Embed Size (px)
Citation preview

Combined Assessment of Myocardial Perfusion and left Ventricular Function
With Exercise technetium=99m Sestamibi Gated Single-Photon Emission Computed tomography Can Differentiate
Between lschemic and Nonischemic Dilated Cardiomyopathy
Peter G. Danias, MD, PhD, Alan W. Ahlberg, MA, Bernard A. Clark III, MD,
Frank Messineo, MD, Michael G. Levine, MD, Carol C. McGill, LPN, April Mann, CNMT,
Jonathan Clive, PhD, James E. Dougherty, MD, David D. Waters, MD, and Gary V. Heller, MD, PhD
The purpose of this study was to determine whether exercise technetium-99m sestamibi gated single-photon emission computed tomography (SPECT) accurately dis- tinguishes between patients with ischemic cardiomyop athy and patients with nonischemic left ventricular sys- tolic dysfunction. Noninvasive tests have previously failed to accurately separate patients with ischemic car- diomyopathy from those with nonischemic cardiomyop athy. TechnetiumMm gated SPECT imaging offers ad- vantages that have the potential to overcome the limitations of previous studies. Thirty-seven adults with a left ventricular ejection fraction ~35%, including 24 pa- tients with nonischemic cardiomyopathy and 13 patients with ischemic cardiomyopathy, were prospectively eval- uated using symptom-limited metabolic ex&cise tread- mill testing with technetium-99m sestamibi gated SPECT imaging. Interpretation of myocardial perfusion and re- gional wall motion was performed, using a 17- ment model. Summed stress, rest, and reversibility pe 7 usion
defect scores were determined, and the variance of segmental wall motion scores was computed. Summed stress, rest, and reversibility perfusion defect scores were significantly lower in nonischemic cardiomyopathy patients, compared with those with ischemic cardiomy opathy (summed stress defect score: 6.9 + 3.8 vs 32.9 4 7.7, respectively, p ~0.001). Variability in seg- mental wall motion was also significantly lower in pa- tients with nonischemic cardiomyopathy compared with those with ischemic cardiomyopathy (variance: 0.3 f 0.3 vs 1.2 + 0.8, respectively, p ~0.001). Thus, assess- ment of myocardial perfusion and regional ventricular function with exercise technetium-99m sestamibi gated SPECT imaging can reliably distinguish between patients with ischemic cardiomyopathy and patients with non- ischemic dilated cardiomyopathy. o 1998 by Excerpta Medica, Inc.
(Am J Cardiol 1998;82: 1253-l 258)
C oronary angiography can distinguish between ischemic and nonischemic cardiomyopathy, but a
reliable noninvasive method would be preferable. Pre- vious studies of myocardial perfusion with thallium- 201 imaging’-9 or 13-N ammonia positron emission tomography, lo,’ 1 and ventricular wall motion alone with either radionuclide ventriculography’~8*9~12~13 or echocardiography,14-‘7 reveal group differences be- tween ischemic and nonischemic patients. However,
From the Nuclear Cardiology Laboratory of the Cardiology Division, Hartford Hospitol, Hartford, the Cardiology Dwision and the Heart Failure Working Group, University of Connecticut Health Center, Farmington and the Hoffman Heart Institute, St. Francis Hospital and Medical Center, Hartford, Connecticut. The study WCIS supported in port by grants from the Hartford Hospital Research Fund, Hartford,
Connecticut, and DuPont Radiopharmaceuticals, Billerico, Massachu~ setts. Manuscript received May 5, 1998; revised manuscript received
and accepted June 19, 1998 Address for reprints: Gary V. Heller, MD, PhD, Nuclear Cardiol-
ogy, Hartford Hospital, 80 Seymour Street, Hartford, Connecticut 06102. E-mail: [email protected].
01998 by Excerpta Medica, Inc All rights reserved.
the considerable overlap between these groups limits the usefulness of these techniques for the classification of individual patients. Recent advances in nuclear cardiology, including the use of technetium-99m agents, single-photon emission computed tomography (SPECT), and electrocardiographic gating for simul- taneous evaluation of both myocardial perfusion and ventricular function, offer the potential to overcome the limitations of older methods. These newer tech- niques have not been adequately assessed in patients with cardiomyopathy. This study evaluates whether exercise electrocardiogram-gated SPECT technetium- 99m sestamibi imaging can accurately distinguish be- tween patients with ischemic cardiomyopathy from those with nonischemic cardiomyopathy.
METHODS Patients: Patients with left ventricular systolic dys-
function (ejection fraction 535%) documented by re- cent radionuclide ventriculography, contrast ventricu-
OOOZ-9149/98/$19.00 1253 PII SOOO2-9 149(98)00609-2

lography, or echocardiography were considered for enrollment. Patient identification was performed pro- spectively, based on clinical information from hospital or clinic records. Patients were excluded if they had uncontrolled hypertension, decompensated congestive heart failure, unstable angina, left bundle branch block, pregnancy, or an inability to perform treadmill exercise. Patients were also excluded from further analysis if, at the time of testing, the left ventricular ejection fraction had improved to >40% as measured by automated quantitative gated SPECT analysis.18 Medications were not changed or discontinued. Writ- ten informed consent was obtained frqm all partici- pants, and the study was approved by the Institutional Review Board of all participating centers.
The study population comprised 37 patients. Thir- teen patients had ischemic cardiomyopathy, defined as having significant coronary disease (>70% diameter stenosis in 11 major arteries) by angiography; 24 patients had nonischemic cardiomyopathy. Twenty- one patients (88%) with nonischemic cardiomyopathy had angiographic confirmation of normal coronary arteries or minimal luminal irregularities (<40% di- ameter stenosis) in no >l major epicardial coronary artery. Three patients with nonischemic cardiomyop- athy did not undergo angiography because they had <5% likelihood of having coronary disease. All pa- tients with ischemic cardiomyopathy had previous myocardial infarctions and 11 (85%) had undergone revascularization.
Test description: All patients underwent a symptom- limited metabolic treadmill exercise test. A modified Naughton protocol (Zminute stages, 1 metabolic equivalent [MET] increment per stage) was used, and heart rate, blood pressure, 12-lead electrocardiogram, and expired gases were monitored. Expired oxygen, carbon dioxide, and ventilatory volume were deter- mined using a Sensormedics 2900 metabolic cart (Sensormedics, Anaheim, California) with a breath- by-breath method, by averaging values every 10 sec- onds. Resting and peak oxygen consumption (VO,) were determined by averaging 3 successive values during breathing at rest and peak exercise, respec- tively.
Image acquisition and processing: Stress image ac- quisition was performed 15 to 60 minutes after intra- venous injection of 25 to 30 mCi (0.93 to 1.11 GBq) technetium-99m sestamibi (DuPont Radiopharmaceu- ticals, Billerica, Massachusetts) at peak exercise. Im- ages at rest were acquired on a separate day within 1 week from the stress study, 45 to 60 minutes after intravenous injection of 25 to 30 mCi (0.93 to 1.11 GBq) technetium-99m sestamibi. All images were ac- quired using an ADAC dual-head Vertex gamma cam- era (ADAC Laboratories, Milpitas, California) equipped with low energy, high resolution Vertex collimators. Each data set was acquired over an 180” arc, from 45” right anterior oblique to 45” left poste- rior oblique. Sixty-four projections were obtained (25 s/projection for stress), and gated SPECT was per- formed on the image at rest (30 s/projection with a 100% window) in patients with no significant arrhyth-
Apical Short Axis Mid Shon Axis Basal Short Axis Apical Vertical View
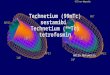
FIGURE 1. Seventeen segment model used for interpretation of myocardial perfusion and ventricular wall motion. The left ante- rior coronary artery distribution includes segments 1,4, 5, 10, 11, 16, and 17. The right coronary artery territory includes seg- ments 2,6,7, 12, and 13, and the left circumflex coronary ar- tery includes segments 3, 8,9, 14, and 15.
mia. All images were stored in a 64 X 64 X 16 matrix. Filtered back-projection was performed using a low- pass Butterworth filter, with a cut-off frequency of 0.6 and an order of 5.0 for the transaxial slices, to a thickness of 6.6 mm.
Test interpretation: All electrocardiograms were in- terpreted by consensus of 2 experienced readers, with- out knowledge of patients’ identity. The exercise elec- trocardiogram was interpreted as positive if there was 20. 1-mV downsloping or horizontal ST-segment de- pression persisting for >0.08 second after the J-point, in patients not receiving digoxin and with no preex- isting ST-segment depression.
Interpretation of myocardial perfusion images was by consensus of 3 experienced readers without knowl- edge of specific diagnosis or patients’ identity. Myo- cardial perfusion was scored using a 17-segment mod- e1,19 on a 0 to 4 scale (0 = normal perfusion, 1 = mild decrease of photon counts, 2 = moderate decrease of photon counts, 3 = severe decrease of photon counts, 4 = absent photon counts). In this model, the left anterior descending coronary artery distribution terri- tory comprised 7 segments, and the left circumflex and right coronary arteries were each assigned 5 seg- ments (Figure 1). Adjusted per segment scores were calculated for all major coronary artery territories by dividing the sum of scores of the individual segments corresponding to a vascular territory by the number of segments in the same territory. Summed stress and rest perfusion defect scores were calculated by adding all 17 individual segment scores for stress and image at rest, respectively. Segmental and summed revers- ibility scores were derived by subtracting the remain- ing scores from the corresponding stress scores. Left and right ventricular size were scored on a 0 to 4 scale (0 = normal, 1 = mildly dilated, 2 = moderately dilated, 3 = moderately to severely dilated, 4 = severely dilated).
Quantitation of regional wall motion was per- formed by visually assessing the endocardial border excursion during systole. Segmental left ventricular wall motion was scored on a 0 to 5 scale (0 = normal, 1 = mildly hypokinetic, 2 = moderately hypokinetic, 3 = severely hypokinetic, 4 = akinetic, 5 = dyski- netic), using the previously described 17-segment model. The variability in regional wall motion was expressed both as the variance of the wall motion
1254 THE AMERICAN JOURNAL OF CARDIOLOGY@ VOL. 82 NOVEMBER 15, 1998

TABLE I Demographic Characteristics and Exercise Data of the Study Population
Nonischemic Cardiomyopathy lschemic Cardiomyopathy
(n = 24) (n = 13) p Value
Age (yrsl 43 + 13 (19-69) 57 2 8 (44-75) 0.002 Men 20 (83%) 11 (85%) 1
left ventricular ejection fraction (%) (QGS) 23.1 5 9.6 (8-37) 22.0 L 5.4 (1 l-29) 0.7 Weight (kg] 93 k 25 (53-162) 81 f 24 (53-100) 0.057 Medications
p blockers 6 7 0.2 Calcium antagonists - 3 0.068
Digoxin 18 7 0.3 Amiodarone
HR at rest (beats/min) 97 + 21 (61T147)
742 18 (5;-117) 0.4
0.003
VO, at rest (ml/kg/min) 3.6 + 0.9 (1.2-5.7) 3.6 k 0.3 (3.2-4.6) 0.9 Exercise time (min) 22.2 k 7.0 (4.1-27) 14.7 k 6.4 (5.8-20.6) 0.15 Workload (METS) 6.4 + 2.0 (2.2-9.3) 5.4 2 0.6 (3.7-6.1) 0.03 Peak HR (beots/min) 157 + 27 (102-212) 129 + 34 (76-214) 0.01
Percentage of maximum predicted HR 89 t 17 (62-126) 79 ? 21 (47-136) 0.13 Maximum HR X systolic BP 22,421 ? 5,672 (12,240-35,192) 17,636 2 5,683 (9,120-29,960) 0.02 Peak VO, (ml/kg/min) 22.2 ? 7.0 (7.5-32.6) 18.8 2 2.2 (13.0-21.2) 0.035
Values are presented CIS mean 2 1 SD or number (%) as appropriate. The range is also shown in parentheses.
BP = blood pressure; HR = heart rate; METS = metabolic equivalent units; QGS = quantitative gated SPECT analysis; V02 = oxygen consumption. -
0 . . . . . . . 1
L
lschemic Nonischemic
Cardiomyopathy Cardiomyopathy
FIGURE 2. Summed stress perfusion defect scores for ischemic and nonischemic cardiomyopathy groups. The solid horizontal lines inside the boxes represent the median values. The dotted . . horizontal lower box
lines represent the mean group values. The upper and
soectivelv. borders indicate the 75th and 25th percentiles, re- The whisker caps represent the 95th and 5th percen-
tiles. T&wide separation between patienk with ischemic and nonischemic cardiomyopathy is apparent.
scores of all 17 segments (segmental wall motion variability) and as the variance of the average wall motion score for individual coronary territories (re- gional wall motion variability). The left ventricular ejection fraction was measured using an automated quantitative method. I8 The measured ejection fraction values were reviewed for accuracy at the time of image interpretation, by visual inspection of the gated SPECT tine loops at various ventricular levels. Right ventricular systolic function was visually assessed and scored on a 0 to 4 scale (0 = normal, 1 = mildly hypokinetic, 2 = moderately hypokinetic, 3 = se- verely hypokinetic, 4 = akinetic).
Statistical analysis: All ordinal data are expressed as mean values ? 1 SD unless otherwise indicated. Two- tailed Student’s t test was used to evaluate differences between continuous numerical data; the chi-square test was used for contingency tables of nominal data. Comparisons between groups for perfusion defect scores and wall motion variability were performed with the Mann-Whitney U test. Logistic regression analysis was used to identify variables that could discriminate between patients with ischemic cardio- myopathy and patients with nonischemic cardiomyop- athy. Missing values were excluded from the multi- variate analysis. Odds ratio (OR) and 95% confidence intervals (CI) were determined for all variables in the model. A p value of ~0.05 was predetermined to be statistically significant. Statistical calculations were performed using the SAS (SAS Institute, Cary, North Carolina) and SPSS (SPSS Inc., Chicago, Illinois) software packages.
RESULTS Baseline demographic characteristics and exercise
data (Table I): At the time of testing, the left ventricular ejection fraction was similar for both ischemic and nonischemic cardiomyopathy groups. Two of isch- emit and none of nonischemic cardiomyopathy pa- tients, developed exercise-induced angina (p = NS). No patient in either group developed ischemic elec- trocardiographic ST-segment depression.
Technetium-99m myocardial petfusion: The mean summed stress, rest, and reversibility scores of pa- tients with ischemic cardiomyopathy were signifi- cantly greater than the corresponding scores of pa- tients with nonischemic cardiomyopathy. The summed stress defect scores of patients with ischemic cardiomyopathy (mean 32.92, 95% CI 28.75 to 37.09) and with nonischemic cardiomyopathy (mean 6.88, 95% CI 5.37 to 8.39) were widely separated (summed stress score ~21 for all ischemic patients and 114 for
METHODS/GATED SPECT IMAGING IN CARDIOMYOPATHY 1255

SfieaS Rest
-- Short Axis
Vertical Long Axis
III Horizontal Long Agis
FGURE 3. Representative images from a patient with ischemic cardiomyopathy (to (bottom panel). In
pane/) and nonischemic cardiomyopathy tL first case, large severe anterior and apical
perfusion defects represent extensive scarring, following m ocar- dial infarction in the distribution of the left anterior desce J mg coronary artery. In the patient with nonischemic cardiomyopa- thy, myocardial perfusion is uniform, with a mild, fixed-inferior defect, which likely represents dia hra matic attenuation arti- fact. The left ventricle is severely &ate! in both patients.
circumflex coronary artery territories (0.12 t 0.18, p <O.OOl). In contrast to nonischemic cardiomyopathy, the regional appearance of defects among vascular territories in the group with ischemic cardiomyopathy was evenly distributed. Representative images from patients with ischemic and nonischemic cardiomyop- athy are shown in Figure 3.
Gated SPECT analysis of ventricular function (Table II): Presence of arrhythmia precluded electrocardio- gram-gated acquisition in 3 patients with nonischemic and 2 patients with ischemic cardiomyopathy. Addi- tionally, 1 patient with ischemic cardiomyopathy was excluded from analysis because of complete absence of photon counts in a large territory, which precluded assessment of wall motion in that region. Left and right ventricular sizes were similar in the 2 groups. Patients with ischemic cardiomyopathy had more fo- cal wall motion abnormalities, whereas patients with nonischemic cardiomyopathy had more uniform global systolic dysfunction. Accordingly, the variabil- ity in segmental wall motion was significantly lower in patients with nonischemic cardiomyopathy, com- pared with those with ischemic cardiomyopathy (vari- ance 0.27 IT 0.28 vs 1.08 5 0.77, respectively, p <O.Ol). Similarly, the regional wall motion variability (per vascular territory) was also significantly lower in patients with nonischemic cardiomyopathy than those with ischemic cardiomyopathy (0.08 + 0.08 vs 0.49 + 0.31, respectively, p <O.OOl) (Figure 4). Vari-
ability in regional wall motion cor- rectly classified etiology of cardio- myopathy in 36 of 37 patients (97%).
Discriminants of ischemic from nonischemic cardiomyopathy: Uni- variate analysis identified the summed stress and rest perfusion de- fect scores as the best parameters for classification of patients with cardio- myopathy. Both these indexes com- pletely separated patients in the 2 groups. Because of such ideal sepa- ration, these 2 variables were ex- cluded from analysis for the con- struction of a multivariate logistic re- gression model. In the multivariable model, regional wall motion variabil- ity was identified as the only predic- tor of ischemic versus nonischemic
TABLE II Myocardial Perfusion and Gated Single-Photon Emission Computed Tomography Data in 37 Patients With Dilated Cardiomyopathy
Nonischemic lschemic Cardiomyopathy Cardiomyopathy p Value
Left ventricular stress cavity size* 2.96 + 0.81 2.54 + 0.88 0.23
Left ventricular rest cavity size* 2.96 k 0.81 2.54 2 0.88 0.23 Right ventricular stress cavity size* 2.00 2 1.15 1.11 2 1.05 0.068 Right ventricular systolic function* 1.63 + 1.30 1.11 ~0.78 0.37 Variability in segmental wall motion+ 0.27 + 0.28 1.18 + 0.81 10.001 Regional wall motion variability$ 0.08 + 0.02 0.58 ? 0.10 <O.OOl
*Left and right ventricular size and right ventricular function were scored on a 0 to 4 scale (see
Methods).
Variability is expressed CIS the variance of +individuol or &rage (per vascular territory) wall motion
scores (scale 0 to 5, see Methods).
all nonischemic patients) (Figure 2). The summed rest defect scores also had no overlap between ischemic and nonischemic patients (29.92 k 9.28 vs 5.96 2 3.64, respectively, p <O.OOl). In contrast, there was patient overlap for summed reversibility scores, de- spite the statistically significant difference between ischemic and nonischemic cardiomyopathy groups (3 2 3.49 vs 0.96 2 2.33, respectively, p <O.OOl).
Patients with nonischemic cardiomyopathy fre- quently (83%) had mild and nonreversible defects in the right coronary artery distribution. The average stress perfusion score of this territory (0.92 k 0.58) was higher than that of the left anterior descending coronary artery (0.24 2 0.24, p <O.OOl) and the left
etiology of cardiomyopathy (OR 0.14,95% CI 0.02 to 1.01, p = 0.05). None of the clinical indexes were identified as statistically significant discriminators be- tween ischemic and nonischemic cardiomyopathy. The combined use of myocardial perfusion imaging and regional wall motion by gated SPECT imaging resulted in even wider separation of patients with ischemic cardiomyopathy and those with nonischemic cardiomyopathy (Figure 5).
DISCUSSION This prospective study demonstrates that techne-
tium-99m gated SPECT sestamibi exercise imaging, with combined assessment of myocardial perfusion
1256 THE AMERICAN JOURNAL OF CARDIOLOGY~ VOL. 82 NOVEMSER 15, 1998

0.00 /
T
A lschemic Nonischemic
Cardiomyopathy Cardiomyopathy
FIGURE 4. Individual patient wall motion variance among vascu- lar territories, for ischemic and nonischemic cardiomyopathy groups. The horizontal solid lines inside the boxes represent the median values. The doffed lines represent the mean group val- ues. The upper and lower box borders indicate the 75th and 25th percentiles, respectively. The whisker caps represent the 95th and 5th percentiles.
50 T
h
o&z : / 0.0 0.2 0.4 0.6 0.8 1.0 1.2 1.4
Regional Wall Motion Varibility (Variance)
FIGURE 5. Combined assessment of m ocardial perfusion and regional wall motion clearly separa drtients with ischemic cardiomyopathy [open hiangles) from ose with nonischemic cardiomyopathy (black circles].
and function, can clearly and accurately differentiate ischemic from nonischemic cardiomyopathy in a se- lected series of patients with documented left ventric- ular dysfunction. The summed stress and rest perfu- sion defect scores, and the regional wall motion vari- ability were the best discriminants.
Myocardial perfusion imaging-comparison with previous studies: Previous studies have shown that patients with ischemic cardiomyopathy have more ex- tensive and more severe defects than patients with nonischemic cardiomyopathy.5J.1 i However, the ex- tent, severity, or reversibility of perfusion defects had considerable overlap between groups,2-5,8,9,20 preclud- ing the use of noninvasive myocardial perfusion im- aging alone for accurate classification of individual patients. The etiology of such perfusion defects re-
mains unclear, although a variety of possible expla- nations have been proposed.3-5,7,8.11.*1,**
In the present study, myocardial perfusion imaging with technetium-99m could clearly separate patients with ischemic cardiomyopathy from those with non- ischemic cardiomyopathy. The favorable imaging characteristics of technetium-99m agents over thalli- um-201 (particularly for SPECT and gated SPECT imaging) likely account for the wide group separation. The frequent, mild inferior-fixed defects seen in our study were similar to those seen by positron emission tomography. I 1 The location and characteristics of these defects in a cohort of primarily male patients suggests that diaphragmatic attenuation is the likely explanation. Finally, the wide group separation may partially be due to inclusion only of patients with well-defined ischemic and nonischemic cardiomyop- athy. For example, patients with left bundle branch block were excluded, and this conduction abnormality is known to cause anterior wall and septal perfusion defects, even in the absence of epicardial coronary disease.*3,24
Regional wall motion: Nonischemic cardiomyopa- thy has been reported to have uniform systolic dys- function, whereas ischemic cardiomyopathy is char- acterized by more focal regional abnormali- ties,‘,l i,r4,16,25 but significant group overlap has been reported.5.9,12-i7 Using a semi-quantitative assessment of segmental wall motion, we were able to almost completely separate patients with ischemic cardiomy- opathy from those with nonischemic cardiomyopathy. The assessment of gated SPECT regional systolic function appeared to augment the group differences of stress myocardial perfusion, accentuating the separa- tion between ischemic and nonischemic groups. Thus, we believe that the combined evaluation of regional perfusion and wall motion offers potential advantages in the diagnosis and evaluation of patients with car- diomyopathy. However, the use of gated SPECT in this patient population may be limited by arrhythmias or poor counts in territories of severe perfusion de- fects.
Clinical parameters in cardiomyopathy: The distinc- tion between ischemic and nonischemic cardiomyop- athy cannot be made on clinical grounds (including history, physical examination, resting and exercise electrocardiogram) alone. 7x26-*8 Our findings agree with previous studies. Although the prognostic signif- icance of peak exercise VO, in patients with cardio- myopathy has been established,*” it has not been pre- viously examined as a potential discriminator between ischemic and nonischemic patients. The considerable overlap and the small group difference in peak VO, in our study indicate that peak exercise VO, is unlikely to be a helpful index in differentiating etiologies of cardiomyopathy.
Study limitations: Most of our patients were men. Ins a recent study including patients with ischemic and nonischemic cardiomyopathy,3O men exercised longer and had higher peak VO, than women. Additionally, gender differences in nuclear imaging exist in patterns of soft tissue attenuation (i.e., breast vs diaphragm
METHODS,‘GATED SPECT IMAGING IN CARDIOMYOPATHY 1257

causing anterior vs inferior attenuation, respectively). Thus, the utility of gated SPECT should be validated in a larger population with more women. The small degree of reversibility found in the present study in patients with ischemic cardiomyopathy is probably related to patient selection criteria: only clinically stable patients were included and only a small per- centage of the patients with ischemic cardiomyopathy had exertional angina. Therefore, reversibility of per- fusion defects may have additional value in differen- tiating ischemic from nonischemic cardiomyopathy. Finally, we evaluated a well-defined population with a clear-cut distinction between ischemic and nonisch- emit cardiomyopathy. Patients with nonischemic car- diomyopathy, but also co-existent coronary athero- sclerosis, may have different image characteristics.
Acknowledgment: The authors would like to thank Mary-Beth Barry, RN, Laura Kearney, RN, Erin Proc- tor, RN and Beth Vossler, RN, for valuable assistance with patient recruitment and data collection, and Mi- chael White, CNMT, for his excellent technical assis- tance.
1. Bulkley BH, Hutchins GM, Bailey I, Strauss HW, Pitt B. Thallium-201 imaging and gated blood pool scans in patients with ischemic and idiopathic congestive cardiomyopathy: a clinical and pathologic study. Circulation 1977: 55553-760. 2. Saltissi S, Hockings B, Croft DN, Webb-Peploe MM. Thallium-201 myocar- dial imaging in patients with dilated and ischemic cardiomyopathy. Br Heart .I 1981;46:290-295. 3. Dunn RF, Uren RF, Sadick N, Bautovich G, McLaughlin A, Hiroe M, Kelly DT. Comparison of thallium-201 scanning in idiopathic dilated cardiomyopathy and severe coronary artery disease. Circulation 1982;66:804-810. 4. Iskandtian AS, Hakki AH, Kane S. Resting thallium-201 myocardial perfusion patterns in patients with severe left ventricular dysfunction: differences between patients with primary cardiomyopathy, chronic coronary artery disease, or acute myocardial infarction. Am Heart J 1986; 111:760-767. 5. Eichhom EJ. Kosinski EJ, Lewis SM, Hill TC, Emend LH, Leland OS. Usefulness of dipyridamole-thallium-201 perfusion scanning for distinguishing ischemic from nonischemic cardiomyopathy. Am .I Cordial 1988;62:945-951. 6. Glamann DB, Lange RA, Corbett JR, Hillis LD. Utility of various radionuclide techniques for distinguishing ischemic from nonischemic dilated cardiomyopa- thy. Arch Intern Med 1992;152:769-772. 7. Chikamori T, Doi YL, Yonezawa Y, Yamada M, Seo H, Ozawa T. Value of dipyridamole thallium-201 imaging in noninvasive differentiation of idiopathic dilated cardiomyopathy from coronary artery disease with left ventricular dys- function. Am .I Cardiol 1992;69:650-653. 8. Taoberg SG, Orie JE, Bartlett BE, Cottington EM, Flares AR. Usefulness of thallium-201 for distinction of ischemic from idiopathic dilated cardiomyopathy. Am J Cardiol 1993;71:674-680. 9. Juilli&e Y. Marie PY, Danchin N, Gillet C, Paille F, Karcher G, Bertrand A, Cherrier F. Radionuclide assessment of regional differences in left ventricular wall motion and myocardial perfusion in idiopathic dilated cardiomyopathy. Eur Heart J 1993;14:1163-1169. 10. Eisenberg JD, Sobel BE, Geltman EM. Differentiation of ischemic from nonischemic cardiomyopathy with positron emission tomography. Am J Cardiol 1987;59:1410-1414.
11. Mody VF, Bnmken RC, Warner Stevenson L, Nienaber CA, Phelps ME, Schelbect HR. Differentiating cardiomyopathy of coronary artery disease from nonischemic dilated cardiomyopathy utilizing positron emission tomography. JAm Co/l Cardiol 1991;17:373-383. 12. Wallis DE, O’Connell JB, Henkin RE, Constanzo-Nordin MR. Scanlon PJ. Segmental wall motion abnormalities in dilated cardiomyopathy: a common finding and good prognostic sign. J Am Co11 Cardiol 1984;4:674-679. 13. Greenberg JM. Murphy JH, Okada RD, Pohost GM, Strauss HW, Boucher CA. Value and limitations of radionuclide artetiography in determining the cause of reduced left ventricular ejection fraction: comparison of idiopathic dilated cardiomyopathy and coronary artery disease. Am J Cardiol 1985;55:541-544. 14. Shors CM, Kozul VJ, Henderson F. The differential diagnosis of congestive cardiomyopathy and ischemic cardiomyopathy by echocardiography. Angiology 1975;26:723-733. IS. Medina R, Panidis IP, Morganroth J, Kotler MN, Mintz GS. The value of echocardiogmphic regional wall motion abnormalities in detecting coronary artery disease in patients with or without a dilated left ventricle. Am Heart J 1985;109:799-803. 16. Diaz RA, Nihoyannopoulos P, Athanassopoulos G, Oakley CM. Usefulness of echocardiography to differentiate dilated cardiomyopathy from coronary- induced congestive heart failure. Am J Cardiol 1991;68:1224-1227. 17. Sharp SM. Sawada SG, Segar DS, Ryan T, Kovacs R, Fineberg NS, Feigen- baum H. Dobutamine stress echocardiography: detection of coronary artery disease in patients with dilated cardiomyopathy. J Am Co11 Cardiol 1994;24: 934-939. 18. German0 G, Kiat H, Kavanagh PB, Moriel M, Mazzanti M, So HT, Van Train KF. Berman DS. Automatic quantification of ejection fraction from gated myo- cardial perfusion SPECT. J Nucl Med 1995:36:2138-2147. 19. Kiat H, Maddahi J, Roy LT, Van Train K, Friedman J, Resser K, Berman DS. Comparison of technetium-99m methoxy-isobutetyle and thallium-201 for eval- uation of coronary artery disease by planar and tomographic methods. Am Heart J 1989;117:1-11. 20. Doi YL, Chikamori T, Tukata J, Yonezawa Y, Poloniecki JD, Ozawa T, McKenna WJ. Prognostic value of thallium-201 perfusion defects in idiopathic dilated cardiomyopathy. Am J Cardiol 1991;67: 188-193. 21. Factor SM, Minase T, Cho S, Dominitz R, Sonneblick EH. Microvascular spasm in the cardiomyopathic Syrian hamster: a preventable cause of focal myocardial necrosis. Circularion 1982;66:342-354. 22. Gewirtz H, Grotte GJ, SFauss HW, O’Keefe DD, Akins CW, Daggett WM. Pohost GM. The influence of left ventricular volume and wall motion on myo- cardial images. Circulation 1979;59: 1172-l 177. 23. Knapp WH, Bentmp A, Schmidt U, Ohlmeier H. Myocardial scintigmphy with thallium-201 and technetium-99m-hexakis-methoxyisobutylisonitrile in left bundle branch block: a study in patients with and without coronary artery disease. Eur J Nucl Med 1993;20:219-224. 24. O’Keefe JH Jr, Bateman TM, Barnhart CS. Adenosine thallium-201 is superior to exercise thallium-201 for detecting coronary artery disease in patients with left bundle branch block. J Am Co11 Cardiol 1993;21:1332-1338. 25. Goldman MR, Boucher CA. Value of radionuclide imaging techniques in assessing cardiomyopathy. Am J Cardiol 1980;46:1232-1236. 26. Johnson RA, Palacios I. Dilated cardiomyopathies of the adult (second of two parts). N Engl JMed 1982;307:1119-1126. 27. Gau GT, Goodwin JF, Oakley CM, Olsen EG, Rahimtoola SH, Raphael MJ, Steiner RE. Q waves and coronary arteriography in cardiomyopathy. Br Heart J 1972;34:1034-1041. 28. Franciosa JA, Park M, Levine TB. Lack of correlation between exercise capacity and indexes of left ventricular pelfomunce in heart failure. Am J Cnrdiol 1981;47:33-39. 29. Stelken AM, Younis LT, Jennison SH, Miller DD, Miller LW, Shaw LJ, Kargl D, Chaitman BR. Prognostic value of cardiopulmonary exercise testing using percent achieved of predicted peak oxygen uptake for patients with isch- emit and dilated cardiomyopathy. J Am Coil Cardiol 1996;27:345-352. 30. Daida H, Allison TG, Johnson BD, Squires RW, Gau GT. Comparison of peak exercise oxygen uptake in men versus women in chronic heart failure secondary to ischemic or idiopathic dilated cardiomyopathy. Am J Cnrdiol 1997;80:85-88.
1258 THE AMERICAN JOURNAL OF CARDIOLOGY@ VOL. 82 NOVEMBER 15, 1998