Embed Size (px)
Citation preview

not require a decompressive procedure.5
Despite a normal flexible bronchoscopyandnaso-endoscopy,ourpatient is likelyto have sustained a subclinical injuryto the tracheobronchial tree and/or oesophagus related to a forcedValsalva manoeuvre from self-inducedvomiting.5 Although severe asthma iswell known to cause free air leaks,3
this patient did not have signs ofsignificant bronchoconstriction on
presentation and did not respond toburst bronchodilators.
The life threat is potential upperairway obstruction1 from rapidly pro-gressive laryngeal and upper airway in-filtration. This patient’s voice changeis likely to have resulted from exten-sive paralaryngeal infiltration alter-ing resonance. With the potential needto secure an urgent, difficult and de-finitive airway, there is need for closesurveillance to detect upper airway ob-struction. The patient is required to bepositioned in the most comfortable po-sition (sat up), urgent ear, nose andthroat consultation sought and prepa-rations made for a difficult and failedintubation, including a surgical rescueairway.
AcknowledgementThe authors thank Dr Rino Olivottofor helpful and detailed feedback onthe CT chest and barium swallow thatwas performed.
Competing interests
None declared.
References1. Gibney RT, Finnegan B, Fitzgerald
MX, Lynch V. Upper airway obstruc-tion caused by massive subcutaneous
emphysema. Intensive Care Med. 1984;10: 43–4.
2. Yilmaz S, Koc A. Traumatic rightpericardial laceration with tensionpneumopericardium associated withhemodynamic instability: a case report.ARYA Atheroscler. 2013; 9: 210–2.
3. Jones MG, Rae W, Lwin AA,Kurukulaaratchy RJ. Pneumome-diastinum leading to respiratory com-promise as a complication of acutesevere asthma. Am. J. Respir. Crit. CareMed. 2013; 187: e5–6.
4. Adachi T, Oki M, Kajikawa S, SakaH. A case of bronchial asthma com-plicated by epidural emphysema. Res-piration 2012; 84: 69.
5. Natale C, D’Journo XB, Duconseil P,Thomas PA. Recurrent spontaneouspneumomediastinum in an adult. Eur.J. Cardiothorac Surg. 2012; 41: 1199–201.
Joseph TING1,2 andCarla HOPPER2
1Faculty of Health and Social Work,Queensland University of
Technology, Brisbane, Queensland,Australia, and 2Department of
Emergency Medicine, Mater HealthServices, Brisbane, Queensland,
Australiadoi: 10.1111/1742-6723.12220
Complete airway obstruction in an infant causedby a toy balloon
Dear Editor,Inhalation of a foreign body (FB) inchildren is a relatively common oc-currence where symptoms vary fromnegligible to severe airway obstruc-tion. Death caused by suffocation afterinhalation of a FB is the leading causeof unintentional-injury mortality inchildren younger than 1 year of age inthe USA.1
Accidental chokingon toy rubberbal-loons is a well-known hazard, and treat-ing a balloon aspiration can prove verydifficult. The usual treatment pro-cedures for choking, for example theHeimlich manoeuvre and back blows,are ineffective.2 Balloons are elasticobjects and do not break apart easily,which would facilitate their expul-sion.2 Several case reports describe
suffocation by rubber balloons;however, to the authors’ knowledge allreported cases have had a fataloutcome.2–5
We report a case of accidental tra-cheal aspiration of a toy balloon in aninfant causing complete airway ob-struction along with its management.
A 7-month-old previously healthyboy was, without prior warning of
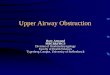
Figure 1. CT chest with oral contrastshowing extensive pneumomediastinum,pneumopericardium and chest wall sub-cutaneous emphysema. There was exten-sive cervical tracking of air into tissuessurrounding the larynx without infiltra-tion into the vocal cords or laryngealcomplex.
bs_bs_banner
310 CASE LETTERS
© 2014 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine

their arrival, brought to the ED by hisparents with respiratory failure andcardiac arrest. The parents informedthe doctors that the child had beenplaying unsupervised when they sud-denly heard troubled breathing andafter a short while the child becameunconscious. They suspected he hadchoked on a FB. On exam the patientwas comatose, with dilated pupils, hewas cyanotic and one last paradox res-piration was observed, there was nopalpable pulse. It was unknown howlong the patient had been in cardiacarrest.
Cardiopulmonary resuscitation wasstarted and positive pressure ventila-tion with a bag-mask was initiated;however, the patient could not be ven-tilated. Inspection of the oral cavity,pharynx and larynx showed no signof a FB. The patient was intubated byan anaesthesiologist with an ETT sizeof 3.5; this was done smoothly withfull view of glottis Cormack-Lehane 1.However, the patient could not be ven-tilated through the ETT; the ventila-tion bag could not be compressed.Simultaneously monitors were at-tached to the patient. Pulsoxymetrie(SpO2) was non-detectable, and ECGshowed asystoli.
The ETT was advanced into thetrachea to push the FB into the rightmain-stem bronchus to clear thetrachea. Resistance was felt, and theETT was withdrawn to the trachea;however, ventilation was still not pos-sible. There was no bronchoscopyavailable so it was decided to extubatethe patient, and a plastic suction cath-eter Ch 14 was passed through thevocal cords until resistance was felt.Suction with 200 mmHg was applied,and an intact pear-shaped toy rubber
balloon was removed. The patientwas re-intubated with an ETT, andventilation was now possible. After ap-proximately 30 s the patient sponta-neously converted to a sinus rhythm30 /min and after 1 min 100 /min SpO2
98% with FiO2 (fraction of inspiredoxygen) 100%. After a few minutesthe pupils contracted, and sponta-neous respiration occurred. The patienthas made a full recovery, and thefollowing paediatric follow upshave shown normal neurologicaldevelopment.
A FB that is wedged below the vocalcords might completely obstruct thetrachea. In these situations the tracheamight be intubated and the ETT ad-vanced into the right main-stem bron-chus in an attempt to push the FB intothe right main-stem bronchus. TheETT is then withdrawn to a pointabove carina, and ventilation on theleft lung would be possible.6 There isno evidence to support the effective-ness of this approach in a situationwith a complete subglottic airway ob-struction.6 By advancing the ETTfurther down the trachea blindly thereis also a risk of wedging the FB morefirmly; however, it might be the onlyopportunity to oxygenate and venti-late the patient, particularly in aprehospital setting. The difficult airwaymanagement algorithm by the Ameri-can Society of Anesthesiologists sug-gests that if mask ventilation andintubation is not possible, establish-ment of an emergency surgical airwayis the next cause of actions. However,none of these possibilities would haveovercome the problem in the presentcase.
As a last resort in an emergencysituation with complete subglottic ob-
struction, an attempt can be made toadvance a suction catheter throughthe ETT and apply suction whileextubating, hereby trying to remove theFB or pass a suction catheter throughthe vocal cords and apply suction withthe same purpose.
Competing interests
None declared.
References1. WISQARS Leading causes of death
reports, 1999–2001. National Centerfor Injury Prevention and Control.[Cited 15 Dec 2013.] Available fromURL: http://webapp.cdc.gov/sasweb/ncipc/leadcaus10.html
2. Abdel-Rahman HA. Fatal suffoca-tion by rubber balloons in children:mechanism and prevention. ForensicSci. Int. 2000; 108: 97–105.
3. Dias E. An unusual case of foreignbody aspiration in an infant. Ann.Med. Health Sci. Res. 2012; 2: 209–10.
4. Meel BL. An accidental suffocation bya rubber balloon. Med. Sci. Law 1998;38: 81–2.
5. Ryan CA, Yacoub W, Paton T, AvardD. Childhood deaths from toy bal-loons. Am. J. Dis. Child. 1990; 144:1221–4.
6. Pfleger A, Eber E. Management ofacute severe upper airway obstruc-tion in children. Paediatr. Respir. Rev.2013; 14: 70–7.
Hanne Beck MIERITZ andJan Peter KÜHNE
Aabenraa Hospital,Aabenraa, Denmark
doi: 10.1111/1742-6723.12212
CASE LETTERS 311
© 2014 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine