development
Adequate intake of iodine in pregnancy is important as in utero deficiency may have lifelong
consequences for the offspring Data on the iodine status of UK pregnant women are sparse
and there are no such data for pregnant women in the South East of the UK A total of 100
pregnant women were recruited to a cross-sectional study carried out at the Royal Surrey
County Hospital Guildford at their first-trimester visit for an ultrasound scan The participants
provided a spot-urine sample (for the measurement of urinary iodine concentration (UIC) and
creatinine concentration) and 24 h iodine excretion was estimated from the urinary
iodinecreatinine ratio Women completed a general questionnaire and a FFQ The median UIC
(85middot3 μgl) indicated that the group was iodine deficient by World Health Organisation criteria
The median values of the iodinecreatinine ratio (122middot9 μgg) and of the estimated 24 h iodine
excretion (151middot2 μgd) were also suggestive of iodine deficiency UIC was significantly higher in
women taking an iodine-containing prenatal supplement (n 42) than in those not taking such a
supplement (Plt 0middot001) In the adjusted analyses milk intake maternal age and iodine-
containing prenatal supplement use were positively associated with the estimated 24 h urinary
iodine excretion Our finding of iodine deficiency in these women gives cause for concern We
suggest that women of childbearing age and pregnant women should be given advice on how to
improve their iodine status through dietary means A national survey of iodine status in UK
pregnant women is required
Maternal and in utero determinants of type 2 diabetes risk in the
young Bruce KD Abstract
The global prevalence of diabetes mellitus has reached epidemic proportions In 2010 it was estimated
that 64 of the adult population (285 million) have diabetes In recent years the incidence of type 2
diabetes (T2D) a condition traditionally associated with aging has been steadily increasing among
younger individuals It is now a well-established notion that the early-life period is a critical window of
development and that influences during this period can developmentally prime the metabolic status of the
adult This review discusses the role of maternal and in utero influences on the developmental priming of
T2D risk Both human epidemiological studies and experimental animal models are beginning to
demonstrate that early dietary challenges can accelerate the onset of age-associated metabolic
disturbances including insulin resistance T2D obesity hypertension and cardiovascular disease These
findings show that poor maternal nutrition can prime a prediabetes phenotype often manifest as insulin
resistance by very early stages of life Thus the maternal diet is a critical determinant of premature T2D
risk While the mechanisms that link early nutrition to age-associated metabolic decline are currently
unclear preliminary findings suggest perturbations in a number of processes involved in cellular aging
such as changes in longevity-associated Sirtuin activity epigenetic regulation of key metabolic genes and
mitochondrial dysfunction Preliminary studies show that pharmacological interventions in utero and dietary
supplementation in early postnatal life may alleviate insulin resistance and reduce T2D risk However
further studies are warranted to fully understand the relationship between the early environment and long-
term effects on metabolism Such mechanistic insights will facilitate strategic interventions that prevent
accelerated metabolic decline and the premature onset of T2D in the current and future generations
Counteracting oxidative stress in pregnancy through modulation
of maternal micronutrients and omega-3 fatty acids DSouza V1 Chavan-Gautam P Joshi S Abstract
During pregnancy oxidative stress has been implicated in the pathophysiology of
preeclampsia and preterm birth leading to poor birth outcome Hyperhomocysteinemia
caused as a consequence of altered micronutrients like folic acid and vitamin B12 is
associated with increased production of reactive oxygen species that generate oxidative
stress These micronutrients are important determinants of methyl donor s-adenosyl
methionine while phospholipids are important methyl acceptors in the one-carbon
metabolic cycle A series of our studies in women during pregnancy have demonstrated
altered levels of these micronutrients and the negative association of docosahexaenoic
acid with homocysteine Various strategies to counteract oxidative stress
during pregnancy such as antioxidant therapy have been examined and found to be
inconsistent In this review we focus on the role of oxidative stress in pregnancy and
discuss the possibility of ameliorating it through modulation of maternal micronutrients
and omega 3 fatty acids especially docosahexaenoic acid We propose for the first time
that manipulation of one-carbon metabolism by maternal diet could be a potential
mechanism to counteract oxidative stress through homocysteine lowering effects and
help in reducing the risk for adverse pregnancyoutcomes
The influence of a low glycemic index dietary intervention on maternal
dietary intake glycemic index and gestational weight gain
during pregnancy a randomized controlled trial McGowan CA Walsh JM Byrne J Curran S McAuliffe FM1 Abstract
BACKGROUND Maternal diet is known to impact pregnancy outcome Following a low glycemic index (GI) diet during pregnancy has been shown
to improve maternal glycemia and reduce infant birthweight and may be associated with a higher fibre intake We assessed the
impact of a low GI dietary intervention on maternal GI nutritional intake and gestational weight gain (GWG) during pregnancy Compliance and acceptability of the low GIdiet was also examined METHOD Eight hundred women were randomised in early pregnancy to receive low GI and healthy eating dietary advice or to receive
standard maternity care The intervention group received dietary advice at a group education session before 22 weeks gestation
All women completed a 3 day food diary during each trimester of pregnancy Two hundred and thirty five women from the intervention arm and 285 women from the control arm returned complete 3x3d FDs and were included in the present analysis RESULTS Maternal GI was significantly reduced in the intervention group at trimester 2 and 3 The numbers of women within the lowest
quartile of GI increased from 37 in trimester 1 to 52 in trimester 3 (Pthinspltthinsp0001) among the intervention group The intervention
group had significantly lower energy intake (Pthinspltthinsp005) higher protein ( TE) (Pthinspltthinsp001) and higher dietary fibre intake (Pthinspltthinsp001)
post intervention Consumption of food groups with known high GI values were significantly reduced among the intervention group Women in the intervention low GI group were less likely to exceed the Institute of Medicines GWG goals CONCLUSION A dietary intervention in early pregnancy had a positive influence on maternal GI food and nutrient intakes and GWG Following
a low GI diet may be particularly beneficial for women at risk of exceeding the GWG goals for pregnancy
laumento del peso corporeo durante la
prima metagrave della gravidanza egrave dovuto
allaumento dei tessuti di riserva mentre
successivamente egrave rappresentato dal
prodotto del concepimento
Varia comunque a seconda delletagrave della
paritagrave e della costituzione corporea
In gravidanza crsquoegrave un aumento di richiesta di
energia necessaria per la sintesi dei nuovi
tessuti sia del prodotto del concepimento
che degli organi materni (utero mammelle
grasso) per lattivitagrave metabolica della unitagrave
feto placentare e per il normale lavoro della
gestante
La richiesta giornaliera di calorie egrave di circa
2100 2200 e 2300 kcal al di nei trimestri 1
2 e 3deg
Componenti che determinano lrsquoaumento i peso in gravidanza
Il regime dietetico deve considerare le condizioni nutrizionali
al momento del concepimento e il bisogno alimentare attuale
e remoto
Lalimentazione inadeguata si ripercuote negativamente sullevoluzione della gravidanza e sullaccrescimento fetale Una riduzione dellapporto quantitativo ma ancor piugrave di quello qualitativo puograve esitare in
bullneonato di insufficiente peso alla nascita con sviluppo osseo e dentale insufficiente bullcomplicazioni della gestazione quali parto pretermine distocia del travaglio
bulldifficoltagrave nellallattamento lalimentazione ipercalorica puograve d altro canto determinare
bullgestosi bulldisturbi digestivi bulldiabete gestazionale bullmacrosomia fetale con possibile conseguente distocia da sproporzione fetopelvica
EQUILIBRIO GLICEMICO = IG CG
durante tutta la gravidanza egrave importante
mantenere lequilibrio glicemico
costante ed adeguato apporto proteico
adeguata introduzione di liquidi
adeguato apporto di vitamine e sali
le modificazioni in senso diabetogeno del
metabolismo degli zuccheri in senso
chetogenico del metabolismo dei grassi e la
necessita di incrementare la quota proteica
giornaliera consigliano
bull5 pasti al di
bullcarboidrati ad ogni pasto
bullolio vergine doliva
bullsemi
bullesclusione degli zuccheri raffinati
bullproteine ad ogni pasto
esempio di colazione
frullato di
2 cucchiai di yogurth
2 cucchiai di olio di lino
12 banana
12 succo di limone
1 cucchiaio di riso integrale
1 cucchiaio di miele
2 cucchiaini di semi oleosi
Lalimentazione deve apportare una adeguata
quantitagrave di colesterolo utile nella produzione
attraverso il pregnenolone del progesterone uova
uova di pesce acciughe crostacei e molluschi
alimenti ricchi di omega 3 pesce azzurro almeno tre
volte alla settimana
Lapporto di folati indispensabili per la prevenzione
in questa epoca delle patologie del tubo neurale puograve
essere assicurato con le verdure e la frutta (kiwi
fragole arance) il Calcio puograve essere introdotto con
semi di sesamo e formaggio caprino
I TRIMESTRE
Modificazioni materne embriogenesi e placentazione
II TRIMESTRE
IN QUESTO PERIODO egrave MOLTO IMPORTANTE ATTIVARE LA
TIROIDE ATTRAVERSO LrsquoASSUNZIONE DI SELENIO
Componente delle selenoproteine ha effetti immunomodulatori e
svolge un ruolo chiave nel metabolismo degli ormoni tiroidei nella
famiglia delle deiodinasi Il suo deficit egrave responsabile del cretinismo
edematoso endemico
Fonti naturali di selenio sono le frattaglie pesce molluschi carne
latte lievito di birra pasta riso funghi noci
La seleneproteina detta GPx ( glutatione perossidasi) egrave un potente
regolatore della sintesi degli ormoni tiroidei e protegge dal danno
ossidativo
II TRIMESTRE
Tra le deiodinasi la D3 egrave particolarmente localizzate nelle cellule del
cervello fegato fetale placenta e pelle Protegge il concepito dalla
eccessiva esposizione agli ormoni tiroidei
Lipotiroidismo subclinico si associa a distacco di placenta parto
pretermine e aborto (Casey 2005) e al rischio di sviluppo nel post
partum di tiroidite autoimmune e di sviluppo cognitivo subottimale nella
prole (Papi e coll 2007) Dose giornaliera selenio egrave 60 microgrammi
Le richieste fetali impongono di introdurre con la dieta anche agenti
antiossidanti vit C vit E betacarotene
III TRIMESTRE
In questo periodo della gestazione il notevole
accrescimento ponderale fetale e le variazione in senso
procoagulatorio dei parametri ematici consigliano di
ridurre i carboidrati di aumentare le proteine di origine
vegetale e di favorire la funzione renale
Si evitino funghi e asparagi e si limitino ananas kiwi
salvia per la loro azione sulla coagulazione
NAUSEA ED EMESI GRAVIDICA
Dobbiamo ridurre i carboidrati evitare dolci e liquidi limitare le proteine
Nella dieta sono utili
verdure amare
limone
zenzero
aceto
Per stabilizzare lambiente gastrico bisogna alcalinizzarlo
Migliorare la funzione epatica evitando fritti limitando gli ortaggi gialli
(carotenoidi) e le crucifere (per lo zolfo)
dare carboidrati facili senza glutine
coleretici e colagoghi tipo zucchine marinate con aglio menta e aceto
fragole kiwi papaya (aiuta a digerire ed egrave drenante ricca di K) e avocado
LA MINACCIA DABORTO
Dobbiamo fornire lorganismo di
Magnesio fonti sono germe di grano fagioli ceci cereali integrali riso
avena banane kiwi uva mais
Antiossidanti antinfiammatori ottenere lequilibrio glicemico omega 3 e
fibre Possiamo consigliare olio di semi di lino noci e frutta fresca uova
tonno e pesce spada Per lacido lipoico patate broccoli spinaci fegato
cuore carni rosse
ALIMENTAZIONE ED AMNIOCENTESI
evitare le contrazioni con alimenti ricchi di Mg e K riso patate
fagiolini zucchine banane
favorire la funzione epatica in senso procoagulante uova fegato
pomodori fragole peperonicarote zucca soiabrassicacee e
formaggio fuso
evitare le infezioni aglio zenzero cipolla prezzemolo chiodi di
garofano limone per la loro funzione immunostimolante
PREVENZIONE DELLE INFEZIONI GRAVIDICHE
Ligiene degli alimenti egrave fondamentale per la
prevenzione della toxoplasmosi
Bisogna mantenere un buon equilibrio glicemico e
seguire una dieta ricca di fibre e di antiossidanti quali
cipolla olio di oliva curcuma mirtilli riso integrale
frutta secca zenzero e aglio
IMPORTANZA DELLA COTTURA DEI
CIBI PER OTTENERE IL MIGLIOR
RISULTATO SOTTO IL PROFILO DELLA
DIGERIBILITA E DELLA QUALITA
PREVENZIONE DELLA GESTOSI
Consigliabile introdurre con la dieta pochi zuccheri molte
proteine (molto pesce e latte poche carni rosse) alimenti a
basso indice glicemico e verdure ricche di acqua come
fragole patate cipolle e cicoria
Per diminuire le resistenze vascolari e i grassi circolanti egrave
utile assumere prezzemolo ananas finocchio cipolla melone
aglio e fragole
Per migliorare la funzione cuore-reni sono utili legumi frutta
secca miele cereali integrali rucola vongole e uova
Iodine deficiency in pregnant women living in the South East
of the UK the influence of diet and nutritional supplements
on iodine status Bath SC Walter A Taylor A Wright J Rayman MP Author information
Iodine is a key component of the thyroid hormones which are crucial for brain development
Adequate intake of iodine in pregnancy is important as in utero deficiency may have lifelong
consequences for the offspring Data on the iodine status of UK pregnant women are sparse
and there are no such data for pregnant women in the South East of the UK A total of 100
pregnant women were recruited to a cross-sectional study carried out at the Royal Surrey
County Hospital Guildford at their first-trimester visit for an ultrasound scan The participants
provided a spot-urine sample (for the measurement of urinary iodine concentration (UIC) and
creatinine concentration) and 24 h iodine excretion was estimated from the urinary
iodinecreatinine ratio Women completed a general questionnaire and a FFQ The median UIC
(85middot3 μgl) indicated that the group was iodine deficient by World Health Organisation criteria
The median values of the iodinecreatinine ratio (122middot9 μgg) and of the estimated 24 h iodine
excretion (151middot2 μgd) were also suggestive of iodine deficiency UIC was significantly higher in
women taking an iodine-containing prenatal supplement (n 42) than in those not taking such a
supplement (Plt 0middot001) In the adjusted analyses milk intake maternal age and iodine-
containing prenatal supplement use were positively associated with the estimated 24 h urinary
iodine excretion Our finding of iodine deficiency in these women gives cause for concern We
suggest that women of childbearing age and pregnant women should be given advice on how to
improve their iodine status through dietary means A national survey of iodine status in UK
pregnant women is required
Maternal and in utero determinants of type 2 diabetes risk in the
young Bruce KD Abstract
The global prevalence of diabetes mellitus has reached epidemic proportions In 2010 it was estimated
that 64 of the adult population (285 million) have diabetes In recent years the incidence of type 2
diabetes (T2D) a condition traditionally associated with aging has been steadily increasing among
younger individuals It is now a well-established notion that the early-life period is a critical window of
development and that influences during this period can developmentally prime the metabolic status of the
adult This review discusses the role of maternal and in utero influences on the developmental priming of
T2D risk Both human epidemiological studies and experimental animal models are beginning to
demonstrate that early dietary challenges can accelerate the onset of age-associated metabolic
disturbances including insulin resistance T2D obesity hypertension and cardiovascular disease These
findings show that poor maternal nutrition can prime a prediabetes phenotype often manifest as insulin
resistance by very early stages of life Thus the maternal diet is a critical determinant of premature T2D
risk While the mechanisms that link early nutrition to age-associated metabolic decline are currently
unclear preliminary findings suggest perturbations in a number of processes involved in cellular aging
such as changes in longevity-associated Sirtuin activity epigenetic regulation of key metabolic genes and
mitochondrial dysfunction Preliminary studies show that pharmacological interventions in utero and dietary
supplementation in early postnatal life may alleviate insulin resistance and reduce T2D risk However
further studies are warranted to fully understand the relationship between the early environment and long-
term effects on metabolism Such mechanistic insights will facilitate strategic interventions that prevent
accelerated metabolic decline and the premature onset of T2D in the current and future generations
Counteracting oxidative stress in pregnancy through modulation
of maternal micronutrients and omega-3 fatty acids DSouza V1 Chavan-Gautam P Joshi S Abstract
During pregnancy oxidative stress has been implicated in the pathophysiology of
preeclampsia and preterm birth leading to poor birth outcome Hyperhomocysteinemia
caused as a consequence of altered micronutrients like folic acid and vitamin B12 is
associated with increased production of reactive oxygen species that generate oxidative
stress These micronutrients are important determinants of methyl donor s-adenosyl
methionine while phospholipids are important methyl acceptors in the one-carbon
metabolic cycle A series of our studies in women during pregnancy have demonstrated
altered levels of these micronutrients and the negative association of docosahexaenoic
acid with homocysteine Various strategies to counteract oxidative stress
during pregnancy such as antioxidant therapy have been examined and found to be
inconsistent In this review we focus on the role of oxidative stress in pregnancy and
discuss the possibility of ameliorating it through modulation of maternal micronutrients
and omega 3 fatty acids especially docosahexaenoic acid We propose for the first time
that manipulation of one-carbon metabolism by maternal diet could be a potential
mechanism to counteract oxidative stress through homocysteine lowering effects and
help in reducing the risk for adverse pregnancyoutcomes
The influence of a low glycemic index dietary intervention on maternal
dietary intake glycemic index and gestational weight gain
during pregnancy a randomized controlled trial McGowan CA Walsh JM Byrne J Curran S McAuliffe FM1 Abstract
BACKGROUND Maternal diet is known to impact pregnancy outcome Following a low glycemic index (GI) diet during pregnancy has been shown
to improve maternal glycemia and reduce infant birthweight and may be associated with a higher fibre intake We assessed the
impact of a low GI dietary intervention on maternal GI nutritional intake and gestational weight gain (GWG) during pregnancy Compliance and acceptability of the low GIdiet was also examined METHOD Eight hundred women were randomised in early pregnancy to receive low GI and healthy eating dietary advice or to receive
standard maternity care The intervention group received dietary advice at a group education session before 22 weeks gestation
All women completed a 3 day food diary during each trimester of pregnancy Two hundred and thirty five women from the intervention arm and 285 women from the control arm returned complete 3x3d FDs and were included in the present analysis RESULTS Maternal GI was significantly reduced in the intervention group at trimester 2 and 3 The numbers of women within the lowest
quartile of GI increased from 37 in trimester 1 to 52 in trimester 3 (Pthinspltthinsp0001) among the intervention group The intervention
group had significantly lower energy intake (Pthinspltthinsp005) higher protein ( TE) (Pthinspltthinsp001) and higher dietary fibre intake (Pthinspltthinsp001)
post intervention Consumption of food groups with known high GI values were significantly reduced among the intervention group Women in the intervention low GI group were less likely to exceed the Institute of Medicines GWG goals CONCLUSION A dietary intervention in early pregnancy had a positive influence on maternal GI food and nutrient intakes and GWG Following
a low GI diet may be particularly beneficial for women at risk of exceeding the GWG goals for pregnancy
In gravidanza crsquoegrave un aumento di richiesta di
energia necessaria per la sintesi dei nuovi
tessuti sia del prodotto del concepimento
che degli organi materni (utero mammelle
grasso) per lattivitagrave metabolica della unitagrave
feto placentare e per il normale lavoro della
gestante
La richiesta giornaliera di calorie egrave di circa
2100 2200 e 2300 kcal al di nei trimestri 1
2 e 3deg
Componenti che determinano lrsquoaumento i peso in gravidanza
Il regime dietetico deve considerare le condizioni nutrizionali
al momento del concepimento e il bisogno alimentare attuale
e remoto
Lalimentazione inadeguata si ripercuote negativamente sullevoluzione della gravidanza e sullaccrescimento fetale Una riduzione dellapporto quantitativo ma ancor piugrave di quello qualitativo puograve esitare in
bullneonato di insufficiente peso alla nascita con sviluppo osseo e dentale insufficiente bullcomplicazioni della gestazione quali parto pretermine distocia del travaglio
bulldifficoltagrave nellallattamento lalimentazione ipercalorica puograve d altro canto determinare
bullgestosi bulldisturbi digestivi bulldiabete gestazionale bullmacrosomia fetale con possibile conseguente distocia da sproporzione fetopelvica
EQUILIBRIO GLICEMICO = IG CG
durante tutta la gravidanza egrave importante
mantenere lequilibrio glicemico
costante ed adeguato apporto proteico
adeguata introduzione di liquidi
adeguato apporto di vitamine e sali
le modificazioni in senso diabetogeno del
metabolismo degli zuccheri in senso
chetogenico del metabolismo dei grassi e la
necessita di incrementare la quota proteica
giornaliera consigliano
bull5 pasti al di
bullcarboidrati ad ogni pasto
bullolio vergine doliva
bullsemi
bullesclusione degli zuccheri raffinati
bullproteine ad ogni pasto
esempio di colazione
frullato di
2 cucchiai di yogurth
2 cucchiai di olio di lino
12 banana
12 succo di limone
1 cucchiaio di riso integrale
1 cucchiaio di miele
2 cucchiaini di semi oleosi
Lalimentazione deve apportare una adeguata
quantitagrave di colesterolo utile nella produzione
attraverso il pregnenolone del progesterone uova
uova di pesce acciughe crostacei e molluschi
alimenti ricchi di omega 3 pesce azzurro almeno tre
volte alla settimana
Lapporto di folati indispensabili per la prevenzione
in questa epoca delle patologie del tubo neurale puograve
essere assicurato con le verdure e la frutta (kiwi
fragole arance) il Calcio puograve essere introdotto con
semi di sesamo e formaggio caprino
I TRIMESTRE
Modificazioni materne embriogenesi e placentazione
II TRIMESTRE
IN QUESTO PERIODO egrave MOLTO IMPORTANTE ATTIVARE LA
TIROIDE ATTRAVERSO LrsquoASSUNZIONE DI SELENIO
Componente delle selenoproteine ha effetti immunomodulatori e
svolge un ruolo chiave nel metabolismo degli ormoni tiroidei nella
famiglia delle deiodinasi Il suo deficit egrave responsabile del cretinismo
edematoso endemico
Fonti naturali di selenio sono le frattaglie pesce molluschi carne
latte lievito di birra pasta riso funghi noci
La seleneproteina detta GPx ( glutatione perossidasi) egrave un potente
regolatore della sintesi degli ormoni tiroidei e protegge dal danno
ossidativo
II TRIMESTRE
Tra le deiodinasi la D3 egrave particolarmente localizzate nelle cellule del
cervello fegato fetale placenta e pelle Protegge il concepito dalla
eccessiva esposizione agli ormoni tiroidei
Lipotiroidismo subclinico si associa a distacco di placenta parto
pretermine e aborto (Casey 2005) e al rischio di sviluppo nel post
partum di tiroidite autoimmune e di sviluppo cognitivo subottimale nella
prole (Papi e coll 2007) Dose giornaliera selenio egrave 60 microgrammi
Le richieste fetali impongono di introdurre con la dieta anche agenti
antiossidanti vit C vit E betacarotene
III TRIMESTRE
In questo periodo della gestazione il notevole
accrescimento ponderale fetale e le variazione in senso
procoagulatorio dei parametri ematici consigliano di
ridurre i carboidrati di aumentare le proteine di origine
vegetale e di favorire la funzione renale
Si evitino funghi e asparagi e si limitino ananas kiwi
salvia per la loro azione sulla coagulazione
NAUSEA ED EMESI GRAVIDICA
Dobbiamo ridurre i carboidrati evitare dolci e liquidi limitare le proteine
Nella dieta sono utili
verdure amare
limone
zenzero
aceto
Per stabilizzare lambiente gastrico bisogna alcalinizzarlo
Migliorare la funzione epatica evitando fritti limitando gli ortaggi gialli
(carotenoidi) e le crucifere (per lo zolfo)
dare carboidrati facili senza glutine
coleretici e colagoghi tipo zucchine marinate con aglio menta e aceto
fragole kiwi papaya (aiuta a digerire ed egrave drenante ricca di K) e avocado
LA MINACCIA DABORTO
Dobbiamo fornire lorganismo di
Magnesio fonti sono germe di grano fagioli ceci cereali integrali riso
avena banane kiwi uva mais
Antiossidanti antinfiammatori ottenere lequilibrio glicemico omega 3 e
fibre Possiamo consigliare olio di semi di lino noci e frutta fresca uova
tonno e pesce spada Per lacido lipoico patate broccoli spinaci fegato
cuore carni rosse
ALIMENTAZIONE ED AMNIOCENTESI
evitare le contrazioni con alimenti ricchi di Mg e K riso patate
fagiolini zucchine banane
favorire la funzione epatica in senso procoagulante uova fegato
pomodori fragole peperonicarote zucca soiabrassicacee e
formaggio fuso
evitare le infezioni aglio zenzero cipolla prezzemolo chiodi di
garofano limone per la loro funzione immunostimolante
PREVENZIONE DELLE INFEZIONI GRAVIDICHE
Ligiene degli alimenti egrave fondamentale per la
prevenzione della toxoplasmosi
Bisogna mantenere un buon equilibrio glicemico e
seguire una dieta ricca di fibre e di antiossidanti quali
cipolla olio di oliva curcuma mirtilli riso integrale
frutta secca zenzero e aglio
IMPORTANZA DELLA COTTURA DEI
CIBI PER OTTENERE IL MIGLIOR
RISULTATO SOTTO IL PROFILO DELLA
DIGERIBILITA E DELLA QUALITA
PREVENZIONE DELLA GESTOSI
Consigliabile introdurre con la dieta pochi zuccheri molte
proteine (molto pesce e latte poche carni rosse) alimenti a
basso indice glicemico e verdure ricche di acqua come
fragole patate cipolle e cicoria
Per diminuire le resistenze vascolari e i grassi circolanti egrave
utile assumere prezzemolo ananas finocchio cipolla melone
aglio e fragole
Per migliorare la funzione cuore-reni sono utili legumi frutta
secca miele cereali integrali rucola vongole e uova
Iodine deficiency in pregnant women living in the South East
of the UK the influence of diet and nutritional supplements
on iodine status Bath SC Walter A Taylor A Wright J Rayman MP Author information
Iodine is a key component of the thyroid hormones which are crucial for brain development
Adequate intake of iodine in pregnancy is important as in utero deficiency may have lifelong
consequences for the offspring Data on the iodine status of UK pregnant women are sparse
and there are no such data for pregnant women in the South East of the UK A total of 100
pregnant women were recruited to a cross-sectional study carried out at the Royal Surrey
County Hospital Guildford at their first-trimester visit for an ultrasound scan The participants
provided a spot-urine sample (for the measurement of urinary iodine concentration (UIC) and
creatinine concentration) and 24 h iodine excretion was estimated from the urinary
iodinecreatinine ratio Women completed a general questionnaire and a FFQ The median UIC
(85middot3 μgl) indicated that the group was iodine deficient by World Health Organisation criteria
The median values of the iodinecreatinine ratio (122middot9 μgg) and of the estimated 24 h iodine
excretion (151middot2 μgd) were also suggestive of iodine deficiency UIC was significantly higher in
women taking an iodine-containing prenatal supplement (n 42) than in those not taking such a
supplement (Plt 0middot001) In the adjusted analyses milk intake maternal age and iodine-
containing prenatal supplement use were positively associated with the estimated 24 h urinary
iodine excretion Our finding of iodine deficiency in these women gives cause for concern We
suggest that women of childbearing age and pregnant women should be given advice on how to
improve their iodine status through dietary means A national survey of iodine status in UK
pregnant women is required
Maternal and in utero determinants of type 2 diabetes risk in the
young Bruce KD Abstract
The global prevalence of diabetes mellitus has reached epidemic proportions In 2010 it was estimated
that 64 of the adult population (285 million) have diabetes In recent years the incidence of type 2
diabetes (T2D) a condition traditionally associated with aging has been steadily increasing among
younger individuals It is now a well-established notion that the early-life period is a critical window of
development and that influences during this period can developmentally prime the metabolic status of the
adult This review discusses the role of maternal and in utero influences on the developmental priming of
T2D risk Both human epidemiological studies and experimental animal models are beginning to
demonstrate that early dietary challenges can accelerate the onset of age-associated metabolic
disturbances including insulin resistance T2D obesity hypertension and cardiovascular disease These
findings show that poor maternal nutrition can prime a prediabetes phenotype often manifest as insulin
resistance by very early stages of life Thus the maternal diet is a critical determinant of premature T2D
risk While the mechanisms that link early nutrition to age-associated metabolic decline are currently
unclear preliminary findings suggest perturbations in a number of processes involved in cellular aging
such as changes in longevity-associated Sirtuin activity epigenetic regulation of key metabolic genes and
mitochondrial dysfunction Preliminary studies show that pharmacological interventions in utero and dietary
supplementation in early postnatal life may alleviate insulin resistance and reduce T2D risk However
further studies are warranted to fully understand the relationship between the early environment and long-
term effects on metabolism Such mechanistic insights will facilitate strategic interventions that prevent
accelerated metabolic decline and the premature onset of T2D in the current and future generations
Counteracting oxidative stress in pregnancy through modulation
of maternal micronutrients and omega-3 fatty acids DSouza V1 Chavan-Gautam P Joshi S Abstract
During pregnancy oxidative stress has been implicated in the pathophysiology of
preeclampsia and preterm birth leading to poor birth outcome Hyperhomocysteinemia
caused as a consequence of altered micronutrients like folic acid and vitamin B12 is
associated with increased production of reactive oxygen species that generate oxidative
stress These micronutrients are important determinants of methyl donor s-adenosyl
methionine while phospholipids are important methyl acceptors in the one-carbon
metabolic cycle A series of our studies in women during pregnancy have demonstrated
altered levels of these micronutrients and the negative association of docosahexaenoic
acid with homocysteine Various strategies to counteract oxidative stress
during pregnancy such as antioxidant therapy have been examined and found to be
inconsistent In this review we focus on the role of oxidative stress in pregnancy and
discuss the possibility of ameliorating it through modulation of maternal micronutrients
and omega 3 fatty acids especially docosahexaenoic acid We propose for the first time
that manipulation of one-carbon metabolism by maternal diet could be a potential
mechanism to counteract oxidative stress through homocysteine lowering effects and
help in reducing the risk for adverse pregnancyoutcomes
The influence of a low glycemic index dietary intervention on maternal
dietary intake glycemic index and gestational weight gain
during pregnancy a randomized controlled trial McGowan CA Walsh JM Byrne J Curran S McAuliffe FM1 Abstract
BACKGROUND Maternal diet is known to impact pregnancy outcome Following a low glycemic index (GI) diet during pregnancy has been shown
to improve maternal glycemia and reduce infant birthweight and may be associated with a higher fibre intake We assessed the
impact of a low GI dietary intervention on maternal GI nutritional intake and gestational weight gain (GWG) during pregnancy Compliance and acceptability of the low GIdiet was also examined METHOD Eight hundred women were randomised in early pregnancy to receive low GI and healthy eating dietary advice or to receive
standard maternity care The intervention group received dietary advice at a group education session before 22 weeks gestation
All women completed a 3 day food diary during each trimester of pregnancy Two hundred and thirty five women from the intervention arm and 285 women from the control arm returned complete 3x3d FDs and were included in the present analysis RESULTS Maternal GI was significantly reduced in the intervention group at trimester 2 and 3 The numbers of women within the lowest
quartile of GI increased from 37 in trimester 1 to 52 in trimester 3 (Pthinspltthinsp0001) among the intervention group The intervention
group had significantly lower energy intake (Pthinspltthinsp005) higher protein ( TE) (Pthinspltthinsp001) and higher dietary fibre intake (Pthinspltthinsp001)
post intervention Consumption of food groups with known high GI values were significantly reduced among the intervention group Women in the intervention low GI group were less likely to exceed the Institute of Medicines GWG goals CONCLUSION A dietary intervention in early pregnancy had a positive influence on maternal GI food and nutrient intakes and GWG Following
a low GI diet may be particularly beneficial for women at risk of exceeding the GWG goals for pregnancy

