Embed Size (px)
Citation preview

AJR:203, August 2014 W199
increasing [5]. Therefore, precise description of ACL rupture patterns could lead to a more refined approach for reconstructive surgery [6]. A few studies regarding the ability of MRI to detect isolated anteromedial or pos-terolateral bundle tears in patients with ACL injury have been reported. Van Dyck et al. [7] reported that only 6% of surgically con-firmed partial ACL tears were correctly di-agnosed as isolated ACL bundle tears and suggested that it is frequently not possible to specify whether the tear is in the anteromedial
Comparison Between Arthroscopic Findings and 1.5-T and 3-T MRI of Oblique Coronal and Sagittal Planes of the Knee for Evaluation of Selective Bundle Injury of the Anterior Cruciate Ligament
Hee Jin Park1,2 Sam Soo Kim2 So Yeon Lee1 Noh Hyuck Park3 Jin Hwan Ahn4 Eun Chul Chung1 Ji Yeon Park1 Mi-Sung Kim1
Park HJ, Kim SS, Lee SY, et al.
1 Department of Radiology, Sungkyunkwan University School of Medicine, Kangbuk Samsung Hospital, Seoul, Korea.
2 Department of Radiology, Kangwon National University School of Medicine, Kangwon, Korea.
3 Department of Radiology, Myongji Hospital. Dugyang-ku, Hwajong-dong 697-24, Koyang Kyunggido 412-270, Korea. Address correspondence to N. H. Park ([email protected]).
4 Department of Orthopaedic Surgery, Sungkyunkwan University School of Medicine, Kangbuk Samsung Hospital, Seoul, Korea.
Musculoskeleta l Imaging • Or ig ina l Research
WEB This is a web exclusive article.
AJR 2014; 203:W199–W206
0361–803X/14/2032–W199
© American Roentgen Ray Society
The anterior cruciate ligament (ACL) is composed of two bun-dles, the anteromedial and pos-terolateral bundles, which have
complementary roles in stabilization [1, 2]. MRI is the most commonly used diagnostic modality for ACL injuries [3]. However, MRI diagnosis of partial ACL tears is diffi-cult, as is clinical assessment [4]. Because the aim of ACL reconstruction is to repro-duce the function of the native ACL, double-bundle or selective-bundle reconstruction is
Keywords: anterior cruciate ligament, MRI, oblique, selective-bundle tear
DOI:10.2214/AJR.13.11571
Received July 15, 2013; accepted after revision October 31, 2013.
OBJECTIVE. The purpose of this study was to evaluate the diagnostic usefulness of combining oblique sagittal and oblique coronal MRI views of the anterior cruciate ligament (ACL) with traditional orthogonal views for the evaluation of selective-bundle ACL injury and to evaluate whether there is a statistical difference in diagnostic ability between 1.5-T and 3-T MRI.
MATERIALS AND METHODS. This retrospective study included 114 patients who underwent knee MRI (46 on 1.5 T and 68 on 3 T) and arthroscopy at our institution. Two ra-diologists evaluated orthogonal views and ACL views on 1.5-T and 3-T MRI in variable com-binations. They diagnosed ACL views as normal, entire ligament tear, anteromedial bundle tear, or posterolateral bundle tear. The surgeon then confirmed tears in the anteromedial or posterolateral bundle of the ACL arthroscopically if a selective-bundle tear did exist. The arthroscopically confirmed diagnoses were used as the reference standard. The values were statistically analyzed.
RESULTS. Sixty-seven percent of patients showed an ACL tear on arthroscopy, and 33% had a selective bundle tear; of these, 75% were anteromedial bundle tears and 25% were pos-terolateral bundle tears. On 1.5-T MRI, specificities of each view and combined views were the same (80%). The sensitivities and accuracies of the combined views were higher than the individual views; differences between individual views ranged from 4% to 15%. Reader 1 saw statistically significant differences between the oblique coronal and combined views. Al-though the performances of reader 2 showed similar results, the p values exceeded the critical value of statistical significance (0.063). On 3-T MRI, differences in specificities between the orthogonal and combined views and between the orthogonal and oblique coronal views were statistically significant (p, 0.016 and 0.008 for readers 1 and 2, respectively). There were no significant differences in the diagnostic performance of 1.5-T and 3-T MRI.
