Embed Size (px)
Citation preview

1
Community Water Fluoridation
HCC Briefing
October 2016
Author: Tim Fielding, City Health and Wellbeing Manager Acknowledgement: This briefing is based primarily on several Public Health England (PHE) reports that are listed at section 11.
Contents
1. Introduction
2. Summary
3. What is fluoride
4. Current situation re fluoridation in UK
5. Evidence regarding the effect of water fluoridation
5.1. Dental benefits
5.2. Impact of water fluoridation on inequalities in oral health
5.3. Dental fluorosis (mottling)
5.4. Other (non-dental) health effects
6. Cost benefits
7. Ethical issues regarding fluoridated water
8. Funding for water fluoridation schemes
9. Key agencies and stakeholders and their roles
9.1. Key agencies in legislation
9.2. Other key stakeholders
9.3. Other relevant agencies
10. The process for an area considering implementing water fluoridation
10.1. Key steps towards introducing a new fluoridation scheme
10.2. Joint decision-making by local authorities
11. References and sources of further information
Appendix 1: Map – Areas of fluoridation schemes and naturally occurring fluoride
Appendix 2: Outline of statutory and other processes for a local authority wishing to propose a scheme of community water fluoridation

2
1. Introduction: This report is intended as an internal HCC briefing document to summarise the facts regarding
water fluoridation in a balanced manner. It is not intended to make the case for or against
water fluoridation in Hull, but to ensure that relevant officers and elected members have the
necessary information to inform them.
The briefing provides a summary of the evidence, legislation and issues regarding water
fluoridation. For more detail or to discuss any aspects of the report or water fluoridation,
council officers and elected members are encouraged to contact Tim Fielding, City Health and
Wellbeing Manager or Julia Weldon, Director of Public Health.
This briefing is based primarily on several Public Health England reports that are listed at
section 11. The key documents for an oversight of the issue and the steps involved for any
area considering introducing water fluoridation are the ‘Water Fluoridation: Health monitoring
report for England 2014’ (PHE, 2014) and ‘Improving oral health: a community water
fluoridation toolkit for local authorities’ (PHE, 2016).
2. Summary
Fluoride is naturally present in water supplies. In a number of areas the level is adjusted to
improve oral health. This process is governed by primary and secondary legislation. Since
April 2013 decision-making regarding fluoridation rests with upper tier and unitary local
authorities.
Systematic reviews of the scientific evidence have reported that water fluoridation substantially
reduces levels of tooth decay in both child and adult populations served by this measure.
There is also evidence that water fluoridation is associated with improved outcomes such as
reduced levels of child hospital admission for tooth extraction.
A small minority of children in both non-fluoridated and fluoridated areas of the UK have
noticeable dental fluorosis (mottling of the teeth), though severe dental fluorosis is rare. The
rate of fluorosis is higher in fluoridated areas.
Systematic reviews of the scientific evidence have found no adverse impacts on general health
that could be attributed to fluoride in water at a concentration of 1 part per million, whether
naturally occurring or added.
Naturally occurring fluoride exists in all water supplies. Community water fluoridation ensures
that, where the natural fluoride concentration is too low to provide dental health benefits, it is
raised to and maintained at the optimum level (one part per million or 1mg/litre).
Parliament has given its express consent to the deployment of water fluoridation as a public
health measure, by passing legislation to that end. However, parliament has also decreed that
3
decisions about particular water fluoridation schemes should be made locally, not nationally,
and only through a rigorous process defined in legislation. From April 2013 the decision-
makers are the local authorities defined in the legislation.
3. What is fluoride
Fluoride is widely present in the environment, ranking thirteenth among the elements in order
of abundance in the earth’s crust. It occurs naturally in virtually all water.
The concentration of fluoride in water is normally expressed as milligrams of fluoride per one
litre of water (mg/l) or in parts fluoride per million parts of water (ppm). One mg/l equates to
1ppm. The concentration of fluoride naturally occurring in water is extremely variable, being
affected by many factors including geology. In some parts of Africa and the Indian sub-
continent, for example, fluoride levels in water may reach 10 or 20mg/l.
In the UK, the naturally occurring level of fluoride in water is typically around 0.1 to 0.2 mg/l,
although in some localities (for example Hartlepool and Uttoxeter) it is about 1.0mg/l and in
some private water supplies (springs, wells, boreholes ) can reach 3 or 4mg/l before correction.
About a third of a million people in England have a water supply in which the naturally
occurring background level of fluoride is around the optimal level of 1mg/l.
The most advantageous level of fluoride in water, in temperate climates, to be one part of
fluoride per million parts of water, or 1mg fluoride per litre of water (1mg/l). At this level the
benefits of fluoride in reducing decay are optimal. Higher levels of fluoride confer little
additional benefit in terms of decay reduction while increasing the risk of dental fluorosis.
4. Current situation regarding water fluoridation in UK
Naturally occurring fluoride exists in all water supplies. Community water fluoridation ensures
that, where the natural fluoride concentration is too low to provide dental health benefits, it is
raised to and maintained at the optimum level (one part per million or 1mg/litre).
Community water fluoridation schemes were first introduced in the US in 1945. Following
successful trials in the UK in the 1950s, pioneer local authorities in England adopted
fluoridation to tackle the problem of tooth decay in children. Birmingham led the way in 1964
and was quickly followed in the same decade by a number of other local authorities, some
urban, some rural. Today, fluoridation schemes in England cover approximately six million
people.
Most of the existing schemes in England were introduced by local authorities. Further
schemes, predominantly in the West Midlands, were introduced by the NHS from the late
1970s onwards. Currently, 26 local authorities have fluoridation schemes covering the whole or
parts of their area with approximately six million people in England receiving a fluoridated water

4
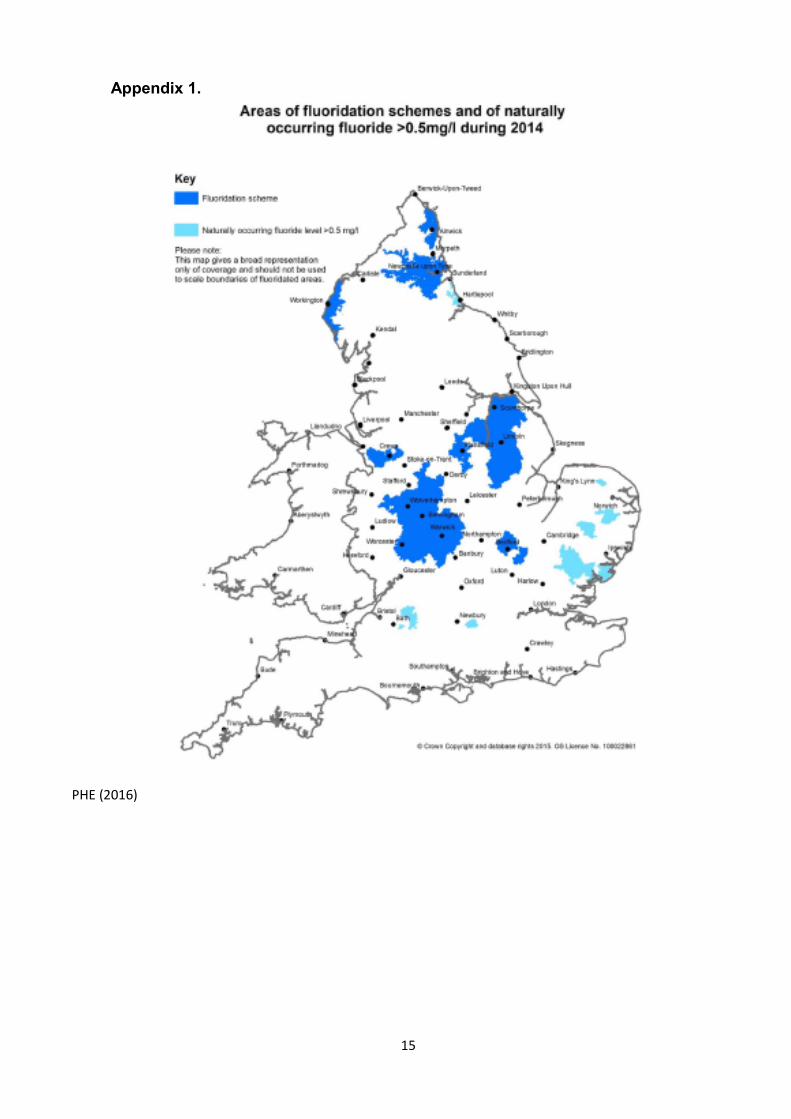
supply, principally in the North-East and in the West and East Midlands. A map of fluoridated
areas is in Appendix 1.
Countries with fluoridation schemes include the United States, Canada, Brazil, Argentina,
Chile, England, Ireland, Spain, Australia, New Zealand, Malaysia, Singapore and South Korea.
Major cities around the world with fluoridation schemes include New York, Los Angeles,
Chicago, Washington DC, Philadelphia, Atlanta, Boston, Miami, Rio de Janeiro, Sao Paolo,
Buenos Aires, Santiago, Birmingham, Newcastle upon Tyne, Coventry, Dublin, Cork, Seville,
Bilbao, Hong Kong, Sydney, Melbourne, Brisbane, Adelaide, Perth, Auckland and Wellington.
Over the past ten years there has been an increase in fluoridation coverage around the world,
particularly in the United States, Brazil, Chile, Australia and Malaysia, adding around 50 million
people who receive this public health measure.
5. Evidence regarding the effect of water fluoridation
Fluoride in water can reduce the likelihood of experiencing dental decay and minimise its
severity. Evidence reviews confirm that it is an effective, safe public health measure suitable
for consideration in localities where levels of dental decay are of concern.
The evidence in support of the effectiveness and safety of water fluoridation is considered to be
robust and high quality by Public Health England.
Some fluoride occurs naturally throughout the world in water used for drinking, but the amount
is hugely variable. A very low level of natural fluoride, as found in most parts of England, has
no documented impact on health. At the other extreme, as in parts of Africa, India and Asia,
very high levels of naturally occurring fluoride in water consumed over the long-term can cause
a serious condition called skeletal fluorosis. This is extremely rare in western countries.
Within the UK water fluoridation is endorsed as a public health intervention by Public Health
England (PHE), the British Medical Association Board of Science, the Faculty of Public Health
of the Royal College of Physicians, the Faculty of Dental Surgery of the Royal College of
Surgeons of England, the British Dental Association, the British Society for Paediatric Dentistry
and many bodies representing health professionals. Fluoridation is widely supported
internationally including by the World Health Organisation (WHO).
5.1. Dental benefits
A very large number of studies and ‘reviews’ and ‘systematic reviews’ of studies over the
last 10-20 years have demonstrated a clear dental health benefit from water fluoridation.
The exact estimate of the size of the benefits varies depending on the methodology used,
the time period included and the countries covered. Typical examples of the benefits
identified include:

5
• Children in fluoridated communities having fewer decayed, missing and filled
teeth than children in non-fluoridated communities e.g.
o 2.25 fewer decayed, missing and filled teeth among 5-15 year olds across a
range of countries (York Review, 2000, see PHE, 2015)
o between 30% and 50% fewer teeth decayed, missing and filled in 4-17 year olds
in United States (Center for Disease Control and Prevention, 2002, see PHE,
2015)
o 35% fewer decayed, missing and filled baby teeth and 26% fewer decayed,
missing and filled permanent teeth (Cochrane Oral Health Group, 2015, see PHE,
2015)
o 15% increase in children with no decay in their baby teeth and a 14% increase in
children with no decay in their permanent teeth (Cochrane Oral Health Group,
2015, see PHE, 2015)
o On average, five-year olds in fluoridated areas are 15% less likely to have had
tooth decay than those in non-fluoridated areas. When deprivation and ethnicity
(important factors for dental health) are taken into account, five-year olds in
fluoridated areas are 28% less likely to have had tooth decay
than those in non-fluoridated areas. (PHE, 2014)
o On average, 12-year olds in fluoridated areas are 11% less likely to have had
tooth decay than those in non-fluoridated areas. When deprivation and ethnicity
are into account, 12-year olds in fluoridated areas are 21% less likely to have had
tooth decay than those in non-fluoridated areas. (PHE, 2014)
• Reduction in tooth decay in adults living in fluoridated areas compared to non-
fluoridated areas e.g.
o between 27% and 35% lower among those who have lived all their lives in
fluoridated areas (Griffen et al, 2007)
• Reduction in hospital admissions and general anaesthetic for children
o in fluoridated areas there were 45% fewer hospital admissions of children aged
one to four for dental caries (mostly for extraction of decayed teeth under a
general anaesthetic) than in non-fluoridated areas (when deprivation was
accounted for, this figure rose to 55%) (PHE, 2014)

6
5.2. Impact of water fluoridation on inequalities in oral health
PHE’s health monitoring report (2014) states:
“The reduction in tooth decay in children of both ages in fluoridated areas appears
greatest among those living in the most deprived local authorities.”
The evidence-base however for the impact of water fluoridation on reducing health
inequalities is less clear than for the overall dental benefits of fluoridation.
5.3. Dental fluorosis (mottling)
There is a well-established adverse association between levels of fluoride in water and the
prevalence of dental fluorosis (mottling of the teeth).
Dental fluorosis is one of a number of different conditions that can affect the appearance of
teeth. In England it is usually seen as paper-white flecks or fine white lines but it can vary
in appearance from barely visible white lines to patches which may be of aesthetic concern.
The risk period for the development of dental fluorosis in permanent (adult) teeth is when
the teeth are growing in the jaws; dental fluorosis cannot develop after teeth are formed.
The first two to three years of life are generally accepted to be the period of highest
susceptibility for fluorosis affecting the front teeth (the incisors).
The impact of milder forms fluorosis on measured quality of life (using the Oral Health
Related Quality of Life scale) is certainly less than that of tooth decay, and may be non-
existent or even positive.
A positive effect on quality of life may seem counter-intuitive but may be explained by the
fact that the white flecking of enamel associated with very mild fluorosis can give the
impression of having teeth that are whiter than average. More severe dental fluorosis can
cause brown staining and pitting of teeth but is generally seen in those countries with very
high naturally occurring levels of fluoride in groundwater rather than in areas with
community water fluoridation schemes. It should be noted that dental fluorosis can also
occur in the absence of water fluoridation, through ingestion of other sources of fluoride
during tooth formation, particularly toothpaste and other fluoride supplements.
A Medical Research Council report in 2002 concluded that, as far as artificially fluoridated
areas in the UK and Europe are concerned, around 3% to 4% of children may have dental
fluorosis of possible aesthetic concern, compared with around 1% in non-fluoridated areas.
A comparison of (fluoridated) Newcastle and (unfluoridated) Manchester used a scoring
system with a scale of 0-9 for severity and found that the percentage of children with mild or
mild to moderate (score 3) was 6% in fluoridated Newcastle and 1% in unfluoridated
7
Manchester. However, the prevalence of higher scores (TF4 or greater) was very low in
both cities – 1% in fluoridated Newcastle and 0.2% in unfluoridated Manchester. Of these,
very few children were seen with a score of 5, representing the lower end of severe
fluorosis scores - 0.1% in fluoridated Newcastle and 0.2% in unfluoridated Manchester and
no children were found with higher scores.
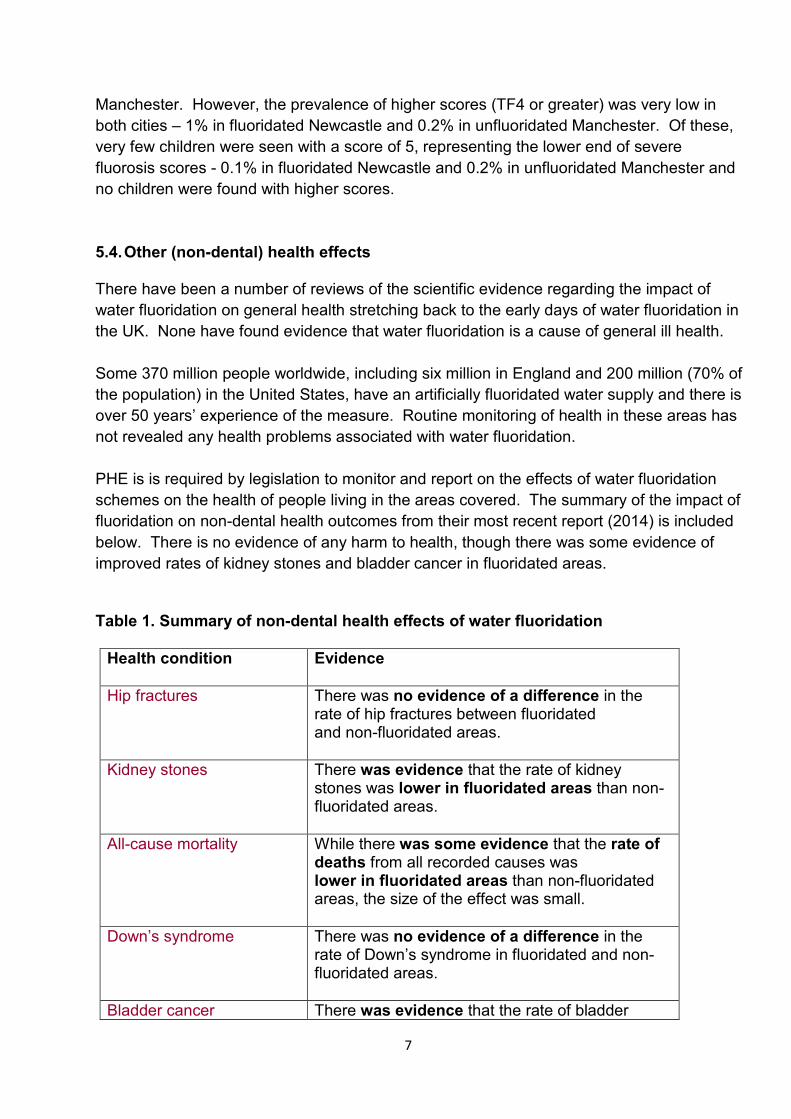
5.4. Other (non-dental) health effects
There have been a number of reviews of the scientific evidence regarding the impact of
water fluoridation on general health stretching back to the early days of water fluoridation in
the UK. None have found evidence that water fluoridation is a cause of general ill health.
Some 370 million people worldwide, including six million in England and 200 million (70% of
the population) in the United States, have an artificially fluoridated water supply and there is
over 50 years’ experience of the measure. Routine monitoring of health in these areas has
not revealed any health problems associated with water fluoridation.
PHE is is required by legislation to monitor and report on the effects of water fluoridation
schemes on the health of people living in the areas covered. The summary of the impact of
fluoridation on non-dental health outcomes from their most recent report (2014) is included
below. There is no evidence of any harm to health, though there was some evidence of
improved rates of kidney stones and bladder cancer in fluoridated areas.
Table 1. Summary of non-dental health effects of water fluoridation
Health condition
Evidence
Hip fractures
There was no evidence of a difference in the rate of hip fractures between fluoridated and non-fluoridated areas.
Kidney stones
There was evidence that the rate of kidney stones was lower in fluoridated areas than non-fluoridated areas.
All-cause mortality
While there was some evidence that the rate of deaths from all recorded causes was lower in fluoridated areas than non-fluoridated areas, the size of the effect was small.
Down’s syndrome
There was no evidence of a difference in the rate of Down’s syndrome in fluoridated and non-fluoridated areas.
Bladder cancer There was evidence that the rate of bladder

8
cancer was lower in fluoridated areas than non-fluoridated areas.
Osteosarcoma (a form of bone cancer) among under 25-year olds
There was no evidence of a difference in the rate of osteosarcoma between fluoridated and non-fluoridated areas.
Osteosarcoma (a form of bone cancer) among people aged 50 and over
There was no evidence of a difference in the rate of osteosarcoma between fluoridated and non-fluoridated areas.
All cancer
There was no evidence of a difference in the rate for all types of cancer between fluoridated and non-fluoridated areas.
(PHE, 2014)
6. Cost benefits
The cost-effectiveness of any fluoridation scheme is dependent on the local costs of the
scheme compared to the savings in the treatment of dental decay and disease, reduced
hospital admissions and the indirect or societal costs of the disease and its consequences.
The cost-effectiveness of fluoridation will be greater in areas with poorer dental health. These
are generally areas with high levels of deprivation.
Work is ongoing locally to calculate the estimated potential costs and savings from water
fluoridation to inform decision making.
7. Ethical issues regarding fluoridated water
The topic of water fluoridation can prompt ethical debates about adding a relatively small
amount of fluoride to local water supplies and arguments that individuals have a right to drink
water without added fluoride and that the local authority would be interfering with this right.
This is needed to be balanced against arguments claiming that any such concerns are
outweighed by the need and opportunity to prevent avoidable pain and suffering from tooth
decay with a safe and effective public health measure.
9
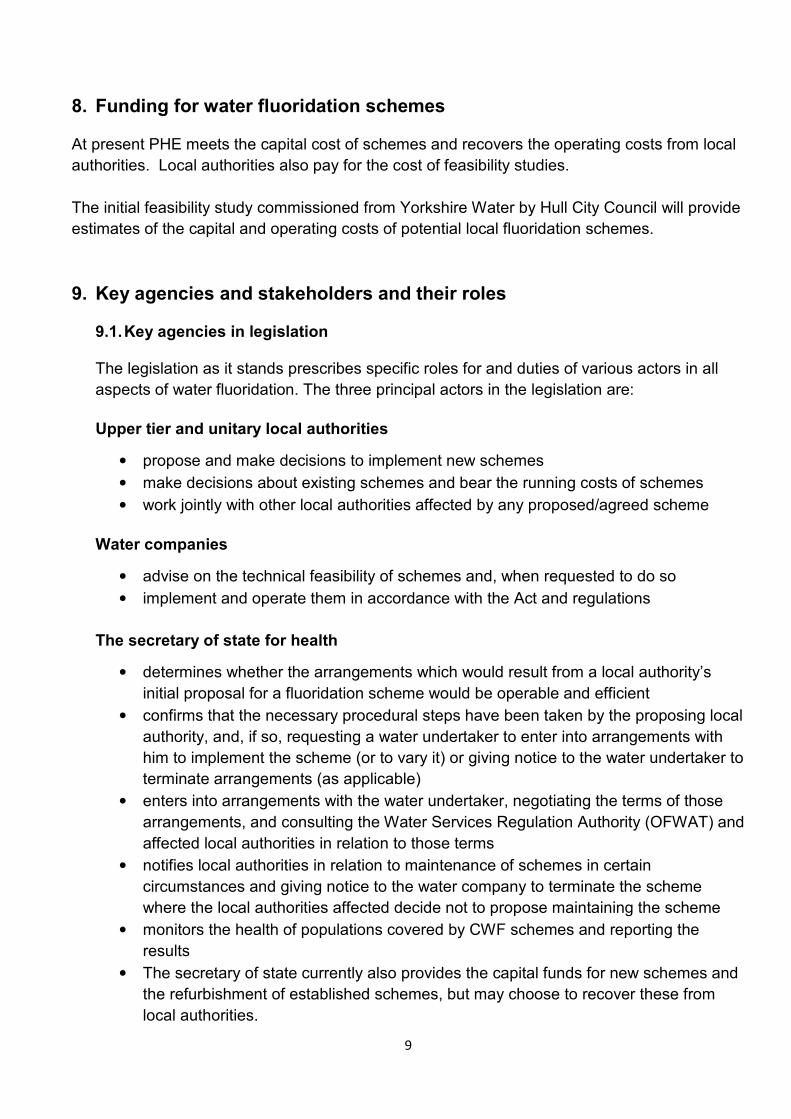
8. Funding for water fluoridation schemes
At present PHE meets the capital cost of schemes and recovers the operating costs from local
authorities. Local authorities also pay for the cost of feasibility studies.
The initial feasibility study commissioned from Yorkshire Water by Hull City Council will provide
estimates of the capital and operating costs of potential local fluoridation schemes.
9. Key agencies and stakeholders and their roles 9.1. Key agencies in legislation
The legislation as it stands prescribes specific roles for and duties of various actors in all
aspects of water fluoridation. The three principal actors in the legislation are:
Upper tier and unitary local authorities
• propose and make decisions to implement new schemes
• make decisions about existing schemes and bear the running costs of schemes
• work jointly with other local authorities affected by any proposed/agreed scheme
Water companies
• advise on the technical feasibility of schemes and, when requested to do so
• implement and operate them in accordance with the Act and regulations
The secretary of state for health
• determines whether the arrangements which would result from a local authority’s
initial proposal for a fluoridation scheme would be operable and efficient
• confirms that the necessary procedural steps have been taken by the proposing local
authority, and, if so, requesting a water undertaker to enter into arrangements with
him to implement the scheme (or to vary it) or giving notice to the water undertaker to
terminate arrangements (as applicable)
• enters into arrangements with the water undertaker, negotiating the terms of those
arrangements, and consulting the Water Services Regulation Authority (OFWAT) and
affected local authorities in relation to those terms
• notifies local authorities in relation to maintenance of schemes in certain
circumstances and giving notice to the water company to terminate the scheme
where the local authorities affected decide not to propose maintaining the scheme
• monitors the health of populations covered by CWF schemes and reporting the
results
• The secretary of state currently also provides the capital funds for new schemes and
the refurbishment of established schemes, but may choose to recover these from
local authorities.
10
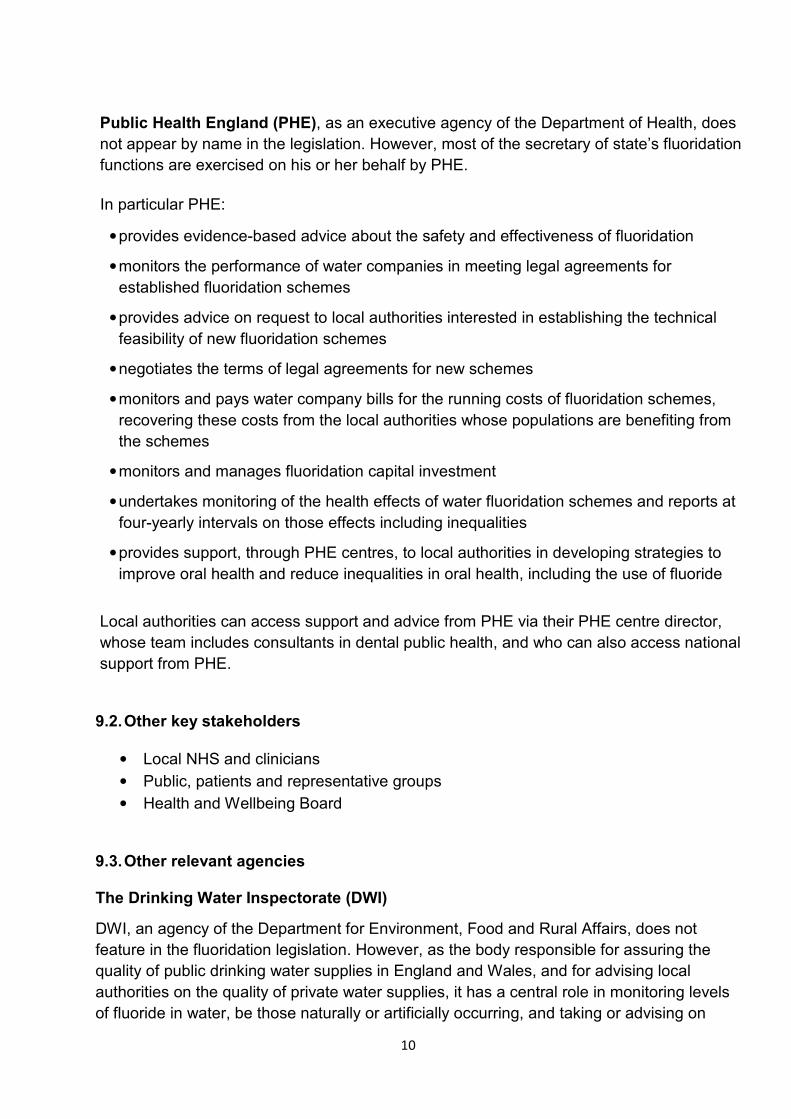
Public Health England (PHE), as an executive agency of the Department of Health, does
not appear by name in the legislation. However, most of the secretary of state’s fluoridation
functions are exercised on his or her behalf by PHE.
In particular PHE:
• provides evidence-based advice about the safety and effectiveness of fluoridation
• monitors the performance of water companies in meeting legal agreements for
established fluoridation schemes
• provides advice on request to local authorities interested in establishing the technical
feasibility of new fluoridation schemes
• negotiates the terms of legal agreements for new schemes
• monitors and pays water company bills for the running costs of fluoridation schemes,
recovering these costs from the local authorities whose populations are benefiting from
the schemes
• monitors and manages fluoridation capital investment
• undertakes monitoring of the health effects of water fluoridation schemes and reports at
four-yearly intervals on those effects including inequalities
• provides support, through PHE centres, to local authorities in developing strategies to
improve oral health and reduce inequalities in oral health, including the use of fluoride
Local authorities can access support and advice from PHE via their PHE centre director,
whose team includes consultants in dental public health, and who can also access national
support from PHE.
9.2. Other key stakeholders
• Local NHS and clinicians
• Public, patients and representative groups
• Health and Wellbeing Board
9.3. Other relevant agencies
The Drinking Water Inspectorate (DWI)
DWI, an agency of the Department for Environment, Food and Rural Affairs, does not
feature in the fluoridation legislation. However, as the body responsible for assuring the
quality of public drinking water supplies in England and Wales, and for advising local
authorities on the quality of private water supplies, it has a central role in monitoring levels
of fluoride in water, be those naturally or artificially occurring, and taking or advising on
11
compliance action in the event of breaches of the drinking water standard for fluoride. DWI
also publishes the technical code of practice on the design and operation of fluoridation
plant and may provide technical advice to PHE on such matters.
The Water Services Regulation Authority
The Water Services Regulation Authority (OFWAT) is a non-ministerial government
department and is the economic regulator of the water sector in England and Wales. Its role
in water fluoridation is that of a statutory consultee on the terms to be included in the
proposed legal agreement for a new fluoridation scheme and, in particular, terms which
affect the operation of the water undertaker's supply system.
10. The process for an area considering implementing water fluoridation
Local authorities were the driving force behind the introduction of water fluoridation schemes in
England in the 1960s. In 1974 the responsibility for fluoridation was transferred to the NHS.
The Health and Social Care Act 2012, by amending the Water Industry Act 1991 (the Act),
returned responsibility for those decisions to local authorities with public health responsibilities.
10.1. Key steps towards introducing a new fluoridation scheme
Upper tier and unitary local authorities are responsible for determining the need for new
fluoridation schemes. They are required to undertake public consultations before they
make a final decision. This applies when just a single local authority is involved and when a
number of authorities receiving water from the same sources are involved. In the latter
case, they must form a joint committee to oversee the process and make the decision.
The consultation process is defined in the legislation. It is essential that a local authority
considering a fluoridation scheme understands the legislation and obtains independent
legal advice throughout the whole process.

12
Table 2. Summary of key steps towards a new scheme
Phase Content
1 Preliminary scoping phase (non-statutory) and informal discussion with any other affected local authorities.
2 Commencement of statutory process – making an initial proposal, perhaps with multiple proposers.
3 Assessment of operability and efficiency, including agreement of secretary of state to proceed.
4 Consultation with other affected local authorities (if any), and securing their consent to proceed.
5
Public consultation and subsequent decision-making including, in the case of multiple local authorities, joint committee arrangements. In the latter instance, decisions may need to be made by a process of weighted population voting.
6
Making an agreement between the secretary of state and the water company including issuing an indemnity to the company.
7 Scheme implementation.
Further detail regarding the process for implementing a new fluoridation scheme is at Appendix 2. As at September 2016, Hull City Council is still within Phase 1, undertaking preliminary scoping.
10.2. Joint decision-making by local authorities
Because their boundaries are defined by water distribution systems, not by administrative
boundaries, water fluoridation schemes usually extend beyond the boundary of a single local
authority. All formal consideration of proposals for fluoridation arrangements covering more
than one authority has to involve each of the affected local authorities in a way prescribed in
the fluoridation legislation, and in the absence of unanimity about a particular proposal, has to
be determined in a way again prescribed in the legislation.
In a multi-authority situation where one or more of the authorities concerned believes that a
new scheme should be introduced, it is necessary for at least one of the affected authorities
initially to make a formal proposal to the secretary of state for the desired action. Except in
circumstances where it would not be necessary to undertake a public consultation about the

13
proposal, the proposer first has to consult and secure the support of the other affected
authorities to undertake public consultation.
It will be important to ensure that all affected authorities are actively involved in that
consultation. In the absence of unanimity the regulations prescribe that the matter should be
resolved by a process of weighted voting between the authorities, each authority having in
effect a single block vote the size of which is determined by the proportion of the whole
population affected by the proposal which is resident in the area of that authority. It is
necessary for the proposal to secure at least 67% of the total block vote to succeed. The
method of calculating the voting is set out in the schedule to the regulations.
Should it be determined that the formal proposal should proceed to public consultation, it is
then necessary for the authorities affected to agree on and establish joint committee
arrangements for progressing the matter. The options for joint committee arrangements are
defined in s88F of the Act.
Following public consultation, decisions about the outcome are taken in the joint committee
established for that purpose and have to take account of certain matters prescribed in the
legislation. In the absence of unanimity the outcome decision is again taken by the process of
weighted voting between the affected local authorities. Each authority represented on the joint
committee has a single block vote the size of which is determined by the proportion of the
whole population affected by the proposal which is resident in the area of that authority. It is
again necessary for the proposal to secure at least 67% of the total block vote to succeed.
11. References and sources of further information
Specific references regarding water fluoridation:
• Public Health England (2014), Water Fluoridation: Health monitoring report for England 2014.
• Public Health England (2015), An overview of water fluoridation [nb. this briefing was written specifically for the information session held for Hull Councillors in November 2015. Contact Tim Fielding for a copy]
• Public Health England (2016) Improving oral health: a community water fluoridation toolkit for local authorities.
References regarding improving oral health at a local level:
• Public Health England (2014),Local Authorities Improving Oral Health: Commissioning Better Oral Health for Children and Young People
• NICE (2014) Public health guidance – Oral health: local authorities and partners
14
Local documents and references:
• Hull’s Oral Health Action Plan 2015-20
• Dental Health sections of Joint Strategic Needs Assessment (JSNA):
o Full chapter on Dental health
o Oral Health Needs in Hull summary 2015 [Contact Tim Fielding for a copy]
15
PHE (2016)
Appendix 1.
16
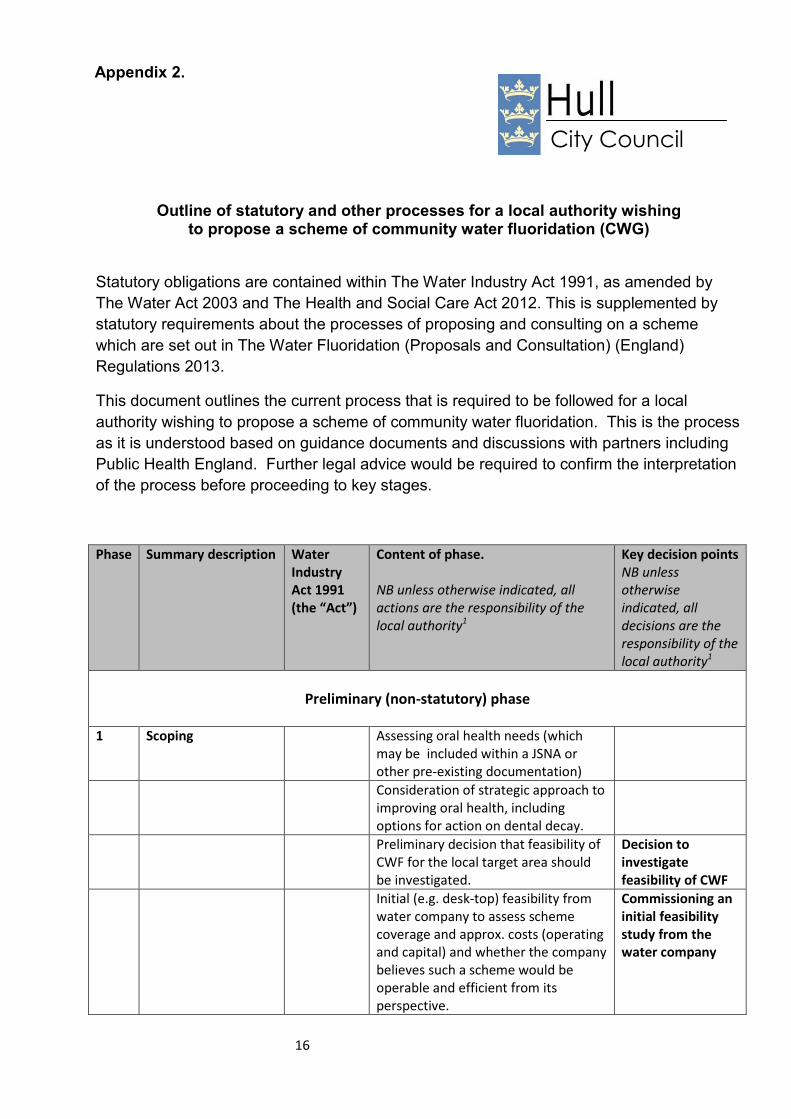
Outline of statutory and other processes for a local authority wishing to propose a scheme of community water fluoridation (CWG)
Statutory obligations are contained within The Water Industry Act 1991, as amended by
The Water Act 2003 and The Health and Social Care Act 2012. This is supplemented by
statutory requirements about the processes of proposing and consulting on a scheme
which are set out in The Water Fluoridation (Proposals and Consultation) (England)
Regulations 2013.
This document outlines the current process that is required to be followed for a local
authority wishing to propose a scheme of community water fluoridation. This is the process
as it is understood based on guidance documents and discussions with partners including
Public Health England. Further legal advice would be required to confirm the interpretation
of the process before proceeding to key stages.
Phase Summary description Water
Industry
Act 1991
(the “Act”)
Content of phase.
NB unless otherwise indicated, all
actions are the responsibility of the
local authority1
Key decision points
NB unless
otherwise
indicated, all
decisions are the
responsibility of the
local authority1
Preliminary (non-statutory) phase
1 Scoping Assessing oral health needs (which
may be included within a JSNA or
other pre-existing documentation)
Consideration of strategic approach to
improving oral health, including
options for action on dental decay.
Preliminary decision that feasibility of
CWF for the local target area should
be investigated.
Decision to
investigate
feasibility of CWF
Initial (e.g. desk-top) feasibility from
water company to assess scheme
coverage and approx. costs (operating
and capital) and whether the company
believes such a scheme would be
operable and efficient from its
perspective.
Commissioning an
initial feasibility
study from the
water company
City Council
Appendix 2.
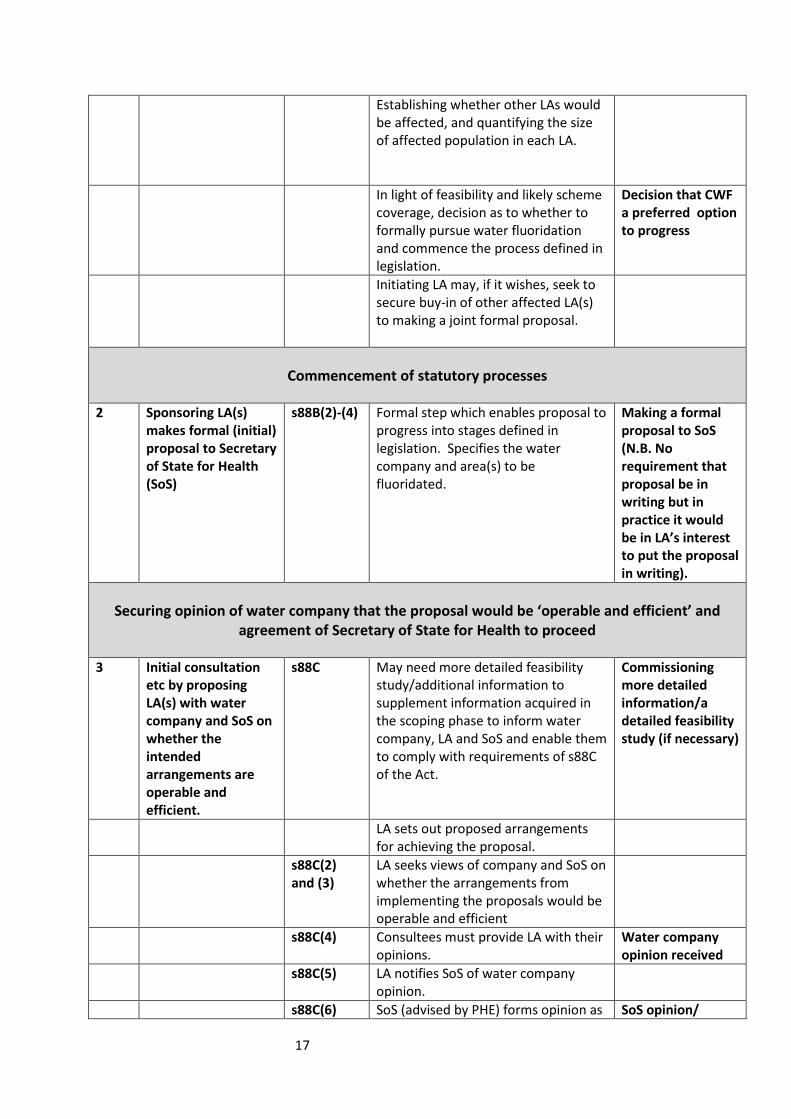
17
Establishing whether other LAs would
be affected, and quantifying the size
of affected population in each LA.
In light of feasibility and likely scheme
coverage, decision as to whether to
formally pursue water fluoridation
and commence the process defined in
legislation.
Decision that CWF
a preferred option
to progress
Initiating LA may, if it wishes, seek to
secure buy-in of other affected LA(s)
to making a joint formal proposal.
Commencement of statutory processes
2 Sponsoring LA(s)
makes formal (initial)
proposal to Secretary
of State for Health
(SoS)
s88B(2)-(4) Formal step which enables proposal to
progress into stages defined in
legislation. Specifies the water
company and area(s) to be
fluoridated.
Making a formal
proposal to SoS
(N.B. No
requirement that
proposal be in
writing but in
practice it would
be in LA’s interest
to put the proposal
in writing).
Securing opinion of water company that the proposal would be ‘operable and efficient’ and
agreement of Secretary of State for Health to proceed
3 Initial consultation
etc by proposing
LA(s) with water
company and SoS on
whether the
intended
arrangements are
operable and
efficient.
s88C May need more detailed feasibility
study/additional information to
supplement information acquired in
the scoping phase to inform water
company, LA and SoS and enable them
to comply with requirements of s88C
of the Act.
Commissioning
more detailed
information/a
detailed feasibility
study (if necessary)
LA sets out proposed arrangements
for achieving the proposal.
s88C(2)
and (3)
LA seeks views of company and SoS on
whether the arrangements from
implementing the proposals would be
operable and efficient
s88C(4) Consultees must provide LA with their
opinions.
Water company
opinion received
s88C(5) LA notifies SoS of water company
opinion.
s88C(6) SoS (advised by PHE) forms opinion as SoS opinion/

18
to whether or not the proposal would
be operable and efficient. If not,
proposal falls.
Clearance to LA to
proceed to next
stage
Phase required if any other LA(s) would be affected by the proposal
4 Consultation by
proposing LA(s) with
other affected LAs (if
proposal covers
more than one LA
area and other LAs
are not joint
proposers)
s88D(2)-(3) Consult other affected LAs by giving
them certain information about the
proposal and allowing them a period
of at least three months for a
response as per Regulations1 (Reg 3).
Each LA decides whether it wishes to
proceed to public consultation on the
proposed scheme and notifies the
proposing LA of its views.
See Regulations 3(5) and 4(2)
Requires LAs
representing 67%
or more of
affected
population to
agree to proceed
to public
consultation.
Undertaking public consultation
5 Public consultation s88E(2) LA(s) consult public for at least three
months as per Regs.
See Regulation 5 for content and
approach.
s88F Where more than one LA is affected
by the proposal (and wishes to
participate in the process), the LAs
concerned must agree joint
committee arrangements to consider
the outcome of the consultation and
make decisions.
Establishing LA
joint committee
arrangements
Post-consultation, LA(s) make decision
as to whether to implement the
fluoridation proposal as per Regs.,
including whether any modification to
the proposal is required.2
If no unanimous
decision reached,
LAs representing
67% of affected
population must
agree to
1 The Water Fluoridation (Proposals and Consultation)(England) Regulations 2013
2 NB if any modification to the area covered by the proposal would extend or reduce the boundary of the proposal by
more than 20% of the houses included in the initial proposal, full re-consultation would be necessary (Regulations,
Reg 15(1)(b) and 15(2)
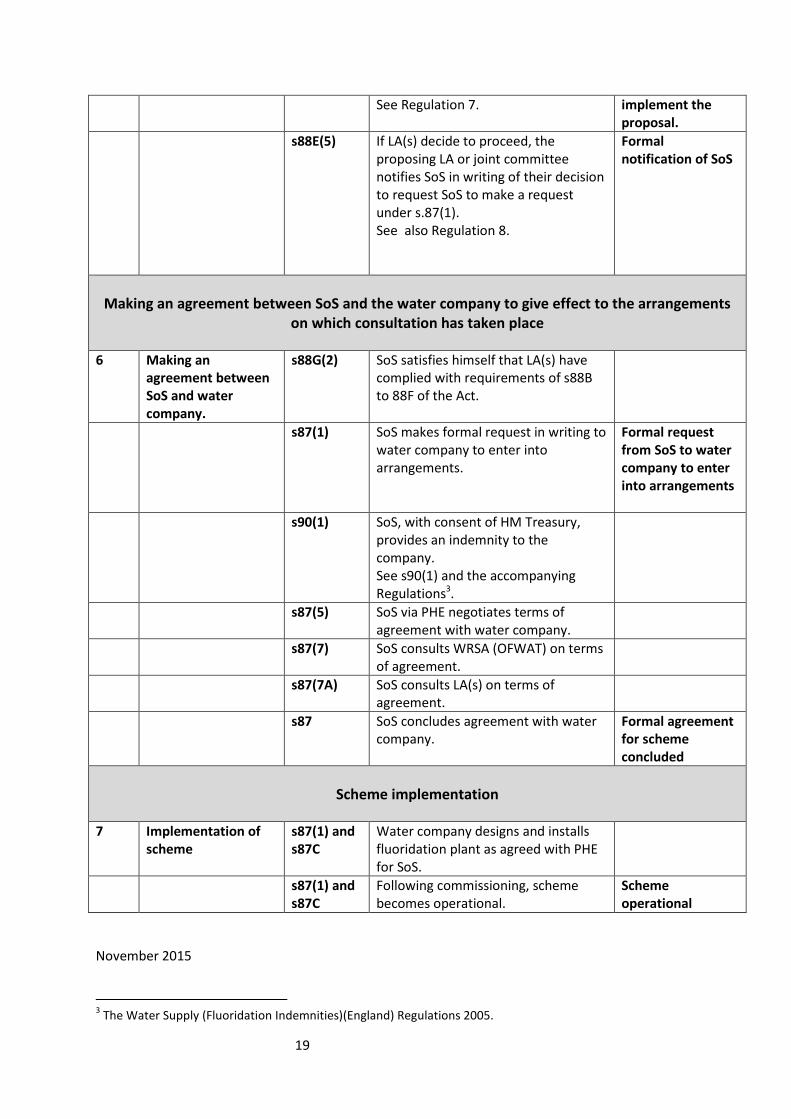
19
See Regulation 7. implement the
proposal.
s88E(5) If LA(s) decide to proceed, the
proposing LA or joint committee
notifies SoS in writing of their decision
to request SoS to make a request
under s.87(1).
See also Regulation 8.
Formal
notification of SoS
Making an agreement between SoS and the water company to give effect to the arrangements
on which consultation has taken place
6 Making an
agreement between
SoS and water
company.
s88G(2) SoS satisfies himself that LA(s) have
complied with requirements of s88B
to 88F of the Act.
s87(1) SoS makes formal request in writing to
water company to enter into
arrangements.
Formal request
from SoS to water
company to enter
into arrangements
s90(1) SoS, with consent of HM Treasury,
provides an indemnity to the
company.
See s90(1) and the accompanying
Regulations3.
s87(5) SoS via PHE negotiates terms of
agreement with water company.
s87(7) SoS consults WRSA (OFWAT) on terms
of agreement.
s87(7A) SoS consults LA(s) on terms of
agreement.
s87 SoS concludes agreement with water
company.
Formal agreement
for scheme
concluded
Scheme implementation
7 Implementation of
scheme
s87(1) and
s87C
Water company designs and installs
fluoridation plant as agreed with PHE
for SoS.
s87(1) and
s87C
Following commissioning, scheme
becomes operational.
Scheme
operational
November 2015
3 The Water Supply (Fluoridation Indemnities)(England) Regulations 2005.





























