Embed Size (px)
Citation preview

Comparative Immunogenicity of Enhanced Influenza Vaccines in Older Adults in Hong Kong: A Randomized
Controlled Trial
Ben Cowling
School of Public HealthThe University of Hong Kong
2 Feb 2020

Influenza disease burden in older adults
In Hong Kong, persons ≥ 65y contribute:
• 57% of all influenza-associated hospitalisations
• 96% of all influenza-associated excess P&I deaths
• This despite high influenza vaccination coverage
Wu P et al. 2017 Sci Rep

Waning in vaccine effectiveness within a year
Vaccine effectiveness against H3N2 declines by time since vaccination, I-MOVE study, 2011/12 – 2014/15, persons ≥60y
Kissling et al. 2016 Eurosurveillance3

Vaccination and influenza activity in the US, 2010-18
Shaded blue areas show influenza epidemics, more recent years are plotted in darker shades.
4

Vaccination and influenza activity in Hong Kong, 2010-18
5
Shaded red areas show influenza epidemics, more recent years are plotted in darker shades.

Potent Influenza Vaccination strategies in Older adults –randomized immunogenicity Trial
Inclusion criteria - 62-82 years of age, living in the community in Hong Kong, no cognitive impairment or contraindication to vaccination
Blood draw at days 0, 30 and 182 each round for serology
• 10% of participants provided additional blood for CMI at days 0, 7, 30, 182, and additional blood for serology at day 91 and 273
Cowling et al. 2019 CID

Results – Baseline characteristics (n=1,861)
4 • CID 2019:XX (XX XXXX) • Cowling et!al
Sample Size Justification
For the present comparison of responses to 4 different vaccines in Year 1, we sought to detect small to moderate but meaningful relative differences in immunogenicity. A! sample size of 200 participants per group would permit 80% power to detect in-creases of !14% in the proportion of enhanced vaccine recipi-ents with !4-fold rises in titer, and GMT ratios of 1.4 or higher in the enhanced vaccine groups, compared to a SD vaccine. Overall, we aimed to enroll 2200 participants into our study, anticipating a 10% dropout rate per year and a final sample size of at least 146 participants in each group through to the fourth year of the planned trial (see the Supplementary Appendix).
RESULTS
We screened 3283 older adults, of whom 2695 were eligible and 2039 agreed to participate. We obtained signed informed con-sent from 2008 persons and were able to randomize and vacci-nate 1861 participants from 7 October 2017 through 12 January 2018, of whom 1826 provided Day 30 postvaccination serum samples (Figure 1). About 10% of participants were asked to give additional blood; 168 contributed PBMCs for analyses of cell-mediated immunity.
Participants were balanced by age, sex, underlying medical conditions, and prior vaccination history between the 4 study groups, with no statistically signi"cant di#erences in these key
variables overall or among those contributing to the primary antibody "ndings reported here (Table 1). $e most common underlying conditions were hypertension, osteoarthritis, and diabetes. Most participants (66%) had received an in%uenza vac-cination in the preceding year (2016–2017), and only 22% had not received any in%uenza vaccination in the preceding 5!years. All prior in%uenza vaccinations were with an SD vaccine. We selected 200 participants from each group for a serologic anal-ysis, and the characteristics of this subset were representative of the entire cohort (Table 2). Pre- and post-vaccination GMTs and corresponding MFRs are described in Table 3 for each vac-cine group, and Figure 2 presents comparisons of the MFRs be-tween the enhanced vaccine groups and the SD group. Table 4 shows the proportions of participants achieving speci"c titer thresholds a&er vaccination.
$ere were no statistically signi"cant baseline di#erences between the groups in prevaccination GMTs for each of the antigens tested, except that the baseline GMTs to the B/Victoria antigen were statistically signi"cantly lower in the SD group (Table 3). As shown in Table 3, among SD QIV re-cipients, the HAI GMT to A(H1N1) increased from 17 to 69. MF59-adjuvanted and HD recipients achieved a signi"cantly higher postvaccination GMT to A(H1N1) than SD recipi-ents; recombinant-HA recipients did not. Nonetheless, MFRs for A(H1N1) were statistically signi"cantly higher for all 3
Table 1. Baseline Characteristics of the 1861 Participants, by Vaccination Group!
Characteristics All Participants
Standard-dose quadrivalent vaccine,
n!=!508
MF59-adjuvanted trivalent vaccine,
n!=!508High-dose trivalent vaccine, n!=!510
Recombinant-HA quadrivalent
vaccine, n!=!335
n (%) n (%) n (%) n (%)
Age, years 65–70 269 (53%) 248 (49%) 258 (51%) 171 (51%) 71–76 130 (26%) 149 (29%) 143 (28%) 82 (24%) 77–82 109 (21%) 111 (22%) 109 (21%) 82 (24%)Female sex 301 (59%) 308 (61%) 327 (64%) 195 (58%)Underlying medical conditions Hypertension 230 (45%) 262 (52%) 239 (47%) 161 (48%) Osteoarthritis 110 (22%) 102 (20%) 109 (21%) 70 (21%) Diabetes 98 (19%) 104 (20%) 88 (17%) 61 (18%) Heart diseases 52 (10%) 47 (9%) 52 (10%) 29 (9%) Cancer 46 (9%) 43 (8%) 40 (8%) 22 (7%) Othersa 209 (41%) 221 (44%) 226 (44%) 141 (42%)Received influenza vaccination in 2016–2017 season 328 (65%) 332 (65%) 351 (69%) 226 (67%)Number of times received influenza vaccination in the preceding 5!yearsb
0 126 (25%) 104 (20%) 111 (22%) 71 (21%) 1–2 113 (22%) 120 (24%) 112 (22%) 68 (20%) 3–4 54 (11%) 45 (9%) 61 (12%) 38 (11%) 5–6 195 (38%) 201 (40%) 212 (42%) 144 (43%)
Abbreviation: HA, hemagglutinin.aOther underlying conditions included: stroke, chronic lung disease, kidney disease, liver disease, depression or anxiety disorder, neurologic disorder, autoimmune disease, disease of the digestive system, hypothyroidism, dermatological disease, etc.bThere were 6 possible influenza vaccines, including the 5 Northern hemisphere influenza vaccines from 2012–2013 through 2016–2017 plus the Southern hemisphere 2015 vaccine, which was available in Hong Kong for a special vaccination campaign [20]. The Southern hemisphere formulation is not usually available in Hong Kong.
Dow
nlo
aded fro
m h
ttps://a
cadem
ic.o
up.c
om
/cid
/advance-a
rticle
-abstra
ct/d
oi/1
0.1
093/c
id/c
iz1034/5
673516 b
y U
niv
ers
ity o
f Hong K
ong, B
enja
min
Cow
ling o
n 1
2 D
ecem
ber 2
019
Cowling et al. 2019 CID

Mean fold rises from pre- to post-vaccination
Values significantly different from SD QIV MFR are shown in bold and underlined
* Note that MF59-adj and HD vaccines were trivalent and did not include B/Yamagata lineage virus
† Cell-grown antigen, MDCK 4 passages, SIAT 1-2 passages
Motivation Methods Results Comments
Mean fold rises from pre- to post-vaccination
Assay Strain Mean fold rise (post/pre)SD Adj HD Rec
HAI A/Michigan/45/2015 (H1N1) 4.32 5.74 6.90 5.86HAI A/Hong Kong/4801/2014 (H3N2) egg 3.81 4.56 6.07 4.44MN A/Hong Kong/4801/2014 (H3N2) cell† 2.60 2.89 3.42 4.47HAI B/Brisbane/60/2008 4.53 3.48 6.03 3.66HAI B/Phuket/3073/2013⇤ 3.76 1.54 1.66 3.25
Values signi�cantly di�erent from SD QIV MFR are shown in bold and underlined
⇤ Note that MF59-adj and HD vaccines were trivalent and did not includeB/Yamagata lineage virus† Cell-grown antigen, MDCK 4 passages, SIAT 1-2 passages
Ben Cowling Slide 19
Cowling et al. 2019 CID

