Embed Size (px)
Citation preview

1
Colorectal cancer screening in First Nations People living in Manitoba
Kathleen M. Decker1,2, Alain A. Demers1,3, Erich V. Kliewer1,3,4, Grace Musto3, Emma Shu3,
Natalie Biswanger2, Brenda Elias1, Jane Griffith1,3, Donna Turner1,3
1. Department of Community Health Sciences, University of Manitoba, Winnipeg, Manitoba
2. Screening Programs, CancerCare Manitoba, Winnipeg, Manitoba
3. Epidemiology and Cancer Registry, CancerCare Manitoba, Winnipeg, Manitoba
4. Cancer Control Research, British Columbia Cancer Agency, Vancouver, British Columbia
Running title: Colorectal cancer screening in First Nations people
Key words: cancer, colorectal, Indigenous health, mass screening,
Financial support: This work was supported by the Canadian Institute of Health Research
(CIHR-AQC 83508).
Corresponding author: Dr. Donna Turner, Epidemiology and Cancer Registry, CancerCare
Manitoba, 675 McDermot, Winnipeg, Manitoba R3E 0V9,
Tel: 204-787-2573
Email: [email protected]
Conflicts of interest: The authors of this study declare that there are no conflicts of interest that
could bias the results of this study. The results and conclusions presented are those of the
authors. No official endorsement by Manitoba Health is intended or should be inferred.
Word count: 3,733
Total number of tables and figures: 6
on May 29, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on October 21, 2014; DOI: 10.1158/1055-9965.EPI-14-1008

2
Abstract
Background: Since the burden of colorectal cancer (CRC) appears to be increasing in First
Nations, it is important to better understand CRC screening utilization. The objective of this
study was to describe CRC screening among First Nations living in Manitoba.
Methods: The Federal Indian Register was linked to two provincial databases. A negative
binomial model was used to compare the probability of First Nations having a fecal occult blood
test (FOBT), colonoscopy, or flexible sigmoidoscopy (FS) with all other Manitobans.
Results: First Nations who lived Winnipeg were significantly less likely to have had a FOBT in
the previous two years than all other Manitobans who lived in Winnipeg (Rate Ration
(RR)=0.40, 95% Confidence Interval (CI) 0.37-0.44). There was no difference in the likelihood
of having a colonoscopy or FS for First Nations individuals who resided in northern Manitoba
compared all other Manitobans (RR=1.04, 955 CI 0.91-1.19). However, First Nations who lived
in the rural south or urban areas were less likely than all other Manitobans to have had a
colonoscopy or FS (RR=0.81, 95% CI 0.75-0.87, rural south; RR=0.86, 95% CI 0.81-0.92,
urban).
Conclusions: First Nations living in Winnipeg were significantly less likely to be screened for
CRC using the FOBT. Colonoscopy and FS use depended on area of residence.
Impact: First Nations experience barriers that impede the use of CRC screening. Further
research is needed to understand these barriers to extend the benefit of CRC screening to this
population.
on May 29, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on October 21, 2014; DOI: 10.1158/1055-9965.EPI-14-1008

3
Introduction
Colorectal cancer (CRC) is the third most common cancer and the second most frequent
cause of cancer deaths among Canadians (1). Although it is responsible for a large component of
cancer burden, CRC incidence in Canada has been declining in men and women since 2000 (1).
Recent analyses in Manitoba have also found that the incidence of CRC in the province has
decreased (2). However, when examined by ethnicity, CRC incidence for First Nations
individuals has increased over time. The age-standardized CRC incidence increased from 29.6
per 100,000 in 1984-88 to 79.0 per 100,000 in 2004-08 for First Nations individuals but
decreased from 68.4 per 100,000 in 1984-88 to 66.8 per 100,000 in 2004-08 for all other
Manitobans (2).
The observed reduction in CRC incidence among in Canada and all other Manitobans is
likely due to changes in exposures to risk factors and the early detection and removal of
precancerous polyps through screening. Several large randomized controlled trials have found
that screening for CRC using the guaiac-based fecal occult blood test (FOBT) reduced mortality
from CRC by 15 to 33% (3). In 2001, the Canadian Task Force on Preventive Health Care
recommended screening for CRC using a FOBT annually or biennially or flexible
sigmoidoscopy (FS) (with an unspecified interval) for average risk individuals over 50 years of
age (4). The Canadian Association of Gastroenterology currently recommends that average risk
individuals over 50 years of age be screened with a FOBT every two years, FS every five years,
or colonoscopy every ten years (5).
Presently, Canadian provincial screening guidelines vary slightly with respect to the
population eligible for screening and the type of FOBT recommended (guaiac-based FOBT or
fecal immunochemical test (FIT)) but the majority recommend screening using a FOBT or FIT
on May 29, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on October 21, 2014; DOI: 10.1158/1055-9965.EPI-14-1008

4
every two years for individuals 50 to 74 years of age with colonoscopy follow-up for positive
screening results (6). Although the sensitivity of colonoscopy is higher than FOBT, since
colonoscopy can result in serious harms such as bowel perforation, it is not currently
recommended by any province for population-based screening (7).
In 2007, Manitoba launched a province-wide CRC screening program using the guaiac-
based FOBT Hemoccult II SENSA for average risk individuals 50 to 74 years of age. At that
time, 44% of Manitobans 50 to 74 years of age reported having had a FOBT in the previous two
years (8). Previous Canadian studies have examined screening for breast and cervical cancer
among First Nations people but none have examined the utilization of CRC screening. Since the
burden of CRC appears to be increasing in First Nations communities, it is important to
understand CRC screening utilization among First Nations people. The objective of this study
was to describe the frequency of CRC screening among First Nations people living in Manitoba
in comparison to all other Manitobans.
Materials and Methods
Setting and Population
The province of Manitoba, located in central Canada, has a population of approximately
1.2 million. Half of the population lives in the capital city of Winnipeg. In 2011, there were
105,815 registered First Nations individuals living in Manitoba, which represented 8.8% of the
provincial population (9). Registered refers to those First Nations individuals who, under the
Federal Indian Act, are entitled to Treaty rights (10). First Nations groups in Manitoba include
Ojibway, Cree, Ojibway-Cree, Dakota, and Dene. First Nations are the largest Indigenous group
in Canada (45.5% of the total Indigenous population living in Canada that includes First Nations,
Inuit, Métis and 1.9% of the total Canadian population) (11). First Nations individuals reside in
on May 29, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on October 21, 2014; DOI: 10.1158/1055-9965.EPI-14-1008

