Embed Size (px)
Citation preview

Community Ear & Hearing Health Volume 9 • Issue 12 (2012) 1
&Community
Ear HearingHealth
Addressing ear and hearing problems at primary level
T he World Health Organization estimates that around half of all deafness and hearing impairment could be prevented if common causes were dealt with at primary
healthcare level. Primary care has a particularly important role to play in low- and middle-income countries, home to 80% of the 275 million persons estimated to have disabling hearing impairment worldwide.1
Addressing causes and risk factors By increasing community awareness, providing early treatment and timely referral to specialist services, primary care interventions can address the most common causes of hearing impairment worldwide, namely acute and chronic otitis media, genetic factors and ageing. Primary care can also target other causes of deafness, such as infections during pregnancy (e.g. rubella or syphilis) or during childhood (e.g. meningitis, measles, mumps or cerebral malaria). For example, by providing immunisations, public health education, acute care and regular follow-ups for children with respiratory diseases and/or acute otitis media, a primary care programme can reduce both short- and long-term hearing disability due to eardrum perforations and complications of long-standing ear discharge.
Reducing the impact of hearing impairment Primary care can also help reduce the penalty of deafness and hearing impairment by offering rehabilitation and making the community aware of deaf people’s rights to education, employment and wellbeing. This has benefi cial effects not just on affected individuals, but also on their families who stand to be impoverished by the burden of supporting a disabled relative and by the absence of a potentially productive worker.
Making primary care a reality Although few would disagree with the potential benefi ts of primary ear and hearing care, it remains an unfulfi lled promise in too many low- and middle-income regions. For primary care to become a reality, four critical components must be present:
Competent and empowered primary care workers: suffi cient numbers of personnel need to be trained to provide timely, appropriate and respectful care to people at risk for or suffering from deafness. These personnel must implement care pathways and protocols that integrate hearing testing and otoscopy in routine clinical encounters and home visits. They should also be able to ensure hearing-impaired patients
Jose M AcuinProfessor in Ear, Nose and Throat & Head and Neck SurgeryDe La Salle University Health Sciences Institute; Director for Medical Quality Improvement,The Medical City, Manila, Philippines
PIET VAN HASSELT
Volume 9Issue 122012
Ear examination with an otoscope. MADAGASCAR
We hope youwill enjoy the journal’s new design and
user-friendly format
Continues overleaf !

2 Community Ear & Hearing Health Volume 9 • Issue 12 (2012)2
have access to healthcare services and are included in social welfare programmes. The pool of health personnel available for primary ear and hearing care training will vary in each region. In low- and middle-income countries with challenging geographies, most village clinics are manned by a midwife or a volunteer healthcare worker; evenin sprawling urban centres, general practitioners, nurses and midwives in both private and government facilities must wear many hats and provide a variety of primary care services.
Cost-effective technologies to detect and manage hearing problems: sturdy, portable fi eld audiometers, tympanometers and devices for screening the newborn for hearing loss must be mass-produced. Providing hearing amplifi cation devices at the primary care level and ensuring their continued use is still a challenge. The ideal hearing amplifi cation device for a poor country would be one which is so cheap as to be almost free, shock-proof, weather-proof, rechargeable, possesses the required technical specifi cations and blends with culturally defi ned appearances so as to be virtually invisible. But even such an ideal device would have a limited lifespan, would need to be serviced regularly and changed as the hearing loss evolved. Given that hearing aid dispensing facilities and hearing aid technicians are nearly nonexistent in primary care settings, a technology must be found that allows users themselves to try on and discard cheap hearing devices without committing to costly ear moulds, batteries, repairs and maintenance costs.
Working referral systems and adequate hospital facilities: the credibility of the deafness prevention programme and of the primary care workers will be undermined if the entire system fails people after hearing loss has been identifi ed or if deaf patients continue to suffer from poor access to hearing services. Primary care workers must be supported by higher-level facilities staffed by adequately trained specialists who can provide further assessment and defi nitive management. Where referral systems are limited by unequal distribution of human resources, primary care workers must develop their own personal networks of colleagues to facilitate access to more advanced care. Government and private facilities as well as providers must be urged to establish formal and informal partnerships to provide services for hearing-impaired people.
Government and community support: government and civil societies must support and invest in primary care infrastructure, human resources, promotive and preventive interventions, as well as treatment and rehabilitation services for hearing-impaired people at all levels of the health system.
Conclusion By promoting community health, by targeting potential causes of deafness and by harnessing the capacity of communities to implement local interventions to improve the welfare of persons with hearing impairment, primary ear and hearing care workers can not only reduce the incidence of deafness but also mitigate its devastating effects.
This issue aims to support any personnel providing primary ear and hearing care, by offering tips on how to address common ear and hearing problems.
1 World Health Organization, Deafness and hearing impairment,Fact sheet Nº300, February 2012. www.who.int
Editorial
Addressing ear and hearing problems at primary levelJose M Acuin 1
Common ear and hearing complaints:tips for assessment at primary levelPadman Ratnesar 3
Primary care of the external earPadman Ratnesarand Ian Mackenzie 5
Conditions affecting the middle ear: what to do at primary levelDiego J Santana-Hernández,Padman Ratnesarand Paddy Ricard 6
How to refer a patient: practical tipsAndrew Smith 9
Improving communication with patients who have a hearing impairmentValerie E Newton and Seema Rupani Shah 10
‘Red fl ag’ situationsat primary level 12
IN THIS ISSUE
PIET
VAN
HAS
SELT
EditorDr Paddy Ricard
Editorial committeeProfessor Andrew Smith (Chair)Dr Ian MackenzieProfessor Valerie E NewtonDr Padman Ratnesar
Regional consultantDr Jose M Acuin (Philippines)
Editorial assistantAnita Shah
DesignLance Bellers
Printing Newman Thomson
Online editionSee ‘Publications’ on http://disabilitycentre.lshtm.ac.uk
How to subscribeThe journal is sent free of charge to readers working in low- and middle-income countries. To subscribe, please send your name, occupation, postal address, phone number and email address to: Anita Shah,
Community Ear and Hearing Health, International Centre for Eye Health, London School of Hygiene and Tropical Medicine, Keppel Street, London WC1E 7HT, United Kingdom. Email: [email protected]
We recommend that readers in high-income countries make an annual donationof UK £10. To subscribe, please contact Anita Shah (as above).
CorrespondencePlease send all enquiries to: Anita Shah (for contact details, see left).