CONCLUSION. The oblique coronal view and the combination of the orthogonal view and both additional ACL views provide better diagnostic information with an improvement in specificity on 3-T MRI compared with orthogonal views alone in the diagnosis of selec-tive-bundle tears. Although diagnostic performance was not improved with the addition of the oblique views over orthogonal views on 1.5-T imaging, diagnostic performance was im-proved on 3-T MRI. Accuracies for individual imaging planes were not significantly different when comparing 1.5-T and 3-T MRI.
Park et al.MRI of Anterior Cruciate Ligament
Musculoskeletal ImagingOriginal Research
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
58.1
21.2
47.6
0 on
08/
21/1
4 fr
om I
P ad
dres
s 15
8.12
1.24
7.60
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

W200 AJR:203, August 2014
Park et al.
A
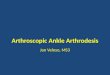
Fig. 1—Normal anterior cruciate ligament (ACL).A, Coronal T2-weighted image shows technique for obtaining oblique sagittal series. Lines indicate 3-mm-thick sections in plane parallel to medial border of lateral femoral condyle.B, Oblique sagittal ACL image shows normal ACL.C and D, Orthogonal sagittal images show poor delineation of ACL.E, Sagittal T2-weighted image shows technique for obtaining oblique coronal series. Lines indicate 3-mm-thick sections in plane parallel to intercondylar roof.F, Oblique coronal ACL image shows normal ACL.G and H, Orthogonal coronal images show poor delineation of ACL.
CB
D FE
G H
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
58.1
21.2
47.6
0 on
08/
21/1
4 fr
om I
P ad
dres
s 15
8.12
1.24
7.60
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

AJR:203, August 2014 W201
MRI of Anterior Cruciate Ligament
or posterolateral bundle of the injured ACL using standard MRI sequences and imaging planes. They also reported that the advan-tages of 3-T over 1.5-T MRI are questionable in correct diagnosis of selective bundle ACL tears. Steckel et al. [3] reported that particu-lar bundle tears can be diagnosed through 3-T MRI, but their results were based on a cadaver study. Compared with 1.5-T MRI, 3-T MRI introduces the possibility of a dou-bled signal-to-noise ratio (SNR) and the pos-sibility of decreased scanning times without reduction in quality. An increased SNR can improve contrast or spatial resolution [8]. Craig et al. [9] reported that 3-T MRI showed increased SNR, increased resolu-tion, and improved image quality of both the anatomy and pathology in the knee joint. Several studies have shown that additional oblique MRI is helpful for diagnosing ACL tears and single-bundle reconstructed ACL graft injury [10, 11]. Ng et al. [12] reported that the addition of oblique axial imaging improves diagnostic accuracy for detecting individual bundle tears. However, studies using oblique sagittal and oblique coronal imaging were not performed. We wanted to find the diagnostic efficacy of using addi-tional oblique sagittal and oblique coronal views of 1.5-T and 3-T knee MRI in selec-tive-bundle ACL injury. The purpose of this study was to evaluate the diagnostic useful-ness of combining oblique sagittal and oblique coronal imaging (ACL views) with traditional orthogonal views for evaluating selective-bundle ACL tears and whether there is a significant difference between the diagnostic ability of 1.5-T and 3-T MRI.
Materials and MethodsCase Selection
This study was approved by our hospital insti-tutional review board, and the requirement for in-formed consent was waived because of the retro-spective study design. We retrospectively evaluated 114 consecutive patients who were suspected to have cruciate ligament injury or internal derange-ment of the knee and underwent knee arthrosco-py between August 2011 and December 2012. All patients underwent MRI with additional oblique sagittal and coronal imaging. One experienced or-thopedic surgeon performed all arthroscopic diag-noses and treatments. The orthopedic surgeon had fellowship training in knee joint procedures and had 30 years of experience. Patients with an in-terval longer than 60 days were excluded from the study. No additional medical therapy, such as non-steroidal antiinflammatory drugs or physical thera-py, was provided during this interval. Once the two fellowship-trained musculoskeletal radiologists with 13 and 9 years of experience had finished their blind radiologic diagnosis of the MR images, the surgeon and radiologists correlated the MRI find-ings and surgical results.
Arthroscopic DiagnosisArthroscopic findings are the current reference
standard for diagnosis. Anteromedial and antero-lateral portals were used with probing and distrac-tion of the ligament to evaluate integrity. An in-tact ACL had taut and visibly intact fibers from the tibial to the femoral attachment [12]. When one bundle lost continuity and tautness but the other remained intact, it was considered a selective bun-dle tear. The surgeon tried to designate tears in the anteromedial or posterolateral bundle of the ACL. Both bundle tears referred to complete dis-
continuation of both anteromedial and posterolat-eral bundles. The Lachman, anterior drawer, and pivot shift tests were also conducted presurgically and interpreted as positive or negative [7].
MRI ParametersMRI examinations were performed using the
same protocol on a 1.5-T scanner (Intera, Phil-ips Healthcare) and a 3-T scanner (Achieva, Phil-ips Healthcare) (46 cases at 1.5 T and 68 cases at 3 T) using an eight-channel knee coil. The gradient strengths of each MRI were 66 mT/m and 80 mT/m with a slew rate of 80 mT/m/ms and 200 mT/m/ms, respectively. The sequences and imaging parameters are summarized in Tables 1 and 2. The ACL oblique sagittal image was obtained in the plane parallel to the medial border of the lateral femoral condyle on the orthogonal coronal image. The ACL oblique cor-onal view was obtained in the plane parallel to the course of the femoral intercondylar roof on the basis of the conventional sagittal image [10] (Fig. 1).
Image AnalysisThe MR images were interpreted independent-
ly by two musculoskeletal radiologists who were unaware of radiologic reports or clinical history. First, the readers evaluated orthogonal views only of all patients on 1.5-T and 3-T MRI. During ses-sions spaced 2 weeks apart, they evaluated the oblique sagittal ACL view and the oblique coro-nal ACL view on 1.5-T and 3-T MRI and evaluat-ed all MRI sequences containing both additional ACL views on 1.5-T and 3-T MR in another ses-sion with an interval of 2 weeks. Each reader in-terpreted the individual oblique images and com-bined images, which were separated from each other. The ACL tear group and the healthy group were interpreted in a randomly selected order. If
TABLE 1: Imaging Parameters for 3-T MRI Sequences
Imaging ParameterCoronal Proton
Density FSECoronal Fat-Saturated
T2-Weighted FSESagittal Fat-Saturated
Proton Density FSESagittal T2-Weighted
FSEACL View Sagittal T2-Weighted FSE
ACL View Coronal T2-Weighted FSE
TR (ms) 3000–3500 5500–6500 4000–4500 3500–5000 2500–3000 2500–3000
TE (ms) 30–40 70–90 30–40 50–100 50–80 50–80
Flip angle (°) 90 90 90 90 90 90
Matrix size 450 × 300 450 × 300 300 × 230 430 × 300 500 × 300 500 × 300
FOV (cm) 16 16 16 16 15 15
Slice thickness (mm) 3 3 3 3 3 3
Interslice gap (mm) 0.3 0.3 0.3 0.3 0.3 0.3
Bandwidth (kHz) 460 240 240 290 400 400
Echo-train length 15 16 14 17 16 16
Signal average 1 1 1 1 1 1
Scanning time (min:s) 2:22 3:23 2:47 2:00 2:04 1:55
Note—FSE = fast spin-echo, ACL = anterior cruciate ligament.
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
58.1
21.2
47.6
0 on
08/
21/1
4 fr
om I
P ad
dres
s 15
8.12
1.24
7.60
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

W202 AJR:203, August 2014
Park et al.
the ACL was visibly intact and depicted as a con-tinuous linear band of normal hypointense signal intensity, the MRI was diagnosed as normal. If complete disruption of all of its fibers with an as-sociated wavy or lax contour of the ligament was seen or if the ACL was completely replaced by an edematous mass, the diagnosis was rupture of both bundles [4]. If fiber disruption or focal swell-ing could be clearly detected in the anteromedi-al or posterolateral bundle, the patient was diag-nosed with isolated bundle tear [7].
Statistical AnalysisInterobserver agreement of diagnostic perfor-
mance of the selective bundle injury was analyzed using kappa statistics. The kappa value was inter-preted as follows: poor (< 0.1), slight (0.1 to < 0.2),
fair (≥ 0.2 to < 0.4), moderate (≥ 0.4 to < 0.6), sub-stantial (≥ 0.6 to < 0.8), and almost perfect (≥ 0.8 to 1) [13]. Diagnostic performance of the orthogo-nal, oblique sagittal, oblique coronal, and orthogo-nal images with additional ACL views were evalu-ated using the specificity, sensitivity, and accuracy for diagnosing selective ACL bundle injury. The arthroscopically confirmed diagnoses were used as the reference standard. The values were statisti-cally analyzed using the McNemar test to evaluate in differences of diagnostic performance among variable MRI sequence combinations. We used a Pearson chi-square test to evaluate differences of diagnostic performance between 1.5-T and 3-T MRI. Statistical analyses were performed using PASW software, version 18.0 (IBM). A p value ≤ 0.05 was considered statistically significant.