Componenti che determinano lrsquoaumento i peso in gravidanza
Il regime dietetico deve considerare le condizioni nutrizionali
al momento del concepimento e il bisogno alimentare attuale
e remoto
Lalimentazione inadeguata si ripercuote negativamente sullevoluzione della gravidanza e sullaccrescimento fetale Una riduzione dellapporto quantitativo ma ancor piugrave di quello qualitativo puograve esitare in
bullneonato di insufficiente peso alla nascita con sviluppo osseo e dentale insufficiente bullcomplicazioni della gestazione quali parto pretermine distocia del travaglio
bulldifficoltagrave nellallattamento lalimentazione ipercalorica puograve d altro canto determinare
bullgestosi bulldisturbi digestivi bulldiabete gestazionale bullmacrosomia fetale con possibile conseguente distocia da sproporzione fetopelvica
EQUILIBRIO GLICEMICO = IG CG
durante tutta la gravidanza egrave importante
mantenere lequilibrio glicemico
costante ed adeguato apporto proteico
adeguata introduzione di liquidi
adeguato apporto di vitamine e sali
le modificazioni in senso diabetogeno del
metabolismo degli zuccheri in senso
chetogenico del metabolismo dei grassi e la
necessita di incrementare la quota proteica
giornaliera consigliano
bull5 pasti al di
bullcarboidrati ad ogni pasto
bullolio vergine doliva
bullsemi
bullesclusione degli zuccheri raffinati
bullproteine ad ogni pasto
esempio di colazione
frullato di
2 cucchiai di yogurth
2 cucchiai di olio di lino
12 banana
12 succo di limone
1 cucchiaio di riso integrale
1 cucchiaio di miele
2 cucchiaini di semi oleosi
Lalimentazione deve apportare una adeguata
quantitagrave di colesterolo utile nella produzione
attraverso il pregnenolone del progesterone uova
uova di pesce acciughe crostacei e molluschi
alimenti ricchi di omega 3 pesce azzurro almeno tre
volte alla settimana
Lapporto di folati indispensabili per la prevenzione
in questa epoca delle patologie del tubo neurale puograve
essere assicurato con le verdure e la frutta (kiwi
fragole arance) il Calcio puograve essere introdotto con
semi di sesamo e formaggio caprino
I TRIMESTRE
Modificazioni materne embriogenesi e placentazione
II TRIMESTRE
IN QUESTO PERIODO egrave MOLTO IMPORTANTE ATTIVARE LA
TIROIDE ATTRAVERSO LrsquoASSUNZIONE DI SELENIO
Componente delle selenoproteine ha effetti immunomodulatori e
svolge un ruolo chiave nel metabolismo degli ormoni tiroidei nella
famiglia delle deiodinasi Il suo deficit egrave responsabile del cretinismo
edematoso endemico
Fonti naturali di selenio sono le frattaglie pesce molluschi carne
latte lievito di birra pasta riso funghi noci
La seleneproteina detta GPx ( glutatione perossidasi) egrave un potente
regolatore della sintesi degli ormoni tiroidei e protegge dal danno
ossidativo
II TRIMESTRE
Tra le deiodinasi la D3 egrave particolarmente localizzate nelle cellule del
cervello fegato fetale placenta e pelle Protegge il concepito dalla
eccessiva esposizione agli ormoni tiroidei
Lipotiroidismo subclinico si associa a distacco di placenta parto
pretermine e aborto (Casey 2005) e al rischio di sviluppo nel post
partum di tiroidite autoimmune e di sviluppo cognitivo subottimale nella
prole (Papi e coll 2007) Dose giornaliera selenio egrave 60 microgrammi
Le richieste fetali impongono di introdurre con la dieta anche agenti
antiossidanti vit C vit E betacarotene
III TRIMESTRE
In questo periodo della gestazione il notevole
accrescimento ponderale fetale e le variazione in senso
procoagulatorio dei parametri ematici consigliano di
ridurre i carboidrati di aumentare le proteine di origine
vegetale e di favorire la funzione renale
Si evitino funghi e asparagi e si limitino ananas kiwi
salvia per la loro azione sulla coagulazione
NAUSEA ED EMESI GRAVIDICA
Dobbiamo ridurre i carboidrati evitare dolci e liquidi limitare le proteine
Nella dieta sono utili
verdure amare
limone
zenzero
aceto
Per stabilizzare lambiente gastrico bisogna alcalinizzarlo
Migliorare la funzione epatica evitando fritti limitando gli ortaggi gialli
(carotenoidi) e le crucifere (per lo zolfo)
dare carboidrati facili senza glutine
coleretici e colagoghi tipo zucchine marinate con aglio menta e aceto
fragole kiwi papaya (aiuta a digerire ed egrave drenante ricca di K) e avocado
LA MINACCIA DABORTO
Dobbiamo fornire lorganismo di
Magnesio fonti sono germe di grano fagioli ceci cereali integrali riso
avena banane kiwi uva mais
Antiossidanti antinfiammatori ottenere lequilibrio glicemico omega 3 e
fibre Possiamo consigliare olio di semi di lino noci e frutta fresca uova
tonno e pesce spada Per lacido lipoico patate broccoli spinaci fegato
cuore carni rosse
ALIMENTAZIONE ED AMNIOCENTESI
evitare le contrazioni con alimenti ricchi di Mg e K riso patate
fagiolini zucchine banane
favorire la funzione epatica in senso procoagulante uova fegato
pomodori fragole peperonicarote zucca soiabrassicacee e
formaggio fuso
evitare le infezioni aglio zenzero cipolla prezzemolo chiodi di
garofano limone per la loro funzione immunostimolante
PREVENZIONE DELLE INFEZIONI GRAVIDICHE
Ligiene degli alimenti egrave fondamentale per la
prevenzione della toxoplasmosi
Bisogna mantenere un buon equilibrio glicemico e
seguire una dieta ricca di fibre e di antiossidanti quali
cipolla olio di oliva curcuma mirtilli riso integrale
frutta secca zenzero e aglio
IMPORTANZA DELLA COTTURA DEI
CIBI PER OTTENERE IL MIGLIOR
RISULTATO SOTTO IL PROFILO DELLA
DIGERIBILITA E DELLA QUALITA
PREVENZIONE DELLA GESTOSI
Consigliabile introdurre con la dieta pochi zuccheri molte
proteine (molto pesce e latte poche carni rosse) alimenti a
basso indice glicemico e verdure ricche di acqua come
fragole patate cipolle e cicoria
Per diminuire le resistenze vascolari e i grassi circolanti egrave
utile assumere prezzemolo ananas finocchio cipolla melone
aglio e fragole
Per migliorare la funzione cuore-reni sono utili legumi frutta
secca miele cereali integrali rucola vongole e uova
Iodine deficiency in pregnant women living in the South East
of the UK the influence of diet and nutritional supplements
on iodine status Bath SC Walter A Taylor A Wright J Rayman MP Author information
Iodine is a key component of the thyroid hormones which are crucial for brain development
Adequate intake of iodine in pregnancy is important as in utero deficiency may have lifelong
consequences for the offspring Data on the iodine status of UK pregnant women are sparse
and there are no such data for pregnant women in the South East of the UK A total of 100
pregnant women were recruited to a cross-sectional study carried out at the Royal Surrey
County Hospital Guildford at their first-trimester visit for an ultrasound scan The participants
provided a spot-urine sample (for the measurement of urinary iodine concentration (UIC) and
creatinine concentration) and 24 h iodine excretion was estimated from the urinary
iodinecreatinine ratio Women completed a general questionnaire and a FFQ The median UIC
(85middot3 μgl) indicated that the group was iodine deficient by World Health Organisation criteria
The median values of the iodinecreatinine ratio (122middot9 μgg) and of the estimated 24 h iodine
excretion (151middot2 μgd) were also suggestive of iodine deficiency UIC was significantly higher in
women taking an iodine-containing prenatal supplement (n 42) than in those not taking such a
supplement (Plt 0middot001) In the adjusted analyses milk intake maternal age and iodine-
containing prenatal supplement use were positively associated with the estimated 24 h urinary
iodine excretion Our finding of iodine deficiency in these women gives cause for concern We
suggest that women of childbearing age and pregnant women should be given advice on how to
improve their iodine status through dietary means A national survey of iodine status in UK
pregnant women is required
Maternal and in utero determinants of type 2 diabetes risk in the
young Bruce KD Abstract
The global prevalence of diabetes mellitus has reached epidemic proportions In 2010 it was estimated
that 64 of the adult population (285 million) have diabetes In recent years the incidence of type 2
diabetes (T2D) a condition traditionally associated with aging has been steadily increasing among
younger individuals It is now a well-established notion that the early-life period is a critical window of
development and that influences during this period can developmentally prime the metabolic status of the
adult This review discusses the role of maternal and in utero influences on the developmental priming of
T2D risk Both human epidemiological studies and experimental animal models are beginning to
demonstrate that early dietary challenges can accelerate the onset of age-associated metabolic
disturbances including insulin resistance T2D obesity hypertension and cardiovascular disease These
findings show that poor maternal nutrition can prime a prediabetes phenotype often manifest as insulin
resistance by very early stages of life Thus the maternal diet is a critical determinant of premature T2D
risk While the mechanisms that link early nutrition to age-associated metabolic decline are currently
unclear preliminary findings suggest perturbations in a number of processes involved in cellular aging
such as changes in longevity-associated Sirtuin activity epigenetic regulation of key metabolic genes and
mitochondrial dysfunction Preliminary studies show that pharmacological interventions in utero and dietary
supplementation in early postnatal life may alleviate insulin resistance and reduce T2D risk However
further studies are warranted to fully understand the relationship between the early environment and long-
term effects on metabolism Such mechanistic insights will facilitate strategic interventions that prevent
accelerated metabolic decline and the premature onset of T2D in the current and future generations
Counteracting oxidative stress in pregnancy through modulation
of maternal micronutrients and omega-3 fatty acids DSouza V1 Chavan-Gautam P Joshi S Abstract
During pregnancy oxidative stress has been implicated in the pathophysiology of
preeclampsia and preterm birth leading to poor birth outcome Hyperhomocysteinemia
caused as a consequence of altered micronutrients like folic acid and vitamin B12 is
associated with increased production of reactive oxygen species that generate oxidative
stress These micronutrients are important determinants of methyl donor s-adenosyl
methionine while phospholipids are important methyl acceptors in the one-carbon
metabolic cycle A series of our studies in women during pregnancy have demonstrated
altered levels of these micronutrients and the negative association of docosahexaenoic
acid with homocysteine Various strategies to counteract oxidative stress
during pregnancy such as antioxidant therapy have been examined and found to be
inconsistent In this review we focus on the role of oxidative stress in pregnancy and
discuss the possibility of ameliorating it through modulation of maternal micronutrients
and omega 3 fatty acids especially docosahexaenoic acid We propose for the first time
that manipulation of one-carbon metabolism by maternal diet could be a potential
mechanism to counteract oxidative stress through homocysteine lowering effects and
help in reducing the risk for adverse pregnancyoutcomes
The influence of a low glycemic index dietary intervention on maternal
dietary intake glycemic index and gestational weight gain
during pregnancy a randomized controlled trial McGowan CA Walsh JM Byrne J Curran S McAuliffe FM1 Abstract
BACKGROUND Maternal diet is known to impact pregnancy outcome Following a low glycemic index (GI) diet during pregnancy has been shown
to improve maternal glycemia and reduce infant birthweight and may be associated with a higher fibre intake We assessed the
impact of a low GI dietary intervention on maternal GI nutritional intake and gestational weight gain (GWG) during pregnancy Compliance and acceptability of the low GIdiet was also examined METHOD Eight hundred women were randomised in early pregnancy to receive low GI and healthy eating dietary advice or to receive
standard maternity care The intervention group received dietary advice at a group education session before 22 weeks gestation
All women completed a 3 day food diary during each trimester of pregnancy Two hundred and thirty five women from the intervention arm and 285 women from the control arm returned complete 3x3d FDs and were included in the present analysis RESULTS Maternal GI was significantly reduced in the intervention group at trimester 2 and 3 The numbers of women within the lowest
quartile of GI increased from 37 in trimester 1 to 52 in trimester 3 (Pthinspltthinsp0001) among the intervention group The intervention
group had significantly lower energy intake (Pthinspltthinsp005) higher protein ( TE) (Pthinspltthinsp001) and higher dietary fibre intake (Pthinspltthinsp001)
post intervention Consumption of food groups with known high GI values were significantly reduced among the intervention group Women in the intervention low GI group were less likely to exceed the Institute of Medicines GWG goals CONCLUSION A dietary intervention in early pregnancy had a positive influence on maternal GI food and nutrient intakes and GWG Following
a low GI diet may be particularly beneficial for women at risk of exceeding the GWG goals for pregnancy

Il regime dietetico deve considerare le condizioni nutrizionali
al momento del concepimento e il bisogno alimentare attuale
e remoto
Lalimentazione inadeguata si ripercuote negativamente sullevoluzione della gravidanza e sullaccrescimento fetale Una riduzione dellapporto quantitativo ma ancor piugrave di quello qualitativo puograve esitare in
bullneonato di insufficiente peso alla nascita con sviluppo osseo e dentale insufficiente bullcomplicazioni della gestazione quali parto pretermine distocia del travaglio
bulldifficoltagrave nellallattamento lalimentazione ipercalorica puograve d altro canto determinare
bullgestosi bulldisturbi digestivi bulldiabete gestazionale bullmacrosomia fetale con possibile conseguente distocia da sproporzione fetopelvica
EQUILIBRIO GLICEMICO = IG CG
durante tutta la gravidanza egrave importante
mantenere lequilibrio glicemico
costante ed adeguato apporto proteico
adeguata introduzione di liquidi
adeguato apporto di vitamine e sali
le modificazioni in senso diabetogeno del
metabolismo degli zuccheri in senso
chetogenico del metabolismo dei grassi e la
necessita di incrementare la quota proteica
giornaliera consigliano
bull5 pasti al di
bullcarboidrati ad ogni pasto
bullolio vergine doliva
bullsemi
bullesclusione degli zuccheri raffinati
bullproteine ad ogni pasto
esempio di colazione
frullato di
2 cucchiai di yogurth
2 cucchiai di olio di lino
12 banana
12 succo di limone
1 cucchiaio di riso integrale
1 cucchiaio di miele
2 cucchiaini di semi oleosi
Lalimentazione deve apportare una adeguata
quantitagrave di colesterolo utile nella produzione
attraverso il pregnenolone del progesterone uova
uova di pesce acciughe crostacei e molluschi
alimenti ricchi di omega 3 pesce azzurro almeno tre
volte alla settimana
Lapporto di folati indispensabili per la prevenzione
in questa epoca delle patologie del tubo neurale puograve
essere assicurato con le verdure e la frutta (kiwi
fragole arance) il Calcio puograve essere introdotto con
semi di sesamo e formaggio caprino
I TRIMESTRE
Modificazioni materne embriogenesi e placentazione
II TRIMESTRE
IN QUESTO PERIODO egrave MOLTO IMPORTANTE ATTIVARE LA
TIROIDE ATTRAVERSO LrsquoASSUNZIONE DI SELENIO
Componente delle selenoproteine ha effetti immunomodulatori e
svolge un ruolo chiave nel metabolismo degli ormoni tiroidei nella
famiglia delle deiodinasi Il suo deficit egrave responsabile del cretinismo
edematoso endemico
Fonti naturali di selenio sono le frattaglie pesce molluschi carne
latte lievito di birra pasta riso funghi noci
La seleneproteina detta GPx ( glutatione perossidasi) egrave un potente
regolatore della sintesi degli ormoni tiroidei e protegge dal danno
ossidativo
II TRIMESTRE
Tra le deiodinasi la D3 egrave particolarmente localizzate nelle cellule del
cervello fegato fetale placenta e pelle Protegge il concepito dalla
eccessiva esposizione agli ormoni tiroidei
Lipotiroidismo subclinico si associa a distacco di placenta parto
pretermine e aborto (Casey 2005) e al rischio di sviluppo nel post
partum di tiroidite autoimmune e di sviluppo cognitivo subottimale nella
prole (Papi e coll 2007) Dose giornaliera selenio egrave 60 microgrammi
Le richieste fetali impongono di introdurre con la dieta anche agenti
antiossidanti vit C vit E betacarotene
III TRIMESTRE
In questo periodo della gestazione il notevole
accrescimento ponderale fetale e le variazione in senso
procoagulatorio dei parametri ematici consigliano di
ridurre i carboidrati di aumentare le proteine di origine
vegetale e di favorire la funzione renale
Si evitino funghi e asparagi e si limitino ananas kiwi
salvia per la loro azione sulla coagulazione
NAUSEA ED EMESI GRAVIDICA
Dobbiamo ridurre i carboidrati evitare dolci e liquidi limitare le proteine
Nella dieta sono utili
verdure amare
limone
zenzero
aceto
Per stabilizzare lambiente gastrico bisogna alcalinizzarlo
Migliorare la funzione epatica evitando fritti limitando gli ortaggi gialli
(carotenoidi) e le crucifere (per lo zolfo)
dare carboidrati facili senza glutine
coleretici e colagoghi tipo zucchine marinate con aglio menta e aceto
fragole kiwi papaya (aiuta a digerire ed egrave drenante ricca di K) e avocado
LA MINACCIA DABORTO
Dobbiamo fornire lorganismo di
Magnesio fonti sono germe di grano fagioli ceci cereali integrali riso
avena banane kiwi uva mais
Antiossidanti antinfiammatori ottenere lequilibrio glicemico omega 3 e
fibre Possiamo consigliare olio di semi di lino noci e frutta fresca uova
tonno e pesce spada Per lacido lipoico patate broccoli spinaci fegato
cuore carni rosse
ALIMENTAZIONE ED AMNIOCENTESI
evitare le contrazioni con alimenti ricchi di Mg e K riso patate
fagiolini zucchine banane
favorire la funzione epatica in senso procoagulante uova fegato
pomodori fragole peperonicarote zucca soiabrassicacee e
formaggio fuso
evitare le infezioni aglio zenzero cipolla prezzemolo chiodi di
garofano limone per la loro funzione immunostimolante
PREVENZIONE DELLE INFEZIONI GRAVIDICHE
Ligiene degli alimenti egrave fondamentale per la
prevenzione della toxoplasmosi
Bisogna mantenere un buon equilibrio glicemico e
seguire una dieta ricca di fibre e di antiossidanti quali
cipolla olio di oliva curcuma mirtilli riso integrale
frutta secca zenzero e aglio
IMPORTANZA DELLA COTTURA DEI
CIBI PER OTTENERE IL MIGLIOR
RISULTATO SOTTO IL PROFILO DELLA
DIGERIBILITA E DELLA QUALITA
PREVENZIONE DELLA GESTOSI
Consigliabile introdurre con la dieta pochi zuccheri molte
proteine (molto pesce e latte poche carni rosse) alimenti a
basso indice glicemico e verdure ricche di acqua come
fragole patate cipolle e cicoria
Per diminuire le resistenze vascolari e i grassi circolanti egrave
utile assumere prezzemolo ananas finocchio cipolla melone
aglio e fragole
Per migliorare la funzione cuore-reni sono utili legumi frutta
secca miele cereali integrali rucola vongole e uova
Iodine deficiency in pregnant women living in the South East
of the UK the influence of diet and nutritional supplements
on iodine status Bath SC Walter A Taylor A Wright J Rayman MP Author information
Iodine is a key component of the thyroid hormones which are crucial for brain development
Adequate intake of iodine in pregnancy is important as in utero deficiency may have lifelong
consequences for the offspring Data on the iodine status of UK pregnant women are sparse
and there are no such data for pregnant women in the South East of the UK A total of 100
pregnant women were recruited to a cross-sectional study carried out at the Royal Surrey
County Hospital Guildford at their first-trimester visit for an ultrasound scan The participants
provided a spot-urine sample (for the measurement of urinary iodine concentration (UIC) and
creatinine concentration) and 24 h iodine excretion was estimated from the urinary
iodinecreatinine ratio Women completed a general questionnaire and a FFQ The median UIC
(85middot3 μgl) indicated that the group was iodine deficient by World Health Organisation criteria
The median values of the iodinecreatinine ratio (122middot9 μgg) and of the estimated 24 h iodine
excretion (151middot2 μgd) were also suggestive of iodine deficiency UIC was significantly higher in
women taking an iodine-containing prenatal supplement (n 42) than in those not taking such a
supplement (Plt 0middot001) In the adjusted analyses milk intake maternal age and iodine-
containing prenatal supplement use were positively associated with the estimated 24 h urinary
iodine excretion Our finding of iodine deficiency in these women gives cause for concern We
suggest that women of childbearing age and pregnant women should be given advice on how to
improve their iodine status through dietary means A national survey of iodine status in UK
pregnant women is required
Maternal and in utero determinants of type 2 diabetes risk in the
young Bruce KD Abstract
The global prevalence of diabetes mellitus has reached epidemic proportions In 2010 it was estimated
that 64 of the adult population (285 million) have diabetes In recent years the incidence of type 2
diabetes (T2D) a condition traditionally associated with aging has been steadily increasing among
younger individuals It is now a well-established notion that the early-life period is a critical window of
development and that influences during this period can developmentally prime the metabolic status of the
adult This review discusses the role of maternal and in utero influences on the developmental priming of
T2D risk Both human epidemiological studies and experimental animal models are beginning to
demonstrate that early dietary challenges can accelerate the onset of age-associated metabolic
disturbances including insulin resistance T2D obesity hypertension and cardiovascular disease These
findings show that poor maternal nutrition can prime a prediabetes phenotype often manifest as insulin
resistance by very early stages of life Thus the maternal diet is a critical determinant of premature T2D
risk While the mechanisms that link early nutrition to age-associated metabolic decline are currently
unclear preliminary findings suggest perturbations in a number of processes involved in cellular aging
such as changes in longevity-associated Sirtuin activity epigenetic regulation of key metabolic genes and
mitochondrial dysfunction Preliminary studies show that pharmacological interventions in utero and dietary
supplementation in early postnatal life may alleviate insulin resistance and reduce T2D risk However
further studies are warranted to fully understand the relationship between the early environment and long-
term effects on metabolism Such mechanistic insights will facilitate strategic interventions that prevent
accelerated metabolic decline and the premature onset of T2D in the current and future generations
Counteracting oxidative stress in pregnancy through modulation
of maternal micronutrients and omega-3 fatty acids DSouza V1 Chavan-Gautam P Joshi S Abstract
During pregnancy oxidative stress has been implicated in the pathophysiology of
preeclampsia and preterm birth leading to poor birth outcome Hyperhomocysteinemia
caused as a consequence of altered micronutrients like folic acid and vitamin B12 is
associated with increased production of reactive oxygen species that generate oxidative
stress These micronutrients are important determinants of methyl donor s-adenosyl
methionine while phospholipids are important methyl acceptors in the one-carbon
metabolic cycle A series of our studies in women during pregnancy have demonstrated
altered levels of these micronutrients and the negative association of docosahexaenoic
acid with homocysteine Various strategies to counteract oxidative stress
during pregnancy such as antioxidant therapy have been examined and found to be
inconsistent In this review we focus on the role of oxidative stress in pregnancy and
discuss the possibility of ameliorating it through modulation of maternal micronutrients
and omega 3 fatty acids especially docosahexaenoic acid We propose for the first time
that manipulation of one-carbon metabolism by maternal diet could be a potential
mechanism to counteract oxidative stress through homocysteine lowering effects and
help in reducing the risk for adverse pregnancyoutcomes
The influence of a low glycemic index dietary intervention on maternal
dietary intake glycemic index and gestational weight gain
during pregnancy a randomized controlled trial McGowan CA Walsh JM Byrne J Curran S McAuliffe FM1 Abstract
BACKGROUND Maternal diet is known to impact pregnancy outcome Following a low glycemic index (GI) diet during pregnancy has been shown
to improve maternal glycemia and reduce infant birthweight and may be associated with a higher fibre intake We assessed the
impact of a low GI dietary intervention on maternal GI nutritional intake and gestational weight gain (GWG) during pregnancy Compliance and acceptability of the low GIdiet was also examined METHOD Eight hundred women were randomised in early pregnancy to receive low GI and healthy eating dietary advice or to receive
standard maternity care The intervention group received dietary advice at a group education session before 22 weeks gestation
All women completed a 3 day food diary during each trimester of pregnancy Two hundred and thirty five women from the intervention arm and 285 women from the control arm returned complete 3x3d FDs and were included in the present analysis RESULTS Maternal GI was significantly reduced in the intervention group at trimester 2 and 3 The numbers of women within the lowest
quartile of GI increased from 37 in trimester 1 to 52 in trimester 3 (Pthinspltthinsp0001) among the intervention group The intervention
group had significantly lower energy intake (Pthinspltthinsp005) higher protein ( TE) (Pthinspltthinsp001) and higher dietary fibre intake (Pthinspltthinsp001)
post intervention Consumption of food groups with known high GI values were significantly reduced among the intervention group Women in the intervention low GI group were less likely to exceed the Institute of Medicines GWG goals CONCLUSION A dietary intervention in early pregnancy had a positive influence on maternal GI food and nutrient intakes and GWG Following
a low GI diet may be particularly beneficial for women at risk of exceeding the GWG goals for pregnancy