5
urban and rural areas including 63 First Nations communities in Manitoba some of which are
isolated, northern communities (9).
Data sources
Three data sources were used for this study: the Federal Indian Register, the Manitoba
Health Population Registry (MHPR), and the Medical Claims database. The Federal Indian
Register is the official record identifying Registered Indians in Canada. Registered Indians are
people who are registered with the federal government as defined by the Federal Indian Act (12).
Registered Indians have certain rights and benefits that are not available to non-registered
Indians or Métis people. The Indian Register was initiated in 1951 which explains the use of the
outdated term “Indian” instead of First Nations. Permission from Aboriginal Affairs and
Northern Development Canada (the federal data steward) was received to link the Federal Indian
Register to the MHPR (13). The MHPR includes all Manitoba residents covered by the
Manitoba Health insurance program (approximately 99% of the population). Through a multi-
step data linkage process, registered First Nations individuals were identified in the MHPR
creating a First Nations file (13). The Indian Register file contained 143,274 records; 133,882
(93.4%) were successfully linked to the MHPR. This de-identified First Nations file also
included a scrambled identifier unique to CancerCare Manitoba.
The First Nations file was then linked to the Medical Claims database using the
scrambled identifier to identify individuals who had had a FOBT, colonoscopy, or FS. The
provincial Medical Claims database is generated by claims filed by physicians for payment of
services and includes a billing tariff code, service date, an International Classification of
Diseases 9th version (ICD-9) diagnosis code, and provider identification. Both the MHPR and
on May 29, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on October 21, 2014; DOI: 10.1158/1055-9965.EPI-14-1008

6
the Medical Claims databases have been previously validated for accuracy and have been used
extensively to study many health outcomes (14,15).
A person was considered screened for CRC if they had at least one medical claim with a
FOBT tariff code in the two years before the last day of the screening time period and/or a
colonoscopy or flexible sigmoidoscopy in the five years before the last day of the screening time
period. Individuals who lived outside of Winnipeg were excluded from the analyses that only
examined FOBT use because a significant proportion of FOBTs in rural and northern areas are
not registered in the Medical Claims database. Therefore, rural and northern FOBT rates likely
underestimate the true FOBT utilization rate.
Statistical analyses
Descriptive statistics were used to illustrate the characteristics of the individuals in the
study. Negative binomial regression modelling was used to compare the rates of FOBT,
colonoscopy, and flexible sigmoidoscopy use in First Nations and all other Manitobans. The
following co-variables were included in the regression model: age group (50-54, 55-59, 60-64,
65-69, and 70-74), gender (female and male), area of residence (urban, north, and rural south),
and time period. These variables were included since previous research has found that CRC
screening increases with age, is higher for females than males, and may be lower for individuals
who live in a rural area (16,17). For FOBT, time period was defined as the two years prior to
December 31st of each index year. For colonoscopy and FS, time period was defined as the five
years prior to December 31st of each index year. Index years were 1996, 1998, 2000, 2002,
2004, 2006, and 2008. All analyses were conducted in SAS version 9.2 (SAS Institute Inc.,
Cary, NC).
on May 29, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on October 21, 2014; DOI: 10.1158/1055-9965.EPI-14-1008

7
Ethics approvals were received from the University of Manitoba Health Research Ethics
Board, Manitoba Health’s Information Privacy Committee, the Research and Resource Impact
Committee at CancerCare Manitoba, and the Assembly of Manitoba Chief’s Health Information
and Research Governance Committee.
Results
Between 1995-96 and 2007-08, 453,124 AOM and 18,416 First Nations individuals 50
and 74 years of age were identified as living in Manitoba. Table 1 shows the characteristics of
First Nations and all other Manitobans in 1995-96 compared to 2007-08. Overall, the
distribution of demographic characteristics in 2007-08 did not change substantially from 1995-
96. In 1995-96, 2.6% of all other Manitobans lived in the north compared to 38.7% of First
Nations. This distribution changed only slightly in 2007-08 (2.6% of all other Manitobans lived
in the north compared to 36.8% of First Nations). In 1995-96, fewer all other Manitobans were
50-54 years of age (25.5%) compared to First Nations (32.4%) and more were 70-74 years of age
(17.3% for all other Manitobans compared to 9.3% for First Nations). By 2007-08, 28% of all
other Manitobans were 50-54 years of age and 12.2% were 70-74 years of age while 35% of First
Nations individuals were 50-54 years of age and 8.7% were 70-74 years of age. The sex
distribution was similar in both time periods (51.5% of all other Manitobans and 51.4% of First
Nations individuals were female).
FOBT use
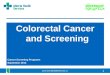
Figure 1 shows the percentage of First Nations and all other Manitobans who resided in
Winnipeg who had an FOBT in the two years before the last day of each index year. For First
Nations individuals, FOBT use increased from 4.9% (95% Confidence Interval (CI) 3.9-5.9) in
1995-96 to 13.4% (95% CI 12.3-14.6) in 2007-08 (p<0.0001). For all other Manitobans who
on May 29, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on October 21, 2014; DOI: 10.1158/1055-9965.EPI-14-1008

8
resided in Winnipeg, FOBT use increased from 12.2% (95% CI 12.0-12.3) in 1995-96 to 32.9%
(95% CI 32.7-33.1) in 2007-08 (p<0.0001). The average percentage change in FOBT rates per
two-year time period from 1995-96 to 2007-08 was 20.0% for First Nations and 18.2% for all
other Manitobans. However, the gap in FOBT use between First Nations and all other
Manitobans increased from 7.3% in 1996 to 19.5% in 2008 (Table 2). In all time periods, FOBT
rates were higher for all other Manitobans than for First Nations (p<0.0001).
After adjusting for gender, age group, and time period, First Nations individuals who
resided in Winnipeg were significantly less likely than all other Manitobans who resided in
Winnipeg to have had an FOBT (Rate Ratio (RR)=0.40, 95% CI 0.37-0.44, p=0.0001) (Table3).
Men were less likely to be screened for CRC in the previous two years using an FOBT than
women (RR=0.88, 95% CI 0.85-0.92, p=0.002). FOBT use was highest for individuals 65 to 69
years of age compared to those 50 to 54 years of age (RR=1.65, 95% CI 1.53-1.77, p=0.08) and
increased with time (RR=2.80, 95% CI 2.70-2.90, p=0.02 for 2007-2008 compared to 1995-96).
There were no significant interactions between any of the variables.
FOBT, colonoscopy, and flexible sigmoidoscopy use
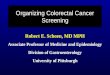
Figure 2 shows the percentage of First Nations and all other Manitobans 50 to 74 years of
age who resided in Winnipeg who had an FOBT in the two years or a colonoscopy or FS in the
five years before the last day of each index year. In all time periods, FOBT, colonoscopy, and
FS rates were lower for First Nations compared to all other Manitobans and the differential
increased over time (p<0.0001). For First Nations who resided in Winnipeg, FOBT,
colonoscopy, or FS use increased from 11.7% (95% CI 10.2-13.2) in 1996 to 25.5% (95% CI
24.1-27.0) in 2008 (p<0.0001). For all other Manitobans who resided in Winnipeg, FOBT,
colonoscopy, or FS use increased from 18.8% (95% CI 18.6-19.0) in 1996 to 42.9% (95% CI
on May 29, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on October 21, 2014; DOI: 10.1158/1055-9965.EPI-14-1008

9
42.7-43.1) in 2008 (p<0.0001). The gap in FOBT, FS, and colonoscopy use between First
Nations and all other Manitobans increased from 17.1% in 1996 to 17.4% in 2008 (Table 2).
Colonoscopy or flexible sigmoidoscopy use
Although FOBT data were only available for the city of Winnipeg, information on
colonoscopy and FS use was available for the entire province. For First Nations in Manitoba, the
rate of colonoscopy or FS use increased from 5.9% (95% CI 5.4-6.5) during 1992-96 to 12.8%
(95% CI 12.2-13.4) during 2004-08. For all other Manitobans, the rate of colonoscopy or FS use
increased from 8.2% (95% CI 8.1-8.3) in 1992-96 to 17.3% (95% CI 17.2-17.4) in 2004-08.
Figure 3 illustrates the percentage of First Nations and all other Manitobans who had a
colonoscopy or FS in the five years before the last day of each index year by area of residence.
In the north, the percentage of individuals who had a colonoscopy or FS was similar or slightly
higher for First Nations (5.2%, 95% CI 4.5-6.0 from 1992-96 to 11.4%, 95% CI 10.5-12.3 from
2004-08) compared to all other Manitobans (4.7%, 95% CI 4.2-5.3 from 1992-96 to 10.6%, 95%
CI 9.9-11.3 from 2004-08). In the rural south, the percentage of individuals who had a
colonoscopy or FS was lower for First Nations (5.6%, 95% CI 4.8-6.4 from 1992-96 to 12.6%,
95% CI 11.7-13.5 from 2004-08) compared to all other Manitobans (6.9%, 95% CI 6.7-7.1 from
1992-96 to 19.9%, 95% CI 16.7-17.1 from 2004-08). Lower rates of colonoscopy or FS use for
First Nations compared to all other Manitobans were also observed in urban areas (7.7%, 95% CI
6.5-8.9 from 1992-96 to 14.9%, 95% CI 13.8-16.1 from 2004-08 for First Nations and 9.0%,
95% CI 8.8-9.1 from 1992-96 to 17.8%, 95% CI 17.6-17.9 from 2004-08 for all other
Manitobans).
Table 4 shows the relative rate of having a colonoscopy or FS in the previous five years
by ethnicity, residence, gender, age group, and index year. In the unadjusted models, there was
on May 29, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on October 21, 2014; DOI: 10.1158/1055-9965.EPI-14-1008

10
no difference in the likelihood of having a colonoscopy or FS for First Nations individuals
compared to all other Manitobans (RR=0.90, 95% CI 0.77-1.05, p=0.21). After adjusting for
area of residence, gender, age group, and year, there was a significant interaction between
ethnicity and residence. In the rural south and urban areas, First Nations were less likely than all
other Manitobans to have a colonoscopy or FS (RR=0.81, 95% CI 0.75-0.87 for the rural south,
RR=0.86, 95% CI 0.81-0.92 for urban areas, p=0.02). However, there was no difference in the
likelihood of having a colonoscopy or FS for First Nations and all other Manitobans who lived in
the north (RR=1.04, 95% CI 0.91-1.19). Males were significantly less likely to have had a
colonoscopy or FS compared to females (RR=0.82, 95% CI 0.78-0.86), p<0.0001). The relative
rate of colonoscopy and FS use increased with age (RR=1.21, 95% CI 1.14-1.29 for 50-54 years
of age to 1.85, 95% CI 1.68-2.02 for 70-74 years of age, p<0.0001) and time period (RR=1.17,
95% CI 1.14-1.19 for 1996 to 2.23, 95% CI 21.3-2.35 for 2008, p<0.0001).
Discussion
Previous analyses have found that the CRC incidence among First Nations individuals
living in Manitoba has increased over time (2). This trend has also been observed in other
jurisdictions; American Indians and Alaska Natives who live in the Unites States have a higher
burden of CRC and stable or increasing CRC mortality (18). Population-based, organized
screening using an FOBT is an important strategy that can help reduce the incidence and
mortality of CRC. Our study found that over time, the rate of FOBT use has increased for both
FN and AOMs living in Winnipeg but the participation of First Nations individuals remained
significantly lower than that for all other Manitobans (13.4% for First Nations in 2008 compared
to 32.7% for all other Manitobans). In addition, the gap in screening rates between First Nations
and all other Manitobans has increased over time. The first CRC screening guidelines appeared
on May 29, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on October 21, 2014; DOI: 10.1158/1055-9965.EPI-14-1008

11
in the United States in late 1990s and in Canada in 2001; compliance with these guidelines is
likely to occur earlier and more rapidly among individuals that have fewer barriers to screening
which may partially explain the observed gap (4,19).
Screening, regardless of ethnicity, remains below the recommended Canadian national
target of 60% (20). These findings are consistent with other studies examining FOBT use among
Indigenous groups outside of Canada. In the United States, CRC screening rates using the FOBT
are lower for American Indians compared to other ethnic groups (21,22). In Australia, 17% of
individuals who identified themselves as Indigenous accepted an offer of FOBT use compared to
38.6% of non-Indigenous people (23).
Our study also found that the rate of colonoscopy or FS in the province has increased
over time for First Nations although the rate was significantly lower than that for all other
Manitobans. As well, the likelihood of having a colonoscopy or FS depended on area of
residence. First Nations individuals who lived in northern Manitoba had the same rate of
colonoscopy or FS as all other Manitobans while First Nations who lived in the rural south or
urban area were less likely than AOM to have had a colonoscopy or FS. This suggests a referral
inequity for endoscopy services for First Nations individuals based on where they reside in the
province.
Barriers to CRC screening arise from a variety of demographic, psychological, and
provider-related factors (24). In a review of literature on the equity of participation in CRC
screening among different ethnic populations, Javanparast et al. (2010) found that socio-cultural
factors play an important role in the acceptability, accessibility, and utilization of screening (16).
Culturally-specific barriers found among First Nations individuals include speaking an
Indigenous language and perceived discrimination in a health care setting (25,26). Filippi et al.
on May 29, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on October 21, 2014; DOI: 10.1158/1055-9965.EPI-14-1008

12
(2012) explored American Indian women’s barriers to CRC screening and found that
embarrassment, privacy issues, fear of the procedure and possible results, and cost were key
factors in screening participation (27). Logistical issues, such as child care duties, work
schedules, long wait periods, and lack of transportation, were also important barriers (27). The
most common barriers cited among American Indian men were privacy, embarrassment, and
distrust of the health care system (28). American Indian community leaders also felt that there
was little knowledge about CRC, risk factors, or screening recommendations (24).
Additional barriers to CRC screening include the required dietary and drug restrictions
and the practicality of completing the guaiac-based FOBT (29-31). Since its introduction in the
1950s, the use of the guaiac-based FOBT has necessitated the elimination of red meat, high-
peroxidase vegetables, vitamin C, and non-steroidal anti-inflammatory drugs for several days
before and during the testing period. Newer, more sensitive guaiac-based FOBTs, such as the
Hemoccult II SENSA currently used by the CRC screening program in Manitoba, require
removing only vitamin C from the diet. Whether or not a reduction in the number of dietary
restrictions will lead to improved screening participation has yet to be determined.
Research has also found that individuals are more reluctant to participate in CRC
screening if they perceive the test as impractical, awkward, or embarrassing (32-34). The
guaiac-based FOBT requires individuals to apply a small sample from three separate bowel
movements onto a test card with the aid of a cardboard spatula (35). The responsibility for
completing the screening test by the individual and any perceived difficulty may lead to lower
levels of participation. Von Wagner et al. (2011) found that the intention to participate in CRC
screening decreased when participants were given detailed information about how to collect fecal
samples for a guaiac-based FOBT (32). The FIT, which does not require dietary restrictions and
on May 29, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on October 21, 2014; DOI: 10.1158/1055-9965.EPI-14-1008

13
only one stool sample, has been found to result in significantly higher participation rates than the
guaiac-based FOBT (30,36). The effect of using a FIT on screening participation is currently
being evaluated in Manitoba.
Until 2008, CRC screening in Manitoba using the FOBT was provided opportunistically,
which relies on the recommendation and provision of the test by a primary care provider.
However, in a recent survey, only 38% of Manitobans stated that their physician had initiated a
conversation with them about CRC screening (8). Kelly et al. (2007) found that less than 40% of
Native American women and men reported a physician recommendation for FOBT screening
(37). Ideally, providing CRC screening as part of an organized, population-based program
should achieve better accessibility by directly inviting eligible individuals to participate (38).
Since its introduction, the provincial CRC screening program has used several multi-level
strategies to encourage screening participation within First Nations communities, including
working with Health Canada’s First Nations and Inuit Health Branch and local primary health
care providers, sending personalized invitation letters, media messaging, and social marketing
campaigns. Previous research has found that addressing First Nations cultural structures and
traditional ways are important aspects of reducing cancer screening disparities (24,28).
Therefore, further work exploring the comprehensibility of the FOBT kit’s instructions in First
Nations communities and the development of culturally-specific education and training is
underway.
Our findings should be considered in the context of several study limitations. FOBT data
were not available from the Medical Claims database for rural and northern Manitoba.
Therefore, the results for Winnipeg may not be generalizable to other areas of the province. We
were also not able to distinguish between colonoscopy and FS performed for screening versus
on May 29, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on October 21, 2014; DOI: 10.1158/1055-9965.EPI-14-1008

14
those performed because of symptoms or for diagnostic purposes. It is likely in Manitoba that
most colonoscopy and FS are diagnostic since population-based screening using these tests is not
currently recommended.
We did not include any measures of socio-economic status (SES) in the analysis.
Previous studies have found that education and income are often independent predictors of
screening and that differences in screening uptake due to ethnicity are reduced after the
adjustment for SES (39). Finally, this study included registered First Nations who represented
93% of all First Nations living in Manitoba; it did not include First Nations not registered nor did
we distinguish between several distinct First Nations cultural groups. This information,
however, is an important part of collaborating with FN communities and planning local strategies
designed to improve cancer screening in the population.
In summary, First Nations individuals who resided in Winnipeg were significantly less
likely to be screened for CRC using the FOBT. Throughout Manitoba, First Nations who lived
in the north had the same rate of colonoscopy or flexible sigmoidoscopy as all other Manitobans
while First Nations who lived in the rural south or urban area were less likely to have had a
colonoscopy or FS. The disparities identified in FOBT, colonoscopy, and FS use are likely
related to many factors and suggest that barriers to CRC screening exist for First Nations
individuals. Addressing these barriers and improving CRC screening rates are particularly
important since the incidence of CRC in First Nations is increasing and First Nations people
have higher rates of diabetes and obesity which also increase the risk of CRC (11,40-42).
This research on CRC screening provides a baseline which can be used to assess the
effectiveness of new strategies and changes in screening service delivery. Further research is
needed to understand the barriers to CRC screening for First Nations people and to evaluate the
on May 29, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on October 21, 2014; DOI: 10.1158/1055-9965.EPI-14-1008

15
effectiveness of interventions that will help extend the benefit of CRC screening to the entire
population. It is also important that future research include First Nations individuals and health
care providers when identifying barriers and solutions to the lower CRC screening rates observed
in Manitoba. Finally, more analyses are needed to evaluate whether or not the introduction of the
organized, province-wide, population-based CRC screening program in 2008 has improved CRC
screening participation for First Nations people and reduced the gap in screening observed in this
study.
on May 29, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on October 21, 2014; DOI: 10.1158/1055-9965.EPI-14-1008

16
Acknowledgements
We gratefully acknowledge the statistical support of Mr. Pascal Lambert and Dr. Rashid Ahmed.
We also thank the Health Information and Research Committee, Manitoba Health and the Health
Information and Research Committee of the Assembly of Manitoba Chiefs. This work was
supported by the Canadian Institute of Health Research (CIHR-AQC 83508).
on May 29, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on October 21, 2014; DOI: 10.1158/1055-9965.EPI-14-1008

17
References
(1) Canadian Cancer Society's Steering Committee on Cancer Statistics. Canadian Cancer Statistics 2013. Toronto, ON: Canadian Cancer Society; 2013.
(2) Kliewer EV, Demers AA, Elias B, Hall M, Turner D, Musto G. Cancer incidence among status First Nations in Manitoba, Canada. Unpublished manuscript;2014.
(3) Hewitson P, Glasziou PP, Irwig L, Towler B, Watson E. Screening for colorectal cancer using the faecal occult blood test, Hemmocult (Review). Cochrane Database of Systematic Reviews 2011(1).
(4) Canadian Task Force on Preventive Health Care. Colorectal cancer screening. JAMC 2001;25(2):206-208.
(5) Leddin DJ, Enns R, Hilsden R, Plourde V, Rabeneck L, et al. Canadian Association of Gastroenterology position statement on screening individuals at average risk for developing colorectal cancer: 2010. Can J Gastroenterol 2010;24(12):705-714.
(6) Canadian Partnership Against Cancer. Colorectal Cancer Screening in Canada: Program Performance Results Report, January 2009 to December 2011. Toronto, ON: Canadian Partnership Against Cancer; 2013.
(7) Dunfield L, Shane A, Fitzpatrick-Lewis D, Bacchus M. Protocol: Screening for colorectal cancer. Edmonton AB: Canadian Task Force on Preventive Health Care; 2014.
(8) Canadian Partnership Against Cancer. The 2012 Cancer System Performance Report. Toronto, ON: Canadian Partnership Against Cancer; 2012.
(9) Government of Canada. Aboriginal Peoples in Canada: First Nations People, Metis, and Inuit. 2013; Available at: http://www12.statcan.gc.ca/nhs-enm/2011/as-sa/99-011-x/99-011-x2011001-eng.cfm. Accessed July, 2013.
(10) Martens PJ, Sanderson D, Jebamani LS. Mortality comparison of First Nations to All Other Manitobans. Can J Public Health 2005;96(Suppl 1):S33-S38.
(11) Elias B, Kliewer E, Hall M, Demers AA, Turner D, et al. The burden of cancer risk in Canada's indigenous population: a comparative study of know risks in a Canadian region. Int J Gen Medicine 2011;4:699-709.
(12) Jebamani LS, Burchill CA, Martens PJ. Using data linkage to identify First Nations Manitobans. Technical, ethical, and political issues. Can J Public Health 2005;96(1):S28-S32.
(13) Elias B, Busby K. One little, too little: Counting Indigenous people for improved health reporting in Canada. Unpublished Manuscript; 2014.
on May 29, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on October 21, 2014; DOI: 10.1158/1055-9965.EPI-14-1008

