Embed Size (px)
Citation preview

¿Cómo tratamos al paciente EGFRm?, la importancia de buscar el mecanismo de resistencia
Antonio Calles
Servicio de Oncología Médica
Hospital General Universitario Gregorio Marañón
Instituto Investigación Sanitaria Gregorio Marañón
Madrid, España

NSCLC: From Histology to Genomics
Adenocarcinoma
“Druggable” genomic alterations

2004

Osimertinib Rociletinib Olmutinib
2014
3rd Generation EGFR TKIs presented at ASCO
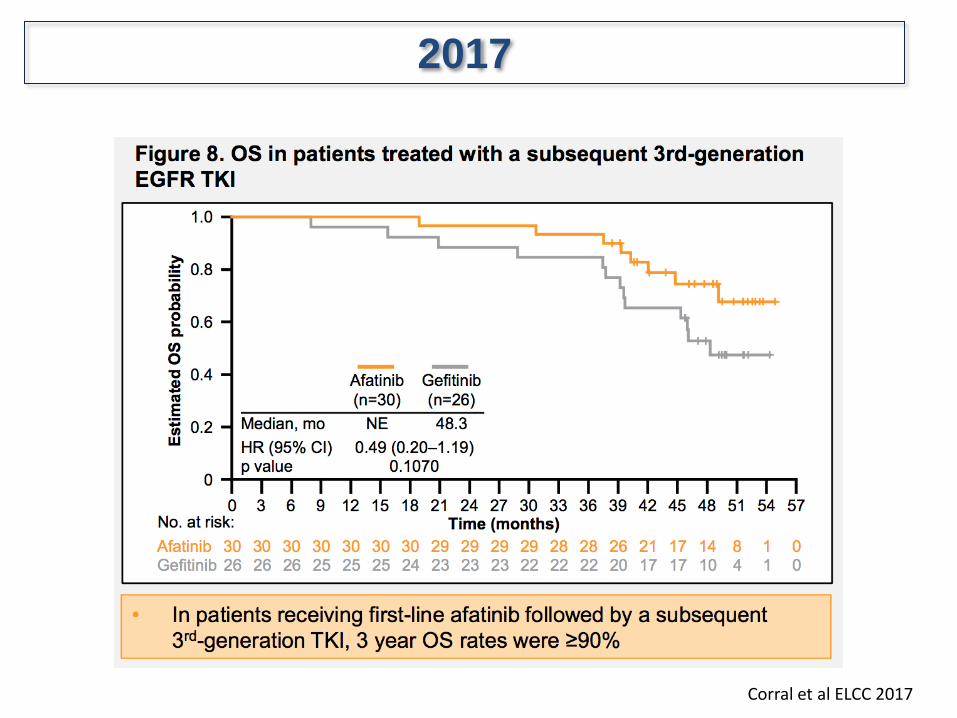
Corral et al ELCC 2017
2017

Resistance to targeted therapy may have different underlying
mechanisms
Camidge et al, Nat Rev Clin Oncol 2014

Baseline: Start erlotinib 3m: Response 14m: PD
30m: Re-biopsy
37m: Offered trial 39m: First dyspnea
18m 24m
35m
Radiographic progression does not always result in
clinical or symptomatic progression
Courtesy Dr. Jänne

Aquired EGFR-TKI resistance: different resistance mechanisms
PD: rebiopsy Initial biopsy
Erlotinib, Gefitinib,
Afatinib (8-12m)
EGFR
del 19
L858R
Yu et al., Clin Cancer Res 2013
On target
Off target

How does resistance develop during targeted therapy ?
Treatment pressure – bottleneck phenomenon
Adapted from Gerlinger M & Swanton C, Br J Cancer 2010;103:1139‒1143.