Lalimentazione inadeguata si ripercuote negativamente sullevoluzione della gravidanza e sullaccrescimento fetale Una riduzione dellapporto quantitativo ma ancor piugrave di quello qualitativo puograve esitare in
bullneonato di insufficiente peso alla nascita con sviluppo osseo e dentale insufficiente bullcomplicazioni della gestazione quali parto pretermine distocia del travaglio
bulldifficoltagrave nellallattamento lalimentazione ipercalorica puograve d altro canto determinare
bullgestosi bulldisturbi digestivi bulldiabete gestazionale bullmacrosomia fetale con possibile conseguente distocia da sproporzione fetopelvica
EQUILIBRIO GLICEMICO = IG CG
durante tutta la gravidanza egrave importante
mantenere lequilibrio glicemico
costante ed adeguato apporto proteico
adeguata introduzione di liquidi
adeguato apporto di vitamine e sali
le modificazioni in senso diabetogeno del
metabolismo degli zuccheri in senso
chetogenico del metabolismo dei grassi e la
necessita di incrementare la quota proteica
giornaliera consigliano
bull5 pasti al di
bullcarboidrati ad ogni pasto
bullolio vergine doliva
bullsemi
bullesclusione degli zuccheri raffinati
bullproteine ad ogni pasto
esempio di colazione
frullato di
2 cucchiai di yogurth
2 cucchiai di olio di lino
12 banana
12 succo di limone
1 cucchiaio di riso integrale
1 cucchiaio di miele
2 cucchiaini di semi oleosi
Lalimentazione deve apportare una adeguata
quantitagrave di colesterolo utile nella produzione
attraverso il pregnenolone del progesterone uova
uova di pesce acciughe crostacei e molluschi
alimenti ricchi di omega 3 pesce azzurro almeno tre
volte alla settimana
Lapporto di folati indispensabili per la prevenzione
in questa epoca delle patologie del tubo neurale puograve
essere assicurato con le verdure e la frutta (kiwi
fragole arance) il Calcio puograve essere introdotto con
semi di sesamo e formaggio caprino
I TRIMESTRE
Modificazioni materne embriogenesi e placentazione
II TRIMESTRE
IN QUESTO PERIODO egrave MOLTO IMPORTANTE ATTIVARE LA
TIROIDE ATTRAVERSO LrsquoASSUNZIONE DI SELENIO
Componente delle selenoproteine ha effetti immunomodulatori e
svolge un ruolo chiave nel metabolismo degli ormoni tiroidei nella
famiglia delle deiodinasi Il suo deficit egrave responsabile del cretinismo
edematoso endemico
Fonti naturali di selenio sono le frattaglie pesce molluschi carne
latte lievito di birra pasta riso funghi noci
La seleneproteina detta GPx ( glutatione perossidasi) egrave un potente
regolatore della sintesi degli ormoni tiroidei e protegge dal danno
ossidativo
II TRIMESTRE
Tra le deiodinasi la D3 egrave particolarmente localizzate nelle cellule del
cervello fegato fetale placenta e pelle Protegge il concepito dalla
eccessiva esposizione agli ormoni tiroidei
Lipotiroidismo subclinico si associa a distacco di placenta parto
pretermine e aborto (Casey 2005) e al rischio di sviluppo nel post
partum di tiroidite autoimmune e di sviluppo cognitivo subottimale nella
prole (Papi e coll 2007) Dose giornaliera selenio egrave 60 microgrammi
Le richieste fetali impongono di introdurre con la dieta anche agenti
antiossidanti vit C vit E betacarotene
III TRIMESTRE
In questo periodo della gestazione il notevole
accrescimento ponderale fetale e le variazione in senso
procoagulatorio dei parametri ematici consigliano di
ridurre i carboidrati di aumentare le proteine di origine
vegetale e di favorire la funzione renale
Si evitino funghi e asparagi e si limitino ananas kiwi
salvia per la loro azione sulla coagulazione
NAUSEA ED EMESI GRAVIDICA
Dobbiamo ridurre i carboidrati evitare dolci e liquidi limitare le proteine
Nella dieta sono utili
verdure amare
limone
zenzero
aceto
Per stabilizzare lambiente gastrico bisogna alcalinizzarlo
Migliorare la funzione epatica evitando fritti limitando gli ortaggi gialli
(carotenoidi) e le crucifere (per lo zolfo)
dare carboidrati facili senza glutine
coleretici e colagoghi tipo zucchine marinate con aglio menta e aceto
fragole kiwi papaya (aiuta a digerire ed egrave drenante ricca di K) e avocado
LA MINACCIA DABORTO
Dobbiamo fornire lorganismo di
Magnesio fonti sono germe di grano fagioli ceci cereali integrali riso
avena banane kiwi uva mais
Antiossidanti antinfiammatori ottenere lequilibrio glicemico omega 3 e
fibre Possiamo consigliare olio di semi di lino noci e frutta fresca uova
tonno e pesce spada Per lacido lipoico patate broccoli spinaci fegato
cuore carni rosse
ALIMENTAZIONE ED AMNIOCENTESI
evitare le contrazioni con alimenti ricchi di Mg e K riso patate
fagiolini zucchine banane
favorire la funzione epatica in senso procoagulante uova fegato
pomodori fragole peperonicarote zucca soiabrassicacee e
formaggio fuso
evitare le infezioni aglio zenzero cipolla prezzemolo chiodi di
garofano limone per la loro funzione immunostimolante
PREVENZIONE DELLE INFEZIONI GRAVIDICHE
Ligiene degli alimenti egrave fondamentale per la
prevenzione della toxoplasmosi
Bisogna mantenere un buon equilibrio glicemico e
seguire una dieta ricca di fibre e di antiossidanti quali
cipolla olio di oliva curcuma mirtilli riso integrale
frutta secca zenzero e aglio
IMPORTANZA DELLA COTTURA DEI
CIBI PER OTTENERE IL MIGLIOR
RISULTATO SOTTO IL PROFILO DELLA
DIGERIBILITA E DELLA QUALITA
PREVENZIONE DELLA GESTOSI
Consigliabile introdurre con la dieta pochi zuccheri molte
proteine (molto pesce e latte poche carni rosse) alimenti a
basso indice glicemico e verdure ricche di acqua come
fragole patate cipolle e cicoria
Per diminuire le resistenze vascolari e i grassi circolanti egrave
utile assumere prezzemolo ananas finocchio cipolla melone
aglio e fragole
Per migliorare la funzione cuore-reni sono utili legumi frutta
secca miele cereali integrali rucola vongole e uova
Iodine deficiency in pregnant women living in the South East
of the UK the influence of diet and nutritional supplements
on iodine status Bath SC Walter A Taylor A Wright J Rayman MP Author information
Iodine is a key component of the thyroid hormones which are crucial for brain development
Adequate intake of iodine in pregnancy is important as in utero deficiency may have lifelong
consequences for the offspring Data on the iodine status of UK pregnant women are sparse
and there are no such data for pregnant women in the South East of the UK A total of 100
pregnant women were recruited to a cross-sectional study carried out at the Royal Surrey
County Hospital Guildford at their first-trimester visit for an ultrasound scan The participants
provided a spot-urine sample (for the measurement of urinary iodine concentration (UIC) and
creatinine concentration) and 24 h iodine excretion was estimated from the urinary
iodinecreatinine ratio Women completed a general questionnaire and a FFQ The median UIC
(85middot3 μgl) indicated that the group was iodine deficient by World Health Organisation criteria
The median values of the iodinecreatinine ratio (122middot9 μgg) and of the estimated 24 h iodine
excretion (151middot2 μgd) were also suggestive of iodine deficiency UIC was significantly higher in
women taking an iodine-containing prenatal supplement (n 42) than in those not taking such a
supplement (Plt 0middot001) In the adjusted analyses milk intake maternal age and iodine-
containing prenatal supplement use were positively associated with the estimated 24 h urinary
iodine excretion Our finding of iodine deficiency in these women gives cause for concern We
suggest that women of childbearing age and pregnant women should be given advice on how to
improve their iodine status through dietary means A national survey of iodine status in UK
pregnant women is required
Maternal and in utero determinants of type 2 diabetes risk in the
young Bruce KD Abstract
The global prevalence of diabetes mellitus has reached epidemic proportions In 2010 it was estimated
that 64 of the adult population (285 million) have diabetes In recent years the incidence of type 2
diabetes (T2D) a condition traditionally associated with aging has been steadily increasing among
younger individuals It is now a well-established notion that the early-life period is a critical window of
development and that influences during this period can developmentally prime the metabolic status of the
adult This review discusses the role of maternal and in utero influences on the developmental priming of
T2D risk Both human epidemiological studies and experimental animal models are beginning to
demonstrate that early dietary challenges can accelerate the onset of age-associated metabolic
disturbances including insulin resistance T2D obesity hypertension and cardiovascular disease These
findings show that poor maternal nutrition can prime a prediabetes phenotype often manifest as insulin
resistance by very early stages of life Thus the maternal diet is a critical determinant of premature T2D
risk While the mechanisms that link early nutrition to age-associated metabolic decline are currently
unclear preliminary findings suggest perturbations in a number of processes involved in cellular aging
such as changes in longevity-associated Sirtuin activity epigenetic regulation of key metabolic genes and
mitochondrial dysfunction Preliminary studies show that pharmacological interventions in utero and dietary
supplementation in early postnatal life may alleviate insulin resistance and reduce T2D risk However
further studies are warranted to fully understand the relationship between the early environment and long-
term effects on metabolism Such mechanistic insights will facilitate strategic interventions that prevent
accelerated metabolic decline and the premature onset of T2D in the current and future generations
Counteracting oxidative stress in pregnancy through modulation
of maternal micronutrients and omega-3 fatty acids DSouza V1 Chavan-Gautam P Joshi S Abstract
During pregnancy oxidative stress has been implicated in the pathophysiology of
preeclampsia and preterm birth leading to poor birth outcome Hyperhomocysteinemia
caused as a consequence of altered micronutrients like folic acid and vitamin B12 is
associated with increased production of reactive oxygen species that generate oxidative
stress These micronutrients are important determinants of methyl donor s-adenosyl
methionine while phospholipids are important methyl acceptors in the one-carbon
metabolic cycle A series of our studies in women during pregnancy have demonstrated
altered levels of these micronutrients and the negative association of docosahexaenoic
acid with homocysteine Various strategies to counteract oxidative stress
during pregnancy such as antioxidant therapy have been examined and found to be
inconsistent In this review we focus on the role of oxidative stress in pregnancy and
discuss the possibility of ameliorating it through modulation of maternal micronutrients
and omega 3 fatty acids especially docosahexaenoic acid We propose for the first time
that manipulation of one-carbon metabolism by maternal diet could be a potential
mechanism to counteract oxidative stress through homocysteine lowering effects and
help in reducing the risk for adverse pregnancyoutcomes
The influence of a low glycemic index dietary intervention on maternal
dietary intake glycemic index and gestational weight gain
during pregnancy a randomized controlled trial McGowan CA Walsh JM Byrne J Curran S McAuliffe FM1 Abstract
BACKGROUND Maternal diet is known to impact pregnancy outcome Following a low glycemic index (GI) diet during pregnancy has been shown
to improve maternal glycemia and reduce infant birthweight and may be associated with a higher fibre intake We assessed the
impact of a low GI dietary intervention on maternal GI nutritional intake and gestational weight gain (GWG) during pregnancy Compliance and acceptability of the low GIdiet was also examined METHOD Eight hundred women were randomised in early pregnancy to receive low GI and healthy eating dietary advice or to receive
standard maternity care The intervention group received dietary advice at a group education session before 22 weeks gestation
All women completed a 3 day food diary during each trimester of pregnancy Two hundred and thirty five women from the intervention arm and 285 women from the control arm returned complete 3x3d FDs and were included in the present analysis RESULTS Maternal GI was significantly reduced in the intervention group at trimester 2 and 3 The numbers of women within the lowest
quartile of GI increased from 37 in trimester 1 to 52 in trimester 3 (Pthinspltthinsp0001) among the intervention group The intervention
group had significantly lower energy intake (Pthinspltthinsp005) higher protein ( TE) (Pthinspltthinsp001) and higher dietary fibre intake (Pthinspltthinsp001)
post intervention Consumption of food groups with known high GI values were significantly reduced among the intervention group Women in the intervention low GI group were less likely to exceed the Institute of Medicines GWG goals CONCLUSION A dietary intervention in early pregnancy had a positive influence on maternal GI food and nutrient intakes and GWG Following
a low GI diet may be particularly beneficial for women at risk of exceeding the GWG goals for pregnancy
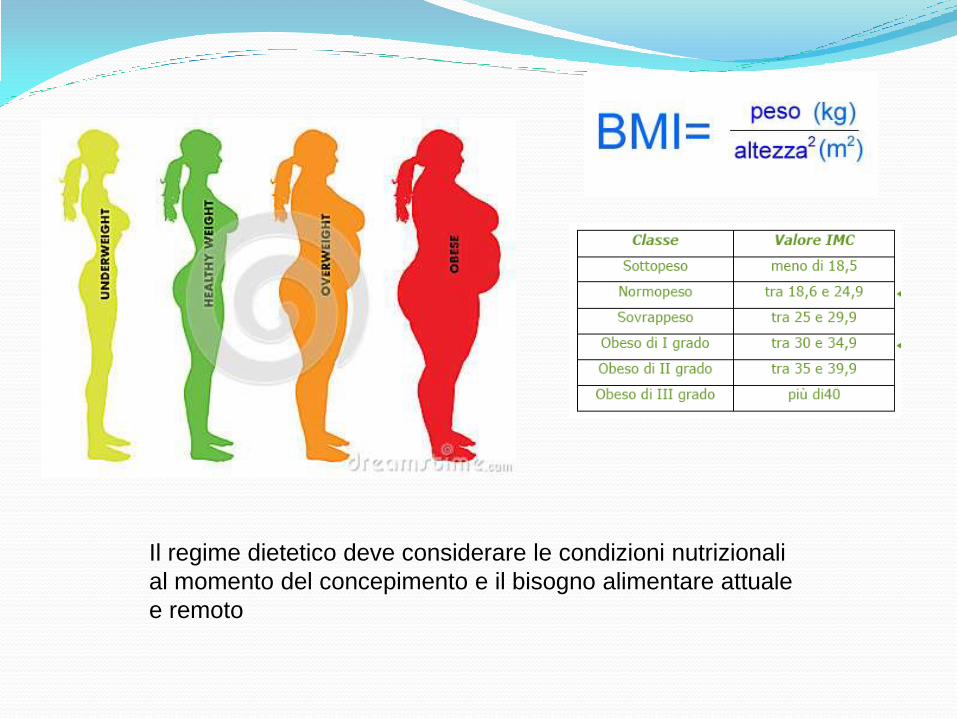
EQUILIBRIO GLICEMICO = IG CG
durante tutta la gravidanza egrave importante
mantenere lequilibrio glicemico
costante ed adeguato apporto proteico
adeguata introduzione di liquidi
adeguato apporto di vitamine e sali
le modificazioni in senso diabetogeno del
metabolismo degli zuccheri in senso
chetogenico del metabolismo dei grassi e la
necessita di incrementare la quota proteica
giornaliera consigliano
bull5 pasti al di
bullcarboidrati ad ogni pasto
bullolio vergine doliva
bullsemi
bullesclusione degli zuccheri raffinati
bullproteine ad ogni pasto
esempio di colazione
frullato di
2 cucchiai di yogurth
2 cucchiai di olio di lino
12 banana
12 succo di limone
1 cucchiaio di riso integrale
1 cucchiaio di miele
2 cucchiaini di semi oleosi
Lalimentazione deve apportare una adeguata
quantitagrave di colesterolo utile nella produzione
attraverso il pregnenolone del progesterone uova
uova di pesce acciughe crostacei e molluschi
alimenti ricchi di omega 3 pesce azzurro almeno tre
volte alla settimana
Lapporto di folati indispensabili per la prevenzione
in questa epoca delle patologie del tubo neurale puograve
essere assicurato con le verdure e la frutta (kiwi
fragole arance) il Calcio puograve essere introdotto con
semi di sesamo e formaggio caprino
I TRIMESTRE
Modificazioni materne embriogenesi e placentazione
II TRIMESTRE
IN QUESTO PERIODO egrave MOLTO IMPORTANTE ATTIVARE LA
TIROIDE ATTRAVERSO LrsquoASSUNZIONE DI SELENIO
Componente delle selenoproteine ha effetti immunomodulatori e
svolge un ruolo chiave nel metabolismo degli ormoni tiroidei nella
famiglia delle deiodinasi Il suo deficit egrave responsabile del cretinismo
edematoso endemico
Fonti naturali di selenio sono le frattaglie pesce molluschi carne
latte lievito di birra pasta riso funghi noci
La seleneproteina detta GPx ( glutatione perossidasi) egrave un potente
regolatore della sintesi degli ormoni tiroidei e protegge dal danno
ossidativo
II TRIMESTRE
Tra le deiodinasi la D3 egrave particolarmente localizzate nelle cellule del
cervello fegato fetale placenta e pelle Protegge il concepito dalla
eccessiva esposizione agli ormoni tiroidei
Lipotiroidismo subclinico si associa a distacco di placenta parto
pretermine e aborto (Casey 2005) e al rischio di sviluppo nel post
partum di tiroidite autoimmune e di sviluppo cognitivo subottimale nella
prole (Papi e coll 2007) Dose giornaliera selenio egrave 60 microgrammi
Le richieste fetali impongono di introdurre con la dieta anche agenti
antiossidanti vit C vit E betacarotene
III TRIMESTRE
In questo periodo della gestazione il notevole
accrescimento ponderale fetale e le variazione in senso
procoagulatorio dei parametri ematici consigliano di
ridurre i carboidrati di aumentare le proteine di origine
vegetale e di favorire la funzione renale
Si evitino funghi e asparagi e si limitino ananas kiwi
salvia per la loro azione sulla coagulazione
NAUSEA ED EMESI GRAVIDICA
Dobbiamo ridurre i carboidrati evitare dolci e liquidi limitare le proteine
Nella dieta sono utili
verdure amare
limone
zenzero
aceto
Per stabilizzare lambiente gastrico bisogna alcalinizzarlo
Migliorare la funzione epatica evitando fritti limitando gli ortaggi gialli
(carotenoidi) e le crucifere (per lo zolfo)
dare carboidrati facili senza glutine
coleretici e colagoghi tipo zucchine marinate con aglio menta e aceto
fragole kiwi papaya (aiuta a digerire ed egrave drenante ricca di K) e avocado
LA MINACCIA DABORTO
Dobbiamo fornire lorganismo di
Magnesio fonti sono germe di grano fagioli ceci cereali integrali riso
avena banane kiwi uva mais
Antiossidanti antinfiammatori ottenere lequilibrio glicemico omega 3 e
fibre Possiamo consigliare olio di semi di lino noci e frutta fresca uova
tonno e pesce spada Per lacido lipoico patate broccoli spinaci fegato
cuore carni rosse
ALIMENTAZIONE ED AMNIOCENTESI
evitare le contrazioni con alimenti ricchi di Mg e K riso patate
fagiolini zucchine banane
favorire la funzione epatica in senso procoagulante uova fegato
pomodori fragole peperonicarote zucca soiabrassicacee e
formaggio fuso
evitare le infezioni aglio zenzero cipolla prezzemolo chiodi di
garofano limone per la loro funzione immunostimolante
PREVENZIONE DELLE INFEZIONI GRAVIDICHE
Ligiene degli alimenti egrave fondamentale per la
prevenzione della toxoplasmosi
Bisogna mantenere un buon equilibrio glicemico e
seguire una dieta ricca di fibre e di antiossidanti quali
cipolla olio di oliva curcuma mirtilli riso integrale
frutta secca zenzero e aglio
IMPORTANZA DELLA COTTURA DEI
CIBI PER OTTENERE IL MIGLIOR
RISULTATO SOTTO IL PROFILO DELLA
DIGERIBILITA E DELLA QUALITA
PREVENZIONE DELLA GESTOSI
Consigliabile introdurre con la dieta pochi zuccheri molte
proteine (molto pesce e latte poche carni rosse) alimenti a
basso indice glicemico e verdure ricche di acqua come
fragole patate cipolle e cicoria
Per diminuire le resistenze vascolari e i grassi circolanti egrave
utile assumere prezzemolo ananas finocchio cipolla melone
aglio e fragole
Per migliorare la funzione cuore-reni sono utili legumi frutta
secca miele cereali integrali rucola vongole e uova
Iodine deficiency in pregnant women living in the South East
of the UK the influence of diet and nutritional supplements
on iodine status Bath SC Walter A Taylor A Wright J Rayman MP Author information
Iodine is a key component of the thyroid hormones which are crucial for brain development
Adequate intake of iodine in pregnancy is important as in utero deficiency may have lifelong
consequences for the offspring Data on the iodine status of UK pregnant women are sparse
and there are no such data for pregnant women in the South East of the UK A total of 100
pregnant women were recruited to a cross-sectional study carried out at the Royal Surrey
County Hospital Guildford at their first-trimester visit for an ultrasound scan The participants
provided a spot-urine sample (for the measurement of urinary iodine concentration (UIC) and
creatinine concentration) and 24 h iodine excretion was estimated from the urinary
iodinecreatinine ratio Women completed a general questionnaire and a FFQ The median UIC
(85middot3 μgl) indicated that the group was iodine deficient by World Health Organisation criteria
The median values of the iodinecreatinine ratio (122middot9 μgg) and of the estimated 24 h iodine
excretion (151middot2 μgd) were also suggestive of iodine deficiency UIC was significantly higher in
women taking an iodine-containing prenatal supplement (n 42) than in those not taking such a
supplement (Plt 0middot001) In the adjusted analyses milk intake maternal age and iodine-
containing prenatal supplement use were positively associated with the estimated 24 h urinary
iodine excretion Our finding of iodine deficiency in these women gives cause for concern We
suggest that women of childbearing age and pregnant women should be given advice on how to
improve their iodine status through dietary means A national survey of iodine status in UK
pregnant women is required
Maternal and in utero determinants of type 2 diabetes risk in the
young Bruce KD Abstract
The global prevalence of diabetes mellitus has reached epidemic proportions In 2010 it was estimated
that 64 of the adult population (285 million) have diabetes In recent years the incidence of type 2
diabetes (T2D) a condition traditionally associated with aging has been steadily increasing among
younger individuals It is now a well-established notion that the early-life period is a critical window of
development and that influences during this period can developmentally prime the metabolic status of the
adult This review discusses the role of maternal and in utero influences on the developmental priming of
T2D risk Both human epidemiological studies and experimental animal models are beginning to
demonstrate that early dietary challenges can accelerate the onset of age-associated metabolic
disturbances including insulin resistance T2D obesity hypertension and cardiovascular disease These
findings show that poor maternal nutrition can prime a prediabetes phenotype often manifest as insulin
resistance by very early stages of life Thus the maternal diet is a critical determinant of premature T2D
risk While the mechanisms that link early nutrition to age-associated metabolic decline are currently
unclear preliminary findings suggest perturbations in a number of processes involved in cellular aging
such as changes in longevity-associated Sirtuin activity epigenetic regulation of key metabolic genes and
mitochondrial dysfunction Preliminary studies show that pharmacological interventions in utero and dietary
supplementation in early postnatal life may alleviate insulin resistance and reduce T2D risk However
further studies are warranted to fully understand the relationship between the early environment and long-
term effects on metabolism Such mechanistic insights will facilitate strategic interventions that prevent
accelerated metabolic decline and the premature onset of T2D in the current and future generations
Counteracting oxidative stress in pregnancy through modulation
of maternal micronutrients and omega-3 fatty acids DSouza V1 Chavan-Gautam P Joshi S Abstract
During pregnancy oxidative stress has been implicated in the pathophysiology of
preeclampsia and preterm birth leading to poor birth outcome Hyperhomocysteinemia
caused as a consequence of altered micronutrients like folic acid and vitamin B12 is
associated with increased production of reactive oxygen species that generate oxidative
stress These micronutrients are important determinants of methyl donor s-adenosyl
methionine while phospholipids are important methyl acceptors in the one-carbon
metabolic cycle A series of our studies in women during pregnancy have demonstrated
altered levels of these micronutrients and the negative association of docosahexaenoic
acid with homocysteine Various strategies to counteract oxidative stress
during pregnancy such as antioxidant therapy have been examined and found to be
inconsistent In this review we focus on the role of oxidative stress in pregnancy and
discuss the possibility of ameliorating it through modulation of maternal micronutrients
and omega 3 fatty acids especially docosahexaenoic acid We propose for the first time
that manipulation of one-carbon metabolism by maternal diet could be a potential
mechanism to counteract oxidative stress through homocysteine lowering effects and
help in reducing the risk for adverse pregnancyoutcomes
The influence of a low glycemic index dietary intervention on maternal
dietary intake glycemic index and gestational weight gain
during pregnancy a randomized controlled trial McGowan CA Walsh JM Byrne J Curran S McAuliffe FM1 Abstract
BACKGROUND Maternal diet is known to impact pregnancy outcome Following a low glycemic index (GI) diet during pregnancy has been shown
to improve maternal glycemia and reduce infant birthweight and may be associated with a higher fibre intake We assessed the
impact of a low GI dietary intervention on maternal GI nutritional intake and gestational weight gain (GWG) during pregnancy Compliance and acceptability of the low GIdiet was also examined METHOD Eight hundred women were randomised in early pregnancy to receive low GI and healthy eating dietary advice or to receive
standard maternity care The intervention group received dietary advice at a group education session before 22 weeks gestation
All women completed a 3 day food diary during each trimester of pregnancy Two hundred and thirty five women from the intervention arm and 285 women from the control arm returned complete 3x3d FDs and were included in the present analysis RESULTS Maternal GI was significantly reduced in the intervention group at trimester 2 and 3 The numbers of women within the lowest
quartile of GI increased from 37 in trimester 1 to 52 in trimester 3 (Pthinspltthinsp0001) among the intervention group The intervention
group had significantly lower energy intake (Pthinspltthinsp005) higher protein ( TE) (Pthinspltthinsp001) and higher dietary fibre intake (Pthinspltthinsp001)
post intervention Consumption of food groups with known high GI values were significantly reduced among the intervention group Women in the intervention low GI group were less likely to exceed the Institute of Medicines GWG goals CONCLUSION A dietary intervention in early pregnancy had a positive influence on maternal GI food and nutrient intakes and GWG Following
a low GI diet may be particularly beneficial for women at risk of exceeding the GWG goals for pregnancy

