Embed Size (px)
Citation preview

Comparison of Aortic ElasticityDetermined by Cardiovascular Magnetic
Resonance Imaging in Obese VersusLean Adults
Peter G. Danias, MD, PhD, Nicholas A. Tritos, MD, DSc, Matthias Stuber, PhD,Rene M. Botnar, PhD, Kraig V. Kissinger, BS, RTR, RTMR, and Warren J. Manning, MD
The vascular properties of large vessels in the obesehave not been adequately studied. We used cardiovas-cular magnetic resonance imaging to quantify the cross-sectional area and elastic properties of the ascendingthoracic and abdominal aorta in 21 clinically healthyobese young adult men and 25 men who were age-matched lean controls. Obese subjects had greater max-imal cross-sectional area of the ascending thoracic aorta(984 � 252 vs 786 � 109 mm2, p <0.01) and of theabdominal aorta (415 � 71 vs 374 � 51 mm2, p<0.05). When indexed for height the differences per-sisted, but when indexed for body surface area, a sig-nificant difference between groups was found only forthe maximal abdominal aortic cross-sectional area. Theobese subjects also had decreased abdominal aortic
elasticity, characterized by 24% lower compliance(0.0017 � 0.0004 vs 0.0021 � 0.0005 mm2/kPa/mm,p <0.01), 22% higher stiffness index � (6.0 � 1.5 vs 4.9� 0.7, p <0.005), and 41% greater pressure–strainelastic modulus (72 � 25 vs 51 � 9, p <0.005). At theascending thoracic aorta, only the pressure–strain elas-tic modulus was different between obese and lean sub-jects (85 � 42 vs 65 � 26 kPa, respectively; p <0.05),corresponding to a 31% difference—but arterial com-pliance and stiffness index were not significantly dif-ferent between groups. In clinically healthy youngadult obese men, obesity is associated with increasedcross-sectional aortic area and decreased aorticelasticity. �2003 by Excerpta Medica, Inc.
(Am J Cardiol 2003;91:195–199)
Vascular elasticity of the small and medium sizevessels is most commonly measured by ultra-
sonography. However, this approach has limited valuefor the evaluation of large vessels—such as the aor-ta—due to decreased acoustic penetration, particu-larly in obese subjects. As an alternative strategy,cardiovascular magnetic resonance imaging (MRI)can accurately assess aortic elasticity. It providescross-sectional images of the aorta with combinedhigh spatial and temporal resolution, and data acqui-sition is not restricted by body habitus or imagingplane.1–3 Accordingly, we used MRI to measure aorticelasticity of the ascending thoracic and abdominalaorta in a well-defined population of clinically healthyobese adult men, and compared these data with acontrol group of age-matched healthy lean adult men.
METHODSThe study was approved by the hospital Committee
on Clinical Investigation, and written informed con-
sent was obtained from all subjects. All testing wasperformed in the morning, after an overnight fast. Thesubjects’ height and weight were measured using awall-mounted stadiometer (Holtain Ltd., CrymychPembs, United Kingdom) and a 600-lb capacity elec-tronic scale (model 0501; ACME, San Leandro, Cal-ifornia). The subjects’ body mass index (BMI), calcu-lated as weight (kilograms) divided by height (meters)squared, and body surface area4 were recorded. Toensure that subjects were not hypertensive at rest,bilateral arm blood pressure was obtained (using alarge size cuff for obese subjects) with an automaticsphygmomanometer (Dinamap; GE Medical Systems,Milwaukee, Wisconsin). Fasting venous blood “fin-gerstick” glucose was measured on a portable glucom-eter (OneTouch; LifeScan, Milpitas, California) toexclude subjects with unknown diabetes. Data regard-ing subjects’ habits on exercise (hours per week),coffee (cups per week), and alcohol consumption(servings per week) were also collected.
Subjects: Forty-six healthy men aged 20 to 40years, including 21 obese subjects (BMI�30 kg/m2)and 25 lean controls (BMI 19 to 25 kg/m2), wererecruited. Exclusion criteria were: (1) known coexis-tent cardiac diseases; (2) hypertension under dietary orpharmacologic treatment, or cuff arm blood pressureat the time of testing�160/90 mm Hg; (3) endocrinediseases, including diabetes mellitus under dietary orpharmacologic treatment, or fasting venous blood fin-gerstick glucose�105 mg/dl; (4) use of any hormonepreparations or other medications that directly affectendocrine function within 2 months of participation;
From the Cardiovascular and Endocrinology Divisions, Departments ofMedicine and Radiology, Beth Israel Deaconess Medical Center,Boston, Massachusetts; Joslin Diabetes Center, Harvard MedicalSchool, Boston, Massachusetts; and Philips Medical Systems, Best,The Netherlands. This study was supported in part by Grant RR 01032to the Beth Israel Deaconess Medical Center General Clinical Re-search Center from the National Institutes of Health, Bethesda,Maryland. Manuscript received June 6, 2002; revised manuscriptreceived and accepted August 30, 2002.
Address for reprints: Peter G. Danias, MD, PhD, Beth Israel Dea-coness Medical Center, 330 Brookline Avenue, Boston, Massachu-setts 02215. E-mail: [email protected].
195©2003 by Excerpta Medica, Inc. All rights reserved. 0002-9149/03/$–see front matterThe American Journal of Cardiology Vol. 91 January 15, 2003 PII S0002-9149(02)03109-0

(5) known hepatic or renal dysfunction; (6) previouslydiagnosed sleep-apnea syndrome, or �2 symptomssuggestive of this disorder, including loud snoring,frequent nocturnal awakening (�3/night period), day-time hypersomnolence, and frequent early-morningheadaches; (7) recent (�2 weeks) acute illness orinjury; (8) recent (�1 month) weight gain or weightloss of �5 kg; (9) previous or current use of cocaineor intravenous recreational drugs; and (10) contrain-dications to MRI, including severe claustrophobia andimplanted metallic prostheses or devices.
Cardiovascular MRI: All imaging was performedusing a commercial 1.5-T whole body scanner (PhilipsGyroscan ACS/NT, Best, The Netherlands) with a60-cm diameter bore, Powertrak 6000 (Philips Gy-roscan) gradients (23 mT/min, rise time 219 �s), a5-element cardiac synergy coil for imaging of theascending thoracic aorta, and a body coil for imagingof the abdominal aorta.
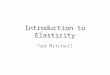
After initial localizing “scout” images to identifythe heart, aorta, and kidneys, oblique cine images(slice thickness 8 mm) were obtained perpendicular tothe long axis of the aorta at 2 levels: (1) at theascending thoracic aorta, immediately distal to thesinotubular ridge, and (2) at the abdominal aorta,immediately proximal (cephalad) to the renal arteries(Figure 1). The imaging sequence was a fast-fieldecho echoplanar gradient-echo sequence,5 with a tem-poral resolution of 25 ms. For the ascending thoracicaorta, we used breath holding to minimize respiratorymotion artifacts. The breath-hold duration was 12 to15 seconds, depending on the subjects’ heart rate.
During the MRI examination, blood pressure wasnoninvasively measured with an automated sphygmo-manometer (Dinamap, GE Medical Systems) using alarge cuff on the left leg. At least 5 measurementswere obtained during the MRI examination. The 2extreme values were disregarded, and the mean of theremaining values was used for systolic and diastolicblood pressure in the data analysis. The mean arterialblood pressure was calculated using the formula:mean blood pressure � [systolic blood pressure � (2� diastolic blood pressure)] � 3 .
Data analysis: Aortic contours for all short-axisimages were manually traced off-line on a commercialanalysis workstation (EasyVision 4; Philips MedicalSystems, Best, The Netherlands). All tracing was per-formed by a single experienced observer, blinded tosubject identity. Zoomed-in images were used to min-imize tracing error and remove potential bias fromappreciation of amount of subcutaneous adipose tis-sue. Using the commercially available analysis pack-age, the aortic area was calculated for all phases of thecardiac cycle. Using a similar analytic method, aninterobserver variability of 5% has been reported byGroenink et al,2 and a measurement error of 4% to 6%has been reported by Vulliemoz et al.3 We performed2 separate analyses; in the first (actual), we used theraw data to determine the maximal and minimal aorticcross-sectional areas and to calculate aortic elasticity.The time-to-maximal cross-sectional area was alsorecorded and expressed as percent of the RR cycle
FIGURE 1. Images of the aorta were obtained at the sinotubularridge of the ascending thoracic aorta (A) and just cephalad tothe origin of the renal arteries of the abdominal aorta (B).
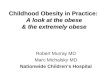
FIGURE 2. Actual measurements of the cross-sectional aortic areaat the ascending thoracic aorta (A) and abdominal aorta (B) in 1study subject. The third order polynomial fitted curves, whichsmoothen the data and may underestimate observed differences,and the corresponding equations are shown. CSA � cross-sec-tional area.
196 THE AMERICAN JOURNAL OF CARDIOLOGY� VOL. 91 JANUARY 15, 2003

(%RR). In the second analysis (modeled), we fitted athird-order polynomial equation to the raw data andused this equation to determine the curve maximumsand minimums that corresponded to the maximal andminimal cross-sectional areas of the aorta, respective-ly.2 This analysis offers a “smoothening” effect on thedata and may decrease individual measurement errors,but this analysis may underestimate differences be-tween the 2 groups (Figure 2).
The parameters measured and used to describeaortic elasticity were6:
1. Arterial compliance (AC), defined as the abso-lute volume increase in a segment of the aorta duringthe cardiac cycle divided by the arterial pulse pres-sure. The AC per unit length, measured in millimeterssquared per kilo-Pascals per millimeter is:
AC � ��D�s2 � D�d2/�4�P�s � P�d�
(1)
where D(s) and D(d) are the systolic and diastolicdiameters of the artery and P(s) and P(d) are thesystolic and diastolic blood pressures, respectively.
2. Stiffness index (SI), defined as the natural log-arithm of the ratio of systolic to diastolic blood pres-sure divided by the circumferential arterial strain(CAS), which is the fractional increase in arterialdiameter during the cardiac cycle. Thus, SI is a unit-less quantity and considered to be relatively indepen-dent of blood pressure:
SI � ln�P�s/P�d/CAS, (2)
where CAS � [D(s) D(d)]/D(d).3. Pressure–strain elastic modulus (Ep), defined as
the arterial pulse pressure divided by the CAS, and itis measured in kilo-Pascals:
Ep � �P�s � P�d/CAS. (3)
Statistical analysis: All data are presented as mean� 1 SD. Comparisons between groups were per-formed using the Student’s t test for all variables.When appropriate, analysis of covariance was per-formed to adjust for possible covariates. All statistical
comparisons were 2-tailed, and p�0.05 was considered significant.
RESULTSThe demographic characteristics
of the entire study population arelisted in Table 1. All subjects com-pleted the cardiovascular MRI exam-ination without complications.
Analysis of the measured (actual)values of the aortic cross-sectionalarea are listed in Table 2. The obesesubjects had larger maximal andminimal cross-sectional areas of theascending thoracic aorta and the ab-dominal aorta, even when adjustedfor height or height2.7 (p �0.05 for
all comparisons, data not shown). However, whenbody surface area was indexed, aortic cross-sectionaldifferences persisted only for the maximal abdominalaortic cross-sectional area (p �0.05).
The time-to-maximal cross-sectional aortic areawas similar between the obese and lean groups for theascending aorta (p � NS). There was a trend toward adelay in attaining maximal cross-sectional area in theabdominal aorta in obese subjects compared with thelean controls (RR% 0.42 � 0.07% vs 0.38 � 0.09%,p � 0.07, in obese subjects vs lean controls, respec-tively).
In the ascending thoracic aorta, obese subjects hadhigher Ep (p �0.05) but there were no significantdifferences between obese and lean subjects in ACand SI. With respect to the abdominal aorta, obesesubjects had significantly lower aortic elasticity by allmeasures, indicated by lower AC (p �0.05), higher SI(p �0.005), and greater Ep (p �0.001). When adjust-ment was performed for mean arterial blood pressure,differences between groups persisted for the SI andthe Ep of the abdominal aorta (p �0.05 for bothcomparisons).
Analysis of the modeled maximums and mini-mums of the aortic cross-sectional area values derivedfrom the fitted third order polynomial curves is pre-sented in Table 3. Again, obese subjects had largermaximal cross-sectional areas in the ascending tho-racic aorta (p �0.01) and the abdominal aorta (p�0.05). There were no significant differences in anyof the aortic elasticity indexes between obese and leansubjects with respect to the ascending thoracic aorta.However, regarding the abdominal aorta, obese sub-jects had significantly lower aortic elasticity, indicatedby lower AC (p �0.05) and higher Ep (p �0.05).Obese subjects tended to also have a higher SI com-pared with the lean controls (p � 0.06).
DISCUSSIONIn this cross-sectional study of obese and lean
young adult men, we used cardiovascular MRI tocharacterize the aortic elastic properties associatedwith obesity and leanness. Obese subjects had a largercross-sectional area of both the ascending thoracic andabdominal aorta. The abdominal aortic elasticity was
TABLE 1 Demographic Characteristics of the Study Population
Variable Obese Subjects Lean Subjects p Value
Age (yrs) 30 � 8 29 � 5 NSHeight (m) 1.77 � 0.06 1.76 � 0.07 NSWeight (kg) 109.3 � 12.6 70.4 � 5.9 �0.001BMI (kg/m2) 34.7 � 3.0 22.7 � 1.7 �0.001Exercise (hours/wk) 3.5 � 2.9 3.7 � 3.4 NSCoffee (cups/wk) 2.7 � 4.1 5.1 � 6.5 NSAlcohol (servings/wk) 1.5 � 1.4 2.2 � 1.6 NSSystolic blood pressure (mm Hg) 138 � 18 115 � 16 �0.001Diastolic blood pressure (mm Hg) 54 � 9 50 � 8 NSMean pulse pressure (mm Hg) 84 � 15 65 � 12 �0.001Mean blood pressure (mm Hg)* 82 � 11 72 � 10 �0.005
*Mean blood pressure � ([2 � diastolic blood pressure � systolic blood pressure] /3).
MISCELLANEOUS/AORTIC ELASTICITY IN OBESITY 197

also decreased in the obese compared with lean con-trols. To our knowledge this is the first study usingMRI to evaluate aortic elasticity in the obese and ithighlights the potential advantages of this technologyin a patient population that is often difficult to assessusing conventional noninvasive imaging modalities.
Although we specifically excluded subjects withhypertension and those with known or probable sleepapnea (a well-known predisposing factor for hyper-tension in the obese7,8), systolic blood pressure at restwas still higher in the obese group. Without excludingsubjects with sleep apnea, previous studies9,10 havealso shown that even within the normal range, theobese tend to have higher blood pressures than age-and gender-matched lean persons. Therefore, it wouldbe impractical to perfectly match the obese and leangroups for age and blood pressure. Another inherentlimitation of our approach is that it was not feasible tononinvasively obtain an accurate central (aortic) pres-sure measurement. The measured peripheral bloodpressure is influenced by reflectance pressure wavesthat cannot be accounted for by our methods. Notwith-standing these inherent methodologic limitations, andalthough the increased systolic arterial blood pressurefound in the obese could contribute to differences inaortic elasticity between the obese and lean groups,our analysis adjusting for mean arterial blood pressuresuggested that obesity also likely impairs abdominal
aortic elasticity directly, independent of hemodynamicparameters. We speculate that abnormal aortic elastic-ity in the obese may be associated with structuralchanges in the vascular wall, or simply may be due toexternal compression of the vessel by the increasedabdominal contents and fat. The latter possibility mayalso explain why the differences in aortic elasticitybetween obese and lean subjects were more pro-nounced at the abdominal aorta, a location subject todirect compression from intra-abdominal contents andsubcutaneous abdominal fat in the supine position.
The cross-sectional area of the aorta was larger inthe obese subjects. Such small changes in aortic cross-sectional area could only be detected with imagingtechniques that have high resolution and are not at-tenuated by fat content, such as MRI and computedtomography. The aortic enlargement may represent anadaptation process to accommodate for the increasedblood volume that is seen in obese persons.11,12 Analternative explanation may be that the larger aorticlumen is associated with higher systolic blood pres-sure. An underlying abnormality specific to obesitycould also be speculated, given the coexistence ofstructural (increased cross-sectional area) and func-tional (decreased elasticity) aortic abnormalities.
Our data contradict a previous study by Oren etal,12 who measured ascending aortic compliance asthe ratio of the pulse pressure divided by the stroke
TABLE 2 Aortic Dimensions and Elasticity Measures in Obese and Lean Subjects, Based on the Measured (actual) Maximal andMinimal Aortic Cross-sectional Areas
Obese Subjects Lean Subjects % Difference* p Value
Ascending thoracic aortaMaximal cross-sectional area (mm2) 948 � 252 786 � 109 �21 �0.01Minimal cross-sectional area (mm2) 727 � 218 600 � 92 �21 �0.05AC (mm2/kPa/mm) 0.0036 � 0.0016 0.0039 � 0.0015 8 NSSI 7.2 � 3.1 6.3 � 2.2 �14 NSEp (kPa) 85 � 42 65 � 26 �31 �0.05
Abdominal aortaMaximal cross-sectional area (mm2) 415 � 71 374 � 51 �11 �0.05Minimal cross-sectional area (mm2) 308 � 63 273 � 37 �13 �0.05AC (mm2/kPa/mm) 0.0017 � 0.0004 0.0021 � 0.0005 19 �0.01SI 6.0 � 1.5 4.9 � 0.7 �22 �0.005Ep (kPa) 72 � 25 51 � 9 �41 �0.001
*The percent difference was calculated using the mean for the lean group as the reference value.
TABLE 3 Aortic Elasticity Indexes in the Obese and Lean Groups, Based on the Fitted Third Polynomial Curves With ModeledMaximal and Minimal Aortic Diameters
Obese Subjects Lean Subjects % Difference p Value
Ascending thoracic aortaMaximal cross-sectional area (mm2) 898 � 225 753 � 109 �19 �0.01Minimal cross-sectional area (mm2) 745 � 231 608 � 108 �23 �0.05AC (mm2/kPa/mm) 0.0025 � 0.0011 0.0031 � 0.0019 19 0.2SI 11.4 � 5.8 10.9 � 8.9 �5 0.8Ep (kPa) 137 � 78 112 � 90 �22 0.3
Abdominal aortaMaximal cross-sectional area (mm2) 392 � 69 353 � 48 �11 �0.05Minimal cross-sectional area (mm2) 286 � 67 256 � 40 �12 0.06AC (mm2/kPa/mm) 0.0017 � 0.0005 0.0020 � 0.0005 15 �0.05SI 5.9 � 2.5 4.9 � 1.2 �20 0.064Ep (kPa) 72 � 38 51 � 16 �41 �0.05
198 THE AMERICAN JOURNAL OF CARDIOLOGY� VOL. 91 JANUARY 15, 2003

volume in 11 normotensive obese and 13 nonobeseadults. The investigators reported that the obese sub-jects had lower peripheral vascular resistance associ-ated with increased vascular compliance. In our study,the pulse pressure divided by the stroke volume wassimilar between the obese and lean groups (p � 0.10,data not shown). There are several possible explana-tions for this discrepancy. In the study by Oren et al,12
fewer subjects were evaluated, the presence of cardio-vascular diseases or other conditions that could affectvascular elasticity were not excluded, the subjectswere older than in our study, and both men andwomen were included. Furthermore, in the study byOren et al,12 the diastolic decay of the blood pressuretracing (another measure of aortic compliance) wasfound to be similar between the 2 groups, demonstrat-ing internal inconsistency. Our analysis evaluated sev-eral indexes that are accepted as more accurate de-scriptors of vascular elasticity,6 many of which rely onthe aortic cross-sectional area, a parameter that dif-fered between the obese and lean groups, but wasneither assessed nor adjusted for by Oren et al.12
1. Resnick LM, Militianu D, Cunnings AJ, Pipe JG, Evelhoch JL, Soulen RL.Direct magnetic resonance determination of aortic distensibility in essential
hypertension: relation to age, abdominal visceral fat, and in situ intracellular freemagnesium. Hypertension 1997;30:654–659.2. Groenink M, de Roos A, Mulder BJ, Spaan JA, van der Wall EE. Changes inaortic distensibility and pulse wave velocity assessed with magnetic resonanceimaging following beta-blocker therapy in the Marfan syndrome. Am J Cardiol1998;82:203–208.3. Vulliemoz S, Stergiopulos N, Meuli R. Estimation of local aortic elasticproperties with MRI. Magn Reson Med 2002;47:649–654.4. Dubois D, Dubois EF. A formula to estimate the approximate surface area ifheight and weight are known. Arch Intern Med 1916;17:863–871.5. Salton CJ, Chuang ML, O’Donnell CJ, Kupka MJ, Larson MG, Kissinger KV,Edelman RR, Levy D, Manning WJ. Gender differences and normal left ventric-ular anatomy in an adult population free of hypertension. A cardiovascularmagnetic resonance study of the Framingham Heart Study offspring cohort. J AmColl Cardiol 2002;39:1055–1060.6. Salomaa V, Riley W, Kark JD, Nardo C, Folsom AR. Non–insulin-dependentdiabetes mellitus and fasting glucose and insulin concentrations are associatedwith arterial stiffness indexes. The ARIC Study. Atherosclerosis Risk in Com-munities Study. Circulation 1995;91:1432–1443.7. Weiss JW, Remsburg S, Garpestad E, Ringler J, Sparrow D, Parker JA.Hemodynamic consequences of obstructive sleep apnea. Sleep 1996;19:388–397.8. Pankow W, Lies A, Lohmann FW. Sleep-disordered breathing and hyperten-sion. N Engl J Med 2000;343:966.9. de Simone G, Devereux RB, Roman MJ, Alderman MH, Laragh JH. Relationof obesity and gender to left ventricular hypertrophy in normotensive and hyper-tensive adults. Hypertension 1994;23:600–606.10. Pozzan R, Brandao AA, da Silva SL, Brandao AP. Hyperglycemia, hyper-insulinemia, overweight, and high blood pressure in young adults: the Rio deJaneiro Study. Hypertension 1997;30:650–653.11. Messerli FH, Christie B, DeCarvalho JG, Aristimuno GG, Suarez DH,Dreslinski GR, Frohlich ED. Obesity and essential hypertension. Hemodynamics,intravascular volume, sodium excretion, and plasma renin activity. Arch InternMed 1981;141:81–85.12. Oren S, Grossman E, Frohlich ED. Arterial and venous compliance in obeseand nonobese subjects. Am J Cardiol 1996;77:665–667.
MISCELLANEOUS/AORTIC ELASTICITY IN OBESITY 199