Embed Size (px)
Citation preview

Official reprint from UpToDatewww.uptodate.com ©2017 UpToDate, Inc. and/or its affiliates. All Rights Reserved.
Comprehensive geriatric assessment for patients with cancer
Authors: Arti Hurria, MD, Harvey Jay Cohen, MDSection Editors: Reed E Drews, MD, Kenneth E Schmader, MDDeputy Editor: Sadhna R Vora, MD
All topics are updated as new evidence becomes available and our peer review process is complete.Literature review current through: Sep 2017. | This topic last updated: Jun 22, 2017.
INTRODUCTION — Approximately 60 percent of new cases and 70 percent of mortality from canceroccur in patients ≥65 years of age [1]. As a result, the care of older patients constitutes an importantpart of the everyday practice for the adult oncologist.
Despite the high incidence of cancer in this group, older patients have been underrepresented inclinical trials that set the standards for care in oncology practice [2-4]. Less data exist regarding therisks and benefits of cancer treatment in this population, and there are few guidelines that specificallyaddress the evaluation and treatment of the older patient.
Older patients are less likely to receive all types of standard cancer therapies compared with youngerindividuals [5-12]. Possible reasons include concerns regarding increased toxicity, competing causesof morbidity and mortality, lack of access to care, and clinician or patient preference.
Chronologic age alone provides relatively little information regarding an individual's tolerance tocancer treatment. Among patients of the same age, there is wide heterogeneity in the ability toundergo aggressive therapy.
Identifiable comorbid conditions and organ-specific physiologic changes due to aging can limit apatient's ability to tolerate cancer therapy. In addition, the aging process can be associated withdecreased physiologic reserve affecting multiple systems. This can be manifested as frailty and caninterfere with the functional status of the patient, even in the absence of specific comorbidities. Themanifestations of frailty include various components of weight loss, exhaustion, weakness, relativeimmobility, and a general decrease in physical activity.
There is a need to identify the seemingly frail older individual who is likely to benefit from and toleratestandard therapy, as well as the seemingly fit older individual who is apt to experience undue sideeffects and requires a modified treatment plan. The evaluation of frailty in older adults (clinical andpotential physiologic predictors) is discussed separately. (See "Failure to thrive in elderly adults:Evaluation", section on 'Frailty'.)
Information about specific issues may guide interventions that can improve the ability to undergocancer treatment. A comprehensive geriatric assessment (CGA) looking at all of the factors that caninfluence the outcome of therapy is useful in addressing these needs.
The key components of a CGA as applied to patients with cancer will be reviewed here, along with
®
Comprehensive geriatric assessment for patients with cancer - U... https://www.uptodate.com/contents/comprehensive-geriatric-ass...
1 z 27 22.10.2017, 20:26
the different approaches for obtaining this information. A more detailed discussion of the CGA,general aspects of the treatment of cancer in the older adult patients, and the management of olderadult patients with specific types of cancer are presented separately. (See "Comprehensive geriatricassessment" and "Systemic chemotherapy for cancer in elderly persons".)
POTENTIAL BENEFITS — A CGA is a standard part of a geriatrician's baseline evaluation of anolder individual. Several studies have suggested a wide range of possible benefits from using a CGAin patients with cancer. These include (see 'Use of CGA results' below):
Who needs a CGA? — Consensus guidelines from both the National Comprehensive CancerNetwork (NCCN) and the International Society for Geriatric Oncology (SIOG) recommend the routineuse of a geriatric assessment for the older patient with cancer (defined as age 65 or older) [31,32].However, although a CGA is helpful for clinicians to develop a coordinated plan for cancer treatmentand to guide appropriate interventions for specific problems, it can be time consuming and may notbe practical for all patients. Nevertheless, in our practice, we utilize a CGA in every patient age 65and older, using a mainly self-administered CGA assessment tool, as described in more detail below[33]. (See 'Self-administered CGA' below.)
Pre-CGA screening tools — Some, including the SIOG, have suggested the use of a screening toolto identify vulnerable patients for whom a CGA could potentially optimize their cancer treatment[32,34]. Multiple approaches have been made to develop "simplified CGAs" (assessment ofautonomy, malnutrition, depression, cognition, and comorbidity), which are intended to be quickscreening tools to determine who could benefit from a full CGA [34].
Predicting complications and side effects from treatment [13-19]●
Estimating survival [17,18,20,21]●
Assisting in cancer treatment decisions [22-24]●
Detecting problems not found by routine history and physical examination in the initial evaluation[18,24-28]
●
Identification and treatment of new problems during follow-up care [27,29]●
Improving mental health and well being [30]●
Better pain control [30]●
An abbreviated CGA was developed by performing a retrospective chart review of 500 patientswho underwent a geriatric assessment consisting of an evaluation of functional status (Activitiesof Daily Living [ADLs] and Instrumental Activities of Daily Living [IADLs]), cognition (MMSE), andpsychological state (Geriatric Depression Scale). The authors identified 15 items from thesescales that demonstrated the highest item to total correlation [35].
●
Another alternative tool is the Vulnerable Elders Survey-13 (VES-13) (table 1) [36-39]. Thisapproach utilizes a function-based scoring system that considers age, self-rated health, physicallimitations, and functional disabilities.
●
Other instruments include the French G8 tool [40] and the Flemish version of the Triage RiskScreening Tool (fTRST) [41]. One group used both tools to screen 937 patients aged 70 or olderwith a malignant tumor and a new cancer event requiring a treatment decision [42]. Both toolsshowed high sensitivity for detecting patients with a geriatric risk profile (as determined by formal
●
Comprehensive geriatric assessment for patients with cancer - U... https://www.uptodate.com/contents/comprehensive-geriatric-ass...
2 z 27 22.10.2017, 20:26
All frailty screening methods, including the VES-13, have a limited power to predict outcome of aCGA. A systematic review of several frailty screening methods, including the VES-13, concluded thatthey all had limited specificity and that the negative predictive value of the most sensitive screeningtool was only 60 percent [43]. Nevertheless, a prospective study of 1021 patients with cancerevaluated four frailty tools (Balducci [44], SIOG 1 and 2 [45,46], and Ferrat [47]) and found that eachhad good prognostic ability to predict six-month unscheduled admissions and one-year mortality,suggesting that such tools may be helpful in decision-making regarding cancer treatments in olderpatients [48]. (See "Frailty", section on 'Instruments developed to assess frailty'.)
These tools are not intended to be a CGA or replace the need for one. They do not really identifyissues that can be followed up specifically to try to improve outcomes. While they have been used forprognostication and probably work almost as well as a full CGA for that, they do not substitute for aCGA for all purposes.
DOMAINS OF A CGA — The typical domains of a CGA include evaluations of functional status,comorbid medical conditions, cognitive status, psychological state, social support, nutritional status,and a review of the medication list.
Impaired functional status and significant comorbidity can have significant effects on the ability toadminister systemic chemotherapy in the older adult patient. (See "Systemic chemotherapy forcancer in elderly persons".)
Functional status — Functional status refers to a patient's ability to perform routine daily tasks. Thecommonly used performance status scores (eg, Karnofsky or Eastern Cooperative Oncology Group(ECOG) scales (table 2 and table 3)) tend to underrepresent the degree of functional impairment inthe older patient [26].
A more comprehensive understanding of an older patient's functional state can be obtained by theActivities of Daily Living (ADL) and Instrumental Activities of Daily Living (IADL) scales. ADLs are theskills that are necessary for basic living, and include feeding, grooming, transferring, and toileting.IADLs are required to live independently in the community and include activities such as shopping,managing finances, housekeeping, preparing meals, and taking medications. In a study of 363cancer patients aged ≥65 years, an ECOG performance status <2 (table 3) was associated withlimitations of ADL and IADL in 9 and 38 percent of patients, respectively [26]. The frequency of IADLlimitations was more common in patients aged ≥80 years.
Functional disability is common in older patients with cancer. This was illustrated by a nationalsample of 9745 community-based Medicare beneficiaries, in which older adults with cancer had morelimitations in ADLs, IADLs, and greater health care utilization than individuals without cancer [49].
Similar results were seen in another study of 303 patients aged ≥65 years with solid tumors orhematologic malignancies, in which limitations in ADLs and IADLs were found in 17 and 59 percentof patients, respectively [50].
The impact of functional status on the overall survival of older patients with cancer was illustrated bya study of 566 patients with advanced non-small cell lung cancer age ≥70 years receivingchemotherapy [20]. In this study, improved overall survival was associated with independence inperforming IADLs (p = 0.04) and higher quality of life (p = 0.0003) scores. Limitations in basic ADLsand the presence of comorbidity were not predictors of a decrease in overall survival.
geriatric assessment, which was carried out in all patients) and were prognostic for functionaldecline during therapy and higher mortality rates.
Comprehensive geriatric assessment for patients with cancer - U... https://www.uptodate.com/contents/comprehensive-geriatric-ass...
3 z 27 22.10.2017, 20:26
Impaired functional status is associated with an increased risk of toxicity due to chemotherapy. Thiswas demonstrated in two multicenter studies that identified predictors of chemotherapy toxicity[14,15]. In both of these studies, the patient’s functional status was a key predictor.
In the study by the Cancer and Aging Research Group, the functional measures that predictedchemotherapy toxicity risk included falls in the last six months, limitations in walking one block, needfor assistance with taking medications, and decreased social activities [15]. The Chemotherapy RiskAssessment Scale for High-Age Patients (CRASH) score identified the need for assistance withIADLs as a predictor of chemotherapy toxicity. Another study of patients aged ≥70 years with ovariancancer who were receiving carboplatin and cyclophosphamide identified functional dependence(defined as living at home with assistance or living with medical assistance in a specializedinstitution) and ECOG performance status ≥2 as predictors of chemotherapy toxicity [13].