durante tutta la gravidanza egrave importante
mantenere lequilibrio glicemico
costante ed adeguato apporto proteico
adeguata introduzione di liquidi
adeguato apporto di vitamine e sali
le modificazioni in senso diabetogeno del
metabolismo degli zuccheri in senso
chetogenico del metabolismo dei grassi e la
necessita di incrementare la quota proteica
giornaliera consigliano
bull5 pasti al di
bullcarboidrati ad ogni pasto
bullolio vergine doliva
bullsemi
bullesclusione degli zuccheri raffinati
bullproteine ad ogni pasto
esempio di colazione
frullato di
2 cucchiai di yogurth
2 cucchiai di olio di lino
12 banana
12 succo di limone
1 cucchiaio di riso integrale
1 cucchiaio di miele
2 cucchiaini di semi oleosi
Lalimentazione deve apportare una adeguata
quantitagrave di colesterolo utile nella produzione
attraverso il pregnenolone del progesterone uova
uova di pesce acciughe crostacei e molluschi
alimenti ricchi di omega 3 pesce azzurro almeno tre
volte alla settimana
Lapporto di folati indispensabili per la prevenzione
in questa epoca delle patologie del tubo neurale puograve
essere assicurato con le verdure e la frutta (kiwi
fragole arance) il Calcio puograve essere introdotto con
semi di sesamo e formaggio caprino
I TRIMESTRE
Modificazioni materne embriogenesi e placentazione
II TRIMESTRE
IN QUESTO PERIODO egrave MOLTO IMPORTANTE ATTIVARE LA
TIROIDE ATTRAVERSO LrsquoASSUNZIONE DI SELENIO
Componente delle selenoproteine ha effetti immunomodulatori e
svolge un ruolo chiave nel metabolismo degli ormoni tiroidei nella
famiglia delle deiodinasi Il suo deficit egrave responsabile del cretinismo
edematoso endemico
Fonti naturali di selenio sono le frattaglie pesce molluschi carne
latte lievito di birra pasta riso funghi noci
La seleneproteina detta GPx ( glutatione perossidasi) egrave un potente
regolatore della sintesi degli ormoni tiroidei e protegge dal danno
ossidativo
II TRIMESTRE
Tra le deiodinasi la D3 egrave particolarmente localizzate nelle cellule del
cervello fegato fetale placenta e pelle Protegge il concepito dalla
eccessiva esposizione agli ormoni tiroidei
Lipotiroidismo subclinico si associa a distacco di placenta parto
pretermine e aborto (Casey 2005) e al rischio di sviluppo nel post
partum di tiroidite autoimmune e di sviluppo cognitivo subottimale nella
prole (Papi e coll 2007) Dose giornaliera selenio egrave 60 microgrammi
Le richieste fetali impongono di introdurre con la dieta anche agenti
antiossidanti vit C vit E betacarotene
III TRIMESTRE
In questo periodo della gestazione il notevole
accrescimento ponderale fetale e le variazione in senso
procoagulatorio dei parametri ematici consigliano di
ridurre i carboidrati di aumentare le proteine di origine
vegetale e di favorire la funzione renale
Si evitino funghi e asparagi e si limitino ananas kiwi
salvia per la loro azione sulla coagulazione
NAUSEA ED EMESI GRAVIDICA
Dobbiamo ridurre i carboidrati evitare dolci e liquidi limitare le proteine
Nella dieta sono utili
verdure amare
limone
zenzero
aceto
Per stabilizzare lambiente gastrico bisogna alcalinizzarlo
Migliorare la funzione epatica evitando fritti limitando gli ortaggi gialli
(carotenoidi) e le crucifere (per lo zolfo)
dare carboidrati facili senza glutine
coleretici e colagoghi tipo zucchine marinate con aglio menta e aceto
fragole kiwi papaya (aiuta a digerire ed egrave drenante ricca di K) e avocado
LA MINACCIA DABORTO
Dobbiamo fornire lorganismo di
Magnesio fonti sono germe di grano fagioli ceci cereali integrali riso
avena banane kiwi uva mais
Antiossidanti antinfiammatori ottenere lequilibrio glicemico omega 3 e
fibre Possiamo consigliare olio di semi di lino noci e frutta fresca uova
tonno e pesce spada Per lacido lipoico patate broccoli spinaci fegato
cuore carni rosse
ALIMENTAZIONE ED AMNIOCENTESI
evitare le contrazioni con alimenti ricchi di Mg e K riso patate
fagiolini zucchine banane
favorire la funzione epatica in senso procoagulante uova fegato
pomodori fragole peperonicarote zucca soiabrassicacee e
formaggio fuso
evitare le infezioni aglio zenzero cipolla prezzemolo chiodi di
garofano limone per la loro funzione immunostimolante
PREVENZIONE DELLE INFEZIONI GRAVIDICHE
Ligiene degli alimenti egrave fondamentale per la
prevenzione della toxoplasmosi
Bisogna mantenere un buon equilibrio glicemico e
seguire una dieta ricca di fibre e di antiossidanti quali
cipolla olio di oliva curcuma mirtilli riso integrale
frutta secca zenzero e aglio
IMPORTANZA DELLA COTTURA DEI
CIBI PER OTTENERE IL MIGLIOR
RISULTATO SOTTO IL PROFILO DELLA
DIGERIBILITA E DELLA QUALITA
PREVENZIONE DELLA GESTOSI
Consigliabile introdurre con la dieta pochi zuccheri molte
proteine (molto pesce e latte poche carni rosse) alimenti a
basso indice glicemico e verdure ricche di acqua come
fragole patate cipolle e cicoria
Per diminuire le resistenze vascolari e i grassi circolanti egrave
utile assumere prezzemolo ananas finocchio cipolla melone
aglio e fragole
Per migliorare la funzione cuore-reni sono utili legumi frutta
secca miele cereali integrali rucola vongole e uova
Iodine deficiency in pregnant women living in the South East
of the UK the influence of diet and nutritional supplements
on iodine status Bath SC Walter A Taylor A Wright J Rayman MP Author information
Iodine is a key component of the thyroid hormones which are crucial for brain development
Adequate intake of iodine in pregnancy is important as in utero deficiency may have lifelong
consequences for the offspring Data on the iodine status of UK pregnant women are sparse
and there are no such data for pregnant women in the South East of the UK A total of 100
pregnant women were recruited to a cross-sectional study carried out at the Royal Surrey
County Hospital Guildford at their first-trimester visit for an ultrasound scan The participants
provided a spot-urine sample (for the measurement of urinary iodine concentration (UIC) and
creatinine concentration) and 24 h iodine excretion was estimated from the urinary
iodinecreatinine ratio Women completed a general questionnaire and a FFQ The median UIC
(85middot3 μgl) indicated that the group was iodine deficient by World Health Organisation criteria
The median values of the iodinecreatinine ratio (122middot9 μgg) and of the estimated 24 h iodine
excretion (151middot2 μgd) were also suggestive of iodine deficiency UIC was significantly higher in
women taking an iodine-containing prenatal supplement (n 42) than in those not taking such a
supplement (Plt 0middot001) In the adjusted analyses milk intake maternal age and iodine-
containing prenatal supplement use were positively associated with the estimated 24 h urinary
iodine excretion Our finding of iodine deficiency in these women gives cause for concern We
suggest that women of childbearing age and pregnant women should be given advice on how to
improve their iodine status through dietary means A national survey of iodine status in UK
pregnant women is required
Maternal and in utero determinants of type 2 diabetes risk in the
young Bruce KD Abstract
The global prevalence of diabetes mellitus has reached epidemic proportions In 2010 it was estimated
that 64 of the adult population (285 million) have diabetes In recent years the incidence of type 2
diabetes (T2D) a condition traditionally associated with aging has been steadily increasing among
younger individuals It is now a well-established notion that the early-life period is a critical window of
development and that influences during this period can developmentally prime the metabolic status of the
adult This review discusses the role of maternal and in utero influences on the developmental priming of
T2D risk Both human epidemiological studies and experimental animal models are beginning to
demonstrate that early dietary challenges can accelerate the onset of age-associated metabolic
disturbances including insulin resistance T2D obesity hypertension and cardiovascular disease These
findings show that poor maternal nutrition can prime a prediabetes phenotype often manifest as insulin
resistance by very early stages of life Thus the maternal diet is a critical determinant of premature T2D
risk While the mechanisms that link early nutrition to age-associated metabolic decline are currently
unclear preliminary findings suggest perturbations in a number of processes involved in cellular aging
such as changes in longevity-associated Sirtuin activity epigenetic regulation of key metabolic genes and
mitochondrial dysfunction Preliminary studies show that pharmacological interventions in utero and dietary
supplementation in early postnatal life may alleviate insulin resistance and reduce T2D risk However
further studies are warranted to fully understand the relationship between the early environment and long-
term effects on metabolism Such mechanistic insights will facilitate strategic interventions that prevent
accelerated metabolic decline and the premature onset of T2D in the current and future generations
Counteracting oxidative stress in pregnancy through modulation
of maternal micronutrients and omega-3 fatty acids DSouza V1 Chavan-Gautam P Joshi S Abstract
During pregnancy oxidative stress has been implicated in the pathophysiology of
preeclampsia and preterm birth leading to poor birth outcome Hyperhomocysteinemia
caused as a consequence of altered micronutrients like folic acid and vitamin B12 is
associated with increased production of reactive oxygen species that generate oxidative
stress These micronutrients are important determinants of methyl donor s-adenosyl
methionine while phospholipids are important methyl acceptors in the one-carbon
metabolic cycle A series of our studies in women during pregnancy have demonstrated
altered levels of these micronutrients and the negative association of docosahexaenoic
acid with homocysteine Various strategies to counteract oxidative stress
during pregnancy such as antioxidant therapy have been examined and found to be
inconsistent In this review we focus on the role of oxidative stress in pregnancy and
discuss the possibility of ameliorating it through modulation of maternal micronutrients
and omega 3 fatty acids especially docosahexaenoic acid We propose for the first time
that manipulation of one-carbon metabolism by maternal diet could be a potential
mechanism to counteract oxidative stress through homocysteine lowering effects and
help in reducing the risk for adverse pregnancyoutcomes
The influence of a low glycemic index dietary intervention on maternal
dietary intake glycemic index and gestational weight gain
during pregnancy a randomized controlled trial McGowan CA Walsh JM Byrne J Curran S McAuliffe FM1 Abstract
BACKGROUND Maternal diet is known to impact pregnancy outcome Following a low glycemic index (GI) diet during pregnancy has been shown
to improve maternal glycemia and reduce infant birthweight and may be associated with a higher fibre intake We assessed the
impact of a low GI dietary intervention on maternal GI nutritional intake and gestational weight gain (GWG) during pregnancy Compliance and acceptability of the low GIdiet was also examined METHOD Eight hundred women were randomised in early pregnancy to receive low GI and healthy eating dietary advice or to receive
standard maternity care The intervention group received dietary advice at a group education session before 22 weeks gestation
All women completed a 3 day food diary during each trimester of pregnancy Two hundred and thirty five women from the intervention arm and 285 women from the control arm returned complete 3x3d FDs and were included in the present analysis RESULTS Maternal GI was significantly reduced in the intervention group at trimester 2 and 3 The numbers of women within the lowest
quartile of GI increased from 37 in trimester 1 to 52 in trimester 3 (Pthinspltthinsp0001) among the intervention group The intervention
group had significantly lower energy intake (Pthinspltthinsp005) higher protein ( TE) (Pthinspltthinsp001) and higher dietary fibre intake (Pthinspltthinsp001)
post intervention Consumption of food groups with known high GI values were significantly reduced among the intervention group Women in the intervention low GI group were less likely to exceed the Institute of Medicines GWG goals CONCLUSION A dietary intervention in early pregnancy had a positive influence on maternal GI food and nutrient intakes and GWG Following
a low GI diet may be particularly beneficial for women at risk of exceeding the GWG goals for pregnancy

le modificazioni in senso diabetogeno del
metabolismo degli zuccheri in senso
chetogenico del metabolismo dei grassi e la
necessita di incrementare la quota proteica
giornaliera consigliano
bull5 pasti al di
bullcarboidrati ad ogni pasto
bullolio vergine doliva
bullsemi
bullesclusione degli zuccheri raffinati
bullproteine ad ogni pasto
esempio di colazione
frullato di
2 cucchiai di yogurth
2 cucchiai di olio di lino
12 banana
12 succo di limone
1 cucchiaio di riso integrale
1 cucchiaio di miele
2 cucchiaini di semi oleosi
Lalimentazione deve apportare una adeguata
quantitagrave di colesterolo utile nella produzione
attraverso il pregnenolone del progesterone uova
uova di pesce acciughe crostacei e molluschi
alimenti ricchi di omega 3 pesce azzurro almeno tre
volte alla settimana
Lapporto di folati indispensabili per la prevenzione
in questa epoca delle patologie del tubo neurale puograve
essere assicurato con le verdure e la frutta (kiwi
fragole arance) il Calcio puograve essere introdotto con
semi di sesamo e formaggio caprino
I TRIMESTRE
Modificazioni materne embriogenesi e placentazione
II TRIMESTRE
IN QUESTO PERIODO egrave MOLTO IMPORTANTE ATTIVARE LA
TIROIDE ATTRAVERSO LrsquoASSUNZIONE DI SELENIO
Componente delle selenoproteine ha effetti immunomodulatori e
svolge un ruolo chiave nel metabolismo degli ormoni tiroidei nella
famiglia delle deiodinasi Il suo deficit egrave responsabile del cretinismo
edematoso endemico
Fonti naturali di selenio sono le frattaglie pesce molluschi carne
latte lievito di birra pasta riso funghi noci
La seleneproteina detta GPx ( glutatione perossidasi) egrave un potente
regolatore della sintesi degli ormoni tiroidei e protegge dal danno
ossidativo
II TRIMESTRE
Tra le deiodinasi la D3 egrave particolarmente localizzate nelle cellule del
cervello fegato fetale placenta e pelle Protegge il concepito dalla
eccessiva esposizione agli ormoni tiroidei
Lipotiroidismo subclinico si associa a distacco di placenta parto
pretermine e aborto (Casey 2005) e al rischio di sviluppo nel post
partum di tiroidite autoimmune e di sviluppo cognitivo subottimale nella
prole (Papi e coll 2007) Dose giornaliera selenio egrave 60 microgrammi
Le richieste fetali impongono di introdurre con la dieta anche agenti
antiossidanti vit C vit E betacarotene
III TRIMESTRE
In questo periodo della gestazione il notevole
accrescimento ponderale fetale e le variazione in senso
procoagulatorio dei parametri ematici consigliano di
ridurre i carboidrati di aumentare le proteine di origine
vegetale e di favorire la funzione renale
Si evitino funghi e asparagi e si limitino ananas kiwi
salvia per la loro azione sulla coagulazione
NAUSEA ED EMESI GRAVIDICA
Dobbiamo ridurre i carboidrati evitare dolci e liquidi limitare le proteine
Nella dieta sono utili
verdure amare
limone
zenzero
aceto
Per stabilizzare lambiente gastrico bisogna alcalinizzarlo
Migliorare la funzione epatica evitando fritti limitando gli ortaggi gialli
(carotenoidi) e le crucifere (per lo zolfo)
dare carboidrati facili senza glutine
coleretici e colagoghi tipo zucchine marinate con aglio menta e aceto
fragole kiwi papaya (aiuta a digerire ed egrave drenante ricca di K) e avocado
LA MINACCIA DABORTO
Dobbiamo fornire lorganismo di
Magnesio fonti sono germe di grano fagioli ceci cereali integrali riso
avena banane kiwi uva mais
Antiossidanti antinfiammatori ottenere lequilibrio glicemico omega 3 e
fibre Possiamo consigliare olio di semi di lino noci e frutta fresca uova
tonno e pesce spada Per lacido lipoico patate broccoli spinaci fegato
cuore carni rosse
ALIMENTAZIONE ED AMNIOCENTESI
evitare le contrazioni con alimenti ricchi di Mg e K riso patate
fagiolini zucchine banane
favorire la funzione epatica in senso procoagulante uova fegato
pomodori fragole peperonicarote zucca soiabrassicacee e
formaggio fuso
evitare le infezioni aglio zenzero cipolla prezzemolo chiodi di
garofano limone per la loro funzione immunostimolante
PREVENZIONE DELLE INFEZIONI GRAVIDICHE
Ligiene degli alimenti egrave fondamentale per la
prevenzione della toxoplasmosi
Bisogna mantenere un buon equilibrio glicemico e
seguire una dieta ricca di fibre e di antiossidanti quali
cipolla olio di oliva curcuma mirtilli riso integrale
frutta secca zenzero e aglio
IMPORTANZA DELLA COTTURA DEI
CIBI PER OTTENERE IL MIGLIOR
RISULTATO SOTTO IL PROFILO DELLA
DIGERIBILITA E DELLA QUALITA
PREVENZIONE DELLA GESTOSI
Consigliabile introdurre con la dieta pochi zuccheri molte
proteine (molto pesce e latte poche carni rosse) alimenti a
basso indice glicemico e verdure ricche di acqua come
fragole patate cipolle e cicoria
Per diminuire le resistenze vascolari e i grassi circolanti egrave
utile assumere prezzemolo ananas finocchio cipolla melone
aglio e fragole
Per migliorare la funzione cuore-reni sono utili legumi frutta
secca miele cereali integrali rucola vongole e uova
Iodine deficiency in pregnant women living in the South East
of the UK the influence of diet and nutritional supplements
on iodine status Bath SC Walter A Taylor A Wright J Rayman MP Author information
Iodine is a key component of the thyroid hormones which are crucial for brain development
Adequate intake of iodine in pregnancy is important as in utero deficiency may have lifelong
consequences for the offspring Data on the iodine status of UK pregnant women are sparse
and there are no such data for pregnant women in the South East of the UK A total of 100
pregnant women were recruited to a cross-sectional study carried out at the Royal Surrey
County Hospital Guildford at their first-trimester visit for an ultrasound scan The participants
provided a spot-urine sample (for the measurement of urinary iodine concentration (UIC) and
creatinine concentration) and 24 h iodine excretion was estimated from the urinary
iodinecreatinine ratio Women completed a general questionnaire and a FFQ The median UIC
(85middot3 μgl) indicated that the group was iodine deficient by World Health Organisation criteria
The median values of the iodinecreatinine ratio (122middot9 μgg) and of the estimated 24 h iodine
excretion (151middot2 μgd) were also suggestive of iodine deficiency UIC was significantly higher in
women taking an iodine-containing prenatal supplement (n 42) than in those not taking such a
supplement (Plt 0middot001) In the adjusted analyses milk intake maternal age and iodine-
containing prenatal supplement use were positively associated with the estimated 24 h urinary
iodine excretion Our finding of iodine deficiency in these women gives cause for concern We
suggest that women of childbearing age and pregnant women should be given advice on how to
improve their iodine status through dietary means A national survey of iodine status in UK
pregnant women is required
Maternal and in utero determinants of type 2 diabetes risk in the
young Bruce KD Abstract
The global prevalence of diabetes mellitus has reached epidemic proportions In 2010 it was estimated
that 64 of the adult population (285 million) have diabetes In recent years the incidence of type 2
diabetes (T2D) a condition traditionally associated with aging has been steadily increasing among
younger individuals It is now a well-established notion that the early-life period is a critical window of
development and that influences during this period can developmentally prime the metabolic status of the
adult This review discusses the role of maternal and in utero influences on the developmental priming of
T2D risk Both human epidemiological studies and experimental animal models are beginning to
demonstrate that early dietary challenges can accelerate the onset of age-associated metabolic
disturbances including insulin resistance T2D obesity hypertension and cardiovascular disease These
findings show that poor maternal nutrition can prime a prediabetes phenotype often manifest as insulin
resistance by very early stages of life Thus the maternal diet is a critical determinant of premature T2D
risk While the mechanisms that link early nutrition to age-associated metabolic decline are currently
unclear preliminary findings suggest perturbations in a number of processes involved in cellular aging
such as changes in longevity-associated Sirtuin activity epigenetic regulation of key metabolic genes and
mitochondrial dysfunction Preliminary studies show that pharmacological interventions in utero and dietary
supplementation in early postnatal life may alleviate insulin resistance and reduce T2D risk However
further studies are warranted to fully understand the relationship between the early environment and long-
term effects on metabolism Such mechanistic insights will facilitate strategic interventions that prevent
accelerated metabolic decline and the premature onset of T2D in the current and future generations
Counteracting oxidative stress in pregnancy through modulation
of maternal micronutrients and omega-3 fatty acids DSouza V1 Chavan-Gautam P Joshi S Abstract
During pregnancy oxidative stress has been implicated in the pathophysiology of
preeclampsia and preterm birth leading to poor birth outcome Hyperhomocysteinemia
caused as a consequence of altered micronutrients like folic acid and vitamin B12 is
associated with increased production of reactive oxygen species that generate oxidative
stress These micronutrients are important determinants of methyl donor s-adenosyl
methionine while phospholipids are important methyl acceptors in the one-carbon
metabolic cycle A series of our studies in women during pregnancy have demonstrated
altered levels of these micronutrients and the negative association of docosahexaenoic
acid with homocysteine Various strategies to counteract oxidative stress
during pregnancy such as antioxidant therapy have been examined and found to be
inconsistent In this review we focus on the role of oxidative stress in pregnancy and
discuss the possibility of ameliorating it through modulation of maternal micronutrients
and omega 3 fatty acids especially docosahexaenoic acid We propose for the first time
that manipulation of one-carbon metabolism by maternal diet could be a potential
mechanism to counteract oxidative stress through homocysteine lowering effects and
help in reducing the risk for adverse pregnancyoutcomes
The influence of a low glycemic index dietary intervention on maternal
dietary intake glycemic index and gestational weight gain
during pregnancy a randomized controlled trial McGowan CA Walsh JM Byrne J Curran S McAuliffe FM1 Abstract
BACKGROUND Maternal diet is known to impact pregnancy outcome Following a low glycemic index (GI) diet during pregnancy has been shown
to improve maternal glycemia and reduce infant birthweight and may be associated with a higher fibre intake We assessed the
impact of a low GI dietary intervention on maternal GI nutritional intake and gestational weight gain (GWG) during pregnancy Compliance and acceptability of the low GIdiet was also examined METHOD Eight hundred women were randomised in early pregnancy to receive low GI and healthy eating dietary advice or to receive
standard maternity care The intervention group received dietary advice at a group education session before 22 weeks gestation
All women completed a 3 day food diary during each trimester of pregnancy Two hundred and thirty five women from the intervention arm and 285 women from the control arm returned complete 3x3d FDs and were included in the present analysis RESULTS Maternal GI was significantly reduced in the intervention group at trimester 2 and 3 The numbers of women within the lowest
quartile of GI increased from 37 in trimester 1 to 52 in trimester 3 (Pthinspltthinsp0001) among the intervention group The intervention
group had significantly lower energy intake (Pthinspltthinsp005) higher protein ( TE) (Pthinspltthinsp001) and higher dietary fibre intake (Pthinspltthinsp001)
post intervention Consumption of food groups with known high GI values were significantly reduced among the intervention group Women in the intervention low GI group were less likely to exceed the Institute of Medicines GWG goals CONCLUSION A dietary intervention in early pregnancy had a positive influence on maternal GI food and nutrient intakes and GWG Following
a low GI diet may be particularly beneficial for women at risk of exceeding the GWG goals for pregnancy

