Embed Size (px)
Citation preview

Infectious Diseases
Sepis, SIRS
I/R Injury
Psoriasis
Myasthenia Gravis
SLE
PNH
Hereditary Angioedema
Multiple Sclerosis
Trauma, Burn Injury
Capillary Leak Syndrome
Obesity, Diabetes
Cancer
Alzheimer’s Disease, Stroke, Schizophrenia,
Epilepsy
AMD,Glaucoma,
Diabetic Retinopathy
Asthma, Allergy, ARDS, Cystic Fibrosis
Myocardial Infraction
aHUS (and HUS), MPGN-II Lupus Nephritis
Crohn’s Disease
Rheumatoid Arthritis
Atherosclerosis Vasculitis
Transplant Rejection Fetal Loss Biomaterial Reactions (Hemodialysis, Implants...)
INTELLIGENT INSIGHTS. SMART RESULTS.
Complement Disorders and Potential Therapiesfor Complement Mediated Diseases: A Spotlight
There is a renewed interest in pursuing the complement
pathway as drug targets based on the success of
eculizumab (Soliris; Alexion Pharmaceuticals) in the
treatment of an orphan disease, paroxysmal nocturnal
haemoglobinuria. There are now multiple anti-
complement drugs in the market, including Soliris/Alexion
(PNH and aHUS), Cinryze (HAE), Berinert and
Haegarda/CSL Behring (HAE), Ruconest/Pharming (HAE),
and many more are being developed across a broad
spectrum of diseases.
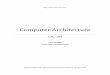
Figure 1. Complement system mediated diseases
The complement system is considered to be an immune mediated defense against infection and is an important driver
of inflammation. However, uncontrolled activation of complement can lead to local and/or systemic inflammation
and tissue damage causing inflammatory, autoimmune and degenerative diseases. More than 50 conditions are now
widely recognized as diseases with demonstrated or suspected involvement of the complement system.
Complement pathway and its regulation
The complement system is a tightly regulated network of
more than 30 proteins, largely designated by the letter C
and number in the order of discovery (e.g., C1, C2, C3,
etc.). These proteins are present as an inactive form or
zymogens in blood or as bound to membranes. Sequential
cascade of enzymatic reactions cleaves and activates
these proteins to form potent anaphylatoxins that elicit
physiological responses ranging from chemo attraction
to apoptosis.
Figure 2. Complement system
SMARTImmunologySMARTImmunologyThe Immunology Newsletter from SMARTANALYSTThe Immunology Newsletter from SMARTANALYST
The SMARTImmunology Newsletter Team: Anupam Goyal, PhD, Anil Lele, Rohit Katoch
Copyright © 2017 SMARTANALYST
Volume 1, Issue 2 Immunology Newsletter | August 2017
C3
C3bBb3b
FB and FD FB and FDMASPsC1r and C1s
FB and FD
Lectin pathway Alternative pathway initiation
Alternative pathway amplification
Terminal pathway
C3bBb
C3(H2O)BbC3BbP
C4b2b
C4b2b3b
Classical pathway
C3(H2O)
C3b
C2C4
C3
C5
C3b
iC3b
C3a
C3bg
C5a
C5b MAC
Extrinsic proteases
MBL Fcn CL-11
FP
C6, C7, C8, C9n
Extrinsic proteases
CD35 and FI
FPC1q
AssociationCleavageTransformation

2Top of Document
Volume 1, Issue 2 Immunology Newsletter | August 2017
Complement activation is usually initiated by the
interaction of several pattern-recognition receptors with
foreign surface structures. Depending on the activation
trigger, the complement cascade follows one of three
pathways: the classical, lectin or alternative pathway.
All three pathways converge at the cleavage of
complement C3.
• The Classical Pathway (CP) is initiated by antibody
complexes. These complexes are formed by binding
of pathogens to IgG or IgM. Antibody complex binds
to the C1 complex and activate C1s and C1r. C1s then
cleaves C4 and C2 to form the C3 convertase.
• The Lectin Pathway (LP) is activated by binding of
mannose binding lectin (MBL) or Ficolin to
carbohydrates on surfaces of pathogens including
yeast, bacteria, parasites and viruses. This pathway is
activated similar to the classic pathway except that
lectin replaces the immune complex and mannan-
binding lectin–associated proteases (MAPS) replace
C1 enzymatic activity which activate C4 and C2 and
form the C3 convertase.