Comorbidity — Comorbidity represents the extent of an individual's physical and psychologicaldisease in addition to the disease for which he or she is seeking treatment [51]. As an individualages, the number of comorbid medical conditions increases [52]. The impact of these comorbidmedical conditions on life expectancy and treatment tolerance should be considered when estimatingthe risks and benefits of treatment [53].
The importance of comorbidity is illustrated by analyses from three large series:
In addition to its effect on survival, the presence of comorbid medical conditions also affects apatient's ability to tolerate cancer therapy. In a study of patients aged ≥70 years with advanced non–small cell lung cancer, for example, those with a Charlson Comorbidity Index of ≥2 were more likelyto discontinue chemotherapy early than patients with a comorbidity score <2 [57].
An assessment of comorbid medical conditions can provide information that is independent of theindividual's functional status. This was illustrated by a study of 203 older patients with cancer, inwhom there was little or no correlation between comorbidity (as measured by either the CharlsonComorbidity Index or Cumulative Illness Rating Scale – Geriatric) and functional status (as assessedby ECOG performance status or ADLs). Thus it is important to assess comorbidity as well asfunctional status [58].
Cognitive function — Cognitive function is another important component of the overall assessment
A longitudinal observational study of 936 women with breast cancer ages 40 to 84 found thatpatients who had three or more comorbid medical conditions had a 20-fold higher rate ofmortality from causes other than breast cancer and a four-fold higher all-cause mortality ratecompared with those who had no comorbid medical conditions [54].
●
A second report analyzed 1255 patients with non-small cell lung cancer who were enrolled intwo randomized trials conducted by the National Cancer Institute of Canada [55]. Patients atleast 65 years of age were significantly more likely to have a Charlson Comorbidity Index score≥1 than younger patients (42 versus 26 percent) (table 4). Although age was not an independentfactor influencing survival, comorbidity, as evidenced by a Charlson Comorbidity Index score ≥1,was associated with increased mortality (hazard ratio [HR] 1.28, 95% CI 1.09-1.50).
●
A third study analyzed the impact of comorbidity using three different instruments in a series of496 patients (mean age, 67 years) undergoing surgery for colorectal cancer [56]. Analysis usingthe Charlson Comorbidity Index, the National Institute on Aging and National Cancer InstituteComorbidity Index, and the Adult Comorbidity Evaluation-27 all found that patients with thehighest comorbidity burden had the poorest overall and colon cancer-specific survival.
●
Comprehensive geriatric assessment for patients with cancer - U... https://www.uptodate.com/contents/comprehensive-geriatric-ass...
4 z 27 22.10.2017, 20:26
of the geriatric patient with cancer. (See "Evaluation of cognitive impairment and dementia".)
In the general geriatric population, dementia is an independent prognostic factor for survival. Thepresence of dementia influences the likelihood of both cancer diagnosis and treatment [59]. In apopulation cohort study using the Surveillance, Epidemiology and End Results (SEER) Medicaredatabase, patients with invasive colon cancer and dementia were more likely to have a cancerdiagnosis reported after death based upon either an autopsy or death certificate than patients whodid not have dementia [60]. In addition, patients with dementia were less likely to have a biopsy-proven diagnosis of cancer and were less likely to receive surgery or chemotherapy. In another studyusing the SEER database, patients with Alzheimer disease and breast cancer were more likely to bediagnosed with a later stage of breast cancer and were less likely to receive treatment for theirmalignancy [61].
From a practical standpoint, an assessment of cognitive status is important prior to beginningchemotherapy treatment in order to ensure that the patient can comply with instructions regardingsupportive medications or oral chemotherapy, and in order to understand and remember to seekmedical attention if side effects develop.
Nutrition — Nutritional status is an important prognostic factor in all geriatric patients. (See "Dietaryassessment in adults".)
In the general older population, there are several reports demonstrating the adverse impact of weightloss or low body mass index (BMI) even when subjects do not have cancer (figure 1) [62-66]. Theimportance of weight loss was illustrated by a study of 4714 community-dwelling adults age ≥65years, in which weight loss ≥5 percent was associated with an increased risk of mortality [62]. Similarresults were seen in another study of 7527 individuals age ≥70 years, in which a BMI <19.4 kg/m(the lowest 10 percent of the population) was associated with an increased risk of mortality [63].
Among patients with cancer, the deleterious effect of weight loss on survival was demonstrated in astudy of 3047 patients enrolled in 12 ECOG chemotherapy protocols [67]. In this analysis, weightloss was an independent prognostic factor for survival and was associated with a lower performancestatus. Furthermore, weight loss was associated with a decrease in chemotherapy response rates inwomen with breast cancer, although this correlation was not present in other tumor types. Even alimited weight loss (0 to 5 percent) can be clinically significant in patients with cancer.
Thus, the adverse effects of weight loss and low BMI have been demonstrated in all older patientsincluding those with cancer. Future studies are needed to determine whether nutritional interventioncan decrease these risks. (See "Pathogenesis, clinical features, and assessment of cancer cachexia"and "Pharmacologic management of cancer anorexia/cachexia".)
Psychological state and social support — Although the incidence and severity of psychologicaldistress are reported to be less than that observed in younger patients [68,69], approximately one-third of older patients with cancer experience psychological distress. (See "Diagnosis of psychiatricdisorders in patients with cancer".)
This most typically takes the form of depression. The prevalence of clinically significant depression isestimated to be 3 to 25 percent in the older population with cancer [68]. The consequences ofdepression in this group include an increased risk of subsequent functional decline and withincreased utilization of healthcare resources [70]. This was illustrated in a survey of 6649 patientsaged >70 years, in which the presence of increasing numbers of depressive symptoms wasassociated with a need for more hours of informal caregiving [71].
2
Comprehensive geriatric assessment for patients with cancer - U... https://www.uptodate.com/contents/comprehensive-geriatric-ass...
5 z 27 22.10.2017, 20:26
The patients who are most vulnerable to psychological distress are those with inadequate socialsupport. This was illustrated by a study of breast cancer survivors, in which older age was associatedwith less distress [72]. However, patients with less adequate social support experienced increaseddistress. In addition, social isolation is also an independent predictor of mortality in the geriatricpopulation [73].
Medication review — For older patients with cancer, careful review of medications is an importantcomponent of a CGA. Regular and comprehensive review of all medications (both prescription andover the counter) is needed to remove any unnecessary or potentially inappropriate medications andto assess for potential drug interactions [74-76]. As an example, the diagnosis of terminal cancershould prompt the discontinuation of certain drugs that are no longer potentially beneficial, such aslipid-lowering medications [77].
Physiologic changes associated with aging can have a major impact on drug pharmacokinetics andpharmacodynamics. With aging, body fat increases, total body water and renal function decrease,and hepatic mass and blood flow decrease. In addition, the number of medications that an individualtakes also increases. This combination of age-related changes in physiology and polypharmacy isassociated with an increased risk of adverse drug events in the older patient. (See "Drug prescribingfor older adults".)
Older adults with cancer are particularly prone to medication errors attributed to medication changes,complex regimens, and incomplete information handoff between providers [78]. Cancer-relatedtherapy adds to the use of multiple medications and/or the consumption of potentially inappropriatemedications and compounds the risk for adverse drug effects, drug-drug interactions, andnonadherence as a result of increased pill burden and regimen complexity [79,80]. In onepharmacist-led medication review of 248 ambulatory senior adults with cancer who were receiving ageriatric oncology assessment over an 18-month period, the mean number of medications used was9.23, and 43 percent were receiving more than 10 medications [80]. The prevalence of potentiallyinappropriate medication use (as assessed by 2012 Beers criteria, Screening Tool of Older Person’sPrescriptions [STOPP], and the Healthcare Effectiveness Data and Information Set [HEDIS]) was 51percent. (See "Drug prescribing for older adults", section on 'Inappropriate medications'.)
OBTAINING PATIENT DATA — Although consensus guidelines recommend that older patients withcancer undergo a CGA, there is no consensus regarding an optimal tool [31,81]. The variousapproaches that have been studied recognize the limited resources available in an oncology practice,and several different methods of obtaining this information have been explored. These screeningtools can potentially identify older adults who would benefit from a more thorough evaluation orcollaborative care with a geriatrician. Here we will briefly review several assessment methods.
Mailed CGA — A self-reported, mailed CGA was evaluated in a population of male oncology patients(mean age 68, range 42 to 87) at the Durham, North Carolina Veterans Administration MedicalCenter [82]. The assessment evaluated functional status, pain, financial wellbeing, social support,psychological state, spiritual wellbeing, and quality of life (table 5).
The CGA was sent to participants prior to their initial clinic visit, and 76 percent of patients kept theirclinic visit and returned the assessment. The mailed CGA was effective in capturing salientinformation about the different assessment domains. For example, 58 percent of patients requiredassistance with one or more instrumental activities of daily living (IADLs), 61 percent requiredassistance with one or more activities of daily living (ADLs), the mean number of comorbid medicalconditions was five, and the mean number of medications was six.
Comprehensive geriatric assessment for patients with cancer - U... https://www.uptodate.com/contents/comprehensive-geriatric-ass...
6 z 27 22.10.2017, 20:26

Self-administered CGA — Investigators from the Cancer and Leukemia Group B (CALGB), Cancerin the Elderly Committee, developed a CGA that is primarily self-administered [33]. This assessmentis a compilation of well-validated instruments that evaluate functional status, comorbidity, cognition,nutritional status, psychological state, social support, and medication use (table 6).
Three of the instruments are performed by the healthcare provider: the Blessed Orientation-Memory-Concentration Test (a measure of cognition), Timed Up and Go (a performance-based measure offunctional status), and Karnofsky performance status (table 2). The remainder of the assessment isself-administered by the patient.
Pilot data demonstrate that the mean time to complete the assessment is 27 minutes, and 78 percentof participants could complete the self-administered portion on their own. Overall, 90 percent ofparticipants were satisfied with the length of the questionnaire, 83 percent reported that it was easyto understand, and 100 percent stated that there were no upsetting items [33]. The CALGB, Cancerin the Elderly Committee evaluated the feasibility of including this primarily self-administeredassessment in CALGB trials [15]. The median time to complete the geriatric assessment tool was 22minutes. The majority (87 percent) of patients completed the assessment without assistance.Furthermore, patient satisfaction with the questionnaire was high (92 percent reported satisfactionwith the questionnaire length, 95 percent reported no difficult questions, and 96 percent reported noupsetting questions). The assessment met the feasibility criteria specified in the protocol for inclusionin future cooperative group studies.
Clinical interview — A third approach, using a clinical interview for the CGA, was evaluated in 30patients aged 65 and older with a variety of tumor types [83]. The Multidimensional AssessmentProtocol for Cancer (MACE) includes an evaluation of the socioeconomic status, cognitive status,depression, physical performance, disability, and tumor characteristics (table 7). The mean time foradministering the MACE was 27 minutes.
USE OF CGA RESULTS — The information from the CGA can be used in a number of ways toassist in decision-making regarding overall management of the older patient with cancer. Asexamples:
Some authors have classified the older population into specific groups for the purpose ofselecting the treatment strategy, based upon their functional status, rehabilitative potential, lifeexpectancy, and tolerance of stress (table 8 and algorithm 1) [84-87].
●
Others have developed tools such as prognostic indices and nomograms based upon domainsand elements of the CGA that predict the probability of one-, two- and three-year overall survivalfor older adult patients with cancer [88,89].
●
A frailty index derived from information gleaned from the CGA has been used to predict thelikelihood of discontinuing chemotherapy and hospitalization in older patients [90].
●
In older adults with lung cancer, chemotherapy treatment allocation based on CGA results isassociated with reduced treatment toxicity and treatment failures compared with treatmentallocated based on performance status and age alone [19].
●
The information obtained from the CGA has also been combined with other information,including the proposed chemotherapy regimen, hematologic and renal function, hearingimpairment, and cancer type, to derive a model used to predict chemotherapy toxicity in theolder adult population (table 9 and table 10) [15]. This predictive model was developed (studyinga cohort of 500 patients) [15] and validated (in a cohort of 250 patients) in a prospective
●
Comprehensive geriatric assessment for patients with cancer - U... https://www.uptodate.com/contents/comprehensive-geriatric-ass...
7 z 27 22.10.2017, 20:26
There have been few studies that have evaluated whether routine geriatric assessment impactsoutcomes or influences treatment decision-making in older patients with cancer. A systematic reviewof 34 studies of geriatric assessment in older cancer patients included 18 prospective, 11 cross-sectional, and five retrospective studies; none of the included studies were randomized trialsspecifically designed to examine the effectiveness of geriatric assessment with regard to medicaldecision-making [93]. Specific domains of the geriatric assessment were associated with outcomesor treatment decisions as follows:
The authors concluded that further research examining the impact of geriatric assessment ontreatment decisions and oncologic outcomes is needed, particularly randomized trials.
SUMMARY AND RECOMMENDATIONS
multicenter trial [91]. (See "Systemic chemotherapy for cancer in elderly persons", section on'Models predicting chemotherapy toxicity and early death'.)
A cohort of geriatric oncology experts developed algorithms for geriatric assessment-guided careprocesses and developed geriatric assessment-guided interventions. Impairment in a specificgeriatric assessment domain could influence cancer treatment decision-making [92].
●
Three studies focusing on treatment decision-making impact found that treatment decisionswere changed for fewer than one-half of patients who underwent geriatric assessment.
●
Seven studies examining the predictive ability of the CGA for treatment toxicity/complicationsreported conflicting findings.
●
Eleven studies addressing CGA predictions of mortality concluded that difficulty withinstrumental activities of daily living (IADLs), poor performance status, and more numerousgeriatric assessment deficits were associated with higher mortality.
●
Cancer is an important and disproportionate cause of morbidity and mortality in the geriatricpopulation. A comprehensive geriatric assessment (CGA) can help achieve the required balancebetween the potential benefits and side effects of therapy. (See "Comprehensive geriatricassessment".)
●
The key domains that are included in the CGA are the functional status, comorbidity, cognition,nutrition, psychological state, social support, and medication review. Various approaches togathering this information have been used including a mailed or self-administered assessment.(See 'Domains of a CGA' above.)
●
Randomized trials are needed to examine the effectiveness of geriatric assessment in olderpatients with cancer. However, despite the absence of randomized trials showing that routinegeriatric assessment impacts outcomes or influences treatment decision-making in olderpatients with cancer, we suggest a CGA for every oncology patient age 65 and older (Grade2C). (See 'Who needs a CGA?' above.)
●
We utilize a CGA that is primarily self-administered [33]. This assessment is a compilation ofwell-validated instruments that evaluate functional status, comorbidity, cognition, nutritionalstatus, psychological state, social support, and medication use (table 6). Three of theinstruments are performed by the healthcare provider: the Blessed Orientation-Memory-Concentration Test (a measure of cognition), Timed Up and Go (a performance-based measureof functional status), and Karnofsky performance status (table 2). The remainder of theassessment is self-administered by the patient. (See 'Self-administered CGA' above.)
●
Comprehensive geriatric assessment for patients with cancer - U... https://www.uptodate.com/contents/comprehensive-geriatric-ass...
8 z 27 22.10.2017, 20:26