CopyrightArticles may be photocopied, reproduced or translated, provided these are not used for commercial or personal profi t. Acknowledgements should be made to the author(s) and to Community Ear and Hearing Health.
This journal is funded by CBM
This fi ve-day course is organised by the London School of Hygiene and Tropical Medicine several times a year in collaboration with local partners.It is aimed at professionals working in the fi eld of ear and hearing health and/or public health.For information on 2013 courses, please contact: [email protected](+44 207 958 8313)
Forthcoming course:Cape Town, South Africa (26–30 November 2012)Contact [email protected] for more information.
SHORT COURSE: PUBLIC HEALTH PLANNING FOR HEARING IMPAIRMENT
Primary ear care. MALAWI

Community Ear & Hearing Health Volume 9 • Issue 12 (2012) 3
Patients usually consult a health worker about their ear or their hearing when their quality of life is noticeably affected. This article is a guide
to assessing the most common complaints and arriving at a decision on their management.
‘I can’t hear’You need to ask a few questions, examine the ear and test the patient’s hearing to decide how to proceed.
1 Ask the patient:• Has your hearing loss occurred suddenly in the last
48 hours? If the answer is ‘Yes’, then refer the patient to an ear doctor immediately: it may be possible to improve the hearing or stop it getting worse.
• Has your hearing been getting worse gradually?A treatable cause can be found.
• Any noises in the ear or dizziness? (see below). • Any other problems such as earache or an ear
discharge? If the answer is ‘Yes’, these problems will need treating before the hearing loss can be managed with a hearing aid.
Common ear and hearing complaints: tips for assessment at primary level
Common complaints
Padman RatnesarConsultant Otolaryngologist and Head and Neck SurgeonBromley NHS Trust Hospitals (retired),United Kingdom
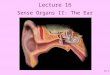
The diagram below1 shows the different components of the external (or outer) ear, middle ear and inner ear:
• The pinna collects sound waves, which are then conducted through the ear canal towards the middle ear.
• Sound waves transmitted by the ear canal cause the eardrum to vibrate, which in turn causes the three ossicles to transmit sound to the inner ear.
• This amplifi ed vibration from the middle ear ossicles is then transmitted through fl uid in the cochlea (the auditory part of the inner ear). The eighth cranial nerve connects the cochlea to the brain.
As a health worker, you should always be aware of the ear’s connection to the nose and throat through the Eustachian tube, which drains fl uid from the middle ear and equalises pressure in it. Any upper respiratory tract infection may lead to a dysfunction of the Eustachian tube and a subsequent infection or infl ammation of the middle ear.
ANATOMY OF THE EAR
2 Examine the ear (see sections below and pages5 to 8). It is preferable to use an otoscope to examine the ear canal and middle ear.
3 Test the patient’s hearing (see Box below).2
Patients with a hearing loss and no associated ear disease need to be referred to a specialist centre for further hearing tests.
If the patient is an adult or a child over fi ve years of age:1 Stand a metre away and hold a notebook in
front of your face or mouth to prevent lip reading.2 Give an instruction very quietly, e.g. ‘Put your
hand on your head’. 3 Estimate the degree of hearing loss by noting if
you have to raise your voice to a moderate or loud level or if there is no response.
4 Repeat the instruction to check reliability.5 If you suspect unilateral hearing loss, block the
ear canal of the better-hearing ear by pressing over its tragus (the bump in front of the ear canal) from behind the patient. Then test the hearing of the affected ear.
If the patient is a child under fi ve years of age:1 Ask the mother to sit the child on her knee,
holding him/her at the waist.2 Stand a metre behind and slightly to the side,
making sure the child does not know you are there. 3 Speak quietly or make a humming sound. 4 Note if the child turns to you, if you have to raise
your voice for this, or if the child does not turn.5 Observe any confusion regarding the direction of
the sound (e.g. does the child look elsewhere fi rst?).6 Repeat the hearing test to check reliability.
SIMPLE INSTRUCTIONSTO TEST A PATIENT’S HEARING
OUTEREAR
MIDDLEEAR
INNEREAR
Cochlea
Vestibular system
Pinna
Eustachian tube
Auditory nerve
Ear canalEardrum
Ossicles
Continues overleaf !

Community Ear & Hearing Health Volume 9 • Issue 12 (2012)4
‘I have an earache’This is a frequent complaint. It can be due to: causes located in the external ear, causes located in the middle ear or referred pain (this pain is perceived in the ear, but its root cause lies elsewhere).
1 Establish whether the pain is referred from a site other than the ear. The three commonest causes of referred pain are a sinus infection, a tooth infection or an infection of the tonsils.
Ask the patient to open their mouth whilst exerting pressure in front of the ear on the temporo-mandibular joint (the joint of the jaw):if the patient then experiences an increase in pain, the ear pain is in fact referred pain and the cause is one of the three mentioned above (infection of the teeth, tonsils or sinuses).
Management: give the patient a painkiller such as paracetamol; treat the infection with antibiotics(by mouth or by injection) or refer the patient to a person able to treat it.
2 If the earache is not referred pain:• Check that there is no infl ammatory condition
affecting the pinna: common conditions (see page 5) are furunculitis, herpes zoster and carcinoma (cancer).
• Examine the ear canal to exclude a foreign body (see instructions for removal on page 5).
• Check that you can see the eardrum and exclude any infl ammation, infection or perforation (see pages 6 to 8). If you cannot see the eardrum, is there an infl ammation or infection of the ear canal, perhaps with signs of pus or fl uid (otitis externa)? (see page 5 for management).
• If there is no perforation, is the eardrum bulging or is it retracted? Fluid in the ear will cause the drum to bulge, which causes pain. If the drum is retracted, this is a sign that the Eustachiantube is blocked, which will also cause pain(see pages 6 to 8).
‘I have an ear discharge’A discharge is more often than not due to an infection. It can be watery or purulent (thick and yellow, sometimes blood-stained) and occasionally have an offensive smell.
1 First, dry mop the discharge to visualise the ear canal. Use dry mops (see left) if you have been trained to use them.3 If not, you can safely employ wicks made of clean cotton material.
2 If there is no perforation of the eardrum, treat as an otitis externa (see page 5 for management).
3 If there is a perforation of the eardrum, this is a middle ear condition. Check for the signs of any complication (see Box on page 8) and refer the
patient to an ear doctor. Until the patient attends the district hospital, manage the condition as acute or chronic otitis media, depending on whether the ear has been discharging for less or more than two weeks, respectively (see pages 6 to 8).
‘There is a buzzing in my ears’ This ‘buzzing’ is referred to as tinnitus: the person hears sounds of different frequencies in their ear in the absence of any external visible source of noise.
1 If tinnitus is associated with vertigo (dizziness), refer immediately as this indicates a problem with the eighth cranial nerve.
2 Exclude any foreign body or abnormalities in the external canal or the eardrum, including the middle ear. A foreign body can cause tinnitus (see instructions for removal on page 5).
3 Look for an abnormality of the eardrum (e.g. perforation): if this is the case, refer to an ear doctor for further treatment.
4 Undertake a simple hearing test to determine whether there is a hearing loss (see page 3). Some hearing losses are associated with tinnitus and a hearing aid may help.
5 Once all possible causes related to the ear have been excluded, consider other causes. Neck problems (cervical spondylosis or arthritis of the neck) can commonly be responsible for tinnitus. Head injuries, high blood pressure, severe anaemia, and acute infection of the oral cavity spreading into the middle ear can also be causes of tinnitus.
‘I’m feeling dizzy’Dizziness (vertigo) is generally related to a disturbance of the balance mechanism (vestibular system) located in the inner ear.
1 If there is no ear disease and normal hearing, possible causes could be related to abnormal blood pressure, anaemia or diabetes. Check for malnutrition, as it is often a cause of anaemia and other metabolic disturbances such as diabetes.
2 If there is an ear disease and/or a hearing loss, refer to an ear doctor. Dizziness is a sign of complication in the inner ear. If the patient presents with deafness in one ear, tinnitus and vertigo, this could be a very serious condition. Refer immediately.
3 If there is no obvious cause such as the ones mentioned above, exclude any abnormality of the cervical spine: ask the patient to move their head to look up sideways and back; if this causes vertigo, then the problem is related to the neck (cervical spondylosis).
4 If all of the above causes have been excluded, refer to a neurologist for further investigation. Dizziness should never be ignored.
1 This diagram is reprinted from: World Health Organization, Primary Ear and Hearing Care Training Resource (WHO: Geneva, 2006). This training resource is a collection of four manuals aimed at primary level health workers and communities in low- and middle-income countries. They provide understanding of ear disease as well as simple, effective methods to prevent and manage common ear and hearing problems and help people use hearing aids effectively. They can be ordered by emailing [email protected] or downloaded from www.who.int/topics/deafness/en2 You will fi nd more detailed instructions on how to test hearing in: World Health Organization, Primary Ear and Hearing Care Training Resource, Trainer’s manual, Intermediate level, Module 6, page 91 (WHO: Geneva, 2006).3 You will fi nd more detailed instructions on how to make and use dry mops in: World Health Organization, Primary Ear and Hearing Care Training Resource, Trainer’s manual, Intermediate level, Module 4, page 57 (WHO: Geneva, 2006).
Common complaints
ABSORBING A DISCHARGE WITHA DRY MOP
PIET
VAN
HAS
SELT
Wrap a piece of loose cotton wool around a fi ne stick no more than 2 mm in diameter(as below1,3).
The cotton wool should be fi rmly attached to the stick at one end and fl uffy at the other end, so that it may absorb any discharge.
Do not insert the dry mop beyond the discharge you can see.
WH
O1 Cotton wool
Thin stick
Dry mop
Dry mopping

Community Ear & Hearing Health Volume 9 • Issue 12 (2012) 5
The external ear consists of the pinna and ear canal (see page 3). Three types of problems commonly affect it: trauma (injury) to the pinna; infl ammatory
conditions affecting the pinna and surrounding structures; blockage (obstruction) of the ear canal.
Trauma to the pinna• If the trauma has just occurred, apply a cold pack
to the pinna.• If there is a haematoma (a swelling under the skin
containing blood), let it resolve by itself (unless expert help is available to drain the haematoma).
• Dress any lacerations and wounds with vaseline gauze, if available; otherwise, use a dry dressing.
• Any wound needing suturing must be referred to a doctor with experience in ear/facial reconstruction.
Otitis externaInfl ammation (with or without infection) of the pinna (Figure 1) and/or ear canal (Figure 2) is generally described broadly as ‘otitis externa’. Causes include:
• non-localised infections as a result of trauma • localised infections such as furunculosis (infection
of a hair follicle) or ulceration (open sore)• herpes zoster or shingles (Figure 3)• eczema• carcinoma (cancer) of the pinna (Figure 4) • diabetes (note: one cannot successfully treat otitis
externa with uncontrolled diabetes, so always refer these patients for treatment of diabetes fi rst).
With all patients, dry mop any discharge and check whether there is a perforation of the eardrum. If there is, this is a middle ear condition (see pages 6 to 8).
If there is no perforation, manage as follows:
Redness and swelling of the pinna• A generalised redness of the pinna could be an
allergic reaction or a bacterial infection. An allergy might be associated with rhinitis and swelling in other areas of the face and body; apply a local antihistamine cream. In the case of a bacterial infection, the patient may feel unwell and have a temperature; give oral antibiotics and apply antibiotic cream.
• If you identify eczema, then treat with an antihistamine cream. If it does not respond after a week, use a steroid cream.
• A localised lesion of the pinna could be suspicious of carcinoma (a common cancer which must be treated early). Refer the patient.
• Herpes zoster should be left to resolve by itself, unless symptomatic treatment is necessary.
Redness and swelling of the ear canalThe simplest form of treatment is the following:
• Fill the ear canal with magnesium sulphate paste, using a 1 ml syringe (do not use a needle!).
• Put cotton wool over the pinna; the paste will drain out onto it.
• Clean with saline and apply paste again the next day. • Do this once a day for three to fi ve consecutive days.
If magnesium sulphate paste is not available, clean the ear with a salt solution. In all cases, if the patient does not respond to treatment after two weeks, refer.
Obstruction of the ear canalThe ear canal can be blocked by a foreign body (seed, bead, etc.) or by wax. In all cases, management will be the same:
Check if there is a perforation of the eardrumIf you cannot see the eardrum, ask the patient to breathe in, close their mouth and pinch their nostrils closed, then blow their cheeks up. If they do not feel a build-up of pressure in the ear and feel instead a sensation of air bubbles, then there is a perforation. In this case, do not syringe and refer the patient to a specialist.
If there is no perforationSyringe the ear to remove the wax or foreign body:
• Put drops of olive oil (once or twice) into the ear canal. It will coat the foreign body, which will help syringing and reduce the trauma exerted by the foreign body on the eardrum.