• The Alternative Pathway is considered to be the
dominant contributor to the overall complement
response and is triggered by carbohydrates, lipids
and proteins found on the foreign surfaces such as on
viruses, fungi, bacteria, and parasites. The alternative
pathway is divided into two arms, one that initiates
complement activation and invokes pattern
recognition (that is, by properdin) or hydrolysis of C3
to form C3 convertase and the other that mediates
amplification independent of the initiating
mechanism.
The common pathway starts with the cleavage of C3 into
its active fragments by C3 convertases, C3a and C3b. C3b
complexes with the C3 convertases to form the C5
convertases. The C5 convertases cleave C5 to form C5a
and C5b. The anaphylatoxins C3a, C3b and C5a, are potent
inflammatory mediators that initiate various processes
including formation of membrane attack complex (MAC),
which culminate in the stimulation of immune cells and
the elimination of the pathogen.
Impact of complement dysregulation
• Complement dysregulation may include both an
inappropriate initiation of the cascade or deficiencies
in specific components or regulators.
Table 1. Impact of complement dysregulation
Complement Dysregulation Diseases Caused
Deficiency in Complement Proteins
Excessive Complement Activation (Dysregulated Modulation)
• aHUS, PNH, Age-related Macular Degeneration (AMD)
• Other diseases include Alzheimer’s syndrome, Asthma and the Acute Response Distress Syndrome (ARDS).
Complement pathway as drug targets and drugs in development
The role of complement in the pathophysiology of major diseases makes it an interesting target for the pharmaceutical industry. The complement cascade offers various points of intervention at almost any level starting from initiation and primary activation to amplification, effector signalling, and lysis.
• Upstream intervention at the level of specific initiation steps of complement pathway may help in regulating uncontrolled activation of classical, lectin pathways and alternative pathways. The inhibition of C1r/s by C1 esterase inhibitor (C1-INH) may effectively shut down complement activation and subsequent generation of effector molecules caused by the classical pathway without affecting the protective functions of the other pathways.
• Blocking the common pathway at the level of C3 activation, either by blocking C3 directly (e.g., using compstatin) or by acting on the convertase, will efficiently block all activation, amplification, and effector routes independent of the disease mechanism. This may pose a higher risk of blocking beneficial complement functions.
• Blockage at the terminal end can be very effective in eliminating specific function (depending on the target) without blocking other complement activity. For example, blocking C5 (Eculizumab) impairs the formation of the MAC and inflammatory signalling by C5a, whereas only the signalling function is blocked by targeting the C5a receptor (C5aR) with antagonists such as PMX53.
A number of promising candidates for the clinical substitution, inhibition or modulation of complement are in development.
• Lupus• Hemolytic Uremic Syndrome
(HUS), etc.

Volume 1, Issue 2 Immunology Newsletter | August 2017
Table 2. List of complement therapeutics that are marketed or are in clinical development (> Phase II)
Diseases Asset Phase Company
C3 & sCR1
Age-related Macular Degeneration APL-2 Phase II Apellis Pharma Common Pathway Target – C5aR
ANCA Associated Vasculitis CCX-168 Phase III (Orphan Drug Status) ChemoCentryx Atypical Hemolytic Uremic Syndrome CCX-168 Phase II (Orphan Drug Status) ChemoCentryx
C3 Glomerulopathy CCX-168 Phase II (Orphan Drug Status) ChemoCentryx Sepsis IFX-1 Phase II InflaRx
Hidradenitis Suppurativa IFX-1 Phase II InflaRx Common Pathway -
Target –
C5
Atypical Hemolytic Uremic Syndrome
Eculizumab
Marketed (Orphan Drug Status)
Alexion
ALXN-1210
Phase III
Alexion
Coversin
Phase II
Akari Therapeutics
Paroxysmal Nocturnal Haemoglobinuria
Eculizumab
Marketed (Orphan Drug Status)
Alexion
ALN-CC5
Phase II
Alnylam Pharma
ALXN-1210
Phase III (Orphan Drug Status)
Alexion LFG 316
Phase II
Morphosys/Novartis
Coversin
Phase II (Fast-track and Orphan
Drug Status)
Akari Therapeutics
RA101348
Phase II (Orphan Drug Status )
Ra Pharmaceuticals
RO-7112689
Phase II
Roche
Myasthenia Gravis
Eculizumab
Pre-registration (Orphan Drug Status)