18
(14) Roos LL, Mustard CA, Nicol JP, McLarran DF, Malenka DJ, et al. Registries and administrative data: organization and accuracy. Med Care 1993;31(3):201-212.
(15) Robinson JR, Young TK, Roos LL, Gelskey DE. Estimating the burden of disease. Comparing administrative data and self-reports. Med Care 1997;35(9):932-947.
(16) Javanparast S, Ward P, Young G, Wilson C, Carter S, et al. How equitable are colorectal cancer screening programs which include FOBTs? A review of qualitative and quantitative studies. Preventive Medicine 2010;50:165-172.
(17) Canadian Partnership Against Cancer. Examining Disparities in Cancer Control. A System Performance Special Report. Toronto, ON: Canadian Partnership Against Cancer; 2014.
(18) Purdue DG, Haverkamp D, Perkins C, Daley CM, Provost E. Geographic variation in colorectal cancer incidence and mortality, age of onset, and stage at diagnosis among American Indian and Alaska Native People, 1990-2009. Am J Public Health 2014;104(S3):S404-S414.
(19) U.S. Preventive Services Task Force. Screening for Colorectal Cancer: Clinical Summary of U.S. Preventive Services Task Force Recommendation. AHRQ Publication No. 08-05124-EF-4 . AHRQ Publication No 08 05124-EF-4 2008.
(20) Canadian Partnership Against Cancer. Quality determinants and indicators for measuring colorectal cancer screening program performance in Canada. Toronto, ON: Canadian Partnership Against Cancer; 2013.
(21) Espey DK, Wu XC, Swan J, et al. Annual report to the Nation on the status of cancer, 1975-2004, featuring American Indians and Alaska Natives. Cancer 2007;110:2119-2152.
(22) Steele CB, Cardinez CJ, Richardson LC, Tom-Orme L, Shaw KM. Surveillance for health behaviours of American Indians and Alaska Natives - findings from the Behavioral Risk Factor Surveillance System, 2000-2006. Cancer 2008;113(5):1131-1141.
(23) Department of Health and Ageing and AIHW. National Bowel Cancer Screening Program Monitoring Report, 2008. Canberra, Australia; Department of Health and Ageing and AIHW; 2008.
(24) Daley CM, James AS, Filippi M, Weir M, Braiuca S, et al. American Indian community leader and provider views of needs and barriers to colorectal cancer screening. J Health Dispar Res Pract 2012;5(2):1-13.
(25) Schumacher MC, Slattery ML, Lanier AP, et al. Prevalence and predictors of cancer screening among American Indian and Alaska Native people: the EARTH study. Cancer Causes Control 2008;19(7):725-737.
on May 29, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on October 21, 2014; DOI: 10.1158/1055-9965.EPI-14-1008

19
(26) Crawley LM, Ahn DK, Winkleby MA. Perceived medical discrimination and cancer screening behaviors of racial and ethnic minority adults. Cancer Epidemiol Biomarkers Prev 2008;17:1937-1944.
(27) Filippi MK, James AS, Brokenleg S, Talawyma M, Perdue DG, Choi WS, et al. Views, barriers, and suggestions for colorectal cancer screening among American Indian women older than 50 years in the Midwest. J Prim Care Community Health 2012;4(3):160-166.
(28) James AS, Filippi MK, Pacheco CM, Cully L, Perdue D, Choi WS, et al. Barriers to colorectal cancer screening among American Indian men aged 50 or older, Kansas and Missouri, 2006-2008. Prev Chronic Dis 2013;10:130067.
(29) Konrad G. Dietary interventions for fecal occult blood test screening. Can Fam Physician 2010;56:229-238.
(30) Vart G, Banzi R, Minozzi S. Comparing participation rates between immunochemical and guaiac fecal occult blood tests: A systematic review and meta-analysis. Prev Med 2012;55:87-92.
(31) Cole SR, Young GP. Effect of dietary restrictions on participation in faecal occult blood test screening for colorectal cancer. MJA 2001;175:195-198.
(32) von Wagner C, Good A, Smith SG, Wardle J. Responses to procedural information about colorectal cancer screening using faecal occult blood testing: the role of consideration of future consequences. Health Expect 2011;15:176-186.
(33) Consedine NS, Ladwig I, Reddig MK, Broadbent EA. The many faeces of colorectal cancer screening embarrassment: preliminary psychometric development and links to screening outcome. Br J Health Psychol 2011;16:559-579.
(34) Lo SH, Wardle J, von Wagner C. Comparing barriers to colorectal cancer screening with barriers to breast anc cervical screening: a population-based survey of screening-age women in Great Britain. J Med Screen 2013:1-7.
(35) Home screening test (FOBT) instructions. 2013; Available at: http://www.cancercare.mb.ca/home/prevention_and_screening/public_screening/coloncheck/resources/index.cfm#instructions, September, 2013.
(36) Federici A, Rossi PG, Borgia P, Bartolozzi F, Farchi S, Gausticchi G. The immunochemical faecal occult blood test leads to higher compliance than the guaiac for colorectal cancer screening programmes: a cluster randomized controlled trial. J Med Screen 2005;12:83-88.
(37) Kelly KM, Dickinson SL. Colorectal cancer screening in 3 racial groups. Am J Health Behav 2007;31(5):502-513.
on May 29, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on October 21, 2014; DOI: 10.1158/1055-9965.EPI-14-1008

20
(38) Strong K, Wald N, Miller A, Alwan A, WHO Consultation Group. Current concepts in screening for noncommunicable disease: World Health Organization Consultation Group Report on methodology of noncommunicable disease screening. J Med Screening 2005;12:12-19.
(39) O'Malley AS, Forrest CB, Feng S, Mandelblatt JS. Disparities despite coverage. Arch Intern Med 2005;165:2129-2135.
(40) Bruce SG, Riediger ND, Zacharias JM, Young TK. Obesity and obesity-related comorbidities in a Canadian First Nation population. Chronic Dis Can 2010;31(1):27-32.
(41) Dyck R, Osgood N, Lin TH, Gao A, Stand MR. Epidemiology of diabetes mellitus among First Nations and non-First Nations adults. Can Med Assoc J 2010;182(3):249-256.
(42) Jiang Y, Ben Q, Shen H, Lu W, Zhang Y, Zhu J. Diabetes mellitus and incidence and mortality of colorectal cancer: a systematic review and meta analysis of cohort studies. Eur J Epidemiol 2011;26:863-876.
on May 29, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on October 21, 2014; DOI: 10.1158/1055-9965.EPI-14-1008

21
Tables Table 1. Characteristics of registered First Nations and all other Manitobans in 1995-96 and
2007-08
1995-96 All other Manitobans First Nations
Region n % n %
North 5,996 2.6 3,087 38.7
Rural south 79,810 34.4 3,071 38.4
Urban 146,358 63.0 1,829 22.9
Age group
50-54 59,194 25.5 2,587 32.4
55-59 47,273 20.4 2,024 25.3
60-64 43,297 18.6 1,531 19.2
65-69 42,186 18.2 1,103 13.8
70-74 40,214 17.3 742 9.3
Gender
Female 119.650 51.5 4,106 51.4
Male 112,514 48.5 3,881 48.6
Total 232,164 7,987
2007-08
Region n % n %
North 7,828 2.6 4,987 36.8
Rural south 102,140 34.3 5,017 37.0
Urban 188,138 63.1 3,553 26.2
Age group
50-54 83,506 28.0 4,746 35.0
55-59 72,451 24.3 3,353 24.7
60-64 60,947 20.4 2,591 19.1
65-69 44,917 15.1 1,683 12.4
70-74 36,285 12.2 1,184 8.7
Gender
on May 29, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on October 21, 2014; DOI: 10.1158/1055-9965.EPI-14-1008

22
Female 150,732 50.6 7,183 53.0
Male 147,374 49.4 6,374 47.0
Total 298,106 13,557
on May 29, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on October 21, 2014; DOI: 10.1158/1055-9965.EPI-14-1008

23
Table 2. Percent increase (gap) in fecal occult blood test use (FOBT) and FOBT, colonoscopy,
and flexible sigmoidoscopy (FS) use for all other Manitobans compared to First Nations by year
Year 1996 1998 2000 2002 2004 2006 2008 Increase in FOBT use (%)
7.3 8.1 9.9 13.4 15.7 15.7 19.5
Increase in FOBT, colonoscopy and FS use (%)
7.1 8.4 9.4 12.4 13.3 13.9 17.4
on May 29, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on October 21, 2014; DOI: 10.1158/1055-9965.EPI-14-1008

24
Table 3. Relative rates of fecal occult blood test utilization for registered First Nations and all
other Manitobans who lived in Winnipeg by demographic characteristic
Crude model Adjusted model
Number of Individuals*
Rate Ratio
95% CI P Value Rate Ratio
95% CI P Value
Ethnicity <.0001 0.0001
All other Manitobans
113,070 1.00 Ref 1.00 Ref
First Nations 989 0.39 0.32 - 0.49 0.40 0.37 - 0.44
Gender 0.39 0.002
Female 62,155 1.00 Ref 1.00 Ref
Male 51,904 0.84 0.55 - 1.27 0.88 0.85 - 0.92
Age group 0.58 0.08
50-54 51,349 1.00 Ref 1.00 Ref
55-59 51,987 1.30 0.73 - 2.33 1.24 1.17 - 1.32
60-64 47,261 1.48 0.80 - 2.73 1.45 1.37 - 1.54
65-69 43,260 1.69 0.92 - 3.11 1.65 1.53 - 1.77
70-74 39,384 1.64 0.85 - 3.14 1.63 1.50 - 1.78
Year 0.003 0.02
1996 16,707 1.00 Ref 1.00 Ref
1998 18,817 1.07 0.96 - 1.19 1.10 1.08 - 1.13
2000 24,112 1.33 1.18 - 1.50 1.38 1.34 - 1.41
2002 30,940 1.56 1.40 - 1.74 1.69 1.64 - 1.74
2004 37,169 1.75 1.55 - 1.96 1.94 1.89 - 2.00
2006 47,201 2.31 2.12 - 2.50 2.39 2.31 - 2.47
2008 58,295 2.68 2.47 - 2.92 2.80 2.70 - 2.90
Notes: CI – Confidence Interval. Includes Winnipeg residents 50 to 74 years of age who had at
least one fecal occult blood test in the two years before the last day of the index year. In the
adjusted model, each variable was adjusted for all other variables. *The number of individuals in
the age group and year categories will not sum to the total number of individuals in the ethnicity
and gender categories as some individuals may have been screened more than once over the 12
year time frame.
on May 29, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on October 21, 2014; DOI: 10.1158/1055-9965.EPI-14-1008

25
Table 4. Relative rates of colonoscopy or flexible sigmoidoscopy utilization for registered First
Nations and all other Manitobans
Crude model Adjusted model
Number of Individuals*
Rate Ratio
95% CI P-value Rate Ratio
95% CI P-value
Ethnicity 0.21 0.0017
All other Manitobans 91,951 1.00 Ref 1.00 Ref
First Nations 2,975 0.90 0.77 - 1.05 0.86 0.81-0.92
Area of residence 0.0008 0.0002
Urban 158,307 1.00 Ref 1.00
North 6,424 0.67 0.57 - 0.79 0.61 0.55-0.68
Rural south 78,278 0.84 0.72 - 0.99 0.87 0.82-0.92
Area of residence: Ethnicity 0.003 0.02
North: All other Manitobans 3,969 1.00 Ref 1.00 Ref
North: First Nations 2,455 1.12 0.89 - 1.40 1.04 0.91 - 1.19
Rural south: All other Manitobans
75,653 1.00 Ref 1.00 Ref
Rural south: First Nations 2,625 0.80 0.64 - 1.01 0.81 0.75 - 0.87
Urban: All other Manitobans 156,086 1.00 Ref 1.00 Ref
Urban: First Nations 2,221 0.88 0.71 - 1.08 0.86 0.81 - 0.92
Gender 0.001 <.0001
Female 51,407 1.00 Ref 1.00 Ref
Male 43,519 0.78 0.67 - 0.91 0.82 0.78 - 0.86
Age group 0.0003 <.0001
50-54 50,470 1.00 Ref 1.00 Ref
55-59 50,844 1.20 1.00 - 1.43 1.21 1.14 - 1.29
60-64 48,074 1.41 1.17 - 1.70 1.43 1.34 - 1.53
65-69 46,774 1.62 1.34 - 1.95 1.66 1.54 - 1.79
70-74 46,847 1.75 1.45 - 2.12 1.84 1.68 - 2.02
Year <.0001 <.0001
1996 19,428 1.00 Ref 1.00 Ref
1998 22,736 1.19 1.15 - 1.23 1.17 1.14 - 1.19
2000 27,931 1.41 1.36 - 1.47 1.41 1.37 - 1.44
2002 33,655 1.63 1.55 - 1.71 1.64 1.58 - 1.71
2004 39,900 1.86 1.77 - 1.95 1.87 1.79 - 1.95
2006 46,085 2.02 1.92 - 2.13 2.04 1.95 - 2.14
2008 53,274 2.20 2.08 - 2.33 2.23 2.13 - 2.35
on May 29, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on October 21, 2014; DOI: 10.1158/1055-9965.EPI-14-1008

26
Notes: CI – Confidence Interval. Includes Manitoba residents 50 to 74 years of age who had at
least one colonoscopy or flexible sigmoidoscopy in the five years before the last day of the index
year. In the adjusted model, each variable was adjusted for all other variables. *The number of
individuals in the area of residence, age group and year categories will not sum to the total
number of individuals in the ethnicity and gender categories as some individuals may have been
screened more than once over the 12 year time frame.
on May 29, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on October 21, 2014; DOI: 10.1158/1055-9965.EPI-14-1008

27
Figure Legends
Figure 1. Percentage of First Nations and all other Manitobans who lived in Winnipeg and had a
fecal occult blood test by index year
Notes: Includes Winnipeg residents 50 to 74 years of age who had at least one fecal occult blood
test in the two years before the last day of the index year.
Figure 2. Percentage of First Nations and all other Manitobans who lived in Winnipeg and had a
fecal occult blood test, colonoscopy, or flexible sigmoidoscopy by index year
Notes: Includes Winnipeg residents 50 to 74 years of age who had at least one fecal occult blood
test in the two years or a colonoscopy or flexible sigmoidoscopy in the five years before the last
day of the index year.
Figure 3. Percentage of First Nations and all other Manitobans who had a colonoscopy or
flexible sigmoidoscopy by area of residence and index year
Notes: Includes Manitoba residents 50 to 74 years of age who had a colonoscopy or flexible
sigmoidoscopy in the five years before the last day of the index year.
on May 29, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on October 21, 2014; DOI: 10.1158/1055-9965.EPI-14-1008

Figure 1
80
90
100
60
70
80
nt
23 128
32.9
30
40
50
Perc
en
First NationsAll other Manitobans
4.9 5.1 6.5 6.8 7.412.3
13.412.2 13.216.4
20.223.1
0
10
20
01996 1998 2000 2002 2004 2006 2008
Index Year
on May 29, 2018. ©
2014 Am
erican Association for C
ancer Research.
cebp.aacrjournals.org D
ownloaded from
Author m
anuscripts have been peer reviewed and accepted for publication but have not yet been edited.
Author M
anuscript Published O
nlineFirst on O
ctober 21, 2014; DO
I: 10.1158/1055-9965.EP
I-14-1008

Figure 2
90
100
60
70
80
25 524 629.1
32.637.7
42.9
30
40
50
Perc
ent
First NationsAll other Manitobans
11.7 12.215.2 16.7 19.3
23.8 25.518.8 20.6
24.6
10
20
30
01996 1998 2000 2002 2004 2006 2008
Index Year
on May 29, 2018. ©
2014 Am
erican Association for C
ancer Research.
cebp.aacrjournals.org D
ownloaded from
Author m
anuscripts have been peer reviewed and accepted for publication but have not yet been edited.
Author M
anuscript Published O
nlineFirst on O
ctober 21, 2014; DO
I: 10.1158/1055-9965.EP
I-14-1008

Figure 3
18
20
12
14
16
First Nations Urban
8
10
12
Perc
ent
First Nations, UrbanFirst Nations, Rural SouthFirst Nations, NorthAll other Manitobans, UrbanAll other Manitobans Rural South
2
4
6All other Manitobans, Rural SouthAll other Manitobans, North
01996 1998 2000 2002 2004 2006 2008
Index Year
on May 29, 2018. ©
2014 Am
erican Association for C
ancer Research.
cebp.aacrjournals.org D
ownloaded from
Author m
anuscripts have been peer reviewed and accepted for publication but have not yet been edited.
Author M
anuscript Published O
nlineFirst on O
ctober 21, 2014; DO
I: 10.1158/1055-9965.EP
I-14-1008

Published OnlineFirst October 21, 2014.Cancer Epidemiol Biomarkers Prev Kathleen M. Decker, Alain A. Demers, Erich V. Kliewer, et al. ManitobaColorectal cancer screening in First Nations People living in
Updated version
10.1158/1055-9965.EPI-14-1008doi:
Access the most recent version of this article at:
Manuscript
Authoredited. Author manuscripts have been peer reviewed and accepted for publication but have not yet been
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cebp.aacrjournals.org/content/early/2014/10/21/1055-9965.EPI-14-1008To request permission to re-use all or part of this article, use this link
on May 29, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on October 21, 2014; DOI: 10.1158/1055-9965.EPI-14-1008