Day 30 GMT ratio enhanced versus standard dose
Cowling et al. 2019 CID
Serology test done on 800 randomly selected participants, 200 in each vaccination arm

Does prior vaccination history modify response to 2017/18 vaccination?
Issues with reduced antibody responses after repeat vaccination
Pre
Tite
r
Not affected
Post Pre
Tite
r
Blunted not reduced
Post Pre
Tite
r
Blunted and reduced
Post
- Previously vaccinated- Previously not vaccinated

Vaccination history* Vaccination armSD (n=200) Adj (n=200) HD (n=200) Rec (n=200)
Self-reported influenza vaccination history each year
2016/17 NH 136 (68.0) 130 (65.0) 139 (69.5) 137 (68.5)2015/16 NH 126 (63.0) 117 (58.5) 133 (66.5) 121 (60.5)2015 SH 8 (4.0) 1 (0.5) 5 (2.5) 6 (3.0)2014/15 NH 105 (52.5) 98 (49.0) 118 (59.0) 102 (51.0)2013/14 NH 90 (45.0) 93 (46.5) 101 (50.5) 96 (48.0)2012/13 NH 81 (40.5) 85 (42.5) 96 (48.0) 98 (49.0)No influenza vaccination in the previous 5 years
45 (22.5) 45 (22.5) 46 (23.0) 46 (23.0)
Year of most recent prior vaccination
2016/17 136 (68.0) 130 (65.0) 139 (69.5) 137 (68.5)2015/16 11 (5.5) 10 (5.0) 9 (4.5) 3 (1.5)2015 (SH vaccine) 0 (0) 0 (0) 0 (0) 0 (0)2014/15 1 (0.5) 1 (0.5) 2 (1.0) 1 (0.5)2013/14 0 (0) 1 (0.5) 0 (0) 1 (0.5)2012/13 1 (0.5) 0 (0) 0 (0) 5 (2.5)Not in last 5 years 45 (22.5) 45 (22.5) 46 (23.0) 46 (23.0)* n=30 unknown vaccination history
Vaccination history (n=800)

A/Michigan/45/2015 (H1N1)
● ●●
●
●
● ●●
<1010204080
160320640
≥ 1280
Geo
met
ric m
ean
HAI
tite
r
D0 D30 D0 D30 D0 D30 D0 D30SD Adj HD Rec
(A)
● Received 2016/17 vaccinationDid not receive 2016/17 vaccination
A/Hong Kong/4801/2014 (H3N2) egg−propagated antigen
● ● ●●
●●
●●
<1010204080
160320640
≥ 1280
Geo
met
ric m
ean
HAI
tite
r
D0 D30 D0 D30 D0 D30 D0 D30SD Adj HD Rec
(B) A/Hong Kong/4801/2014 (H3N2) cell−propagated antigen
●●
●
●●
● ●
●
<1010204080
160320640
≥ 1280
Geo
met
ric m
ean
MN
tite
r
D0 D30 D0 D30 D0 D30 D0 D30SD Adj HD Rec
(C)
B/Brisbane/60/2008 (Victoria lineage)
●
●●
●
●●
●
●
<1010204080
160320640
≥ 1280
Geo
met
ric m
ean
HAI
tite
r
D0 D30 D0 D30 D0 D30 D0 D30SD Adj HD Rec
(D) B/Phuket/3073/2013 (Yamagata lineage)
● ● ● ●
●
● ●
●
<1010204080
160320640
≥ 1280
Geo
met
ric m
ean
HAI
tite
r
D0 D30 D0 D30 D0 D30 D0 D30SD Adj HD Rec
(E)
14
A/Michigan/45/2015 (H1N1)
● ●●
●
●
● ●●
<1010204080
160320640
≥ 1280
Geo
met
ric m
ean
HAI
tite
r
D0 D30 D0 D30 D0 D30 D0 D30SD Adj HD Rec
(A)
● Received 2016/17 vaccinationDid not receive 2016/17 vaccination
A/Hong Kong/4801/2014 (H3N2) egg−propagated antigen
● ● ●●
●●
●●
<1010204080
160320640
≥ 1280
Geo
met
ric m
ean
HAI
tite
r
D0 D30 D0 D30 D0 D30 D0 D30SD Adj HD Rec
(B) A/Hong Kong/4801/2014 (H3N2) cell−propagated antigen
●●
●
●●
● ●
●
<1010204080
160320640
≥ 1280
Geo
met
ric m
ean
MN
tite
r
D0 D30 D0 D30 D0 D30 D0 D30SD Adj HD Rec
(C)
B/Brisbane/60/2008 (Victoria lineage)
●
●●
●
●●
●
●
<1010204080
160320640
≥ 1280
Geo
met
ric m
ean
HAI
tite
r
D0 D30 D0 D30 D0 D30 D0 D30SD Adj HD Rec
(D) B/Phuket/3073/2013 (Yamagata lineage)
● ● ● ●
●
● ●
●
<1010204080
160320640
≥ 1280
Geo
met
ric m
ean
HAI
tite
r
D0 D30 D0 D30 D0 D30 D0 D30SD Adj HD Rec
(E)
A/Michigan/45/2015 (H1N1)
● ●●
●
●
● ●●
<1010204080
160320640
≥ 1280
Geo
met
ric m
ean
HAI
tite
r
D0 D30 D0 D30 D0 D30 D0 D30SD Adj HD Rec
(A)
● Received 2016/17 vaccinationDid not receive 2016/17 vaccination
A/Hong Kong/4801/2014 (H3N2) egg−propagated antigen
● ● ●●
●●
●●
<1010204080
160320640
≥ 1280
Geo
met
ric m
ean
HAI
tite
r
D0 D30 D0 D30 D0 D30 D0 D30SD Adj HD Rec
(B) A/Hong Kong/4801/2014 (H3N2) cell−propagated antigen
●●
●
●●
● ●
●
<1010204080
160320640
≥ 1280
Geo
met
ric m
ean
MN
tite
r
D0 D30 D0 D30 D0 D30 D0 D30SD Adj HD Rec
(C)
B/Brisbane/60/2008 (Victoria lineage)
●
●●
●
●●
●
●
<1010204080
160320640
≥ 1280
Geo
met
ric m
ean
HAI
tite
r
D0 D30 D0 D30 D0 D30 D0 D30SD Adj HD Rec
(D) B/Phuket/3073/2013 (Yamagata lineage)
● ● ● ●
●
● ●
●
<1010204080
160320640
≥ 1280
Geo
met
ric m
ean
HAI
tite
r
D0 D30 D0 D30 D0 D30 D0 D30SD Adj HD Rec
(E)