• Use preferably a 20 ml plastic disposable syringe with Luer lock. Use only the sheath, not the needle! If you use a metal syringe, make sure it has a rounded nozzle which cannot enter the ear canal.
• Use saline or clean salt water (put a teaspoonful of salt in a glass of normal water). Remember it should be at body temperature. Do not use normal water alone, as it would be absorbed by wax or vegetable foreign bodies (thus increasing the blockage).
• Pull back the pinna and place the tip of the syringe at the entrance of the ear canal before slowly pushing the plunger.
• Refer any embedded foreign body or wax you cannot remove.
• Check the patient’s hearing after any intervention in the ear canal.
Deformities of the external earIf there is any deformity of the pinna and/or external auditory canal, the patient may still have good hearing and would benefi t from an expert opinion.
Primary care of the external ear
External ear
Padman RatnesarConsultant Otolaryngologist and Head and Neck SurgeonBromley NHS Trust Hospitals (retired),United Kingdom
Ian MackenzieOtolaryngologist (retired)Head of WHO Collaborating Centre for the Prevention of Deafness and Hearing Impairment, Liverpool School of Tropical Medicine, United Kingdom
Ear syringing. MADAGASCAR
AND
REW
SM
ITH
Figure 3. Herpes zoster
PAD
MAN
RAT
NES
AR
Figure 4. Carcinoma of the pinna
PAD
MAN
RAT
NES
AR
Figure 1. Infection of the pinna
RICH
ARD
WA
GN
ER/G
EO
Figure 2. Infl ammation of the ear canal
RICH
ARD
WA
GN
ER/G
EO

Community Ear & Hearing Health Volume 9 • Issue 12 (2012)6
Common problems affectingthe middle earThe middle ear (see diagram on page 3) is susceptible to infl ammation and infection. Both are often associated with upper respiratory tract infections. Untreated middle ear conditions often become chronic, particularly in low-income countries.
The middle ear conditions you will encounter can be divided into four categories:
1 Serous otitis media (SOM) is a collection of fl uid in the middle ear, as a result of allergy, viral infection or dysfunction of the Eustachian tube.It is also known as ‘glue ear’.
2 Acute otitis media (AOM) is an acute (i.e. less than two weeks old) infection of the middle ear. We will distinguish, for practical reasons, between ‘AOM without a perforation’ (of the eardrum) and ‘AOM with perforation’.
3 Chronic otitis media (COM) is an infection that has been present for more than two weeks. It is characterised by an eardrum perforation with or without discharge. An untreated chronic infection could result in a permanently discharging ear (known as chronic suppurative otitis or CSOM), other complications and even death.
4 A dry perforation of the eardrum is usually the sequela of a middle ear infection (more rarely of a trauma) and is sometimes referred to as ‘inactive COM’. In this case there is a perforated eardrum without ear discharge. Sometimes the ear only discharges after being in contact with water or when the patient has an upper respiratory tract infection.
These middle ear conditions are linked to each other (see Diagram on opposite page) in the following way:
AOM can lead to a bulging eardrum due to a build-up of fl uid. If the condition is untreated, the eardrum may eventually burst to produce a perforation; this perforation relieves the pain and produces a purulent discharge.
When AOM resolves, it can result in a SOM before returning to a normal ear or it may remain as SOM unless treated.
Conversely, a SOM developing in the absence of an infection can evolve into an AOM (when fl uid is not drained properly by the Eustachian tube, this can lead to a middle ear infection).
Some cases of AOM do not heal and develop into COM, especially when repeated infections and ear discharge have occurred or there are underlying conditions affecting the Eustachian tube, such as upper respiratory tract infections, allergies, etc.
Dry perforations can result from a COM that has resolved by itself. If an infection occurs again, a dry perforation can become a COM.
Conditions affecting the middle ear: what to do at primary levelDiego J Santana-HernándezENT Surgeon CBM’s Senior Advisor for Ear and Hearing Care and Coordinator of the EHC Advisory Working Group;Santa Cruz de Tenerife, Spain
Padman RatnesarConsultant Otolaryngologist and Head and Neck SurgeonBromley NHS Trust Hospitals (retired),United Kingdom
Paddy RicardEditor of Community Ear and Hearing HealthEditorial Consultant, London, United Kingdom
Middle ear
No discharge Discharging ear
SOM* Dry perforation
AOM*without perforation
AOM* with perforation
COM*
Discharge No No No Yes, for less than2 weeks
Yes, for more than2 weeks
Pain Moderate or none No Yes, acute and with episode of fever
No (unless intracranial complication)
No (unless intracranial complication)
Perforation of the eardrum
No Yes No Yes Yes
Eardrum Dull, sucked in.No blood vessels visible in the light of the otoscope
Perforation (size may vary). Middle ear structures may be distorted
Bulging, red eardrum. Blood vessels visible in the light of the otoscope
Perforation (usually the size of a pinhole). Sometimes hard to see due to the presence of a purulent discharge
Perforation, with or without granuloma or cholesteatoma visible, usually in the upper posterior quadrant (Fig. 6)
Hearing loss Yes Yes (sometimes unnoticed)
Yes Yes Yes
Vertigo (ask ‘Do you feel dizzy?’)
No (but children may appear clumsy)
May be present Yes or No Yes or No Yes or No
*SOM = serous otitis media AOM= acute otitis media COM= chronic otitis media
Ear discharge
PIET
VAN
HAS
SELT
TABLE 1 DIAGNOSIS OF MIDDLE EAR CONDITIONS AT PRIMARY LEVEL

Community Ear & Hearing Health Volume 9 • Issue 12 (2012) 7
Important facts for primary health care personnelSOM and ‘AOM without perforation’ are reversible conditions: if they are treated early, the infl ammation resolves and hearing is restored.
Once a perforation of the eardrum has occurred (in COM and ‘AOM with perforation’), the middle ear becomes more susceptible to further infections. The hearing loss could become permanent. Ideally,a perforation of the eardrum, with or without discharge, should always be referred to an ear, nose and throat (ENT) specialist or – where such specialists are not available – to the doctor or health worker most experienced in ear matters (e.g. an experienced paediatrician).
All middle ear infections (acute or chronic) can lead to very serious complications and death, as the infection can spread from the middle ear to the mastoid bone, the brain or the facial nerve. It is important to urgently refer any suspected complication (see Box on page 8).
Many chronic middle ear conditions or complications cannot be successfully treated without the help of an ENT specialist. ENT specialists are not readily available in low- and middle-income countries, therefore intervention at primary level is crucial for prevention and early detection.
The role of a primary healthcare worker consists in:
• Detecting patients presenting with a middle ear condition.
• Managing AOM and SOM in a timely manner and following up after treatment. This will prevent the occurrence of COM, which causes irreversible damage and is very diffi cult to manage at primary level.
• Referring all cases of COM to an ENT doctor, where possible, in order to restore a clean, dry, safe ear.
• Recognising and referring very urgently all complications of middle ear conditions (see Box on page 8).
• Increasing awareness at community level of the importance of early presentation and management.
Identifying middle ear problems at primary levelBefore you examine the eardrum, certain warning signs should alert you to the fact that the middle ear could be affected:
• continuous discharge or history of continuous discharge (this indicates a chronic infection)
• any neurological sign, e.g. dizziness or lack of coordination (this may indicate potential complications)
• associated hearing loss or tinnitus.
Understanding common ear conditions and taking a good medical history will provide you with a valid working diagnosis in many cases. It is, however, the examination of the eardrum (preferably with an otoscope) that will allow you to draw diagnostic conclusions.
A normal eardrum is shiny and smooth (Figure 1).It appears translucent (semi-transparent) when you shine a light into the ear canal. An abnormal eardrum signifi es the presence of a middle ear condition.
RICH
ARD
WA
GN
ER/G
EORI
CHAR
D W
AG
NER
/GEO
Figure 1. Normal eardrum
Figure 2. ‘Sucked-in’ eardrum (serous otitis media)
RICH
ARD
WA
GN
ER/G
EORI
CHAR
D W
AG
NER
/GEO
RICH
ARD
WA
GN
ER/G
EO
Figure 3. Infl amed, bulging eardrum (AOM without perforation)
Figure 4. Dry perforation of the eardrum
Figure 5. Perforated eardrum with discharge
Table 1 will help you distinguish between different middle ear conditions at primary level. From a practical point of view, it helps to start by checking if an ear discharge is present or not:
If there is no ear dischargeIf the eardrum is abnormal and there is no discharge, you are generally faced with three possible diagnoses: SOM, AOM without perforation, or dry perforation (see Table 1).
• If there is no perforation, the eardrum appears ‘sucked in’ (Figure 2) and does not appear translucent when you shine a light into the ear canal, the patient is likely to have SOM. He/she should not report any pain, only mild to moderate hearing loss and a sensation of ‘full ear’.
• If there is no perforation, the eardrum appears to be red and bulging (Figure 3) and the patient is experiencing acute pain, this is likely to be AOM without perforation.
• If there is a perforation and there is no discharge in the ear canal or middle ear cavity, this is a dry perforation (Figure 4). The patient should not feel any pain at present and may remember one or several episodes of discharging ear, with or without pain.
The management of these situations is shown in Table 2 on page 8.
If there is an ear dischargeYou must fi rst dry mop the ear with wicks made of clean cotton material or with dry mops if you have been taught to use them (see page 4). Unless there is no other option and you are an experienced primary ear and hearing care worker, do not syringe the ear, as a discharge is likely to indicate a perforation.
If there is no perforation of the eardrum, the discharge is not due to a middle ear problem and you should treat it as otitis externa (see page 5).
If there is a perforation (Figure 5), this indicatesa middle ear infection. The patient should not be reporting any pain (if he/she does, you should treat it as a complication).
• Check for the presence of cholesteatoma (white, caulifl ower-like material in the middle ear cavity – see Figure 6) and for other complications (see Box on page 8).
• If the discharge has been present for less than two weeks, treat as AOM with perforation (see Table 2).
• If the discharge has been present for more than two weeks, treat as COM (see Table 2).
COMMON CONDITIONS AFFECTING THE MIDDLE EAR
Dry perforationChronic otitis media
(COM)
Serous otitis media(SOM)
Normal ear
Acute otitis media(AOM)

Community Ear & Hearing Health Volume 9 • Issue 12 (2012)8
Middle ear
TABLE 2 PRIMARY LEVEL MANAGEMENT OF COMMON MIDDLE EAR CONDITIONSNote: whenever you have the opportunity or facility to do so, you should also assess the patient’s hearing.
Diagnosis Objective Management
SOM* Replace the fl uid in the ear with air
• Tell the patient to breathe in, close their mouth and pinch their nostrils, then blow their cheeks up. The patient can also try blowing up a balloon (or a party blower) with their nose, one nostril at a time, whilst keeping their mouth shut.
• Advise steam inhalations, preferably with hot water and tea leaves (tea contains a mucolytic and a decongestant).
• Review after 1 to 2 weeks: the hearing and eardrum should be back to normal.• If there is no improvement after 2 weeks refer the patient to an ENT doctor.
Dry perforation*
Monitor the ear, as there is a risk of infection to the middle ear and adjoining areas
• Tell the patient to keep their ear dry and to avoid introducing anything into their ears.• Advise the patient to consult an ENT doctor to evaluate the options for repair.• If the patient does not consult an ENT doctor and the ear starts discharging, advise them
to report back.
AOM* without perforation
Prevent the eardrum from rupturing and the infection from becoming chronic. This is still a reversible condition
• Check for complications (see Box on this page).• Advise steam inhalations, preferably with hot water and tea leaves (tea contains a
mucolytic and a decongestant).• Treat the pain with paracetamol in adults or children.• Prescribe an oral antibiotic (ideally for 7 to 10 days) and, if affordable, also an antihistamine.• Review after 2 weeks to evaluate the ear and hearing.• If the eardrum ruptures, wait for 48 hours to see if it heals spontaneously. If it does not,
refer to ‘AOM with perforation’ (below).
AOM* with perforation
Prevent this infection from becoming chronic
• Check for complications (see Box on this page).• Clean up the discharge by using dry mops or wicks (see page 4). • Advise the patient to keep the ear dry and teach them to make a wick to clean any discharge.• Prescribe a systemic antibiotic (only if this has not been done before). The preferred
systemic administration route in children continues to be by mouth.• You can also prescribe antibiotic eardrops to prevent further exacerbation of the infection,
but these should only be administered after cleaning the discharge from the ear. • Review after 1 week: if there is no improvement, refer the patient to an ENT doctor and
advise them to clean the ear discharge and instil the eardrops until then.
COM* Commence treatment and try to dry up the ear (and maintain it dry) until the patient sees a specialist
• Check for complications (see Box on this page).• Clean up the discharge by using dry mops or wicks (see page 4). • You can also prescribe antibiotic eardrops to prevent further exacerbation of the infection,
but these should only be administered after cleaning the discharge from the ear. • Advise the patient to keep the ear dry. Teach the patient (or their carer) how to clean the
ear discharge with a wick before instilling any eardrops. Tell the patient to continue instilling the drops until they are seen by an ear care specialist.
• Refer to an ENT doctor who will advise on treatment, or a health worker experienced in chronic ear management if no ENT doctor is available.
Middle ear problems can lead to the following complications: cholesteatoma, facial paralysis, mastoiditis, brain abscess, meningitis. If the eardrum is abnormal and if you notice any of the following signs, refer very urgently:
• Tenderness or swelling behind the ear. This is indicative of an infection of the mastoid. • Perforation and white build-up inside the middle ear cavity (with a ‘caulifl ower’ aspect). This is
cholesteatoma (Figure 6). The patient might get mastoiditis and brain abscess.• Perforation and associated pain. This is a sign of complication inside the skull. • Facial paralysis.• Fever and headache associated with a perforated, suppurating ear.
This is a sign of impending complication inside the skull. • Any neurological sign: this means the infection has spread to the brain. These signs can be: poor
coordination, dizziness, headache, vomiting, neck stiffness, drowsiness, or loss of consciousness.
CHECKING FOR COMPLICATIONS ASSOCIATED WITH MIDDLE EAR CONDITIONS
RICH
ARD
WA
GN
ER/G
EO
Figure 6. Cholesteatoma (visible through a perforation in the top left quadrant)
*SOM = serous otitis media AOM= acute otitis media COM= chronic otitis media

Community Ear & Hearing Health Volume 9 • Issue 12 (2012) 9
Hearing problem No hearing problem
Ear disease
• If the patient suddenly developed a severe hearing loss in the past 48 hours, REFER URGENTLY to an ear specialist (see page 12).
• If the patient has any of the ‘red fl ag’ conditions mentioned on page 12 of this issue, REFER URGENTLY.
• In all other cases, the ear disease should always be treated fi rst. TREAT or REFER to an ear specialist. The hearing loss can be attended to once the patient’s ear disease has been treated.
• If the patient has any of the ‘red fl ag’ conditions mentioned on page 12, REFER URGENTLY.
• In all other cases TREAT the ear disease if you can or REFER to an ear specialist if you cannot.
No ear disease
• If the patient suddenly developed a severe hearing loss in the past 48 hours, REFER URGENTLY to an ear specialist (see page 12).
• In all other cases, REFER to a hearing specialist.
• No further action necessary.
Establishing a referral networkWhen you work in a health centre at community level, most, if not all, of your referrals will be to a local district hospital or clinic. The places to refer patients and the procedures to do it may be well established in your local health system. However, if this is not the case, you may fi nd it very helpful to establish your own ‘referral network’:
• Identify the ear and hearing specialist facilities to which you will refer patients. Find out their location, what their services and capabilities are, how much they charge for their services, as well as their opening hours.
• Check in advance (preferably in person) that these specialist facilities are willing to accept patients referred from your centre.
• If you can, print practical information sheets for patients about the clinic or hospital to which you are referring them.
• Always give your patient a brief, signed referral note (see Box left) to be taken to the health workerhe/she is being referred to. Having blank notes ready in your offi ce considerably simplifi es and speeds up the process.
Whom should you refer to?First you must decide whether the patient needs a referral or whether you can treat the patient yourself. You should then identify which type of specialist can best deal with the patient’s problem. Page 12 of this issue and Table 1 below should help you make a decision.
A ‘hearing specialist’, as mentioned in the table,is someone who can assess a patient’s hearing and recommend fi tting a hearing aid. An ‘ear specialist’is someone who can treat an ear disease,e.g. a discharging ear.
In countries where there is no shortage of personnel, ‘hearing specialists’ tend to be ‘audiologists’ or ‘audiology technicians’, and ‘ear specialists’ tend tobe ENT doctors (ear, nose and throat), otologists or otorhinolaryngologists. However, in your setting,
there may be other types of personnel, such as Medical or Clinical Offi cers, who have been trained in ear and hearing health.
Before the patient departs from your clinic1 Explain to the patient how quickly they need to
take up the referral: immediately, soon, or when it is convenient for them.
2 Discuss any practical concerns that your patient may have and try to fi nd solutions before the patient leaves. These concerns are likely to infl uence the patient’s decision to take up the referral. Consider the following:
! Transport to and from the clinic: does the patient have their own transport or that of a parent or relative or friend? Does the patient need to go by ambulance or can they go by taxi or bus?
! Accommodation (if the patient stays overnight) ! Costs: can the patient afford to pay for travel, accommodation and referral consultation and treatment, if this is not free? If needed, are there ways to subsidise these costs?
3 Make an appointment for the patient to come and see you on their return from the referral visit. The patient should bring a letter to you from the centre to which you made the referral (or the feedback section of your referral letter).
How to refer a patient: practical tips
• Your contact details (including phone number)
• Patient’s name& contact details
• Date of birth • Name & contact details of carer (if the patient is a child)
• Reason for referral • Why the patient came to your health centre
• What you have observed (include diagnosis if you made one)
• Tests performed & results (if relevant)
• Treatment given to patient
• Other relevant information: e.g. health conditions, medication, hearing aids, etc.
Feedback section(to be brought back by the patient):
• Name of specialist • Examination performed
• Diagnosis • Treatment recommended
• Requests for treatment, management or follow-up by the primary health centre
WHAT TO INCLUDE IN A REFERRAL LETTER
TABLE 1 MAKING A REFERRAL DECISION
Andrew SmithHonorary Professor International Centre for Evidence in Disability, London School of Hygiene and Tropical Medicine,United Kingdom
Referral
People waiting to be seen at a village primary healthcare centre. MADAGASCAR
AND
REW
SM
ITH

Community Ear & Hearing Health Volume 9 • Issue 12 (2012)10
Why good communication is important• to provide reassurance, as many patients in clinics
or hospitals feel anxious• to create a relationship based on trust between
healthcare providers and patients • to make a more accurate diagnosis of the patient’s
illness• to ensure that the patient understands what
treatment is being offered• to ensure that instructions given are correctly
understood by the patient• to improve compliance with treatment or referral• to improve the credibility of healthcare workers
and the way they are perceived by patients.
Barriers to communication Deaf or hearing-impaired patients, with or without hearing instruments, may communicate in a variety of ways with health personnel: some patients speak and speech read or lip read, some use sign language or communicate by writing notes, and some bring someone with them to interpret.
Undesirable misunderstandings are more common when communication barriers exist. For those who are hearing-impaired, the main barriers are social rather than physical. People with hearing impairment are not always included in social situations and the attitude adopted towards them by others, including by health personnel, may hinder communication in different ways.
Many healthcare providers believe that it is diffi cult and time-consuming to communicate with patients who are hearing-impaired. Sign language interpreters are diffi cult to fi nd, even more so interpreters who are culturally and personally sensitive.
Patients with a hearing impairment may feel discouraged that the practitioner is not directly interacting with them (e.g. talking about them rather than to them). They may not feel comfortable enough to express their needs if staff are not aware of them. For example, if the consultation room does not offer privacy, asking health personnel to speak loudly can be embarrassing when you do not want others to know about your condition.
Patients with a hearing impairment have the same rights to full information as other patients, yet they can face prolonged or unnecessary illnesses due to inadequate communication with their healthcare providers. This article suggests simple steps to improve communication with hearing-impaired persons.
In the waiting room and reception areaWaiting areas in clinics can be very busy and noisy places. Patients with a very severe or profound hearing loss will not hear shouted instructions or staff calling out their name. Those with moderate hearing loss can also have diffi culty if the waiting room is very noisy. Patients wearing a hearing aid may need to turn the volume down to avoid discomfort and so will hear less well than usual.
In a primary healthcare facility, there is likely to be a mix of all sorts of patients, some of whom will have a hearing impairment. It is helpful to make the following general provisions:
• In the waiting room, in addition to calling out the patient’s name when it is his/her turn to be seen, use a number system or a sign (e.g. a board with the patient’s name written on it).
Valerie E NewtonProfessor Emerita in Audiological MedicineUniversity of Manchester,United Kingdom
Seema Rupani ShahAudiological ScientistPO Box 20730-00202, Nairobi, Kenya
Examination of a deaf child in the presenceof an interpreter. The doctor (right) is facing his young patient and has a pen and paperat hand. KENYA
SEEM
A RU
PAN
I SH
AH
Improving communication with patients who have a hearing impairment
• A hearing impairment is often invisible. Please inform us if you have a hearing loss.
• Tell the doctor how you prefer to communicate and we will try to help as much as possible.
• Please wear your hearing aids if you have them and fi nd them helpful.
• We can provide you with a sign language interpreter.*
• Do not hesitate to ask for repetition if you do not understand.
*If this service is available in your health facility
INSTRUCTIONS TO HEARING-IMPAIRED PERSONS FOR COMMUNICATINGWITH THEIR HEALTH PROFESSIONAL
Communication

Community Ear & Hearing Health Volume 9 • Issue 12 (2012) 11
• Put the most important information (e.g. consultation fees) in writing, on clearly displayed signs.
• Put up a sign in your waiting room for patients with hearing impairment, indicating how they may contribute to improved communication (see Box on page 10) and whether a sign language interpreter is available.
• If a patient with hearing impairment calls in advance to make an appointment (or if someone else calls on his/her behalf), ask how the patient prefers to communicate and whether a sign language interpreter is needed.
• If you know a patient is deaf or hearing-impaired, make sure the consultation takes place in a suitable setting (see next section).
During a clinical appointment Improving the way you communicateThe Box on the right offers suggestions to improve communication with a hearing-impaired person at a clinical appointment. Keep in mind that what matters is not what you say, but what the patient understands.
Understanding the responses ofa hearing-impaired personIf a patient is able to speak and presents with mild hearing loss, then his/her speech may be normal. The speech of patients with moderate to severe hearing losses may be diffi cult to understand. The ends of words may be left out in their speech, as well as the small joining words, e.g. ‘and’, ‘to’ and ‘but’.
It is important to know what a patient is saying in order to communicate effectively.
If a family member has accompanied the patient, this person may be able to help – as long as the patient agrees to it. However, do not forget that you should still be communicating primarily with the patient and not the person accompanying him/her.
Sometimes patients have reservations about being asked questions in front of family members. This can be the case whether the patient speaks or uses sign language. Patients with a severe hearing loss may prefer to be seen alone and communicate in writing during the consultation.
Having a member of the clinic staff trained as asign language interpreter can be very useful. It will help you understand the patient’s responses with greater accuracy and will help keep the patient’s information private.
If you are not sure you have understood the patient’s responses, ask again.
In the waiting room of any primary health centre, some patients are likely to have a hearing impairment. IVORY COAST
COMMUNICATING WITH A HEARING-IMPAIRED PERSONAT A CLINICAL APPOINTMENT
1 Make adequate provisions in the consultation room• Give the patient privacy: they should be able to ask you to raise your
voice without fear that others will hear about their medical history.
• Minimise distractions. This is even more important if your patient is a child.
• Reduce background noise as much as possible.
• Ensure the room is well lit, so that the patient can see your face or any written information they may be given.
• Ask the patient to wear their hearing aids (if they have them and fi nd them helpful) and sit closer to them than you would to another patient.
• If possible, have a helper in the room of the same gender as the patient.
• When adult patients have come accompanied, always ask them before you start if they would prefer to be alone with health personnel in the consultation room. Do not wait until the questions become uncomfortable for the patient.
2 Remember that your face is an essential communication tool• Face the patient, not their interpreter or carer.
• Remove your mask and face shield.
• Do not have anything between your lips (cigarette, pen, etc.) or in your mouth (chewing gum, sweets, etc.) as this can distort lip movement when speaking. Avoid placing your hand or an object in front of your mouth when talking.
• Have the light on your face rather than on the person you are talking to. This makes it easier for them to read facial expressions and to lip read.
• Support your speech with facial expression where you can, e.g. look happy if you are giving good news and sad if you are giving bad news.
• When signing, hold your hands up at chest level to enable both your face and hands to be clearly seen.
• Understand and use the local culture of gestures, expressions and accepted physical contact (or absence of it).
3 Ensure that you speak effectively• Speak normally, not too fast or too slowly. Certain sounds can be
distorted or lost if speech is rushed or slowed down too much.
• Use short, simple sentences.
• Do not exaggerate your speech or lip movements.
• Ask questions if you are not sure you understand what the patient is saying.
• Patients tend to agree with their health workers, sometimes without understanding what has been said to them. After every important point or message, ask the patient if he/she has understood you and, if necessary, ask him/her to repeat the message or instructions back to you (this is especially important if the patient is unaccompanied).
4 Use other means of communication, e.g. writing and signing• If the patient can sign, use an interpreter. If at all possible, learn the local
sign language yourself.
• Be prepared to write down any questions or answers and give the hearing-impaired person the opportunity to do the same if necessary.
• Write down important information to give to the patient, e.g. instructions for taking medicines.
• Use pictures and drawings to ensure that the patient understands your instructions.
FERD
INAN
D A
MA

12 Community Ear & Hearing Health Volume 9 • Issue 12 (2012)
&Community
Ear HearingHealth
CLI
NIC
AL
SYM
PTO
MS
& S
IGN
SRE
ASO
N F
OR
URG
ENT
REFE
RRA
LC
LIN
IC O
R SP
ECIA
LIST
YO
U S
HO
ULD
REF
ER T
O
Acut
e in
fect
ion
of th
e pi
nna
This
may
indi
cate
an
unde
rlyin
g co
nditi
on s
uch
as d
iabe
tes
ENT*
Clin
ic/O
tolo
gist
Acut
e tr
aum
a of
the
pinn
a or
ear
can
alEx
pose
d ca
rtila
ge n
eeds
to b
e ad
equa
tely
repa
ired
by a
n ex
pert
he
alth
offi
cer t
o av
oid
perm
anen
t def
orm
ity o
r ser
ious
infe
ctio
n
Trau
ma
to th
e bo
ny e
ar c
anal
may
indi
cate
an
unde
rlyin
g sk
ull o
r he
ad tr
aum
a
ENT
Clin
ic/O
tolo
gist
Cons
ider
refe
rrin
g to
:Pl
astic
sur
geon
and
/or
Neu
rosu
rgeo
n
Fore
ign
bodi
es th
at a
re a
live
insi
de th
e ea
r can
alAl
ive
fore
ign
bodi
es (i
nsec
ts) r
equi
re e
mer
genc
y at
tent
ion,
as
they
m
ay p
erfo
rate
the
eard
rum
or g
o th
roug
h an
exi
stin
g pe
rfor
atio
n an
d ca
use
a co
mpl
icat
ion
ENT
Clin
ic/O
tolo
gist
or
Hos
pita
l em
erge
ncy
clin
ic
Perf
orat
ed e
ardr
um a
nd a
ssoc
iate
d pa
in (w
ith o
r with
out b
lood
y or
oth
er e
ar d
isch
arge
)Th
is m
ay b
e a
sign
of i
ntra
cran
ial c
ompl
icat
ion
(pro
blem
insi
deth
e sk
ull)
ENT
Clin
ic/O
tolo
gist
or
Hos
pita
l em
erge
ncy
clin
ic
Eard
rum
per
fora
tion
asso
ciat
ed w
ith a
whi
te s
ubst
ance
(cau
lifl o
wer
-like
) ins
ide
the
mid
dle
ear
This
is li
kely
to b
e ch
oles
teat
oma.
The
pat
ient
mig
ht g
et h
earin
g lo
ss, m
asto
iditi
s, fa
cial
pal
sy o
r bra
in a
bsce
ssEN
T Cl
inic
/Oto
logi
st
Bad-
smel
ling
ear d
isch
arge
, with
feve
r and
hea
dach
eTh
is m
ay in
dica
te im
pend
ing
intr
acra
nial
infe
ctio
n (e
.g. m
enin
gitis
or
bra
in a
bsce
ss)
ENT
Clin
ic/O
tolo
gist
or
Hos
pita
l em
erge
ncy
clin
ic
Abno
rmal
ear
drum
with
tend
erne
ss, s
wel
ling
or fi
stul
a be
hind
the
ear
This
may
be
due
to a
n in
fect
ion
of th
e m
asto
id (a
cute
mas
toid
itis
or p
osta
uric
ular
abs
cess
)EN
T Cl
inic
/Oto
logi
st
Disc
harg
e of
the
ear a
nd/o
r sud
den
onse
t sev
ere
hear
ing
loss
asso
ciat
ed w
ith o
ne o
r mor
e of
the
follo
win
g:
• he
adac
he •
fev
er •
diz
zine
ss •
tin
nitu
s (p
ersi
sten
t buz
zing
or r
ingi
ng in
the
ear)
• pa
infu
l sw
ellin
g be
hind
the
ear
• fa
cial
par
alys
is •
ata
xia
(uns
tead
y w
alki
ng) o
r poo
r coo
rdin
atio
n •
alte
red
cons
ciou
snes
s (‘n
ot th
eir u
sual
sel
f’) o
r los
s of
con
scio
usne
ss (f
aint
ing)
This
may
be
a si
gn o
f int
racr
ania
l com
plic
atio
n (e
.g. m
enin
gitis
or
brai
n ab
sces
s or
tum
our)
EN
T Cl
inic
/Oto
logi
st o
r H
ospi
tal e
mer
genc
y cl
inic
Sudd
en s
ever
e he
arin
g lo
ssRe
fer w
ithin
48
hour
s of
ons
et if
ther
e is
any
cha
nce
of e
valu
atio
n by
an
ENT
doct
or a
nd im
med
iate
com
men
cem
ent o
f med
ical t
reat
men
t, es
peci
ally
in c
ases
whe
re th
e su
dden
hea
ring
loss
is a
ssoc
iate
d w
ith n
oise
trau
ma
or a
sud
den
prob
lem
with
blo
od c
ircul
atio
n
ENT
Clin
ic/O
tolo
gist
*ENT = Ear, Nose and Throat
Figu
re 5
.C
hole
stea
tom
aFi
gure
1. A
cute
in
fect
ion
of t
he p
inna
Figu
re 2
. Acu
te
trau
ma
of t
he p
inna
Figu
re 3
. Liv
e in
sect
in
the
ear
can
alFi
gure
4. L
arge
per
fo-
rati
on o
f the
ear
drum
Figu
re 6
.Ea
r di
scha
rge
Figu
re 7
. Acu
te
mas
toid
itis
Figu
re 8
. Pos
taur
icul
ar
swel
ling
Figu
re 9
. Fac
ial p
alsy
(p
aral
ysis
)
RICHARD WAGNER/GEO
RICHARD WAGNER/GEO
RICHARD WAGNER/GEO
RICHARD WAGNER/GEO
RICHARD WAGNER/GEO
PIET VAN HASSELT
RICHARD WAGNER/GEO
RICHARD WAGNER/GEO
RICHARD WAGNER/GEO
‘Red
fl ag
’ sit
uati
ons
at p
rim
ary
leve
lRe
fer p
atie
nts
urge
ntly
(on
the
sam
e da
y) in
all
of t
he fo
llow
ing
situ
atio
ns: