Embed Size (px)
Citation preview

Comprehensive Outpatient Rehabilitation for Returning Head Injured Veterans:
Ethical vs. Moral Issues
Darlyne G. Nemeth, Ph.D., M.P.Traci Wimberly, B.S.
Amity Lewis, B.S.John Hamilton, B.S.
Presented at Working on the Front: Ethics in Rehabilitation of Veterans
Friday, February 29, 2008Cotillion Ballroom, S.B. Memorial UnionSouthern University, Baton Rouge, LA

TABLE OF CONTENTS
• Abstract• Abandoned Soldiers• Failing to Reintegrate• The Anonymous and The Famous• Congressional Action• The Advantage of Privilege • Barriers to Care• One Extern’s VA Experiences• Blast Related TBIs• Regaining Control Via Inclusion• A Comprehensive Outpatient Neuropsychological
Rehabilitation Program Based on Inclusion• Conclusion• References

AbstractThe recent articles highlighting Bob Woodruff’s post head injury journey to recovery
have uncovered a “crisis of care faced by so many injured soldiers and their families” (Nancy Chadross, ABC News, 2/26/07). Post Iraq/Afghanistan head injury estimates vary from 10 %-20% for returning veterans. Basically, after their inpatient stay, returning veterans and their families have been bewildered by the lack of vocational direction and outpatient services available to them. Mr. Woodruff has been quoted as saying that injured veterans “need support that matches their sacrifice.” Yet, does it?
According to Head (2004) the average age of returning veterans is 19. Rehabilitation efforts must be designed to help the transition and reduce the barriers to functionality and employability. Along with head injuries, at least 1 in 6 soldiers leaving Iraq have major mental health difficulties. In setting up appropriate outpatient intervention programs for veterans, ethical vs. moral standards of care may sometimes clash. For example, one definition of ethical is “conforming to accepted standards of conduct.” One definition of moral is “conforming to a standard of right behavior.” Although these concepts are often used interchangeably, they are not the same. There is frequently a big difference between what is “accepted” vs. what is “right.” Effective intervention programs must strive to do what is “right,” not merely what is “acceptable.”
Is it right for veterans who need the most care, to receive the least care? Without holistic outpatient rehabilitation programs for our head injured veterans, they will most likely be receiving the least care. Proceeding on the belief that we Americans truly want our returning veterans to have the standard of care they deserve, and knowing that successful rehabilitation eventuates in reduced long term costs, a comprehensive outpatient program focusing on brain injury and mental health rehabilitation, vocational reentry, and family reunification will be outlined.

Abandoned Soldiers: A History
• After war causalities, which have been documented to lead to homelessness, have been recorded as far back as the Civil War. These soldiers became known as “wandering veterans.”
• Veterans returning from WWI became known as the “bonus army” because they were not given the benefits they were promised.
• After Vietnam, the American public and the Federal Government turned their backs on the returning veterans in order to forget the pain of defeat.
• During Desert Storm, in 1991, we provided supportive group services to the families of the 321st Division. Upon their return, the Army said, “we’ll take it from here,” but they did not. No transitional services were provided to the veterans and/or their families.

Abandoned Soldiers: A History (continued)
• Today, over 1500 returning Iraq and Afghanistan veterans have been labeled as “homeless” by the Department of Veterans Affairs.
• According to Jack Downing, President of Soldier On, “It’s a disgrace…you have served your country, you get damaged, and you come back and we don’t take care of you. And we make you prove that you need our services.” (McClan, 2008).
• The Advantage of Privilege: The Bob Woodruff Story.

Congressional Action
• Several bills have come before Congress.• H.R. 2201 (5/16/07), “The Caring for Veterans with Traumatic Brain
Injury Act of 2007,” passed the House by a vote of 421 to 0, but has yet to be signed into law.
• H.R. 2199 (5/8/2007), “Traumatic Brain Injury Health Enhancement and Long Term Support Act of 2007” limit services to moderate to severe TBI and exclude veterans of the Persian Gulf War, targeting the date of eligibility as “after 11/11/1998.”
• Senate Bill 1349 (5/9/2007) cited as the “Military and Veterans Traumatic Brain Injury Treatment Act” states that “the highest quality of care possible…in facilities that most appropriately meet the specific needs of the individual”…”be rehabilitated to the fullest extent possible.” It allows for private care if public facilities “do not meet the standard of care.”
• However, these bills have yet to be signed into law.

Failing to Reintegrate: Recent Newspaper Articles
• In East Baton Rouge Parish, two Iraq veterans tried for murder or attempted murder cited PTSD as a defense (Angelette, 2008). Judges and juries rejected this defense even when compelling professional testimony was offered.
• In a case in West Baton Rouge Parish, an Iraq veteran who murdered his 3 month old baby was given 25 years instead of the death penalty reportedly because of his service to his country. Reportedly, he was suffering from PTSD.
• Similar reports of violence, especially against children, are occurring throughout the country. One from Oceanside, California, was of a two-time Iraq veteran, a sergeant honorably discharged from the Marine Corps shortly after his baby’s death (Teri Figueroa, North County Times 1/25/08). Had he been exposed to blast injuries?
• In these cases, it was unclear exactly what type of treatment, if any, these veterans had received. Now they will spend the rest of their lives in prison. Could a good screening have prevented this outcome?

What the V.A. Currently Offers
• New VA adjustment centers (200) and community clinics (900) are steps in the right direction (McClan, 2007).
• Four V.A. “polytrauma centers” at Palo Alto, Minneapolis, Tampa, and Walter Reed, were established by Congress in 2005.
• The Palo Alto Acute TBI program consisted of 45 beds, and takes, on the average 6 months to complete.
• The Livermore facility only offers screenings.

One Extern’s Experiences
• While the acute treatment program offered for vets and active duty soldiers was clearly state-of-the-art, however, “what happens to many after discharge” was unclear. All discharged TBIs were at first followed “by social workers in order to inform and suggest treatment options that the patient and family might pursue upon their return to their home cities.” Again, their further involvement was unclear.
• Most chronic care patients were over 40, and many were 55+.

A Case History from Palo Alto
• Example 1: A mild to moderate TBI due to an IED (blast injury) veteran was admitted who presented with a flat affect and was disinterested in therapy. As one of only two survivors of this experience, it was just too hard for him to face it.
• When the other survivor entered the program, this young veteran went home ASAP.
• Mr. Hamilton stated that, “despite their bright and compassionate staff,” he just did not know “if enough resources existed in the VA system to treat this patient population.”
• Furthermore, he recommended “that further investment be made in identifying individuals with mild TBIs and making sure that all returning soldiers have mandatory psychological/psychiatric screenings.” (emphasis added)

A Case History from Livermore
• Example 2: A 22 year old Hispanic male who was brought to the Livermore VA by his wife for assessment of “forgetfulness.” He had little understanding of his PTSD symptoms such as severe emotional lability and irritability, mood and temper outbursts, and problems sleeping, etc.
• This individual, according to Mr. Hamilton, is quite “representative of many individuals returning home from the wars.”
• He only came because “he wanted to do what was best for his family.”
• In a different circumstance, “his PTSD would not have been discovered or treated”…perhaps until he committed a violent act. (emphasis added)

The Gap
• A gap still exists and our soldiers often times slip through the cracks.
• Most veterans do not know that they can turn to the private sector for treatment.
• The Keesler Institute for Rehabilitation and the Rehabilitation Institute of Chicago are two outstanding (private sector) facilities that have offered to fill the gap.
• But, issues of politics and control continue to interfere with treatment opportunities.

Blast Related TBIs• Blast related TBIs are those sustained from contact with explosives.• There are three types of Blast Related Injuries:
1) Primary – due to changes in atmospheric pressure2) Secondary – due to objects hitting people3) Tertiary – due to people being forcefully put into motion.
• Improvised Explosive Devices (IEDs) are the terrorists’ weapon of choice. They are cheap, easy to prepare, and do significant damage.
• Of all wounded soldiers serving in Iraq who were treated at Echelon II Medical Unit, 88% had been injured by IEDs and 47% of those soldiers had head injuries. For another Marine Unit, the figures were 65% IEDs and 32% mines. Of these individuals, 53% had head and neck injuries.
• Even those who were exposed to blasts, but had no visible injuries, often presented with either retrograde or antereograde amnesia upon regaining consciousness or awareness. Residual symptoms often include severe headaches, tinnitus, hypersensitivity to noise, and tremors. Blast symptoms have been documented as far back as WWI.

Blast Related TBIs
• In primary blasts, injuries result from displacement, stretching, and shearing forces in the brain, the lungs, the bowels, and the middle ear.
• TBIs include contusion, concussion, subdural hemorrhage, edema, and diffuse axonal injury.
• The most common locations of these TBIs are: 1) the corticomedullary junction in the frontal and temporal areas, 2) the internal capsule, 3) deep gray matter, 4) upper brainstem, and 5) corpus callosum.
• According to Taber, et. al, “Contusions occur when the brain moves within the skull enough to impact bone, causing bruising of the brain parenchyma (hemorrhage and edema).” The MRI is the best neuroimaging device to detect these injuries.

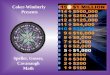
Views of the Brain
• The most common locations for contusions (blue) are the superficial gray matter of the inferior, lateral and anterior aspects of the frontal and temporal lobes, with the occipital poles or cerebellum less often involved.
• The most common locations for subdural hemorrhage (purple) are the frontal and parietal convexities.
• The most common locations for diffuse axonal injury (pink) are the corticomedullary (gray matter-white matter) junction (particularly frontotemporal), internal capsule, deep gray matter, upper brainstem, and corpus callosum.

SB 1349
• TBI research grants must be available for the following purposes:
1. To improve the screening, diagnosis, and treatment of TBI.
2. To improve the rehabilitation of veterans with TBI.
3. To improve the best practices of the above.
4. To identify ways to prevent or ameliorate the secondary effects of brain injuries.

Outpatient Neurocognitive Rehabilitation
• There is a strong need for outpatient neuropsychological rehabilitation programs to fill in the gap.
• Veterans and their families need to receive treatment for managing the stress associated with TBI rehabilitation services.
• Grants must be available for the development of such programs.
• There must be a way around the politics of power and control.

Neurocognitive Rehabilitation
• Definition: Williams and Long (1987) define neurocognitive rehabilitation as a systematic program directed at modifying neurocognitive functioning or neurocognitively oriented activities following some type of brain-behavior dysfunction. It includes the following treatment strategies:
• A. Problem Identification – targeting cognitive and functional domains that need to be assessed given certain types of neurological damage
• B. Selecting Appropriate Interventions –plan, develop, and implement specific individualized neuropsychological treatment approaches given the neurologic profile.
• C. Setting Realistic Outcome Goals – maintaining a focused treatment regimen that is aimed at attaining functional goals that are reasonable in scope and that increase the probability of success given a patient’s specific residual deficits.
• D. Maintaining Realistic Expectation – assisting with setting and sustaining a course of treatment that is clearly attainable.

Definitions
• TBI (Traumatic Brain Injury): “Brain injury caused by an external mechanical force such as a blow to the head, concussive forces, acceleration-deceleration forces, or projective missile (e.g., bullet or explosive).”
• PTSD (Posttraumatic Stress Disorder): “The development of a characteristic set of symptoms after exposure to a psychologically extreme traumatic stressor.”
• PCS (Postconcussive Syndrome): “A constellation of symptoms that is seen in some patients following a mild TBI…symptoms include dizziness, headache, poor concentration, and sensory abnormalities…”

Outpatient Neurocognitive RehabilitationSuccess:
• Undaunted in recovery efforts• Unwillingness to give up
• Family support• Job support
• Available resources
• Rewards for functionality
• Hope, hope, hope!
Failure:
• Lack of resources
• Personality disorder
• Isolation• Reinforcement for being disabled
• Pessimism
• Lack of support

• Many patients are left adrift once released from acute care.
• Patients need to be referred properly when discharged from inpatient care; referrals should include both the patient and the family.
• Few outpatient sources are available for neurocognitive rehabilitation by a neuropsychologist.
• Available resources are often difficult to find.
Problems that Patients Face

Parameters to Target
According to Ponsford and colleagues (1995), recovery requires a multi-dimensional approach that may necessitate addressing one or more of the following parameters:
• Attentional problems and fatigue.• Memory and learning difficulties.• Executive functioning problems like impaired planning and
organization, problem-solving, and self-monitoring.• Poor insight and self-awareness.• Lack of initiative.• Socially inappropriate behavior.• Self-centeredness.• Verbal aggression and/or irritability.• Emotional lability.• Physical aggression.

• Personal desire• Strong support.• Secure attachment• Meaningful family interactions• “Stay adult” messages• Relearning/retaining social skills and judgment• Encourage the patient to “stay an adult”
Maintaining the 5 C’s:• Elicit compliance, cooperation, communication,
connection, and courage.
Keys to Recovery

• Systems problems• Lack of resources• Lack of support • Few incentives• Professional ambivalence• Uniqueness of brain injury sequelae• Lack of access to care• Politics as usual
Barriers to Recovery

1. Increased patient dependency & changes in family dynamics
2. Cognitive inefficiency3. Social reactions to the patient’s disability4. Emotional disturbances5. Executive disorders6. Financial difficulties
Problems that Families Face (Lezak, 1988)

Needed Family Changes
• Develop a clearer definition of what is truly important in life.
• Increase communication with others who have been previously out of touch.
• Increase sensitivity to others who face challenges.• Enhanced ability to face & overcome substantial
personal challenges.• More open & honest communication among friends &
family.• Increased capacity to develop a deeper & more
constructive perspective on problems in life. • Enhanced ability to focus on what is important in the
present & to plan for the future.

Needed Patient Changes: Becoming Socially Adept Again
• Listening– Verbal– Body Language
• Communicating– What is said– What is meant
• Managing feelings– Anger– Anxiety
• Practicing apologizing

The Do’s and Don’ts
Do
For Attention:
1. Call a person by name2. Touch for attention3. Make eye contact4. Give one command
For Rehabilitation:
5. Make the exercise meaningful for generalization to occur6. Use hands on exercises7. Use interactive exercises8. Accountability9. Daily/weekly checkups
For Retention:
10. Use a notebook and have person write down information discussed11. If the person can’t write, use a tape recorder or write for him/her12. Have meaningful practices
Goals:
13. Fit the program to the person14. Realistic15. Time-limited16. Person involved 17. Family involved18. Focus on the Process19. Be related
Don’t
For Attention:
1. Don’t use name2. Don’t touch 3. Don’t look4. Use multiple commands
For Rehabilitation:
5. Use abstract exercises with no generalization6. Use computer exercises7. Use solitary exercises8. No accountability9. Few follow-ups
For Retention:
10. Wing it11. Wing it12. No practices required
Goals:
13. Fit the person to the program14. Unrealistic15. Open-ended16. Person informed17. Family informed18. Focus on the Content19. Be instructive

Educational Interventions
1. Determine basic skill levels in reading, math, and written language.
2. Avoid the traditional classroom setting.3. Reduce reliance on written/printed materials that
require reading.4. Rely on materials that are picture/action oriented.5. Increase interactive learning.6. Encourage repetition.7. Make it meaningful.8. Make it enjoyable.9. Use learning aids.10. Encourage inclusion.

Individual/Group Interventions1. Don’t assume anything, find out.2. Use learning aids—
a. Notebooksb. computersc. tape recorders
2. Make it relevant3. Teach basic feelings.4. Teach logical thinking.5. Encourage sharing of experiences.6. Teach coping strategies.7. Teach compensatory strategies. 8. Teach anger management.9. Teach social skills.10. Rebuild self-esteem.11. Encourage inclusion

Marital/Family Interventions 1. Keep spouse/family informed.2. Encourage interaction/ inclusion.3. Teach communication skills.4. Teach anger management.5. Help build a new role for the veteran in the family.6. Use the RILEE method adapted from Helping Your Angry Child, 2003.
7. Stay on the RILEE Path of family interaction: Polite and Courteous Behavior Respect Trust Comfort Love
The RILEE Side
1. Attachment security 2. Attention (positive)3. Acceptance4. Approval5. Acknowledgement6. Affection
The Angry Side
1. Lack of bonding 2. Negative attention3. Rejection4. Disapproval5. Disregard6. Frustration
Encourage Avoid

Psychopharmacological Interventions for PCS Symptoms
Predominant Symptom Causing Impairment
DSM-IV Classification Possible Therapeutic Agents
Apathy/anergia Personality change due to head trauma/apathetic subtype
Methylphenidate
Dextroamphetamine
Protriptyline
Insomnia Sleep disorder due to head trauma/insomnia subtype
Trazodone
Lorazepam
Clonazepam
Irritability/anger Personality change due to head trauma/aggressive type
Propranolol
Amantidine
Emotional lability Personality change due to head trauma/labile type
Fluoxetine
Nortriptyline
Trazodone
Depression Mood disorder due to head trauma/with depressive features
Fluoxetine
Nortriptyline
Anxiety/restlessness Anxiety disorder due to head trauma/with generalized anxiety
Buspirone
Trazodone
Table 15.2 Postconcussive Symptoms, Diagnosis, and Treatment (from Head Injury and Postconcussive Syndrome by Rizzo & Tranel, 1996.

Vocational Interventions
1. Develop realistic vocational goals.2. Determine the appropriate level of training.3. Set the veteran up for success.4. Help the veteran regain self-respect
and dignity.5. Show the veteran that he/she is valued.6. Encourage inclusiveness.7. Find a meaningful place in society for the
veteran.

Factors Influencing the Course of Rehabilitation
Social Factors
Preinjury Status
Emotional Factors Vocational Factors
Cognitive Functions
CNS Damage
Note: From “The Rehabilitation of Cognitive Disabilities,” by Williams, M. and Long, C. (1987) Plenum Press, New York, NY, p. 81.

A Checklist for Intervention for Individuals
with Executive System Impairment • General Considerations• Appropriateness
– Level of Development– Level of Recovery
• Self-Awareness of Strength and Needs• Goal Setting• Planning• Organizing (see the organizational checklist on next slide)• Self-Initiating• Self-Inhibiting• Self-Monitoring and Evaluating• Problem Solving and Strategic Thinking
Note: From “Cognitive Rehabilitation: Executive Functions,” by M. Ylvisaker, S.Szekeres, and T. Feeney, Traumatic Brain Injury Rehabilitation: Children and Adolescents (2nd ed., p. 260-262), by M. Ylvisaker (Ed.), 1998, Boston: Butterworth-Heinemann. Copyright © 1998 by Butterworth-Heinemann. Adapted with permission.
Adapted from BRIEF-SP

A Checklist for Intervention for Individuals with Organizational Impairment
• Are the individual’s life experiences adequately organized?• Is the content that is used for organizational tasks personally meaningful or directly
related to social, academic, or vocational success?• Are organizing tasks correctly placed on the continuum of involuntary (incidental)
to deliberate (strategic) learning tasks?• Is there an appropriate amount of external organizational support for individuals
who have difficulty organizing?• Is there consistency among staff and family members in how tasks and information
are presented and in the kinds of external organizational support that are provided?
• Do all everyday people understand how to use everyday activities to facilitate improvement in organizational functioning?
• Is there consistency in reducing organizational support as the individual becomes increasingly organized?
• Is the individual as engaged as possible in…
Note: From “Cognitive Rehabilitation: Executive Functions,” by M. Ylvisaker, S. Szekeres, and T. Feeney, Traumatic Brain Injury Rehabilitation: Children and Adolescents (2nd ed., p. 217), by M. Ylvisaker (Ed.), 1998, Boston: Butterworth-Heinemann. Copyright © 1998 by Butterworth-Heinemann. Adapted with permission.
Adapted from BRIEF-SP

Conclusions
• Effective TBI recovery takes years to accomplish. Yet, our VA hospitals are designed and equipped to offer brief screenings and acute care programs for 6 months or less.
• There is simply no room for our young TBI soldiers returning from the wars in Iraq and Afghanistan.
• Many wounded warriors with mild to moderate TBIs are just simply slipping through the cracks.
• The severe TBIs are often un-ignorable; however, after 6 months many severe TBIs find themselves nursing home bound.

Conclusions (continued)• We must address this tragic lack of care for those who gave the
most for their country.• Their future is in our hands. How will we be judged? • Today we must stand up and be accountable. Are we going to do
what is moral or merely what is ethical? • With a competent team and a strong sense of purpose, I know that
we can write grants and develop the programs necessary to establish outpatient clinics in order to complete the TBI/PTSD recovery process with and for our wounded warriors. And I am confident that this can be accomplished in a cost-effective, inclusive manner.
• They kept us safe; now, we must keep them safe, for that is our moral responsibility. Let’s make their American dreams come true. Remember the words of Sgt. Eric Edmundson, “Don’t worry, because if anything happens, the Army will take care of me.”

References
• Angelette, A. (2008, January 23). 2 army vets’ trial defenses allege PTSD. The Advocate, p. 7B.• BRIEF Software Portfolio. Version 300.006 [PARCopS]. Copyright 2008 by Psychological Assessment Resources, Inc. • Chad Ross, N. (2007, February 26). Bob Woodruff: turning personal injury into public inquiry. ABC News.• Dowd, M. (2006, May 31). Live from Baghdad: More dying. The New York Times.• Figueroa, T. (2006, September 20). Officials testify in pretrial hearing for former CP Marine and wife in infant’s death. North
County Times.• H.R. 2199 (2007, May 8). Traumatic Brain Injury Health Enhancement and Long Term Support Act of 2007.• H.R. 2201 (2007, May 16). The Caring for Veterans with Traumatic Brain Injury Act of 2007.• Hamilton, J. (2008). Notes from Mr. Hamilton’s externiship experiences at the Palo Alto and Livermore VA Hospitals.• Hefling, K. (2008). Brain injuries often left untreated. The Advocate.• MacClam, E. (2008, January 20). New cadre of veterans goes homeless. The Advocate, p. 18A.• Maslin, J. (2007, March 12). Visceral tales from Iraq, Where life-changing days are just the start of pain. The New York
Times.• Nemeth, D.G., Ray, K.P., Schexnayder, M.M. (2003). Helping your angry child. New Harbinger Publications, Oakland, CA.• Rizzo, M., and Tranel, D. (1996). Head injury and postconcussive syndrome. Churchill Livingstone. New York, NY.• Pegg, P., Auerbach, S., Seel, R., Buenaver, L.F. (2005). The impact of patient-centered information on patients’ treatment
satisfaction and outcomes in traumatic brain injury rehabilitation. Rehabilitation Psychology, 50(4), pp. 366-374. • Senate Bill 1349 (2007, May 9). Military and Veterans Traumatic Brain Injury Treatment Act.• Sontag, D. and Alvarez, L. (2007, March 12). For war’s gravely injured, challenge to find care. The New York Times.• Stanley, A. (2007, February 27). One man's survival story becomes a rallying cry. The New York Times.• Steinberg, J. (2007, October 25). Recovering from injury, returning to TV, speaking for the wounded. The New York Times.• Taber, K.H., Warden, D.L., Hurley, R.A. (2006). Blast related traumatic brain injury: what is known? Journal of
Neuropsychiatry and Clinical Neuroscience. 18(2). pp. 141-145.• Warden, D. (2006). Military TBI during the Iraq and Afghanistan wars. Journal of Head Trauma and Rehabilitation, 21(5),
pp. 398-402.• Williams, M., and Long, C. (1987). The rehabilitation of cognitive disabilities. Plenum Press. New York, NY.• Ylvisaker, M., Szekeres, S., and Feeney, T., Cognitive rehabilitation: executive functions. Traumatic Brain Injury
Rehabilitation: Children and Adolescents (2nd ed., p. 217, 206-262), by Ylvisaker, M. (Ed.), 1998, Boston: Butterworth-Heinemann. Copyright © 1998 by Butterworth-Heinemann.