Embed Size (px)
Citation preview

Common Suspected Infections: Tools to Improve Communication
and Decision Making
www.ahrq.gov/NH_ASPGuide ● May 2014 AHRQ Pub. No. AHRQ 14-0011-6-EF
Quality Improvement for Antibiotic Prescribing
1. Problems with taking antibiotics
2. Drug resistance and lack of new antibiotics
3. Approaches to antimicrobial stewardship
4. Description of the tools and how to use them
5. Additional information about suspected infections

Problems with Taking Antibiotics
GI: Nausea, vomiting, diarrhea Secondary infections: C difficile, yeast Allergic reactions: rash, anaphylaxis Drug interactions: coumadin, glipizide If on fluoroquinolones tendon rupture Dehydration falls Photosensitivity skin reaction Resistant bacteria

Antibiotic Resistance
Multi-drug resistance is increasingly common
• Streptococcus pneumoniae• Staphylococcus aureus• Enterococcus, E coli, Pseudomonas
aeruginosa• Acinetobacter baumannii • Tuberculosis

Resistant Strains Spread Rapidly
0
10
20
30
40
50
60
1980 1985 1990 1995 2000 2003
MRSA
VRE
FQRP
Per
cent
of I
sola
tes
Source: Infectious Diseases Society of America http://www.idsociety.org/10x.20.htm

Few New Antibiotics
Source: Boucher, Talbot, Benjamin, et al., 10 × '20 Progress—Development of new drugs active against gram-negative bacilli: an update from the Infectious Diseases Society of America. Clin Infect Dis. 2013; 1-10.
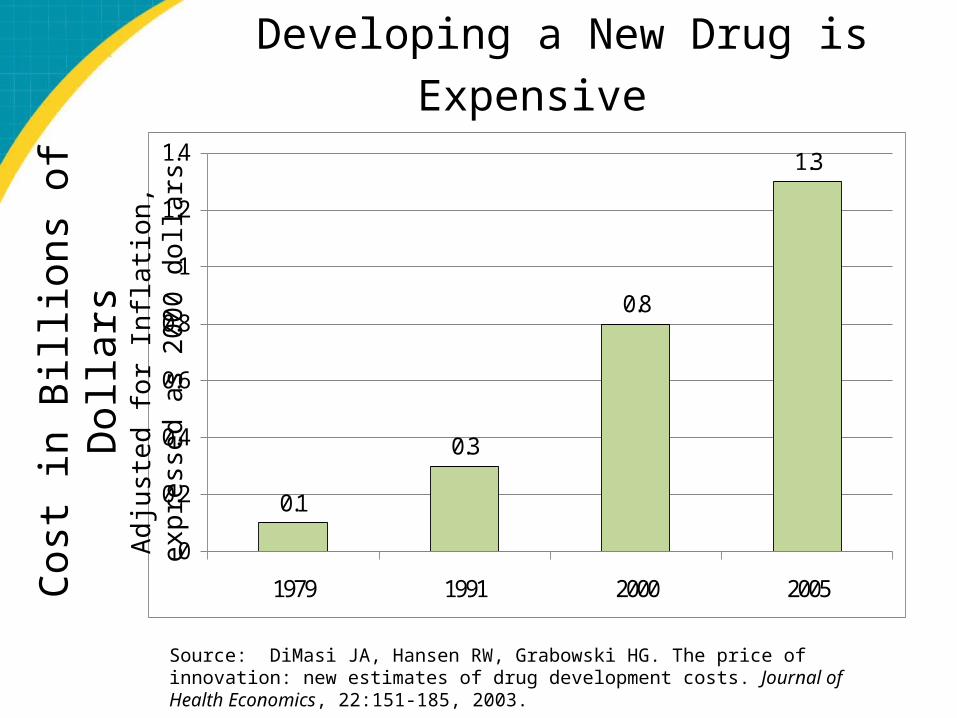
Developing a New Drug is Expensive
0.1
0.3
0.8
1.3
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1979 1991 2000 2005Cos
t in
Bill
ions
of D
olla
rsA
dju
ste
d fo
r In
flatio
n,
exp
ress
ed
as
20
00 d
olla
rs
Source: DiMasi JA, Hansen RW, Grabowski HG. The price of innovation: new estimates of drug development costs. Journal of Health Economics, 22:151-185, 2003.

Consequences
World Health Organization:
“Antibiotic resistance is one of the three biggest threats to
human health”

Indications of Overuse
Between 25 to 75 percent of antibiotic prescriptions in nursing homes do not meet clinical guidelines for prescribing.
Example: One-third of residents receiving antibiotics for UTI are being treated for asymptomatic bacteriuria.
Journal of General Internal Medicine. 16(6): 376-383, 2001.
Approaches to Antimicrobial Stewardship
Encourage research into new classes of antibiotics
Reduce overuse in key areas• Populations with high prescription rates
Respiratory infections in children Long-term care populations
• Developing countries• Veterinary use, food industry, and
aquaculture

Goal: Better Informed Prescribing
Components of the Communication and Decision Making for Four Infections
1. Evidence-based communication between nurses and prescribers using a Medical Care Referral Form (MCRF)
2. Nurse vigilance to 12 common situations and infection control practices (pocket cards)
3. Prescriber training
4. “Be Smart About Antibiotics” resident and family handout
5. Quality improvement practices

Evidence-based Communication Between Nurses and Prescribers:
Using a Medical Care Referral Form (MCRF)
Development and Rationale for Use:Medical Care Referral Form (MCRF)
Researchers:Reviewed prescribing criteria from consensus conference Reviewed prescribing in six nursing homes and extent to which they met components of criteriaDeveloped the MCRF to assure attention to and communication of key signs and symptoms

The Medical Care Referral Form (MCRF)

Medical Care Referral Form (MCRF)
Designed to facilitate evidence-based communication between nurses and prescribers
Intended to be used for ALL situations when a resident has a new problem and infection may be suspected
In those instances, should be used for ALL referrals to medical care providers, including transfer to ED or hospital

MCRF: Components
Description of current problem Vital signs Usual cognitive function Recent/current health status (including falls)
• Falls, minor injury: require on-site first aid treatment (dressing, ice pack, pain medication)
• Falls, serious injury: require stitches, immobilization, ED assessment or treatment, surgery, hospitalization
Medical history (including AD for no antibiotics) Suspected infections – complete only relevant section Use of question mark (“?”)
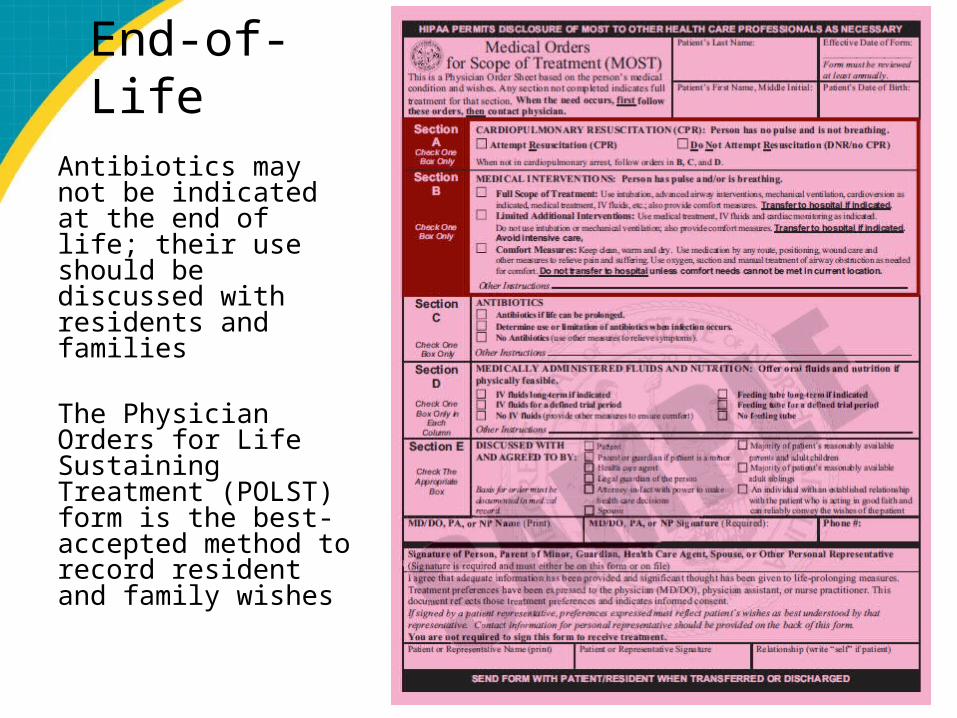
End-of-LifeAntibiotics may not be indicated at the end of life; their use should be discussed with residents and families The Physician Orders for Life Sustaining Treatment (POLST) form is the best-accepted method to record resident and family wishes
Twelve Common Situations and Infection Control
Practices and the Pocket Card
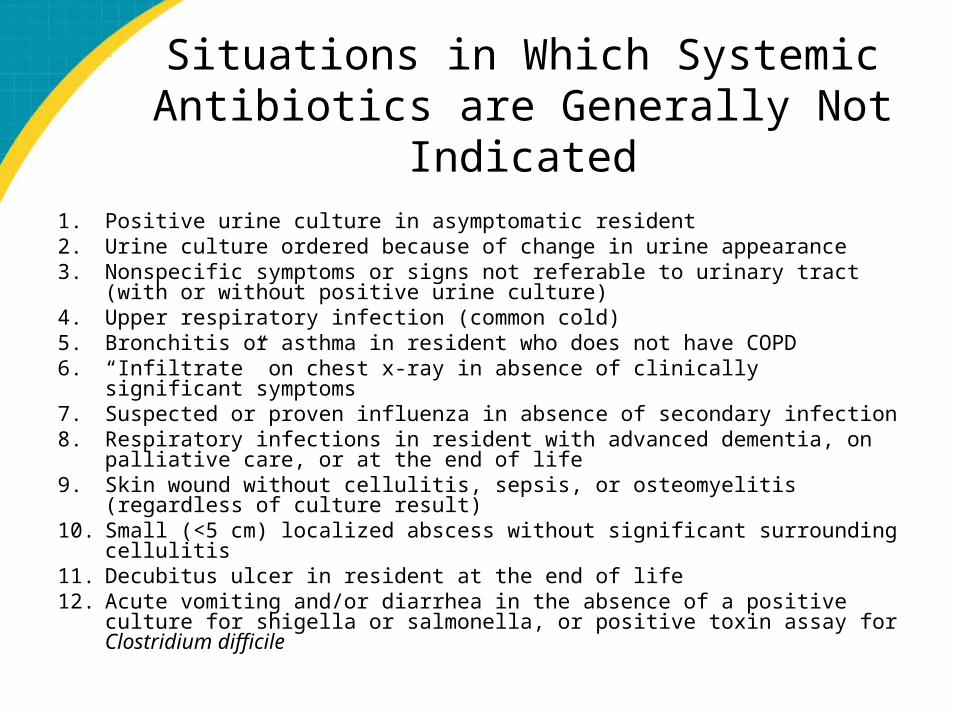
Situations in Which Systemic Antibiotics are Generally Not Indicated
1. Positive urine culture in asymptomatic resident2. Urine culture ordered because of change in urine appearance3. Nonspecific symptoms or signs not referable to urinary tract (with or
without positive urine culture)4. Upper respiratory infection (common cold)5. Bronchitis or asthma in resident who does not have COPD6. “Infiltrate” on chest x-ray in absence of clinically significant symptoms7. Suspected or proven influenza in absence of secondary infection8. Respiratory infections in resident with advanced dementia, on palliative
care, or at the end of life9. Skin wound without cellulitis, sepsis, or osteomyelitis (regardless of culture
result)10. Small (<5 cm) localized abscess without significant surrounding cellulitis11. Decubitus ulcer in resident at the end of life12. Acute vomiting and/or diarrhea in the absence of a positive culture for
shigella or salmonella, or positive toxin assay for Clostridium difficile
Infection Control Guidelines
Vancomycin-resistant enterococci Clostridium difficile Methicillin-resistant
Staphylococcus aureus
Pocket Card
Pocket Card

“Be Smart About
Antibiotics” Handout
“Be Smart About Antibiotics” Handout
“Be Smart about Antibiotics” Handout
Distributed to current and new residents When hospice is considered Primary purposes
• educate about instances when antibiotics may not be indicated
• promote shared decision making

Quality Improvement Practices

Monthly Meetings
Be held monthly to review progress All individuals responsible for the QI
program should attend the meetings

Additional Information AboutInfections and Symptom
Management
Fever and Older Adults
Do you know why a resident DOES NOT need a fever to have an infection?
• Fever may be absent in 30-50% of older adults with serious infections
• Factors such as chronic diseases, medications, and time of day can affect an older person’s temperature
Suspected UTICloudy or Smelly Urine:
To Culture or Not?
Urine changes have many causes• foul-smelling urine may be caused by dehydration,
hygiene, medication, diet, or infection Will overdiagnose infection in one-third of cases Improved toileting and fluid intake is often better
treatment than antibiotics; hydration and perineal hygiene can prevent recurrence
Culture should be ordered only if new urinary symptoms are present
*Archives of Internal Medicine. 160: 678-682, 2000.

When to Order a Urine CultureDiagnostic Pathway
Fever of >37.9°C (100 °F) or 1.5°C (2.4 °F) increase above baseline, on 2 occasions over the last 12 h?
2 or more symptoms/signsof other infection?
Do not orderurine culture
YES
Order urine culture if you observe 1 or more:
•New onset burning urination (dysuria)•Urinary catheter•New or worsening:oUrgencyoFrequencyoFlank painoGross hematuriaoUrinary incontinenceoSuprapubic pain
NO
YES
Order urine culture if you observe 2 or more:
•New onset burning urination (dysuria)•New or worsening:oUrgencyoFrequencyoFlank painoGross hematuriaoUrinary incontinenceoSuprapubic pain
NO
Order urine culture if you observe 1 or more:•New CVA tenderness•Shaking chills (rigors)•New onset of delirium
Urinary catheter?

Suspected Respiratory Infection
Symptomatic care:• Monitor vital signs• Encourage fluid intake• Acetaminophen 650 mg q 6 hrs PRN for fever
and pain reduction• Nasal saline 2 sprays to each nostril PRN for
nasal congestion• Guaifenesin 2 teaspoons every 4 hours as
needed for cough• Antihistamines, especially Benadryl, should
be AVOIDED

Suspected Skin/Soft Tissue Infection
Appropriate care:• Mobility – encourage mobility (passive
or active)• Acetaminophen 650 mg as needed or
prior to cleaning/dressing changes• Cleanse wounds with each dressing
change with saline or warm water; do not use antiseptic cleansers
• Apply dressing as needed