esempio di colazione
frullato di
2 cucchiai di yogurth
2 cucchiai di olio di lino
12 banana
12 succo di limone
1 cucchiaio di riso integrale
1 cucchiaio di miele
2 cucchiaini di semi oleosi
Lalimentazione deve apportare una adeguata
quantitagrave di colesterolo utile nella produzione
attraverso il pregnenolone del progesterone uova
uova di pesce acciughe crostacei e molluschi
alimenti ricchi di omega 3 pesce azzurro almeno tre
volte alla settimana
Lapporto di folati indispensabili per la prevenzione
in questa epoca delle patologie del tubo neurale puograve
essere assicurato con le verdure e la frutta (kiwi
fragole arance) il Calcio puograve essere introdotto con
semi di sesamo e formaggio caprino
I TRIMESTRE
Modificazioni materne embriogenesi e placentazione
II TRIMESTRE
IN QUESTO PERIODO egrave MOLTO IMPORTANTE ATTIVARE LA
TIROIDE ATTRAVERSO LrsquoASSUNZIONE DI SELENIO
Componente delle selenoproteine ha effetti immunomodulatori e
svolge un ruolo chiave nel metabolismo degli ormoni tiroidei nella
famiglia delle deiodinasi Il suo deficit egrave responsabile del cretinismo
edematoso endemico
Fonti naturali di selenio sono le frattaglie pesce molluschi carne
latte lievito di birra pasta riso funghi noci
La seleneproteina detta GPx ( glutatione perossidasi) egrave un potente
regolatore della sintesi degli ormoni tiroidei e protegge dal danno
ossidativo
II TRIMESTRE
Tra le deiodinasi la D3 egrave particolarmente localizzate nelle cellule del
cervello fegato fetale placenta e pelle Protegge il concepito dalla
eccessiva esposizione agli ormoni tiroidei
Lipotiroidismo subclinico si associa a distacco di placenta parto
pretermine e aborto (Casey 2005) e al rischio di sviluppo nel post
partum di tiroidite autoimmune e di sviluppo cognitivo subottimale nella
prole (Papi e coll 2007) Dose giornaliera selenio egrave 60 microgrammi
Le richieste fetali impongono di introdurre con la dieta anche agenti
antiossidanti vit C vit E betacarotene
III TRIMESTRE
In questo periodo della gestazione il notevole
accrescimento ponderale fetale e le variazione in senso
procoagulatorio dei parametri ematici consigliano di
ridurre i carboidrati di aumentare le proteine di origine
vegetale e di favorire la funzione renale
Si evitino funghi e asparagi e si limitino ananas kiwi
salvia per la loro azione sulla coagulazione
NAUSEA ED EMESI GRAVIDICA
Dobbiamo ridurre i carboidrati evitare dolci e liquidi limitare le proteine
Nella dieta sono utili
verdure amare
limone
zenzero
aceto
Per stabilizzare lambiente gastrico bisogna alcalinizzarlo
Migliorare la funzione epatica evitando fritti limitando gli ortaggi gialli
(carotenoidi) e le crucifere (per lo zolfo)
dare carboidrati facili senza glutine
coleretici e colagoghi tipo zucchine marinate con aglio menta e aceto
fragole kiwi papaya (aiuta a digerire ed egrave drenante ricca di K) e avocado
LA MINACCIA DABORTO
Dobbiamo fornire lorganismo di
Magnesio fonti sono germe di grano fagioli ceci cereali integrali riso
avena banane kiwi uva mais
Antiossidanti antinfiammatori ottenere lequilibrio glicemico omega 3 e
fibre Possiamo consigliare olio di semi di lino noci e frutta fresca uova
tonno e pesce spada Per lacido lipoico patate broccoli spinaci fegato
cuore carni rosse
ALIMENTAZIONE ED AMNIOCENTESI
evitare le contrazioni con alimenti ricchi di Mg e K riso patate
fagiolini zucchine banane
favorire la funzione epatica in senso procoagulante uova fegato
pomodori fragole peperonicarote zucca soiabrassicacee e
formaggio fuso
evitare le infezioni aglio zenzero cipolla prezzemolo chiodi di
garofano limone per la loro funzione immunostimolante
PREVENZIONE DELLE INFEZIONI GRAVIDICHE
Ligiene degli alimenti egrave fondamentale per la
prevenzione della toxoplasmosi
Bisogna mantenere un buon equilibrio glicemico e
seguire una dieta ricca di fibre e di antiossidanti quali
cipolla olio di oliva curcuma mirtilli riso integrale
frutta secca zenzero e aglio
IMPORTANZA DELLA COTTURA DEI
CIBI PER OTTENERE IL MIGLIOR
RISULTATO SOTTO IL PROFILO DELLA
DIGERIBILITA E DELLA QUALITA
PREVENZIONE DELLA GESTOSI
Consigliabile introdurre con la dieta pochi zuccheri molte
proteine (molto pesce e latte poche carni rosse) alimenti a
basso indice glicemico e verdure ricche di acqua come
fragole patate cipolle e cicoria
Per diminuire le resistenze vascolari e i grassi circolanti egrave
utile assumere prezzemolo ananas finocchio cipolla melone
aglio e fragole
Per migliorare la funzione cuore-reni sono utili legumi frutta
secca miele cereali integrali rucola vongole e uova
Iodine deficiency in pregnant women living in the South East
of the UK the influence of diet and nutritional supplements
on iodine status Bath SC Walter A Taylor A Wright J Rayman MP Author information
Iodine is a key component of the thyroid hormones which are crucial for brain development
Adequate intake of iodine in pregnancy is important as in utero deficiency may have lifelong
consequences for the offspring Data on the iodine status of UK pregnant women are sparse
and there are no such data for pregnant women in the South East of the UK A total of 100
pregnant women were recruited to a cross-sectional study carried out at the Royal Surrey
County Hospital Guildford at their first-trimester visit for an ultrasound scan The participants
provided a spot-urine sample (for the measurement of urinary iodine concentration (UIC) and
creatinine concentration) and 24 h iodine excretion was estimated from the urinary
iodinecreatinine ratio Women completed a general questionnaire and a FFQ The median UIC
(85middot3 μgl) indicated that the group was iodine deficient by World Health Organisation criteria
The median values of the iodinecreatinine ratio (122middot9 μgg) and of the estimated 24 h iodine
excretion (151middot2 μgd) were also suggestive of iodine deficiency UIC was significantly higher in
women taking an iodine-containing prenatal supplement (n 42) than in those not taking such a
supplement (Plt 0middot001) In the adjusted analyses milk intake maternal age and iodine-
containing prenatal supplement use were positively associated with the estimated 24 h urinary
iodine excretion Our finding of iodine deficiency in these women gives cause for concern We
suggest that women of childbearing age and pregnant women should be given advice on how to
improve their iodine status through dietary means A national survey of iodine status in UK
pregnant women is required
Maternal and in utero determinants of type 2 diabetes risk in the
young Bruce KD Abstract
The global prevalence of diabetes mellitus has reached epidemic proportions In 2010 it was estimated
that 64 of the adult population (285 million) have diabetes In recent years the incidence of type 2
diabetes (T2D) a condition traditionally associated with aging has been steadily increasing among
younger individuals It is now a well-established notion that the early-life period is a critical window of
development and that influences during this period can developmentally prime the metabolic status of the
adult This review discusses the role of maternal and in utero influences on the developmental priming of
T2D risk Both human epidemiological studies and experimental animal models are beginning to
demonstrate that early dietary challenges can accelerate the onset of age-associated metabolic
disturbances including insulin resistance T2D obesity hypertension and cardiovascular disease These
findings show that poor maternal nutrition can prime a prediabetes phenotype often manifest as insulin
resistance by very early stages of life Thus the maternal diet is a critical determinant of premature T2D
risk While the mechanisms that link early nutrition to age-associated metabolic decline are currently
unclear preliminary findings suggest perturbations in a number of processes involved in cellular aging
such as changes in longevity-associated Sirtuin activity epigenetic regulation of key metabolic genes and
mitochondrial dysfunction Preliminary studies show that pharmacological interventions in utero and dietary
supplementation in early postnatal life may alleviate insulin resistance and reduce T2D risk However
further studies are warranted to fully understand the relationship between the early environment and long-
term effects on metabolism Such mechanistic insights will facilitate strategic interventions that prevent
accelerated metabolic decline and the premature onset of T2D in the current and future generations
Counteracting oxidative stress in pregnancy through modulation
of maternal micronutrients and omega-3 fatty acids DSouza V1 Chavan-Gautam P Joshi S Abstract
During pregnancy oxidative stress has been implicated in the pathophysiology of
preeclampsia and preterm birth leading to poor birth outcome Hyperhomocysteinemia
caused as a consequence of altered micronutrients like folic acid and vitamin B12 is
associated with increased production of reactive oxygen species that generate oxidative
stress These micronutrients are important determinants of methyl donor s-adenosyl
methionine while phospholipids are important methyl acceptors in the one-carbon
metabolic cycle A series of our studies in women during pregnancy have demonstrated
altered levels of these micronutrients and the negative association of docosahexaenoic
acid with homocysteine Various strategies to counteract oxidative stress
during pregnancy such as antioxidant therapy have been examined and found to be
inconsistent In this review we focus on the role of oxidative stress in pregnancy and
discuss the possibility of ameliorating it through modulation of maternal micronutrients
and omega 3 fatty acids especially docosahexaenoic acid We propose for the first time
that manipulation of one-carbon metabolism by maternal diet could be a potential
mechanism to counteract oxidative stress through homocysteine lowering effects and
help in reducing the risk for adverse pregnancyoutcomes
The influence of a low glycemic index dietary intervention on maternal
dietary intake glycemic index and gestational weight gain
during pregnancy a randomized controlled trial McGowan CA Walsh JM Byrne J Curran S McAuliffe FM1 Abstract
BACKGROUND Maternal diet is known to impact pregnancy outcome Following a low glycemic index (GI) diet during pregnancy has been shown
to improve maternal glycemia and reduce infant birthweight and may be associated with a higher fibre intake We assessed the
impact of a low GI dietary intervention on maternal GI nutritional intake and gestational weight gain (GWG) during pregnancy Compliance and acceptability of the low GIdiet was also examined METHOD Eight hundred women were randomised in early pregnancy to receive low GI and healthy eating dietary advice or to receive
standard maternity care The intervention group received dietary advice at a group education session before 22 weeks gestation
All women completed a 3 day food diary during each trimester of pregnancy Two hundred and thirty five women from the intervention arm and 285 women from the control arm returned complete 3x3d FDs and were included in the present analysis RESULTS Maternal GI was significantly reduced in the intervention group at trimester 2 and 3 The numbers of women within the lowest
quartile of GI increased from 37 in trimester 1 to 52 in trimester 3 (Pthinspltthinsp0001) among the intervention group The intervention
group had significantly lower energy intake (Pthinspltthinsp005) higher protein ( TE) (Pthinspltthinsp001) and higher dietary fibre intake (Pthinspltthinsp001)
post intervention Consumption of food groups with known high GI values were significantly reduced among the intervention group Women in the intervention low GI group were less likely to exceed the Institute of Medicines GWG goals CONCLUSION A dietary intervention in early pregnancy had a positive influence on maternal GI food and nutrient intakes and GWG Following
a low GI diet may be particularly beneficial for women at risk of exceeding the GWG goals for pregnancy

Lalimentazione deve apportare una adeguata
quantitagrave di colesterolo utile nella produzione
attraverso il pregnenolone del progesterone uova
uova di pesce acciughe crostacei e molluschi
alimenti ricchi di omega 3 pesce azzurro almeno tre
volte alla settimana
Lapporto di folati indispensabili per la prevenzione
in questa epoca delle patologie del tubo neurale puograve
essere assicurato con le verdure e la frutta (kiwi
fragole arance) il Calcio puograve essere introdotto con
semi di sesamo e formaggio caprino
I TRIMESTRE
Modificazioni materne embriogenesi e placentazione
II TRIMESTRE
IN QUESTO PERIODO egrave MOLTO IMPORTANTE ATTIVARE LA
TIROIDE ATTRAVERSO LrsquoASSUNZIONE DI SELENIO
Componente delle selenoproteine ha effetti immunomodulatori e
svolge un ruolo chiave nel metabolismo degli ormoni tiroidei nella
famiglia delle deiodinasi Il suo deficit egrave responsabile del cretinismo
edematoso endemico
Fonti naturali di selenio sono le frattaglie pesce molluschi carne
latte lievito di birra pasta riso funghi noci
La seleneproteina detta GPx ( glutatione perossidasi) egrave un potente
regolatore della sintesi degli ormoni tiroidei e protegge dal danno
ossidativo
II TRIMESTRE
Tra le deiodinasi la D3 egrave particolarmente localizzate nelle cellule del
cervello fegato fetale placenta e pelle Protegge il concepito dalla
eccessiva esposizione agli ormoni tiroidei
Lipotiroidismo subclinico si associa a distacco di placenta parto
pretermine e aborto (Casey 2005) e al rischio di sviluppo nel post
partum di tiroidite autoimmune e di sviluppo cognitivo subottimale nella
prole (Papi e coll 2007) Dose giornaliera selenio egrave 60 microgrammi
Le richieste fetali impongono di introdurre con la dieta anche agenti
antiossidanti vit C vit E betacarotene
III TRIMESTRE
In questo periodo della gestazione il notevole
accrescimento ponderale fetale e le variazione in senso
procoagulatorio dei parametri ematici consigliano di
ridurre i carboidrati di aumentare le proteine di origine
vegetale e di favorire la funzione renale
Si evitino funghi e asparagi e si limitino ananas kiwi
salvia per la loro azione sulla coagulazione
NAUSEA ED EMESI GRAVIDICA
Dobbiamo ridurre i carboidrati evitare dolci e liquidi limitare le proteine
Nella dieta sono utili
verdure amare
limone
zenzero
aceto
Per stabilizzare lambiente gastrico bisogna alcalinizzarlo
Migliorare la funzione epatica evitando fritti limitando gli ortaggi gialli
(carotenoidi) e le crucifere (per lo zolfo)
dare carboidrati facili senza glutine
coleretici e colagoghi tipo zucchine marinate con aglio menta e aceto
fragole kiwi papaya (aiuta a digerire ed egrave drenante ricca di K) e avocado
LA MINACCIA DABORTO
Dobbiamo fornire lorganismo di
Magnesio fonti sono germe di grano fagioli ceci cereali integrali riso
avena banane kiwi uva mais
Antiossidanti antinfiammatori ottenere lequilibrio glicemico omega 3 e
fibre Possiamo consigliare olio di semi di lino noci e frutta fresca uova
tonno e pesce spada Per lacido lipoico patate broccoli spinaci fegato
cuore carni rosse
ALIMENTAZIONE ED AMNIOCENTESI
evitare le contrazioni con alimenti ricchi di Mg e K riso patate
fagiolini zucchine banane
favorire la funzione epatica in senso procoagulante uova fegato
pomodori fragole peperonicarote zucca soiabrassicacee e
formaggio fuso
evitare le infezioni aglio zenzero cipolla prezzemolo chiodi di
garofano limone per la loro funzione immunostimolante
PREVENZIONE DELLE INFEZIONI GRAVIDICHE
Ligiene degli alimenti egrave fondamentale per la
prevenzione della toxoplasmosi
Bisogna mantenere un buon equilibrio glicemico e
seguire una dieta ricca di fibre e di antiossidanti quali
cipolla olio di oliva curcuma mirtilli riso integrale
frutta secca zenzero e aglio
IMPORTANZA DELLA COTTURA DEI
CIBI PER OTTENERE IL MIGLIOR
RISULTATO SOTTO IL PROFILO DELLA
DIGERIBILITA E DELLA QUALITA
PREVENZIONE DELLA GESTOSI
Consigliabile introdurre con la dieta pochi zuccheri molte
proteine (molto pesce e latte poche carni rosse) alimenti a
basso indice glicemico e verdure ricche di acqua come
fragole patate cipolle e cicoria
Per diminuire le resistenze vascolari e i grassi circolanti egrave
utile assumere prezzemolo ananas finocchio cipolla melone
aglio e fragole
Per migliorare la funzione cuore-reni sono utili legumi frutta
secca miele cereali integrali rucola vongole e uova
Iodine deficiency in pregnant women living in the South East
of the UK the influence of diet and nutritional supplements
on iodine status Bath SC Walter A Taylor A Wright J Rayman MP Author information
Iodine is a key component of the thyroid hormones which are crucial for brain development
Adequate intake of iodine in pregnancy is important as in utero deficiency may have lifelong
consequences for the offspring Data on the iodine status of UK pregnant women are sparse
and there are no such data for pregnant women in the South East of the UK A total of 100
pregnant women were recruited to a cross-sectional study carried out at the Royal Surrey
County Hospital Guildford at their first-trimester visit for an ultrasound scan The participants
provided a spot-urine sample (for the measurement of urinary iodine concentration (UIC) and
creatinine concentration) and 24 h iodine excretion was estimated from the urinary
iodinecreatinine ratio Women completed a general questionnaire and a FFQ The median UIC
(85middot3 μgl) indicated that the group was iodine deficient by World Health Organisation criteria
The median values of the iodinecreatinine ratio (122middot9 μgg) and of the estimated 24 h iodine
excretion (151middot2 μgd) were also suggestive of iodine deficiency UIC was significantly higher in
women taking an iodine-containing prenatal supplement (n 42) than in those not taking such a
supplement (Plt 0middot001) In the adjusted analyses milk intake maternal age and iodine-
containing prenatal supplement use were positively associated with the estimated 24 h urinary
iodine excretion Our finding of iodine deficiency in these women gives cause for concern We
suggest that women of childbearing age and pregnant women should be given advice on how to
improve their iodine status through dietary means A national survey of iodine status in UK
pregnant women is required
Maternal and in utero determinants of type 2 diabetes risk in the
young Bruce KD Abstract
The global prevalence of diabetes mellitus has reached epidemic proportions In 2010 it was estimated
that 64 of the adult population (285 million) have diabetes In recent years the incidence of type 2
diabetes (T2D) a condition traditionally associated with aging has been steadily increasing among
younger individuals It is now a well-established notion that the early-life period is a critical window of
development and that influences during this period can developmentally prime the metabolic status of the
adult This review discusses the role of maternal and in utero influences on the developmental priming of
T2D risk Both human epidemiological studies and experimental animal models are beginning to
demonstrate that early dietary challenges can accelerate the onset of age-associated metabolic
disturbances including insulin resistance T2D obesity hypertension and cardiovascular disease These
findings show that poor maternal nutrition can prime a prediabetes phenotype often manifest as insulin
resistance by very early stages of life Thus the maternal diet is a critical determinant of premature T2D
risk While the mechanisms that link early nutrition to age-associated metabolic decline are currently
unclear preliminary findings suggest perturbations in a number of processes involved in cellular aging
such as changes in longevity-associated Sirtuin activity epigenetic regulation of key metabolic genes and
mitochondrial dysfunction Preliminary studies show that pharmacological interventions in utero and dietary
supplementation in early postnatal life may alleviate insulin resistance and reduce T2D risk However
further studies are warranted to fully understand the relationship between the early environment and long-
term effects on metabolism Such mechanistic insights will facilitate strategic interventions that prevent
accelerated metabolic decline and the premature onset of T2D in the current and future generations
Counteracting oxidative stress in pregnancy through modulation
of maternal micronutrients and omega-3 fatty acids DSouza V1 Chavan-Gautam P Joshi S Abstract
During pregnancy oxidative stress has been implicated in the pathophysiology of
preeclampsia and preterm birth leading to poor birth outcome Hyperhomocysteinemia
caused as a consequence of altered micronutrients like folic acid and vitamin B12 is
associated with increased production of reactive oxygen species that generate oxidative
stress These micronutrients are important determinants of methyl donor s-adenosyl
methionine while phospholipids are important methyl acceptors in the one-carbon
metabolic cycle A series of our studies in women during pregnancy have demonstrated
altered levels of these micronutrients and the negative association of docosahexaenoic
acid with homocysteine Various strategies to counteract oxidative stress
during pregnancy such as antioxidant therapy have been examined and found to be
inconsistent In this review we focus on the role of oxidative stress in pregnancy and
discuss the possibility of ameliorating it through modulation of maternal micronutrients
and omega 3 fatty acids especially docosahexaenoic acid We propose for the first time
that manipulation of one-carbon metabolism by maternal diet could be a potential
mechanism to counteract oxidative stress through homocysteine lowering effects and
help in reducing the risk for adverse pregnancyoutcomes
The influence of a low glycemic index dietary intervention on maternal
dietary intake glycemic index and gestational weight gain
during pregnancy a randomized controlled trial McGowan CA Walsh JM Byrne J Curran S McAuliffe FM1 Abstract
BACKGROUND Maternal diet is known to impact pregnancy outcome Following a low glycemic index (GI) diet during pregnancy has been shown
to improve maternal glycemia and reduce infant birthweight and may be associated with a higher fibre intake We assessed the
impact of a low GI dietary intervention on maternal GI nutritional intake and gestational weight gain (GWG) during pregnancy Compliance and acceptability of the low GIdiet was also examined METHOD Eight hundred women were randomised in early pregnancy to receive low GI and healthy eating dietary advice or to receive
standard maternity care The intervention group received dietary advice at a group education session before 22 weeks gestation
All women completed a 3 day food diary during each trimester of pregnancy Two hundred and thirty five women from the intervention arm and 285 women from the control arm returned complete 3x3d FDs and were included in the present analysis RESULTS Maternal GI was significantly reduced in the intervention group at trimester 2 and 3 The numbers of women within the lowest
quartile of GI increased from 37 in trimester 1 to 52 in trimester 3 (Pthinspltthinsp0001) among the intervention group The intervention
group had significantly lower energy intake (Pthinspltthinsp005) higher protein ( TE) (Pthinspltthinsp001) and higher dietary fibre intake (Pthinspltthinsp001)
post intervention Consumption of food groups with known high GI values were significantly reduced among the intervention group Women in the intervention low GI group were less likely to exceed the Institute of Medicines GWG goals CONCLUSION A dietary intervention in early pregnancy had a positive influence on maternal GI food and nutrient intakes and GWG Following
a low GI diet may be particularly beneficial for women at risk of exceeding the GWG goals for pregnancy

II TRIMESTRE
IN QUESTO PERIODO egrave MOLTO IMPORTANTE ATTIVARE LA
TIROIDE ATTRAVERSO LrsquoASSUNZIONE DI SELENIO
Componente delle selenoproteine ha effetti immunomodulatori e
svolge un ruolo chiave nel metabolismo degli ormoni tiroidei nella
famiglia delle deiodinasi Il suo deficit egrave responsabile del cretinismo
edematoso endemico
Fonti naturali di selenio sono le frattaglie pesce molluschi carne
latte lievito di birra pasta riso funghi noci
La seleneproteina detta GPx ( glutatione perossidasi) egrave un potente
regolatore della sintesi degli ormoni tiroidei e protegge dal danno
ossidativo
II TRIMESTRE
Tra le deiodinasi la D3 egrave particolarmente localizzate nelle cellule del
cervello fegato fetale placenta e pelle Protegge il concepito dalla
eccessiva esposizione agli ormoni tiroidei
Lipotiroidismo subclinico si associa a distacco di placenta parto
pretermine e aborto (Casey 2005) e al rischio di sviluppo nel post
partum di tiroidite autoimmune e di sviluppo cognitivo subottimale nella
prole (Papi e coll 2007) Dose giornaliera selenio egrave 60 microgrammi
Le richieste fetali impongono di introdurre con la dieta anche agenti
antiossidanti vit C vit E betacarotene
III TRIMESTRE
In questo periodo della gestazione il notevole
accrescimento ponderale fetale e le variazione in senso
procoagulatorio dei parametri ematici consigliano di
ridurre i carboidrati di aumentare le proteine di origine
vegetale e di favorire la funzione renale
Si evitino funghi e asparagi e si limitino ananas kiwi
salvia per la loro azione sulla coagulazione
NAUSEA ED EMESI GRAVIDICA
Dobbiamo ridurre i carboidrati evitare dolci e liquidi limitare le proteine
Nella dieta sono utili
verdure amare
limone
zenzero
aceto
Per stabilizzare lambiente gastrico bisogna alcalinizzarlo
Migliorare la funzione epatica evitando fritti limitando gli ortaggi gialli
(carotenoidi) e le crucifere (per lo zolfo)
dare carboidrati facili senza glutine
coleretici e colagoghi tipo zucchine marinate con aglio menta e aceto
fragole kiwi papaya (aiuta a digerire ed egrave drenante ricca di K) e avocado
LA MINACCIA DABORTO
Dobbiamo fornire lorganismo di
Magnesio fonti sono germe di grano fagioli ceci cereali integrali riso
avena banane kiwi uva mais
Antiossidanti antinfiammatori ottenere lequilibrio glicemico omega 3 e
fibre Possiamo consigliare olio di semi di lino noci e frutta fresca uova
tonno e pesce spada Per lacido lipoico patate broccoli spinaci fegato
cuore carni rosse
ALIMENTAZIONE ED AMNIOCENTESI
evitare le contrazioni con alimenti ricchi di Mg e K riso patate
fagiolini zucchine banane
favorire la funzione epatica in senso procoagulante uova fegato
pomodori fragole peperonicarote zucca soiabrassicacee e
formaggio fuso
evitare le infezioni aglio zenzero cipolla prezzemolo chiodi di
garofano limone per la loro funzione immunostimolante
PREVENZIONE DELLE INFEZIONI GRAVIDICHE
Ligiene degli alimenti egrave fondamentale per la
prevenzione della toxoplasmosi
Bisogna mantenere un buon equilibrio glicemico e
seguire una dieta ricca di fibre e di antiossidanti quali
cipolla olio di oliva curcuma mirtilli riso integrale
frutta secca zenzero e aglio
IMPORTANZA DELLA COTTURA DEI
CIBI PER OTTENERE IL MIGLIOR
RISULTATO SOTTO IL PROFILO DELLA
DIGERIBILITA E DELLA QUALITA
PREVENZIONE DELLA GESTOSI
Consigliabile introdurre con la dieta pochi zuccheri molte
proteine (molto pesce e latte poche carni rosse) alimenti a
basso indice glicemico e verdure ricche di acqua come
fragole patate cipolle e cicoria
Per diminuire le resistenze vascolari e i grassi circolanti egrave
utile assumere prezzemolo ananas finocchio cipolla melone
aglio e fragole
Per migliorare la funzione cuore-reni sono utili legumi frutta
secca miele cereali integrali rucola vongole e uova
Iodine deficiency in pregnant women living in the South East
of the UK the influence of diet and nutritional supplements
on iodine status Bath SC Walter A Taylor A Wright J Rayman MP Author information
Iodine is a key component of the thyroid hormones which are crucial for brain development
Adequate intake of iodine in pregnancy is important as in utero deficiency may have lifelong
consequences for the offspring Data on the iodine status of UK pregnant women are sparse
and there are no such data for pregnant women in the South East of the UK A total of 100
pregnant women were recruited to a cross-sectional study carried out at the Royal Surrey
County Hospital Guildford at their first-trimester visit for an ultrasound scan The participants
provided a spot-urine sample (for the measurement of urinary iodine concentration (UIC) and
creatinine concentration) and 24 h iodine excretion was estimated from the urinary
iodinecreatinine ratio Women completed a general questionnaire and a FFQ The median UIC
(85middot3 μgl) indicated that the group was iodine deficient by World Health Organisation criteria
The median values of the iodinecreatinine ratio (122middot9 μgg) and of the estimated 24 h iodine
excretion (151middot2 μgd) were also suggestive of iodine deficiency UIC was significantly higher in
women taking an iodine-containing prenatal supplement (n 42) than in those not taking such a
supplement (Plt 0middot001) In the adjusted analyses milk intake maternal age and iodine-
containing prenatal supplement use were positively associated with the estimated 24 h urinary
iodine excretion Our finding of iodine deficiency in these women gives cause for concern We
suggest that women of childbearing age and pregnant women should be given advice on how to
improve their iodine status through dietary means A national survey of iodine status in UK
pregnant women is required
Maternal and in utero determinants of type 2 diabetes risk in the
young Bruce KD Abstract
The global prevalence of diabetes mellitus has reached epidemic proportions In 2010 it was estimated
that 64 of the adult population (285 million) have diabetes In recent years the incidence of type 2
diabetes (T2D) a condition traditionally associated with aging has been steadily increasing among
younger individuals It is now a well-established notion that the early-life period is a critical window of
development and that influences during this period can developmentally prime the metabolic status of the
adult This review discusses the role of maternal and in utero influences on the developmental priming of
T2D risk Both human epidemiological studies and experimental animal models are beginning to
demonstrate that early dietary challenges can accelerate the onset of age-associated metabolic
disturbances including insulin resistance T2D obesity hypertension and cardiovascular disease These
findings show that poor maternal nutrition can prime a prediabetes phenotype often manifest as insulin
resistance by very early stages of life Thus the maternal diet is a critical determinant of premature T2D
risk While the mechanisms that link early nutrition to age-associated metabolic decline are currently
unclear preliminary findings suggest perturbations in a number of processes involved in cellular aging
such as changes in longevity-associated Sirtuin activity epigenetic regulation of key metabolic genes and
mitochondrial dysfunction Preliminary studies show that pharmacological interventions in utero and dietary
supplementation in early postnatal life may alleviate insulin resistance and reduce T2D risk However
further studies are warranted to fully understand the relationship between the early environment and long-
term effects on metabolism Such mechanistic insights will facilitate strategic interventions that prevent
accelerated metabolic decline and the premature onset of T2D in the current and future generations
Counteracting oxidative stress in pregnancy through modulation
of maternal micronutrients and omega-3 fatty acids DSouza V1 Chavan-Gautam P Joshi S Abstract
During pregnancy oxidative stress has been implicated in the pathophysiology of
preeclampsia and preterm birth leading to poor birth outcome Hyperhomocysteinemia
caused as a consequence of altered micronutrients like folic acid and vitamin B12 is
associated with increased production of reactive oxygen species that generate oxidative
stress These micronutrients are important determinants of methyl donor s-adenosyl
methionine while phospholipids are important methyl acceptors in the one-carbon
metabolic cycle A series of our studies in women during pregnancy have demonstrated
altered levels of these micronutrients and the negative association of docosahexaenoic
acid with homocysteine Various strategies to counteract oxidative stress
during pregnancy such as antioxidant therapy have been examined and found to be
inconsistent In this review we focus on the role of oxidative stress in pregnancy and
discuss the possibility of ameliorating it through modulation of maternal micronutrients
and omega 3 fatty acids especially docosahexaenoic acid We propose for the first time
that manipulation of one-carbon metabolism by maternal diet could be a potential
mechanism to counteract oxidative stress through homocysteine lowering effects and
help in reducing the risk for adverse pregnancyoutcomes
The influence of a low glycemic index dietary intervention on maternal
dietary intake glycemic index and gestational weight gain
during pregnancy a randomized controlled trial McGowan CA Walsh JM Byrne J Curran S McAuliffe FM1 Abstract
BACKGROUND Maternal diet is known to impact pregnancy outcome Following a low glycemic index (GI) diet during pregnancy has been shown
to improve maternal glycemia and reduce infant birthweight and may be associated with a higher fibre intake We assessed the
impact of a low GI dietary intervention on maternal GI nutritional intake and gestational weight gain (GWG) during pregnancy Compliance and acceptability of the low GIdiet was also examined METHOD Eight hundred women were randomised in early pregnancy to receive low GI and healthy eating dietary advice or to receive
standard maternity care The intervention group received dietary advice at a group education session before 22 weeks gestation
All women completed a 3 day food diary during each trimester of pregnancy Two hundred and thirty five women from the intervention arm and 285 women from the control arm returned complete 3x3d FDs and were included in the present analysis RESULTS Maternal GI was significantly reduced in the intervention group at trimester 2 and 3 The numbers of women within the lowest
quartile of GI increased from 37 in trimester 1 to 52 in trimester 3 (Pthinspltthinsp0001) among the intervention group The intervention
group had significantly lower energy intake (Pthinspltthinsp005) higher protein ( TE) (Pthinspltthinsp001) and higher dietary fibre intake (Pthinspltthinsp001)
post intervention Consumption of food groups with known high GI values were significantly reduced among the intervention group Women in the intervention low GI group were less likely to exceed the Institute of Medicines GWG goals CONCLUSION A dietary intervention in early pregnancy had a positive influence on maternal GI food and nutrient intakes and GWG Following
a low GI diet may be particularly beneficial for women at risk of exceeding the GWG goals for pregnancy

