Embed Size (px)
Citation preview

Colon CancerColon Cancer
Daniel A. Nikcevich, MD, PhDDaniel A. Nikcevich, MD, PhD
Duluth Clinic Cancer CenterDuluth Clinic Cancer Center
January 26, 2009January 26, 2009

Colon CancerColon Cancer
DiagnosisDiagnosis StagingStaging TreatmentTreatment
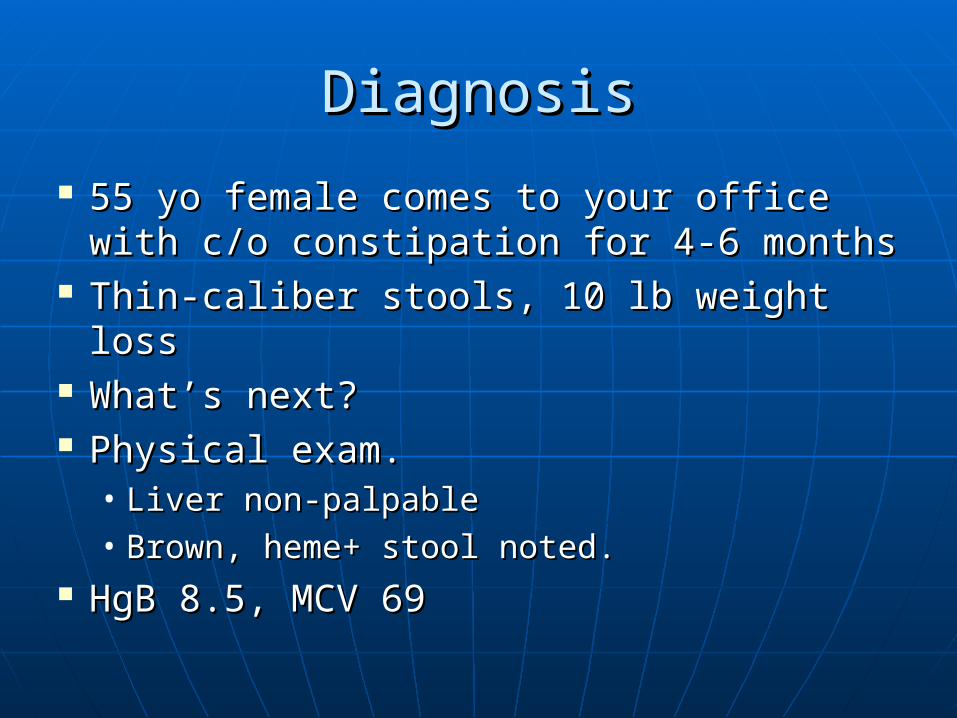
DiagnosisDiagnosis
55 yo female comes to your office 55 yo female comes to your office with c/o constipation for 4-6 monthswith c/o constipation for 4-6 months
Thin-caliber stools, 10 lb weight lossThin-caliber stools, 10 lb weight loss What’s next?What’s next? Physical exam.Physical exam.
• Liver non-palpableLiver non-palpable• Brown, heme+ stool noted.Brown, heme+ stool noted.
HgB 8.5, MCV 69HgB 8.5, MCV 69

DiagnosisDiagnosis
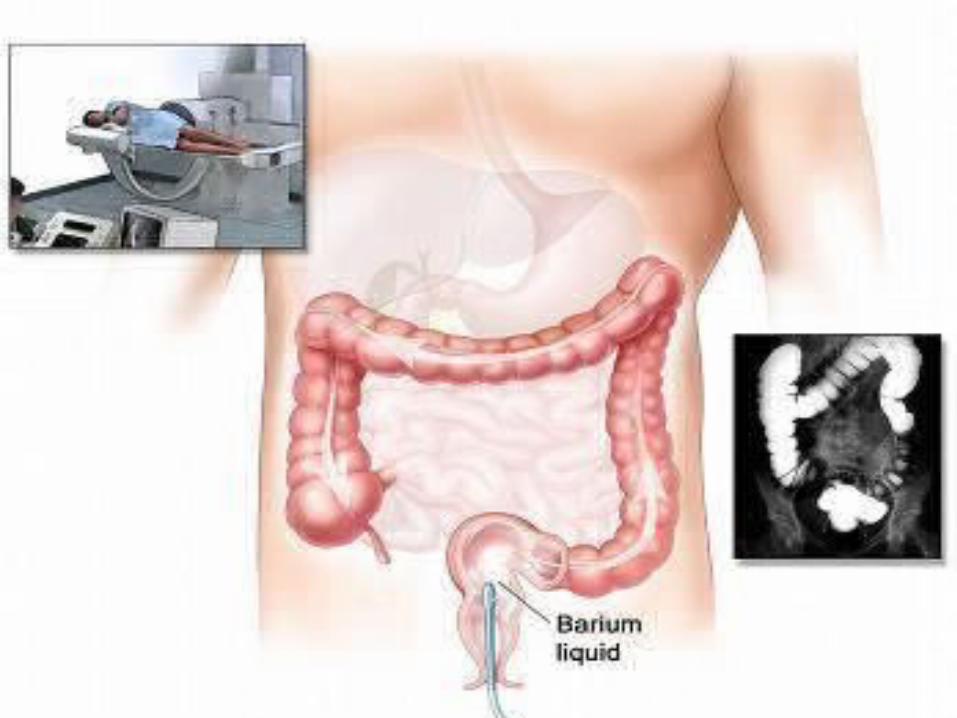
Index of suspicionIndex of suspicion Differential diagnosisDifferential diagnosis ImagingImaging
• ColonoscopyColonoscopy• Flexible sigmoidoscopyFlexible sigmoidoscopy• Virtual colonoscopyVirtual colonoscopy• Barium enemaBarium enema

Annular constricting or napkin-ring carcinoma of Annular constricting or napkin-ring carcinoma of coloncolon
©Copyright Science Press Internet Services



DiagnosisDiagnosis
Index of suspicionIndex of suspicion Differential diagnosisDifferential diagnosis ImagingImaging
• ColonoscopyColonoscopy• Flexible sigmoidoscopyFlexible sigmoidoscopy• Virtual colonoscopyVirtual colonoscopy• Barium enemaBarium enema
BiopsyBiopsy• CANNOT diagnose w/o tissueCANNOT diagnose w/o tissue

Back to our patient…Back to our patient…
Biopsy shows adenocarcinoma in Biopsy shows adenocarcinoma in mass located in distal sigmoid colon.mass located in distal sigmoid colon.
What’s next?What’s next? CT scanCT scan CEA levelCEA level SurgerySurgery

DIAGNOSIS:A, B) Mass, distal sigmoid colon/proximal rectum, segmental colonicresection:- Tumor type and grade: Moderately differentiated adenocarcinoma.- Tumor size and location: 3.0 cm, distal sigmoid colon/proximalrectum.- Extent of invasion: Tumor extends through muscularis propria and intosubserosal fat, and approaches within less than 1/2 mm of serosa.- Lymph nodes: 5 of 16 lymph nodes involved by metastatic neoplasm. Noevidence of extranodal extension by tumor.- Margins: Proximal and distal resection margins uninvolved by neoplasm.Radial margin within proximal rectum of less than 1 mm. Separatelysubmitted anastomotic rings (part B) uninvolved by neoplasm.- Lymphovascular invasion: None seen.- High-risk morphology for microsatellite instability: No.
AJCC Stage: Preliminary stage pending clinical review is AJCC pT3, pN2,MX (Stage IIIC). Correlation with clinical and imaging findings is alsonecessary for accurate staging.


Colon Cancer StagingColon Cancer Staging
Clinical Stage Pathologic Stage 5 year survival
Stage 0 TisN0M0 > 95%
Stage I (A) T1T2N0M0 85-95%
Stage IIA (B) T3N0M0 60-80%
Stage IIB (B2) T4N0M0 60-80%
Stage III (C) T1-4N1-2M0 30-60%
Stage IV (D) M1 < 5%

Colon Cancer TreatmentColon Cancer Treatment
SurgerySurgery• Low-anterior resection (no colostomy)Low-anterior resection (no colostomy)• Abdominoperineal resection (permanent Abdominoperineal resection (permanent
colostomy)colostomy) ChemotherapyChemotherapy Radiation (rectal cancer)Radiation (rectal cancer)

Who should receive Who should receive chemotherapy?chemotherapy?
Stage 1: surgery only.Stage 1: surgery only. Stage IIA/IIB: consider chemotherapy, Stage IIA/IIB: consider chemotherapy,
especially for IIBespecially for IIB Stage III: chemotherapy is standard Stage III: chemotherapy is standard
of careof care Stage IV: chemotherapy is standard Stage IV: chemotherapy is standard
of careof care

Benefits of adjuvant Benefits of adjuvant chemotherapy for colon cancerchemotherapy for colon cancer
40% reduction of recurrence of 40% reduction of recurrence of cancer.cancer.
25% improvement in survival from 25% improvement in survival from cancer.cancer.
Based on 5 years from diagnosis.Based on 5 years from diagnosis.

Which chemotherapy?Which chemotherapy? Adjuvant chemotherapyAdjuvant chemotherapy
• 5-FU plus leucovorin5-FU plus leucovorin• FOLFOX (5-FU, Oxaliplatin, leucovorin)FOLFOX (5-FU, Oxaliplatin, leucovorin)• 33% improvement in disease-free survival for 33% improvement in disease-free survival for
FOLFOX vs 5-FU/LVFOLFOX vs 5-FU/LV• Addition of monoclonal antibody such as Addition of monoclonal antibody such as
bevacizumab or cetuximab in clinical trialsbevacizumab or cetuximab in clinical trials Metastatic diseaseMetastatic disease
• FOLFOX plus bevacizumab is standard of careFOLFOX plus bevacizumab is standard of care• FOLFIRI (substitute irinotecan for oxaliplatin) plus FOLFIRI (substitute irinotecan for oxaliplatin) plus
bevacizumab is standard of carebevacizumab is standard of care• Irinotecan plus cetuximabIrinotecan plus cetuximab• PanitumomabPanitumomab


Recommended Follow UpRecommended Follow Up
Physical exam every 3 months for 2 years, Physical exam every 3 months for 2 years, then every 6 months for 3 years.then every 6 months for 3 years.
CEA every 3 months for 2 years, then CEA every 3 months for 2 years, then every 6 months for 3 years for T2, T3, T4 every 6 months for 3 years for T2, T3, T4 tumors.tumors.
Colonoscopy in 1 yearColonoscopy in 1 year• Repeat in 1 year if abnormal polyps notedRepeat in 1 year if abnormal polyps noted• Repeat every 3-5 years if negativeRepeat every 3-5 years if negative• Repeat in 3-6 months after diagnosis if 1Repeat in 3-6 months after diagnosis if 1stst
colonoscopy with “unprepped” bowel.colonoscopy with “unprepped” bowel.

Colon PolypColon Polyp

Metastatic colon cancerMetastatic colon cancer
IncurableIncurable Treatment goals to improve survival Treatment goals to improve survival
and quality of lifeand quality of life Standard of care is FOLFOX or Standard of care is FOLFOX or
FOLFIRI with bevacizumabFOLFIRI with bevacizumab Second-line options include use of Second-line options include use of
cetuximab or panitumomabcetuximab or panitumomab Clinical trial optionClinical trial option

New approachesNew approaches Gene profilingGene profiling
• Thymidylate synthase expressionThymidylate synthase expression• DPD expressionDPD expression• Microsatellite instabilityMicrosatellite instability• EGF-R expressionEGF-R expression
ChemopreventionChemoprevention• AspirinAspirin• COX-2 inhibitorsCOX-2 inhibitors
Tyrosine kinase inhibitorsTyrosine kinase inhibitors EGF-R inhibitorsEGF-R inhibitors
• CetuximabCetuximab• PanitumomabPanitumomab• MUST be MUST be k-rask-ras wild-type to use either drug wild-type to use either drug
AntiangiogenesisAntiangiogenesis• BevazuzimabBevazuzimab
Oral chemotherapy (capecitabine)Oral chemotherapy (capecitabine)

Anti-angiogenesisAnti-angiogenesis
Bevacizumab: a human anti-vascular Bevacizumab: a human anti-vascular endothelial growth factor monoclonal endothelial growth factor monoclonal antibody.antibody.
Combination of bevacizumab plus IFL Combination of bevacizumab plus IFL superior to IFL in treatment of patients superior to IFL in treatment of patients with metastatic colorectal cancer.with metastatic colorectal cancer.
First human phase III trial to document First human phase III trial to document efficacy of an anti-angiogenesis strategy efficacy of an anti-angiogenesis strategy for treating cancer.for treating cancer.

ChemopreventionChemoprevention COX-2 inhibitors used to prevent in COX-2 inhibitors used to prevent in
adenomas in FAP patientsadenomas in FAP patients Aspirin to prevent adenomas in patients Aspirin to prevent adenomas in patients
with prior colon cancer or family history of with prior colon cancer or family history of colon cancer.colon cancer.

Sandler, R. S. et. al. N Engl J Med 2003;348:883-890
Kaplan-Meier Estimates of the Time to a First Adenoma

Back to our patient…Back to our patient…
Recovered from surgery (LAR).Recovered from surgery (LAR). Stage IIIC colon cancer.Stage IIIC colon cancer. What to do next?What to do next? Discuss chemotherapy optionsDiscuss chemotherapy options
• Standard treatment (FOLFOX)Standard treatment (FOLFOX)• Clinical trial option (FOLFOX +/- Clinical trial option (FOLFOX +/-
cetuximab)cetuximab)


SummarySummary Colon cancer is a curable disease.Colon cancer is a curable disease. Colon cancer is a curable disease.Colon cancer is a curable disease. Chemotherapy improves survival.Chemotherapy improves survival.
• Indicated for stage III (adjuvant) and stage IV Indicated for stage III (adjuvant) and stage IV (metastatic disease)(metastatic disease)
• Possible benefit for patients with stage II diseasePossible benefit for patients with stage II disease New treatments based on enhanced knowledge of New treatments based on enhanced knowledge of
biology and genetics of colon cancerbiology and genetics of colon cancer• New treatments in the context of clinical trialsNew treatments in the context of clinical trials• Can we afford any of this new stuff?Can we afford any of this new stuff?
Colon cancer is a curable diseaseColon cancer is a curable disease

Questions?Questions? [email protected]@smdc.org