Use of UpToDate is subject to the Subscription and License Agreement.
REFERENCES
Ries EM, Kosary CL, Hankey BF, et al. SEER Cancer Statistics Review: 1975-2000. National Cancer Institute, Bethesda, MD.
1.
Hutchins LF, Unger JM, Crowley JJ, et al. Underrepresentation of patients 65 years of age orolder in cancer-treatment trials. N Engl J Med 1999; 341:2061.
2.
Yee KW, Pater JL, Pho L, et al. Enrollment of older patients in cancer treatment trials inCanada: why is age a barrier? J Clin Oncol 2003; 21:1618.
3.
Trimble EL, Carter CL, Cain D, et al. Representation of older patients in cancer treatment trials.Cancer 1994; 74:2208.
4.
Christman K, Muss HB, Case LD, Stanley V. Chemotherapy of metastatic breast cancer in theelderly. The Piedmont Oncology Association experience [see comment]. JAMA 1992; 268:57.
5.
Hurria A, Leung D, Trainor K, et al. Factors influencing treatment patterns of breast cancerpatients age 75 and older. Crit Rev Oncol Hematol 2003; 46:121.
6.
Mandelblatt JS, Hadley J, Kerner JF, et al. Patterns of breast carcinoma treatment in olderwomen: patient preference and clinical and physical influences. Cancer 2000; 89:561.
7.
Newcomb PA, Carbone PP. Cancer treatment and age: patient perspectives. J Natl Cancer Inst1993; 85:1580.
8.
Merchant TE, McCormick B, Yahalom J, Borgen P. The influence of older age on breast cancertreatment decisions and outcome. Int J Radiat Oncol Biol Phys 1996; 34:565.
9.
Bergman L, Dekker G, van Leeuwen FE, et al. The effect of age on treatment choice andsurvival in elderly breast cancer patients. Cancer 1991; 67:2227.
10.
Bergman L, Kluck HM, van Leeuwen FE, et al. The influence of age on treatment choice andsurvival of elderly breast cancer patients in south-eastern Netherlands: a population-basedstudy. Eur J Cancer 1992; 28A:1475.
11.
Schrag D, Cramer LD, Bach PB, Begg CB. Age and adjuvant chemotherapy use after surgeryfor stage III colon cancer. J Natl Cancer Inst 2001; 93:850.
12.
Freyer G, Geay JF, Touzet S, et al. Comprehensive geriatric assessment predicts tolerance tochemotherapy and survival in elderly patients with advanced ovarian carcinoma: a GINECOstudy. Ann Oncol 2005; 16:1795.
13.
Extermann M, Boler I, Reich RR, et al. Predicting the risk of chemotherapy toxicity in olderpatients: the Chemotherapy Risk Assessment Scale for High-Age Patients (CRASH) score.Cancer 2012; 118:3377.
14.
Hurria A, Togawa K, Mohile SG, et al. Predicting chemotherapy toxicity in older adults withcancer: a prospective multicenter study. J Clin Oncol 2011; 29:3457.
15.
Extermann M, Bonetti M, Sledge GW, et al. MAX2--a convenient index to estimate the averageper patient risk for chemotherapy toxicity; validation in ECOG trials. Eur J Cancer 2004;
16.
The information from a geriatric assessment can be used to anticipate and manage toxicity fromtreatment, predict survival, uncover unexpected health problems, improve mental health andwellbeing, and improve pain control. (See 'Potential benefits' above.)
●
Comprehensive geriatric assessment for patients with cancer - U... https://www.uptodate.com/contents/comprehensive-geriatric-ass...
9 z 27 22.10.2017, 20:26

40:1193.
Ramjaun A, Nassif MO, Krotneva S, et al. Improved targeting of cancer care for older patients:a systematic review of the utility of comprehensive geriatric assessment. J Geriatr Oncol 2013;4:271.
17.
Hamaker ME, Prins MC, Stauder R. The relevance of a geriatric assessment for elderly patientswith a haematological malignancy--a systematic review. Leuk Res 2014; 38:275.
18.
Corre R, Greillier L, Le Caër H, et al. Use of a Comprehensive Geriatric Assessment for theManagement of Elderly Patients With Advanced Non-Small-Cell Lung Cancer: The Phase IIIRandomized ESOGIA-GFPC-GECP 08-02 Study. J Clin Oncol 2016; 34:1476.
19.
Maione P, Perrone F, Gallo C, et al. Pretreatment quality of life and functional statusassessment significantly predict survival of elderly patients with advanced non-small-cell lungcancer receiving chemotherapy: a prognostic analysis of the multicenter Italian lung cancer inthe elderly study. J Clin Oncol 2005; 23:6865.
20.
Klepin HD, Geiger AM, Tooze JA, et al. Geriatric assessment predicts survival for older adultsreceiving induction chemotherapy for acute myelogenous leukemia. Blood 2013; 121:4287.
21.
Tucci A, Ferrari S, Bottelli C, et al. A comprehensive geriatric assessment is more effective thanclinical judgment to identify elderly diffuse large cell lymphoma patients who benefit fromaggressive therapy. Cancer 2009; 115:4547.
22.
Cudennec T, Gendry T, Labrune S, et al. Use of a simplified geriatric evaluation in thoraciconcology. Lung Cancer 2010; 67:232.
23.
Kenis C, Bron D, Libert Y, et al. Relevance of a systematic geriatric screening and assessmentin older patients with cancer: results of a prospective multicentric study. Ann Oncol 2013;24:1306.
24.
Balducci L, Extermann M. Management of cancer in the older person: a practical approach.Oncologist 2000; 5:224.
25.
Repetto L, Fratino L, Audisio RA, et al. Comprehensive geriatric assessment adds informationto Eastern Cooperative Oncology Group performance status in elderly cancer patients: anItalian Group for Geriatric Oncology Study. J Clin Oncol 2002; 20:494.
26.
Extermann M, Meyer J, McGinnis M, et al. A comprehensive geriatric intervention detectsmultiple problems in older breast cancer patients. Crit Rev Oncol Hematol 2004; 49:69.
27.
Pope D, Ramesh H, Gennari R, et al. Pre-operative assessment of cancer in the elderly(PACE): a comprehensive assessment of underlying characteristics of elderly cancer patientsprior to elective surgery. Surg Oncol 2006; 15:189.
28.
Chen H, Cantor A, Meyer J, et al. Can older cancer patients tolerate chemotherapy? Aprospective pilot study. Cancer 2003; 97:1107.
29.
Rao AV, Hsieh F, Feussner JR, Cohen HJ. Geriatric evaluation and management units in thecare of the frail elderly cancer patient. J Gerontol A Biol Sci Med Sci 2005; 60:798.
30.
Extermann M, Aapro M, Bernabei R, et al. Use of comprehensive geriatric assessment in oldercancer patients: recommendations from the task force on CGA of the International Society ofGeriatric Oncology (SIOG). Crit Rev Oncol Hematol 2005; 55:241.
31.
Decoster L, Van Puyvelde K, Mohile S, et al. Screening tools for multidimensional healthproblems warranting a geriatric assessment in older cancer patients: an update on SIOGrecommendations†. Ann Oncol 2015; 26:288.
32.
Hurria A, Gupta S, Zauderer M, et al. Developing a cancer-specific geriatric assessment: a33.
Comprehensive geriatric assessment for patients with cancer - U... https://www.uptodate.com/contents/comprehensive-geriatric-ass...
10 z 27 22.10.2017, 20:26