II TRIMESTRE
Tra le deiodinasi la D3 egrave particolarmente localizzate nelle cellule del
cervello fegato fetale placenta e pelle Protegge il concepito dalla
eccessiva esposizione agli ormoni tiroidei
Lipotiroidismo subclinico si associa a distacco di placenta parto
pretermine e aborto (Casey 2005) e al rischio di sviluppo nel post
partum di tiroidite autoimmune e di sviluppo cognitivo subottimale nella
prole (Papi e coll 2007) Dose giornaliera selenio egrave 60 microgrammi
Le richieste fetali impongono di introdurre con la dieta anche agenti
antiossidanti vit C vit E betacarotene
III TRIMESTRE
In questo periodo della gestazione il notevole
accrescimento ponderale fetale e le variazione in senso
procoagulatorio dei parametri ematici consigliano di
ridurre i carboidrati di aumentare le proteine di origine
vegetale e di favorire la funzione renale
Si evitino funghi e asparagi e si limitino ananas kiwi
salvia per la loro azione sulla coagulazione
NAUSEA ED EMESI GRAVIDICA
Dobbiamo ridurre i carboidrati evitare dolci e liquidi limitare le proteine
Nella dieta sono utili
verdure amare
limone
zenzero
aceto
Per stabilizzare lambiente gastrico bisogna alcalinizzarlo
Migliorare la funzione epatica evitando fritti limitando gli ortaggi gialli
(carotenoidi) e le crucifere (per lo zolfo)
dare carboidrati facili senza glutine
coleretici e colagoghi tipo zucchine marinate con aglio menta e aceto
fragole kiwi papaya (aiuta a digerire ed egrave drenante ricca di K) e avocado
LA MINACCIA DABORTO
Dobbiamo fornire lorganismo di
Magnesio fonti sono germe di grano fagioli ceci cereali integrali riso
avena banane kiwi uva mais
Antiossidanti antinfiammatori ottenere lequilibrio glicemico omega 3 e
fibre Possiamo consigliare olio di semi di lino noci e frutta fresca uova
tonno e pesce spada Per lacido lipoico patate broccoli spinaci fegato
cuore carni rosse
ALIMENTAZIONE ED AMNIOCENTESI
evitare le contrazioni con alimenti ricchi di Mg e K riso patate
fagiolini zucchine banane
favorire la funzione epatica in senso procoagulante uova fegato
pomodori fragole peperonicarote zucca soiabrassicacee e
formaggio fuso
evitare le infezioni aglio zenzero cipolla prezzemolo chiodi di
garofano limone per la loro funzione immunostimolante
PREVENZIONE DELLE INFEZIONI GRAVIDICHE
Ligiene degli alimenti egrave fondamentale per la
prevenzione della toxoplasmosi
Bisogna mantenere un buon equilibrio glicemico e
seguire una dieta ricca di fibre e di antiossidanti quali
cipolla olio di oliva curcuma mirtilli riso integrale
frutta secca zenzero e aglio
IMPORTANZA DELLA COTTURA DEI
CIBI PER OTTENERE IL MIGLIOR
RISULTATO SOTTO IL PROFILO DELLA
DIGERIBILITA E DELLA QUALITA
PREVENZIONE DELLA GESTOSI
Consigliabile introdurre con la dieta pochi zuccheri molte
proteine (molto pesce e latte poche carni rosse) alimenti a
basso indice glicemico e verdure ricche di acqua come
fragole patate cipolle e cicoria
Per diminuire le resistenze vascolari e i grassi circolanti egrave
utile assumere prezzemolo ananas finocchio cipolla melone
aglio e fragole
Per migliorare la funzione cuore-reni sono utili legumi frutta
secca miele cereali integrali rucola vongole e uova
Iodine deficiency in pregnant women living in the South East
of the UK the influence of diet and nutritional supplements
on iodine status Bath SC Walter A Taylor A Wright J Rayman MP Author information
Iodine is a key component of the thyroid hormones which are crucial for brain development
Adequate intake of iodine in pregnancy is important as in utero deficiency may have lifelong
consequences for the offspring Data on the iodine status of UK pregnant women are sparse
and there are no such data for pregnant women in the South East of the UK A total of 100
pregnant women were recruited to a cross-sectional study carried out at the Royal Surrey
County Hospital Guildford at their first-trimester visit for an ultrasound scan The participants
provided a spot-urine sample (for the measurement of urinary iodine concentration (UIC) and
creatinine concentration) and 24 h iodine excretion was estimated from the urinary
iodinecreatinine ratio Women completed a general questionnaire and a FFQ The median UIC
(85middot3 μgl) indicated that the group was iodine deficient by World Health Organisation criteria
The median values of the iodinecreatinine ratio (122middot9 μgg) and of the estimated 24 h iodine
excretion (151middot2 μgd) were also suggestive of iodine deficiency UIC was significantly higher in
women taking an iodine-containing prenatal supplement (n 42) than in those not taking such a
supplement (Plt 0middot001) In the adjusted analyses milk intake maternal age and iodine-
containing prenatal supplement use were positively associated with the estimated 24 h urinary
iodine excretion Our finding of iodine deficiency in these women gives cause for concern We
suggest that women of childbearing age and pregnant women should be given advice on how to
improve their iodine status through dietary means A national survey of iodine status in UK
pregnant women is required
Maternal and in utero determinants of type 2 diabetes risk in the
young Bruce KD Abstract
The global prevalence of diabetes mellitus has reached epidemic proportions In 2010 it was estimated
that 64 of the adult population (285 million) have diabetes In recent years the incidence of type 2
diabetes (T2D) a condition traditionally associated with aging has been steadily increasing among
younger individuals It is now a well-established notion that the early-life period is a critical window of
development and that influences during this period can developmentally prime the metabolic status of the
adult This review discusses the role of maternal and in utero influences on the developmental priming of
T2D risk Both human epidemiological studies and experimental animal models are beginning to
demonstrate that early dietary challenges can accelerate the onset of age-associated metabolic
disturbances including insulin resistance T2D obesity hypertension and cardiovascular disease These
findings show that poor maternal nutrition can prime a prediabetes phenotype often manifest as insulin
resistance by very early stages of life Thus the maternal diet is a critical determinant of premature T2D
risk While the mechanisms that link early nutrition to age-associated metabolic decline are currently
unclear preliminary findings suggest perturbations in a number of processes involved in cellular aging
such as changes in longevity-associated Sirtuin activity epigenetic regulation of key metabolic genes and
mitochondrial dysfunction Preliminary studies show that pharmacological interventions in utero and dietary
supplementation in early postnatal life may alleviate insulin resistance and reduce T2D risk However
further studies are warranted to fully understand the relationship between the early environment and long-
term effects on metabolism Such mechanistic insights will facilitate strategic interventions that prevent
accelerated metabolic decline and the premature onset of T2D in the current and future generations
Counteracting oxidative stress in pregnancy through modulation
of maternal micronutrients and omega-3 fatty acids DSouza V1 Chavan-Gautam P Joshi S Abstract
During pregnancy oxidative stress has been implicated in the pathophysiology of
preeclampsia and preterm birth leading to poor birth outcome Hyperhomocysteinemia
caused as a consequence of altered micronutrients like folic acid and vitamin B12 is
associated with increased production of reactive oxygen species that generate oxidative
stress These micronutrients are important determinants of methyl donor s-adenosyl
methionine while phospholipids are important methyl acceptors in the one-carbon
metabolic cycle A series of our studies in women during pregnancy have demonstrated
altered levels of these micronutrients and the negative association of docosahexaenoic
acid with homocysteine Various strategies to counteract oxidative stress
during pregnancy such as antioxidant therapy have been examined and found to be
inconsistent In this review we focus on the role of oxidative stress in pregnancy and
discuss the possibility of ameliorating it through modulation of maternal micronutrients
and omega 3 fatty acids especially docosahexaenoic acid We propose for the first time
that manipulation of one-carbon metabolism by maternal diet could be a potential
mechanism to counteract oxidative stress through homocysteine lowering effects and
help in reducing the risk for adverse pregnancyoutcomes
The influence of a low glycemic index dietary intervention on maternal
dietary intake glycemic index and gestational weight gain
during pregnancy a randomized controlled trial McGowan CA Walsh JM Byrne J Curran S McAuliffe FM1 Abstract
BACKGROUND Maternal diet is known to impact pregnancy outcome Following a low glycemic index (GI) diet during pregnancy has been shown
to improve maternal glycemia and reduce infant birthweight and may be associated with a higher fibre intake We assessed the
impact of a low GI dietary intervention on maternal GI nutritional intake and gestational weight gain (GWG) during pregnancy Compliance and acceptability of the low GIdiet was also examined METHOD Eight hundred women were randomised in early pregnancy to receive low GI and healthy eating dietary advice or to receive
standard maternity care The intervention group received dietary advice at a group education session before 22 weeks gestation
All women completed a 3 day food diary during each trimester of pregnancy Two hundred and thirty five women from the intervention arm and 285 women from the control arm returned complete 3x3d FDs and were included in the present analysis RESULTS Maternal GI was significantly reduced in the intervention group at trimester 2 and 3 The numbers of women within the lowest
quartile of GI increased from 37 in trimester 1 to 52 in trimester 3 (Pthinspltthinsp0001) among the intervention group The intervention
group had significantly lower energy intake (Pthinspltthinsp005) higher protein ( TE) (Pthinspltthinsp001) and higher dietary fibre intake (Pthinspltthinsp001)
post intervention Consumption of food groups with known high GI values were significantly reduced among the intervention group Women in the intervention low GI group were less likely to exceed the Institute of Medicines GWG goals CONCLUSION A dietary intervention in early pregnancy had a positive influence on maternal GI food and nutrient intakes and GWG Following
a low GI diet may be particularly beneficial for women at risk of exceeding the GWG goals for pregnancy

III TRIMESTRE
In questo periodo della gestazione il notevole
accrescimento ponderale fetale e le variazione in senso
procoagulatorio dei parametri ematici consigliano di
ridurre i carboidrati di aumentare le proteine di origine
vegetale e di favorire la funzione renale
Si evitino funghi e asparagi e si limitino ananas kiwi
salvia per la loro azione sulla coagulazione
NAUSEA ED EMESI GRAVIDICA
Dobbiamo ridurre i carboidrati evitare dolci e liquidi limitare le proteine
Nella dieta sono utili
verdure amare
limone
zenzero
aceto
Per stabilizzare lambiente gastrico bisogna alcalinizzarlo
Migliorare la funzione epatica evitando fritti limitando gli ortaggi gialli
(carotenoidi) e le crucifere (per lo zolfo)
dare carboidrati facili senza glutine
coleretici e colagoghi tipo zucchine marinate con aglio menta e aceto
fragole kiwi papaya (aiuta a digerire ed egrave drenante ricca di K) e avocado
LA MINACCIA DABORTO
Dobbiamo fornire lorganismo di
Magnesio fonti sono germe di grano fagioli ceci cereali integrali riso
avena banane kiwi uva mais
Antiossidanti antinfiammatori ottenere lequilibrio glicemico omega 3 e
fibre Possiamo consigliare olio di semi di lino noci e frutta fresca uova
tonno e pesce spada Per lacido lipoico patate broccoli spinaci fegato
cuore carni rosse
ALIMENTAZIONE ED AMNIOCENTESI
evitare le contrazioni con alimenti ricchi di Mg e K riso patate
fagiolini zucchine banane
favorire la funzione epatica in senso procoagulante uova fegato
pomodori fragole peperonicarote zucca soiabrassicacee e
formaggio fuso
evitare le infezioni aglio zenzero cipolla prezzemolo chiodi di
garofano limone per la loro funzione immunostimolante
PREVENZIONE DELLE INFEZIONI GRAVIDICHE
Ligiene degli alimenti egrave fondamentale per la
prevenzione della toxoplasmosi
Bisogna mantenere un buon equilibrio glicemico e
seguire una dieta ricca di fibre e di antiossidanti quali
cipolla olio di oliva curcuma mirtilli riso integrale
frutta secca zenzero e aglio
IMPORTANZA DELLA COTTURA DEI
CIBI PER OTTENERE IL MIGLIOR
RISULTATO SOTTO IL PROFILO DELLA
DIGERIBILITA E DELLA QUALITA
PREVENZIONE DELLA GESTOSI
Consigliabile introdurre con la dieta pochi zuccheri molte
proteine (molto pesce e latte poche carni rosse) alimenti a
basso indice glicemico e verdure ricche di acqua come
fragole patate cipolle e cicoria
Per diminuire le resistenze vascolari e i grassi circolanti egrave
utile assumere prezzemolo ananas finocchio cipolla melone
aglio e fragole
Per migliorare la funzione cuore-reni sono utili legumi frutta
secca miele cereali integrali rucola vongole e uova
Iodine deficiency in pregnant women living in the South East
of the UK the influence of diet and nutritional supplements
on iodine status Bath SC Walter A Taylor A Wright J Rayman MP Author information
Iodine is a key component of the thyroid hormones which are crucial for brain development
Adequate intake of iodine in pregnancy is important as in utero deficiency may have lifelong
consequences for the offspring Data on the iodine status of UK pregnant women are sparse
and there are no such data for pregnant women in the South East of the UK A total of 100
pregnant women were recruited to a cross-sectional study carried out at the Royal Surrey
County Hospital Guildford at their first-trimester visit for an ultrasound scan The participants
provided a spot-urine sample (for the measurement of urinary iodine concentration (UIC) and
creatinine concentration) and 24 h iodine excretion was estimated from the urinary
iodinecreatinine ratio Women completed a general questionnaire and a FFQ The median UIC
(85middot3 μgl) indicated that the group was iodine deficient by World Health Organisation criteria
The median values of the iodinecreatinine ratio (122middot9 μgg) and of the estimated 24 h iodine
excretion (151middot2 μgd) were also suggestive of iodine deficiency UIC was significantly higher in
women taking an iodine-containing prenatal supplement (n 42) than in those not taking such a
supplement (Plt 0middot001) In the adjusted analyses milk intake maternal age and iodine-
containing prenatal supplement use were positively associated with the estimated 24 h urinary
iodine excretion Our finding of iodine deficiency in these women gives cause for concern We
suggest that women of childbearing age and pregnant women should be given advice on how to
improve their iodine status through dietary means A national survey of iodine status in UK
pregnant women is required
Maternal and in utero determinants of type 2 diabetes risk in the
young Bruce KD Abstract
The global prevalence of diabetes mellitus has reached epidemic proportions In 2010 it was estimated
that 64 of the adult population (285 million) have diabetes In recent years the incidence of type 2
diabetes (T2D) a condition traditionally associated with aging has been steadily increasing among
younger individuals It is now a well-established notion that the early-life period is a critical window of
development and that influences during this period can developmentally prime the metabolic status of the
adult This review discusses the role of maternal and in utero influences on the developmental priming of
T2D risk Both human epidemiological studies and experimental animal models are beginning to
demonstrate that early dietary challenges can accelerate the onset of age-associated metabolic
disturbances including insulin resistance T2D obesity hypertension and cardiovascular disease These
findings show that poor maternal nutrition can prime a prediabetes phenotype often manifest as insulin
resistance by very early stages of life Thus the maternal diet is a critical determinant of premature T2D
risk While the mechanisms that link early nutrition to age-associated metabolic decline are currently
unclear preliminary findings suggest perturbations in a number of processes involved in cellular aging
such as changes in longevity-associated Sirtuin activity epigenetic regulation of key metabolic genes and
mitochondrial dysfunction Preliminary studies show that pharmacological interventions in utero and dietary
supplementation in early postnatal life may alleviate insulin resistance and reduce T2D risk However
further studies are warranted to fully understand the relationship between the early environment and long-
term effects on metabolism Such mechanistic insights will facilitate strategic interventions that prevent
accelerated metabolic decline and the premature onset of T2D in the current and future generations
Counteracting oxidative stress in pregnancy through modulation
of maternal micronutrients and omega-3 fatty acids DSouza V1 Chavan-Gautam P Joshi S Abstract
During pregnancy oxidative stress has been implicated in the pathophysiology of
preeclampsia and preterm birth leading to poor birth outcome Hyperhomocysteinemia
caused as a consequence of altered micronutrients like folic acid and vitamin B12 is
associated with increased production of reactive oxygen species that generate oxidative
stress These micronutrients are important determinants of methyl donor s-adenosyl
methionine while phospholipids are important methyl acceptors in the one-carbon
metabolic cycle A series of our studies in women during pregnancy have demonstrated
altered levels of these micronutrients and the negative association of docosahexaenoic
acid with homocysteine Various strategies to counteract oxidative stress
during pregnancy such as antioxidant therapy have been examined and found to be
inconsistent In this review we focus on the role of oxidative stress in pregnancy and
discuss the possibility of ameliorating it through modulation of maternal micronutrients
and omega 3 fatty acids especially docosahexaenoic acid We propose for the first time
that manipulation of one-carbon metabolism by maternal diet could be a potential
mechanism to counteract oxidative stress through homocysteine lowering effects and
help in reducing the risk for adverse pregnancyoutcomes
The influence of a low glycemic index dietary intervention on maternal
dietary intake glycemic index and gestational weight gain
during pregnancy a randomized controlled trial McGowan CA Walsh JM Byrne J Curran S McAuliffe FM1 Abstract
BACKGROUND Maternal diet is known to impact pregnancy outcome Following a low glycemic index (GI) diet during pregnancy has been shown
to improve maternal glycemia and reduce infant birthweight and may be associated with a higher fibre intake We assessed the
impact of a low GI dietary intervention on maternal GI nutritional intake and gestational weight gain (GWG) during pregnancy Compliance and acceptability of the low GIdiet was also examined METHOD Eight hundred women were randomised in early pregnancy to receive low GI and healthy eating dietary advice or to receive
standard maternity care The intervention group received dietary advice at a group education session before 22 weeks gestation
All women completed a 3 day food diary during each trimester of pregnancy Two hundred and thirty five women from the intervention arm and 285 women from the control arm returned complete 3x3d FDs and were included in the present analysis RESULTS Maternal GI was significantly reduced in the intervention group at trimester 2 and 3 The numbers of women within the lowest
quartile of GI increased from 37 in trimester 1 to 52 in trimester 3 (Pthinspltthinsp0001) among the intervention group The intervention
group had significantly lower energy intake (Pthinspltthinsp005) higher protein ( TE) (Pthinspltthinsp001) and higher dietary fibre intake (Pthinspltthinsp001)
post intervention Consumption of food groups with known high GI values were significantly reduced among the intervention group Women in the intervention low GI group were less likely to exceed the Institute of Medicines GWG goals CONCLUSION A dietary intervention in early pregnancy had a positive influence on maternal GI food and nutrient intakes and GWG Following
a low GI diet may be particularly beneficial for women at risk of exceeding the GWG goals for pregnancy
NAUSEA ED EMESI GRAVIDICA
Dobbiamo ridurre i carboidrati evitare dolci e liquidi limitare le proteine
Nella dieta sono utili
verdure amare
limone
zenzero
aceto
Per stabilizzare lambiente gastrico bisogna alcalinizzarlo
Migliorare la funzione epatica evitando fritti limitando gli ortaggi gialli
(carotenoidi) e le crucifere (per lo zolfo)
dare carboidrati facili senza glutine
coleretici e colagoghi tipo zucchine marinate con aglio menta e aceto
fragole kiwi papaya (aiuta a digerire ed egrave drenante ricca di K) e avocado
LA MINACCIA DABORTO
Dobbiamo fornire lorganismo di
Magnesio fonti sono germe di grano fagioli ceci cereali integrali riso
avena banane kiwi uva mais
Antiossidanti antinfiammatori ottenere lequilibrio glicemico omega 3 e
fibre Possiamo consigliare olio di semi di lino noci e frutta fresca uova
tonno e pesce spada Per lacido lipoico patate broccoli spinaci fegato
cuore carni rosse
ALIMENTAZIONE ED AMNIOCENTESI
evitare le contrazioni con alimenti ricchi di Mg e K riso patate
fagiolini zucchine banane
favorire la funzione epatica in senso procoagulante uova fegato
pomodori fragole peperonicarote zucca soiabrassicacee e
formaggio fuso
evitare le infezioni aglio zenzero cipolla prezzemolo chiodi di
garofano limone per la loro funzione immunostimolante
PREVENZIONE DELLE INFEZIONI GRAVIDICHE
Ligiene degli alimenti egrave fondamentale per la
prevenzione della toxoplasmosi
Bisogna mantenere un buon equilibrio glicemico e
seguire una dieta ricca di fibre e di antiossidanti quali
cipolla olio di oliva curcuma mirtilli riso integrale
frutta secca zenzero e aglio
IMPORTANZA DELLA COTTURA DEI
CIBI PER OTTENERE IL MIGLIOR
RISULTATO SOTTO IL PROFILO DELLA
DIGERIBILITA E DELLA QUALITA
PREVENZIONE DELLA GESTOSI
Consigliabile introdurre con la dieta pochi zuccheri molte
proteine (molto pesce e latte poche carni rosse) alimenti a
basso indice glicemico e verdure ricche di acqua come
fragole patate cipolle e cicoria
Per diminuire le resistenze vascolari e i grassi circolanti egrave
utile assumere prezzemolo ananas finocchio cipolla melone
aglio e fragole
Per migliorare la funzione cuore-reni sono utili legumi frutta
secca miele cereali integrali rucola vongole e uova
Iodine deficiency in pregnant women living in the South East
of the UK the influence of diet and nutritional supplements
on iodine status Bath SC Walter A Taylor A Wright J Rayman MP Author information
Iodine is a key component of the thyroid hormones which are crucial for brain development
Adequate intake of iodine in pregnancy is important as in utero deficiency may have lifelong
consequences for the offspring Data on the iodine status of UK pregnant women are sparse
and there are no such data for pregnant women in the South East of the UK A total of 100
pregnant women were recruited to a cross-sectional study carried out at the Royal Surrey
County Hospital Guildford at their first-trimester visit for an ultrasound scan The participants
provided a spot-urine sample (for the measurement of urinary iodine concentration (UIC) and
creatinine concentration) and 24 h iodine excretion was estimated from the urinary
iodinecreatinine ratio Women completed a general questionnaire and a FFQ The median UIC
(85middot3 μgl) indicated that the group was iodine deficient by World Health Organisation criteria
The median values of the iodinecreatinine ratio (122middot9 μgg) and of the estimated 24 h iodine
excretion (151middot2 μgd) were also suggestive of iodine deficiency UIC was significantly higher in
women taking an iodine-containing prenatal supplement (n 42) than in those not taking such a
supplement (Plt 0middot001) In the adjusted analyses milk intake maternal age and iodine-
containing prenatal supplement use were positively associated with the estimated 24 h urinary
iodine excretion Our finding of iodine deficiency in these women gives cause for concern We
suggest that women of childbearing age and pregnant women should be given advice on how to
improve their iodine status through dietary means A national survey of iodine status in UK
pregnant women is required
Maternal and in utero determinants of type 2 diabetes risk in the
young Bruce KD Abstract
The global prevalence of diabetes mellitus has reached epidemic proportions In 2010 it was estimated
that 64 of the adult population (285 million) have diabetes In recent years the incidence of type 2
diabetes (T2D) a condition traditionally associated with aging has been steadily increasing among
younger individuals It is now a well-established notion that the early-life period is a critical window of
development and that influences during this period can developmentally prime the metabolic status of the
adult This review discusses the role of maternal and in utero influences on the developmental priming of
T2D risk Both human epidemiological studies and experimental animal models are beginning to
demonstrate that early dietary challenges can accelerate the onset of age-associated metabolic
disturbances including insulin resistance T2D obesity hypertension and cardiovascular disease These
findings show that poor maternal nutrition can prime a prediabetes phenotype often manifest as insulin
resistance by very early stages of life Thus the maternal diet is a critical determinant of premature T2D
risk While the mechanisms that link early nutrition to age-associated metabolic decline are currently
unclear preliminary findings suggest perturbations in a number of processes involved in cellular aging
such as changes in longevity-associated Sirtuin activity epigenetic regulation of key metabolic genes and
mitochondrial dysfunction Preliminary studies show that pharmacological interventions in utero and dietary
supplementation in early postnatal life may alleviate insulin resistance and reduce T2D risk However
further studies are warranted to fully understand the relationship between the early environment and long-
term effects on metabolism Such mechanistic insights will facilitate strategic interventions that prevent
accelerated metabolic decline and the premature onset of T2D in the current and future generations
Counteracting oxidative stress in pregnancy through modulation
of maternal micronutrients and omega-3 fatty acids DSouza V1 Chavan-Gautam P Joshi S Abstract
During pregnancy oxidative stress has been implicated in the pathophysiology of
preeclampsia and preterm birth leading to poor birth outcome Hyperhomocysteinemia
caused as a consequence of altered micronutrients like folic acid and vitamin B12 is
associated with increased production of reactive oxygen species that generate oxidative
stress These micronutrients are important determinants of methyl donor s-adenosyl
methionine while phospholipids are important methyl acceptors in the one-carbon
metabolic cycle A series of our studies in women during pregnancy have demonstrated
altered levels of these micronutrients and the negative association of docosahexaenoic
acid with homocysteine Various strategies to counteract oxidative stress
during pregnancy such as antioxidant therapy have been examined and found to be
inconsistent In this review we focus on the role of oxidative stress in pregnancy and
discuss the possibility of ameliorating it through modulation of maternal micronutrients
and omega 3 fatty acids especially docosahexaenoic acid We propose for the first time
that manipulation of one-carbon metabolism by maternal diet could be a potential
mechanism to counteract oxidative stress through homocysteine lowering effects and
help in reducing the risk for adverse pregnancyoutcomes
The influence of a low glycemic index dietary intervention on maternal
dietary intake glycemic index and gestational weight gain
during pregnancy a randomized controlled trial McGowan CA Walsh JM Byrne J Curran S McAuliffe FM1 Abstract
BACKGROUND Maternal diet is known to impact pregnancy outcome Following a low glycemic index (GI) diet during pregnancy has been shown
to improve maternal glycemia and reduce infant birthweight and may be associated with a higher fibre intake We assessed the
impact of a low GI dietary intervention on maternal GI nutritional intake and gestational weight gain (GWG) during pregnancy Compliance and acceptability of the low GIdiet was also examined METHOD Eight hundred women were randomised in early pregnancy to receive low GI and healthy eating dietary advice or to receive
standard maternity care The intervention group received dietary advice at a group education session before 22 weeks gestation
All women completed a 3 day food diary during each trimester of pregnancy Two hundred and thirty five women from the intervention arm and 285 women from the control arm returned complete 3x3d FDs and were included in the present analysis RESULTS Maternal GI was significantly reduced in the intervention group at trimester 2 and 3 The numbers of women within the lowest
quartile of GI increased from 37 in trimester 1 to 52 in trimester 3 (Pthinspltthinsp0001) among the intervention group The intervention
group had significantly lower energy intake (Pthinspltthinsp005) higher protein ( TE) (Pthinspltthinsp001) and higher dietary fibre intake (Pthinspltthinsp001)
post intervention Consumption of food groups with known high GI values were significantly reduced among the intervention group Women in the intervention low GI group were less likely to exceed the Institute of Medicines GWG goals CONCLUSION A dietary intervention in early pregnancy had a positive influence on maternal GI food and nutrient intakes and GWG Following
a low GI diet may be particularly beneficial for women at risk of exceeding the GWG goals for pregnancy