<10
10−20
20−40
40−80
80−160
160−320
320−640
640−1280
≥ 1280
<10 10−2020−40
40−8080−160
160−320320−640
640−1280
≥ 1280
HAI titer pre−vaccination
HAI
tite
r pos
t−va
ccin
atio
n
0.0%
5.0%
10.0%
15.0%
20.0%Proportion
SD, 2016/17 unvaccinated
<10
10−20
20−40
40−80
80−160
160−320
320−640
640−1280
≥ 1280
<10 10−2020−40
40−8080−160
160−320320−640
640−1280
≥ 1280
HAI titer pre−vaccination
HAI
tite
r pos
t−va
ccin
atio
n0.0%
5.0%
10.0%
15.0%
20.0%Proportion
Adj, 2016/17 unvaccinated
<10
10−20
20−40
40−80
80−160
160−320
320−640
640−1280
≥ 1280
<10 10−2020−40
40−8080−160
160−320320−640
640−1280
≥ 1280
HAI titer pre−vaccination
HAI
tite
r pos
t−va
ccin
atio
n
0.0%
5.0%
10.0%
15.0%
20.0%Proportion
HD, 2016/17 unvaccinated
<10
10−20
20−40
40−80
80−160
160−320
320−640
640−1280
≥ 1280
<10 10−2020−40
40−8080−160
160−320320−640
640−1280
≥ 1280
HAI titer pre−vaccination
HAI
tite
r pos
t−va
ccin
atio
n
0.0%
5.0%
10.0%
15.0%
20.0%Proportion
Rec, 2016/17 unvaccinated
<10
10−20
20−40
40−80
80−160
160−320
320−640
640−1280
≥ 1280
<10 10−2020−40
40−8080−160
160−320320−640
640−1280
≥ 1280
HAI titer pre−vaccination
HAI
tite
r pos
t−va
ccin
atio
n
0.0%
5.0%
10.0%
15.0%
20.0%Proportion
SD, 2016/17 vaccinated
<10
10−20
20−40
40−80
80−160
160−320
320−640
640−1280
≥ 1280
<10 10−2020−40
40−8080−160
160−320320−640
640−1280
≥ 1280
HAI titer pre−vaccination
HAI
tite
r pos
t−va
ccin
atio
n
0.0%
5.0%
10.0%
15.0%
20.0%Proportion
Adj, 2016/17 vaccinated
<10
10−20
20−40
40−80
80−160
160−320
320−640
640−1280
≥ 1280
<10 10−2020−40
40−8080−160
160−320320−640
640−1280
≥ 1280
HAI titer pre−vaccination
HAI
tite
r pos
t−va
ccin
atio
n
0.0%
5.0%
10.0%
15.0%
20.0%Proportion
HD, 2016/17 vaccinated
<10
10−20
20−40
40−80
80−160
160−320
320−640
640−1280
≥ 1280
<10 10−2020−40
40−8080−160
160−320320−640
640−1280
≥ 1280
HAI titer pre−vaccination
HAI
tite
r pos
t−va
ccin
atio
n
0.0%
5.0%
10.0%
15.0%
20.0%Proportion
Rec, 2016/17 vaccinated
Distribution of pre- vs. post-vaccination titer by 2016/17 vaccination status – A(H3N2) egg (Similar for other strains)
15

Summary of findings
• Improved anti-HA antibody responses to each of the enhanced vaccines
• Compared to the other two enhanced vaccines, FluBlok provided similar anti-HA responses to egg-adapted H3N2 vaccine strain, and superior responses by MN to the cell-like H3N2 vaccine strain
• We found reduced immune responses in participants with prior vaccinations• Weaker boosts but similar post-vaccination titers for H1N1• Weaker boosts and lower post-vaccination titers for H3N2-egg• Weaker boosts and lower post-vaccination titers for H3N2-cell for FluBlok

PIVOT full design (4 years)
Motivation Methods Results Comments
PIVOT full design (4 years)
Standard dose QIV(n=600)
MF59-adjuvanted TIV(n=600)
High-dose TIV(n=600)
Recombinant HA QIV(n=400)
Year 1 Year 2 Year 3 Year 4
Ben Cowling Slide 29
22

Update on 2019-nCoVWork presented here was done in collaboration with China CDC

Data as reported by 1 February 2020*
Novel Coronavirus(2019-nCoV) Situation Report - 12
SITUATION IN NUMBERS total and new cases in last 24 hours
Globally 11953 confirmed (2128 new) China 11821 confirmed (2102 new) 1795 severe (268 new) 259 deaths (46 new) Outside of China 132 confirmed (26 new) 23 countries (4 new) WHO RISK ASSESSMENT China Very High Regional Level High Global Level High
*The situation report includes information reported to WHO Geneva by 10 AM CET
Figure 1. Countries, territories or areas with reported confirmed cases of 2019-nCoV, 01 February 2020
HIGHLIGHTS
x The main driver of transmission, based on currently available data, is
symptomatic cases. WHO is aware of possible transmission of 2019-nCoV from infected people before they developed symptoms. Detailed exposure histories are being taken to better understand the pre-clinical phase of infection and how transmission may have occurred in these few instances. Asymptomatic infection may be rare, and transmission from an asymptomatic person is very rare with other coronaviruses, as we have seen with Middle East Respiratory Syndrome coronavirus. Thus, transmission from asymptomatic cases is likely not a major driver of transmission. Persons who are symptomatic will spread the virus more readily through coughing and sneezing.
x In China, 60.5% of all cases since the start of the outbreak have been reported from Hubei Province (see further information under Technical Focus).
x Additional instances of human-to-human transmission outside China were reported (see further information under Technical Focus).

First 41 cases detected through PUE system
Articles
www.thelancet.com Published online January 24, 2020 https://doi.org/10.1016/S0140-6736(20)30183-5 3
(methylprednisolone 40–120 mg per day) was given as a combined regimen if severe community-acquired pneumonia was diagnosed by physicians at the designated hospital. Oxygen support (eg, nasal cannula and invasive mechanical ventilation) was administered to patients according to the severity of hypoxaemia. Repeated tests for 2019-nCoV were done in patients confirmed to have 2019-nCoV infection to show viral clearance before hospital discharge or discontinuation of isolation.
Data collectionWe reviewed clinical charts, nursing records, laboratory findings, and chest x-rays for all patients with laboratory-confirmed 2019-nCoV infection who were reported by the local health authority. The admission data of these patients was from Dec 16, 2019, to Jan 2, 2020. Epidemiological, clinical, laboratory, and radiological characteristics and treatment and outcomes data were obtained with standardised data collection forms (modified case record form for severe acute respira-tory infection clinical characterisation shared by the International Severe Acute Respiratory and Emerging Infection Consortium) from electronic medical records. Two researchers also independently reviewed the data collection forms to double check the data collected. To ascertain the epidemiological and symptom data, which were not available from electronic medical records, the researchers also directly communicated with patients or their families to ascertain epidemiological and symptom data.
Cytokine and chemokine measurementTo characterise the e!ect of coronavirus on the production of cytokines or chemokines in the acute phase of the illness, plasma cytokines and chemokines (IL1B, IL1RA, IL2, IL4, IL5, IL6, IL7, IL8 (also known as CXCL8), IL9, IL10, IL12p70, IL13, IL15, IL17A, Eotaxin (also known as CCL11), basic FGF2, GCSF (CSF3), GMCSF (CSF2), IFN", IP10 (CXCL10), MCP1 (CCL2), MIP1A (CCL3), MIP1B (CCL4), PDGFB, RANTES (CCL5), TNF#, and VEGFA were measured using Human Cytokine Standard 27-Plex Assays panel and the Bio-Plex 200 system (Bio-Rad, Hercules, CA, USA) for all patients according to the manufacturer’s instructions. The plasma samples from four healthy adults were used as controls for cross-comparison. The median time from being transferred to a designated hospital to the blood sample collection was 4 days (IQR 2–5).
Detection of coronavirus in plasmaEach 80 µL plasma sample from the patients and contacts was added into 240 µL of Trizol LS (10296028; Thermo Fisher Scientific, Carlsbad, CA, USA) in the Biosafety Level 3 laboratory. Total RNA was extracted by Direct-zol RNA Miniprep kit (R2050; Zymo research, Irvine, CA, USA) according to the manufacturer’s instructions and
50 µL elution was obtained for each sample. 5 µL RNA was used for real-time RT-PCR, which targeted the NP gene using AgPath-ID One-Step RT-PCR Reagent (AM1005; Thermo Fisher Scientific). The final reaction mix concentration of the primers was 500 nM and probe was 200 nM. Real-time RT-PCR was per formed using the following conditions: 50°C for 15 min and 95°C for 3 min, 50 cycles of amplification at 95°C for 10 s and 60°C for 45 s. Since we did not perform tests for detecting infectious virus in blood, we avoided the term viraemia and used RNAaemia instead. RNAaemia was defined as a positive result for real-time RT-PCR in the plasma sample.
DefinitionsAcute respiratory distress syndrome (ARDS) and shock were defined according to the interim guidance of WHO
For more on the International Severe Acute Respiratory and Emerging Infection Consortium see https://isaric.tghn.org/
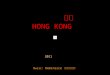
Figure !: Date of illness onset and age distribution of patients with laboratory-confirmed 2019-nCoV infection(A) Number of hospital admissions by age group. (B) Distribution of symptom onset date for laboratory-confirmed cases. The Wuhan local health authority issued an epidemiological alert on Dec 30, 2019, and closed the Huanan seafood market 2 days later.
0<18 18–24 25–49 50–64 !65
5
10
15
20
Num
ber o
f cas
es
Age (years)
AGeneral wardIntensive care unit
Dec 1, 2019
Dec 10, 2019
Dec 11, 2019
Dec 12, 2019
Dec 13, 2019
Dec 14, 2019
Dec 15, 2019
Dec 16, 2019
Dec 17, 2
019
Dec 18, 2019
Dec 19, 2019
Dec 20, 2019
Dec 21, 2019
Dec 22, 2019
Dec 23, 2019
Dec 24, 2019
Dec 25, 2019
Dec 26, 2019
Dec 27, 2
019
Dec 28, 2019
Dec 29, 2019
Dec 30, 2019
Dec 31, 2019
Jan 1, 2020
Jan 2, 20200
2
4
6
8
Num
ber o
f cas
es
Onset date
B
NoYes
Huanan seafood market exposure
Epidemiological alert
Market closed
Huang et al. 2020 Lancet