feasibility study. Cancer 2005; 104:1998.
Valero S, Migeot V, Bouche G. Who needs a Comprehensive Geriatric Assessment? A FrenchOnco-Geriatric Screening tool. J Geriatric Oncol 2011; 2:130.
34.
Overcash JA, Beckstead J, Extermann M, Cobb S. The abbreviated comprehensive geriatricassessment (aCGA): a retrospective analysis. Crit Rev Oncol Hematol 2005; 54:129.
35.
Min LC, Elliott MN, Wenger NS, Saliba D. Higher vulnerable elders survey scores predict deathand functional decline in vulnerable older people. J Am Geriatr Soc 2006; 54:507.
36.
Mohile SG, Bylow K, Dale W, et al. A pilot study of the vulnerable elders survey-13 comparedwith the comprehensive geriatric assessment for identifying disability in older patients withprostate cancer who receive androgen ablation. Cancer 2007; 109:802.
37.
Luciani A, Ascione G, Bertuzzi C, et al. Detecting disabilities in older patients with cancer:comparison between comprehensive geriatric assessment and vulnerable elders survey-13. JClin Oncol 2010; 28:2046.
38.
Spyropoulou D, Pallis AG, Leotsinidis M, Kardamakis D. Completion of radiotherapy isassociated with the Vulnerable Elders Survey-13 score in elderly patients with cancer. J GeriatrOncol 2014; 5:20.
39.
Bellera CA, Rainfray M, Mathoulin-Pélissier S, et al. Screening older cancer patients: firstevaluation of the G-8 geriatric screening tool. Ann Oncol 2012; 23:2166.
40.
Kenis C, Geeraerts A, Braes T. The Flemish version of the Triage Risk Screening Tool. Crit RevOncol Hematol 2006; 60 (suppl 1):31.
41.
Kenis C, Decoster L, Van Puyvelde K, et al. Performance of two geriatric screening tools inolder patients with cancer. J Clin Oncol 2014; 32:19.
42.
Hamaker ME, Jonker JM, de Rooij SE, et al. Frailty screening methods for predicting outcomeof a comprehensive geriatric assessment in elderly patients with cancer: a systematic review.Lancet Oncol 2012; 13:e437.
43.
Balducci L, Beghe C. The application of the principles of geriatrics to the management of theolder person with cancer. Crit Rev Oncol Hematol 2000; 35:147.
44.
Droz JP, Balducci L, Bolla M, et al. Management of prostate cancer in older men:recommendations of a working group of the International Society of Geriatric Oncology. BJU Int2010; 106:462.
45.
Droz JP, Aapro M, Balducci L, et al. Management of prostate cancer in older patients: updatedrecommendations of a working group of the International Society of Geriatric Oncology. LancetOncol 2014; 15:e404.
46.
Ferrat E, Audureau E, Paillaud E, et al. Four Distinct Health Profiles in Older Patients WithCancer: Latent Class Analysis of the Prospective ELCAPA Cohort. J Gerontol A Biol Sci MedSci 2016; 71:1653.
47.
Ferrat E, Paillaud E, Caillet P, et al. Performance of Four Frailty Classifications in Older PatientsWith Cancer: Prospective Elderly Cancer Patients Cohort Study. J Clin Oncol 2017; 35:766.
48.
Stafford RS, Cyr PL. The impact of cancer on the physical function of the elderly and theirutilization of health care. Cancer 1997; 80:1973.
49.
Serraino D, Fratino L, Zagonel V, GIOGer Study Group (Italy). Prevalence of functionaldisability among elderly patients with cancer. Crit Rev Oncol Hematol 2001; 39:269.
50.
Extermann M, Aapro M. Assessment of the older cancer patient. Hematol Oncol Clin North Am51.
Comprehensive geriatric assessment for patients with cancer - U... https://www.uptodate.com/contents/comprehensive-geriatric-ass...
11 z 27 22.10.2017, 20:26

2000; 14:63.
Yancik R. Cancer burden in the aged: an epidemiologic and demographic overview. Cancer1997; 80:1273.
52.
Welch HG, Albertsen PC, Nease RF, et al. Estimating treatment benefits for the elderly: theeffect of competing risks. Ann Intern Med 1996; 124:577.
53.
Satariano WA, Ragland DR. The effect of comorbidity on 3-year survival of women with primarybreast cancer. Ann Intern Med 1994; 120:104.
54.
Asmis TR, Ding K, Seymour L, et al. Age and comorbidity as independent prognostic factors inthe treatment of non small-cell lung cancer: a review of National Cancer Institute of CanadaClinical Trials Group trials. J Clin Oncol 2008; 26:54.
55.
Hines RB, Chatla C, Bumpers HL, et al. Predictive capacity of three comorbidity indices inestimating mortality after surgery for colon cancer. J Clin Oncol 2009; 27:4339.
56.
Frasci G, Lorusso V, Panza N, et al. Gemcitabine plus vinorelbine versus vinorelbine alone inelderly patients with advanced non-small-cell lung cancer. J Clin Oncol 2000; 18:2529.
57.
Extermann M, Overcash J, Lyman GH, et al. Comorbidity and functional status are independentin older cancer patients. J Clin Oncol 1998; 16:1582.
58.
Wolfson C, Wolfson DB, Asgharian M, et al. A reevaluation of the duration of survival after theonset of dementia. N Engl J Med 2001; 344:1111.
59.
Gupta SK, Lamont EB. Patterns of presentation, diagnosis, and treatment in older patients withcolon cancer and comorbid dementia. J Am Geriatr Soc 2004; 52:1681.
60.
Gorin SS, Heck JE, Albert S, Hershman D. Treatment for breast cancer in patients withAlzheimer's disease. J Am Geriatr Soc 2005; 53:1897.
61.
Newman AB, Yanez D, Harris T, et al. Weight change in old age and its association withmortality. J Am Geriatr Soc 2001; 49:1309.
62.
Grabowski DC, Ellis JE. High body mass index does not predict mortality in older people:analysis of the Longitudinal Study of Aging. J Am Geriatr Soc 2001; 49:968.
63.
Wallace JI, Schwartz RS, LaCroix AZ, et al. Involuntary weight loss in older outpatients:incidence and clinical significance. J Am Geriatr Soc 1995; 43:329.
64.
Reynolds MW, Fredman L, Langenberg P, Magaziner J. Weight, weight change, mortality in arandom sample of older community-dwelling women. J Am Geriatr Soc 1999; 47:1409.
65.
Landi F, Onder G, Gambassi G, et al. Body mass index and mortality among hospitalizedpatients. Arch Intern Med 2000; 160:2641.
66.
Dewys WD, Begg C, Lavin PT, et al. Prognostic effect of weight loss prior to chemotherapy incancer patients. Eastern Cooperative Oncology Group. Am J Med 1980; 69:491.
67.
Kua J. The prevalence of psychological and psychiatric sequelae of cancer in the elderly - howmuch do we know? Ann Acad Med Singapore 2005; 34:250.
68.
Vinokur AD, Threatt BA, Vinokur-Kaplan D, Satariano WA. The process of recovery from breastcancer for younger and older patients. Changes during the first year. Cancer 1990; 65:1242.
69.
Penninx BW, Guralnik JM, Ferrucci L, et al. Depressive symptoms and physical decline incommunity-dwelling older persons. JAMA 1998; 279:1720.
70.
Langa KM, Valenstein MA, Fendrick AM, et al. Extent and cost of informal caregiving for olderAmericans with symptoms of depression. Am J Psychiatry 2004; 161:857.
71.
Kornblith AB, Herndon JE 2nd, Weiss RB, et al. Long-term adjustment of survivors of early-72.
Comprehensive geriatric assessment for patients with cancer - U... https://www.uptodate.com/contents/comprehensive-geriatric-ass...
12 z 27 22.10.2017, 20:26