LA MINACCIA DABORTO
Dobbiamo fornire lorganismo di
Magnesio fonti sono germe di grano fagioli ceci cereali integrali riso
avena banane kiwi uva mais
Antiossidanti antinfiammatori ottenere lequilibrio glicemico omega 3 e
fibre Possiamo consigliare olio di semi di lino noci e frutta fresca uova
tonno e pesce spada Per lacido lipoico patate broccoli spinaci fegato
cuore carni rosse
ALIMENTAZIONE ED AMNIOCENTESI
evitare le contrazioni con alimenti ricchi di Mg e K riso patate
fagiolini zucchine banane
favorire la funzione epatica in senso procoagulante uova fegato
pomodori fragole peperonicarote zucca soiabrassicacee e
formaggio fuso
evitare le infezioni aglio zenzero cipolla prezzemolo chiodi di
garofano limone per la loro funzione immunostimolante
PREVENZIONE DELLE INFEZIONI GRAVIDICHE
Ligiene degli alimenti egrave fondamentale per la
prevenzione della toxoplasmosi
Bisogna mantenere un buon equilibrio glicemico e
seguire una dieta ricca di fibre e di antiossidanti quali
cipolla olio di oliva curcuma mirtilli riso integrale
frutta secca zenzero e aglio
IMPORTANZA DELLA COTTURA DEI
CIBI PER OTTENERE IL MIGLIOR
RISULTATO SOTTO IL PROFILO DELLA
DIGERIBILITA E DELLA QUALITA
PREVENZIONE DELLA GESTOSI
Consigliabile introdurre con la dieta pochi zuccheri molte
proteine (molto pesce e latte poche carni rosse) alimenti a
basso indice glicemico e verdure ricche di acqua come
fragole patate cipolle e cicoria
Per diminuire le resistenze vascolari e i grassi circolanti egrave
utile assumere prezzemolo ananas finocchio cipolla melone
aglio e fragole
Per migliorare la funzione cuore-reni sono utili legumi frutta
secca miele cereali integrali rucola vongole e uova
Iodine deficiency in pregnant women living in the South East
of the UK the influence of diet and nutritional supplements
on iodine status Bath SC Walter A Taylor A Wright J Rayman MP Author information
Iodine is a key component of the thyroid hormones which are crucial for brain development
Adequate intake of iodine in pregnancy is important as in utero deficiency may have lifelong
consequences for the offspring Data on the iodine status of UK pregnant women are sparse
and there are no such data for pregnant women in the South East of the UK A total of 100
pregnant women were recruited to a cross-sectional study carried out at the Royal Surrey
County Hospital Guildford at their first-trimester visit for an ultrasound scan The participants
provided a spot-urine sample (for the measurement of urinary iodine concentration (UIC) and
creatinine concentration) and 24 h iodine excretion was estimated from the urinary
iodinecreatinine ratio Women completed a general questionnaire and a FFQ The median UIC
(85middot3 μgl) indicated that the group was iodine deficient by World Health Organisation criteria
The median values of the iodinecreatinine ratio (122middot9 μgg) and of the estimated 24 h iodine
excretion (151middot2 μgd) were also suggestive of iodine deficiency UIC was significantly higher in
women taking an iodine-containing prenatal supplement (n 42) than in those not taking such a
supplement (Plt 0middot001) In the adjusted analyses milk intake maternal age and iodine-
containing prenatal supplement use were positively associated with the estimated 24 h urinary
iodine excretion Our finding of iodine deficiency in these women gives cause for concern We
suggest that women of childbearing age and pregnant women should be given advice on how to
improve their iodine status through dietary means A national survey of iodine status in UK
pregnant women is required
Maternal and in utero determinants of type 2 diabetes risk in the
young Bruce KD Abstract
The global prevalence of diabetes mellitus has reached epidemic proportions In 2010 it was estimated
that 64 of the adult population (285 million) have diabetes In recent years the incidence of type 2
diabetes (T2D) a condition traditionally associated with aging has been steadily increasing among
younger individuals It is now a well-established notion that the early-life period is a critical window of
development and that influences during this period can developmentally prime the metabolic status of the
adult This review discusses the role of maternal and in utero influences on the developmental priming of
T2D risk Both human epidemiological studies and experimental animal models are beginning to
demonstrate that early dietary challenges can accelerate the onset of age-associated metabolic
disturbances including insulin resistance T2D obesity hypertension and cardiovascular disease These
findings show that poor maternal nutrition can prime a prediabetes phenotype often manifest as insulin
resistance by very early stages of life Thus the maternal diet is a critical determinant of premature T2D
risk While the mechanisms that link early nutrition to age-associated metabolic decline are currently
unclear preliminary findings suggest perturbations in a number of processes involved in cellular aging
such as changes in longevity-associated Sirtuin activity epigenetic regulation of key metabolic genes and
mitochondrial dysfunction Preliminary studies show that pharmacological interventions in utero and dietary
supplementation in early postnatal life may alleviate insulin resistance and reduce T2D risk However
further studies are warranted to fully understand the relationship between the early environment and long-
term effects on metabolism Such mechanistic insights will facilitate strategic interventions that prevent
accelerated metabolic decline and the premature onset of T2D in the current and future generations
Counteracting oxidative stress in pregnancy through modulation
of maternal micronutrients and omega-3 fatty acids DSouza V1 Chavan-Gautam P Joshi S Abstract
During pregnancy oxidative stress has been implicated in the pathophysiology of
preeclampsia and preterm birth leading to poor birth outcome Hyperhomocysteinemia
caused as a consequence of altered micronutrients like folic acid and vitamin B12 is
associated with increased production of reactive oxygen species that generate oxidative
stress These micronutrients are important determinants of methyl donor s-adenosyl
methionine while phospholipids are important methyl acceptors in the one-carbon
metabolic cycle A series of our studies in women during pregnancy have demonstrated
altered levels of these micronutrients and the negative association of docosahexaenoic
acid with homocysteine Various strategies to counteract oxidative stress
during pregnancy such as antioxidant therapy have been examined and found to be
inconsistent In this review we focus on the role of oxidative stress in pregnancy and
discuss the possibility of ameliorating it through modulation of maternal micronutrients
and omega 3 fatty acids especially docosahexaenoic acid We propose for the first time
that manipulation of one-carbon metabolism by maternal diet could be a potential
mechanism to counteract oxidative stress through homocysteine lowering effects and
help in reducing the risk for adverse pregnancyoutcomes
The influence of a low glycemic index dietary intervention on maternal
dietary intake glycemic index and gestational weight gain
during pregnancy a randomized controlled trial McGowan CA Walsh JM Byrne J Curran S McAuliffe FM1 Abstract
BACKGROUND Maternal diet is known to impact pregnancy outcome Following a low glycemic index (GI) diet during pregnancy has been shown
to improve maternal glycemia and reduce infant birthweight and may be associated with a higher fibre intake We assessed the
impact of a low GI dietary intervention on maternal GI nutritional intake and gestational weight gain (GWG) during pregnancy Compliance and acceptability of the low GIdiet was also examined METHOD Eight hundred women were randomised in early pregnancy to receive low GI and healthy eating dietary advice or to receive
standard maternity care The intervention group received dietary advice at a group education session before 22 weeks gestation
All women completed a 3 day food diary during each trimester of pregnancy Two hundred and thirty five women from the intervention arm and 285 women from the control arm returned complete 3x3d FDs and were included in the present analysis RESULTS Maternal GI was significantly reduced in the intervention group at trimester 2 and 3 The numbers of women within the lowest
quartile of GI increased from 37 in trimester 1 to 52 in trimester 3 (Pthinspltthinsp0001) among the intervention group The intervention
group had significantly lower energy intake (Pthinspltthinsp005) higher protein ( TE) (Pthinspltthinsp001) and higher dietary fibre intake (Pthinspltthinsp001)
post intervention Consumption of food groups with known high GI values were significantly reduced among the intervention group Women in the intervention low GI group were less likely to exceed the Institute of Medicines GWG goals CONCLUSION A dietary intervention in early pregnancy had a positive influence on maternal GI food and nutrient intakes and GWG Following
a low GI diet may be particularly beneficial for women at risk of exceeding the GWG goals for pregnancy

ALIMENTAZIONE ED AMNIOCENTESI
evitare le contrazioni con alimenti ricchi di Mg e K riso patate
fagiolini zucchine banane
favorire la funzione epatica in senso procoagulante uova fegato
pomodori fragole peperonicarote zucca soiabrassicacee e
formaggio fuso
evitare le infezioni aglio zenzero cipolla prezzemolo chiodi di
garofano limone per la loro funzione immunostimolante
PREVENZIONE DELLE INFEZIONI GRAVIDICHE
Ligiene degli alimenti egrave fondamentale per la
prevenzione della toxoplasmosi
Bisogna mantenere un buon equilibrio glicemico e
seguire una dieta ricca di fibre e di antiossidanti quali
cipolla olio di oliva curcuma mirtilli riso integrale
frutta secca zenzero e aglio
IMPORTANZA DELLA COTTURA DEI
CIBI PER OTTENERE IL MIGLIOR
RISULTATO SOTTO IL PROFILO DELLA
DIGERIBILITA E DELLA QUALITA
PREVENZIONE DELLA GESTOSI
Consigliabile introdurre con la dieta pochi zuccheri molte
proteine (molto pesce e latte poche carni rosse) alimenti a
basso indice glicemico e verdure ricche di acqua come
fragole patate cipolle e cicoria
Per diminuire le resistenze vascolari e i grassi circolanti egrave
utile assumere prezzemolo ananas finocchio cipolla melone
aglio e fragole
Per migliorare la funzione cuore-reni sono utili legumi frutta
secca miele cereali integrali rucola vongole e uova
Iodine deficiency in pregnant women living in the South East
of the UK the influence of diet and nutritional supplements
on iodine status Bath SC Walter A Taylor A Wright J Rayman MP Author information
Iodine is a key component of the thyroid hormones which are crucial for brain development
Adequate intake of iodine in pregnancy is important as in utero deficiency may have lifelong
consequences for the offspring Data on the iodine status of UK pregnant women are sparse
and there are no such data for pregnant women in the South East of the UK A total of 100
pregnant women were recruited to a cross-sectional study carried out at the Royal Surrey
County Hospital Guildford at their first-trimester visit for an ultrasound scan The participants
provided a spot-urine sample (for the measurement of urinary iodine concentration (UIC) and
creatinine concentration) and 24 h iodine excretion was estimated from the urinary
iodinecreatinine ratio Women completed a general questionnaire and a FFQ The median UIC
(85middot3 μgl) indicated that the group was iodine deficient by World Health Organisation criteria
The median values of the iodinecreatinine ratio (122middot9 μgg) and of the estimated 24 h iodine
excretion (151middot2 μgd) were also suggestive of iodine deficiency UIC was significantly higher in
women taking an iodine-containing prenatal supplement (n 42) than in those not taking such a
supplement (Plt 0middot001) In the adjusted analyses milk intake maternal age and iodine-
containing prenatal supplement use were positively associated with the estimated 24 h urinary
iodine excretion Our finding of iodine deficiency in these women gives cause for concern We
suggest that women of childbearing age and pregnant women should be given advice on how to
improve their iodine status through dietary means A national survey of iodine status in UK
pregnant women is required
Maternal and in utero determinants of type 2 diabetes risk in the
young Bruce KD Abstract
The global prevalence of diabetes mellitus has reached epidemic proportions In 2010 it was estimated
that 64 of the adult population (285 million) have diabetes In recent years the incidence of type 2
diabetes (T2D) a condition traditionally associated with aging has been steadily increasing among
younger individuals It is now a well-established notion that the early-life period is a critical window of
development and that influences during this period can developmentally prime the metabolic status of the
adult This review discusses the role of maternal and in utero influences on the developmental priming of
T2D risk Both human epidemiological studies and experimental animal models are beginning to
demonstrate that early dietary challenges can accelerate the onset of age-associated metabolic
disturbances including insulin resistance T2D obesity hypertension and cardiovascular disease These
findings show that poor maternal nutrition can prime a prediabetes phenotype often manifest as insulin
resistance by very early stages of life Thus the maternal diet is a critical determinant of premature T2D
risk While the mechanisms that link early nutrition to age-associated metabolic decline are currently
unclear preliminary findings suggest perturbations in a number of processes involved in cellular aging
such as changes in longevity-associated Sirtuin activity epigenetic regulation of key metabolic genes and
mitochondrial dysfunction Preliminary studies show that pharmacological interventions in utero and dietary
supplementation in early postnatal life may alleviate insulin resistance and reduce T2D risk However
further studies are warranted to fully understand the relationship between the early environment and long-
term effects on metabolism Such mechanistic insights will facilitate strategic interventions that prevent
accelerated metabolic decline and the premature onset of T2D in the current and future generations
Counteracting oxidative stress in pregnancy through modulation
of maternal micronutrients and omega-3 fatty acids DSouza V1 Chavan-Gautam P Joshi S Abstract
During pregnancy oxidative stress has been implicated in the pathophysiology of
preeclampsia and preterm birth leading to poor birth outcome Hyperhomocysteinemia
caused as a consequence of altered micronutrients like folic acid and vitamin B12 is
associated with increased production of reactive oxygen species that generate oxidative
stress These micronutrients are important determinants of methyl donor s-adenosyl
methionine while phospholipids are important methyl acceptors in the one-carbon
metabolic cycle A series of our studies in women during pregnancy have demonstrated
altered levels of these micronutrients and the negative association of docosahexaenoic
acid with homocysteine Various strategies to counteract oxidative stress
during pregnancy such as antioxidant therapy have been examined and found to be
inconsistent In this review we focus on the role of oxidative stress in pregnancy and
discuss the possibility of ameliorating it through modulation of maternal micronutrients
and omega 3 fatty acids especially docosahexaenoic acid We propose for the first time
that manipulation of one-carbon metabolism by maternal diet could be a potential
mechanism to counteract oxidative stress through homocysteine lowering effects and
help in reducing the risk for adverse pregnancyoutcomes
The influence of a low glycemic index dietary intervention on maternal
dietary intake glycemic index and gestational weight gain
during pregnancy a randomized controlled trial McGowan CA Walsh JM Byrne J Curran S McAuliffe FM1 Abstract
BACKGROUND Maternal diet is known to impact pregnancy outcome Following a low glycemic index (GI) diet during pregnancy has been shown
to improve maternal glycemia and reduce infant birthweight and may be associated with a higher fibre intake We assessed the
impact of a low GI dietary intervention on maternal GI nutritional intake and gestational weight gain (GWG) during pregnancy Compliance and acceptability of the low GIdiet was also examined METHOD Eight hundred women were randomised in early pregnancy to receive low GI and healthy eating dietary advice or to receive
standard maternity care The intervention group received dietary advice at a group education session before 22 weeks gestation
All women completed a 3 day food diary during each trimester of pregnancy Two hundred and thirty five women from the intervention arm and 285 women from the control arm returned complete 3x3d FDs and were included in the present analysis RESULTS Maternal GI was significantly reduced in the intervention group at trimester 2 and 3 The numbers of women within the lowest
quartile of GI increased from 37 in trimester 1 to 52 in trimester 3 (Pthinspltthinsp0001) among the intervention group The intervention
group had significantly lower energy intake (Pthinspltthinsp005) higher protein ( TE) (Pthinspltthinsp001) and higher dietary fibre intake (Pthinspltthinsp001)
post intervention Consumption of food groups with known high GI values were significantly reduced among the intervention group Women in the intervention low GI group were less likely to exceed the Institute of Medicines GWG goals CONCLUSION A dietary intervention in early pregnancy had a positive influence on maternal GI food and nutrient intakes and GWG Following
a low GI diet may be particularly beneficial for women at risk of exceeding the GWG goals for pregnancy
PREVENZIONE DELLE INFEZIONI GRAVIDICHE
Ligiene degli alimenti egrave fondamentale per la
prevenzione della toxoplasmosi
Bisogna mantenere un buon equilibrio glicemico e
seguire una dieta ricca di fibre e di antiossidanti quali
cipolla olio di oliva curcuma mirtilli riso integrale
frutta secca zenzero e aglio
IMPORTANZA DELLA COTTURA DEI
CIBI PER OTTENERE IL MIGLIOR
RISULTATO SOTTO IL PROFILO DELLA
DIGERIBILITA E DELLA QUALITA
PREVENZIONE DELLA GESTOSI
Consigliabile introdurre con la dieta pochi zuccheri molte
proteine (molto pesce e latte poche carni rosse) alimenti a
basso indice glicemico e verdure ricche di acqua come
fragole patate cipolle e cicoria
Per diminuire le resistenze vascolari e i grassi circolanti egrave
utile assumere prezzemolo ananas finocchio cipolla melone
aglio e fragole
Per migliorare la funzione cuore-reni sono utili legumi frutta
secca miele cereali integrali rucola vongole e uova
Iodine deficiency in pregnant women living in the South East
of the UK the influence of diet and nutritional supplements
on iodine status Bath SC Walter A Taylor A Wright J Rayman MP Author information
Iodine is a key component of the thyroid hormones which are crucial for brain development
Adequate intake of iodine in pregnancy is important as in utero deficiency may have lifelong
consequences for the offspring Data on the iodine status of UK pregnant women are sparse
and there are no such data for pregnant women in the South East of the UK A total of 100
pregnant women were recruited to a cross-sectional study carried out at the Royal Surrey
County Hospital Guildford at their first-trimester visit for an ultrasound scan The participants
provided a spot-urine sample (for the measurement of urinary iodine concentration (UIC) and
creatinine concentration) and 24 h iodine excretion was estimated from the urinary
iodinecreatinine ratio Women completed a general questionnaire and a FFQ The median UIC
(85middot3 μgl) indicated that the group was iodine deficient by World Health Organisation criteria
The median values of the iodinecreatinine ratio (122middot9 μgg) and of the estimated 24 h iodine
excretion (151middot2 μgd) were also suggestive of iodine deficiency UIC was significantly higher in
women taking an iodine-containing prenatal supplement (n 42) than in those not taking such a
supplement (Plt 0middot001) In the adjusted analyses milk intake maternal age and iodine-
containing prenatal supplement use were positively associated with the estimated 24 h urinary
iodine excretion Our finding of iodine deficiency in these women gives cause for concern We
suggest that women of childbearing age and pregnant women should be given advice on how to
improve their iodine status through dietary means A national survey of iodine status in UK
pregnant women is required
Maternal and in utero determinants of type 2 diabetes risk in the
young Bruce KD Abstract
The global prevalence of diabetes mellitus has reached epidemic proportions In 2010 it was estimated
that 64 of the adult population (285 million) have diabetes In recent years the incidence of type 2
diabetes (T2D) a condition traditionally associated with aging has been steadily increasing among
younger individuals It is now a well-established notion that the early-life period is a critical window of
development and that influences during this period can developmentally prime the metabolic status of the
adult This review discusses the role of maternal and in utero influences on the developmental priming of
T2D risk Both human epidemiological studies and experimental animal models are beginning to
demonstrate that early dietary challenges can accelerate the onset of age-associated metabolic
disturbances including insulin resistance T2D obesity hypertension and cardiovascular disease These
findings show that poor maternal nutrition can prime a prediabetes phenotype often manifest as insulin
resistance by very early stages of life Thus the maternal diet is a critical determinant of premature T2D
risk While the mechanisms that link early nutrition to age-associated metabolic decline are currently
unclear preliminary findings suggest perturbations in a number of processes involved in cellular aging
such as changes in longevity-associated Sirtuin activity epigenetic regulation of key metabolic genes and
mitochondrial dysfunction Preliminary studies show that pharmacological interventions in utero and dietary
supplementation in early postnatal life may alleviate insulin resistance and reduce T2D risk However
further studies are warranted to fully understand the relationship between the early environment and long-
term effects on metabolism Such mechanistic insights will facilitate strategic interventions that prevent
accelerated metabolic decline and the premature onset of T2D in the current and future generations
Counteracting oxidative stress in pregnancy through modulation
of maternal micronutrients and omega-3 fatty acids DSouza V1 Chavan-Gautam P Joshi S Abstract
During pregnancy oxidative stress has been implicated in the pathophysiology of
preeclampsia and preterm birth leading to poor birth outcome Hyperhomocysteinemia
caused as a consequence of altered micronutrients like folic acid and vitamin B12 is
associated with increased production of reactive oxygen species that generate oxidative
stress These micronutrients are important determinants of methyl donor s-adenosyl
methionine while phospholipids are important methyl acceptors in the one-carbon
metabolic cycle A series of our studies in women during pregnancy have demonstrated
altered levels of these micronutrients and the negative association of docosahexaenoic
acid with homocysteine Various strategies to counteract oxidative stress
during pregnancy such as antioxidant therapy have been examined and found to be
inconsistent In this review we focus on the role of oxidative stress in pregnancy and
discuss the possibility of ameliorating it through modulation of maternal micronutrients
and omega 3 fatty acids especially docosahexaenoic acid We propose for the first time
that manipulation of one-carbon metabolism by maternal diet could be a potential
mechanism to counteract oxidative stress through homocysteine lowering effects and
help in reducing the risk for adverse pregnancyoutcomes
The influence of a low glycemic index dietary intervention on maternal
dietary intake glycemic index and gestational weight gain
during pregnancy a randomized controlled trial McGowan CA Walsh JM Byrne J Curran S McAuliffe FM1 Abstract
BACKGROUND Maternal diet is known to impact pregnancy outcome Following a low glycemic index (GI) diet during pregnancy has been shown
to improve maternal glycemia and reduce infant birthweight and may be associated with a higher fibre intake We assessed the
impact of a low GI dietary intervention on maternal GI nutritional intake and gestational weight gain (GWG) during pregnancy Compliance and acceptability of the low GIdiet was also examined METHOD Eight hundred women were randomised in early pregnancy to receive low GI and healthy eating dietary advice or to receive
standard maternity care The intervention group received dietary advice at a group education session before 22 weeks gestation
All women completed a 3 day food diary during each trimester of pregnancy Two hundred and thirty five women from the intervention arm and 285 women from the control arm returned complete 3x3d FDs and were included in the present analysis RESULTS Maternal GI was significantly reduced in the intervention group at trimester 2 and 3 The numbers of women within the lowest
quartile of GI increased from 37 in trimester 1 to 52 in trimester 3 (Pthinspltthinsp0001) among the intervention group The intervention
group had significantly lower energy intake (Pthinspltthinsp005) higher protein ( TE) (Pthinspltthinsp001) and higher dietary fibre intake (Pthinspltthinsp001)
post intervention Consumption of food groups with known high GI values were significantly reduced among the intervention group Women in the intervention low GI group were less likely to exceed the Institute of Medicines GWG goals CONCLUSION A dietary intervention in early pregnancy had a positive influence on maternal GI food and nutrient intakes and GWG Following
a low GI diet may be particularly beneficial for women at risk of exceeding the GWG goals for pregnancy

IMPORTANZA DELLA COTTURA DEI
CIBI PER OTTENERE IL MIGLIOR
RISULTATO SOTTO IL PROFILO DELLA
DIGERIBILITA E DELLA QUALITA
PREVENZIONE DELLA GESTOSI
Consigliabile introdurre con la dieta pochi zuccheri molte
proteine (molto pesce e latte poche carni rosse) alimenti a
basso indice glicemico e verdure ricche di acqua come
fragole patate cipolle e cicoria
Per diminuire le resistenze vascolari e i grassi circolanti egrave
utile assumere prezzemolo ananas finocchio cipolla melone
aglio e fragole
Per migliorare la funzione cuore-reni sono utili legumi frutta
secca miele cereali integrali rucola vongole e uova
Iodine deficiency in pregnant women living in the South East
of the UK the influence of diet and nutritional supplements
on iodine status Bath SC Walter A Taylor A Wright J Rayman MP Author information
Iodine is a key component of the thyroid hormones which are crucial for brain development
Adequate intake of iodine in pregnancy is important as in utero deficiency may have lifelong
consequences for the offspring Data on the iodine status of UK pregnant women are sparse
and there are no such data for pregnant women in the South East of the UK A total of 100
pregnant women were recruited to a cross-sectional study carried out at the Royal Surrey
County Hospital Guildford at their first-trimester visit for an ultrasound scan The participants
provided a spot-urine sample (for the measurement of urinary iodine concentration (UIC) and
creatinine concentration) and 24 h iodine excretion was estimated from the urinary
iodinecreatinine ratio Women completed a general questionnaire and a FFQ The median UIC
(85middot3 μgl) indicated that the group was iodine deficient by World Health Organisation criteria
The median values of the iodinecreatinine ratio (122middot9 μgg) and of the estimated 24 h iodine
excretion (151middot2 μgd) were also suggestive of iodine deficiency UIC was significantly higher in
women taking an iodine-containing prenatal supplement (n 42) than in those not taking such a
supplement (Plt 0middot001) In the adjusted analyses milk intake maternal age and iodine-
containing prenatal supplement use were positively associated with the estimated 24 h urinary
iodine excretion Our finding of iodine deficiency in these women gives cause for concern We
suggest that women of childbearing age and pregnant women should be given advice on how to
improve their iodine status through dietary means A national survey of iodine status in UK
pregnant women is required
Maternal and in utero determinants of type 2 diabetes risk in the
young Bruce KD Abstract
The global prevalence of diabetes mellitus has reached epidemic proportions In 2010 it was estimated
that 64 of the adult population (285 million) have diabetes In recent years the incidence of type 2
diabetes (T2D) a condition traditionally associated with aging has been steadily increasing among
younger individuals It is now a well-established notion that the early-life period is a critical window of
development and that influences during this period can developmentally prime the metabolic status of the
adult This review discusses the role of maternal and in utero influences on the developmental priming of
T2D risk Both human epidemiological studies and experimental animal models are beginning to
demonstrate that early dietary challenges can accelerate the onset of age-associated metabolic
disturbances including insulin resistance T2D obesity hypertension and cardiovascular disease These
findings show that poor maternal nutrition can prime a prediabetes phenotype often manifest as insulin
resistance by very early stages of life Thus the maternal diet is a critical determinant of premature T2D
risk While the mechanisms that link early nutrition to age-associated metabolic decline are currently
unclear preliminary findings suggest perturbations in a number of processes involved in cellular aging
such as changes in longevity-associated Sirtuin activity epigenetic regulation of key metabolic genes and
mitochondrial dysfunction Preliminary studies show that pharmacological interventions in utero and dietary
supplementation in early postnatal life may alleviate insulin resistance and reduce T2D risk However
further studies are warranted to fully understand the relationship between the early environment and long-
term effects on metabolism Such mechanistic insights will facilitate strategic interventions that prevent
accelerated metabolic decline and the premature onset of T2D in the current and future generations
Counteracting oxidative stress in pregnancy through modulation
of maternal micronutrients and omega-3 fatty acids DSouza V1 Chavan-Gautam P Joshi S Abstract
During pregnancy oxidative stress has been implicated in the pathophysiology of
preeclampsia and preterm birth leading to poor birth outcome Hyperhomocysteinemia
caused as a consequence of altered micronutrients like folic acid and vitamin B12 is
associated with increased production of reactive oxygen species that generate oxidative
stress These micronutrients are important determinants of methyl donor s-adenosyl
methionine while phospholipids are important methyl acceptors in the one-carbon
metabolic cycle A series of our studies in women during pregnancy have demonstrated
altered levels of these micronutrients and the negative association of docosahexaenoic
acid with homocysteine Various strategies to counteract oxidative stress
during pregnancy such as antioxidant therapy have been examined and found to be
inconsistent In this review we focus on the role of oxidative stress in pregnancy and
discuss the possibility of ameliorating it through modulation of maternal micronutrients
and omega 3 fatty acids especially docosahexaenoic acid We propose for the first time
that manipulation of one-carbon metabolism by maternal diet could be a potential
mechanism to counteract oxidative stress through homocysteine lowering effects and
help in reducing the risk for adverse pregnancyoutcomes
The influence of a low glycemic index dietary intervention on maternal
dietary intake glycemic index and gestational weight gain
during pregnancy a randomized controlled trial McGowan CA Walsh JM Byrne J Curran S McAuliffe FM1 Abstract
BACKGROUND Maternal diet is known to impact pregnancy outcome Following a low glycemic index (GI) diet during pregnancy has been shown
to improve maternal glycemia and reduce infant birthweight and may be associated with a higher fibre intake We assessed the
impact of a low GI dietary intervention on maternal GI nutritional intake and gestational weight gain (GWG) during pregnancy Compliance and acceptability of the low GIdiet was also examined METHOD Eight hundred women were randomised in early pregnancy to receive low GI and healthy eating dietary advice or to receive
standard maternity care The intervention group received dietary advice at a group education session before 22 weeks gestation
All women completed a 3 day food diary during each trimester of pregnancy Two hundred and thirty five women from the intervention arm and 285 women from the control arm returned complete 3x3d FDs and were included in the present analysis RESULTS Maternal GI was significantly reduced in the intervention group at trimester 2 and 3 The numbers of women within the lowest
quartile of GI increased from 37 in trimester 1 to 52 in trimester 3 (Pthinspltthinsp0001) among the intervention group The intervention
group had significantly lower energy intake (Pthinspltthinsp005) higher protein ( TE) (Pthinspltthinsp001) and higher dietary fibre intake (Pthinspltthinsp001)
post intervention Consumption of food groups with known high GI values were significantly reduced among the intervention group Women in the intervention low GI group were less likely to exceed the Institute of Medicines GWG goals CONCLUSION A dietary intervention in early pregnancy had a positive influence on maternal GI food and nutrient intakes and GWG Following
a low GI diet may be particularly beneficial for women at risk of exceeding the GWG goals for pregnancy

PREVENZIONE DELLA GESTOSI
Consigliabile introdurre con la dieta pochi zuccheri molte
proteine (molto pesce e latte poche carni rosse) alimenti a
basso indice glicemico e verdure ricche di acqua come
fragole patate cipolle e cicoria
Per diminuire le resistenze vascolari e i grassi circolanti egrave
utile assumere prezzemolo ananas finocchio cipolla melone
aglio e fragole
Per migliorare la funzione cuore-reni sono utili legumi frutta
secca miele cereali integrali rucola vongole e uova
Iodine deficiency in pregnant women living in the South East
of the UK the influence of diet and nutritional supplements
on iodine status Bath SC Walter A Taylor A Wright J Rayman MP Author information
Iodine is a key component of the thyroid hormones which are crucial for brain development
Adequate intake of iodine in pregnancy is important as in utero deficiency may have lifelong
consequences for the offspring Data on the iodine status of UK pregnant women are sparse
and there are no such data for pregnant women in the South East of the UK A total of 100
pregnant women were recruited to a cross-sectional study carried out at the Royal Surrey
County Hospital Guildford at their first-trimester visit for an ultrasound scan The participants
provided a spot-urine sample (for the measurement of urinary iodine concentration (UIC) and
creatinine concentration) and 24 h iodine excretion was estimated from the urinary
iodinecreatinine ratio Women completed a general questionnaire and a FFQ The median UIC
(85middot3 μgl) indicated that the group was iodine deficient by World Health Organisation criteria
The median values of the iodinecreatinine ratio (122middot9 μgg) and of the estimated 24 h iodine
excretion (151middot2 μgd) were also suggestive of iodine deficiency UIC was significantly higher in
women taking an iodine-containing prenatal supplement (n 42) than in those not taking such a
supplement (Plt 0middot001) In the adjusted analyses milk intake maternal age and iodine-
containing prenatal supplement use were positively associated with the estimated 24 h urinary
iodine excretion Our finding of iodine deficiency in these women gives cause for concern We
suggest that women of childbearing age and pregnant women should be given advice on how to
improve their iodine status through dietary means A national survey of iodine status in UK
pregnant women is required
Maternal and in utero determinants of type 2 diabetes risk in the
young Bruce KD Abstract
The global prevalence of diabetes mellitus has reached epidemic proportions In 2010 it was estimated
that 64 of the adult population (285 million) have diabetes In recent years the incidence of type 2
diabetes (T2D) a condition traditionally associated with aging has been steadily increasing among
younger individuals It is now a well-established notion that the early-life period is a critical window of
development and that influences during this period can developmentally prime the metabolic status of the
adult This review discusses the role of maternal and in utero influences on the developmental priming of
T2D risk Both human epidemiological studies and experimental animal models are beginning to
demonstrate that early dietary challenges can accelerate the onset of age-associated metabolic
disturbances including insulin resistance T2D obesity hypertension and cardiovascular disease These
findings show that poor maternal nutrition can prime a prediabetes phenotype often manifest as insulin
resistance by very early stages of life Thus the maternal diet is a critical determinant of premature T2D
risk While the mechanisms that link early nutrition to age-associated metabolic decline are currently
unclear preliminary findings suggest perturbations in a number of processes involved in cellular aging
such as changes in longevity-associated Sirtuin activity epigenetic regulation of key metabolic genes and
mitochondrial dysfunction Preliminary studies show that pharmacological interventions in utero and dietary
supplementation in early postnatal life may alleviate insulin resistance and reduce T2D risk However
further studies are warranted to fully understand the relationship between the early environment and long-
term effects on metabolism Such mechanistic insights will facilitate strategic interventions that prevent
accelerated metabolic decline and the premature onset of T2D in the current and future generations
Counteracting oxidative stress in pregnancy through modulation
of maternal micronutrients and omega-3 fatty acids DSouza V1 Chavan-Gautam P Joshi S Abstract
During pregnancy oxidative stress has been implicated in the pathophysiology of
preeclampsia and preterm birth leading to poor birth outcome Hyperhomocysteinemia
caused as a consequence of altered micronutrients like folic acid and vitamin B12 is
associated with increased production of reactive oxygen species that generate oxidative
stress These micronutrients are important determinants of methyl donor s-adenosyl
methionine while phospholipids are important methyl acceptors in the one-carbon
metabolic cycle A series of our studies in women during pregnancy have demonstrated
altered levels of these micronutrients and the negative association of docosahexaenoic
acid with homocysteine Various strategies to counteract oxidative stress
during pregnancy such as antioxidant therapy have been examined and found to be
inconsistent In this review we focus on the role of oxidative stress in pregnancy and
discuss the possibility of ameliorating it through modulation of maternal micronutrients
and omega 3 fatty acids especially docosahexaenoic acid We propose for the first time
that manipulation of one-carbon metabolism by maternal diet could be a potential
mechanism to counteract oxidative stress through homocysteine lowering effects and
help in reducing the risk for adverse pregnancyoutcomes
The influence of a low glycemic index dietary intervention on maternal
dietary intake glycemic index and gestational weight gain
during pregnancy a randomized controlled trial McGowan CA Walsh JM Byrne J Curran S McAuliffe FM1 Abstract
BACKGROUND Maternal diet is known to impact pregnancy outcome Following a low glycemic index (GI) diet during pregnancy has been shown
to improve maternal glycemia and reduce infant birthweight and may be associated with a higher fibre intake We assessed the
impact of a low GI dietary intervention on maternal GI nutritional intake and gestational weight gain (GWG) during pregnancy Compliance and acceptability of the low GIdiet was also examined METHOD Eight hundred women were randomised in early pregnancy to receive low GI and healthy eating dietary advice or to receive
standard maternity care The intervention group received dietary advice at a group education session before 22 weeks gestation
All women completed a 3 day food diary during each trimester of pregnancy Two hundred and thirty five women from the intervention arm and 285 women from the control arm returned complete 3x3d FDs and were included in the present analysis RESULTS Maternal GI was significantly reduced in the intervention group at trimester 2 and 3 The numbers of women within the lowest
quartile of GI increased from 37 in trimester 1 to 52 in trimester 3 (Pthinspltthinsp0001) among the intervention group The intervention
group had significantly lower energy intake (Pthinspltthinsp005) higher protein ( TE) (Pthinspltthinsp001) and higher dietary fibre intake (Pthinspltthinsp001)
post intervention Consumption of food groups with known high GI values were significantly reduced among the intervention group Women in the intervention low GI group were less likely to exceed the Institute of Medicines GWG goals CONCLUSION A dietary intervention in early pregnancy had a positive influence on maternal GI food and nutrient intakes and GWG Following
a low GI diet may be particularly beneficial for women at risk of exceeding the GWG goals for pregnancy

Iodine deficiency in pregnant women living in the South East
of the UK the influence of diet and nutritional supplements
on iodine status Bath SC Walter A Taylor A Wright J Rayman MP Author information
Iodine is a key component of the thyroid hormones which are crucial for brain development
Adequate intake of iodine in pregnancy is important as in utero deficiency may have lifelong
consequences for the offspring Data on the iodine status of UK pregnant women are sparse
and there are no such data for pregnant women in the South East of the UK A total of 100
pregnant women were recruited to a cross-sectional study carried out at the Royal Surrey
County Hospital Guildford at their first-trimester visit for an ultrasound scan The participants
provided a spot-urine sample (for the measurement of urinary iodine concentration (UIC) and
creatinine concentration) and 24 h iodine excretion was estimated from the urinary
iodinecreatinine ratio Women completed a general questionnaire and a FFQ The median UIC
(85middot3 μgl) indicated that the group was iodine deficient by World Health Organisation criteria
The median values of the iodinecreatinine ratio (122middot9 μgg) and of the estimated 24 h iodine
excretion (151middot2 μgd) were also suggestive of iodine deficiency UIC was significantly higher in
women taking an iodine-containing prenatal supplement (n 42) than in those not taking such a
supplement (Plt 0middot001) In the adjusted analyses milk intake maternal age and iodine-
containing prenatal supplement use were positively associated with the estimated 24 h urinary
iodine excretion Our finding of iodine deficiency in these women gives cause for concern We
suggest that women of childbearing age and pregnant women should be given advice on how to
improve their iodine status through dietary means A national survey of iodine status in UK
pregnant women is required
Maternal and in utero determinants of type 2 diabetes risk in the
young Bruce KD Abstract
The global prevalence of diabetes mellitus has reached epidemic proportions In 2010 it was estimated
that 64 of the adult population (285 million) have diabetes In recent years the incidence of type 2
diabetes (T2D) a condition traditionally associated with aging has been steadily increasing among
younger individuals It is now a well-established notion that the early-life period is a critical window of
development and that influences during this period can developmentally prime the metabolic status of the
adult This review discusses the role of maternal and in utero influences on the developmental priming of
T2D risk Both human epidemiological studies and experimental animal models are beginning to
demonstrate that early dietary challenges can accelerate the onset of age-associated metabolic
disturbances including insulin resistance T2D obesity hypertension and cardiovascular disease These
findings show that poor maternal nutrition can prime a prediabetes phenotype often manifest as insulin
resistance by very early stages of life Thus the maternal diet is a critical determinant of premature T2D
risk While the mechanisms that link early nutrition to age-associated metabolic decline are currently
unclear preliminary findings suggest perturbations in a number of processes involved in cellular aging
such as changes in longevity-associated Sirtuin activity epigenetic regulation of key metabolic genes and
mitochondrial dysfunction Preliminary studies show that pharmacological interventions in utero and dietary
supplementation in early postnatal life may alleviate insulin resistance and reduce T2D risk However
further studies are warranted to fully understand the relationship between the early environment and long-
term effects on metabolism Such mechanistic insights will facilitate strategic interventions that prevent
accelerated metabolic decline and the premature onset of T2D in the current and future generations
Counteracting oxidative stress in pregnancy through modulation
of maternal micronutrients and omega-3 fatty acids DSouza V1 Chavan-Gautam P Joshi S Abstract
During pregnancy oxidative stress has been implicated in the pathophysiology of
preeclampsia and preterm birth leading to poor birth outcome Hyperhomocysteinemia
caused as a consequence of altered micronutrients like folic acid and vitamin B12 is
associated with increased production of reactive oxygen species that generate oxidative
stress These micronutrients are important determinants of methyl donor s-adenosyl
methionine while phospholipids are important methyl acceptors in the one-carbon
metabolic cycle A series of our studies in women during pregnancy have demonstrated
altered levels of these micronutrients and the negative association of docosahexaenoic
acid with homocysteine Various strategies to counteract oxidative stress
during pregnancy such as antioxidant therapy have been examined and found to be
inconsistent In this review we focus on the role of oxidative stress in pregnancy and
discuss the possibility of ameliorating it through modulation of maternal micronutrients
and omega 3 fatty acids especially docosahexaenoic acid We propose for the first time
that manipulation of one-carbon metabolism by maternal diet could be a potential
mechanism to counteract oxidative stress through homocysteine lowering effects and
help in reducing the risk for adverse pregnancyoutcomes
The influence of a low glycemic index dietary intervention on maternal
dietary intake glycemic index and gestational weight gain
during pregnancy a randomized controlled trial McGowan CA Walsh JM Byrne J Curran S McAuliffe FM1 Abstract
BACKGROUND Maternal diet is known to impact pregnancy outcome Following a low glycemic index (GI) diet during pregnancy has been shown
to improve maternal glycemia and reduce infant birthweight and may be associated with a higher fibre intake We assessed the
impact of a low GI dietary intervention on maternal GI nutritional intake and gestational weight gain (GWG) during pregnancy Compliance and acceptability of the low GIdiet was also examined METHOD Eight hundred women were randomised in early pregnancy to receive low GI and healthy eating dietary advice or to receive
standard maternity care The intervention group received dietary advice at a group education session before 22 weeks gestation
All women completed a 3 day food diary during each trimester of pregnancy Two hundred and thirty five women from the intervention arm and 285 women from the control arm returned complete 3x3d FDs and were included in the present analysis RESULTS Maternal GI was significantly reduced in the intervention group at trimester 2 and 3 The numbers of women within the lowest
quartile of GI increased from 37 in trimester 1 to 52 in trimester 3 (Pthinspltthinsp0001) among the intervention group The intervention
group had significantly lower energy intake (Pthinspltthinsp005) higher protein ( TE) (Pthinspltthinsp001) and higher dietary fibre intake (Pthinspltthinsp001)
post intervention Consumption of food groups with known high GI values were significantly reduced among the intervention group Women in the intervention low GI group were less likely to exceed the Institute of Medicines GWG goals CONCLUSION A dietary intervention in early pregnancy had a positive influence on maternal GI food and nutrient intakes and GWG Following
a low GI diet may be particularly beneficial for women at risk of exceeding the GWG goals for pregnancy
Maternal and in utero determinants of type 2 diabetes risk in the
young Bruce KD Abstract
The global prevalence of diabetes mellitus has reached epidemic proportions In 2010 it was estimated
that 64 of the adult population (285 million) have diabetes In recent years the incidence of type 2
diabetes (T2D) a condition traditionally associated with aging has been steadily increasing among
younger individuals It is now a well-established notion that the early-life period is a critical window of
development and that influences during this period can developmentally prime the metabolic status of the
adult This review discusses the role of maternal and in utero influences on the developmental priming of
T2D risk Both human epidemiological studies and experimental animal models are beginning to
demonstrate that early dietary challenges can accelerate the onset of age-associated metabolic
disturbances including insulin resistance T2D obesity hypertension and cardiovascular disease These
findings show that poor maternal nutrition can prime a prediabetes phenotype often manifest as insulin
resistance by very early stages of life Thus the maternal diet is a critical determinant of premature T2D
risk While the mechanisms that link early nutrition to age-associated metabolic decline are currently
unclear preliminary findings suggest perturbations in a number of processes involved in cellular aging
such as changes in longevity-associated Sirtuin activity epigenetic regulation of key metabolic genes and
mitochondrial dysfunction Preliminary studies show that pharmacological interventions in utero and dietary
supplementation in early postnatal life may alleviate insulin resistance and reduce T2D risk However
further studies are warranted to fully understand the relationship between the early environment and long-
term effects on metabolism Such mechanistic insights will facilitate strategic interventions that prevent
accelerated metabolic decline and the premature onset of T2D in the current and future generations
Counteracting oxidative stress in pregnancy through modulation
of maternal micronutrients and omega-3 fatty acids DSouza V1 Chavan-Gautam P Joshi S Abstract
During pregnancy oxidative stress has been implicated in the pathophysiology of
preeclampsia and preterm birth leading to poor birth outcome Hyperhomocysteinemia
caused as a consequence of altered micronutrients like folic acid and vitamin B12 is
associated with increased production of reactive oxygen species that generate oxidative
stress These micronutrients are important determinants of methyl donor s-adenosyl
methionine while phospholipids are important methyl acceptors in the one-carbon
metabolic cycle A series of our studies in women during pregnancy have demonstrated
altered levels of these micronutrients and the negative association of docosahexaenoic
acid with homocysteine Various strategies to counteract oxidative stress
during pregnancy such as antioxidant therapy have been examined and found to be
inconsistent In this review we focus on the role of oxidative stress in pregnancy and
discuss the possibility of ameliorating it through modulation of maternal micronutrients
and omega 3 fatty acids especially docosahexaenoic acid We propose for the first time
that manipulation of one-carbon metabolism by maternal diet could be a potential
mechanism to counteract oxidative stress through homocysteine lowering effects and
help in reducing the risk for adverse pregnancyoutcomes
The influence of a low glycemic index dietary intervention on maternal
dietary intake glycemic index and gestational weight gain
during pregnancy a randomized controlled trial McGowan CA Walsh JM Byrne J Curran S McAuliffe FM1 Abstract
BACKGROUND Maternal diet is known to impact pregnancy outcome Following a low glycemic index (GI) diet during pregnancy has been shown
to improve maternal glycemia and reduce infant birthweight and may be associated with a higher fibre intake We assessed the
impact of a low GI dietary intervention on maternal GI nutritional intake and gestational weight gain (GWG) during pregnancy Compliance and acceptability of the low GIdiet was also examined METHOD Eight hundred women were randomised in early pregnancy to receive low GI and healthy eating dietary advice or to receive
standard maternity care The intervention group received dietary advice at a group education session before 22 weeks gestation
All women completed a 3 day food diary during each trimester of pregnancy Two hundred and thirty five women from the intervention arm and 285 women from the control arm returned complete 3x3d FDs and were included in the present analysis RESULTS Maternal GI was significantly reduced in the intervention group at trimester 2 and 3 The numbers of women within the lowest
quartile of GI increased from 37 in trimester 1 to 52 in trimester 3 (Pthinspltthinsp0001) among the intervention group The intervention
group had significantly lower energy intake (Pthinspltthinsp005) higher protein ( TE) (Pthinspltthinsp001) and higher dietary fibre intake (Pthinspltthinsp001)
post intervention Consumption of food groups with known high GI values were significantly reduced among the intervention group Women in the intervention low GI group were less likely to exceed the Institute of Medicines GWG goals CONCLUSION A dietary intervention in early pregnancy had a positive influence on maternal GI food and nutrient intakes and GWG Following
a low GI diet may be particularly beneficial for women at risk of exceeding the GWG goals for pregnancy
Counteracting oxidative stress in pregnancy through modulation
of maternal micronutrients and omega-3 fatty acids DSouza V1 Chavan-Gautam P Joshi S Abstract
During pregnancy oxidative stress has been implicated in the pathophysiology of
preeclampsia and preterm birth leading to poor birth outcome Hyperhomocysteinemia
caused as a consequence of altered micronutrients like folic acid and vitamin B12 is
associated with increased production of reactive oxygen species that generate oxidative
stress These micronutrients are important determinants of methyl donor s-adenosyl
methionine while phospholipids are important methyl acceptors in the one-carbon
metabolic cycle A series of our studies in women during pregnancy have demonstrated
altered levels of these micronutrients and the negative association of docosahexaenoic
acid with homocysteine Various strategies to counteract oxidative stress
during pregnancy such as antioxidant therapy have been examined and found to be
inconsistent In this review we focus on the role of oxidative stress in pregnancy and
discuss the possibility of ameliorating it through modulation of maternal micronutrients
and omega 3 fatty acids especially docosahexaenoic acid We propose for the first time
that manipulation of one-carbon metabolism by maternal diet could be a potential
mechanism to counteract oxidative stress through homocysteine lowering effects and
help in reducing the risk for adverse pregnancyoutcomes
The influence of a low glycemic index dietary intervention on maternal
dietary intake glycemic index and gestational weight gain
during pregnancy a randomized controlled trial McGowan CA Walsh JM Byrne J Curran S McAuliffe FM1 Abstract
BACKGROUND Maternal diet is known to impact pregnancy outcome Following a low glycemic index (GI) diet during pregnancy has been shown
to improve maternal glycemia and reduce infant birthweight and may be associated with a higher fibre intake We assessed the
impact of a low GI dietary intervention on maternal GI nutritional intake and gestational weight gain (GWG) during pregnancy Compliance and acceptability of the low GIdiet was also examined METHOD Eight hundred women were randomised in early pregnancy to receive low GI and healthy eating dietary advice or to receive
standard maternity care The intervention group received dietary advice at a group education session before 22 weeks gestation
All women completed a 3 day food diary during each trimester of pregnancy Two hundred and thirty five women from the intervention arm and 285 women from the control arm returned complete 3x3d FDs and were included in the present analysis RESULTS Maternal GI was significantly reduced in the intervention group at trimester 2 and 3 The numbers of women within the lowest
quartile of GI increased from 37 in trimester 1 to 52 in trimester 3 (Pthinspltthinsp0001) among the intervention group The intervention
group had significantly lower energy intake (Pthinspltthinsp005) higher protein ( TE) (Pthinspltthinsp001) and higher dietary fibre intake (Pthinspltthinsp001)
post intervention Consumption of food groups with known high GI values were significantly reduced among the intervention group Women in the intervention low GI group were less likely to exceed the Institute of Medicines GWG goals CONCLUSION A dietary intervention in early pregnancy had a positive influence on maternal GI food and nutrient intakes and GWG Following
a low GI diet may be particularly beneficial for women at risk of exceeding the GWG goals for pregnancy

The influence of a low glycemic index dietary intervention on maternal
dietary intake glycemic index and gestational weight gain
during pregnancy a randomized controlled trial McGowan CA Walsh JM Byrne J Curran S McAuliffe FM1 Abstract
BACKGROUND Maternal diet is known to impact pregnancy outcome Following a low glycemic index (GI) diet during pregnancy has been shown
to improve maternal glycemia and reduce infant birthweight and may be associated with a higher fibre intake We assessed the
impact of a low GI dietary intervention on maternal GI nutritional intake and gestational weight gain (GWG) during pregnancy Compliance and acceptability of the low GIdiet was also examined METHOD Eight hundred women were randomised in early pregnancy to receive low GI and healthy eating dietary advice or to receive
standard maternity care The intervention group received dietary advice at a group education session before 22 weeks gestation
All women completed a 3 day food diary during each trimester of pregnancy Two hundred and thirty five women from the intervention arm and 285 women from the control arm returned complete 3x3d FDs and were included in the present analysis RESULTS Maternal GI was significantly reduced in the intervention group at trimester 2 and 3 The numbers of women within the lowest
quartile of GI increased from 37 in trimester 1 to 52 in trimester 3 (Pthinspltthinsp0001) among the intervention group The intervention
group had significantly lower energy intake (Pthinspltthinsp005) higher protein ( TE) (Pthinspltthinsp001) and higher dietary fibre intake (Pthinspltthinsp001)
post intervention Consumption of food groups with known high GI values were significantly reduced among the intervention group Women in the intervention low GI group were less likely to exceed the Institute of Medicines GWG goals CONCLUSION A dietary intervention in early pregnancy had a positive influence on maternal GI food and nutrient intakes and GWG Following
a low GI diet may be particularly beneficial for women at risk of exceeding the GWG goals for pregnancy





























