Embed Size (px)
Citation preview
Collaborative e-care: health information exchange for
enhanced care
Wednesday, March 2, 2016 Charles Gutteridge MD
Barts Health NHS Trust UK

Conflict of Interest
Charles Gutteridge MD
Has no real or apparent conflicts of interest to report.

Agenda
•Health economy of East London
•Commissioning for value
•Collaborative e-working in East London
•How are we doing?
•Lessons learnt

Learning Objectives
• Identify lessons learnt in delivering integrated
care across traditional healthcare boundaries
• Distinguish how best to use health information
exchange to support clinical and business
objectives in health delivery systems
• Describe the key steps towards building self
care delivery platforms





1.2 M people US 1.6B budget


3 core elements to our programme
•A people’s health data movement
•Empowering clinicians with point of care information and outcomes data
•Developing data for population health


Enhanced service aims
1. Increase practice availability to patients
2. Identify patients at high risk of emergency admissions
3. Improve hospital discharge processes and coordinate care
4. Internal provider reviews of emergency admissions and ED attendances
5. Patients satisfaction surveys


3 key interventions
•Linking electronic health records
•Health information exchange
•Outcomes tracking

Ris
k s
trat
ific
atio
n
Co
-ord
inat
ed c
are
Reduce
emergency
attendances
Reduce
emergency
admissions
Improve
outcomes QAdmission® algorithm
(Consent)
(Enrol)
East London Integrated Care Programme
High
Moderate
Low
Very low
Very high

Clinical case.
Julia Hippisley-Cox, and Carol Coupland BMJ Open
2013;3:e003482
©2013 by British Medical Journal Publishing Group





Reasons for attending the ED
Pain
Shortness of breath
Generally Unwell
Fall
Chest Pain
Confusion
Chest infection

LRTI
UTI
Gastroenteritis
IHD
COPD
Heart failure
Superficial injury
Fracture
Electrolyte imbalance
Unspecified chest pain
Unspecified fall / collapse
Unspecified abdominal pain
Unspecified MSK pain
Primary diagnosis at discharge (ICD-10)
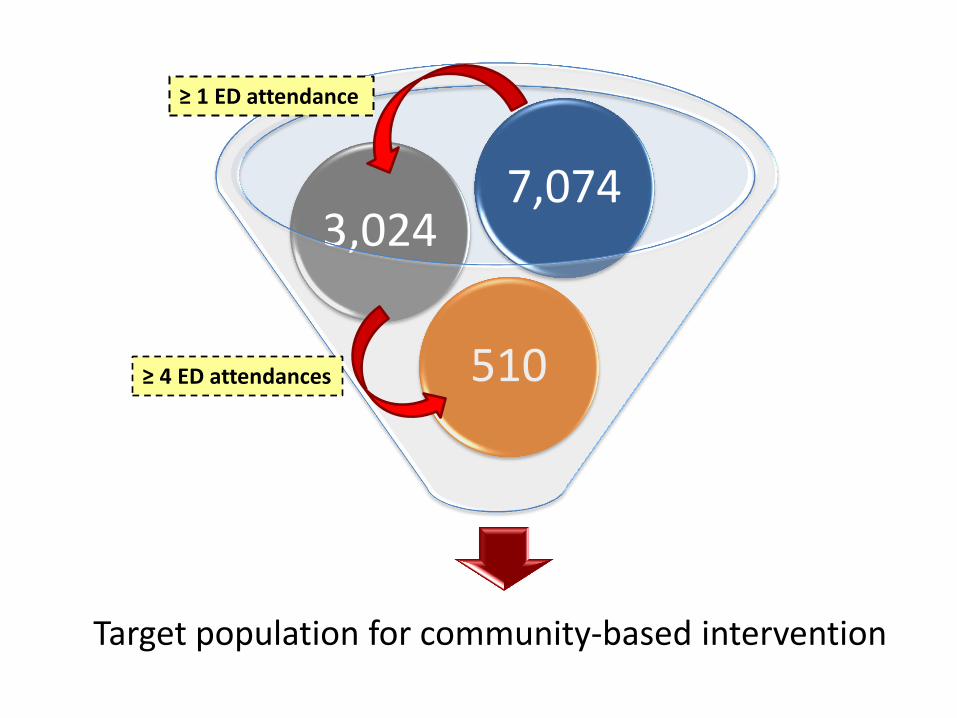
Target population for community-based intervention
510
3,024 7,074
≥ 1 ED attendance
≥ 4 ED attendances
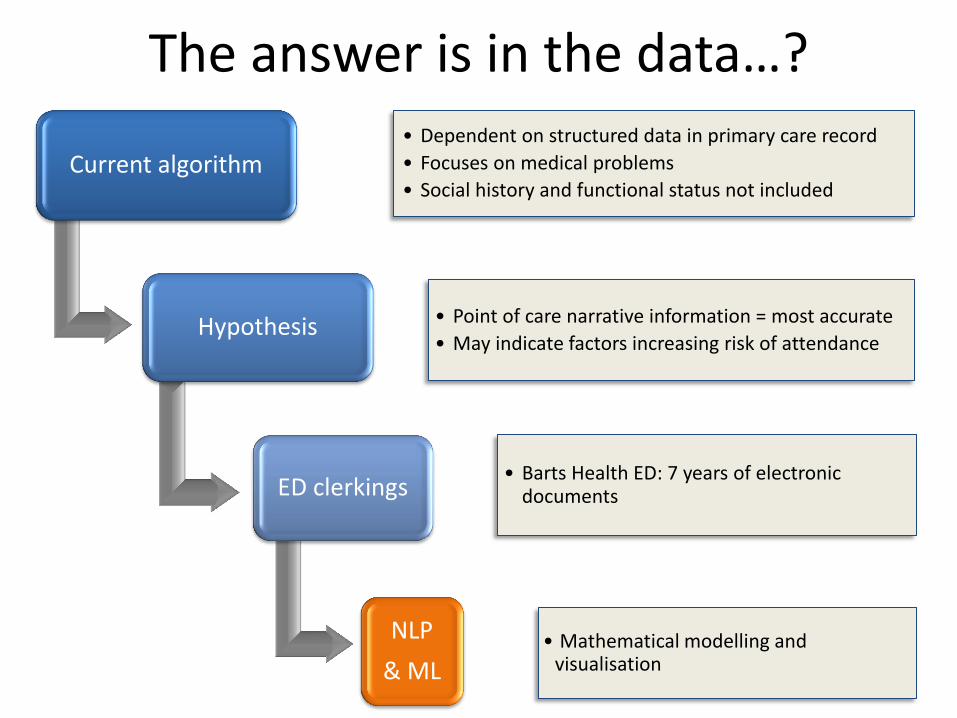
Current algorithm • Dependent on structured data in primary care record
• Focuses on medical problems
• Social history and functional status not included
Hypothesis • Point of care narrative information = most accurate
• May indicate factors increasing risk of attendance
ED clerkings • Barts Health ED: 7 years of electronic
documents
NLP
& ML
The answer is in the data…?
• Mathematical modelling and visualisation


3 different community approaches
Community matrons
Face to face
Community matrons
Face to face
Health analytics
Rapid response team
Telephone consent
GP EMIS web EMIS community
8 networks Care navigators
Telephone consent
Feedback from hospital systems Cerner Millennium HIE Cerner-EMIS
Waltham Forest Newham Tower Hamlets
GP EMIS web EMIS community


In 2011 systematic programme – guideline, IT decision support and recall,
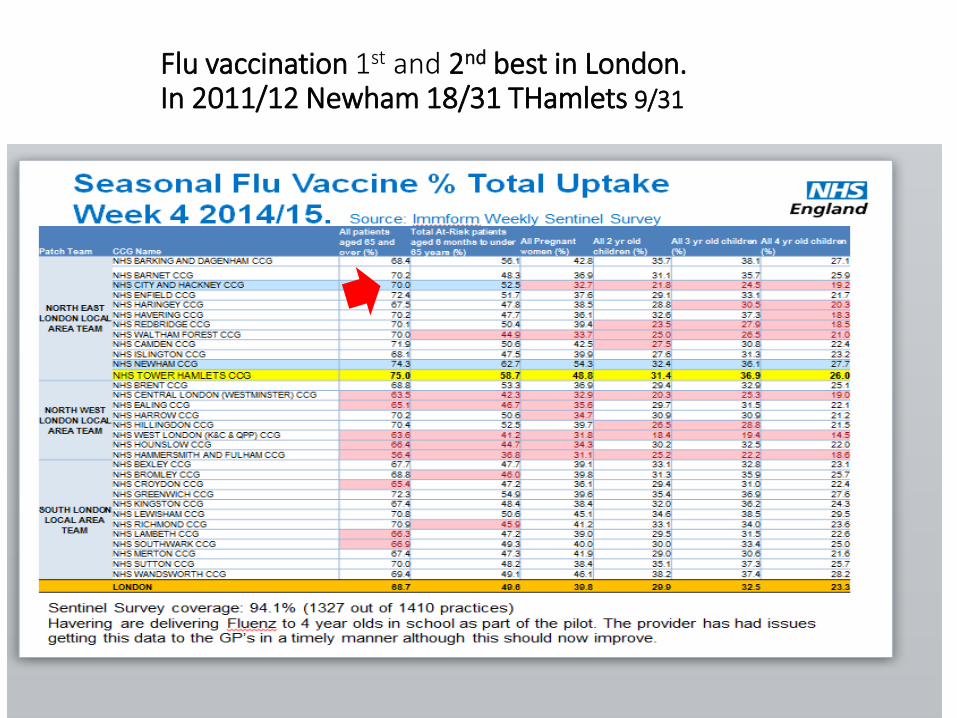
Flu vaccination 1st and 2nd best in London. In 2011/12 Newham 18/31 THamlets 9/31

CCG Variation in high cost - low benefit medicines

Jan 2014
June 2015
City and
Hackney
60.8% 88.2%
Tower Hamlets 54.3% 78.8%
Newham 35.9% 72.6%
% Age 65 yrs or more: Pulse Check
in 5 yrs