Kobayashi et al., NEJM 2005
T790M
secondary EGFR exon 20
gatekeeper-mutation
•Methionine bulk replaces drug from ATP binding-pocket
The EGFR T790M mutation confers resistance to 1st and 2nd gen. EGFR-TKIs

Chmielecki Sci Transl Med 2011 Zhou Nature 2009
EGFR T790M confers resistance to quinazoline inhibitors but sensitivity to
pyrimidine-based inhibitors
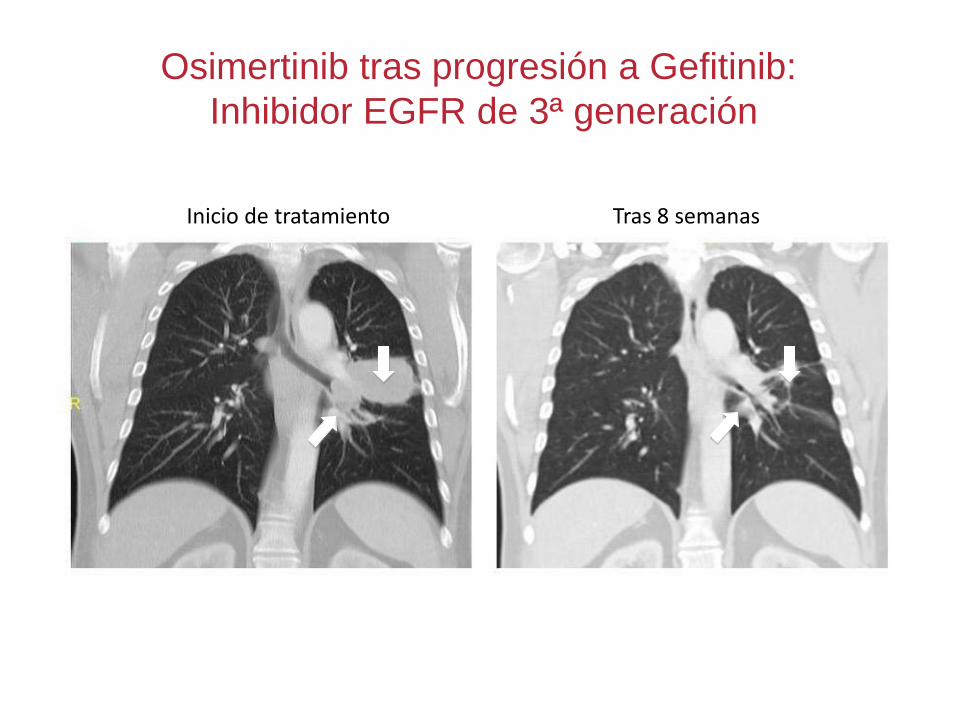
Osimertinib tras progresión a Gefitinib:
Inhibidor EGFR de 3ª generación
Inicio de tratamiento Tras 8 semanas

3rd gen. EGFR-TKI show high efficacy in T790M + acquired resistance
Erlotinib, Gefitinib,
Afatinib (8-12m)
PD: rebiopsy
T790M Osimertinib (8-10m) EGFR
del 19
L858R
Initial biopsy
also: liquid biopsy
Phase I (Aura)
mPFS 9.6 m
ORR: 61%
DCR: 95%
Phase III (Aura 3)
(Osimertinib vs. CT)
mPFS 10.1 vs. 4.4 m
Jänne et al., NEJM 2015 Mok et al., NEJM 2016

AURA3 study design
Key eligibility criteria
• ≥18 years (≥20 years in Japan)
• Locally advanced or metastatic NSCLC
• Evidence of disease progression following first-
line EGFR-TKI therapy
• Documented EGFRm and central confirmation
of tumour EGFR T790M mutation from a tissue
biopsy taken after disease progression on first-
line EGFR-TKI treatment
• WHO performance status of 0 or 1
• No more than one prior line of treatment for
advanced NSCLC
• No prior neo-adjuvant or adjuvant
chemotherapy treatment within 6 months prior
to starting first EGFR-TKI treatment
• Stable* asymptomatic CNS metastases allowed
R
2:1
Osimertinib (n=279)
80 mg orally
QD
Platinum-pemetrexed (n=140)
Pemetrexed 500 mg/m2 +
carboplatin AUC5 or
cisplatin 75 mg/m2
Q3W for up to 6 cycles
+ optional maintenance
pemetrexed# Optional crossover
Protocol amendment allowed patients on
chemotherapy to begin post-BICR confirmed
progression open-label osimertinib treatment
Endpoints
Primary:
• PFS by investigator assessment (RECISTv1.1)
Secondary and exploratory:
• Overall survival
• Objective response rate
• Duration of response
• Disease control rate
• Tumour shrinkage
• BICR-assessed PFS
• Patient reported outcomes
• Safety and tolerability
• Patients were stratified at randomisation based on ethnicity (Asian/Non-Asian)
• RECISTv1.1 assessments performed every 6 weeks until objective disease progression; patients could receive study treatment beyond RECISTv1.1 defined
progression as long as they experienced clinical benefit
• With 221 events of progression or death, the study would have 80% power to reject the null hypothesis of no significant difference in duration of PFS between the
two treatment groups, assuming a treatment effect HR of 0.67 at 5% two-sided significance
*Defined as not requiring corticosteroids for 4 weeks prior to study treatment; #For patients whose disease had not progressed after 4 cycles of platinum-pemetrexed
HR, hazard ratio; Q3W, every 3 weeks; R, randomisation; RECIST, Response Evaluation Criteria In Solid Tumors; WHO, World Health Organization

• Analysis of PFS by BICR was consistent with the investigator-based analysis: HR 0.28 (95% CI 0.20, 0.38), p<0.001;
median PFS 11.0 vs 4.2 months.
Population: intent-to-treat
Progression-free survival defined as time from randomisation until date of objective disease progression or death. Progression included deaths in the absence of RECIST progression.
Tick marks indicate censored data; CI, confidence interval
AURA3 primary endpoint:
PFS by investigator assessment 1.0
0.8
0.6
0.4
0.2
0 0 3 6 9 12 15 18
Pro
ba
bilit
y o
f
pro
gre
ss
ion
-fre
e s
urv
iva
l
No. at risk Osimertinib
Platinum-pemetrexed
Months 279 140
240
93
162
44
88 17
50
7
13
1
0 0
Median PFS, months (95% CI)
HR (95% CI)
10.1 (8.3, 12.3) 0.30 (0.23, 0.41) p<0.001 4.4 (4.2, 5.6)
Osimertinib
Platinum-pemetrexed

PFS benefit in AURA3 patients with
CNS metastases at baseline
With CNS metastases Without CNS metastases
Population: intent-to-treat
Progression-free survival defined as time from randomisation until date of objective disease progression or death. Progression included deaths in the absence of RECIST progression.
Tick marks indicate censored data. CNS metastases determined programmatically from baseline data of CNS lesion site, medical history, and/or surgery, and/or radiotherapy.
Pro
ba
bil
ity o
f
pro
gre
ss
ion
-fre
e s
urv
iva
l
1.0
0.8
0.6
0.4
0.2
0
No. at risk
Osimertinib
Platinum-
pemetrexed
0 3 6 9 12 15 18
93
51
80
32
46
9
27
4
14
2
4
0
0
0
Months
Osimertinib (n=93)
Platinum-pemetrexed (n=51)
Median PFS, months (95% CI)
8.5 (6.8, 12.3)
4.2 (4.1, 5.4)
HR 0.32
(95% CI 0.21, 0.49)
Pro
ba
bil
ity o
f
pro
gre
ss
ion
-fre
e s
urv
iva
l
1.0
0.8
0.6
0.4
0.2
0
0 3 6 9 12 15 18
186
89
160
61
116
35
61
13
36
5
9
1
0
0
Months
Osimertinib (n=186)
Platinum-pemetrexed (n=89)
Median PFS, months (95% CI)
10.8 (8.3, 12.5)
5.6 (4.2, 6.8)
HR 0.40
(95% CI 0.29, 0.55)

All causality adverse events* in AURA3
N (%)
15% cut-off
Osimertinib (N=279) Platinum-pemetrexed (N=136)
Any grade Grade ≥3 Any grade Grade ≥3
Any AE 273 (98) 63 (23) 135 (99) 64 (47)
Diarrhoea 113 (41) 3 (1) 15 (11) 2 (1)
Rash# 94 (34) 2 (1) 8 (6) 0
Dry skin# 65 (23) 0 6 (4) 0
Paronychia# 61 (22) 0 2 (1) 0
Decreased appetite 50 (18) 3 (1) 49 (36) 4 (3)
Cough 46 (16) 0 19 (14) 0
Nausea 45 (16) 2 (1) 67 (49) 5 (4)
Fatigue 44 (16) 3 (1) 38 (28) 1 (1)
Stomatitis 41 (15) 0 21 (15) 2 (1)
Constipation 39 (14) 0 47 (35) 0
Vomiting 31 (11) 1 (<1) 27 (20) 3 (2)
Thrombocytopenia# 28 (10) 1 (<1) 27 (20) 10 (7)
Neutropenia# 22 (8) 4 (1) 31 (23) 16 (12)
Leukopenia# 22 (8) 0 20 (15) 5 (4)
Anaemia# 21 (8) 2 (1) 41 (30) 16 (12)
Asthenia 20 (7) 3 (1) 20 (15) 6 (4)
Select adverse events
Interstitial lung disease# 10 (4) 1 (<1) 1 (1) 1 (1)
QT prolongation 10 (4) 1 (<1) 1 (1) 0
Population: safety analysis set (all patients who received at least one dose of study drug and for whom post-dose data were available)
*Includes AEs with an onset date on or after the date of first dose and up to and including 28 days following discontinuation of randomised treatment or the day before first administration of cross-over
treatment. Some patients had more than one AE. #Grouped term: if a patient has multiple preferred term level events within a specific grouped term AE, then the maximum CTCAE grade across those events is
counted.

• DNA fragments of 120-200bp with half life of ~2 hours
• Real-time, non-invasive, multi-lesions
• Cheaper because it does not require a biopsy
• Often very low amount of ctDNA
in the sea of wild type DNA - ”Needle in a farm”
• Specific to tumor
Diaz J Clin Oncol 2016
Liquid Biopsy


Plasma EGFR T790M • Plasma from AURA trial sent for BEAMing
– Paired tumor and plasma available for 216 patients
• Plasma T790M testing not as predictive as tumor T790M testing
Oxnard et al, JCO, 2016
T790M+
in tumor:
62% RR
T790M-
in tumor
26% RR

• Plasma from AURA trial sent for BEAMing
– Paired tumor and plasma available for 216 patients
18 T790M+
in plasma,
not tumor 111 T790M+
in tumor and
plasma
47
T790M+ in
tumor, not
plasma
40 patients T790M- tumor and
plasma
Plasma EGFR T790M
Oxnard et al, JCO, 2016

• Plasma from AURA trial sent for BEAMing
– Paired tumor and plasma available for 216 patients
18 T790M+
in plasma,
not tumor 111 T790M+
in tumor and
plasma
47
T790M+ in
tumor, not
plasma
40 patients T790M- tumor and
plasma
T790M+ in tumor:
62% RR, 10m PFS
T790M+ in plasma:
63% RR, 10m PFS
Plasma EGFR T790M
Oxnard et al, JCO, 2016

• Plasma from AURA trial sent for BEAMing
– Paired tumor and plasma available for 216 patients
18 T790M+
in plasma,
not tumor 111 T790M+
in tumor and
plasma
47
T790M+ in
tumor, not
plasma
40 patients T790M- tumor and
plasma
T790M+ in tumor:
62% RR, 10m PFS
T790M+ in plasma:
63% RR, 10m PFS
16.5m
PFS
4.3m
PFS
Plasma EGFR T790M
Oxnard et al, JCO, 2016

• Plasma from AURA trial sent for BEAMing
– Paired tumor and plasma available for 216 patients
• Tumor T790M-/plasma T790M+ has lower relative levels of T790M
Plasma EGFR T790M
Oxnard et al, JCO, 2016

WCLC 2017
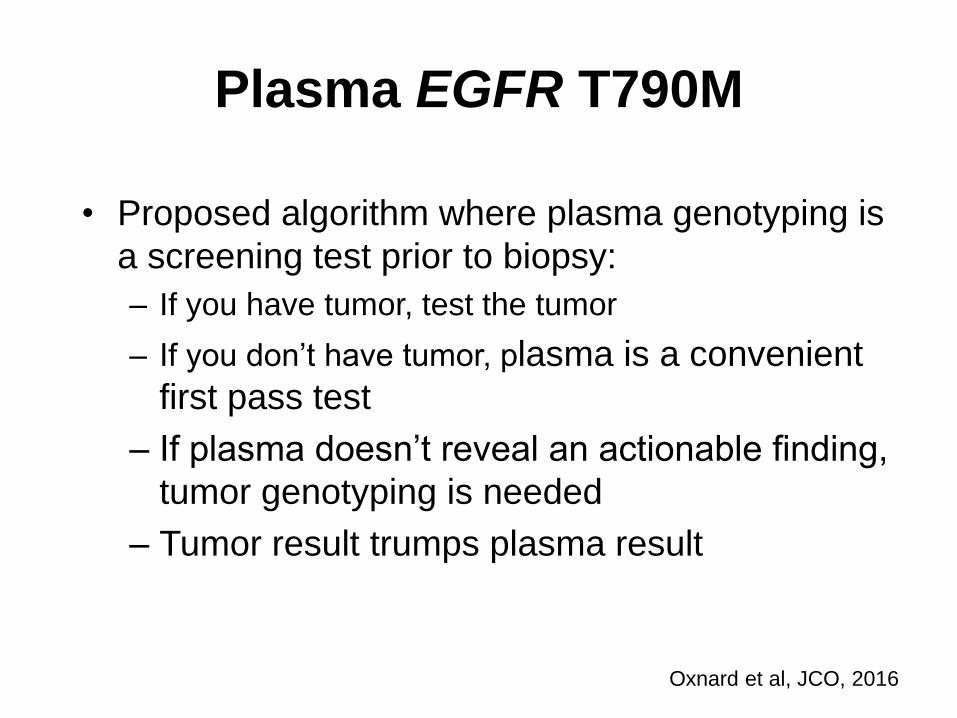
Plasma EGFR T790M
• Proposed algorithm where plasma genotyping is
a screening test prior to biopsy:
– If you have tumor, test the tumor
– If you don’t have tumor, plasma is a convenient
first pass test
– If plasma doesn’t reveal an actionable finding,
tumor genotyping is needed
– Tumor result trumps plasma result
Oxnard et al, JCO, 2016

Challenge 1: about 40% of AR cases are T790M negative
PD: rebiopsy Initial biopsy
Erlotinib, Gefitinib,
Afatinib (8-12m)
EGFRd
el 19
L858R
Yu et al., Clin Cancer Res 2013
On target
Off target

EGFR By-Pass Pathways: MET amplification
Zhang et al, Biomedicines 2015
Engelman Science 2007
MET/CEP7 probe set with specimens HCC827 (A) and HCC827 GR6 (B).

Scheffler et al, J Thorac Oncol 2015
Rebiopsy left arm: EGFR L858R, high-level METamp, TP53 C277*, TP53 R110C
Start crizotinib, continue erlotinib After 8 days of crizotinib + erlotinib
Molecular analysis pleural effusion: EGFR L858R T790M, low-level METamp Stop crizotinib and erlotinib, start AZD9291
Patient with activating EGFR mutation and good response for about 2 years:
now presenting with acquired resistance and massive progression

Waterfall plot based on evaluable patients (n = 64): all patients dosed and with on-treatment assessment or discontinuation prior to first tumour assessment
Data cut-off 31 Aug 2017
*17 patients did not have central FISH confirmation of MET-positive status (n = 6 MET-negative; n = 11 unknown by central lab); †Confirmed by a later scan performed at
least 4 weeks after initial response observed
TATTON Phase Ib expansion cohort: osimertinib plus savolitinib for patients with EGFR-
mutant MET-amplified NSCLC after progression on prior EGFR-TKI
Preliminary anti-tumour activity in all MET-positive patients*, n = 64
100
75
50
25
0
-25
-50
-75
-100
Best %
change fro
m b
aselin
e
in tum
our
lesio
n s
ize
Prior 3rd Gen T790M directed EGFR-TKI
No prior 3rd gen EGFR-TKI, T790M+
No prior 3rd gen EGFR-TKI, T790M-
TATTON Part B
NCT02143466
Objective
response rate,
n (%)
Prior 3rd Gen
T790M
directed
EGFR-TKI
(n = 30)
No prior 3rd Gen T790M
directed EGFR-TKI
Total
(n = 64)
T790M+
(n = 11)
T790M-
(n = 23)
ORR† 10 (33) 6 (55) 14 (61) 30 (47)

Phenotypic changes
1. Ephithelial-Mesenchimal Transition (EMT) 2. Small-Cell Lung Cancer Transformation (SCLCt)


Ercan Cancer Discovery 2009
FISH amplification in MAPK1
Curative effect of W+T treatment in vivo.
Erin M. Tricker et al. Cancer Discovery 2015;5:960-971
EGFR Downstream Activation: ERK Signaling Resistance to EGFR TKI

Targeted and non-targeted treatment options in T790M neg. AR
PD: rebiopsy Initial biopsy
Erlotinib, Gefitinib,
Afatinib T79M
hl
MET
ampl.
HER2
ampl.
SCLC
???
Osimertinib (10m) EGFR
del 19
L858R
EGFR-TKI + METinh.
EGFR-TKI + HER2inh.
Chemo, I-O, anti-DLL3
Chemo
clinical
trials

PD: rebiopsy Initial biopsy
Erlotinib, Gefitinib,
Afatinib (10m) T790M Osimertinib (10m)
EGFR
del 19
L858R
also: liquid biopsy
Osimertinib (20m)
PD: rebiopsy
Challenge 2: acquired resistance to 3rd gen. EGFR inhibitors
?

Yu et al. JAMA Oncology 2015
Erlotinib
AZD9291
EGFR Mutations and Resistance to Irreversible Pyrimidine-Based EGFR Inhibitors

EGFR C797S mutation mediates resistance to 3rd generation EGFR TKI
Zhou et al, Nature 2009; Thress et al, Nature Medicine 2015
abolishes covalent binding
of 3rd gen. EGFR inhibitor
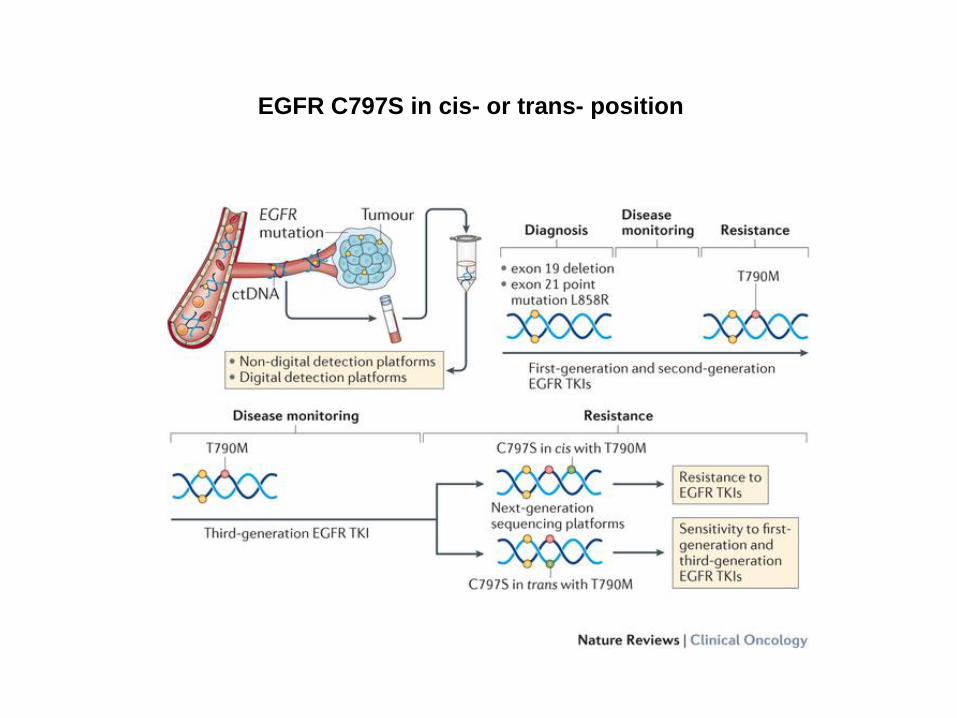
EGFR C797S in cis- or trans- position

Novel dominant EGFR solvent-front mutations in AR to osimertinib
Detection by plasma testing of a 69y old
Caucasian female with AR to osimertinib:
•L858R (MAF 17.9%)
•T790M (MAF 18.2%)
•G796S/R (MAF 14.4%)
•C797S/G (MAF 2.26%)
•L792F/H (MAF 0.35%)
•V802F (MAF 0.36%)
disables osimertinib
binding by sterical
interference
Ou et al, Lung Cancer 2017


Osimertinib resistance on tumor NGS
• EGFR C797S was detected only in patients
with maintained T790M
119 T790M+ patients treated with single-agent
osimertinib for acquired resistance
29 remain on therapy without
progression
10 off due to AE without progression
80 patients eligible for resistance analysis
35 without post-progression biopsy
12 without complete tissue testing
33 patients with progression tumor NGS
11
maintained
T790M
22 lost T790M
7 C797S
5 SCLC histologic
transformation*
1 BRAF V600E
1 KRAS Q61K
1 CCDC6-RET fusion
1 FGFR3-TACC
fusion
3 MET amplification
2 PIK3CA mutation*
1 PIK3CA
mutation
*Patient with both
PIK3CA + SCLC
transformation
• Competing resistance mechanisms were
detected in patients with loss of T790M
0 3 6 9
1 0
1 0 0
1 0 0 0
1 0 0 0 0
M o n th s s in c e s ta r t in g o s im e r t in ib
Co
pie
s/m
L o
f p
las
ma
E G F R e x o n 1 9 d e l
E G F R T 7 9 0 M
K R A S Q 6 1 K
B io p s y d a teS ta r t o f o s im e rtin ib
N /D
Oxnard et al, AACR 2017
Loss of T790M new competing resistance mechanisms

Validation cohort:
loss of T790M associated with early resistance
• Those with T790M loss had a shorter TTF compared to those with maintained T790M
0 6 12 18 24 300
25
50
75
100
TTF (months)
Pe
rce
nt
wit
ho
ut
trea
tme
nt
failu
re
T790M lossMedian: 5.5
T790M+/C797S-Median: 12.6
T790M+/C797S+Median: 12.4
N = 110
<=5.5 >5.5 to <=13 >130
10
20
30
40
TTF (months)
Nu
mb
er
of
pati
en
ts
T790Mloss
T790M+/C797S-
N = 38 N = 36 N = 36
T790M+/C797S+
• Plasma available for 157 subjects on the first-in-human AURA trial, 110 with a detectable
driver at time of osimertinib resistance
• Among those with early resistance (TTF <=5.5 months), 68% had loss of T790M
Oxnard et al, AACR 2017

Serial plasma genotyping on osimertinb
Rapid loss of T790M with
continued increase in driver
mutation in a patient with
small cell transformation on
biopsy
Emergence of C797S mutation with the
re-emergence of exon 19 del and T790M
after initial response to osimertinib
0 3 6 9 12
10
100
1000
10000
Time on osimertinib (months)
Co
pie
s/m
L o
f p
las
ma
Biopsy dateStart of osimertinib
EGFR C797S TA
EGFR C797S GC
N/D
EGFR T790M
EGFR exon 19 del
0 1 2
10
100
1000
10000
Time on osimertinib (months)
Co
pie
s/m
L o
f p
las
ma
EGFR exon 19 del
EGFR T790M
Start of osimertinib
Biopsy date
N/D
Acquired EGFR C797S Small cell transformation
• Resistance due to loss of T790M is often seen early on osimertinib
• Resistance due to EGFR C797S is often seen later on osimertinib

Conclusion
• Loss of T790M does not indicate resensitization to first-generation EGFR TKI, but often indicates overgrowth of a competing resistance mutation [NOMBRE
DE LA CATEGORÍA]
T790M+/ C797S-
Unknown
Other rare genotypes
MET amp
SCLC
T790M loss T790M maintained
• Range of rare genetic resistance mechanisms to look out for:
• KRAS mutations
• RET fusions
• FGFR fusions

Osimertinib resistance
• Timing of resistance impacts biology of resistance
• Repeat plasma T790M testing can guide next steps?
Oxnard et al, AACR 2017
Osimertinib
for T790M+
NSCLC
Early
Resistance
Late
Resistance
Suspect outgrowth of competing
resistance mechanism
Suspect resistance with
maintained EGFR addiction
Consider trial of osimertinib combined with
additional EGFR inhibitor (e.g. necitumumab)
Consider trial of osimertinib combined with
alternate pathway inhibitor (e.g. MET inhibitor)

Nazartinib (EGF816) Phase I dose-escalation part
Presented By Daniel Tan at 2017 ASCO Annual Meeting

Gene alterations at progression and nazartinib efficacy
Presented By Daniel Tan at 2017 ASCO Annual Meeting

Tumor heterogeneity:
different clones may drive
different metastatic sites
Govindan, Science 2014
Clonal heterogeneity
over time
Spatial heterogeneity at given timepoint

Evolutionary patterns of resistance differ on time and location
Treatment at clinical progression
Residual disease:
Treatment at time of response
Preventive Treatments

Immunotherapy is not a good option for 2L EGFRm NSCLC
Akbay, Cancer Discovery 2013

Is progression
clinically significant?
Progression on first-line EGFR TKI
Approach to the management of EGFR mutant NSCLC with progression on first-line EGFR TKI
Sacher, Jänne & Oxnard Cancer 2014
Is progression localized?
Is re-biopsy feasible?
Start chemotherapy +/- continued
TKI
There is not one uniform approach to treating resistance


• Paradigma de tratamiento dirigido en tumores sólidos.
– Rápidos avances, aumento de la complejidad, repercusión en supervivencia del paciente.
• No vamos a “curar” a los pacientes con terapias dirigidas anti-EGFR, pero sí tendremos pacientes “crónicos”
• No todos los EGFR TKIs son iguales y sus mecanismos de resistencia, tampoco.
• Los pacientes con adenocarcinoma de pulmón EGFR mutado requieren de un manejo individualizado (y multidisciplinar):
– Cirugía, Radioterapia, Quimioterapia, Terapias Dirigidas, ¿Inmunoterapia?
• Por definir el “mejor tratamiento” de entrada, la “mejor secuencia” de tratamientos, y ¿la mejor combinación? (sinergias on-target + off-target)
• Entender significado de biopsia líquida (falsos negativos) y monitorización
• Rebiopsiar las progresiones y tener fármacos disponibles
Take Home Messages Mecanismos de resistencia EGFRm