Huanan Seafood Wholesale Market

Wu et al. 2020 Eurosurveillance
Start reporting confirmed 2019−nCoV cases
First exported case confirmed
National task force visited Wuhan
31 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21Dec Jan
0
80
160
240
320
400
480
Date
Cum
ulat
ive n
o. c
ases
Pneumonia of unknown etiologyConfirmed 2019−nCoV infections in mainland ChinaExported 2019−nCoV infections

4 www.eurosurveillance.org
DiscussionIn this article, we describe a preliminary assessment of the outbreak of infections with the newly identified 2019-nCoV. This assessment is based on the cases of infection reported over time by health authorities in Wuhan and then at the national level, as well as the media in China and other countries. One of the most urgent priorities is to determine the degree of human-to-human transmissibility of the novel pathogen, and accordingly, this is where information is most urgently needed. We outline two possible scenarios in the!Table!and find that the early evidence was most consistent with limited human-to-human transmissibil-ity, however more recent data seem to be increasingly more compatible with scenario 2 in which sustained human-to-human transmission has been occurring. Determining the exposure profile among the recently confirmed cases would directly contribute to this
assessment. Additional information on approaches to case identification and laboratory testing protocols in Wuhan and in other cities in China would also be informative. A separate priority is to identify the ani-mal reservoir of this novel pathogen and any intermedi-ary hosts, including potential supply chains of wild or game meat.
It is challenging to judge severity from the informa-tion available to date. We estimated the risk of death among hospitalised cases of around 14% (Figure 2). For both SARS-CoV and MERS-CoV infections, the risk of severe disease increases substantially with age and with the presence of underlying conditions [23-25]. One other caveat with estimating severity is that there can be long delays between hospitalisation and death for infections that are ultimately fatal. For SARS in Hong Kong, the average time from illness to death for fatal
T!"#$Evidence on transmission dynamics of human infections with 2019-nCoV, as at 22 January 2020
Observation Date Interpretation Supports Scenario 1?a Supports Scenario 2?b
By 20 January, 198 laboratory-confirmed cases, 3 fatal, 25 recovered [28]
20 Jan 2020
Fatality risk among hospitalised cases is 11%c Yes Yes
No infections among the more than 700 people under medical surveillance, including HCWs [28]
20 Jan 2020
Very low human-to-human transmissibility Yes
No (Note: assuming adequate contact tracing
and surveillance)Only one likely human-to-human cluster among the first 41 cases [18]
20 Jan 2020
Very low human-to-human transmissibility (R0!of 0.02) Yes No (Note: assuming
adequate contact tracing)
Only approximately 70% of the first 41 cases had exposure to Southern China Seafood Wholesale Market [16]
15 Jan 2020
Low human-to-human transmissibility (R0!of 0.3) Yes
No (Note: possible selection bias towards
identifying cases linked to that market)
New cases with a travel history to Wuhan before onset were confirmed in other cities in China [29]
20 Jan 2020
Indicative of many mild to moderate infections (not
requiring hospitalisation) in Wuhan
Yes Yes
Four exported cases to other countries, all with relatively mild illness [30,31]
12–20 Jan
2020
Indicative of many mild to moderate infections not
necessitating hospitalisation or outpatient medical care in
Wuhan
Yes Yes
Four exported cases, at least three of whom had no contact with Southern China Seafood Wholesale Market [30,31]
12–20 Jan
2020
At least some limited human-to-human transmission
(unclear!R0)Yes Yes
Two family clusters in Guangdong, with family members who did not visit Wuhan but were infected after the other family member(s) returning from Wuhan were confirmed with the infection [29]
20 Jan 2020
At least some limited human-to-human transmission
(unclear!R0)Yes Yes
15 HCWs confirmed with infection of 2019-nCoV (not clear whether infections were from one case or multiple cases) [20]
20 Jan 2020
Super-spreading event? Could still be consistent with limited human-to-human transmission
if an isolated incident (unclear!R0)
Yes Yes
Exported cases identified in Taiwan and the United States with illness onset dates on 11 and 19 January [32,33]
22 Jan 2020
Could be because of surveillance bias, but is more consistent with an increase in
incidence of infections over time
No (Note: possible selection bias
because of enhanced surveillance towards
identifying more recent cases)
Yes
HCWs: healthcare workers; nCoV: novel coronavirus; MHC: Municipal Health Commission.a!Most infections are zoonotic with limited human-to-human transmission (R0 < 1).b!Initial zoonotic spillover with efficient human-to-human transmission (R0 > 1).c!Estimated as (fatal cases) / (fatal cases + recovered cases).
Wu et al. 2020 Eurosurveillance

4 travel-related cases by 17 Jan 2020 implies many infections in Wuhan
17 January 2020 Imperial College London
Page 2 of 4
infection risk than residents. Accounting for either factor correctly requires additional data but would increase our estimate of the total number of cases.
2. We estimate the potential number of symptomatic cases with disease severity of a level requiring hospitalisation (both the cases detected in Thailand and Japan were moderately severe). Our estimates do not include cases with mild or no symptoms.
3. The incubation period of 2019-nCov is not known and has been approximated with the estimates obtained for MERS-CoV and SARS [8,9].
4. We assume that international travel is independent of the risk of exposure to 2019n-CoV or of infection status. If zoonotic exposure was biased towards wealthier people, travel frequency may be correlated with exposure. Also, some travel might be causally linked to infection status (to seek healthcare overseas) or the infection status of contacts in Wuhan (this may apply to the case detected in Japan) [10]. Accounting for either association would increase the probability of a case travelling and therefore reduce our estimates of the total number of cases. .
Sensitivity analysis
We explore the sensitivity of estimates of total cases to our assumptions about: i) the duration of the detection window (exploring a lower value of 8 days); ii) the catchment population size of Wuhan airport (assuming it might be 11 million, the population of Wuhan city [12], rather than 19 million, the population of the entire metropolitan area [1]); and iii) true exportations reported internationally (2, 3 and 4 cases). Table 1 summarises the baseline assumptions and alternative scenarios explored. We note that the currently reported number of cases (44) is substantially lower than the lower bound of our most conservative scenario (190 cases, Scenario 3).
Table 1: Estimated case numbers based on the baseline assumptions and alternative scenarios explored.
Baseline Scenario 1 Scenario 2 Scenario 3 Scenario 4 Exported number of confirmed cases*
3 3 3 2 4
Daily international passengers travelling out of Wuhan International airport1
3,301 3,301 3,301 3,301 3,301
Effective catchment population of Wuhan airport
19 million 11 million 19 million 19 million 19 million
Detection window (days) 10 days 10 days 8 days 10 days 10 days Estimated Total number of cases (95% CI)
1,723 (427 ± 4,471)
996 (246 ± 2,586)
2,155 (535 ± 5,590)
1149 (190 ± 3,549)
2,298 (712 ± 5,341)
*reported number of confirmed cases detected internationally. 1calculated from the 3 month totals reported by [11] corrected for the travel surge during Chinese New Year (see Summary).
Conclusions
It is likely that the Wuhan outbreak of a novel coronavirus has caused substantially more cases of moderate or severe respiratory illness than currently reported. The estimates presented here suggest surveillance should be expanded to include all hospitalised cases of pneumonia or severe respiratory disease in the Wuhan area and other well-connected Chinese cities. This analysis does not directly address transmission routes, but past experience with SARS and MERS-CoV outbreaks of similar scale suggests currently self-sustaining human-to-human transmission should not be ruled out.
Imperial College London

n engl j med nejm.org 4
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
cifically, the latter part of the curve does not indicate a decrease in the number of incident cases but is due to delayed case ascertainment at the cutoff date. Care should be taken in inter-preting the speed of growth in cases in January, given an increase in the availability and use of testing kits as time has progressed. The major-ity of the earliest cases included reported expo-sure to the Huanan Seafood Wholesale Market, but there was an exponential increase in the number of nonlinked cases beginning in late December.
The median age of the patients was 59 years (range, 15 to 89), and 240 of the 425 patients (56%) were male. There were no cases in chil-dren below 15 years of age. We examined char-acteristics of cases in three time periods: the
first period was for patients with illness onset before January 1, which was the date the Huan-an Seafood Wholesale Market was closed; the second period was for those with onset between January 1 and January 11, which was the date when RT-PCR reagents were provided to Wuhan; and the third period was those with illness onset on or after January 12 (Table 1). The patients with earlier onset were slightly younger, more likely to be male, and much more likely to report exposure to the Huanan Seafood Wholesale Market. The proportion of cases in health care workers gradually increased across the three periods (Table 1).
We examined data on exposures among 10 confirmed cases, and we estimated the mean incubation period to be 5.2 days (95% confidence
Figure!1.!Onset!of!Illness!among!the!First!425!Confirmed!Cases!of!Novel!Coronavirus!(2019-nCoV)–Infected!Pneumonia!(NCIP)!!in!Wuhan,!China.
The decline in incidence after January 8 is likely to be due to delays in diagnosis and laboratory confirmation. China CDC denotes Chi-nese Center for Disease Control and Prevention, NHC National Health Commission of the People’s Republic of China, PCR polymerase chain reaction, WHC Wuhan Health Commission, and WHO World Health Organization.
No.
!of!C
ases
45
50
35
40
30
25
15
10
20
5
027 30 3 6 9 12 15 18 21 24 27 30 2 5 8 11 14 17 20
Nov.
2019
Dec.
2020
Jan.
A novel coronavirus was officiallyannounced as the causative
pathogen of the outbreakby China CDC
Huanan Seafood WholesaleMarket closed
Outbreak announced by WHC;NHC and China CDC involvedin investigation and response
Case-finding activated
Pneumonia cases linkedto the Huanan Seafood
Wholesale Market
China CDC publicly shared the gene sequenceof the novel coronavirus; completed PCRdiagnostic reagent development and testing
PCR diagnostic reagents provided to Wuhan
First confirmed case from Wuhanreported outside China (in Thailand)
China CDC emergency response levelupgraded to Level 1 (the highest level);national technical protocols for 2019-nCoV released by NHC
NCIP incorporated as a notifiabledisease in the Infectious DiseaseLaw and Health and QuarantineLaw in China
Reagent probes and primersshared with the public by China CDC
Strict exit screening measures activatedin Wuhan, people with body temperature!37.3ºC were restricted from leaving
First confirmed case reported in anotherprovince in China (in a person whohad traveled from Wuhan); China CDCissued test reagent to all provincesin China
China CDC Level 2 emergencyresponse activated
Emergency monitoring, case investigation,close contact management, and market
investigation initiated, technical protocolsfor Wuhan released; NHC notified WHOand relevant countries and regions; gene
sequencing completed by China CDC
Outbreak!Period
Not linked to Huanan marketLinked to Huanan market
The New England Journal of Medicine Downloaded from nejm.org by Elizabeth Laurencot on January 31, 2020. For personal use only. No other uses without permission.
Copyright © 2020 Massachusetts Medical Society. All rights reserved.
Transmission dynamics in Wuhan
• Analysis of first 425 cases
• Based on early exponential growth in non-linked cases (up to 3 January) we estimated doubling time of 7.4 days, and R0 of 2.2
Li et al. 2020 NEJM

n engl j med nejm.org 5
Early Tr ansmission Dynamics of NCIP
interval [CI], 4.1 to 7.0); the 95th percentile of the distribution was 12.5 days (95% CI, 9.2 to 18) (Fig. 2A). We obtained information on 5 clusters of cases, shown in Figure 3. On the basis of the dates of illness onset of 6 pairs of cases in these clusters, we estimated that the serial interval distribution had a mean (±SD) of 7.5±3.4 days (95% CI, 5.3 to 19) (Fig. 2B).
In the epidemic curve up to January 4, 2020, the epidemic growth rate was 0.10 per day (95% CI, 0.050 to 0.16) and the doubling time was 7.4 days (95% CI, 4.2 to 14). Using the serial interval distribution above, we estimated that R0 was 2.2 (95% CI, 1.4 to 3.9).
The duration from illness onset to first medical visit for 45 patients with illness onset before January 1 was estimated to have a mean of 5.8 days (95% CI, 4.3 to 7.5), which was similar to that for 207 patients with illness onset between January 1 and January 11, with a mean of 4.6 days (95% CI, 4.1 to 5.1) (Fig. 2C). The mean duration from onset to hospital admission was estimated to be 12.5 days (95% CI, 10.3 to 14.8) among 44 cases with illness onset before January 1, which was longer than that among 189 patients with illness onset between January
1 and 11 (mean, 9.1 days; 95% CI, 8.6 to 9.7) (Fig. 2D). We did not plot these distributions for patients with onset on or after January 12, be-cause those with recent onset and longer dura-tions to presentation would not yet have been detected.
Discussion
Here we provide an initial assessment of the transmission dynamics and epidemiologic char-acteristics of NCIP. Although the majority of the earliest cases were linked to the Huanan Sea-food Wholesale Market and the patients could have been infected through zoonotic or environ-mental exposures, it is now clear that human-to-human transmission has been occurring and that the epidemic has been gradually growing in recent weeks. Our findings provide important parameters for further analyses, including evalu-ations of the impact of control measures and predictions of the future spread of infection.
We estimated an R0 of approximately 2.2, meaning that on average each patient has been spreading infection to 2.2 other people. In gen-eral, an epidemic will increase as long as R0 is
CharacteristicBefore!January!1!
(N!=!47)January!1!–January!11!
(N!=!248)January!12!–January!22!
(N!=!130)
Median age (range) — yr 56 (26–82) 60 (21–89) 61 (15–89)
Age group — no./total no. (%)
<15 yr 0/47 0/248 0/130
15–44 yr 12/47 (26) 39/248 (16) 33/130 (25)
45–64 yr 24/47 (51) 106/248 (43) 49/130 (38)
!65 yr 11/47 (23) 103/248 (42) 48/130 (37)
Male sex — no./total no. (%) 31/47 (66) 147/248 (59) 62/130 (48)
Exposure history — no./total no. (%)
Wet market exposure 30/47 (64) 32/196 (16) 5/81 (6)
Huanan Seafood Wholesale Market 26/47 (55) 19/196 (10) 5/81 (6)
Other wet market but not Huanan Seafood Wholesale Market
4/47 (9) 13/196 (7) 0/81
Contact with another person with respiratory symptoms
14/47 (30) 30/196 (15) 21/83 (25)
No exposure to either market or person with respiratory symptoms
12/47 (26) 141/196 (72) 59/81 (73)
Health care worker — no./total no. (%) 0/47 7/248 (3) 8/122 (7)
* Reduced denominators indicate missing data. Percentages may not total 100 because of rounding.
Table!1.!Characteristics!of!Patients!with!Novel!Coronavirus–Infected!Pneumonia!in!Wuhan!as!of!January!22,!2020.*
The New England Journal of Medicine Downloaded from nejm.org by Elizabeth Laurencot on January 31, 2020. For personal use only. No other uses without permission.
Copyright © 2020 Massachusetts Medical Society. All rights reserved.
Li et al. 2020 NEJM

n engl j med nejm.org 6
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
greater than 1, and control measures aim to re-duce the reproductive number to less than 1. The R0 of SARS was estimated to be around 3,12 and SARS outbreaks were successfully controlled by isolation of patients and careful infection con-trol.13 In the case of NCIP, challenges to control include the apparent presence of many mild in-fections14 and limited resources for isolation of cases and quarantine of their close contacts. Our estimate of R0 was limited to the period up to January 4 because increases in awareness of the outbreak and greater availability and use of tests in more recent weeks will have increased the proportions of infections ascertained. It is pos-sible that subsequent control measures in Wu-han, and more recently elsewhere in the country as well as overseas, have reduced transmissibil-ity, but the detection of an increasing number of
cases in other domestic locations and around the world suggest that the epidemic has contin-ued to increase in size. Although the population quarantine of Wuhan and neighboring cities since January 23 should reduce the exportation of cases to the rest of the country and overseas, it is now a priority to determine whether local transmission at a similar intensity is occurring in other locations.
It is notable that few of the early cases oc-curred in children, and almost half the 425 cases were in adults 60 years of age or older, although our case definition specified severe enough ill-ness to require medical attention, which may vary according to the presence of coexisting condi-tions. Furthermore, children might be less likely to become infected or, if infected, may show milder symptoms, and either of these situations
Figure!2.!Key!Time-to-Event!Distributions.
The estimated incubation period distribution (i.e., the time from infection to illness onset) is shown in Panel A. The estimated serial interval distribution (i.e., the time from illness onset in successive cases in a transmission chain) is shown in Panel B. The estimated distributions of times from illness onset to first medical visit are shown in Panel C. The estimated distributions of times from illness onset to hospital admission are shown in Panel D.
A
0 7 14 210.00
0.05
0.10
0.25
0.20
0.15
Days!from!Infection!to!Symptom!Onset
B
0 7 14 210.00
0.05
0.10
0.20
0.15
Serial!Interval!(days)
0 3 6 9 120.00
0.05
0.10
0.15
0.20
0.25
Days!from!Illness!Onset!to!First!Medical!Visit
Onset before January 1Onset during January 1!11
C
0 10 20 300.00
0.05
0.10
0.15
Days!from!Illness!Onset!to!Hospitalization
Rela
tive!
Freq
uenc
y
Rela
tive!
Freq
uenc
y
Rela
tive!
Freq
uenc
y
Rela
tive!
Freq
uenc
y
D
Onset before January 1Onset during January 1!11
The New England Journal of Medicine Downloaded from nejm.org by Elizabeth Laurencot on January 31, 2020. For personal use only. No other uses without permission.
Copyright © 2020 Massachusetts Medical Society. All rights reserved.
• Incubation period mean 6 days, upper limit around 14 days
• Serial interval mean 7 days (but we now think it could be shorter)
• Mean delay from onset to hospitalization around 10 days (proxy for delay from onset to laboratory confirmation)
Li et al. 2020 NEJM

Severity
• Severity appears low initially, but increases as time progresses and cases begin to resolve
• Our early estimate of (fatality risk among hospitalised cases) = 14% based on:
(4 deaths)/(4 deaths + 25 recoveries)
Articles
www.thelancet.com Vol 382 July 13, 2013 141
younger individuals (p=0·0019; fi gure 1, table 2). For the 37 individuals who died, median time to death was 11 days (IQR 6–23). For the 65 individuals who recovered, median time to recovery was 18 days (14–29).
71 (66%) of 108 patients for whom detailed clinical information was available required mechanical ventil-ation, and 83 (75%) of 110 were admitted to ICU. We used multiple imputation to account for missing data for dates of ICU admission for one patient and for mechanical ventilation for 23 patients, and censored in 17 patients who were still in hospital as of May 28. We estimated that risks of ICU admission (p=0·08) and mechanical ventilation (p=0·0067) were higher for patients aged 60 years or older than for younger patients (fi gure 2, table 2). We recorded some evidence that disease progressed or resolved faster in patients younger than 60 years than in older individuals (fi gures 1, 2), but the small sample size meant that we did not have su! cient statistical power to warrant further investigation.
When we estimated the fatality risk of patients admitted to hospital on the basis of information available on di" erent dates, we noted that the estimated risk gradually decreased (fi gure 3). Uncertainty was initially substantial, but decreased with time (fi gure 3), because of the increasing number of cases and follow-up of individuals admitted to hospital.
We estimated that 23 (95% credible interval [CrI] seven to 58) symptomatic individuals infected with avian infl uenza A H7N9 sought medical care at ILI sentinels in Shanghai up to May 28, on the basis that two cases were identifi ed there by ILI surveillance. Additionally, we estimated that 40 (seven to 129) sought medical care at ILI sentinels in Nanjing on the basis that one case was identifi ed by ILI surveillance. With method 1, we estimated that about 0·75% of individuals with symptomatic 2009 infl uenza A H1N1 pandemic virus infection sought medical care. With the assump-tion that a similar proportion of symptomatic individuals infected with avian infl uenza A H7N9 would have
0 7 14 21 28 35 420
10
20
30
40
50
60
70
80
90
100A B C
Fata
lity r
isk (%
)
Time from hospital admission (days)0 7 14 21 28 35 42
Time from hospital admission (days)0 7 14 21 28 35 42
Time from hospital admission (days)Recovery Death Estimated fatality risk when all patients have died or recovered
Figure !: Fatality risk for patients with laboratory-confi rmed infection with avian infl uenza A H7N9 virus who were admitted to hospital(A) 123 patients of all ages, (B) 52 patients younger than 60 years, and (C) 71 patients aged at least 60 years. As of May 28, 2013, 17 patients were still in hospital; the solid lines will converge when these cases resolve.
0 7 14 21 28 35 420
10
20
30
40
50
60
70
80
90
100A B C
Risk
of a
dver
se o
utco
mes
(%)
Time from hospital admission (days)0 7 14 21 28 35 42
Time from hospital admission (days)0 7 14 21 28 35 42
Time from hospital admission (days)Admission to intensive care unit, mechanical ventilation, or death DeathMechanical ventilation or death
Figure ": Risks of adverse outcomes for patients with laboratory-confi rmed infection with avian infl uenza A H7N9 virus who were admitted to hospital(A) 123 patients of all ages, (B) 52 patients younger than 60 years, and (C) 71 patients aged at least 60 years.
Yu, Cowling et al. 2013 LancetWu et al. 2020 Eurosurveillance

Articles
www.thelancet.com Published online January 29, 2020 https://doi.org/10.1016/S0140-6736(20)30211-7 3
patients were clustered and had a history of exposure to the Huanan seafood market. Among them, there were 47 patients with long-term exposure history, most of whom were salesmen or market managers, and two patients with short-term exposure history, who were shoppers. None of the patients were medical sta!. Most patients were men, with a mean age of 55·5 years (SD 13·1; table 1). 50 (51%) patients had chronic diseases, including cardiovascular and cerebro vascular diseases, endocrine system disease, digestive system disease, respiratory system disease, malignant tumour, and nervous system disease (table 1).
On admission, most patients had fever or cough and a third of patients had shortness of breath (table 2). Other symptoms included muscle ache, headache,
confu sion, chest pain, and diarrhoea (table 2). Many patients presented with organ function damage, including 17 (17%) with ARDS, eight (8%) with acute respiratory injury, three (3%) with acute renal injury, four (4%) with septic shock, and one (1%) with venti-lator-associated pneumonia (table 2).
On admission, leucocytes were below the normal range in nine (9%) patients and above the normal range in 24 (24%) patients (table 3). 38 (38%) patients had neutrophils above the normal range. Lymphocytes and haemoglobin were below the normal range in many
Patients (n=99)
Age, years
Mean (SD) 55·5 (13·1)
Range 21–82
!39 10 (10%)
40–49 22 (22%)
50–59 30 (30%)
60–69 22 (22%)
"70 15 (15%)
Sex
Female 32 (32%)
Male 67 (68%)
Occupation
Agricultural worker 2 (2%)
Self-employed 63 (64%)
Employee 15 (15%)
Retired 19 (19%)
Exposure to Huanan seafood market* 49 (49%)
Long-term exposure history 47 (47%)
Short-term exposure history 2 (2%)
Chronic medical illness 50 (51%)
Cardiovascular and cerebrovascular diseases 40 (40%)
Digestive system disease 11 (11%)
Endocrine system disease† 13 (13%)
Malignant tumour 1 (1%)
Nervous system disease 1 (1%)
Respiratory system disease 1 (1%)
Admission to intensive care unit 23 (23%)
Clinical outcome
Remained in hospital 57 (58%)
Discharged 31 (31%)
Died 11 (11%)
Data are n (%) unless specified otherwise. 2019-nCoV=2019 novel coronavirus. *Long-term exposure is having worked at or lived in or around Huanan seafood market, whereas short-term exposure is having been to Huanan seafood market occasionally. †12 were diabetic.
Table !: Demographics, baseline characteristics, and clinical outcomes of 99 patients admitted to Wuhan Jinyintan Hospital (Jan 1–20, 2020) with 2019-nCoV pneumonia
Patients (n=99)
Signs and symptoms at admission
Fever 82 (83%)
Cough 81 (82%)
Shortness of breath 31 (31%)
Muscle ache 11 (11%)
Confusion 9 (9%)
Headache 8 (8%)
Sore throat 5 (5%)
Rhinorrhoea 4 (4%)
Chest pain 2 (2%)
Diarrhoea 2 (2%)
Nausea and vomiting 1 (1%)
More than one sign or symptom 89 (90%)
Fever, cough, and shortness of breath 15 (15%)
Comorbid conditions
Any 33 (33%)
ARDS 17 (17%)
Acute renal injury 3 (3%)
Acute respiratory injury 8 (8%)
Septic shock 4 (4%)
Ventilator-associated pneumonia 1 (1%)
Chest x-ray and CT findings
Unilateral pneumonia 25 (25%)
Bilateral pneumonia 74 (75%)
Multiple mottling and ground-glass opacity 14 (14%)
Treatment
Oxygen therapy 75 (76%)
Mechanical ventilation
Non-invasive (ie, face mask) 13 (13%)
Invasive 4 (4%)
CRRT 9 (9%)
ECMO 3 (3%)
Antibiotic treatment 70 (71%)
Antifungal treatment 15 (15%)
Antiviral treatment 75 (76%)
Glucocorticoids 19 (19%)
Intravenous immunoglobulin therapy 27 (27%)
2019-nCoV=2019 novel coronavirus. ARDS=acute respiratory distress syndrome. ECMO=extracorporeal membrane oxygenation. CRRT=continuous renal replacement therapy.
Table ": Clinical characteristics and treatment of patients with 2019-nCoV pneumonia
Articles
www.thelancet.com Published online January 29, 2020 https://doi.org/10.1016/S0140-6736(20)30211-7 3
patients were clustered and had a history of exposure to the Huanan seafood market. Among them, there were 47 patients with long-term exposure history, most of whom were salesmen or market managers, and two patients with short-term exposure history, who were shoppers. None of the patients were medical sta!. Most patients were men, with a mean age of 55·5 years (SD 13·1; table 1). 50 (51%) patients had chronic diseases, including cardiovascular and cerebro vascular diseases, endocrine system disease, digestive system disease, respiratory system disease, malignant tumour, and nervous system disease (table 1).
On admission, most patients had fever or cough and a third of patients had shortness of breath (table 2). Other symptoms included muscle ache, headache,
confu sion, chest pain, and diarrhoea (table 2). Many patients presented with organ function damage, including 17 (17%) with ARDS, eight (8%) with acute respiratory injury, three (3%) with acute renal injury, four (4%) with septic shock, and one (1%) with venti-lator-associated pneumonia (table 2).
On admission, leucocytes were below the normal range in nine (9%) patients and above the normal range in 24 (24%) patients (table 3). 38 (38%) patients had neutrophils above the normal range. Lymphocytes and haemoglobin were below the normal range in many
Patients (n=99)
Age, years
Mean (SD) 55·5 (13·1)
Range 21–82
!39 10 (10%)
40–49 22 (22%)
50–59 30 (30%)
60–69 22 (22%)
"70 15 (15%)
Sex
Female 32 (32%)
Male 67 (68%)
Occupation
Agricultural worker 2 (2%)
Self-employed 63 (64%)
Employee 15 (15%)
Retired 19 (19%)
Exposure to Huanan seafood market* 49 (49%)
Long-term exposure history 47 (47%)
Short-term exposure history 2 (2%)
Chronic medical illness 50 (51%)
Cardiovascular and cerebrovascular diseases 40 (40%)
Digestive system disease 11 (11%)
Endocrine system disease† 13 (13%)
Malignant tumour 1 (1%)
Nervous system disease 1 (1%)
Respiratory system disease 1 (1%)
Admission to intensive care unit 23 (23%)
Clinical outcome
Remained in hospital 57 (58%)
Discharged 31 (31%)
Died 11 (11%)
Data are n (%) unless specified otherwise. 2019-nCoV=2019 novel coronavirus. *Long-term exposure is having worked at or lived in or around Huanan seafood market, whereas short-term exposure is having been to Huanan seafood market occasionally. †12 were diabetic.
Table !: Demographics, baseline characteristics, and clinical outcomes of 99 patients admitted to Wuhan Jinyintan Hospital (Jan 1–20, 2020) with 2019-nCoV pneumonia
Patients (n=99)
Signs and symptoms at admission
Fever 82 (83%)
Cough 81 (82%)
Shortness of breath 31 (31%)
Muscle ache 11 (11%)
Confusion 9 (9%)
Headache 8 (8%)
Sore throat 5 (5%)
Rhinorrhoea 4 (4%)
Chest pain 2 (2%)
Diarrhoea 2 (2%)
Nausea and vomiting 1 (1%)
More than one sign or symptom 89 (90%)
Fever, cough, and shortness of breath 15 (15%)
Comorbid conditions
Any 33 (33%)
ARDS 17 (17%)
Acute renal injury 3 (3%)
Acute respiratory injury 8 (8%)
Septic shock 4 (4%)
Ventilator-associated pneumonia 1 (1%)
Chest x-ray and CT findings
Unilateral pneumonia 25 (25%)
Bilateral pneumonia 74 (75%)
Multiple mottling and ground-glass opacity 14 (14%)
Treatment
Oxygen therapy 75 (76%)
Mechanical ventilation
Non-invasive (ie, face mask) 13 (13%)
Invasive 4 (4%)
CRRT 9 (9%)
ECMO 3 (3%)
Antibiotic treatment 70 (71%)
Antifungal treatment 15 (15%)
Antiviral treatment 75 (76%)
Glucocorticoids 19 (19%)
Intravenous immunoglobulin therapy 27 (27%)
2019-nCoV=2019 novel coronavirus. ARDS=acute respiratory distress syndrome. ECMO=extracorporeal membrane oxygenation. CRRT=continuous renal replacement therapy.
Table ": Clinical characteristics and treatment of patients with 2019-nCoV pneumonia
Chen et al. 2020 Lancet
Articles
www.thelancet.com Published online January 29, 2020 https://doi.org/10.1016/S0140-6736(20)30211-7 1
Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive studyNanshan Chen*, Min Zhou*, Xuan Dong*, Jieming Qu*, Fengyun Gong, Yang Han, Yang Qiu, Jingli Wang, Ying Liu, Yuan Wei, Jia’an Xia, Ting Yu, Xinxin Zhang, Li Zhang
SummaryBackground In December, 2019, a pneumonia associated with the 2019 novel coronavirus (2019-nCoV) emerged in Wuhan, China. We aimed to further clarify the epidemiological and clinical characteristics of 2019-nCoV pneumonia.
Methods In this retrospective, single-centre study, we included all confirmed cases of 2019-nCoV in Wuhan Jinyintan Hospital from Jan 1 to Jan 20, 2020. Cases were confirmed by real-time RT-PCR and were analysed for epidemiological, demographic, clinical, and radiological features and laboratory data. Outcomes were followed up until Jan 25, 2020.
Findings Of the 99 patients with 2019-nCoV pneumonia, 49 (49%) had a history of exposure to the Huanan seafood market. The average age of the patients was 55·5 years (SD 13·1), including 67 men and 32 women. 2019-nCoV was detected in all patients by real-time RT-PCR. 50 (51%) patients had chronic diseases. Patients had clinical manifestations of fever (82 [83%] patients), cough (81 [82%] patients), shortness of breath (31 [31%] patients), muscle ache (11 [11%] patients), confusion (nine [9%] patients), headache (eight [8%] patients), sore throat (five [5%] patients), rhinorrhoea (four [4%] patients), chest pain (two [2%] patients), diarrhoea (two [2%] patients), and nausea and vomiting (one [1%] patient). According to imaging examination, 74 (75%) patients showed bilateral pneumonia, 14 (14%) patients showed multiple mottling and ground-glass opacity, and one (1%) patient had pneu mothorax. 17 (17%) patients developed acute respiratory distress syndrome and, among them, 11 (11%) patients worsened in a short period of time and died of multiple organ failure.
Interpretation The 2019-nCoV infection was of clustering onset, is more likely to a!ect older males with comorbidities, and can result in severe and even fatal respiratory diseases such as acute respiratory distress syndrome. In general, characteristics of patients who died were in line with the MuLBSTA score, an early warning model for predicting mortality in viral pneumonia. Further investigation is needed to explore the applicability of the MuLBSTA score in predicting the risk of mortality in 2019-nCoV infection.
Funding National Key R&D Program of China.
Copyright © 2020 Elsevier Ltd. All rights reserved.
IntroductionSince Dec 8, 2019, several cases of pneumonia of unknown aetiology have been reported in Wuhan, Hubei province, China.1–3 Most patients worked at or lived around the local Huanan seafood wholesale market, where live animals were also on sale. In the early stages of this pneumonia, severe acute respiratory infection symptoms occurred, with some patients rapidly dev-eloping acute respiratory distress syndrome (ARDS), acute respiratory failure, and other serious complications. On Jan 7, a novel coronavirus was identified by the Chinese Center for Disease Control and Prevention (CDC) from the throat swab sample of a patient, and was subsequently named 2019-nCoV by WHO.4
Coronaviruses can cause multiple system infections in various animals and mainly respiratory tract infections in humans, such as severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS).5–7 Most patients have mild symptoms and good prognosis.
So far, a few patients with 2019-nCoV have developed severe pneumonia, pulmonary oedema, ARDS, or mul-tiple organ failure and have died. All costs of 2019-nCoV treatment are covered by medical insurance in China.
At present, information regarding the epidemiology and clinical features of pneumonia caused by 2019-nCoV is scarce.1–3 In this study, we did a comprehensive exploration of the epidemiology and clinical features of 99 patients with confirmed 2019-nCoV pneumonia admitted to Jinyintan Hospital, Wuhan, which admitted the first patients with 2019-nCoV to be reported on.
MethodsStudy design and participantsFor this retrospective, single-centre study, we recruited patients from Jan 1 to Jan 20, 2020, at Jinyintan Hospital in Wuhan, China. Jinyintan Hospital is a hospital for adults (ie, aged !14 years) specialising in infectious diseases. Accord ing to the arrangements put in place by
Published Online January 29, 2020 https://doi.org/10.1016/ S0140-6736(20)30211-7
*Contributed equally.
Tuberculosis and Respiratory Department (Prof N Chen MD, X Dong PhD, Y Wei MD, J Xia MD, T Yu MD, Prof L Zhang MD), Infection Disease Department (F Gong MD, J Wang MD), Science and Education Department (Y Han PhD), and The Office of Drug Clinical Trial Institution (Y Liu MD), Wuhan Jinyintan Hospital, Wuhan, China; Department of Respiratory and Critical Care Medicine, Ruijin Hospital (Prof M Zhou MD, Prof J Qu MD), Institute of Respiratory Diseases (Prof M Zhou, Prof J Qu), Research Laboratory of Clinical Virology, Ruijin Hospital and Ruijin Hospital North (Prof X Zhang MD), and Clinical Research Center, Ruijin Hospital North (Prof X Zhang), Shanghai Jiaotong University School of Medicine, Shanghai, China; State Key Laboratory of Virology, Wuhan Institute of Virology, Center for Biosafety Mega-Science, Chinese Academy of Sciences, Wuhan, China (Prof Y Qiu PhD, Y Han)
Correspondence to: Prof Li Zhang, Tuberculosis and Respiratory Department, Wuhan Jinyintan Hospital, Dongxihu District, Wuhan 430023, China [email protected]
or
Prof Xinxin Zhang, Research Laboratory of Clinical Virology, Ruijin Hospital and Ruijin Hospital North, Shanghai Jiaotong University School of Medicine, Shanghai 200025, China [email protected]

Key unanswered questions to guide control
• Severity – how many mild cases for every severe (hospitalized) case, is it 10:1, 100:1, 1000:1 ?
• Worrying anecdotes about pre-symptomatic transmission including German cases reported in NEJM – is this common?
• Modes of transmission – large droplets?? Many family clusters but low R0 suggests perhaps prolonged close contact is important?
• Effect of interventions applied to date – travel restrictions, border screening, face mask use and massive social distancing