ResultsThe sample included ninety-two (81%)
men and 22 (19%) women (mean age [± SD], 33.8 ± 13.3 years; range, 14–69 years). Ar-throscopies were performed soon after MRI, with a mean interval of 24 days (range, 1–60 days). Among 114 patients, arthroscopy re-vealed an ACL tear in 76 patients (67%). Among those, 52 patients (68%) showed both-bundle tears (Fig. 2). In 24 (32%) of those cas-es, there was a selective-bundle tear: postero-lateral bundle tears in six cases (25%) (Fig. 3) and anteromedial bundle tears in 18 cases (75%) (Fig. 4). In two patients, both-bundle tears were diagnosed on orthogonal and com-bined views (one on 1.5-T and the other on 3-T MRI), but the ACL was intact on arthrosco-
TABLE 2: Imaging Parameters for 1.5-T MRI Sequences
Imaging ParameterCoronal Proton
Density FSECoronal Fat-Saturated
T2-Weighted FSESagittal Fat-Saturated
Proton Density FSESagittal T2-Weighted
FSEACL View Sagittal T2-Weighted FSE
ACL View Coronal T2-Weighted FSE
TR (ms) 1500–2000 2000–2500 4000–4500 2000–3500 2500–3000 2500–3000
TE (ms) 30–40 70–90 30–40 40–100 50–80 50–80
Flip angle (°) 90 90 90 90 90 90
Matrix size 320 × 300 320 × 300 300 × 250 320 × 300 500 × 300 500 × 300
FOV (cm) 16 16 16 16 15 15
Slice thickness (mm) 3 3 3 3 3 3
Interslice gap (mm) 0.3 0.3 0.3 0.3 0.3 0.3
Bandwidth (kHz) 170 130 200 300 260 240
Echo-train length 12 14 12 15 14 14
Signal average 2 2 2 2 3 3
Scanning time (min:s) 2:05 3:10 2:15 2:33 2:13 1:55
Note—FSE = fast spin-echo, ACL = anterior cruciate ligament.
A
Fig. 2—Both-bundle tear in 23-year-old man with knee pain after playing soccer.A, Orthogonal sagittal T2-weighted image (TR/TE, 3800/100) from 3-T MRI shows tears in both bundles (arrow).B, Oblique sagittal T2-weighted MR image (TR/TE, 2700/75) of anterior cruciate ligament (ACL) also indicates complete tear of both bundles (arrow).C, Arthroscopic image reveals complete rupture and discontinuity of ACL from femoral attachment site (arrow). Some hemorrhage is also seen. This ACL tear appeared to involve both bundles on orthogonal and oblique sagittal images.
CB
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
58.1
21.2
47.6
0 on
08/
21/1
4 fr
om I
P ad
dres
s 15
8.12
1.24
7.60
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

AJR:203, August 2014 W203
MRI of Anterior Cruciate Ligament
py (Fig. 5). Three patients who were confirmed as having both-bundle tears arthroscopical-ly were diagnosed as having selective-bundle tears on orthogonal views and combined views. Eight patients who were confirmed as having selective-bundle tears arthroscopically (five cases of anteromedial bundle tears and three cases of posterolateral bundle tears) were diag-nosed as having both-bundle tears on orthogo-nal views and combined views. Interobserver agreement of the diagnostic performance be-tween readers ranged from 0.766 to 0.882, which suggests substantial or almost perfect agreement (Table 3). On 1.5-T MRI, specifici-ties of each view and of combined views were the same (80%), but the sensitivities and accu-racies of the combined views were higher than other single views (83% vs 68–78%) (Table 4). Statistically significant differences were seen between the oblique coronal view and the com-bined view by reader 1. Although the same p value for reader 2 was low (0.063), the value exceeded the critical value for statistical signif-icance (0.05) (Table 5). On 3-T MRI, marked differences in the specificity of the orthogonal view and additional views were observed (67% vs 82–96%) (Table 6). Among these, differ-ences between the orthogonal view and com-bined view (67% vs 92–96%) and between the orthogonal view and oblique coronal view (67% vs 92–96%) were statistically significant
(p < 0.05) (Table 5). Although differences in the sensitivity and accuracy existed among variable views, statistically significant differ-ences were not observed. There was no signifi-cant difference in the diagnostic performance of 1.5-T MRI and 3-T MRI (Table 5).
DiscussionThe ACL originates from the posterior por-
tion of the medial aspect of the lateral femoral condyle, courses obliquely in an anteromedial direction, and inserts at the central and medial parts of the intercondylar area of the tibia [1].
TABLE 3: Interobserver Reliability According to Kappa Values
Magnet Strength
Kappa Values
Orthogonal Views Oblique Sagittal View Oblique Coronal Views All
1.5 T 0.882 0.848 0.766 0.832
p < 0.001 < 0.001 < 0.001 < 0.001
3 T 0.853 0.839 0.857 0.836
p < 0.001 < 0.001 < 0.001 < 0.001
Note—Kappa value was interpreted as follows: poor (< 0.1), slight (0.1 to < 0.2), fair (≥ 0.2 to < 0.4), moderate (≥ 0.4 to < 0.6), substantial (≥ 0.6 to < 0.8), and almost perfect (≥ 0.8 to 1).
TABLE 4: Specificity, Sensitivity, and Accuracy of Orthogonal, Oblique Sagittal, and Oblique Coronal Views in Diagnosing Selective-Bundle Tear on 1.5-T MRI
Imaging View
Specificity (%) Sensitivity (%) Accuracy (%)
Reader 1 Reader 2 Reader 1 Reader 2 Reader 1 Reader 2
Orthogonal 80.0 (4/5) 80.0 (4/5) 70.7 (29/41) 70.7 (29/41) 71.7 (33/46) 71.7 (33/46)
Oblique sagittal 80.0 (4/5) 80.0 (4/5) 78.0 (32/41) 75.6 (31/41) 78.3 (36/46) 76.1 (35/46)
Oblique coronal 80.0 (4/5) 80.0 (4/5) 68.3 (28/41) 70.7 (29/41) 69.6 (32/46) 71.7 (33/46)
All 80.0 (4/5) 80.0 (4/5) 82.9 (34/41) 82.9 (34/41) 82.6 (38/46) 82.6 (38/46)
Note—Data in parentheses are number/total.
TABLE 5: Specificity, Sensitivity, and Accuracy in Diagnosing Selective Bundle Tear
Magnet Strength Match
Specificity Sensitivity Accuracy
Reader 1 Reader 2 Reader 1 Reader 2 Reader 1 Reader 2
1.5 T A vs B 1.000 1.000 0.453 1.000 0.453 0.500
A vs C 1.000 1.000 1.000 1.000 1.000 1.000
A vs all 1.000 1.000 0.125 0.687 0.125 0.125
B vs C 1.000 1.000 0.344 0.754 0.344 0.754
B vs all 1.000 1.000 0.625 0.375 0.625 0.375
C vs all 1.000 1.000 0.031 0.063 0.031 0.063
3 T A vs B 0.125 0.125 0.687 0.500 0.109 0.180
A vs C 0.016 0.008 1.000 1.000 0.118 0.118
A vs all 0.016 0.008 0.219 0.687 0.003 0.013
B vs C 0.250 0.125 0.687 0.687 1.000 0.754
B vs all 0.250 0.125 0.500 1.000 0.063 0.125
C vs all 1.000 1.000 0.219 0.250 0.219 0.250
1.5 T vs 3 T A 1.000 1.000 0.202 1.000 0.461 0.461
B 1.000 1.000 0.107 1.000 0.659 1.000
C 1.000 1.000 0.237 1.000 0.423 0.612
All 1.000 1.000 0.542 0.542 0.569 0.444
Note—Data are p values according to the McNemar test for specificity, sensitivity, and accuracy among the orthogonal views (A), oblique sagittal views (B), and oblique coronal views (C) in diagnosing selective bundle tear and according to the Pearson chi-square test for specificity, sensitivity, and accuracy between 1.5 T and 3 T.
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
58.1
21.2
47.6
0 on
08/
21/1
4 fr
om I
P ad
dres
s 15
8.12
1.24
7.60
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

W204 AJR:203, August 2014
Park et al.
The ACL is composed of two distinct bundles, the anteromedial and posterolateral bundles, and functions as a stabilizer of the knee with the posterior cruciate ligament [14]. It is diffi-cult to see the whole course of the ligament on an orthogonal MRI view because of the com-plex anatomy of the area [15]. The anterome-dial and posterolateral bundles are parallel to each other when the knee is fully extended, whereas with the knee flexed to 90°, both bun-dles cross each other. Because the two bundles are at an angle to one another, some difference of degrees between bundles can be seen from MRI in the neutral position [16]. In recent stud-ies, 6–10% of ACL tears were arthroscopical-ly proven to be selective-bundle tears [7, 17]. Our results suggested that 32% of tears were selective-bundle tears and that there were three times as many anteromedial bundle tears as there were posterolateral tears confirmed ar-throscopically. Ochi et al. [17] and Dejour et al. [18] have also reported that the anteromedial bundle tear is more frequent than tears in the posterolateral bundle. Previous studies have re-ported that using the oblique coronal view can be useful in the visualization of the whole ana-
tomic course of the ACL [15, 19]. In our study, statistically significant differences in diagnos-tic performance were seen between the orthog-onal view and the oblique coronal view and between the orthogonal view and combined views (p < 0.05) on 3-T MRI. Both readers showed higher specificity on the oblique coro-nal view and combined images than on the or-thogonal view. On 1.5-T MRI, the combined view showed higher sensitivity and accuracy than the oblique coronal view for reader 1. Al-though the values were not statistically signifi-cant, the same p values for reader 2 were very
low (0.063), which approach the critical value of 0.05. Tables 4 and 6 show that the reason the combined view is better than the oblique coro-nal view is that the oblique coronal view alone has lower sensitivity and accuracy in diagnos-ing ACL tears on both 1.5-T and 3-T MRI, al-though the difference is more apparent on 1.5-T MRI. Moon et al. [11] reported that an oblique coronal image can show transverse width of the ACL easily in the study of graft injury and reported that the oblique coronal angle is less subject to volume averaging. There were no sig-nificant differences in diagnostic performance
A
Fig. 3—Posterolateral bundle tear in 15-year-old boy with knee pain after playing soccer.A, Orthogonal sagittal T2-weighted image (TR/TE, 3600/100) from 3-T MRI shows complete rupture of both bundles (arrow).B, Oblique sagittal T2-weighted MR image (TR/TE, 2700/75) of anterior cruciate ligament (ACL) also indicates complete tear of both bundles (arrow).C, Oblique coronal T2-weighted MR image (TR/TE, 2700/75) reveals intact anteromedial bundle of ACL (arrows).D, Arthroscopic image shows selective tear of posterolateral bundle (long arrow). Anteromedial bundle is intact (short arrow). Arrowhead indicates posterior cruciate ligament. This ACL tear appeared to involve both bundles on orthogonal and oblique sagittal images, but oblique coronal image shows that anteromedial bundle is intact.
C
B
D
TABLE 6: Specificity, Sensitivity, and Accuracy of Orthogonal, Oblique Sagittal, and Oblique Coronal Views in Diagnosing Selective Bundle Tear on 3T MRI
View
Specificity (%) Sensitivity (%) Accuracy (%)
Reader 1 Reader 2 Reader 1 Reader 2 Reader 1 Reader 2
Orthogonal 66.7 (18/27) 66.7 (18/27) 80.5 (33/41) 85.4 (35/41) 75.0 (51/68) 77.9 (53/68)
Oblique sagittal 81.5 (22/27) 81.5 (22/27) 85.4 (35/41) 87.8 (36/41) 83.8 (57/68) 85.3 (58/68)
Oblique coronal 92.6 (25/27) 96.3 (26/27) 80.5 (33/41) 82.9 (34/41) 85.3 (58/68) 88.2 (60/68)
All 92.6 (25/27) 96.3 (26/27) 90.2 (37/41) 90.2 (37/41) 91.2 (62/68) 92.6 (63/68)
Note—Data in parentheses are number/total.
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
58.1
21.2
47.6
0 on
08/
21/1
4 fr
om I
P ad
dres
s 15
8.12
1.24
7.60
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

AJR:203, August 2014 W205
MRI of Anterior Cruciate Ligament
A
Fig. 4—Anteromedial bundle tear in 52-year-old woman with knee pain after playing tennis.A, Orthogonal sagittal T2-weighted image (TR/TE, 2000/40) from 1.5-T MRI reveals both bundle tears (arrow).B, Oblique sagittal T2-weighted MR image (TR/TE, 2700/80) of anterior cruciate ligament (ACL) indicates anteromedial bundle disruption (long arrow) but intact posterolateral bundle (short arrow).C, Arthroscopic image shows selective tear of anteromedial bundle (long arrow). Posterolateral bundle is intact (short arrow). This ACL tear appeared to involve both bundles on orthogonal image, but oblique sagittal image shows that posterolateral bundle is intact.
CB
A
Fig. 5—Posterolateral bundle tear in 34-year-old man with knee pain after running.A, Orthogonal sagittal T2-weighted image (TR/TE, 3800/100) on 3-T MRI shows tears in both bundles (arrow).B, Oblique sagittal T2-weighted MR image (TR/TE, 2700/75) of anterior cruciate ligament (ACL) also reveals complete tear of both bundles (arrow).C, Oblique coronal T2-weighted MR image (TR/TE, 2600/60) indicates disruption of both bundles (arrow).D, Arthroscopic image shows intact anteromedial bundle (arrow).E, Arthroscopic image obtained after retracting intact anteromedial bundle with probe reveals typical “lateral empty wall” sign (arrow), which means disruption of posterolateral bundle. This ACL tear appeared to involve both bundles on orthogonal image and both oblique images, but anteromedial bundle was intact.
CB
D E
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
58.1
21.2
47.6
0 on
08/
21/1
4 fr
om I
P ad
dres
s 15
8.12
1.24
7.60
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

W206 AJR:203, August 2014
Park et al.
between 1.5-T and 3-T MRI, although some au-thors have reported that 3-T MRI provides im-proved diagnostic performance given its high-er SNR and resultant improved image quality [20]. Adriaensen et al. [21] and Kaya et al. [22] reported that the double-bundle anatomy of the ACL is seen in 94% of patients on 3-T MRI but only 38% of patients on 1.5-T MRI. We think that these differences do not influence diagnostic performance because those studies were based on normal ACLs. Though statisti-cally significant differences in specificity were seen between the orthogonal view and oblique coronal view and between the orthogonal view and combined views, overall diagnostic perfor-mance of the additional views in the evaluation of selective bundle tear were disappointing, especially on 1.5-T MRI. Although the sensi-tivities and accuracies of the combined views increased about 10% compared with orthogo-nal views, the specificities did not increase on 1.5-T MRI. On the other hand, the specificities, sensitivities, and accuracies of combined views increased from 5% to 30% compared with or-thogonal views (Tables 4 and 6). The mean in-creased scanning time did not exceed 4 min-utes, which accounts for less than 20% of total procedure time (not total scanning time). Be-cause most medical centers perform at least one of the additional views in the imaging of the knee joint, superimposed scanning time would be much less. Therefore, because we could prevent patients from going to surgery unnecessarily, it might be helpful to add both oblique views in the evaluation of the ACL of the knee joint even if a small number of cases could be diagnosed more accurately (selective- or both-bundle tears). Had we been able to cor-rectly diagnose eight cases of false double-bun-dle tears that were proven to be single-bundle tears, the surgeon might have acquired more useful information to establish a treatment plan from the radiology department.
Several limitations of our study should be mentioned. First, this study had a selec-tion bias because we included only those pa-tients who underwent arthroscopy. Second, our study included only a small number of pa-tients with selective-bundle tears. Posterolat-eral bundle tears occurred in only six of the examined cases. Third, the readers’ aware-ness of whether the sequence was an addition-al image or orthogonal image may have re-sulted in bias during evaluation of the ACL. A completely blinded study was impossible be-cause of the different anatomic structures, al-though sequence parameters were not visible. Fourth, the surgeon might have been aware
of the MRI findings, which could have influ-enced the arthroscopic diagnosis.
In conclusion, we could find 24 patients (32%) with selective-bundle tears from 76 ACL tears; 75% were anteromedial bun-dle tears and 25% were posterolateral tears. The oblique coronal view and the combina-tion of orthogonal views and both additional ACL views provided better diagnostic perfor-mance with improvement in specificity on 3-T MRI than orthogonal views alone in the diag-nosis of selective-bundle tears. Furthermore, although each individual view does not add a lot of benefit, the combination of the views might be helpful for accurate diagnosis of the ACL tears. Although 3-T MRI showed higher specificity, sensitivity, and accuracy when the orthogonal view was combined with an addi-tional view and showed higher specificity on the oblique coronal view, we could not find a statistically significant difference in diagnos-tic capability between 1.5-T and 3-T MRI.
References 1. Duc SR, Zanetti M, Kramer J, Kach KP, Zol-
likofer CL, Wentz KU. Magnetic resonance imag-
ing of anterior cruciate ligament tears: evaluation
of standard orthogonal and tailored paracoronal
images. Acta Radiol 2005; 46:729–733
2. Zelle BA, Vidal AF, Brucker PU, Fu FH. Double-
bundle reconstruction of the anterior cruciate lig-
ament: anatomic and biomechanical rationale. J
Am Acad Orthop Surg 2007; 15:87–96
3. Steckel H, Vadala G, Davis D, Musahl V, Fu FH.
3-T MR imaging of partial ACL tears: a cadaver
study. Knee Surg Sports Traumatol Arthrosc
2007; 15:1066–1071
4. Van Dyck P, Vanhoenacker FM, Gielen JL, et al.
Three tesla magnetic resonance imaging of the
anterior cruciate ligament of the knee: can we dif-
ferentiate complete from partial tears? Skeletal
Radiol 2011; 40:701–707
5. Hara K, Kubo T, Suginoshita T, Shimizu C, Hira-
sawa Y. Reconstruction of the anterior cruciate
ligament using a double bundle. Arthroscopy
2000; 16:860–864
6. Petersen W, Zantop T. Partial rupture of the ante-
rior cruciate ligament. Arthroscopy 2006;
22:1143–1145
7. Van Dyck P, Smet ED, Veryser J, et al. Partial tear
of the anterior cruciate ligament of the knee: in-
jury patterns on MR imaging. Knee Surg Sports
Traumatol Arthrosc 2012; 20:256–261
8. Phalke VV, Gujar S, Quint DJ. Comparison of 3.0
T versus 1.5 T MR: imaging of the spine. Neuro-
imaging Clin N Am 2006; 16:241–248
9. Craig JG, Go L, Blechinger J, et al. Three-tesla
imaging of the knee: initial experience. Skeletal
Radiol 2005; 34:453–461
10. Kwon JW, Yoon YC, Kim YN, Ahn JH, Choe BK.
Which oblique plane is more helpful in diagnos-
ing an anterior cruciate ligament tear? Clin Radiol
2009; 64:291–297
11. Moon SG, Hong SH, Choi JY, et al. Grading ante-
rior cruciate ligament graft injury after ligament
reconstruction surgery: diagnostic efficacy of
oblique coronal MR imaging of the knee. Korean
J Radiol 2008; 9:155–161
12. Ng AW, Griffith JF, Hung EH, Law KY, Yung PS.
MRI diagnosis of ACL bundle tears: value of
oblique axial imaging. Skeletal Radiol 2013;
42:209–217
13. Viera AJ, Garrett JM. Understanding interobserv-
er agreement: the kappa statistic. Fam Med 2005;
37:360–363
14. Dienst M, Burks RT, Greis PE. Anatomy and bio-
mechanics of the anterior cruciate ligament. Or-
thop Clin North Am 2002; 33:605–620
15. Staeubli HU, Adam O, Becker W, Gurgkart R.
Anterior cruciate ligament and intercondylar
notch in the coronal oblique plane: anatomy com-
plemented by magnetic resonance imaging in cru-
ciate ligament–intact knees. Arthroscopy 1999;
15:349–359
16. Hensler D, Van Eck CF, Fu FH, Irrgang JJ. Ana-
tomic anterior cruciate ligament reconstruction
utilizing the double-bundle technique. J Orthop
Sports Phys Ther 2012; 42:184–195
17. Ochi M, Adachi N, Deie M, Kanaya A. Anterior
cruciate ligament augmentation procedure with a
1-incision technique: anteromedial bundle or pos-
terolateral bundle reconstruction. Arthroscopy
2006; 22:463. E1–463.E5
18. Dejour D, Ntagiopoulos PG, Saggin PR, Panisset
JC. The diagnostic value of clinical tests, mag-
netic resonance imaging and instrumented laxity
in the differentiation of complete versus partial
anterior cruciate ligament tears. Arthroscopy
2013; 29:491–499
19. Katahira K, Yamashita Y, Takahashi M, et al. MR
imaging of the anterior cruciate ligament: values
of thin slice direct oblique coronal technique. Ra-
diat Med 2001; 19:1–7
20. Tung GA, Davis LM, Wiggins ME, Fadale PD.
Tears of the anterior cruciate ligament: primary
and secondary signs at MR imaging. Radiology
1993; 188:661–667
21. Adriaensen ME, Hogan B, Al-Bulushi HI, Kava-
nach EC. Double-bundle depiction of the anterior
cruciate ligament at 3 Tesla. Skeletal Radiol 2012;
41:831–834
22. Kaya A, Karadag D, Guclu B, Ucar F, Benli IT.
Evaluation of the two bundles of the anterior cru-
ciate ligament with 1.5 tesla magnetic resonance
imaging. Acta Orthop Traumatol Turc 2010;
44:54–62
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
58.1
21.2
47.6
0 on
08/
21/1
4 fr
om I
P ad
dres
s 15
8.12
1.24
7.60
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved