Embed Size (px)
Citation preview

Common learning issuesFirst case block

echocardiography• Normal findings: normal position, size and movement of
cardiac valves and heart muscle wall, normal directional flow of blood within heart chambers
• Indications: evaluate heart wall motion (measure of heart wall function) to detect valvular disease, evaluate the heart during stress testing and identify and quantify pericardial fluid
• Non-invasive ultrasound to evaluate structure and function of the heart
• Uses m-mode recordings, 2D and 3D images, Doppler• M-mode 1D recording of amplitude and rate of motion of
heart structures in real time

echocardiography• 2D spatial relationships of the heart• 3D adds images of heart wall and valves• Color flow doppler: direction and velocity of blood flow within the heart
and great vessels alter ultrasound frequency. Altered direction and velocity can be coded as shades of colors. Assessing flow across prosthetic valves and regurgitant or narrow valves
• Diagnose effusion, valvular heart disease, subaortic stenosis, myocardial wall abnormalities, infarction, aneurysm and cardiac tumors, ASD and VSD
• Used during exercise stress tests to diagnose areas of hypokinetic myocardium
• Perflutren (DEFINITY or Optison) opacifying agent enhancing endocardial borders
• Interfering factors: patients with COPD because of the substantial amount of air between heart and chest cavity; obese patients space between heart and transducer is enlarged
Cardiac catheterization• Normal findings: normal heart muscle motion, normal and
patent coronary arteries, normal great vessels, and normal intracardiac pressure and volume
• Indications:• Visualize heart chambers, arteries, and great vessels• Evaluate chest pain• Locate region of occlusion in positive stress test• Determine effects of valvular disease• Right heart measures CO, and PE

catheterization• Test explanation:
• Catheter passed into heart through peripheral vein or artery (left heart)• Pressures are recorded and radiographic dyes are injected measure CO • Identify locate, and quantify congenital valvular or septal defects• Evaluate severity of acquired defects• Presence and degree of abnormalities such as transposition of great vessels,
patent ductus arteriosus and anomalous venous return to the heart• Evaluate success of previous cardiac surgery or balloon angio• Evaluate cardiac muscle function• Identify and quantify ventricular aneurysms • Locate acquired diseases of the great vessels i.e. atherosclerosis and aneurysms• Monitor right sided heart pressure and pulmonary wedge pressures, measure
CO • Dilate stenotic coronary arteries, place stent or laser atherectomy• Femoral vein and artery• Blood is sampled for analysis of oxygen content• Dye allows for visualization of heart chambers, valves, and coronary arteries

Reading frontal chest x-ray• Designed to look at lungs, not trauma to the ribs etc.• R marker should be on your left side• Glance over the image for any obvious abnormality always look at your four corners• Anterior posterior and posteroanterior• Start at top and make sure trachea is midline• Move to heart, transverse diameter of cardiac silhouette should not be more than 50%
transverse diameter of thoracic cage• Greater the distance between and object and film, the greater the magnification• Right heart convex, left cardiac border at the top should be concave• Left ventricle makes up left heart• SVC makes straight right border• In enlargement left superior border becomes convex• Left enlargement cardiac apex moves down and out• Right enlarges right border is more protuberant• Left and right pulmonary arteries form hilar shadows, left should be more cephalad• Aorta forms knob• Aortopulmonary window between knob and pulmonary artery shadow; should be
concave or suspect mass or adenopathy

Frontal chest X-ray• Mediastinum shadow is caused by great vessels and vascular
pedicle• Pedicle extends from thoracic inlet to base of heart; right
border is SVC left is aortic knob• Divide lungs into horizontal thirds• Domed diaphragm with right side higher than left• Lateral costophrenic angles should be sharp and acute• Look at lower cervical spine and ribs• Ribs we see are posterior arcs anterior ribs are angled
downward
Lateral radiograph• Right ventricle is anterior border• Left ventricle is inferior-posterior cardiac border• Left atrium forms superior-posterior cardiac border• IVC can be seen as it enters from abdomen• If left ventricle is 2 cm or more posterior to IVC then it is
enlarged• Evaluating hila left is posterior to line drawn down from
tracheal air column and one third the size of the right• Silhouette sign when two objects of similar density are in
direct juxtaposition interface or borders are lost

TSH aka thyrotropin• Used to diagnose primarily hypothyroidism and to differentiate it from
secondary (pituitary) and tertiary (hypothalamus)• TSH is stimulated by hypothalamic TRH• Low levels of T3 and T4 are underlying stimuli for TRH and TSH • A compensatory elevation of TRH and TSH can occur with primary
hypothyroidism such as surgical or radioactive ablation, burned out thyroiditis, agenesis, idiopathic, congenital cretinism or antithyroid meds
• Function of pituitary or hypothalamus is faulty because of a tumor, trauma, or infarction so T3 and T4 are low along with TRH and TSH
• TSH test monitors exogenous thyroid replacement or suppression• Thyroid replacement goal is to keep TSH in low normal range• Thyroid suppression keeps TSH low used to diminish size of large goiter• Detect primary hypothyroidism in newborns with low T4• Low T4 and normal or elevated TSH is thyroid• Low T4 and low TSH means pituitary • Interfering factors: radioisotope administration, severe illness, diurnal, drugs like
antithyroid, lithium, potassium iodide, and TSH injection

Free thyroxine index
• Evaluate thyroid function• Corrects for changes in thyroid hormone binding serum proteins that can
affect T4 • Diagnose hypo and hyperthyroidism• Measures the amount of free thyroxine T4 which is only 1% unbound goes
into cells and is activated • Not affected by TBG abnormalities so it correlates more closely to hormonal
status than total T4 and T3 • If TBG is increased the T3 uptake decreases and correcs for increased T4
associated with increased TBG• If TBG is normal and T4 is elevated FT4 will be elevated indicating true
hyperthyroidism• Low FT4 indicates hypothyroidism• Increased levels primary hyperthyroidism, thyroiditis, facticious
hyperthyroidism, struma ovarii• Decreased: hypo, pituitary insufficiency, hypothalamic, iodine insufficiency

Thyroxine total
• Diagnose thyroid function and to monitor replacement and suppressive therapy• Makes up most of what we call thyroid hormone and it is bound to protein • Measured by radioimmunoassay or enzyme linked immunosorbent assay techniques• TSH stimulates thyroid to secrete thyroid hormone high levels of hormone inhibit
TRH• Serum test indicates all T4 high levels indicate hyperthyroid, low is hypothyroid• TBG affects results• Interfering factors: increased after iodinated contrast x-ray, pregnancy causes
increased levels, amphetamines, clofibrate, estrogens, heroin, iodinated contrast media, iodine, methadone, and oral contraceptives increase
• Decrease levels: anabolic steroids, androgens, anti-inflammatory drugs, antithyroid drugs, barbituates, furosemide, nonsteroidal lithium phenytoin, propranolol, propylthiouracil
• High: hyper, thyroiditis, dysalbuminemic, hyperthyroxemia, facticious hyperthyroidism, struma ovarii, TBG increase
• Low: hypo, pituitary insufficiency, hypothalamic failure, protein malnutrition and other protein depleted states, iodine insufficiency, non-thyroid illness
Cardiac stress test• Normal finding is that patient is able to maintain and obtain
maximal heart rate of 85% for predicted age and gender with no cardiac symptoms or EKG change
• Evaluate chest pain in a patient with suspected coronary artery disease
• Determine limits of safe exercise during cardiac rehab or assist patients with cardiac disease in maintaining good physical fitness
• Detect labile or exercise related hypertension• Detect intermittent claudication in patients with suspected
vascular occlusive disease in extremeties• Evaluate effectiveness of treatment in patients taking antianginal
or antiarrhythmics• Evaluate effectiveness of cardiac intervention

Cardiac stress test• Provides info about cardiac function• Heart is stressed and then evaluated• Changes indicating ischemia point to coronary occlusion• EKG, HR, and BP are monitored and patient pedals or walks on a treadmill
increasing pace or resistance to stress heart to get heart to target heart rate• Occluded arteries will be unable to meet heart’s increased demand for blood
during the test• Chemical stress testing used when unable to exercise• Dippyridamole causes steal from ischemic areas due to its powerful vasodilation• Dobutamine can also stress the heart • Contraindications: people with unstable angina, patients with severe aortic
valvular heart disease, those who cannot participate in exercise program because of lung or motor function, patients with MI, patients with severe congestive heart failure
• Potential issues: MI, fainting, sever angina, fatal cardiac arrhythmias• Indicates angina, intermittent claudication, abnormal rhythms, coronary artery
occlusive

urinalysis
• Normal: • Appearance: clear• Color: amber yellow• Odor: aromatic• pH 4.6-8• Protein 0-8 mg/dL• Nitrites none• Crystals none• Bilirubin none• Urobilinogen 0.1-1• Casts none• Glucose none• WBC 0-4 low power field• RBC <2• RBC casts none• Specific gravity 1.005-1.030• Leukocyte esterase negative• Ketones none
Ua• Indications: used as part of routine diagnostic and screening
evaluations can give info on kidneys, performed on essentially everyone
• Test explanation: divided one is sent to UA the other half is cultured
• Lab exam:• Color: clear, cloudy indicates WBC, RBC or bacteria, color
indicates concentration of urine and varies specific gravity, abnormal color may indicate bleeding from kidney (dark red) bleeding from lower UT (bright red)
• Dark yellow indicates urobilinogen or bilirubin• Pseudomonas could cause green urine

UA• Odor:
• Diabetics have strong, sweet smell of acetone• UTI causes foul odor• Fecal odor could be a fistula
• pH• Alkaline indicates alkalemia, bacteria, UTI or citrus fruits or
vegetables, common after eating• Acidic urine: dehydration, high meats and cranberries,• Alkaline causes calcium carbonate, phosphate and magnesium
phosphate stones

UA• Protein
• Indicates if glomerular membrane is intact like in glomerularnephritis, protein then seeps into urine and can lead to hypoproteinemia which decreases capillary oncotic pressure causing edema called nephrotic syndrome
• Proteinuria indicates renal disease or preeclampsia • Indicates complications of DM, glomerularnephritis, amyloidosis, multiple
myeloma• Specific gravity
• High indicates concentrated urine• Low is dilute urine• Weight of urine compared to that of pure water• Chronic diseases associated with low specific gravity measure of hydration
status• Dehydration causes it to be really high
• Leukocyte esterase• Positive indicates UTI

UA• Nitrites
• Screening for UTI, bacteria produce reducase converting nitrates to nitrites
• Ketones• Poorly controlled diabetes and hyperglycemia, massive fatty acid
catabolism• Bilirubin and urobilinogen
• Conjugated bilirubin is water soluble, indicates disease affecting bilirubin affecting bilirubin metabolism after conjugation or defects in excretion indicate previously suspected liver disease, gallstones, or drug toxicity
• Crystals• Indicate renal stone formation is imminent• Can be with high serum uric acid levels• Parathyroid causes high phosphate and calcium crystals

UA• Casts
• Rectangular clumps that form renal distal and collecting tubules, pH must be acidic and urine concentrated• Hyaline
• Conglomerations of protein, proteinuria• Cellular
• Conglomerations of degenerated cells• Granular
• After exercise and renal disease, result from disintegration of cellular material into granular particles within a WBC
• Fatty• Some diseases epithelial cells desquamate into renal tubule fatty droplets become free oval fat bodies or
incorporated into proteins associate with nephrotic syndrome or nephrosis, fatty emboli or bone fractures• Waxy
• Cell, hyaline, renal failure or further degeneration of granular casts, associated with chronic renal disease and renal failure or diabetic nephropathy, malignant hypertension, and glomerularnephritis
• Epithelial• Shed from bladder from tumor, infection, or polyps• Tubule epithelial casts indicate glomerulonephritis
• WBC• Five or more indicate UTI involving bladder, kidneys, or both• Inflammatory nephritis, glomerulonephritis • pyelonephritis
• RBC• Bladder, urethral, and ureteral disease, tumor, trauma stones infection, glomerloneprhitis, renal infarct,
goodpasture, vasculitis, sickle cell, interstitial nephritis, tubular necrosis, pyelonephritis

Cardiac cath• Normal heart muscle motion, normal and patent coronary
arteries, normal great vessels, and normal intracardiac pressure and volume
• Indications:• Visualize heart chambers, arteries, and great vessels• Evaluate chest pain• Locate region or coronary occlusion in patients with positive
stress test• Right heart determines CO measures right heart pressures and
can identify pulmonary emboli

cath• Test explanation:
• Identify, locate, and quantify severity of atherosclerotic, occlusive disease• Evaluate severity of septal defects• Presence and degree of congenital cardiac anomalies• Evaluate previous cardiac surgery• Evaluate muscle function• Identify ventricular aneurysms• Identify and locate acquired disease of great vessels• Evaluate and treat patients with acute MI• Insert a cath monitor right sided heart pressures and pulmonary wedge
pressures• Dilate stenotic coronary arteries place coronary stent or laser arterectomy• In right sided jugular, subclavian, brachial or femoral vein• Left right femoral artery is cannulated or brachial or radial artery • Percutaneous transluminal coronary angioplasty balloon and stent• Arterectomy involves using a rotating knife to breakout plaques
cath• Contra
• Unable to cooperate• Refuse intervention if an amenable lesion were found• Iodine dye allergy• Pregnant patients• Renal disorders• Bleeding propensity
• Complications• Arrhythmias• Perforation of myocardium• Renal failure• Catheter induced embolic cerebrovascular accident (stroke)• Arterial thrombosis, embolism, or pseudoaneurysm• Infection• Pneumothorax after subclavian insertion• Hypoglycemia or acidosis

Pulmonary function• Indication:
• Preoperative evaluation of lungs and pulmonary reserve when planned surgery will cause loss of functional pulmonary tissue like lobectomy or pneumonectomy risk of pulmonary failure exists or if preoperative compromised by COPD
• Evaluate response to bronchodilator therapy in patients with COPD
• Differentiate between restrictive and obstructive forms of chronic pulmonary disease restrictive (fibrosis, tumors, chest wall trauma) obstructive (emphysema, bronchitis, asthma)
• Determine diffusing capacity of lungs• Perfomance of inhalation tests in patients with inhalation
allergies

Pulmonary function• Test explanation
• Detect abnormalities in respiratory function determine extent of abnormality• Include spirometry, measurement of airflow rates, calculation of lung volumes
and capacities• Spirometer measures air volumes values greater than 80% are normal provides
info about obstruction or restriction• Add a time element plotted on an X-Y axis, maximally inhale then forcefully
exhale while being timed, if diminished a bronchodilator can be given to monitor improvement
• Nitrogen and helium techniques monitor lung capacity• Gas exchange measure diffusing capacity of lung using CO abnormal in CHF,
pneumonia and other diseases that fill alveoli with fluid or exudate• Forced vital capacity: amount of air forcefully expelled from maximal inflation• Forced expiratory volume in 1 second (FEV1) in obstructive disease airways are
narrowed and resistance to flow is high therefore not as much air can be expelled in one second and is less than predicted value restrictive it is decreased because amount of air inhaled is low in restrictive FEV/FVC is 80% obstructive is a lot less
• Maximal midexpiratory flow or force midexpiratory flow maximal rate of airflow through the pulmonary tree during forced expiration low in obstructive

Pulmonary function• Maximal volume ventilation maximal volume of air that a patient can breathe in and out
during one minute low in restrictive and obstructive• Tidal volume: volume of air inspired and expired with each normal respiration• Inspiratory reserve volume maximum that can be inspired from end of normal inspiration• Expiratory reserve colume max volume of air that can be exhaled after normal expiration• Residual volume: volume of air remaining of air that can be inspired after normal
expiration• Functional residual capacity amount of air left in the lungs after normal expiration• Vital capacity max amount of air that can be expired after max inspiration• Total lung capacity volume to which lungs can be expanded with greatest inspiratory
volume• Minute volume volume of air inhaled and exhaled per minute• Dead space part of VT that does not participate in alveolar gas exchange• Forced expiratory flow portion of airflow curve most affected by airway obstruction• Peak inspiratory flow rate flow rate of inspired air during max inspiration indicates large
airway disease• Peak expiratory flow rate max airflow rate during forced expiration
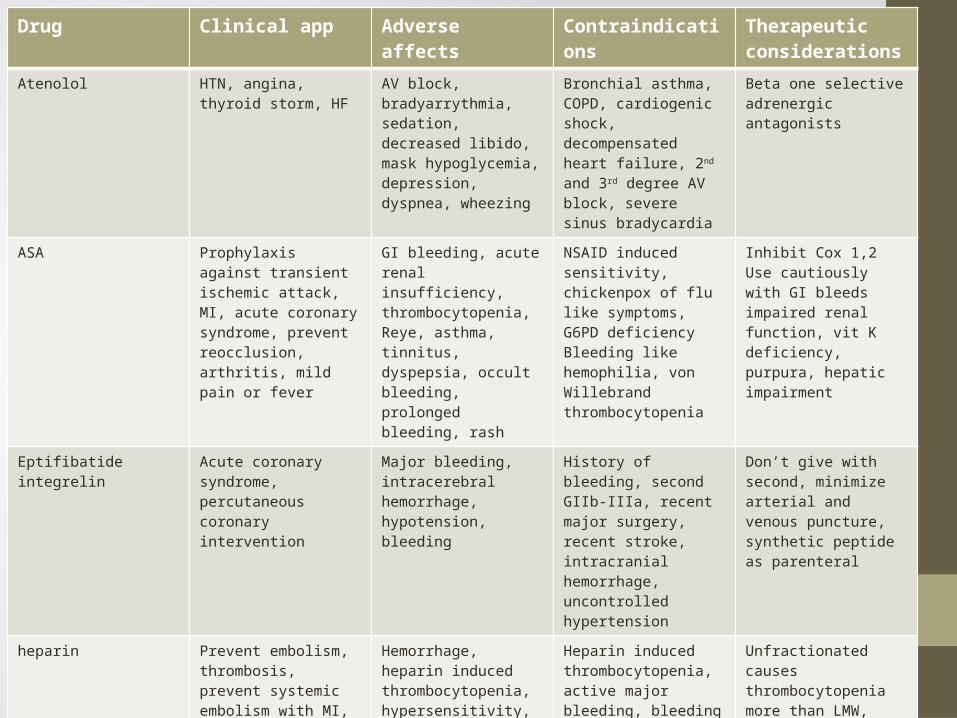
Drug Clinical app Adverse affects Contraindications Therapeutic considerations
Atenolol HTN, angina, thyroid storm, HF
AV block, bradyarrythmia, sedation, decreased libido, mask hypoglycemia, depression, dyspnea, wheezing
Bronchial asthma, COPD, cardiogenic shock, decompensated heart failure, 2nd and 3rd degree AV block, severe sinus bradycardia
Beta one selective adrenergic antagonists
ASA Prophylaxis against transient ischemic attack, MI, acute coronary syndrome, prevent reocclusion, arthritis, mild pain or fever
GI bleeding, acute renal insufficiency, thrombocytopenia, Reye, asthma, tinnitus, dyspepsia, occult bleeding, prolonged bleeding, rash
NSAID induced sensitivity, chickenpox of flu like symptoms, G6PD deficiencyBleeding like hemophilia, von Willebrand thrombocytopenia
Inhibit Cox 1,2Use cautiously with GI bleeds impaired renal function, vit K deficiency, purpura, hepatic impairment
Eptifibatide integrelin Acute coronary syndrome, percutaneous coronary intervention
Major bleeding, intracerebral hemorrhage, hypotension, bleeding
History of bleeding, second GIIb-IIIa, recent major surgery, recent stroke, intracranial hemorrhage, uncontrolled hypertension
Don’t give with second, minimize arterial and venous puncture, synthetic peptide as parenteral
heparin Prevent embolism, thrombosis, prevent systemic embolism with MI, unstable angina, open heart surgery, DIC, maintain patency IV cath
Hemorrhage, heparin induced thrombocytopenia, hypersensitivity, prolonged clotting time, mucosal ulceration, hematoma
Heparin induced thrombocytopenia, active major bleeding, bleeding tendencies, open ulcerative wounds, conditions that increase capillary permeability, severe HTN, bacterial endocarditis
Unfractionated causes thrombocytopenia more than LMW, antihistamines, cardiac glycosides, nicotine and tetracycline affect abilityCephalosporins, penicillins, oral anticoagulants, platelet inhibitors may increase affectsDon’t use ginger, garlic, ginkgo
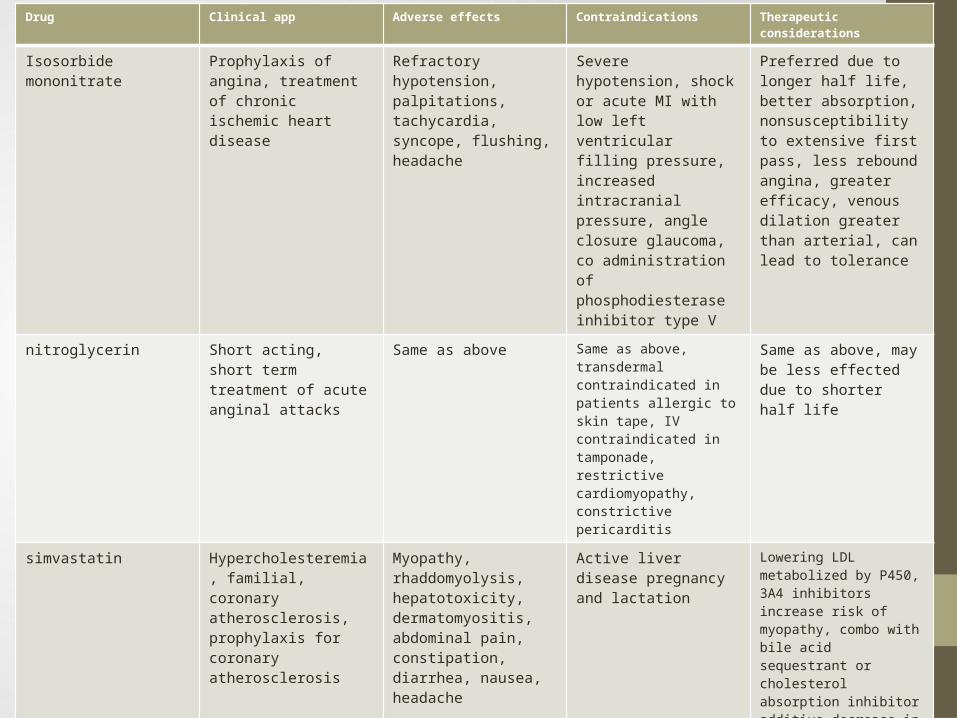
Drug Clinical app Adverse effects Contraindications Therapeutic considerations
Isosorbide mononitrate Prophylaxis of angina, treatment of chronic ischemic heart disease
Refractory hypotension, palpitations, tachycardia, syncope, flushing, headache
Severe hypotension, shock or acute MI with low left ventricular filling pressure, increased intracranial pressure, angle closure glaucoma, co administration of phosphodiesterase inhibitor type V
Preferred due to longer half life, better absorption, nonsusceptibility to extensive first pass, less rebound angina, greater efficacy, venous dilation greater than arterial, can lead to tolerance
nitroglycerin Short acting, short term treatment of acute anginal attacks
Same as above Same as above, transdermal contraindicated in patients allergic to skin tape, IV contraindicated in tamponade, restrictive cardiomyopathy, constrictive pericarditis
Same as above, may be less effected due to shorter half life
simvastatin Hypercholesteremia, familial, coronary atherosclerosis, prophylaxis for coronary atherosclerosis
Myopathy, rhaddomyolysis, hepatotoxicity, dermatomyositis, abdominal pain, constipation, diarrhea, nausea, headache
Active liver disease pregnancy and lactation
Lowering LDL metabolized by P450, 3A4 inhibitors increase risk of myopathy, combo with bile acid sequestrant or cholesterol absorption inhibitor additive decrease in LDL, combo with niacin maybe used in high LDL and low HDL increases risk of myopathy, gemfibrozil decreases statin clearance induce rhabdo
HCTZ/ triamterene HTN, adjunct in edema states associated with HF, cirrhosis, renal dysfunction, corticosteroid and estrogen
Arrhythmia, stevens-johnson, pancreatitis, hepatotoxicity, SLE, hypotension, alkalosis, vasculitis, photosensitivity, electrolyte abnormalities, impotence, restlessness, blurrred vision, headache, hyperglycemia, hyperuricemia
Anuria, hypersensitivity to sulfonamides, co administration with agents that prolong QT
First line in treating HTN, diminish hypercalcuria in patients at risk for nephrolithiasis, decreases glucose tolerance may unmask diabetes, don’t use with antiarrhythmic
Ocular exam• Done without dilating the eye looking at posterior structures of retina• To see peripheral structures like macula you dilate with mydriatic drops• Darken room, turn on light, turn lens to 0 diopter• Shine line over pupil and look for orange/red glow• Opacity of lens is a cataract or detached retina or retinoblastoma• Hippus (spasm) of pupil if you shine light too brightly• Optic disc and retina should be yellowish orange to creamy pink• Vessels become progressively larger as they approach the disc• Minus diopter for nearsighted, positive for farsighted• Look for sharpness or clarity of disc outline, color, size and central physiology,
symmetry• Bulging swelled cup caused by increased intracranial pressure called papilledema
may be caused by meningitis, subarachnoid hemorrhage, trauma, and mass lesions• Spontaneous venous pulsations are normal, follow vessels to the periphery notice
shape, color, size, and distribution• Fovea should be a tiny bright light reflection have patient look directly into the
light• Look for opacities in vitreous or lens rotating diopters to +10 or 12• Physiologic cup is a small whitish depression from which retinal vessels emerge,
grayish spots are normal• Rings and crescents can be seen as well as medulated nerve fibers (irregular white
patches) both are normal

Serum amylase• Critical when 3x upper limit (60-120 normal)• Detect and monitor the clinical course of pancreatitis • Ordered frequently when a patient presents with acute abdominal pain• Test explanation
• Most specific for pancreatitis • Amylase is normally secreted from pancreatic acinaar cells into pancreatic
duct and into duodenum• Aids in the digestion of carbs• Damage to acinar or obstruction of duct by carcinoma or gallstones causes
outpouring into intrapancreatic lymph and free peritoneum• Abnormal levels rise within 12 hours of the onset of the disease• It is rapidly excreted to persistence will show if pathology is persistent • Not specific can be elevated for bowel perforation, penetrating peptic ulcer,
duodenal obstruction, salivary gland infection, ectopic pregnancies, severe diabetic ketoacidosis
• Patients with chronic pancreatic necrosis due to tumor or massive hemorrhage may cause low amylase levels

Serum amylase• Interfering factors
• Serum lipidemia factitiously decreases amylase• IV dextrse lowers amylase• Aminosalicylic acid, aspirin, azathioprine, corticosteroids, dexamethasone, ethyl
alcohol, glucocorticoids, iodine containing contrast medium, loop diuretics, methyldopa, narcotic analgesics, oral contraceptives, prednisone
• Increased levels• Acute pancreatitis, chronic relapsing pancreatitis, penetrating peptic ulcer into
the pancreas• GI disease• Acute cholecystitis• Parotiditis (mumps)• Ruptured ectopic pregnancy• Renal failure• Diabetic ketoacidosis• Pulmonary infarction• After endoscopic retrograde pancreatography

Urine amylase• Normal value up to 5000 somogyi units• Used to assist in making the diagnosis of pancreatitis although
other nonpancreatic diseases can cause elevated urine amylase levels
• Levels rise later than blood amylase levels• Several days after the onset of disease serum mmay be normal but
urine levels are significantly elevated, useful for detecting pancreatitis late in the disease course
• Test explanation:• Kidneys clear amylase, disorders that affect pancreas cause
increased amylase levels in urine• Serum levels rise transiently after resolution of acute phase of
disease, urine levels remain elevated 5-7 days after onset• Not specific for disorders: parotiditis, cholecystitis, perforated
bowel, peptic ulcer, ectopic pregnancy and renal disease
Tc99 sestamibe• Measures left ventricular muscle function and coronary artery blood distribution• Tc99 given intravenously then a radiation detector is placed over heart• Myocardial cells take up substance and appear as hotspots on the photoscan where as
areas of ischemia appear as cold spots• First pass gives the best images• A Tc can be given that binds to calcium when ischemia or early infarction has occurred
the calcium leaks out of cardiac cells which shows an MI hotspot scan used when LVH or LBBB is hard to see on EKG good for those with chest pain 5-10 days before seeing the doctor
• Can be used to assess ischemia during stress testing radionuclide injected IV at point of maximal cardiac stress accumulates in the myocardium in proportion to regional blood flow, normal will have higher radionuclide activity good for post operative bypass monitoring and the diagnosis of CAD
• Can also evaluate ejection fraction with pertechnate values less than 65% indicates ischemia, infarction, myopathy
• Cardiac flow rapid injection obtaining images immediately to avoid first pass provides info about direction of flow to and from ventricles good for kids in determining CHD
• Computer assisted gated scan allow for myocardial wall photography while in motion showing myocaytes during cardiac cycle

Drug Clinical applications Adverse affects Contraindications Therapeutic considerations
Omeprazole Peptic ulcer disease, GERD, erosive esophagitis, gastic acid hypersecretionh. Pylori GI tract infection
Pancreatitis, hepatotoxicity, interstitial nephritis, may affect effects of clopidigrel increased risk of hip, wrist and spine fracture, hospital acquired pneumonia, and enteric infections including clostridium difficile, salmonella, E. coli, headache, rash, GI discomfort, diarrhea, anorexia, asthenia, back pain
hypersensitivity Proton pump inhibitors metabolized in liver by CYP2C19 and CYP3A4 drug interaction with ketoconazle or itraconazle due to acid environment needed to absorb azole drugs
Aluminum hydroxide Symptomatic relief of dyspepsia associated with peptic ulcer disease, GERD or hiatal hernia
Phosphate depletion (severe weakness, malaise anorexia), constipation, osteomalacia in patients with renal failure
hypersensitivity All antacids can potentially increase or decrease the rate or extent of absorption of concurrently administered oral drugs by changing transit time or by binding the drug
Magnesium hydroxide Same as above Diarrhea, hypermagnesemia in patients with renal failure
Hypersensitivity Same as above

Abdominal painGI disorders Urinary and renal disorders
Abdominal pain acute and chronic Suprapubic pain
Indigestion, nausea, vomiting including blood, loss of appetite, early satiety
Dysuria, urgency or frequency
Dysphagia and/or odynophagia Hesitancy, decreased stream in males
Change in bowel function Polyuria or nocturia
Diarrhea, constipation hematuria
Jaundice Kidney or flank pain
Ureteral colic
Urinary incontinence

Abdominal pain• Visceral pain occurs when hollow abdominal organs like intestines or biliary
tree contract unusually forcefully or are distended or stretched • solid organs become painful when their capsules are stretched• Pain usually near the midline at levels that vary according to the structure
involved• May be gnawing, burning, cramping or aching• Sweating, pallor, nausea, vomiting, and restlessness
• Parietal• Inflammation in the parietal peritoneum• Steady, aching pain that is usually more severe than visceral• Aggravated by moving or coughing
• Referred pain• Develops as the initial pain becomes more intense and thus seems to radiate
or travel from the initial site• Duodenal or pancreatic refers to the back• Biliary tree to the right shoulder or right posterior chest• Pleurisy or acute MI may appear as epigastric pain

Abdominal pain• Determine timing, ask where it starts, ask patient to point to pain, ask if it radiates, ask
severity• Pay attention to exascerbating or remediating factors: association with meals, alcohol,
medications, stress, body position, use of antacids• Dyspepsia is chronic or recurrent discomfort or pain centered in the upper abdomen• Discomfort is subjective negative feeling that may be bloating, nausea, upper abdominal
fullness, and heartburn• Inflammatory bowel might be related to bloating• Function or nonulcer dyspepsia with 3 month history of nonspecfic abdominal discomfort
or nausea not from an ulcer• Heartburn, acid reflux or regurg more than once a week likely to have GERD related to
prolonged acid clearance damping actions of bicarb, delayed emptying, hiatal hernia• Heartburn is rising retrosternal burning pain or discomfort occurring weekly or more often
associated with chocolate, citrus, coffee, onions, peppermints, alcohol, bending over, exercise, lifting or lying supine
• GERD may cause coughing, wheezing, and aspiration pneumonia or pharyngeal symptoms like hoarseness and chronic sore throat
• “alarm symptoms” difficulty swallowing (dysphagia), pain with swallowing (odyophagia), recurrent vomiting, GI bleeding, weight loss, anemia are low risk for gastric cancer

BUN• > 100 mg/dL indicates serious impairment of renal function• Indirect and rough measurement of renal function and GFR• Measurement of liver function• Measures the amount of urea nitrogen in the blood• Formed in the liver as the end product of protein metabolism and
digestion• Related to the metabolic function of the liver and excretory function of
the kidney• Elevated BUN is called azotemia• Usually indicates bilateral disease, unilateral can compensate• Shock, dehydration, CHF, and excessive protein catabolism causes
increased levels• GI bleeding can also increase because blood proteins are broken down
and absorbed in the intestines• Ureteral and urethral obstruction can cause postrenal azotemia

BUN• Synthesis of urea depends on the liver• Decreased BUN indicates liver disease• BUN is taken with creatinine ratio is 6-25• Interfering factors:
• Changes in protein intake, low protein diets decrease BUN• Muscle mass determines BUN• Advanced pregnancy• GI bleeding• Over and underhydration over dilutes BUN• Drugs that increase: allopurinol, aminoglycosides, cephalosporins,
chloral hydrate, cisplatin, furosemide, guanethidine, indomethacin, methotrexate, methyldopa, nephrotoxic drugs (aspirin, amphotericin B, carbamazepine, colistin, gentamicin, methicillin, neomycin, penicillin, polymyxin B, probenecid, vancomysin), propanolol, rifampin, spironolactone, tetracycline, thiazide and triamterene
• Drugs that decrease chloramphenicol and streptomycin

Stool hemoccult• Screening for colorectal cancer• Test explanation
• Tumors of the intestine grow into the lumen and are subjected to repeat trauma by the fecal stream
• The friable neovascular tumor ulcerates and bleeds• Guaiac chemistry performed on the stool to detect blood peroxidase like
activity of hgb catalyzes reaction of peroxide and a chromogen forming ortholidine
• OB can be detected by immunochemical methods called fecal immunochemical test (FIT) or immunochemical fecal occult blood test not affected by red meats or plants like Guaiac may fail to recognize upper GI blood
• DNA stool sample test is twice as sensitive as guaiac for colorectal precancerous, benign or malignant tumors because some polyps don’t shed blood
• Benign, malignant GI tumors, ulcers, inflammatory bowel disease, arteriovenous malformations, diverticulosis, hematobilia all cause OB
• Hemorrhoids swallowed blood
Stool hemoccult• Interfering factors
• Bleeding gums following dental procedure or disease• Animal hemoglobin of ingested animal meat• Peroxidase rich vegetables (turnips, horseradish, artichokes, mushrooms,
radishes, broccoli, bean sprouts, cauliflower, oranges, bananas, cantaloupes, grapes)
• Anticoags, aspirin, colchicine, iron, nonsteroidal antiarthritics, and steroids• drugs that instigate peroxidation reaction Boric acid, bromides, colchicine,
iodine, iron, rauwolfia• Vitamin C inhibits peroxidation reaction causing false negatives
• Results and significance• GI tumor and polyps• Peptic ulcers• Varices from portal hypertension• IBS• GI trauma or surgery• Hemorrhoids and other anorectal problems
Drug Clinical application
Adverse affects Contraindications
Therapeutic consideration
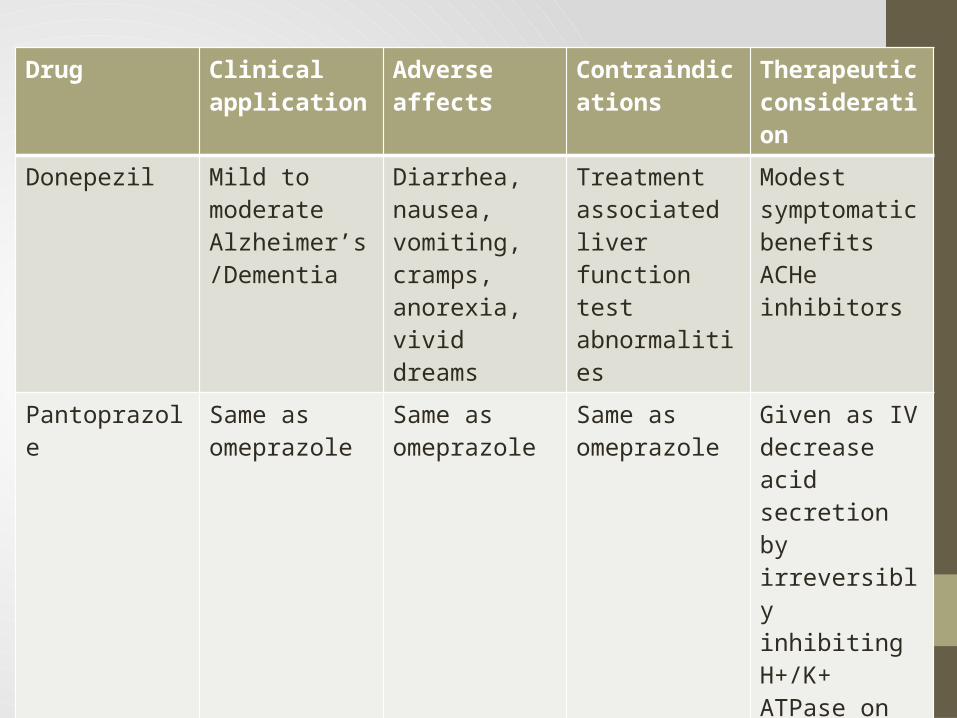
Donepezil Mild to moderate Alzheimer’s/Dementia
Diarrhea, nausea, vomiting, cramps, anorexia, vivid dreams
Treatment associated liver function test abnormalities
Modest symptomatic benefitsACHe inhibitors
Pantoprazole Same as omeprazole
Same as omeprazole
Same as omeprazole
Given as IV decrease acid secretion by irreversibly inhibiting H+/K+ ATPase on parietal cells

Drug Applications Adverse effects Contraindications Therapeutic considerations
Naproxen Propionic acid, mild to moderate pain, fever, osteoarthritis, RA, dysmenorrhea, gout
GI hemorrhage, ulceration, perforation, Stevens-Johnson syndrome, pseudoporphyria, GI disturbance, tinnitus
GI or intracranial bleeding, coag defects, asthma, urticaria, allergic type reactions, significant renal insufficiency
Longer half life, 20x more potent causes fewer GI adverse affects
Ketorolac Acetic acid Same as above Same as above Analgesia in postsurgical patients, used for no more than 3-5 days
FeSO4 Iron supplement for anemia due to blood loss and iron insufficiency
Stomach upset or pain, constipation, diarrhea, nausea or vomiting
Diabetes, infants, may upset ulcers, not to be take with thalassemias, may irritate IBS

Alkaline phosphatase• Used to detect and monitor diseases of the liver or bone• Test explanation
• Highest concentration found in liver, biliary tract epithelium, and bone, intestinal mucosa and placenta
• Functions in alkaline pH• ALP in kupffer cells lining biliary collecting system and is excreted in the bile• Increased in extra and intrahepatic obstructive biliary disease and cirrhosis• Hepatic tumors, hepatotoxic drugs, and hepatitis increase levels• Most sensitive test to detect tumor metastasis to the liver• New bone growth elevates ALP• Osteoblastic metastatic (breast, prostate) tumors• Paget, healing fractures, RA, hyperparathyroidism, and normal growing
bones are sources of elevated ALP• ALP1 is liver origin and is heat stable• ALP2 is inactivated by heat and is bone• ALP 5’ nucleotidase are elevated in diseases of the liver

ALP• Interfering factors:
• Recent ingestion of a meal can increase levels• Young children with rapid bone growth• Albumin made from placental tissue, allopurinol, antibiotics,
azathioprine, colchicine, fluorides, indomethacin, isoniazid, methotrexate, methyldopa, nicotinic acid, phenothiazine, probenecid, tetracycline, and verapamil may increase ALP
• Arsencials, cyanides, fluorides, nitrofurantoin, oxalates, and zinc salts may lower ALP

GGT• Sensitive to hepatobiliary disease, indicates heavy and chronic alcohol use• Test explanation
• Enzyme participates in the transfer of amino acids and peptides across the cell membrane
• Highest concentrations found in liver and biliary tract• Smaller concentrations found in kidney, spleen, heart, intestine, brain, and prostate
gland• Detect liver cell dysfunction highly accurate in indicating even slightest degree of
cholestasis• Detects biliary obstruction, cholangitis, or cholecystitis• Parallels elevation of ALP but more sensitive• Not increased in bone disease• Elevated in 75% of patients that chronically drink• Elevated with MI
• Interfering factors• May decrease late in pregnancy• Drugs that increase: alcohol, phenobarbitol, and phenytoin• Drugs that decrease: clofibrate and oral contraceptives

Gliadin antibodies• Endomysial IgA, gliadin IgA, tissue transglutaminase• Diagnose celiac disease and sprue by identifying ab to gliadin
and gluten in affected patients• Crohn, colitis, and severe lactose intolerance may increase
levels• Test explanation
• Patients cannot tolerate ingestion of gliadin and gluten which are toxic to intestinal mucosa
• Patients experience severe malabsorptive symptoms• Gliadin and gluten cause direct mucosal damage and Ig appear
in gut mucosa and in serum

Lactose tolerance test• Used to diagnose lactose intolerance caused by lactase
insufficiency, intestinal malabsorption, maldigestion, or bacterial overgrowth in small intestine
• Test explanation:• Glucose plasma will not rise after the ingestion and the small
bowel is flooded with a high lactose load• Bacterial catabolism occurs in the intestine creates flatus and
hydrogen• Symptoms include flatulence, abdominal cramping, bloating,
diarrhea, and failure to thrive in infants• Lactose load is given and if lactase is absent then the serum
glucose will not rise• Given glucose tolerance test to isolate lack of lactase• Breath test in which expelled air is analyzed for hydrogen content
for when bacteria have taken over small intestine

Lactose tolerance test• Interfering factors
• Enterogenous steatorrhea (malabsorption) • Strenuous exercise will reduce glucose• Diabetics have high glucose• Smoking may increase blood glucose• Ethnicity• Antibiotics can decrease bacteria and cause false negative

Ptt
• Assess the intrinsic and common pathway of coag• Evaluates fibrinogen, prothrombin, V, VIII, IX, X, XI, and XII• Hepatocellular disease prolongs PTT and obstruction which
precludes GI absorption of fat soluble vitamins prolongs time• Heparin prolongs PTT so it is used for therapy monitoring• Antihistamines, ascorbic acid, chlorpromazine, heparin and
salicylates prolong PTT• Early DIC and extensive cancer causes decreased levels
PT and INR• Evaluate extrinsic and common pathway• Fibrinogen, prothrombin, V, VII, X• Decreased levels: hepatocellular disease affect factors I, II, V, VII, IX,
and X• Obstructive biliary disease causes fat malabsorption A, D, E, and K
affected• Coumarin ingestion• INR is organized data• Warfarin interferes with vitamin K may be enhanced by aspirin,
quinidine, sulfa, and indomethacin• Barbituates, chloral hydrate and oral contraceptives cause increased
coumarin drug binding decreasing the effects• Alcohol can prolong• Diet high in fat or leafy vegetables may shorten OT• Diarrhea or malabsorption can prolong

Upper GI series• Visualize esophagus, stomach, and duodenum to evaluate
dysphagia, weight loss, early satiety, upper abdominal pain, ulcer symptoms or dyspepsia, alcoholism and suspected varices, results of barium swallow or x-ray shows pathologic condition
• Channels for air, scope, cauterizing tools• AV malformations, tumors, enteropathies (celiac) and
ulcerations• Video capsule for small intestine and detecting polyps, IBS,
ulcers, tumors of small intestines• Not for patients who don’t cooperate, severe bleeding,
esophageal diverticula, suspected perf, recent GI surgery• May cause pulmonary aspiration, perf, bleeding from biopsy,
oversedation, local IV phlebitic reaction, hypotension

sigmoidoscopy• Direct visualization of rectum and sigmoid colon• Diagnose suspected pathology of those organs• Recommended for patients with a change in bowel habits or
obvious occult blood or abdominal pain• May remove polyps, reduce volvulus, obliterate hemorrhoids• Could perf colon, bleeding from biopsy sites• Poor bowel prep may obscure visualization, rectal bleeding
may obstruct lens• Not for patients with diverticulitis, painful anorectal
conditions, severe bleeding or suspected perf• Detect colorectal cancer, polyp, ulcerative proctitis,
pseudomembranous colitis, intestinal ischemia

Fecal fat• Confirm diagnosis of steatorrhea, when patient has large,
greasy, and foul-smelling stools• Children with CF have obstructed pancreatic ducts so they
cannot be expelled into the intestine • Any condition that causes malabsorption (sprue, Crohn,
whipple, gallstones, tumor, duct obstructions)• Short gut causes higher fecal fat• Enemas and laxatives may increase fat• Barium and fiber laxatives decrease • Increased: CF, malabsorption due to celiac, sprue, whipple,
crohn or radiation enteritis, short gut
Barium enema• Visualize colon, distal small bowel, and appendix indicated when:
abdominal pain, obvious or occult blood in the stools, IBS, suspected cancer, volvulus ro obstruction
• Determines presence of polyps, tumors, and diverticula also anatomic abnormalities
• Assess filling of the appendix failure to fill means appendicitis• Affects diseases of ileum like Crohn, IBS, and fistulas• Air contrast can be sufflated with polyp to increase accuracy• Not to be performed with perf, non cooperative, megacolon• May cause perf, fecal impaction• Residual stool, spasm, and old barium may affect study• Detect: fistula, perf, appendicitis, extrinsic compression of colon from
extracolonic tumor, malrotation, colon volvulus, intussusception, hernia, colonic stenosis due to ischemia, infection or previous surgery, IBS, polyps, diverticula, tumor

Lower abdominal pain• For right lower quadrant ask if the pain is sharp, continuous, intermittent,
and cramping if it migrates to pre-umbilical area it is appendicitis or PID, ruptured ovarian follicle, ectopic pregnancy
• Renal stones cause cramping in left or right lower quad• Left lower quad or diffuse abdominal pain can be associated with fever
and loss of appetite with a mass it may be diverticulitis • Absent bowel sounds and firmness, guarding or rebound indicates small or
large bowel obstruction• Chronic pain ask about diarrhea or constipation• Changes in bowel habits indicate colon cancer without structural
abnormalities it can be IBS• Nausea may progress to retching and vomiting• Retching describes involuntary spasm of stomach, diaphragm, and
esophagus precedes and culminates in vomiting• Seen in pregnancy, diabetic ketoacidosis, adrenal insufficiency, hyper
calcemia, uremia, liver disease, emotional states, adverse drug reactions

Lower abdominal pain• Regurgitation occurs in GERD, esophageal stricture and cancer• Vomiting and pain may be small bowel obstruction• Fecal odor occurs with small bowel obstruction or gastrocolic
fistula• Make sure vomit doesn’t contain blood brownish or coffee
grounds, blood comes with esophageal or gastric varices, gastritis or peptic ulcer disease
• Lightheaded? Syncope• Anorexia is loss of appetite• Diabetic gastroparesis, anticholingergic meds, gastric outlet
obstruction, gastric cancer, hepatitis cause early satiety• Dysphagia difficulty swallowing orpharyngeal symptoms include
drooling, nasopharyngeal regurg, and coughing• Pointing below sternoclavicluar notch is esophageal dysphagia

Abdominal series• Anterior posterior “KUB” kidneys, ureter, bladder• Upright radiograph searching for free intraperitoneal air and/or intestinal air-
fluid levels• Glance over entire radiograph in relaxed manner allowing for obvious
abnormalities to jump out• Water dense organs like the liver and spleen will pop out presence of bowel
gas in right and left upper quadrant indicate size because they are at lower edges of liver and spleen
• A liver shadow to the iliac crest indicates enlargement • Psoas muscles are usually visible• Renal shadows should be visible as gray structures surrounded by black
retroperitoneal fat • Look for calcifications in kidneys, ureters, urinary bladder, and gallbladder• Evaluate the bowel gas pattern• Look at bones systematically beginning with ribs and visible spine• Free intraperitoneal air is usually visualized on upright radiograph
Abdominal series• In adynamic ileus (paralytic ileus or ileus) there is too much bowel gas in
the entire GI tract, may arise from intra-abdominal cases or as a reflex phenomenon from disease elsewhere
• In an obstruction there is usually air-filled, dilated intestine proximal to point of obstruction and little to no air distal to obstruction
• If obstruction versus ileus is unclear you can use a barium series, CT, and ultrasound
• Large bowel obstruction there is dilated colon proximal to obstruction little to none after
• Valvulae conniventes are regularly spaced thin mucosal folds that extend across the entire small bowel lumen
• Somewhat irregularly spaced transverse bands called colon septa or haustral folds do not extend all the way across colon lumen
• Sigmoid volvulus is common in the elderly: chronic constipation results in redundant sigmoid mesentery that twists on itself causing complete or partial obstruction showing dramatically dilated sigmoid colon
Abdominal series• Perforation shows air outside abdominal lumen, AP supine and upright radiographs• Upright allows air to escape to subdiaphragmatic areas• Pneumatosis intestinalis causes air in the wrong place• Gas filled abscesses can be found in abdominal locations• Gut lumen and wall using a GI contrast is cheaper than endoscopy• Upper GI
• Patient swallows liquid barium with gas producing crystals • Visualize esophagus, stomach, and small intestine• Use water based medium when perf is suspected
• Antegrade small bowel• Patient drinks additional barium radiographs taken at 15 and 30 min
• Enteroclysis• Use a nasointestinal tube extended to duodenal jejunal junction • Can distend small bowel and stomach and duodenum don’t obstruct visualization
• Retrograde small bowel• Barium refluxed fro filled colon into the ileum• Must give antispasmodic drugs
• Barium enema• Must have a clean colon give barium via rectal tube• To diagnose ulcers and polyps• Virtual colonoscopy can be done after giving a medication that tags fecal matter• Insufflate the colon with air• For colon cancer discovery

Imaging features of GI abnormalities
• To detect: intraluminal lesions (polyp, foreign body or exophytic tumor), mucosal lesion (inflammation), mural lesion ( tumor, transmucosal inflammation and edema leads to a napkin ring appearance), extrinsic lesions(large mesenteric nodes adjacent to the gut displacing gut by external force), extraluminal projections (ulcerations and diverticula)
• Heart burn and dysphagia can lead to hiatal hernias common with GERD can be detected on barium esophagus along with strictures
• Esophagography is useful in studying motility disorders• Upper GI series used to detect peptic ulcer diseases seen easily with double
contrast• Ulcers appear as blob of increased density filled with barium recurrent deformities
of the adjacent bowel accompany an ulcer• Stomach cancer is ulcerated, irregular mucosal mass• Crohn’s is inflammation with ulcerations and thickening of the bowel, deeper
lesions with skip lesions and deeper ulcerations• Sprue shows small bowel dilation• Ulcerative colitis ulcerations with loss of haustrations• Polyps and cancer can be detected with double contrast barium enema

Imaging features of GI abnormalities
• Polyposis of the colon is characterized b multiple adenomas all with malignant potential
• Polyps and tumors detected early with virtual colonoscopy• Acute appendicitis doesn’t need to be radiographed if physical
exam strongly points to it• Plain films aren’t really helpful unless calcification is present• CT can be difficult but will be seen as a small tubular structure
with distended lumen, thickening of the periappendiceal wall and inflammation of adjacent fat

Signs and symptoms of hypothyroidism
• Symptoms:• Fatigue, lethargy• Modest weight gain with anorexia• Dry, coarse skin and cold intolerance• Swelling of face, hands, and legs• Constipation• Weakness, muscle cramps, arthralgias, paresthesia, impaired memory and
hearing• Signs:
• Dry, coarse cool skin, sometimes yellowish from carotene, with nonpitting edema and loss of hair
• Periorbital puffiness• Decreased systolic and increased diastolic BP• Bradycardia and in late stages hypothermia• Intensity of heart sounds sometimes decreased• Impaired memory, mixed hearing loss, somnolence, peripheral neuropathy,
carpal tunnel syndrome• Slowed relaxation phase of reflexes such as the ankle reflex

CBC with Diff• RBC, hgb, HCT, MCH, MCHC, MCV, WBC, neutrophils,
lymphocytes, monocytes, eosinophils, basophils• Infection• Anemia• Indirect coombs is blood antibody screening to determine type
before transfusion• Add donor serum to recipients blood• Then do coombs to see if there was a reaction

Coombs test• Used to detect the patient’s ab coating the transfused RBC evaluating suspected
transfusion reactions• Symptoms of transfusion reaction: fever, chills, rash, flank/back pain, bloody urine,
fainting or dizziness• Methyldopa and levodopa can cause non-blood group antigens to develop on RBC
causing hemolysis• Shows that RBCs have been attacked by ab in the bloodstream• In lymphoma this can develop idiopathically• If RBC have ab on them then coombs serum will cause agglutination greater the
quantity the more clumping • Interfering factors: antiphospholipid ab cause false positive, false positive:
ampicillins, captopril, cephalosporin, chlorpromazine, chlopropamide, hydralazine, indomethacin, insulin, isoniazid, levodopa, methyldopa, penicillin, phenytoin, procainamide, quinidine, quinine, rifampin, steptomycin, sulfonamides, and tetracyclines
• Indicates hemolytic disease of newborn, incompatible blood transfusion, lymphoma, autoimmune hemolytic anemia (SLE, RA), mycoplasmal infection, mono, hemolytic anemia after heart bypass, adult idiopathic hemolytic anemia
Iron, TIBC, and Transferrin• Evaluate iron metabolism in deficiency, overload, or poisoning• Test explanation
• Serum iron• Iron deficient anemia: insufficient iron intake, inadequate gut absorption,
increased requirements, loss of blood in menstruation, ulcer, colon neoplasm• Decreased hgb causing microcytic, hypochromic RBC• Decreased MCV and MCHC • Decreased in serum level, elevated TIBC, and low transferrin are anemia
• TIBC and transferrin• Proteins available to bind free iron• During iron overload transferrin stays about the same• In acute inflammatory reactions transferrin lowers also diminished in chronic
illness like malignancy, collagen vascular disease, or liver disease• Hypoproteinemia associated with low transferrin• Increased transferrin in pregnancy and estrogen therapy• TIBC measured by adding excess iron to serum saturating all transferrin,
excess iron is removed iron left is a measurement of TIBC reflective of liver function and nutrition

IRON, tibc, and transferrin• Transferrin saturation (serum iron x 100%)/TIBC• Normal level is 20-50%• Below 15% is iron deficient anemia• Increased with hemolytic anemia, sideroblastic, or megaloblastic and iron
overload or iron poisoning• Chronic illness lowers serum iron decreased TIBC normal transferrin
saturation• Increased intake or absorption of iron leads to elevated iron levels TIBC is
unchanged, saturation is very high• Interfering factors
• Recent transfusion• High iron meal• Estrogen may increase like chloramphenicol, ethanol, BCP, methyldopa• Decrease: ACTH, cholestyramine, colchicine, chloramphenicol, deferoxamine,
methicillin, testosterone• TIBC increased by fluoride and BCP• TIBC decreased by ACTH and chloramphenicol

Iron test results• Serum iron increase
• Hemosiderosis, hemochromatosis• Iron poisoning• Hemolytic anemia• Massive blood transfusion• Hepatitis or hepatic necrosis• Lead toxicity
• Serum iron decrease• Insufficient dietary iron, chronic blood loss, inadequate absorption, pregnancy (late), iron deficient
anemia, neoplasia• Increased TIBC or transferrin
• Estrogen therapy• Pregnancy late• Polycythemia vera• Iron deficient anemia
• Decreased TIBC or transferrin• Malnutrition, hypoproteinemia, inflammatory disease, cirrhosis, hemolytic anemia, pernicious anemia,
sickle cell anemia• Increased saturation
• Hemochromatosis or hemosiderosis, increased iron intake, hemolytic anemia• Decreased saturation
• Iron deficient anemia, chronic illness

Drug Clinical applications
Adverse reactions
Contraindications
Therapeutic considerations
levothyroxine T4, for hypothyroidism, myxedema comaReplaces missing hormone
Hyperthyroidism, osteopenia, pseudotumor cerebri, seizure, myocardial infarction
Acute MI, uncorrected adrenal cortical insufficiencyUntreated thyrotoxicosis
Cholestyramine and sodium polystyrene sulfonate decrease absorption of synthetic thyroid hormoneRifampin and phenytoin increase metabolismT4 desirable because of its longer half life





























