Embed Size (px)
Citation preview

Thorax 1988;43:441-445
Computed tomographic staging of anteriormediastinal neoplasmsERINO A RENDINA, FEDERICO VENUTA, LUIGI CERONI,MASSIMO MARTELLI, GIANFRANCO GUALDI, MAURO CATERINO,COSTANTE RICCI
From the Departments of Thoracic Surgery and Radiology, Universita "La Sapienza," Rome, Italy
ABSTRACT Sixty patients with anterior mediastinal neoplasms undergoing computed tomographybefore surgical exploration were entered in a prospective study to assess the value of computedtomography in the preoperative staging of anterior mediastinal tumours. Correct prediction oflocation, size, and tissue density was obtained in all 60 cases. Correct identification of the nature ofthetumours was achieved by computed tomography in 37 of the 54 previously undiagnosed cases.Particular attention was given to the evaluation of the relation of the tumour to adjacent mediastinalstructures, to predict the feasibility of radical surgical procedures. Overall sensitivity, specificity, andaccuracy in identifying resectability were 46%, 85%, and 64%, with positive and negative predictiveindices of 78% and 58%. Capsulated or highly invasive lesions were clearly distinguished, and thepresence or absence of infiltration of mediastinal vessels, pericardium, and chest wall was correctlyrecognised in most cases. It is suggested that the evaluation of anterior mediastinal neoplasms shouldinclude computed tomography because of its accuracy in predicting size, location, and tissue densityof the neoplasm. Computed tomography may suggest, often with good reliability, the histologicaltype of the tumour and its relation to contiguous mediastinal structures, thus contributing to thechoice of the appropriate surgical approach or route for biopsy.
Computed tomography has proved to be an excellenttool for investigation of the mediastinum; it allowsprecise location ofmediastinal masses and may predictwith good accuracy their solid or cystic nature. Inaddition, computed tomography causes little discom-fort for the patient and may drastically reduce the needfor other diagnostic procedures.'The encouraging results obtained by computed
tomography with other intrathoracic neoplasms2stimulated us to ascertain the value of the technique inthe assessment of anterior mediastinal tumours, withregard to their accurate localisation and, in particular,to invasion of adjacent structures for determining thefeasibility of radical resection. We have thereforeconducted a prospective study on consecutive patientswho were referred to our department for the evalua-tion of an anterior mediastinal mass and who sub-sequently underwent surgery that established thenature and extent of the tumour.
Address for reprint requests: Dr E A Rendina, Cattedra di ChirurgiaToracica, Universita di Roma "La Sapienza," Policlinico Umberto 1,00161 Rome, Italy.
A ccepted 21 January 1988
Methods
The study was a prospective survey based on 60consecutive patients-33 men and 27 women, age 14-84 (mean 41) years-investigated or treated surgicallyfor tumours in the anterior mediastinum in thedepartment of thoracic surgery of the University ofRome from January 1983 to April 1987.Computed tomography of the chest and abdomen
was performed by a third generation computedtomography scanner (Siemens DRI); scans 8 mmthick were obtained at 1[5 cm intervals from thethoracic inlet to the diaphragm; abdominal scans werenegative in all patients. Repeated bolus injections ofcontrast material (Selectografin 70%, 20-30 ml up to atotal of 120-140 ml) were performed in 59 patients; allscans were interpreted by the same team of radiolog-ists. All 60 patients underwent surgery within twoweeks of computed tomography. The operativeprocedures undertaken were partial or total mediansternotomy in 50 patients, thoracotomy in five, andmediastinotomy or mediastinoscopy in five patients.Resection was complete in 30 patients and subtotal in16; in 14 patients only a biopsy was performed.
441
on October 6, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.43.6.441 on 1 June 1988. D
ownloaded from

Rendina, Venuta, Ceroni, Martelli, Gualdi, Caterino, RicciTable I Histology of the tumours
Thymoma: 25Stage I 10 (2 cystic)Stage II 3 (1 cystic)Stage III 12 (3 recurrent)
Lymphoma: 23Hodgkin's 12Non-Hodgkin's 11
Dysgerminoma 2Morgagni hernia 2Goitre 3Haemangioma 1Thymolipoma IHamartoma IMesodermal cyst 2
Total 60
Histological findings are reported in table 1.Thymomas were classified as stage I (capsulatedlesion), stage II (infiltration ofthe capsule), or stage III(infiltration of surrounding organs).3 Nine patientswith thymoma (three stage I or II and six stage III) hadmyasthenia gravis.We evaluated the ability of computed tomography
to determine (1) the location, (2) the nature, and (3) thelocal extent of disease.
Local extension and invasion by tumour was sug-gested by one or more of the following criteria:obliteration of fat planes; indentation or irregularityof vascular, pleural, or pericardial margins in contactwith the tumour; apparent infiltration into intercostalmuscles or periostium. On the basis of the presence orabsence of these features the neoplasms was classifiedas likely to be totally resectable (cleavage planepresent, no features suggesting infiltration), partially
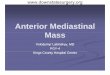
Fig 1 Retrosternal goitre. Computed tomography correctlydetected the benign attitude of the neoplasm (arrows show the
cleavage plane), butfailed to characterise the masshistologically (computed tomography diagnosis:non-invasivethymoma).
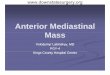
4W,Fig 2 Stage II thymoma (microscopic evidence ofcapsularinvasion) diagnosed correctly by computed tomography.Absence of infiltration of the aortic wall was correctlyreported (black arrow), but irregular mediastinal pleuralmargins suggested infiltration (white arrow), which was notconfirmed at surgery, when a good cleavage plane wasidentified.
resectable, or non-resectable (cleavage plane incom-plete or absent, infiltration apparently present). Inaddition, we separately assessed the relation of thetumour to lung parenchyma, mediastinal vessels,mediastinal wall, and chest wall. Uncertain resultsconcerning location, characterisation of the tumour,or relation to adjacent structures were classified aseither false negative (feature present at surgery) orfalse positive (feature absent at surgery).
Fifty four patients had radical surgery and sixbiopsy only. All pathological material was carefullyexamined to identify adhesion to or infiltration of thestructures that were resected along with the tumour.
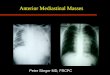
Fig 3 Hodgkin's disease showing presence ofa cleavageplane with the aortic wall (black arrows) and inner chest wall(white arrows). The histological diagnosis and absence ofinfiltration were correctly predicted.
442
on October 6, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.43.6.441 on 1 June 1988. D
ownloaded from

Computed tomographic staging ofanterior mediastinal neoplasms
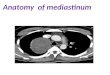
Fig 4 Yolk sac tumour. Computed tomography diagnosis(thymoma) and prediction oflack ofinvasion by tumour wereincorrect. Tumour infiltration ofthe lung parenchyma (whitearrows) and chest wall (black arrows) wasfound atoperation.
After surgical exploration sensitivity, specificity,accuracy, and positive and negative predictive value4were calculated for the overall resectability of thetumour, and separately for the infiltration of lungparenchyma, mediastinal vessels, mediastinal wall(pleura, pericardium), and inner chest wall.
Results
In all 60 cases computed tomography allowed accuratelocalisation of the tumour (see fig 1) and also correctlydistinguished whether it was solid or cystic.The ability of computed tomography to predict the
histological nature of the neoplasm was evaluated in54 patients. This was already known in the remainingsix, ofwhom three had recurrent thymoma and threeunderwent surgery for restaging of previously diag-
Table 2 Sensitivity, specifcity, and accuracy of computedtomography in assessing resectability and local invasion
Criterion % %
Overall resectability Sensitivity 46 PPI 78(60 cases) Specificity 85 NPI 58
Accuracy 64Invasion of vessels Sensitivity 54 PPI 90
(60 cases) Specificity 94 NPI 77Accuracy 80
Invasion of lung Sensitivity 41 PPI 100(58 cases) Specificity 100 NPI 72
Accuracy 76Invasion of mediastinum* Sensitivity 60 PPI 72
(58 cases) Specificity 85 NPI 77Accuracy 76
*Includes pericardium, mediastinal pleura, endothoracic fascia, inter-costal muscles.PPI, positive predictive index; NPI, negative predictive index.
nosed lymphoma. Correct diagnosis was achieved in37 patients (68 5%). Prediction was more accuratewith stage I and II thymomas, especially whenevidence of myasthenia gravis was present (threepatients); 12 of 12 such cases were correctly inter-preted. Stage II (fig 2) and stage III moderatelyinvasive thymomas and non-infiltrative lymphomaspresenting as multiple, conglomerate, and enlargedanterior mediastinal nodes (fig 3) were characterisedwith good accuracy. Fat containing lesions such asMorgagni hernias (two cases) were correctly inter-preted, but in one patient with a thymolipoma thecomputed tomography result was equivocal. Widelyinfiltrative, aggressive neoplasms (fig 4) were variouslyclassified as stage III thymoma, lymphoma, or dysger-minoma, and there was no relation between thecomputed tomography prediction and the histology.The relation of the tumour to adjacent structures
was evaluated by computed tomography to assess thevalue of the technique in the preoperative assessmentof disease. The results are summarised in table 2.
Discussion
The management ofpatients with anterior mediastinalneoplasms is often difficult.5 The surgical approachvaries with the histology of the tumour and its localinvasiveness; none of the conventional radiographicimaging techniques is accurate in providing thesedata,6 so that on occasion the decision to performsimple biopsy, debulking procedures, or radical resec-tion is made only in the operating theatre.The increasing sophistication of computed
tomography scanners and greater experience in read-ing the scans78 have improved the preoperative assess-ment and characterisation of mediastinal masses.9Computed tomography has been reported to behelpful in identifying thymic lesions,'°" reaching anaccuracy of 91% in patients with myasthenia gravis.Lymphoma may also be recognised by computedtomography,'2 especially when it presents as in figure3; uninodular capsulated lymphoma was, however,misinterpreted as stage I thymoma twice in our series,and very aggressive disease could not be distinguishedfrom stage III thymoma or germ cell tumour (fig 4). '3 14
Computed tomography may allow mediastinalthyroid tissue to be identified by its continuity with thethyroid in the neck.'516 Goitres that are completelyintrathoracic, however, arising from ectopic thyroidtissue, represent 0-2-1% of all goitres.9 1'1' Two ofourcases showed these features and the first of these wasincorrectly interpreted (fig 1). In our experience stageI, II, and III moderately invasive thymomas (fig 2);enlarged conglomerate lymph nodes due to lymphoma(fig 3); and Morgagni hernias were interpreted withhighest accuracy.
443
on October 6, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.43.6.441 on 1 June 1988. D
ownloaded from

Rendina, Venuta, Ceroni, Martelli, Gualdi, Caterino, RicciThe main purpose of our study was to assess the
ability of computed tomography to determine therelation of anterior mediastinal tumours to surround-ing structures. Such neoplasms not infrequently showunpredicted invasiveness at operation, so that moreaccurate preoperative imaging might modify treat-ment plans. In addition, tumours such as thymoma orlymphoma may impinge on or invade mediastinalpleura, pericardium, phrenic nerves, great vessels, orlung parenchyma. Appropriate treatment is stronglyinfluenced by such factors, especially where age,cardiorespiratory condition, and general health areadverse factors.88 According to the data ofBrown andcolleagues,6 none of the conventional radiographicimaging techniques is accurate in predicting whether athymoma is locally invasive. Although in many casescomputed tomography may determine whether thelesion is invasive,7 Nakata and associates9 concludedthat differentiating a benign from a malignantthymoma is impossible in some cases. Graeber andcolleagues' reported that invasiveness was correctlyidentified from the computed tomography scan in nineof 1 I patients with solid mediastinal tumours. We havereported2 a computed tomography accuracy of70% indiscriminating direct mediastinal infiltration by lungcancer. The complexity of the relationship within theanterior compartment of the mediastinum, however,requires a more specific approach.
Overall, when the lesions were relatively benign-for example, stage I thymoma, lymphoma, intra-thoracic goitre, Morgagni hernia, mesodermal cyst, orteratoma-computed tomography staging wasaccurate; with appearances suggesting possibleinvasion-for example, stage II (three false negativeswere due to microscopic invasion) and stage IIIthymoma (fig 2) and dubiously infiltrative lymphoma,dysgerminoma (fig 4) or haemangioma-computedtomography was less reliable diagnostically. On theother hand, when the tumour displays definite charac-teristics of invasiveness on the computed tomographyscan (stage III thymoma, aggressive lymphoma)prediction is again fairly reliable (positive predictiveindex 78%). For each of the three areas of possibleinvasion taken separately (lung, vessels, and medias-tinal wall) the accuracy of identifying invasion wasbetter than the overall estimate of resectability; forexample, an error in interpreting infiltrations of thebrachiocephalic vein would not influence the figuresregarding the lung or mediastinal pleura, but wouldlower the overall accuracy. Specificity was consistentlygood in each of these areas, reflecting the presence ofsome capsulated tumours in our series. The 100%specificity for recognition of lung parenchymal infil-tration is, however, atypical; this is relatively easy withcapsulated masses, but the prediction of diseaseaffecting the lung is more difficult and often impossible
when the tumour abuts on the mediastinal pleura (figs2 and 4). The value ofcomputed tomography is likelyto be greater when infiltration of mediastinal vessels,pericardium, and endothoracic fascia is investigated;intravenous injection of contrast material allowsdetection of any irregularity of the vascular wall, andthe presence of fat tissue planes between the tumourand these organs offers better contrast than does air inthe lung.
In conclusion, we suggest that the evaluation of ananterior mediastinal mass detected on a plain chestradiograph should always include computed tomogra-phy. This is rapid, cost effective, and safe, and providesvery accurate information about location, size, andtissue density of the mass and its relation toanatomical structures. In addition, computedtomography may suggest, often with good reliability,the histological type of the tumour, and it may alsosuggest whether invasion of adjacent mediastinalorgans has occurred, thus contributing to the decisionabout surgical strategy.
References
I Graeber GM, Shriver CD, Albus RA, et al. The use ofcomputed tomography in the evaluation ofmediastinalmasses. J Thorac Cardiovasc Surg 1986;91:662-6.
2 Rendina EA, Bognolo DA, Mineo TC, et al. Computedtomography in the evaluation ofintrathoracic invasionby lung cancer. J Thorac Cardiovasc Surg 1987;94:57-63.
3 Bergh NP, Gatzinsky P, Larsson S, Lundin P, Riddel B.Tumours of the thymus and thymic region: I. Clin-icopathological studies on thymomas. Ann ThoracSurg 1987;25:91-8.
4 Feinstein AR. On the sensitivity, specificity, and dis-crimination of diagnostic tests. In: Feinstein AR, ed.Clinical biostatistics. St Louis: Mosby, 1977:214-6.
5 Ricci C. Chirurgia radicale dei tumori del mediastino. In:Proceedings of the XX Congresso Nazionale ChirurgiaToracica. Rome: SEROS, 1986:124-40.
6 Brown LR, Muhm JR, Gray JE. Radiographic detectionof thymoma. AJR 1980;134:1181-8.
7 Brown LR, Muhm JR. Computed tomography of thethorax: current perspectives. Chest 1983;83:806-13.
8 Webb WR. Advances in computed tomography of thethorax. Radiol Clin N Am 1983;21:723-39.
9 Nakata H, Nakayama C, Nobe T, Koga M. Computedtomography characterization of anterior mediastinaltumors. J Comput Tomogr 1985;9: 161-66.
10 Baron RL, Lee JKT, Sagel SS, Levitt RG. Computedtomography of the abnormal thymus. Radiology1982;142: 127-34.
11 Moore AV, Korobkin M, Powers B, et al. Thymomadetection by mediastinal CT: patients with myastheniagravis. AJR 1982;138:217-22.
444
on October 6, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.43.6.441 on 1 June 1988. D
ownloaded from

Computed tomographic staging ofanterior mediastinal ne12 Ellert J, Kreel L. The role ofcomputed tomography in the
initial staging and subsequent management of thelymphomas. J Comput Assist Tomogr 1980;4:368-91.
13 Levitt RG, Husband JE, Glazer GS. CT ofprimary germ-cell tumors of the mediastinum. AJR 1984;142:73-8.
14 Maggi G. I tumori del timo. Minerva Chir 1984;39: 1-1 0.15 Bashist B, Ellis K, Gold RP. Computed tomography of
intrathoracic goiters. AJR 1983;140:455-60.16 Glazer GM, Axel L, Mass AA. CT diagnosis of medias-
tinal thyroid. AJR 1982;138:495-8.
oplasms 44517 Falor WH, Kelly TR, Jackson JB. Intrathoracic goiters.
Surg Gynecol Obstet 1963; 117:604- 10.18 Ferrante G, Cecere C, laccarino V, Sava M. I1 gozzo
mediastinico. In: Proceedings of the Congresso Straor-dinario Chirurgia Toracica. Roma: SEROS, 1981:213-20.
19 Ricci C, DeLeo G, Bombi G, Mineo TC. Chirurgia dellelocalizzazioni mediastiniche isolate del morbo di Hod-gkin. Osservazioni su 7 casi operati. Minerva Chir1973;28:469-78.
on October 6, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.43.6.441 on 1 June 1988. D
ownloaded from