Embed Size (px)
Citation preview

KNEE
Comparison of results after anterior cruciate ligamentreconstruction using a four-strand single semitendinosusor a semitendinosus and gracilis tendon
Hee-Soo Kyung • Hyun-Joo Lee • Chang-Wug Oh •
Han-Pyo Hong
Received: 11 February 2013 / Accepted: 8 May 2014
� Springer-Verlag Berlin Heidelberg 2014
Abstract
Purposes To compare the clinical and functional results
of anterior cruciate ligament (ACL) reconstruction using an
autologous four-strand single semitendinosus (ST) ten-
don or a ST and gracilis tendon. It was hypothesized that
successful ACL reconstruction using a single ST tendon
without the gracilis tendon could provide comparable knee
stability and reduce donor site morbidity.
Methods This study evaluated 144 cases of single-bundle
ACL reconstruction using an autologous hamstring tendon.
The ST group included 85 cases of reconstruction using a
single ST tendon, and the ST/G group included 59 cases of
reconstruction using a ST tendon and a gracilis tendon. An
extracortical suspension device and a suture tied around a
screw post with an additional bioabsorbable screw were
used to fix the femoral and tibial tunnels, respectively.
Clinical evaluations involved the Lachman, pivot-shift, and
one-leg hop tests; an isokinetic test; a KT-2000 arthrome-
ter; an assessment of return to pre-injury activities; and
Lysholm, Tegner activity, and International Knee Docu-
mentation Committee (IKDC) subjective scores.
Results No significant differences were found between
the ST and ST/G groups with respect to the Lysholm,
Tegner activity, and subjective IKDC scores; the Lachman,
pivot-shift, and one-leg hop tests; KT-2000 arthrometer
side-to-side differences; or return to pre-injury activities.
However, mean peak torque deficit, as determined using
the isokinetic test during flexion at 60�/s, was significantly
lower in the ST group than in the ST/G group (p = 0.047).
Conclusion This study showed good results for ACL
reconstruction using a single ST tendon without deterio-
ration of stability. This provides the evidence that ACL
reconstruction using a single ST tendon without the gracilis
tendon decreases donor site morbidity without compro-
mising joint stability.
Level of evidence IV.
Keywords Anterior cruciate ligament reconstruction �Semitendinosus � Gracilis � Single semitendinosus
Introduction
Many options are available for anterior cruciate liga-
ment (ACL) reconstruction, including an autologous
bone–patellar tendon–bone graft, a hamstring tendon
graft, and an allograft. The bone–patellar tendon–bone
graft is more likely to result in normal knee joint laxity
and less incidence of significant flexion loss. In con-
trast, hamstring grafts reduce the incidence of patel-
lofemoral crepitus, kneeling pain, and extension loss
[10]. Holm et al. [11] published a randomized study
with a 10-year follow-up, comparing knee function and
osteoarthritis prevalence after ACL reconstruction for a
four-strand hamstring autograft versus a bone–patellar
tendon–bone autograft. No significant difference
between clinical outcomes was found between the two
grafts at 10 years postoperatively, although osteoarthri-
tis prevalence was significantly higher in the operated
than in the contralateral leg. Pinczewski et al. [21]
published a comparative meta-analysis on bone–patellar
tendon–bone and hamstring autografts obtained in two
consecutive series with a 10-year follow-up and rec-
ommended the hamstring graft as the first choice. A
H.-S. Kyung (&) � H.-J. Lee � C.-W. Oh � H.-P. Hong
Department of Orthopaedic Surgery, School of Medicine,
Kyungpook National University Hospital, 130 Dongduk-Ro
Jung-Gu, Daegu 700-721, Korea
e-mail: [email protected]
123
Knee Surg Sports Traumatol Arthrosc
DOI 10.1007/s00167-014-3076-4
significantly higher incidence of radiographic osteoar-
thritic changes was found in knees reconstructed with a
bone–patellar tendon–bone autograft than with a ham-
string autograft. Allografts have the advantage of no
donor site morbidity and good graft source availability,
but they incorporate and remodel more slowly than
autografts and introduce risk of inflammatory reactions
(chronic effusion) and disease transmission, and exhibit
tensile property reductions after sterilization and pres-
ervation [23, 24]. Mariscalco et al. [18] published a
systematic comparative review on autografted versus
non-irradiated allografted tissue for ACL reconstruction
and found no significant differences between graft
failure rates, postoperative laxities, or patient-reported
outcome scores. However, these findings were obtained
for patients in their late 20 s and early 30 s; thus,
caution was advised regarding extrapolating these find-
ings to younger, more active cohorts. Barrett et al. [3]
published a comparative study on ACL graft failure and
compared graft types with respect to age and Tegner
activity level. In patients aged B25 years, autograft
hamstrings and allografts were found to have signifi-
cantly higher failure rates than bone–patellar tendon–
bone autografts, indicating bone–patellar tendon–bone
autografts might be a better graft source for young,
active individuals.
Recently, use of the autologous hamstring tendon has
become more common than the patellar tendon for ACL
reconstruction [1, 21], and the majority of surgeons use
both the semitendinosus (ST) and gracilis tendons to pro-
duce a four-strand hamstring tendon [4, 16]. Furthermore,
the use of bone–patellar tendon–bone autografts, which
were previously considered the ‘‘gold standard,’’ is
decreasing owing to high levels of donor site morbidity [4].
However, although hamstring tendon harvesting causes
less donor site morbidity than bone–patellar tendon–bone
harvesting [16], some authors have suggested that a knee
flexion strength deficit may occur [8], and others have
reported that the flexion strength deficit in deep knee
flexion is more severe [8, 20, 26] after harvesting the ST
and gracilis tendons. Accordingly, it appears that ACL
reconstruction using ST and gracilis tendons causes greater
flexion strength deficit and donor site morbidity than
reconstruction using a single ST tendon.
The hypothesis of this study was that, if ACL recon-
struction using a single four-strand ST tendon without the
gracilis tendon could be accomplished, comparable knee
stability could be achieved and donor site morbidity is
reduced. Accordingly, this study was undertaken to com-
pare the clinical and functional results of ACL recon-
struction using an autologous four-strand ST tendon and a
gracilis (ST/G) tendon or a single autologous four-strand
ST tendon.
Materials and methods
Of 201 patients that underwent single-bundle ACL recon-
struction using a hamstring tendon between 2004 and 2010,
the medical records of 144 patients were evaluated retro-
spectively. These were ACL reconstruction cases in which
an extracortical suspension device was used for femoral
fixation, and a suture tied around a screw post and an
additional bioabsorbable screw were used for tibial fixa-
tion. Patients in the ST group (N = 85) underwent ACL
reconstruction using a single four-strand ST tendon,
whereas patients in the ST/G group (N = 59) underwent
ACL reconstruction using a four-strand ST tendon and a
gracilis tendon. As gender would have affected the results,
especially isokinetics muscle strength, only male patients
were included [7, 15, 19]. Exclusion criteria were multiple
ligament injuries (except a conservatively treated medial
collateral ligament [MCL] tear), subtotal or total menis-
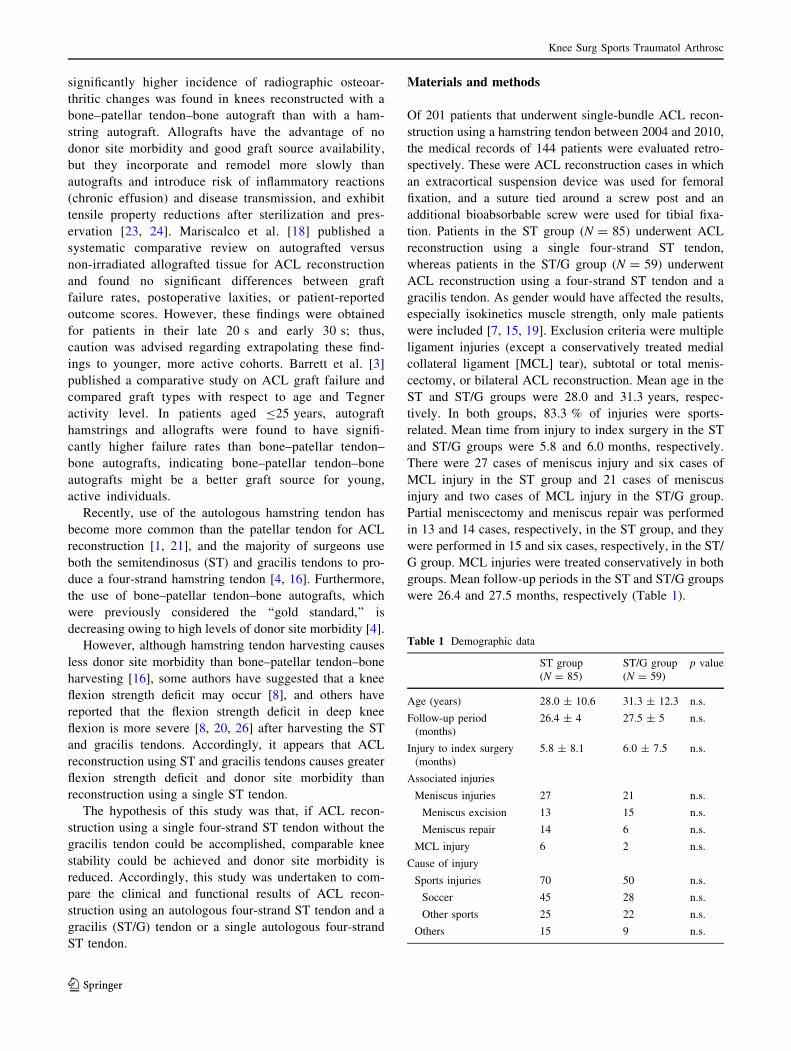
cectomy, or bilateral ACL reconstruction. Mean age in the
ST and ST/G groups were 28.0 and 31.3 years, respec-
tively. In both groups, 83.3 % of injuries were sports-
related. Mean time from injury to index surgery in the ST
and ST/G groups were 5.8 and 6.0 months, respectively.
There were 27 cases of meniscus injury and six cases of
MCL injury in the ST group and 21 cases of meniscus
injury and two cases of MCL injury in the ST/G group.
Partial meniscectomy and meniscus repair was performed
in 13 and 14 cases, respectively, in the ST group, and they
were performed in 15 and six cases, respectively, in the ST/
G group. MCL injuries were treated conservatively in both
groups. Mean follow-up periods in the ST and ST/G groups
were 26.4 and 27.5 months, respectively (Table 1).
Table 1 Demographic data
ST group
(N = 85)
ST/G group
(N = 59)
p value
Age (years) 28.0 ± 10.6 31.3 ± 12.3 n.s.
Follow-up period
(months)
26.4 ± 4 27.5 ± 5 n.s.
Injury to index surgery
(months)
5.8 ± 8.1 6.0 ± 7.5 n.s.
Associated injuries
Meniscus injuries 27 21 n.s.
Meniscus excision 13 15 n.s.
Meniscus repair 14 6 n.s.
MCL injury 6 2 n.s.
Cause of injury
Sports injuries 70 50 n.s.
Soccer 45 28 n.s.
Other sports 25 22 n.s.
Others 15 9 n.s.
Knee Surg Sports Traumatol Arthrosc
123
Surgical technique
The ST tendon was detected at the posteromedial tibial
margin and then detached from the periosteal membrane at
the proximal tibia. This technique allowed retrieval of an
additional 2 cm of ST tendon. The distal end of the ST
tendon was sutured with No. 2 Ti-Cron (Covidien�,
Argyle, NY). If the length of harvested ST tendon was
[28 cm, a 7-cm four-strand ST tendon was constructed by
double-folding; if the length was \28 cm, the gracilis
tendon was harvested, and a 10-cm four-strand ST/G ten-
don was constructed. The ACL remnant and stump was
preserved to the extent possible. A 7-mm diameter tunnel
was made to the tibial footprint center of the ACL. The
diameter of the four-strand ST tendon was 8.4 mm
(7–10 mm) and that of the ST/G tendon was 7.9 mm
(6–9 mm, p \ 0.05). The center of the femoral footprint
was targeted at the 10:30 (right knee) or 1:30 (left knee)
position to make the femoral tunnel. Femoral fixation was
performed using extracortical suspension devices (CL-En-
doButton, Smith and Nephew, Andover, MA or XO-But-
ton, Linvatec, Largo, FL). Graft cyclic loading was applied
20 times at 50 N. The knee flexion angle for tibial fixation
was 20� under 50 N of distal tension. Tibial fixation was
performed by tying sutures around a screw post with an
additional bioabsorbable screw. The portion of the distal
tibial tunnel not filled by the tendon was grafted using bone
obtained during reaming of the tibial tunnel.
Postoperative rehabilitation was performed using the
same protocol in both study groups. Briefly, quadriceps-
muscle-strengthening exercises were started immediately
after surgery. Weight bearing was allowed as tolerated with
an extension-locking brace, and active range of motion
exercises were started 2 weeks after surgery. In cases with
combined meniscus repair, range of motion exercises was
restricted to 90� of flexion until 6 weeks. Closed kinetic
chain exercises were allowed until 3 months after surgery,
after which open kinetic chain exercises were allowed.
Contact sports were allowed after 12 months if extension
and flexion power had recovered to 85 % of the normal,
contralateral side.
Outcome analysis
Clinical evaluations were performed using range of
motion; the Lachman test; the pivot-shift test; a KT-2000
arthrometer; the one-leg hop test; isokinetic muscle
strength; time of return to pre-injury activities; and Lys-
holm, Tegner activity; and International Knee Documen-
tation Committee (IKDC) subjective scores. A Biodex
system 3 pro and MVP dynamometer (Biodex Medical
Systems, Shirley, NY) were used for testing isokinetic
muscle strength in the sitting position. Briefly, patients
were seated on the Biodex testing device, and peak torque
in extension and flexion was measured four times at
angular velocities of 60 and 180�/s. Deficits of the involved
versus the uninvolved sides were compared between the
two study groups. The one-leg hop test was performed
three times per leg, and maximal distances were evaluated.
The limb symmetric index (involved versus uninvolved
sides) was also evaluated.
This retrospective study was approved by the Institu-
tional Review Board (certified by the Forum for Ethical
Review Committees in the Asian and Western Pacific
Region, ID number: 2013-08-009).
Statistical analysis
Student’s t test was used to analyze parametric continuous
data, the Mann–Whitney U test for non-parametric data,
and the Chi-square test for non-continuous data. Post hoc
power analysis was performed for the peak torque deficit.
Post hoc power was 42.5 % for the muscle strength ana-
lysis. Statistical significance was accepted for p values of
\0.05, and SPSS version 19 (SPSS; Chicago, IL, USA)
was used for all analyses.
Results
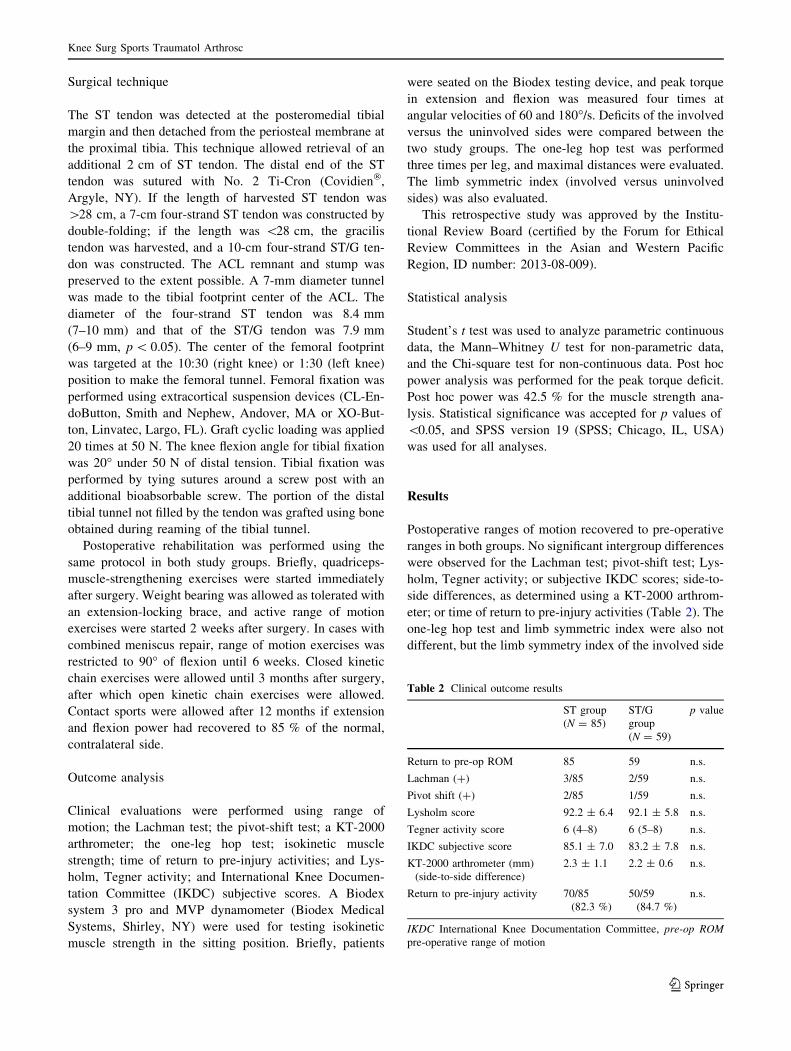
Postoperative ranges of motion recovered to pre-operative
ranges in both groups. No significant intergroup differences
were observed for the Lachman test; pivot-shift test; Lys-
holm, Tegner activity; or subjective IKDC scores; side-to-
side differences, as determined using a KT-2000 arthrom-
eter; or time of return to pre-injury activities (Table 2). The
one-leg hop test and limb symmetric index were also not
different, but the limb symmetry index of the involved side
Table 2 Clinical outcome results
ST group
(N = 85)
ST/G
group
(N = 59)
p value
Return to pre-op ROM 85 59 n.s.
Lachman (?) 3/85 2/59 n.s.
Pivot shift (?) 2/85 1/59 n.s.
Lysholm score 92.2 ± 6.4 92.1 ± 5.8 n.s.
Tegner activity score 6 (4–8) 6 (5–8) n.s.
IKDC subjective score 85.1 ± 7.0 83.2 ± 7.8 n.s.
KT-2000 arthrometer (mm)
(side-to-side difference)
2.3 ± 1.1 2.2 ± 0.6 n.s.
Return to pre-injury activity 70/85
(82.3 %)
50/59
(84.7 %)
n.s.
IKDC International Knee Documentation Committee, pre-op ROM
pre-operative range of motion
Knee Surg Sports Traumatol Arthrosc
123
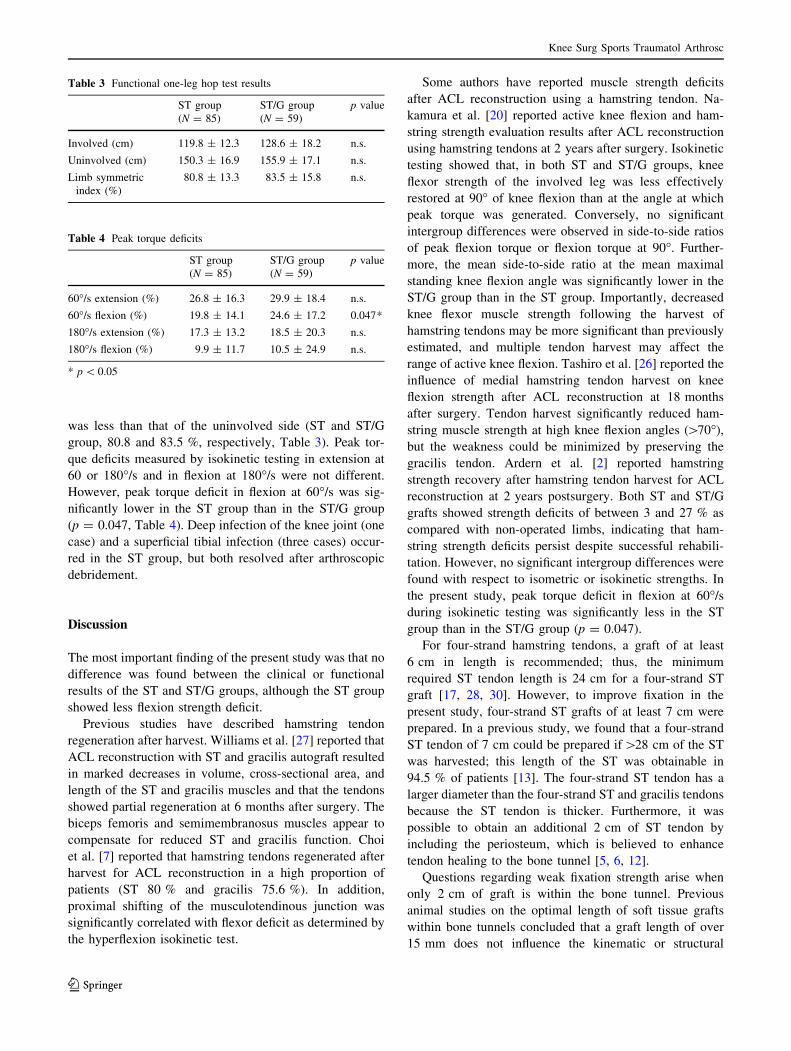
was less than that of the uninvolved side (ST and ST/G
group, 80.8 and 83.5 %, respectively, Table 3). Peak tor-
que deficits measured by isokinetic testing in extension at
60 or 180�/s and in flexion at 180�/s were not different.
However, peak torque deficit in flexion at 60�/s was sig-
nificantly lower in the ST group than in the ST/G group
(p = 0.047, Table 4). Deep infection of the knee joint (one
case) and a superficial tibial infection (three cases) occur-
red in the ST group, but both resolved after arthroscopic
debridement.
Discussion
The most important finding of the present study was that no
difference was found between the clinical or functional
results of the ST and ST/G groups, although the ST group
showed less flexion strength deficit.
Previous studies have described hamstring tendon
regeneration after harvest. Williams et al. [27] reported that
ACL reconstruction with ST and gracilis autograft resulted
in marked decreases in volume, cross-sectional area, and
length of the ST and gracilis muscles and that the tendons
showed partial regeneration at 6 months after surgery. The
biceps femoris and semimembranosus muscles appear to
compensate for reduced ST and gracilis function. Choi
et al. [7] reported that hamstring tendons regenerated after
harvest for ACL reconstruction in a high proportion of
patients (ST 80 % and gracilis 75.6 %). In addition,
proximal shifting of the musculotendinous junction was
significantly correlated with flexor deficit as determined by
the hyperflexion isokinetic test.
Some authors have reported muscle strength deficits
after ACL reconstruction using a hamstring tendon. Na-
kamura et al. [20] reported active knee flexion and ham-
string strength evaluation results after ACL reconstruction
using hamstring tendons at 2 years after surgery. Isokinetic
testing showed that, in both ST and ST/G groups, knee
flexor strength of the involved leg was less effectively
restored at 90� of knee flexion than at the angle at which
peak torque was generated. Conversely, no significant
intergroup differences were observed in side-to-side ratios
of peak flexion torque or flexion torque at 90�. Further-
more, the mean side-to-side ratio at the mean maximal
standing knee flexion angle was significantly lower in the
ST/G group than in the ST group. Importantly, decreased
knee flexor muscle strength following the harvest of
hamstring tendons may be more significant than previously
estimated, and multiple tendon harvest may affect the
range of active knee flexion. Tashiro et al. [26] reported the
influence of medial hamstring tendon harvest on knee
flexion strength after ACL reconstruction at 18 months
after surgery. Tendon harvest significantly reduced ham-
string muscle strength at high knee flexion angles ([70�),
but the weakness could be minimized by preserving the
gracilis tendon. Ardern et al. [2] reported hamstring
strength recovery after hamstring tendon harvest for ACL
reconstruction at 2 years postsurgery. Both ST and ST/G
grafts showed strength deficits of between 3 and 27 % as
compared with non-operated limbs, indicating that ham-
string strength deficits persist despite successful rehabili-
tation. However, no significant intergroup differences were
found with respect to isometric or isokinetic strengths. In
the present study, peak torque deficit in flexion at 60�/s
during isokinetic testing was significantly less in the ST
group than in the ST/G group (p = 0.047).
For four-strand hamstring tendons, a graft of at least
6 cm in length is recommended; thus, the minimum
required ST tendon length is 24 cm for a four-strand ST
graft [17, 28, 30]. However, to improve fixation in the
present study, four-strand ST grafts of at least 7 cm were
prepared. In a previous study, we found that a four-strand
ST tendon of 7 cm could be prepared if[28 cm of the ST
was harvested; this length of the ST was obtainable in
94.5 % of patients [13]. The four-strand ST tendon has a
larger diameter than the four-strand ST and gracilis tendons
because the ST tendon is thicker. Furthermore, it was
possible to obtain an additional 2 cm of ST tendon by
including the periosteum, which is believed to enhance
tendon healing to the bone tunnel [5, 6, 12].
Questions regarding weak fixation strength arise when
only 2 cm of graft is within the bone tunnel. Previous
animal studies on the optimal length of soft tissue grafts
within bone tunnels concluded that a graft length of over
15 mm does not influence the kinematic or structural
Table 3 Functional one-leg hop test results
ST group
(N = 85)
ST/G group
(N = 59)
p value
Involved (cm) 119.8 ± 12.3 128.6 ± 18.2 n.s.
Uninvolved (cm) 150.3 ± 16.9 155.9 ± 17.1 n.s.
Limb symmetric
index (%)
80.8 ± 13.3 83.5 ± 15.8 n.s.
Table 4 Peak torque deficits
ST group
(N = 85)
ST/G group
(N = 59)
p value
60�/s extension (%) 26.8 ± 16.3 29.9 ± 18.4 n.s.
60�/s flexion (%) 19.8 ± 14.1 24.6 ± 17.2 0.047*
180�/s extension (%) 17.3 ± 13.2 18.5 ± 20.3 n.s.
180�/s flexion (%) 9.9 ± 11.7 10.5 ± 24.9 n.s.
* p \ 0.05
Knee Surg Sports Traumatol Arthrosc
123

properties of the knee joint [22, 29, 32]. In addition, pre-
vious clinical studies have reported good results for ACL
reconstruction using a single ST tendon [9, 14, 25, 31].
The limitations of this study are that it was performed
retrospectively, associated injuries differed in the two
groups, muscle strengths were not compared in hyperflex-
ion, and correlations between functional test results and
flexion strength deficits were not analyzed. Furthermore,
the sample size was not calculated adequately because the
study had multiple end results, including clinical outcomes
(knee stability, clinical score, and return to pre-injury
activity) and muscle strength; thus, the statistical power
might be low.
Conclusion
This study shows that good results can be obtained using a
single ST graft without the gracilis tendon for ACL
reconstruction without adversely affecting stability and
with less donor site morbidity. The clinical relevance of the
present study is that it shows ACL reconstruction using a
single ST tendon reduces donor site morbidity without
compromising joint stability.
Acknowledgments This research was supported by the Kyungpook
National University Research Fund, 2012.
References
1. Amis AA, Jakob RP (1998) Anterior cruciate ligament graft
positioning, tensioning and twisting. Knee Surg Sports Traumatol
Arthrosc 6(Suppl 1):S2–12
2. Ardern CL, Webster KE, Taylor NF, Feller JA (2010) Hamstring
strength recovery after hamstring tendon harvest for anterior
cruciate ligament reconstruction: a comparison between graft
types. Arthroscopy 26:462–469
3. Barrett AM, Craft JA, Replogle WH, Hydrick JM, Barrett GR
(2011) Anterior cruciate ligament graft failure: a comparison of
graft type based on age and Tegner activity level. Am J Sports
Med 39:2194–2198
4. Chechik O, Amar E, Khashan M, Lador R, Eyal G, Gold A
(2013) An international survey on anterior cruciate ligament
reconstruction practices. Int Orthop 37:201–206
5. Chen CH, Chen WJ, Shih CH, Chou SW (2004) Arthroscopic
anterior cruciate ligament reconstruction with periosteum-envel-
oping hamstring tendon graft. Knee Surg Sports Traumatol
Arthrosc 12:398–405
6. Chen CH, Chen WJ, Shih CH, Yang CY, Liu SJ, Lin PY (2003)
Enveloping the tendon graft with periosteum to enhance tendon–
bone healing in a bone tunnel: a biomechanical and histologic
study in rabbits. Arthroscopy 19:290–296
7. Choi JY, Ha JK, Kim YW, Shim JC, Yang SJ, Kim JG (2012)
Relationships among tendon regeneration on MRI, flexor
strength, and functional performance after anterior cruciate lig-
ament reconstruction with hamstring autograft. Am J Sports Med
40:152–162
8. Coombs R, Cochrane T (2001) Knee flexor strength following
anterior cruciate ligament reconstruction with the semitendinosus
and gracilis tendons. Int J Sports Med 22:618–622
9. Gobbi A, Domzalski M, Pascual J, Zanazzo M (2005) Hamstring
anterior cruciate ligament reconstruction: is it necessary to sac-
rifice the gracilis? Arthroscopy 21:275–280
10. Goldblatt JP, Fitzsimmons SE, Balk E, Richmond JC (2005)
Reconstruction of the anterior cruciate ligament: meta-analysis of
patellar tendon versus hamstring tendon autograft. Arthroscopy
21:791–803
11. Holm I, Oiestad BE, Risberg MA, Aune AK (2010) No difference
in knee function or prevalence of osteoarthritis after reconstruc-
tion of the anterior cruciate ligament with 4-strand hamstring
autograft versus patellar tendon–bone autograft: a randomized
study with 10-year follow-up. Am J Sports Med 38:448–454
12. Kyung HS, Kim SY, Oh CW, Kim SJ (2003) Tendon-to-bone
tunnel healing in a rabbit model: the effect of periosteum aug-
mentation at the tendon-to-bone interface. Knee Surg Sports
Traumatol Arthrosc 11:9–15
13. Kyung HS, Kim TG, Oh CW, Yoon SH (2009) Anterior cruciate
ligament reconstruction with a four-strand single semitendinosus
tendon autograft. J Korean Arthrosc Soc 13:138–142
14. Kyung HS, Oh CW, Lee HJ (2011) Clinical evaluation of anterior
cruciate ligament reconstruction with remnant-preserving tech-
nique: method using single four-strand semitendinosus tendon.
J Korean Orthop Assoc 46:60–67
15. Lephart SM, Ferris CM, Riemann BL, Myers JB, Fu FH (2002)
Gender differences in strength and lower extremity kinematics
during landing. Clin Orthop Relat Res 401:162–169
16. Li S, Chen Y, Lin Z, Cui W, Zhao J, Su W (2012) A systematic
review of randomized controlled clinical trials comparing ham-
string autografts versus bone–patellar tendon–bone autografts for
the reconstruction of the anterior cruciate ligament. Arch Orthop
Trauma Surg 132:1287–1297
17. Maeda A, Shino K, Horibe S, Nakata K, Buccafusca G (1996)
Anterior cruciate ligament reconstruction with multistranded
autogenous semitendinosus tendon. Am J Sports Med 24:504–509
18. Mariscalco MW, Magnussen RA, Mehta D, Hewett TE, Flanigan
DC, Kaeding CC (2014) Autograft versus nonirradiated allograft
tissue for anterior cruciate ligament reconstruction: a systematic
review. Am J Sports Med 42:492–499
19. Myer GD, Ford KR, Barber Foss KD, Liu C, Nick TG, Hewett TE
(2009) The relationship of hamstrings and quadriceps strength to
anterior cruciate ligament injury in female athletes. Clin J Sport
Med 19:3–8
20. Nakamura N, Horibe S, Sasaki S et al (2002) Evaluation of active
knee flexion and hamstring strength after anterior cruciate liga-
ment reconstruction using hamstring tendons. Arthroscopy
18:598–602
21. Pinczewski L, Roe J, Salmon L (2009) Why autologous ham-
string tendon reconstruction should now be considered the gold
standard for anterior cruciate ligament reconstruction in athletes.
Br J Sports Med 43:325–327
22. Qi L, Chang C, Jian L, Xin T, Gang Z (2011) Effect of varying
the length of soft-tissue grafts in the tibial tunnel in a canine
anterior cruciate ligament reconstruction model. Arthroscopy
27:825–833
23. Scheffler SU, Schmidt T, Gangey I, Dustmann M, Unterhauser F,
Weiler A (2008) Fresh-frozen free-tendon allografts versus
autografts in anterior cruciate ligament reconstruction: delayed
remodeling and inferior mechanical function during long-term
healing in sheep. Arthroscopy 24:448–458
24. Scheffler SU, Unterhauser FN, Weiler A (2008) Graft remodeling
and ligamentization after cruciate ligament reconstruction. Knee
Surg Sports Traumatol Arthrosc 16:834–842
Knee Surg Sports Traumatol Arthrosc
123

25. Streich NA, Friedrich K, Gotterbarm T, Schmitt H (2008)
Reconstruction of the ACL with a semitendinosus tendon graft: a
prospective randomized single blinded comparison of double-
bundle versus single-bundle technique in male athletes. Knee
Surg Sports Traumatol Arthrosc 16:232–238
26. Tashiro T, Kurosawa H, Kawakami A, Hikita A, Fukui N (2003)
Influence of medial hamstring tendon harvest on knee flexor
strength after anterior cruciate ligament reconstruction. A
detailed evaluation with comparison of single- and double-tendon
harvest. Am J Sports Med 31:522–529
27. Williams GN, Snyder-Mackler L, Barrance PJ, Axe MJ, Buchanan
TS (2004) Muscle and tendon morphology after reconstruction of
the anterior cruciate ligament with autologous semitendinosus–
gracilis graft. J Bone Joint Surg Am 86-A:1936–1946
28. Xie G, Huangfu X, Zhao J (2012) Prediction of the graft size of
4-stranded semitendinosus tendon and 4-stranded gracilis tendon
for anterior cruciate ligament reconstruction: a Chinese Han
patient study. Am J Sports Med 40:1161–1166
29. Yamazaki S, Yasuda K, Tomita F, Minami A, Tohyama H (2006)
The effect of intraosseous graft length on tendon–bone healing in
anterior cruciate ligament reconstruction using flexor tendon.
Knee Surg Sports Traumatol Arthrosc 14:1086–1093
30. Yasumoto M, Deie M, Sunagawa T, Adachi N, Kobayashi K,
Ochi M (2006) Predictive value of preoperative 3-dimensional
computer tomography measurement of semitendinosus tendon
harvested for anterior cruciate ligament reconstruction. Arthros-
copy 22:259–264
31. Zamarra G, Fisher MB, Woo SL, Cerulli G (2009) Biomechanical
evaluation of using one hamstrings tendon for ACL reconstruc-
tion: a human cadaveric study. Knee Surg Sports Traumatol
Arthrosc 18:11–19
32. Zantop T, Ferretti M, Bell KM, Brucker PU, Gilbertson L, Fu FH
(2008) Effect of tunnel-graft length on the biomechanics of
anterior cruciate ligament-reconstructed knees: intra-articular
study in a goat model. Am J Sports Med 36:2158–2166
Knee Surg Sports Traumatol Arthrosc
123





