Alexion
Neuromyelitis Optica
Eculizumab
Phase III (Orphan Drug Status)
Alexion
Stec HUS
Eculizumab
Phase II/III (Orphan Drug Status)
Alexion
Acute Antibody Mediated Rejection
Eculizumab
Phase II
Alexion
Age-related Macular Degeneration
LFG 316
Phase II
Morphosys/Novartis
Zimura
Phase III
Ophthotech
Polypoidal Choroidal Vasculopathy
Zimura
Phase II
Ophthotech
Panuveitis
LFG 316
Phase II
Morphosys/Novartis
Transplant Associated Microangiopathy
LFG 316
Phase II
Morphosys/Novartis
C1 Esterase Inhibitor (C1-INH)
Hereditary Angioedema
C1 INH (Human)
Marketed
CSL Behring
C1 INH (Human)
Marketed (Orphan Drug Status)
Shire Viropharma
Conestat alfa
Marketed (Orphan Drug Status)
Pharming
Acute Antibody Mediated Rejection
C1 INH (Human)
Phase III (Orphan Drug Status)
Shire Viropharma
Target –
MASP-2
Atypical Hemolytic Uremic Syndrome
OMS 721
Phase III (Fast Track Status and Orphan Drug Status)
Omeros
Membranoproliferative Glomerulonephritis
Phase II
IgA Nephropathy
Phase II (Fast Track Status and
Orphan Drug Status)
Transplant Associated Microangiopathy
Phase II (Orphan Drug Status)
Thrombotic Thrombocytopenic Purpura
Phase II
Lupus Nephritis
Phase II
C3 Glomerulopathy Phase II
C3- Conv
Age-related Macular Degeneration Lampalizumab Phase III Roche
3Top of Document

Volume 1, Issue 2 Immunology Newsletter | August 2017
Risks associated with complement therapies:
The biggest risk associated with complement therapies is
that a drug blocking a complement pathway can
significantly increase the risk of infections and other
immune mediated diseases.
• Drugs that inhibit the classical pathway may affect
the clearance of immune complexes and apoptotic
cells
• Inhibition of the activation pathways may disrupt an
adaptive immune response and recurrent infections
may become life-threatening
• Anti-complement drugs may also disrupt normal lipid
metabolism or interfere with the healing and
resolution of injuries
These potential consequences need to be considered
while deciding whether and when to use an anti-
complement drug and which part of the system to target.
With appropriate prophylactic measures such as
immunization and antibiotic therapy, and with careful
consideration of the target, these consequences can be
managed. Research is ongoing to devise strategies to
inhibit complement without risking significant infections
and immune mediated diseases. Some strategies being
considered are:
• Delivering therapies directly to disease sites so that
systemic inhibition is avoided. One such example is
C3 blocker compstatin and an antibody antigen-
binding fragment (Fab) directed against Factor D
(FD), administered intravitreally for the treatment of
AMD (currently in Phase III clinical trials)
• Treating acute conditions by inhibiting complement
transiently
Conclusion
While the role of complement system has been
demonstrated in a number of diseases, the extent of the
role played by the complement system in the
pathophysiology of certain diseases, such as Myocardial
infarction, Myasthenia gravis, and Asthma remains
unclear. Therefore, further studies are needed to
understand the extent of role of complement system in
these diseases and benefits that can be derived by
modulating the pathway. As the role of complement
system becomes clearer, newer treatment options will be
developed.
References:
1. B. Paul Morgan and Claire L. Harris. Complement, a target for
therapy in inflammatory and degenerative diseases. Nature
Reviews Drug Discovery. Volume 14 , December 2015: 857
2. Horiuchi and Tsukamoto. Complement-targeted therapy:
development of C5- and C5a-targeted inhibition. Inflammation
and Regeneration 2016, 36:11
3. Holers et al. Complement Therapeutics, Advances in Experimental
Medicine and Biology 735
4. Daniel Ricklin and John D Lambris. Complement-targeted
therapeutics. Nat Biotechnol. 2007 November; 25(11):
1265–1275
5. Jason R Dunkelberger, Wen-Chao Song. Complement and its role in
innate and adaptive immune responses. Cell Research (2010)
20:34-50
6. J. Vidya Sarma and Peter A. Ward. The Complement System. Cell
Tissue Res. 2011 January; 343(1): 227–235
7. Daniel Ricklin, Edimara S. Reis and John D. Lambris. Complement
in disease: a defence system turning offensive. Nature Reviews
Nephrology. Volume 12, July 2016: 383
4Top of Document
The SMARTImmunology Newsletter Team: Anupam Goyal, PhD, Anil Lele, Rohit Katoch
Copyright © 2017 SMARTANALYST