stage breast carcinoma, 20 years after adjuvant chemotherapy. Cancer 2003; 98:679.
Seeman TE, Berkman LF, Kohout F, et al. Intercommunity variations in the association betweensocial ties and mortality in the elderly. A comparative analysis of three communities. AnnEpidemiol 1993; 3:325.
73.
Avorn J, Gurwitz JH. Geriatric Medicine, Springer-Verlag, 1997.74.
Lichtman SM, Villani G. Chemotherapy in the elderly: pharmacologic considerations. CancerControl 2000; 7:548.
75.
Vestal RE. Aging and pharmacology. Cancer 1997; 80:1302.76.
Kutner JS, Blatchford PJ, Taylor DH Jr, et al. Safety and benefit of discontinuing statin therapyin the setting of advanced, life-limiting illness: a randomized clinical trial. JAMA Intern Med2015; 175:691.
77.
Coleman EA, Smith JD, Raha D, Min SJ. Posthospital medication discrepancies: prevalenceand contributing factors. Arch Intern Med 2005; 165:1842.
78.
Puts MT, Costa-Lima B, Monette J, et al. Medication problems in older, newly diagnosed cancerpatients in Canada: How common are they? A prospective pilot study. Drugs Aging 2009;26:519.
79.
Nightingale G, Hajjar E, Swartz K, et al. Evaluation of a pharmacist-led medication assessmentused to identify prevalence of and associations with polypharmacy and potentially inappropriatemedication use among ambulatory senior adults with cancer. J Clin Oncol 2015; 33:1453.
80.
National Comprehensive Cancer Network (NCCN). NCCN Clinical practice guidelines in oncology. http://www.nccn.org/professionals/physician_gls/f_guidelines.asp (Accessed on February 27, 2016).
81.
Ingram SS, Seo PH, Martell RE, et al. Comprehensive assessment of the elderly cancerpatient: the feasibility of self-report methodology. J Clin Oncol 2002; 20:770.
82.
Monfardini S, Ferrucci L, Fratino L, et al. Validation of a multidimensional evaluation scale foruse in elderly cancer patients. Cancer 1996; 77:395.
83.
Hamerman D. Toward an understanding of frailty. Ann Intern Med 1999; 130:945.84.
Caillet P, Canoui-Poitrine F, Vouriot J, et al. Comprehensive geriatric assessment in thedecision-making process in elderly patients with cancer: ELCAPA study. J Clin Oncol 2011;29:3636.
85.
Olivieri A, Gini G, Bocci C, et al. Tailored therapy in an unselected population of 91 elderlypatients with DLBCL prospectively evaluated using a simplified CGA. Oncologist 2012; 17:663.
86.
Spina M, Balzarotti M, Uziel L, et al. Modulated chemotherapy according to modifiedcomprehensive geriatric assessment in 100 consecutive elderly patients with diffuse large B-celllymphoma. Oncologist 2012; 17:838.
87.
Kanesvaran R, Li H, Koo KN, Poon D. Analysis of prognostic factors of comprehensive geriatricassessment and development of a clinical scoring system in elderly Asian patients with cancer.J Clin Oncol 2011; 29:3620.
88.
Brunello A, Fontana A, Zafferri V, et al. Development of an oncological-multidimensionalprognostic index (Onco-MPI) for mortality prediction in older cancer patients. J Cancer Res ClinOncol 2016; 142:1069.
89.
Cohen HJ, Smith D, Sun CL, et al. Frailty as determined by a comprehensive geriatricassessment-derived deficit-accumulation index in older patients with cancer who receive
90.
Comprehensive geriatric assessment for patients with cancer - U... https://www.uptodate.com/contents/comprehensive-geriatric-ass...
13 z 27 22.10.2017, 20:26
chemotherapy. Cancer 2016; 122:3865.
Hurria A, Mohile S, Gajra A, et al. Validation of a Prediction Tool for Chemotherapy Toxicity inOlder Adults With Cancer. J Clin Oncol 2016; 34:2366.
91.
Mohile SG, Velarde C, Hurria A, et al. Geriatric Assessment-Guided Care Processes for OlderAdults: A Delphi Consensus of Geriatric Oncology Experts. J Natl Compr Canc Netw 2015;13:1120.
92.
Puts MT, Santos B, Hardt J, et al. An update on a systematic review of the use of geriatricassessment for older adults in oncology. Ann Oncol 2014; 25:307.
93.
Topic 2808 Version 25.0
Comprehensive geriatric assessment for patients with cancer - U... https://www.uptodate.com/contents/comprehensive-geriatric-ass...
14 z 27 22.10.2017, 20:26

GRAPHICS
The Vulnerable Elders Survey (VES) 13 scale
Domain Score
Age
75-85 1
>85 3
Self-rated health
Good, very good, and excellent 0
Fair and poor 1
Activities of daily living (ADLs)/instrumental ADLs (IADLs)
Needs assistance with
Bathing or showering 1
Shopping 1
Money management 1
Transfer 1
Light housework 1
Difficulty in special activities
Kneeling, bending, and stooping 1
Performance of housework (example: scrubbing the floor) 1
Reaching out and lifting upper extremities above the shoulder 1
Lifting and carrying 10 pounds 1
Walking 0.25 miles 1
Writing or handling and grasping small objects 1
Score ≥3: Vulnerable elderly
Data from: Saliba D, Elliott M, Rubenstein LZ, et al. The Vulnerable Elders Survey: a tool for identifyingvulnerable older people in the community. J Am Geriatr Soc 2001; 49:1691.
Graphic 73154 Version 3.0
Comprehensive geriatric assessment for patients with cancer - U... https://www.uptodate.com/contents/comprehensive-geriatric-ass...
15 z 27 22.10.2017, 20:26

Karnofsky Performance Status scale
Value Level of functional capacity Definition
100 Normal, no complaints, no evidence ofdisease
Able to carry on normal activity and to work; nospecial care needed
90 Able to carry on normal activity, minorsigns or symptoms of disease
80 Normal activity with effort, some signsor symptoms of disease
70 Cares for self, unable to carry onnormal activity or to do active work
Unable to work; able to live at home and care formost personal needs; various degrees of assistanceneeded
60 Requires occasional assistance but isable to care for most needs
50 Requires considerable assistance andfrequent medical care
40 Disabled, requires special care andassistance
Unable to care for self; requires equivalent ofinstitutional or hospital care; disease may beprogressing rapidly
30 Severely disabled, hospitalization isindicated although death is notimminent
20 Hospitalization is necessary, very sick,active supportive treatment necessary
10 Moribund, fatal processes progressingrapidly
0 Dead
Graphic 58785 Version 6.0
Comprehensive geriatric assessment for patients with cancer - U... https://www.uptodate.com/contents/comprehensive-geriatric-ass...
16 z 27 22.10.2017, 20:26

Eastern Cooperative Oncology Group (ECOG, Zubrod, World HealthOrganization) performance scale
Performancestatus
Definition
0 Fully active; no performance restrictions.
1 Strenuous physical activity restricted; fully ambulatory and able to carry outlight work.
2 Capable of all self-care but unable to carry out any work activities. Up andabout >50% of waking hours.
3 Capable of only limited self-care; confined to bed or chair >50% of wakinghours.
4 Completely disabled; cannot carry out any self-care; totally confined to bed orchair.
Excerpted from: Oken MM, Creech RH, Tormey DC, et al. Toxicity and response criteria of the EasternCooperative Oncology Group. Am J Clin Oncol 1982; 5:649.
Graphic 72901 Version 9.0
Comprehensive geriatric assessment for patients with cancer - U... https://www.uptodate.com/contents/comprehensive-geriatric-ass...
17 z 27 22.10.2017, 20:26
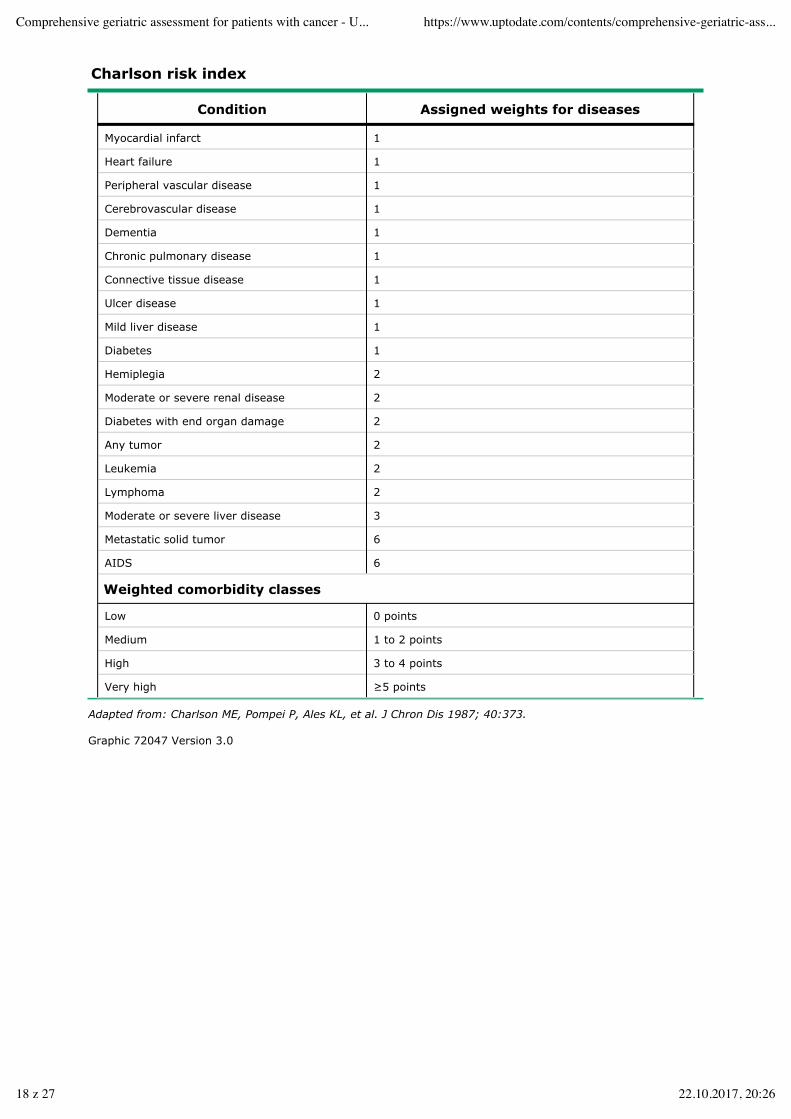
Charlson risk index
Condition Assigned weights for diseases
Myocardial infarct 1
Heart failure 1
Peripheral vascular disease 1
Cerebrovascular disease 1
Dementia 1
Chronic pulmonary disease 1
Connective tissue disease 1
Ulcer disease 1
Mild liver disease 1
Diabetes 1
Hemiplegia 2
Moderate or severe renal disease 2
Diabetes with end organ damage 2
Any tumor 2
Leukemia 2
Lymphoma 2
Moderate or severe liver disease 3
Metastatic solid tumor 6
AIDS 6
Weighted comorbidity classes
Low 0 points
Medium 1 to 2 points
High 3 to 4 points
Very high ≥5 points
Adapted from: Charlson ME, Pompei P, Ales KL, et al. J Chron Dis 1987; 40:373.
Graphic 72047 Version 3.0
Comprehensive geriatric assessment for patients with cancer - U... https://www.uptodate.com/contents/comprehensive-geriatric-ass...
18 z 27 22.10.2017, 20:26

Nomogram for determining body mass index
The nomogram is used by placing a ruler or other straight edge between thebody weight in kilograms or pounds (the left-hand line) and the height incentimeters or inches (the right-hand line). The body mass index is read fromthe middle of the scale, in metric units.
Graphic 65305 Version 1.0
Comprehensive geriatric assessment for patients with cancer - U... https://www.uptodate.com/contents/comprehensive-geriatric-ass...
19 z 27 22.10.2017, 20:26

Mailed geriatric assessment
Domain Measures
Functional status 1) Activities of Daily Living [Subscale of the EORTC QLQ-C30]
2) Instrumental Activities of Daily Living [Subscale of the OARS]
3) Exercise scale
Comorbidity Physical Health Section [Subscale of the OARS]
Pain Visual Analog Pain Thermometer Scale
Psychological Hospital Anxiety and Depression Scale
Financial well-being Subscale of the OARS
Social support Medical Outcomes Study Social Support Survey
Spiritual well-being Symptoms of Belief Inventory
Quality of life EORTC QLQ-C30
Also captures information on demographics.
OARS: Older American Resources and Services.
Graphic 60695 Version 2.0
Comprehensive geriatric assessment for patients with cancer - U... https://www.uptodate.com/contents/comprehensive-geriatric-ass...
20 z 27 22.10.2017, 20:26

Primarily self-administered comprehensive geriatric assessment tool*
Domain Measures
Functional status 1) Activities of Daily Living [Subscale of Medical Outcomes Study Physical HealthScale]
2) Instrumental Activities of Daily Living [Subscale of the OARS]
3) Karnofsky performance status (Physician-Rated)
4) Karnofsky performance status (Patient-Rated)
5) Timed Up and Go
6) Number of falls in last six months
Comorbidity Physical Health Section [Subscale of the OARS]
Cognition Blessed Orientation-Memory-Concentration Test
Psychological Hospital Anxiety and Depression Scale
Socialfunctioning
Medical Outcomes Study Social Activity Limitations Measure
Social support Medical Outcomes Study Social Support Survey: Emotional/Information & TangibleSubscales
Nutrition 1) Body mass index
2) Percent unintentional weight loss in the last 6 months
OARS: Older Americans Resources and Services.* Also captures information on demographics and cancer characteristics.
Graphic 70657 Version 5.0
Comprehensive geriatric assessment for patients with cancer - U... https://www.uptodate.com/contents/comprehensive-geriatric-ass...
21 z 27 22.10.2017, 20:26
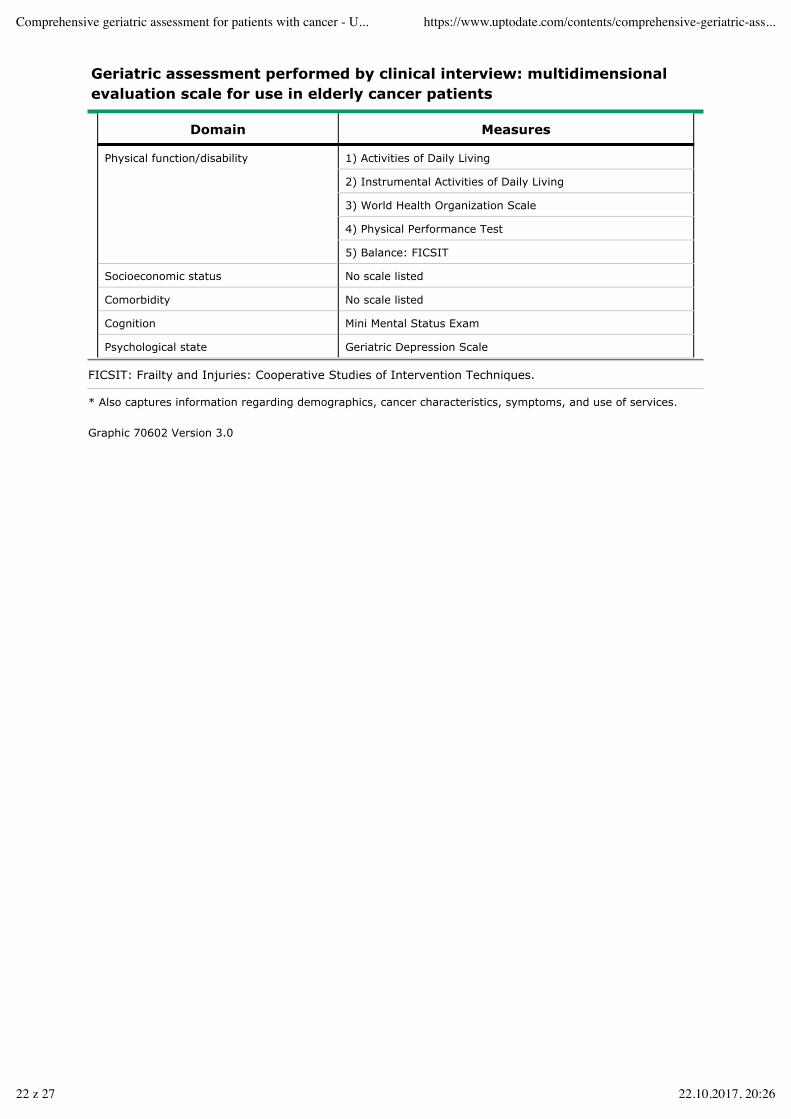
Geriatric assessment performed by clinical interview: multidimensionalevaluation scale for use in elderly cancer patients
Domain Measures
Physical function/disability 1) Activities of Daily Living
2) Instrumental Activities of Daily Living
3) World Health Organization Scale
4) Physical Performance Test
5) Balance: FICSIT
Socioeconomic status No scale listed
Comorbidity No scale listed
Cognition Mini Mental Status Exam
Psychological state Geriatric Depression Scale
FICSIT: Frailty and Injuries: Cooperative Studies of Intervention Techniques.
* Also captures information regarding demographics, cancer characteristics, symptoms, and use of services.
Graphic 70602 Version 3.0
Comprehensive geriatric assessment for patients with cancer - U... https://www.uptodate.com/contents/comprehensive-geriatric-ass...
22 z 27 22.10.2017, 20:26

Taxonomy of aging
Group Characteristics
Primary No functional dependence; negligible comorbidity
Intermediate Dependence in one or more IADLs; stable comorbidity (eg, stable angina, chronic renalinsufficiency, etc)
Secondary orfrail
One of the following criteria:
(i) Dependence in one or more ADLS;
(ii) Three or more comorbid conditions or one poorly controlled comorbid condition;
(iii) One or more geriatric syndromes (delirium, dementia, depression, falls,incontinence, spontaneous bone fractures, neglect or abuse, failure to thrive)
Near death
ADLs: activities of daily living; IADLs: instrumental activities of daily living.
Reproduced with permission from: Balducci L. Geriatric oncology. Crit Rev Oncol Hematol 2003; 46:212.Copyright © 2003 Elsevier.
Graphic 60632 Version 2.0
Comprehensive geriatric assessment for patients with cancer - U... https://www.uptodate.com/contents/comprehensive-geriatric-ass...
23 z 27 22.10.2017, 20:26

Comprehensive geriatric assessment (CGA) and itsimplications for patients being treated for breast cancer
Reproduced with permission from: Balducci L. Geriatric oncology. Crit Rev OncolHematol 2003; 46:212. Copyright © 2003 Elsevier.
Graphic 67375 Version 4.0
Comprehensive geriatric assessment for patients with cancer - U... https://www.uptodate.com/contents/comprehensive-geriatric-ass...
24 z 27 22.10.2017, 20:26

CARG model for predicting chemotherapy toxicity in older adults
Risk factorPrevalence
Grades 3 to 5toxicity OR
95%CI
Score
No. Percent No. Percent
Age ≥72 years 270 54 163 60 1.85 1.22 to2.82
2
Cancer type GI or GU 185 37 120 65 2.13 1.39 to3.24
2
Chemotherapy dosing, standard dose 380 76 204 54 2.13 1.29 to3.52
2
Number of chemotherapy drugs,polychemotherapy
351 70 192 55 1.69 1.08 to2.65
2
Hemoglobin <11 g/dL (male), <10g/dL (female)
62 12 46 74 2.31 1.15 to4.64
3
Creatinine clearance (Jelliffe, idealweight) <34 mL/min
44 9 34 77 2.46 1.11 to5.44
3
Hearing, fair or worse 123 25 76 62 1.67 1.04 to2.69
2
Number of falls in last six months, oneor more
91 18 61 67 2.47 1.43 to4.27
3
IADL: Taking medications, with somehelp/unable
39 8 28 72 1.50 0.66 to3.38
1
MOS: Walking one block, somewhatlimited/limited a lot
109 22 69 63 1.71 1.02 to2.86
2
MOS: Decreased social activitybecause of physical/emotional health,limited at least sometimes
218 44 126 58 1.36 0.90 to2.06
1
CARG: Cancer and Aging Research Group; OR: odds ratio; GI: gastrointestinal; GU: genitourinary; IADL:instrumental activities of daily living; MOS: Medical Outcomes Study.
From: Hurria A, Togawa K, Mohile SG, et al. Predicting chemotherapy toxicity in older adults with cancer: aprospective multicenter study. J Clin Oncol 2011; 29:3457. Reprinted with permission. Copyright © 2011American Society of Clinical Oncology. All rights reserved.
Graphic 78775 Version 4.0
Comprehensive geriatric assessment for patients with cancer - U... https://www.uptodate.com/contents/comprehensive-geriatric-ass...
25 z 27 22.10.2017, 20:26

Ability of CARG risk score versus physician-rated Karnofsky performancestatus (KPS) to predict chemotherapy toxicity
Riskstrata
No toxicity ToxicityTotal p ROC
No. Percent No. Percent
By total score
0-5 (low) 89 70 39 30 128 <0.001 0.72*
6-9 (mid) 110 48 117 52 227
10-19(high)
19 17 90 83 109
By physician-rated KPS (percent)
90-100 125 49 128 51 253 0.19 0.53*
80 73 49 76 51 149
≤70 33 38 53 62 86
CARG: Cancer and Aging Research Group; ROC: receiver operating characteristic; KPS: Karnofsky performancestatus.* Risk score and physician-rated KPS were treated as continuous to calculate the ROC.
From: Hurria A, Togawa K, Mohile SG, et al. Predicting chemotherapy toxicity in older adults with cancer: aprospective multicenter study. J Clin Oncol 2011; 29:3457. Reprinted with permission. Copyright © 2011American Society of Clinical Oncology. All rights reserved.
Graphic 60649 Version 6.0
Comprehensive geriatric assessment for patients with cancer - U... https://www.uptodate.com/contents/comprehensive-geriatric-ass...
26 z 27 22.10.2017, 20:26

Contributor Disclosures
Arti Hurria, MD Grant/Research/Clinical Trial Support: GSK; Novartis [Breast cancer (Lapatinib)];Celgene [Breast cancer (Nab-paclitaxel)]. Consultant/Advisory Boards: Boehringer IngelheimParmaceuticals; Carevive; Sanofi, Pierian Biosciences [Geriatric Oncology (None)]. Harvey JayCohen, MD Nothing to disclose Reed E Drews, MD Nothing to disclose Kenneth E Schmader,MD Grant/Research/Clinical Trial Support: Merck [Herpes zoster (Zoster vaccine)]; GlaxoSmithKline[Herpes zoster (Zoster vaccine)]. Sadhna R Vora, MD Nothing to disclose
Contributor disclosures are reviewed for conflicts of interest by the editorial group. When found,these are addressed by vetting through a multi-level review process, and through requirements forreferences to be provided to support the content. Appropriately referenced content is required of allauthors and must conform to UpToDate standards of evidence.
Conflict of interest policy
Comprehensive geriatric assessment for patients with cancer - U... https://www.uptodate.com/contents/comprehensive-geriatric-ass...
27 z 27 22.10.2017, 20:26



























![geriatric assessment [EDocFind.com].ppt](https://img.dokumen.tips/doc/110x75/56d6c0791a28ab30169a87ff/geriatric-assessment-edocfindcomppt.jpg)