Embed Size (px)
Citation preview
10.1192/bjp.bp.106.023655Access the most recent version at DOI: 2006, 189:484-493.BJP
Peter Bower, Simon Gilbody, David Richards, Janine Fletcher and Alex Suttonmeta-regressionof a complex intervention: systematic review and Collaborative care for depression in primary care: Making sense
Referenceshttp://bjp.rcpsych.org/content/189/6/484#BIBLThis article cites 75 articles, 20 of which you can access for free at:
permissionsReprints/
[email protected] to To obtain reprints or permission to reproduce material from this paper, please
to this article atYou can respond http://bjp.rcpsych.org/letters/submit/bjprcpsych;189/6/484
from Downloaded
The Royal College of PsychiatristsPublished by on September 5, 2014http://bjp.rcpsych.org/
http://bjp.rcpsych.org/site/subscriptions/ go to: The British Journal of PsychiatryTo subscribe to

BackgroundBackground ThemanagementofThemanagementof
depression inprimarycare is a significantdepression inprimarycare is a significant
issue forhealth servicesworldwide.issue forhealth servicesworldwide.
‘Collaborative care’ interventions are‘Collaborative care’ interventions are
effective, but little is known aboutwhicheffective, but little is known aboutwhich
aspectsofthesecomplexinterventions areaspectsofthesecomplexinterventions are
essential.essential.
AimsAims Tousemeta-regressionto identifyTousemeta-regressionto identify
‘active ingredients’ in collaborative care‘active ingredients’ in collaborative care
models fordepression inprimarycare.models fordepression inprimarycare.
MethodMethod Studieswere identifiedusingStudieswere identifiedusing
systematic searches of electronicsystematic searches of electronic
databases.The contentof collaborativedatabases.The contentof collaborative
care interventionswas coded, togethercare interventionswas coded, together
with outcome data on antidepressantusewith outcome data on antidepressantuse
and depressive symptoms.Meta-and depressive symptoms.Meta-
regressionwasused to examineregressionwasused to examine
relationships between interventionrelationships between intervention
content and outcomes.content and outcomes.
ResultsResults Therewasno significantTherewasno significant
predictorofthe effectofcollaborative carepredictorofthe effectofcollaborative care
on antidepressantuse.Keypredictors ofon antidepressantuse.Keypredictors of
depressive symptomoutcomes includeddepressive symptomoutcomes included
systematic identification of patients,systematic identification of patients,
professionalbackground of staff andprofessional background of staff and
specialist supervision.specialist supervision.
ConclusionsConclusions Meta-regressionmaybeMeta-regressionmaybe
useful in examining‘active ingredients’ inuseful in examining‘active ingredients’ in
complex interventions inmentalhealth.complex interventions inmentalhealth.
Declaration of interestDeclaration of interest None.None.
Depression is prevalent in primary care, butDepression is prevalent in primary care, but
current management is suboptimal (Simoncurrent management is suboptimal (Simon
& Von Korff, 1995). There is increasing& Von Korff, 1995). There is increasing
evidence of the effectiveness of ‘collab-evidence of the effectiveness of ‘collab-
orative care’ (Gilbodyorative care’ (Gilbody et alet al, 2003), a, 2003), a
multifaceted organisational interventionmultifaceted organisational intervention
involving new staff and ways of workinginvolving new staff and ways of working
(Von Korff & Goldberg, 2001). However,(Von Korff & Goldberg, 2001). However,
collaborative care interventions vary incollaborative care interventions vary in
content and intensity, and it is unclearcontent and intensity, and it is unclear
which aspects are crucial determinants ofwhich aspects are crucial determinants of
effectiveness (the ‘active ingredients’). Mosteffectiveness (the ‘active ingredients’). Most
of the current collaborative care literatureof the current collaborative care literature
derives from the USA, and designing collab-derives from the USA, and designing collab-
orative care interventions for use in otherorative care interventions for use in other
settings requires an understanding of thesesettings requires an understanding of these
‘active ingredients’.‘active ingredients’.
Collaborative care is an example of aCollaborative care is an example of a
complex intervention, involving a numbercomplex intervention, involving a number
of separate mechanisms, where the ‘activeof separate mechanisms, where the ‘active
ingredient’ is difficult to specify (Campbellingredient’ is difficult to specify (Campbell
et alet al, 2000). If different collaborative care, 2000). If different collaborative care
interventions vary in their inclusion ofinterventions vary in their inclusion of
‘active ingredients’, then this should lead‘active ingredients’, then this should lead
to significant variation in outcomes. Suchto significant variation in outcomes. Such
variation in outcomes in a meta-analysis isvariation in outcomes in a meta-analysis is
described as statistical heterogeneity.described as statistical heterogeneity.
Meta-regression is a method used toMeta-regression is a method used to
explore statistical heterogeneity in meta-explore statistical heterogeneity in meta-
analysis (Suttonanalysis (Sutton et alet al, 1998; Thompson &, 1998; Thompson &
Higgins, 2002).Higgins, 2002).
A phased approach to the developmentA phased approach to the development
of complex interventions has been pro-of complex interventions has been pro-
posed (Campbellposed (Campbell et alet al, 2000). Modelling, 2000). Modelling
of complex interventions, where the ‘activeof complex interventions, where the ‘active
ingredients’ are explored, is a critical step iningredients’ are explored, is a critical step in
the phased model prior to further trials.the phased model prior to further trials.
However, there are relatively few examplesHowever, there are relatively few examples
of the phased model in the literatureof the phased model in the literature
(Bradley(Bradley et alet al, 1999; Campbell, 1999; Campbell et alet al,,
2000; Medical Research Council, 2000;2000; Medical Research Council, 2000;
Loeb, 2002) and a lack of consensus as toLoeb, 2002) and a lack of consensus as to
the optimal modelling methods.the optimal modelling methods.
The authors are developing and testingThe authors are developing and testing
a collaborative care intervention in the UKa collaborative care intervention in the UK
using the phased approach, and usedusing the phased approach, and used
meta-regression to examine the relationshipmeta-regression to examine the relationship
between the content of collaborative carebetween the content of collaborative care
interventions and outcomes, to identifyinterventions and outcomes, to identify
‘active ingredients’ and thus assist in the‘active ingredients’ and thus assist in the
design of a UK collaborative care modeldesign of a UK collaborative care model
for the care of depression.for the care of depression.
METHODMETHOD
Data sourcesData sources
We based our meta-regression on a sys-We based our meta-regression on a sys-
tematic review. A published systematictematic review. A published systematic
review of organisational interventions inreview of organisational interventions in
primary care mental health completed byprimary care mental health completed by
S.G. was used as the initial source of studiesS.G. was used as the initial source of studies
(Gilbody(Gilbody et alet al, 2003); this review included, 2003); this review included
collaborative care as well as other typescollaborative care as well as other types
of organisational interventions used toof organisational interventions used to
improve the management of depression.improve the management of depression.
Searches included Medline, EMBASE,Searches included Medline, EMBASE,
CINAHL, PsycINFO, the Cochrane LibraryCINAHL, PsycINFO, the Cochrane Library
and the Database of Abstracts of Reviewsand the Database of Abstracts of Reviews
of Effectiveness (DARE), and were runof Effectiveness (DARE), and were run
from the inception date of each databasefrom the inception date of each database
to 2003. We updated the comprehensiveto 2003. We updated the comprehensive
search strategies from this review (withoutsearch strategies from this review (without
language restriction) to June 2004 to findlanguage restriction) to June 2004 to find
recent studies, and then conducted a secondrecent studies, and then conducted a second
update to November 2005 (Fig. 1). Detailsupdate to November 2005 (Fig. 1). Details
of the exact search methods and a table ofof the exact search methods and a table of
excluded studies are available from theexcluded studies are available from the
authors upon request. From this compre-authors upon request. From this compre-
hensive database, we then identified thehensive database, we then identified the
subset of collaborative care studies.subset of collaborative care studies.
Inclusion criteriaInclusion criteria
The population of interest was patientsThe population of interest was patients
with depressive symptoms or diagnosed de-with depressive symptoms or diagnosed de-
pressive disorders in primary care settings.pressive disorders in primary care settings.
Primary care was defined as the provisionPrimary care was defined as the provision
of medical care by professionals whoof medical care by professionals who
provide first contact and ongoing care toprovide first contact and ongoing care to
patients, regardless of the patient’s age,patients, regardless of the patient’s age,
gender or presenting problem.gender or presenting problem.
Although we have published a broadAlthough we have published a broad
typology of models of quality improvementtypology of models of quality improvement
which includes collaborative care (Bowerwhich includes collaborative care (Bower
& Gilbody, 2005), developing precise& Gilbody, 2005), developing precise
inclusion criteria for such complex inter-inclusion criteria for such complex inter-
ventions is more problematic, because byventions is more problematic, because by
definition it is not cleardefinition it is not clear a prioria priori whichwhich
mechanisms have to be in place in ordermechanisms have to be in place in order
to define an intervention as ‘collaborativeto define an intervention as ‘collaborative
care’. Therefore, any definition is poten-care’. Therefore, any definition is poten-
tially arbitrary, reflected by publishedtially arbitrary, reflected by published
reviews of collaborative care that disagreereviews of collaborative care that disagree
on which studies and interventions areon which studies and interventions are
included and excluded (Von Korff &included and excluded (Von Korff &
Goldberg, 2001; GilbodyGoldberg, 2001; Gilbody et alet al, 2003; Bijl, 2003; Bijl
et alet al, 2004)., 2004).
4 8 44 8 4
BR IT I SH JOURNAL OF P SYCHIATRYBR IT I SH JOURNAL OF P SYCHIATRY ( 2 0 0 6 ) , 1 8 9, 4 8 4 ^ 4 9 3 . d o i : 1 0 . 11 9 2 / b j p . b p .1 0 6 . 0 2 3 6 5 5( 2 0 0 6 ) , 1 8 9 , 4 8 4 ^ 4 9 3 . d o i : 1 0 .11 9 2 / b jp . b p .1 0 6 . 0 2 3 6 5 5 R E V I E W A R T I C L ER E V I E W A R T I C L E
Collaborative care for depression in primary careCollaborative care for depression in primary care
Making sense of a complex intervention: systematic reviewMaking sense of a complex intervention: systematic review
and meta-regressionand meta-regression
PETER BOWER, SIMON GILBODY, DAVID RICHARDS, JANINE FLETCHERPETER BOWER, SIMON GILBODY, DAVID RICHARDS, JANINE FLETCHERand ALEX SUTTONand ALEX SUTTON

COLLABORATIVE CARE FOR DEPRES S IONCOLLABORATIVE CARE FOR DEPRES S ION
The purpose of the study was toThe purpose of the study was to
examine the relationship between variationexamine the relationship between variation
in the interventions within collaborativein the interventions within collaborative
care studies, and outcomes. Therefore, wecare studies, and outcomes. Therefore, we
used a broad definition, and definedused a broad definition, and defined
‘collaborative care’ as a multifaceted‘collaborative care’ as a multifaceted
organisational intervention, which couldorganisational intervention, which could
include a number of components:include a number of components:
(a)(a) the introduction of a new role (casethe introduction of a new role (case
manager) into primary care, to assistmanager) into primary care, to assist
in the management of patients within the management of patients with
depression through structured anddepression through structured and
systematic delivery of interventions;systematic delivery of interventions;
(b)(b) the introduction of mechanisms tothe introduction of mechanisms to
foster closer liaison between primaryfoster closer liaison between primary
care clinicians and mental healthcare clinicians and mental health
specialists (including case managers)specialists (including case managers)
around individual patient care;around individual patient care;
(c)(c) the introduction of mechanisms tothe introduction of mechanisms to
collect and share information on thecollect and share information on the
progress of individual patients.progress of individual patients.
We excluded educational and trainingWe excluded educational and training
interventions and the provision of briefinterventions and the provision of brief
psychological therapy where these werepsychological therapy where these were
the sole intervention and were notthe sole intervention and were not
supported by other enhancements of caresupported by other enhancements of care
outlined above. The full list of studies isoutlined above. The full list of studies is
given in Table 1.given in Table 1.
Data extractionData extraction
Content of collaborative careContent of collaborative care
We initially tested published codingWe initially tested published coding
schemes relating to quality improvementschemes relating to quality improvement
(Weingarten(Weingarten et alet al, 2002; Bero, 2002; Bero et alet al, 2006),, 2006),
but these lacked the detail to capture thebut these lacked the detail to capture the
specific issues of relevance to collaborativespecific issues of relevance to collaborative
care. Therefore, a basic coding frame wascare. Therefore, a basic coding frame was
developed on the basis of the ‘prototypical’developed on the basis of the ‘prototypical’
collaborative care model, described incollaborative care model, described in
terms of the three roles potentiallyterms of the three roles potentially
involved in patient care: primary careinvolved in patient care: primary care
provider, mental health specialist and caseprovider, mental health specialist and case
manager (Katonmanager (Katon et alet al, 2001, 2001bb). Variables). Variables
were created relating to the professionalwere created relating to the professional
background of each worker and additionalbackground of each worker and additional
intervention-specific training. These codesintervention-specific training. These codes
were then supplemented by variableswere then supplemented by variables
describing the potential interprofessionaldescribing the potential interprofessional
relationships (e.g. specialist supervision ofrelationships (e.g. specialist supervision of
the case manager, and case manager feed-the case manager, and case manager feed-
back of information to the primary careback of information to the primary care
provider). Because professional–patientprovider). Because professional–patient
contact within collaborative care is focusedcontact within collaborative care is focused
on the case manager–patient relationship,on the case manager–patient relationship,
we added variables relating to the intensitywe added variables relating to the intensity
and nature of that contact. Finally, weand nature of that contact. Finally, we
added three variables related to theadded three variables related to the
characteristics of the patients and study set-characteristics of the patients and study set-
ting (see Appendix).ting (see Appendix).
After piloting the data extractionAfter piloting the data extraction
among the team, data from each study wereamong the team, data from each study were
extracted by two different members of theextracted by two different members of the
research team working independently.research team working independently.
There was no formal measurement of relia-There was no formal measurement of relia-
bility, but disagreements were few and werebility, but disagreements were few and were
resolved by discussion. Owing to incon-resolved by discussion. Owing to incon-
sistent reporting of data in the publishedsistent reporting of data in the published
papers we were only able to extractpapers we were only able to extract
comprehensive data on 8 of the originalcomprehensive data on 8 of the original
27 variables (see Table 2).27 variables (see Table 2).
Concealment of allocation is the qualityConcealment of allocation is the quality
attribute with the best evidence for an asso-attribute with the best evidence for an asso-
ciation with outcomes (Schultz & Grimes,ciation with outcomes (Schultz & Grimes,
2002), and we extracted data on conceal-2002), and we extracted data on conceal-
ment to test whether outcomes were relatedment to test whether outcomes were related
to study quality.to study quality.
Intervention outcomesIntervention outcomes
Collaborative care interventions often seekCollaborative care interventions often seek
to improve adherence to antidepressantto improve adherence to antidepressant
medication, and the first outcome measuremedication, and the first outcome measure
was changes in measures of antidepressantwas changes in measures of antidepressant
use. Most studies reported data in dicho-use. Most studies reported data in dicho-
tomous form, e.g. the proportion oftomous form, e.g. the proportion of
patients taking antidepressants or meetingpatients taking antidepressants or meeting
standardised guidelines for antidepressantstandardised guidelines for antidepressant
use.use.
The second outcome measure was re-The second outcome measure was re-
duction in depressive symptoms. A wideduction in depressive symptoms. A wide
variety of outcomes were reported at avariety of outcomes were reported at a
number of different time points. Becausenumber of different time points. Because
the meta-regression required as large athe meta-regression required as large a
sample of studies as possible for reliablesample of studies as possible for reliable
analysis (Thompson & Higgins, 2002), weanalysis (Thompson & Higgins, 2002), we
restricted the analysis to short-term out-restricted the analysis to short-term out-
comes (approximately 6 months aftercomes (approximately 6 months after
randomisation), as these outcomes wererandomisation), as these outcomes were
by far the most frequently reported. Whereby far the most frequently reported. Where
alternative measures of depressive out-alternative measures of depressive out-
comes were reported within the same study,comes were reported within the same study,
the data extracted were chosen on the basisthe data extracted were chosen on the basis
of anof an a prioria priori decision rule which extracteddecision rule which extracted
any identified primary outcome first, andany identified primary outcome first, and
then prioritised observer-rated scales overthen prioritised observer-rated scales over
self-report measures where available.self-report measures where available.
We extracted all measures of anti-We extracted all measures of anti-
depressant use as dichotomous outcomes,depressant use as dichotomous outcomes,
analysed using odds ratios. Measures ofanalysed using odds ratios. Measures of
depressive symptoms included a mix ofdepressive symptoms included a mix of
dichotomous and continuous outcomes.dichotomous and continuous outcomes.
We translated continuous measures to aWe translated continuous measures to a
standardised effect size, i.e. the mean ofstandardised effect size, i.e. the mean of
the intervention group minus the mean ofthe intervention group minus the mean of
the control group, divided by the pooledthe control group, divided by the pooled
standard deviation. We translated out-standard deviation. We translated out-
comes reported as dichotomous variablescomes reported as dichotomous variables
4 8 54 8 5
Fig. 1Fig. 1 QUOROM (Quality of Reporting Meta-analyses) flow diagram.QUOROM (Quality of Reporting Meta-analyses) flow diagram.
BOWER ET ALBOWER ET AL
4 8 64 8 6
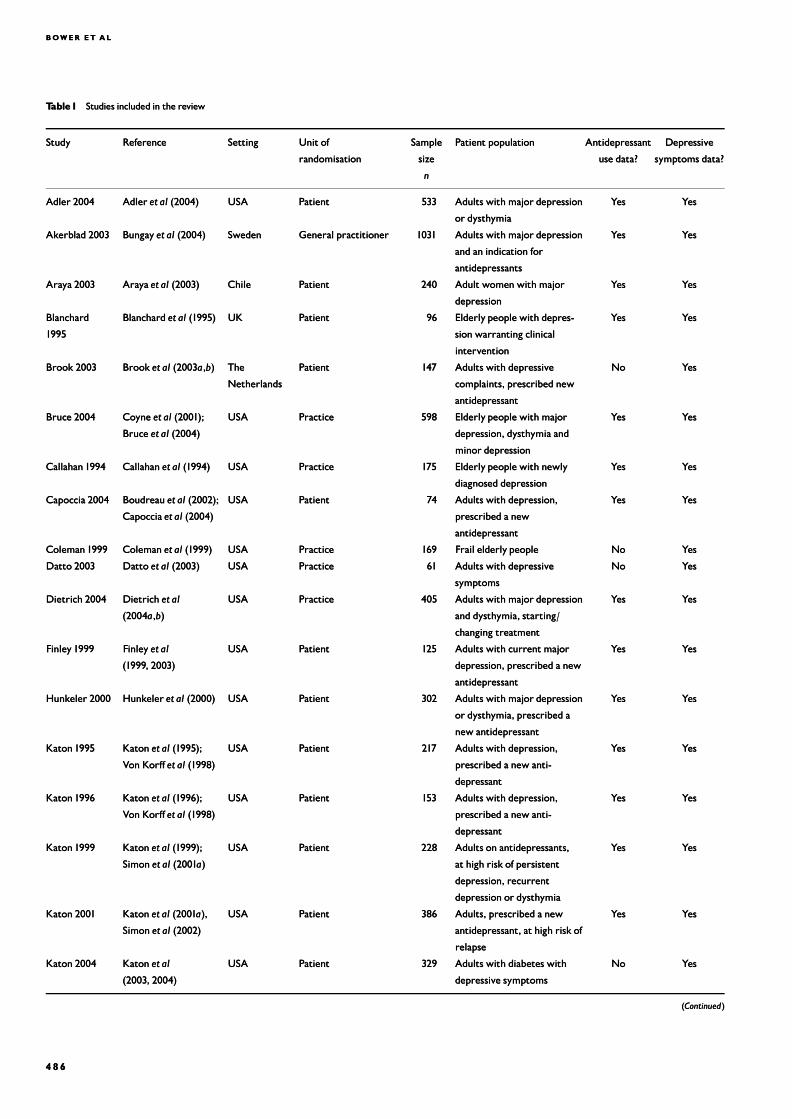
Table1Table1 Studies included in the reviewStudies included in the review
StudyStudy ReferenceReference SettingSetting Unit ofUnit of
randomisationrandomisation
SampleSample
sizesize
nn
Patient populationPatient population AntidepressantAntidepressant
use data?use data?
DepressiveDepressive
symptoms data?symptoms data?
Adler 2004Adler 2004 AdlerAdler et alet al (2004)(2004) USAUSA PatientPatient 533533 Adults withmajor depressionAdults with major depression
or dysthymiaor dysthymia
YesYes YesYes
Akerblad 2003Akerblad 2003 BungayBungay et alet al (2004)(2004) SwedenSweden General practitionerGeneral practitioner 10311031 Adults withmajor depressionAdults with major depression
and an indication forand an indication for
antidepressantsantidepressants
YesYes YesYes
Araya 2003Araya 2003 ArayaAraya et alet al (2003)(2003) ChileChile PatientPatient 240240 Adult womenwith majorAdult womenwithmajor
depressiondepression
YesYes YesYes
BlanchardBlanchard
19951995
BlanchardBlanchard et alet al (1995)(1995) UKUK PatientPatient 9696 Elderly people with depres-Elderly people with depres-
sion warranting clinicalsion warranting clinical
interventionintervention
YesYes YesYes
Brook 2003Brook 2003 BrookBrook et alet al (2003(2003aa,,bb)) TheThe
NetherlandsNetherlands
PatientPatient 147147 Adults with depressiveAdults with depressive
complaints, prescribed newcomplaints, prescribed new
antidepressantantidepressant
NoNo YesYes
Bruce 2004Bruce 2004 CoyneCoyne et alet al (2001);(2001);
BruceBruce et alet al (2004)(2004)
USAUSA PracticePractice 598598 Elderly people with majorElderly people with major
depression, dysthymia anddepression, dysthymia and
minor depressionminor depression
YesYes YesYes
Callahan 1994Callahan 1994 CallahanCallahan et alet al (1994)(1994) USAUSA PracticePractice 175175 Elderly people with newlyElderly people with newly
diagnosed depressiondiagnosed depression
YesYes YesYes
Capoccia 2004Capoccia 2004 BoudreauBoudreau et alet al (2002);(2002);
CapocciaCapoccia et alet al (2004)(2004)
USAUSA PatientPatient 7474 Adults with depression,Adults with depression,
prescribed a newprescribed a new
antidepressantantidepressant
YesYes YesYes
Coleman1999Coleman1999 ColemanColeman et alet al (1999)(1999) USAUSA PracticePractice 169169 Frail elderly peopleFrail elderlypeople NoNo YesYes
Datto 2003Datto 2003 DattoDatto et alet al (2003)(2003) USAUSA PracticePractice 6161 Adults with depressiveAdults with depressive
symptomssymptoms
NoNo YesYes
Dietrich 2004Dietrich 2004 DietrichDietrich et alet al
(2004(2004aa,,bb))
USAUSA PracticePractice 405405 Adults withmajor depressionAdults with major depression
and dysthymia, starting/and dysthymia, starting/
changing treatmentchanging treatment
YesYes YesYes
Finley 1999Finley 1999 FinleyFinley et alet al
(1999, 2003)(1999, 2003)
USAUSA PatientPatient 125125 Adults with currentmajorAdults with currentmajor
depression, prescribed a newdepression, prescribed a new
antidepressantantidepressant
YesYes YesYes
Hunkeler 2000Hunkeler 2000 HunkelerHunkeler et alet al (2000)(2000) USAUSA PatientPatient 302302 Adults withmajor depressionAdults with major depression
or dysthymia, prescribed aor dysthymia, prescribed a
new antidepressantnew antidepressant
YesYes YesYes
Katon 1995Katon 1995 KatonKaton et alet al (1995);(1995);
Von KorffVon Korff et alet al (1998)(1998)
USAUSA PatientPatient 217217 Adults with depression,Adults with depression,
prescribed a new anti-prescribed a new anti-
depressantdepressant
YesYes YesYes
Katon 1996Katon 1996 KatonKaton et alet al (1996);(1996);
Von KorffVon Korff et alet al (1998)(1998)
USAUSA PatientPatient 153153 Adults with depression,Adults with depression,
prescribed a new anti-prescribed a new anti-
depressantdepressant
YesYes YesYes
Katon 1999Katon 1999 KatonKaton et alet al (1999);(1999);
SimonSimon et alet al (2001(2001aa))
USAUSA PatientPatient 228228 Adults on antidepressants,Adults on antidepressants,
at high risk of persistentat high risk of persistent
depression, recurrentdepression, recurrent
depression or dysthymiadepression or dysthymia
YesYes YesYes
Katon 200Katon 20011 KatonKaton et alet al (2001(2001aa),),
SimonSimon et alet al (2002)(2002)
USAUSA PatientPatient 386386 Adults, prescribed a newAdults, prescribed a new
antidepressant, at high risk ofantidepressant, at high risk of
relapserelapse
YesYes YesYes
Katon 2004Katon 2004 KatonKaton et alet al
(2003, 2004)(2003, 2004)
USAUSA PatientPatient 329329 Adults with diabetes withAdults with diabetes with
depressive symptomsdepressive symptoms
NoNo YesYes
((ContinuedContinued))

COLLABORATIVE CARE FOR DEPRES S IONCOLLABORATIVE CARE FOR DEPRES S ION
4 8 74 8 7
Table1Table1 ((ContinuedContinued))
StudyStudy ReferenceReference SettingSetting Unit ofUnit of
randomisationrandomisation
SampleSample
sizesize
nn
Patient populationPatient population AntidepressantAntidepressant
use data?use data?
DepressiveDepressive
symptoms data?symptoms data?
Katzelnick 2000Katzelnick 2000 KatzelnickKatzelnick et alet al (2000);(2000);
SimonSimon et alet al (2001(2001bb))
USAUSA PracticePractice 407407 Adults, high users of services,Adults, high users of services,
with depressive symptomswith depressive symptoms
YesYes YesYes
Mann1998Mann1998 MannMann et alet al (1998)(1998) UKUK PatientPatient 419419 Adults with depressionAdults with depression YesYes YesYes
Oslin 2003Oslin 2003 OslinOslin et alet al (2003)(2003) USAUSA PhysicianPhysician 9797 Adults with depression orAdults with depression or
dysthymia, at risk drinkingdysthymia, at risk drinking
NoNo YesYes
Peveler 1999Peveler 1999 PevelerPeveler et alet al (1999)(1999) UKUK PatientPatient 160160 Diagnosis of depression,Diagnosis of depression,
prescribed a new anti-prescribed a new anti-
depressantdepressant
YesYes YesYes
Rickles 2003Rickles 2003 Rickles (2003)Rickles (2003) USAUSA PatientPatient 6363 Prescribed a new anti-Prescribed a new anti-
depressantdepressant
NoNo YesYes
Rost 200Rost 20011aa RostRost et alet al (2000, 2001);(2000, 2001);
PynePyne et alet al (2003)(2003)
USAUSA PracticePractice 243243 Adults with majorAdults withmajor
depression, prescribed a newdepression, prescribed a new
antidepressant, recentlyantidepressant, recently
treatedtreated
YesYes YesYes
Rost 200Rost 20011bb As aboveAs above USAUSA PracticePractice 189189 Adults with majorAdults withmajor
depression, prescribed a newdepression, prescribed a new
antidepressant, beginningantidepressant, beginning
new episodenew episode
YesYes YesYes
Simon 2000Simon 2000 SimonSimon et alet al (2000)(2000) USAUSA PatientPatient 392392 Adults with depression,Adults with depression,
prescribed a new anti-prescribed a new anti-
depressantdepressant
YesYes YesYes
Simon 2004Simon 2004aa SimonSimon et alet al (2004)(2004) USAUSA PatientPatient 402402 Adults with depression,Adults with depression,
prescribed a new anti-prescribed a new anti-
depressantdepressant
YesYes YesYes
Simon 2004Simon 2004bb As aboveAs above USAUSA PatientPatient 393393 Adults with depression,Adults with depression,
prescribed a new anti-prescribed a new anti-
depressantdepressant
YesYes YesYes
Swindle 2003Swindle 2003 SwindleSwindle et alet al (2003)(2003) USAUSA FirmFirm 268268 Adults with majorAdults withmajor
depression, dysthymia ordepression, dysthymia or
partially remittedmajorpartially remittedmajor
depressiondepression
YesYes YesYes
Unutzer 2002Unutzer 2002 UnutzerUnutzer et alet al
(200(20011aa, 2003), 2003)
USAUSA PatientPatient 18018011 Elderlypeople withmajorElderly people with major
depression, dysthymia, ordepression, dysthymia, or
bothboth
YesYes YesYes
Wells 2000Wells 2000aa WellsWells et alet al (2000);(2000);
SherbourneSherbourne et alet al (2001);(2001);
SchoenbaumSchoenbaum et alet al
(200(2001);Unutzer1);Unutzer et alet al
(200(20011bb); Wells);Wells et alet al
(2004)(2004)
USAUSA PracticePractice 867867 Adults withmajor depressionAdults withmajor depression
or dysthymiaor dysthymia
YesYes YesYes
Wells 2000Wells 2000bb As aboveAs above USAUSA PracticePractice 932932 Adults withmajor depressionAdults withmajor depression
or dysthymiaor dysthymia
YesYes YesYes
Whooley 2000Whooley 2000 WhooleyWhooley et alet al (2000)(2000) USAUSA PracticePractice 331331 Elderlypeople withElderly people with
depressive symptomsdepressive symptoms
YesYes YesYes
Wilkinson 1993Wilkinson 1993 WilkinsonWilkinson et alet al (1993)(1993) UKUK PatientPatient 6161 Adults with depression,Adults with depression,
prescribed a new anti-prescribed a new anti-
depressantdepressant
YeYess YYeses
BOWER ET ALBOWER ET AL
to standardised effect sizes using the logitto standardised effect sizes using the logit
transformation (Lipsey & Wilson, 2001).transformation (Lipsey & Wilson, 2001).
In 5 of 62 (8%) comparisons, missing dataIn 5 of 62 (8%) comparisons, missing data
(e.g. standard deviations) were imputed(e.g. standard deviations) were imputed
from other relevant studies, in line withfrom other relevant studies, in line with
accepted practice (Furukawaaccepted practice (Furukawa et alet al, 2006)., 2006).
Previous reviews have identified thatPrevious reviews have identified that
unit of analysis errors are common in theunit of analysis errors are common in the
evaluation of collaborative care (Gilbodyevaluation of collaborative care (Gilbody
et alet al, 2003), making studies more suscep-, 2003), making studies more suscep-
tible to type 1 errors. We identified alltible to type 1 errors. We identified all
studies using cluster randomisation andstudies using cluster randomisation and
where necessary adjusted the precision ofwhere necessary adjusted the precision of
these studies in the meta-analysis usingthese studies in the meta-analysis using
methods recommended by the Effectivemethods recommended by the Effective
Practice and Organisation of Care (EPOC)Practice and Organisation of Care (EPOC)
group of the Cochrane Collaborationgroup of the Cochrane Collaboration
(Bero(Bero et alet al, 2006) and assuming an, 2006) and assuming an
intraclass correlation of 0.02. The effectsintraclass correlation of 0.02. The effects
of adjustment for clustering were examinedof adjustment for clustering were examined
in a sensitivity analysis using intraclassin a sensitivity analysis using intraclass
correlations of 0.00 and 0.05 (Donner &correlations of 0.00 and 0.05 (Donner &
Klar, 2002).Klar, 2002).
AnalysisAnalysis
Analyses were conducted in Stata version 8Analyses were conducted in Stata version 8
for Windows, using thefor Windows, using the metanmetan andand metaregmetareg
macros. The initial meta-analyses usedmacros. The initial meta-analyses used
random effects modelling (Suttonrandom effects modelling (Sutton et alet al,,
1998) to provide an overall pooled measure1998) to provide an overall pooled measure
of effect of collaborative care on the twoof effect of collaborative care on the two
outcomes. However, the main focus of theoutcomes. However, the main focus of the
analysis was on heterogeneity. Hetero-analysis was on heterogeneity. Hetero-
geneity was measured using thegeneity was measured using the II22 statistic,statistic,
which estimates the percentage of totalwhich estimates the percentage of total
variation across studies that can be attri-variation across studies that can be attri-
buted to heterogeneity rather than chance.buted to heterogeneity rather than chance.
As a guide,As a guide, II22 values of 25% may be con-values of 25% may be con-
sidered low, 50% moderate and 75% highsidered low, 50% moderate and 75% high
(Higgins(Higgins et alet al, 2003)., 2003).
The main analysis used random effectsThe main analysis used random effects
meta-regression, which provided estimatesmeta-regression, which provided estimates
of the relationships between eight inter-of the relationships between eight inter-
vention content variables and the two out-vention content variables and the two out-
comes. The permutation test was used tocomes. The permutation test was used to
calculatecalculate PP values (using 1000 Monte Carlovalues (using 1000 Monte Carlo
simulations) and to reduce the chance ofsimulations) and to reduce the chance of
spurious false-positive findings (Higgins &spurious false-positive findings (Higgins &
Thompson, 2004). The amount of hetero-Thompson, 2004). The amount of hetero-
geneity explained by the intervention con-geneity explained by the intervention con-
tent variables was examined by reductionstent variables was examined by reductions
in thein the II22 statistic. Initial univariate analysesstatistic. Initial univariate analyses
(using a criterion of significance of(using a criterion of significance of
PP550.10) were followed by estimation of a0.10) were followed by estimation of a
multivariate model. The multivariate modelmultivariate model. The multivariate model
was not based on any automated selectionwas not based on any automated selection
procedure, but involved examination of aprocedure, but involved examination of a
number of candidate models involving dif-number of candidate models involving dif-
ferent combinations of variables. The finalferent combinations of variables. The final
model was chosen on the basis of the great-model was chosen on the basis of the great-
est reduction in heterogeneity. A secondaryest reduction in heterogeneity. A secondary
meta-regression provided an estimate of themeta-regression provided an estimate of the
relationships between the two outcomesrelationships between the two outcomes
(i.e. whether antidepressant use predicted(i.e. whether antidepressant use predicted
depressive symptoms).depressive symptoms).
RESULTSRESULTS
We identified 28 published studies of colla-We identified 28 published studies of colla-
borative care interventions with outcomeborative care interventions with outcome
data on antidepressant use and 34 studiesdata on antidepressant use and 34 studies
with outcome data on depressive symptomswith outcome data on depressive symptoms
(Table 1). Intervention content variables(Table 1). Intervention content variables
are summarised in Table 2.are summarised in Table 2.
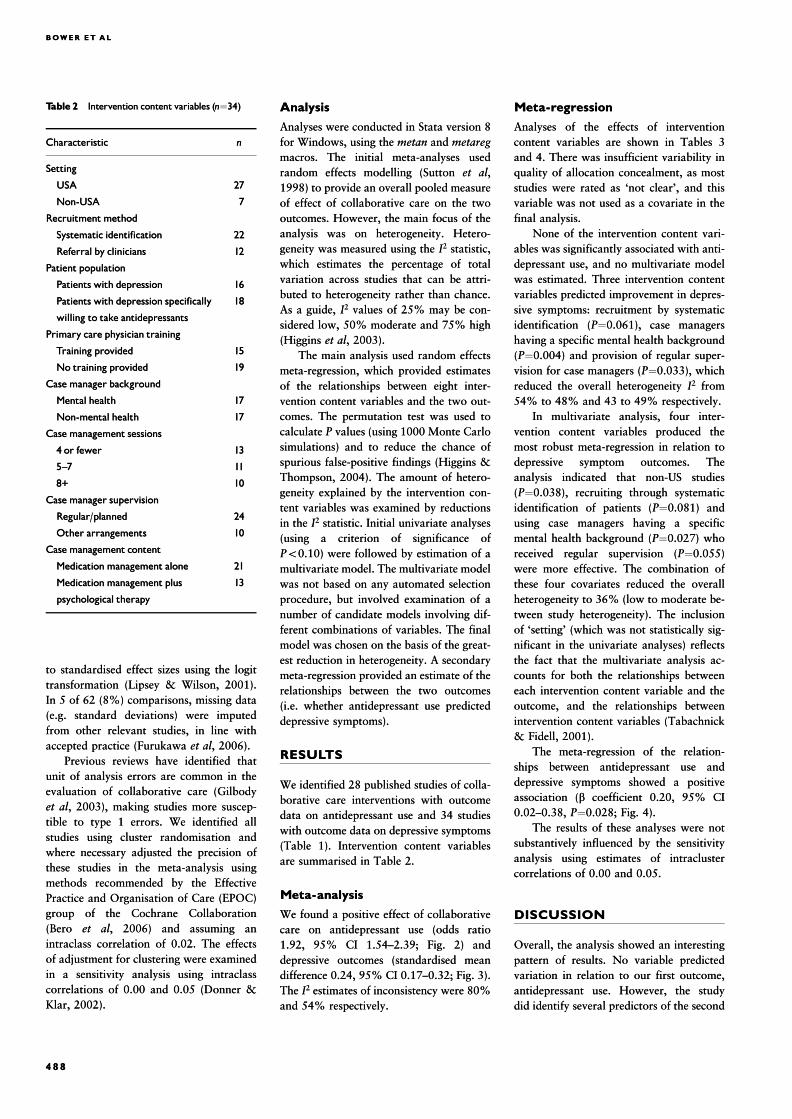
Meta-analysisMeta-analysis
We found a positive effect of collaborativeWe found a positive effect of collaborative
care on antidepressant use (odds ratiocare on antidepressant use (odds ratio
1.92, 95% CI 1.54–2.39; Fig. 2) and1.92, 95% CI 1.54–2.39; Fig. 2) and
depressive outcomes (standardised meandepressive outcomes (standardised mean
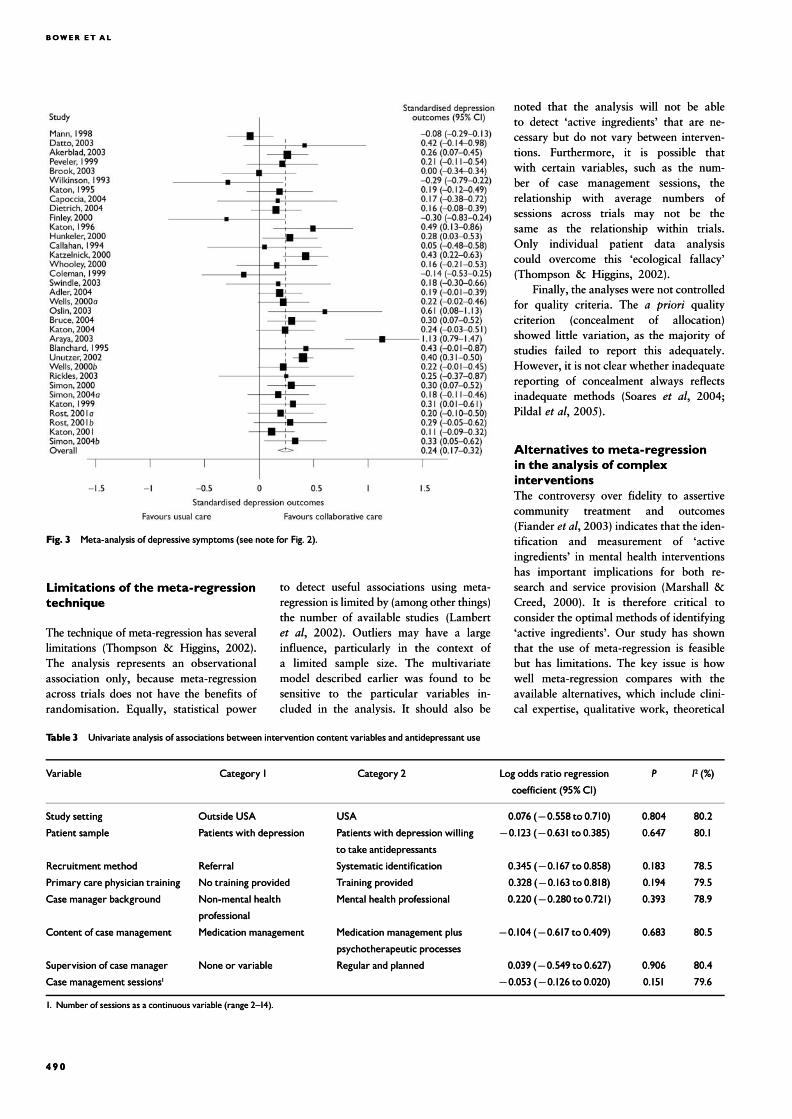
difference 0.24, 95% CI 0.17–0.32; Fig. 3).difference 0.24, 95% CI 0.17–0.32; Fig. 3).
TheThe II22 estimates of inconsistency were 80%estimates of inconsistency were 80%
and 54% respectively.and 54% respectively.
Meta-regressionMeta-regression
Analyses of the effects of interventionAnalyses of the effects of intervention
content variables are shown in Tables 3content variables are shown in Tables 3
and 4. There was insufficient variability inand 4. There was insufficient variability in
quality of allocation concealment, as mostquality of allocation concealment, as most
studies were rated as ‘not clear’, and thisstudies were rated as ‘not clear’, and this
variable was not used as a covariate in thevariable was not used as a covariate in the
final analysis.final analysis.
None of the intervention content vari-None of the intervention content vari-
ables was significantly associated with anti-ables was significantly associated with anti-
depressant use, and no multivariate modeldepressant use, and no multivariate model
was estimated. Three intervention contentwas estimated. Three intervention content
variables predicted improvement in depres-variables predicted improvement in depres-
sive symptoms: recruitment by systematicsive symptoms: recruitment by systematic
identification (identification (PP¼0.061), case managers0.061), case managers
having a specific mental health backgroundhaving a specific mental health background
((PP¼0.004) and provision of regular super-0.004) and provision of regular super-
vision for case managers (vision for case managers (PP¼0.033), which0.033), which
reduced the overall heterogeneityreduced the overall heterogeneity II22 fromfrom
54% to 48% and 43 to 49% respectively.54% to 48% and 43 to 49% respectively.
In multivariate analysis, four inter-In multivariate analysis, four inter-
vention content variables produced thevention content variables produced the
most robust meta-regression in relation tomost robust meta-regression in relation to
depressive symptom outcomes. Thedepressive symptom outcomes. The
analysis indicated that non-US studiesanalysis indicated that non-US studies
((PP¼0.038), recruiting through systematic0.038), recruiting through systematic
identification of patients (identification of patients (PP¼0.081) and0.081) and
using case managers having a specificusing case managers having a specific
mental health background (mental health background (PP¼0.027) who0.027) who
received regular supervision (received regular supervision (PP¼0.055)0.055)
were more effective. The combination ofwere more effective. The combination of
these four covariates reduced the overallthese four covariates reduced the overall
heterogeneity to 36% (low to moderate be-heterogeneity to 36% (low to moderate be-
tween study heterogeneity). The inclusiontween study heterogeneity). The inclusion
of ‘setting’ (which was not statistically sig-of ‘setting’ (which was not statistically sig-
nificant in the univariate analyses) reflectsnificant in the univariate analyses) reflects
the fact that the multivariate analysis ac-the fact that the multivariate analysis ac-
counts for both the relationships betweencounts for both the relationships between
each intervention content variable and theeach intervention content variable and the
outcome, and the relationships betweenoutcome, and the relationships between
intervention content variables (Tabachnickintervention content variables (Tabachnick
& Fidell, 2001).& Fidell, 2001).
The meta-regression of the relation-The meta-regression of the relation-
ships between antidepressant use andships between antidepressant use and
depressive symptoms showed a positivedepressive symptoms showed a positive
association (association (bb coefficient 0.20, 95% CIcoefficient 0.20, 95% CI
0.02–0.38,0.02–0.38, PP¼0.028; Fig. 4).0.028; Fig. 4).
The results of these analyses were notThe results of these analyses were not
substantively influenced by the sensitivitysubstantively influenced by the sensitivity
analysis using estimates of intraclusteranalysis using estimates of intracluster
correlations of 0.00 and 0.05.correlations of 0.00 and 0.05.
DISCUSSIONDISCUSSION
Overall, the analysis showed an interestingOverall, the analysis showed an interesting
pattern of results. No variable predictedpattern of results. No variable predicted
variation in relation to our first outcome,variation in relation to our first outcome,
antidepressant use. However, the studyantidepressant use. However, the study
did identify several predictors of the seconddid identify several predictors of the second
4 8 84 8 8
Table 2Table 2 Intervention content variables (Intervention content variables (nn¼34)34)
CharacteristicCharacteristic nn
SettingSetting
USAUSA 2727
Non-USANon-USA 77
RecruitmentmethodRecruitmentmethod
Systematic identificationSystematic identification 2222
Referral by cliniciansReferral by clinicians 1212
Patient populationPatient population
Patients with depressionPatients with depression 1616
Patients with depression specificallyPatients with depression specifically
willing to take antidepressantswilling to take antidepressants
1818
Primary care physician trainingPrimary care physician training
Training providedTraining provided 1515
No training providedNo training provided 1919
Case manager backgroundCase manager background
Mental healthMental health 1717
Non-mental healthNon-mental health 1717
Case management sessionsCase management sessions
4 or fewer4 or fewer 1313
5^75^7 1111
8+8+ 1010
Case manager supervisionCase manager supervision
Regular/plannedRegular/planned 2424
Other arrangementsOther arrangements 1010
Case management contentCase management content
Medicationmanagement aloneMedicationmanagement alone 2121
Medicationmanagement plusMedication management plus
psychological therapypsychological therapy
1313
COLLABORATIVE CARE FOR DEPRES S IONCOLLABORATIVE CARE FOR DEPRES S ION
outcome, depressive symptoms. Further-outcome, depressive symptoms. Further-
more, antidepressant use did predictmore, antidepressant use did predict
depressive symptom outcomes, whichdepressive symptom outcomes, which
suggests that effects of collaborative caresuggests that effects of collaborative care
on the latter may be mediated throughon the latter may be mediated through
changes in the former. However, it ischanges in the former. However, it is
not clear whether this association wouldnot clear whether this association would
remain significant if the antidepressant useremain significant if the antidepressant use
variables were analysed alongside the othervariables were analysed alongside the other
intervention content variables. Clearly theintervention content variables. Clearly the
causal pathways between interventioncausal pathways between intervention
content variables, intermediate outcomescontent variables, intermediate outcomes
(such as antidepressant use) and final(such as antidepressant use) and final
outcomes (such as depressive symptoms)outcomes (such as depressive symptoms)
are potentially complex, and analyticare potentially complex, and analytic
techniques such as path analysis might betechniques such as path analysis might be
useful in examining these relationshipsuseful in examining these relationships
further.further.
If the associations between interventionIf the associations between intervention
content variables and depressive symptomcontent variables and depressive symptom
outcomes are robust, they have interestingoutcomes are robust, they have interesting
implications for the design of collaborativeimplications for the design of collaborative
care interventions. For example, the use ofcare interventions. For example, the use of
case managers with a mental health back-case managers with a mental health back-
ground and regular specialist supervisionground and regular specialist supervision
both predict outcomes, which suggests thatboth predict outcomes, which suggests that
expertise is important. This may have im-expertise is important. This may have im-
plications for the involvement of the newplications for the involvement of the new
paraprofessional graduate workers in colla-paraprofessional graduate workers in colla-
borative care models (Whitty & Gilbody,borative care models (Whitty & Gilbody,
2005).2005).
Clearly the meta-regression cannotClearly the meta-regression cannot
determine the process by which expertisedetermine the process by which expertise
has its influence. This may relate to specifichas its influence. This may relate to specific
technical skills, such as knowledge of anti-technical skills, such as knowledge of anti-
depressants or the effective use of psy-depressants or the effective use of psy-
chotherapeutic techniques, or may reflectchotherapeutic techniques, or may reflect
non-specific skills, such as the ability to en-non-specific skills, such as the ability to en-
gage with patients or to work effectively ingage with patients or to work effectively in
collaboration with other professionals.collaboration with other professionals.
Exploration of this issue might benefit fromExploration of this issue might benefit from
qualitative research on the nature ofqualitative research on the nature of
patient–professional and interprofessionalpatient–professional and interprofessional
contact in collaborative care, and thecontact in collaborative care, and the
influence of context and organisationalinfluence of context and organisational
variables (Weavervariables (Weaver et alet al, 2003)., 2003).
However, models of care which requireHowever, models of care which require
personnel with significant expertise arepersonnel with significant expertise are
likely to be more difficult to implement inlikely to be more difficult to implement in
some contexts, which may limit their use-some contexts, which may limit their use-
fulness, reflecting the potential tensionfulness, reflecting the potential tension
between ‘efficacy’ as demonstrated in trialsbetween ‘efficacy’ as demonstrated in trials
and ‘effectiveness’ in routine contexts. Also,and ‘effectiveness’ in routine contexts. Also,
models using expert personnel may be moremodels using expert personnel may be more
costly, which raises issues about trade-offscostly, which raises issues about trade-offs
between effectiveness and cost that need tobetween effectiveness and cost that need to
be considered when designing collaborativebe considered when designing collaborative
care interventions.care interventions.
Limitations of the systematicLimitations of the systematicreviewreview
As a complex intervention, collaborativeAs a complex intervention, collaborative
care defies simple definition. Our decisionscare defies simple definition. Our decisions
about inclusion and exclusion were in-about inclusion and exclusion were in-
formed by our previous conceptual workformed by our previous conceptual work
(Bower & Gilbody, 2005), but we took a(Bower & Gilbody, 2005), but we took a
liberal approach to inclusion precisely be-liberal approach to inclusion precisely be-
cause the study focused on the degree tocause the study focused on the degree to
which variability in collaborative carewhich variability in collaborative care
models influenced outcomes. Clearly the in-models influenced outcomes. Clearly the in-
clusion or exclusion of particular studiesclusion or exclusion of particular studies
may have important implications, and thusmay have important implications, and thus
our findings should be considered explora-our findings should be considered explora-
tory rather than definitive. It should alsotory rather than definitive. It should also
be noted that most studies were conductedbe noted that most studies were conducted
in the USA and the results may notin the USA and the results may not
generalise to other contexts. Setting was ageneralise to other contexts. Setting was a
significant predictor in the multivariatesignificant predictor in the multivariate
analysis.analysis.
The validity of the coding scheme usedThe validity of the coding scheme used
to extract data on the interventions hasto extract data on the interventions has
not been confirmed. As noted previously,not been confirmed. As noted previously,
there were problems of inconsistent report-there were problems of inconsistent report-
ing and missing data in the publisheding and missing data in the published
studies. A significant proportion of inter-studies. A significant proportion of inter-
vention content variables could not bevention content variables could not be
included as they were not reported consis-included as they were not reported consis-
tently, and it is unlikely that it would havetently, and it is unlikely that it would have
been possible to extract data on many addi-been possible to extract data on many addi-
tional issues. However, it remains possibletional issues. However, it remains possible
that other variables might be more effectivethat other variables might be more effective
predictors than those included in ourpredictors than those included in our
analyses.analyses.
The difficulties encountered in derivingThe difficulties encountered in deriving
a full description of the interventionsa full description of the interventions
echoes traditional problems with poor re-echoes traditional problems with poor re-
porting in randomised trials. There mayporting in randomised trials. There may
be a case for adopting a more standardisedbe a case for adopting a more standardised
approach to the reporting of the content ofapproach to the reporting of the content of
complex interventions (equivalent tocomplex interventions (equivalent to
CONSORT (Consolidated Standards ofCONSORT (Consolidated Standards of
Reporting Trials; MoherReporting Trials; Moher et alet al, 2001) and, 2001) and
QUOROM (Quality of Reporting Meta-QUOROM (Quality of Reporting Meta-
analyses; Moheranalyses; Moher et alet al, 1999) in order to, 1999) in order to
overcome these problems. The proliferationovercome these problems. The proliferation
of web-based journal archives for the pre-of web-based journal archives for the pre-
sentation of data outside the word limitssentation of data outside the word limits
of the paper-based journals provides anof the paper-based journals provides an
appropriate platform. However, determin-appropriate platform. However, determin-
ing the appropriate content and structureing the appropriate content and structure
of such standardised reports would be chal-of such standardised reports would be chal-
lenging, given the potential range of pro-lenging, given the potential range of pro-
cesses involved in complex interventions.cesses involved in complex interventions.
4 8 94 8 9
Fig. 2Fig. 2 Meta-analysis of antidepressant use.Note: theWells (2000) and Simon (2004) studies involved twoMeta-analysis of antidepressant use.Note: theWells (2000) and Simon (2004) studies involved two
intervention groups compared against a single control; to avoid double-counting the controls, the sample sizeintervention groups compared against a single control; to avoid double-counting the controls, the sample size
and event rate in the control were divided by 2.The Rost 2001study data are only available analysed in twoand event rate in the control were divided by 2.The Rost 2001study data are only available analysed in two
subgroups, rather than as an overall analysis; in our analysis these subgroups were treated as separatesubgroups, rather than as an overall analysis; in our analysis these subgroups were treated as separate
comparisons.comparisons.
BOWER ET ALBOWER ET AL
Limitations of the meta-regressionLimitations of the meta-regressiontechniquetechnique
The technique of meta-regression has severalThe technique of meta-regression has several
limitations (Thompson & Higgins, 2002).limitations (Thompson & Higgins, 2002).
The analysis represents an observationalThe analysis represents an observational
association only, because meta-association only, because meta-regressionregression
across trials does not have the benefits ofacross trials does not have the benefits of
randomisation. Equally, statistical powerrandomisation. Equally, statistical power
to detect useful associations using meta-to detect useful associations using meta-
regression is limited by (among other things)regression is limited by (among other things)
the number of availablethe number of available studies (Lambertstudies (Lambert
et alet al, 2002). Outliers may have a large, 2002). Outliers may have a large
influence, particularly in the context ofinfluence, particularly in the context of
a limited sample size. The multivariatea limited sample size. The multivariate
model described earlier was found to bemodel described earlier was found to be
sensitive to the particular variables in-sensitive to the particular variables in-
cluded in the analysis. It should also becluded in the analysis. It should also be
noted that the analysis will not be ablenoted that the analysis will not be able
to detect ‘active ingredients’ that are ne-to detect ‘active ingredients’ that are ne-
cessary but do not vary between interven-cessary but do not vary between interven-
tions. Furthermore, it is possible thattions. Furthermore, it is possible that
with certain variables, such as the num-with certain variables, such as the num-
ber of case management sessions, theber of case management sessions, the
relationship with average numbers ofrelationship with average numbers of
sessions across trials may not be thesessions across trials may not be the
same as the relationship within trials.same as the relationship within trials.
Only individual patient data analysisOnly individual patient data analysis
could overcome this ‘ecological fallacy’could overcome this ‘ecological fallacy’
(Thompson & Higgins, 2002).(Thompson & Higgins, 2002).
Finally, the analyses were not controlledFinally, the analyses were not controlled
for quality criteria. Thefor quality criteria. The a prioria priori qualityquality
criterion (concealment of allocation)criterion (concealment of allocation)
showed little variation, as the majority ofshowed little variation, as the majority of
studies failed to report this adequately.studies failed to report this adequately.
However, it is not clear whether inadequateHowever, it is not clear whether inadequate
reporting of concealment always reflectsreporting of concealment always reflects
inadequate methods (Soaresinadequate methods (Soares et alet al, 2004;, 2004;
PildalPildal et alet al, 2005)., 2005).
Alternatives to meta-regressionAlternatives to meta-regressionin the analysis of complexin the analysis of complexinterventionsinterventionsThe controversy over fidelity to assertiveThe controversy over fidelity to assertive
community treatment and outcomescommunity treatment and outcomes
(Fiander(Fiander et alet al, 2003) indicates that the iden-, 2003) indicates that the iden-
tification and measurement of ‘activetification and measurement of ‘active
ingredients’ in mental health interventionsingredients’ in mental health interventions
has important implications for both re-has important implications for both re-
search and service provision (Marshall &search and service provision (Marshall &
Creed, 2000). It is therefore critical toCreed, 2000). It is therefore critical to
consider the optimal methods of identifyingconsider the optimal methods of identifying
‘active ingredients’. Our study has shown‘active ingredients’. Our study has shown
that the use of meta-regression is feasiblethat the use of meta-regression is feasible
but has limitations. The key issue is howbut has limitations. The key issue is how
well meta-regression compares with thewell meta-regression compares with the
available alternatives, which include clini-available alternatives, which include clini-
cal expertise, qualitative work, theoreticalcal expertise, qualitative work, theoretical
4 9 04 9 0
Fig. 3Fig. 3 Meta-analysis of depressive symptoms (see note for Fig. 2).Meta-analysis of depressive symptoms (see note for Fig. 2).
Table 3Table 3 Univariate analysis of associations between intervention content variables and antidepressant useUnivariate analysis of associations between intervention content variables and antidepressant use
VariableVariable Category1Category1 Category 2Category 2 Log odds ratio regressionLog odds ratio regression
coefficient (95% CI)coefficient (95% CI)
PP II22 (%)(%)
Study settingStudy setting Outside USAOutside USA USAUSA 0.076 (0.076 (770.558 to 0.710)0.558 to 0.710) 0.8040.804 80.280.2
Patient samplePatient sample Patients with depressionPatients with depression Patients with depression willingPatients with depression willing
to take antidepressantsto take antidepressants
770.123 (0.123 (770.631 to 0.385)0.631 to 0.385) 0.6470.647 80.180.1
RecruitmentmethodRecruitmentmethod ReferralReferral Systematic identificationSystematic identification 0.345 (0.345 (770.167 to 0.858)0.167 to 0.858) 0.1830.183 78.578.5
Primary care physician trainingPrimary care physician training No training providedNo training provided Training providedTraining provided 0.328 (0.328 (770.163 to 0.818)0.163 to 0.818) 0.1940.194 79.579.5
Case manager backgroundCase manager background Non-mental healthNon-mental health
professionalprofessional
Mental health professionalMental health professional 0.220 (0.220 (770.280 to 0.721)0.280 to 0.721) 0.3930.393 78.978.9
Content of case managementContent of case management MedicationmanagementMedicationmanagement Medicationmanagement plusMedicationmanagement plus
psychotherapeutic processespsychotherapeutic processes
770.104 (0.104 (770.617 to 0.409)0.617 to 0.409) 0.6830.683 80.580.5
Supervision of case managerSupervision of case manager None or variableNone or variable Regular and plannedRegular and planned 0.039 (0.039 (770.549 to 0.627)0.549 to 0.627) 0.9060.906 80.480.4
Case management sessionsCase management sessions11 770.053 (0.053 (770.126 to 0.020)0.126 to 0.020) 0.1510.151 79.679.6
1. Number of sessions as a continuous variable (range 2^14).1. Number of sessions as a continuous variable (range 2^14).

COLLABORATIVE CARE FOR DEPRES S IONCOLLABORATIVE CARE FOR DEPRES S ION
models and ‘dismantling’ or ‘factorial’models and ‘dismantling’ or ‘factorial’
trials.trials.
Clinical expertise is a potentially usefulClinical expertise is a potentially useful
source of hypotheses, and rigorous qualita-source of hypotheses, and rigorous qualita-
tive work is ideally suited to capture thetive work is ideally suited to capture the
complexity of care processes, and is espe-complexity of care processes, and is espe-
cially useful at exploring the perspectivescially useful at exploring the perspectives
of stakeholders and illuminating contextof stakeholders and illuminating context
(Weaver(Weaver et alet al, 2003; Marshall, 2003; Marshall et alet al,,
2004). However, it is unclear whether pa-2004). However, it is unclear whether pa-
tients and professionals can reliably identifytients and professionals can reliably identify
‘active ingredients’. Acknowledgement of‘active ingredients’. Acknowledgement of
the limitations of clinical expertise in iden-the limitations of clinical expertise in iden-
tifying causal mechanisms is fundamentaltifying causal mechanisms is fundamental
to evidence-based medicine, and patientsto evidence-based medicine, and patients
will presumably face many of the samewill presumably face many of the same
challenges as professionals. Insights fromchallenges as professionals. Insights from
theoretical models are another usefultheoretical models are another useful
source, but few theoretical models withinsource, but few theoretical models within
mental health services research are so wellmental health services research are so well
validated that they provide a comprehen-validated that they provide a comprehen-
sive description of ‘active ingredients’, andsive description of ‘active ingredients’, and
complex mental health issues such ascomplex mental health issues such as
depression will have many competingdepression will have many competing
theories. Although theory is a necessarytheories. Although theory is a necessary
aspect of the development of a complexaspect of the development of a complex
intervention, it will rarely be sufficient.intervention, it will rarely be sufficient.
Dismantling and factorial studies testDismantling and factorial studies test
different combinations of ingredientsdifferent combinations of ingredients
within a randomised comparison. Relevantwithin a randomised comparison. Relevant
examples exist in the collaborative careexamples exist in the collaborative care
literature. For example, a recent studyliterature. For example, a recent study
compared outcomes in patients randomisedcompared outcomes in patients randomised
to a depression care programme (includingto a depression care programme (including
systematic follow-up) and systematicsystematic follow-up) and systematic
follow-up alone. There was no differencefollow-up alone. There was no difference
in outcomes, suggesting that systematicin outcomes, suggesting that systematic
follow-up is critical (Vergouwenfollow-up is critical (Vergouwen et alet al,,
2005). The advantage of such designs is2005). The advantage of such designs is
that randomisation is preserved, allowingthat randomisation is preserved, allowing
causal inference. However, the use of suchcausal inference. However, the use of such
costly designs to identify ‘active ingredi-costly designs to identify ‘active ingredi-
ents’ may not always be the optimal useents’ may not always be the optimal use
of limited research resources.of limited research resources.
Clearly comparisons of the differentClearly comparisons of the different
methods are required, and the interventionmethods are required, and the intervention
development currently being conducted bydevelopment currently being conducted by
the authors also includes qualitative workthe authors also includes qualitative work
which can be compared with the findingswhich can be compared with the findings
of the meta-regression. It is likely thatof the meta-regression. It is likely that
complex interventions will increasingly becomplex interventions will increasingly be
required to improve patient care withinrequired to improve patient care within
mental health, and the evaluation of suchmental health, and the evaluation of such
interventions raises particular challenges.interventions raises particular challenges.
Although there are potential problems withAlthough there are potential problems with
the application of meta-regression, wethe application of meta-regression, we
conclude that the technique has potentialconclude that the technique has potential
in developing useful insights into the activein developing useful insights into the active
ingredients in complex interventions iningredients in complex interventions in
mental health, and thus assist in the designmental health, and thus assist in the design
and evaluation of future interventions.and evaluation of future interventions.
ACKNOWLEDGEMENTSACKNOWLEDGEMENTS
The study was implemented in the context ofThe study was implemented in the context ofresearch led by D.R. (funded by the Medicalresearch led by D.R. (funded by the MedicalResearch Council) in which P.B. and S.G. are grantResearch Council) in which P.B. and S.G. are grantholders. P.B. and J.F. are funded through the Depart-holders. P.B. and J.F. are funded through the Depart-ment of Health, but the views expressed in thisment of Health, but the views expressed in thispaper are those of the authors alone. P.B. thankspaper are those of the authors alone. P.B. thanksJohn Cape for useful input into the paper.John Cape for useful input into the paper.
REFERENCESREFERENCES
Adler, D., Bungay, K.,Wilson, I.,Adler, D., Bungay, K.,Wilson, I., et alet al (2004)(2004) TheTheimpact of a pharmacist intervention on 6 monthimpact of a pharmacist intervention on 6 monthoutcomes in depressed primary care patients.outcomes in depressed primary care patients.GeneralGeneralHospital PsychiatryHospital Psychiatry,, 2626, 199^209., 199^209.
4 914 91
Table 4Table 4 Univariate analysis of associations between intervention content variables and depressive symptomsUnivariate analysis of associations between intervention content variables and depressive symptoms
VariableVariable Category1Category1 Category 2Category 2 Effect size regressionEffect size regression
coefficient (95% CI)coefficient (95% CI)
PP II22 (%)(%)
Study settingStudy setting Outside USAOutside USA USAUSA 0.007 (0.007 (770.193 to 0.206)0.193 to 0.206) 0.9300.930 54.454.4
Patient samplePatient sample Patients with depressionPatients with depression Patients with depression willingPatients with depression willing
to take antidepressantsto take antidepressants
770.087 (0.087 (770.243 to 0.070)0.243 to 0.070) 0.2850.285 52.152.1
RecruitmentmethodRecruitmentmethod ReferralReferral Systematic identificationSystematic identification 0.146 (0.146 (770.014 to 0.306)0.014 to 0.306) 0.0610.061 47.847.8
Primary care physician trainingPrimary care physician training No training providedNo training provided Training providedTraining provided 0.093 (0.093 (770.065 to 0.252)0.065 to 0.252) 0.2370.237 54.954.9
Case manager backgroundCasemanager background Non-mental healthNon-mental health
professionalprofessional
Mental health professionalMental health professional 0.187 (0.046 to 0.327)0.187 (0.046 to 0.327) 0.0040.004 42.742.7
Content of case managementContent of case management MedicationmanagementMedicationmanagement Medicationmanagement plusMedicationmanagement plus
psychotherapeutic processespsychotherapeutic processes
0.093 (0.093 (770.064 to 0.250)0.064 to 0.250) 0.2060.206 50.750.7
Supervision of case managerSupervision of case manager None or variableNone or variable Regular and plannedRegular and planned 0.169 (0.002 to 0.337)0.169 (0.002 to 0.337) 0.0330.033 49.349.3
Case management sessionsCase management sessions11 0.015 (0.015 (770.008 to 0.039)0.008 to 0.039) 0.1740.174 50.950.9
1. Number of sessions as a continuous variable (range 2^14).1. Number of sessions as a continuous variable (range 2^14).
Fig. 4Fig. 4 Relationship between antidepressant use outcomes and depressive symptoms outcomes.Relationship between antidepressant use outcomes and depressive symptoms outcomes.

BOWER ET ALBOWER ET AL
Araya, R., Rojas, G., Fritsch, R.,Araya, R., Rojas,G., Fritsch, R., et alet al (2003)(2003) TreatingTreatingdepression in primary care in low income women indepression in primary care in low income women inSantiago,Chile: a randomised controlled trial.Santiago,Chile: a randomised controlled trial. LancetLancet,,361361, 995^1000., 995^1000.
Bero, L., Eccles, M., Grilli, R.,Bero, L., Eccles, M.,Grilli, R., et alet al (2006)(2006) About theAbout theCochrane Collaboration (Art.No. EPOC).Cochrane Collaboration (Art.No. EPOC). CochraneCochraneReview GroupsReview Groups, Issue 2.Chichester:Wiley Interscience., Issue 2.Chichester:Wiley Interscience.
Bijl, D., van Marwijk,W., de Haan, M.,Bijl, D., van Marwijk,W., de Haan, M., et alet al (2004)(2004)Effectiveness of disease management programmes forEffectiveness of disease management programmes forrecognition, diagnosis and treatment of depression inrecognition, diagnosis and treatment of depression inprimary care: a review.primary care: a review. European Journal of GeneralEuropean Journal of GeneralPracticePractice,, 1010, 6^12., 6^12.
Blanchard, M.,Waterreus, A. & Mann, A. (1995)Blanchard, M.,Waterreus, A. & Mann, A. (1995) TheTheeffect of primary care nurse intervention upon oldereffect of primary care nurse intervention upon olderpeople screened as depressed.people screened as depressed. International Journal ofInternational Journal ofGeriatric PsychiatryGeriatric Psychiatry,, 1010, 289^298., 289^298.
Boudreau, D.,Capoccia, K., Sullivan, S.,Boudreau, D., Capoccia, K., Sullivan, S., et alet al (2002)(2002)Collaborative care to improve outcomes in majorCollaborative care to improve outcomes in majordepression.depression. Annals of PharmacotherapyAnnals of Pharmacotherapy,, 3636, 585^591., 585^591.
Bower, P. & Gilbody, S. (2005)Bower, P. & Gilbody, S. (2005) Managing commonManaging commonmental health disorders in primary care: conceptualmental health disorders in primary care: conceptualmodels and evidence base.models and evidence base. BMJBMJ,, 330330, 839^842., 839^842.
Bradley, F., Kinmonth, A., Mant, D.,Bradley, F., Kinmonth, A., Mant, D., et alet al (1999)(1999)Development and evaluation of complex interventions inDevelopment and evaluation of complex interventions inhealth services research: case study of the Southamptonhealth services research: case study of the Southamptonheart integrated care project (SHIP).heart integrated care project (SHIP). BMJBMJ,, 318318, 711^715., 711^715.
Brook,O., van Hout,H., Nieuwenhuyse,H.,Brook,O., van Hout,H., Nieuwenhuyse,H., et alet al(2003(2003aa)) Effects of coaching by community pharmacistsEffects of coaching by community pharmacistson psychological symptoms of antidepressant users: aon psychological symptoms of antidepressant users: arandomised controlled trial.randomised controlled trial. EuropeanEuropeanNeuropsychopharmacologyNeuropsychopharmacology,, 1313, 347^354., 347^354.
Brook,O., van Hout,H., Nieuwenhuyse,H.,Brook,O., van Hout,H., Nieuwenhuyse,H., et alet al(2003(2003bb)) Impact of coaching by community pharmacistsImpact of coaching by community pharmacistson drug attitude of depressive primary care patients andon drug attitude of depressive primary care patients andacceptability to patients: a randomized controlled trial.acceptability to patients: a randomized controlled trial.European NeuropsychopharmacologyEuropean Neuropsychopharmacology,, 1313, 1^9., 1^9.
Bruce, M.,Ten Have,T., Reynolds,C.,Bruce, M.,Ten Have,T., Reynolds,C., et alet al (2004)(2004)Reducing suicidal ideation and depressive symptoms inReducing suicidal ideation and depressive symptoms indepressed older primary care patients.depressed older primary care patients. JAMAJAMA,, 291291,,1081^1091.1081^1091.
Bungay, K., Adler, D., Rogers,W.,Bungay, K., Adler, D., Rogers,W., et alet al (2004)(2004)Description of a clinical pharmacist interventionDescription of a clinical pharmacist interventionadministered to primary care patients with depression.administered to primary care patients with depression.General Hospital PsychiatryGeneral Hospital Psychiatry,, 2626, 210^218., 210^218.
Callahan,C.,Hendrie,H., Dittus, R.,Callahan,C.,Hendrie,H., Dittus, R., et alet al (1994)(1994)Improving treatment of late life depression in primaryImproving treatment of late life depression in primarycare: a randomized clinical trial.care: a randomized clinical trial. Journal of the AmericanJournal of the AmericanGeriatrics SocietyGeriatrics Society,, 4242, 839^846., 839^846.
Campbell, M., Fitzpatrick, R.,Haines, A.,Campbell, M., Fitzpatrick, R.,Haines, A., et alet al(2000)(2000) Framework for design and evaluation of complexFramework for design and evaluation of complexinterventions to improve health.interventions to improve health. BMJBMJ,, 321321, 694^696., 694^696.
Capoccia, K., Boudreau, D., Blough, D.,Capoccia, K., Boudreau, D., Blough, D., et alet al (2004)(2004)Randomized trial of pharmacist interventions to improveRandomized trial of pharmacist interventions to improve
depression care and outcomes in primary care.depression care and outcomes in primary care. AmericanAmericanJournal of Health System PharmacyJournal of Health System Pharmacy,, 6161, 364^372., 364^372.
Coleman, E.,Grothaus, L., Sandhu,N.,Coleman, E., Grothaus, L., Sandhu,N., et alet al (1999)(1999)Chronic care clinics: a randomized controlled trial of aChronic care clinics: a randomized controlled trial of anew model of primary care for frail older adults.new model of primary care for frail older adults. JournalJournalof the American Geriatrics Societyof the American Geriatrics Society,, 4747, 775^783., 775^783.
Coyne, J., Brown,G., Datto,C.,Coyne, J., Brown,G., Datto,C., et alet al (2001)(2001) TheThebenefits of a broader perspective in case-finding forbenefits of a broader perspective in case-finding fordisease management of depression: early lessons fromdisease management of depression: early lessons fromthe PROSPECTstudy.the PROSPECTstudy. International Journal of GeriatricInternational Journal of GeriatricPsychiatryPsychiatry,, 1616, 570^576., 570^576.
Datto,C.,Thompson, R.,Horowitz, D.,Datto,C.,Thompson, R.,Horowitz, D., et alet al (2003)(2003)The pilot study of a telephone disease managementThe pilot study of a telephone disease managementprogram for depression.program for depression. General Hospital PsychiatryGeneral Hospital Psychiatry,, 2525,,169^177.169^177.
Dietrich, A.,Oxman,T.,Williams, J.,Dietrich, A.,Oxman,T.,Williams, J., et alet al (2004(2004aa))Going to scale: re-engineering systems for primary careGoing to scale: re-engineering systems for primary caretreatment of depression.treatment of depression. Annals of Family MedicineAnnals of Family Medicine,, 22,,301^304.301^304.
Dietrich, A.,Oxman,T.,Williams, J.,Dietrich, A.,Oxman,T.,Williams, J., et alet al (2004(2004bb))Re-engineering systems for the treatment of depressionRe-engineering systems for the treatment of depressionin primary care: cluster randomised controlled trial.in primary care: cluster randomised controlled trial. BMJBMJ,,329329, 605., 605.
Donner, A. & Klar,N. (2002)Donner, A. & Klar, N. (2002) Issues in the meta-Issues in the meta-analysis of cluster randomized trials.analysis of cluster randomized trials. Statistics inStatistics inMedicineMedicine,, 2121, 2971^2980., 2971^2980.
Fiander, M., Burns,T., McHugo,G.,Fiander, M., Burns,T., McHugo,G., et alet al (2003)(2003)Assertive community treatment across the Atlantic:Assertive community treatment across the Atlantic:comparison of model fidelity in the UK and USA.comparison of model fidelity in the UK and USA. BritishBritishJournal of PsychiatryJournal of Psychiatry,, 182182, 248^254., 248^254.
Finley, P., Rens, H., Gess, S.,Finley, P., Rens, H.,Gess, S., et alet al (1999)(1999) CaseCasemanagement of depression by clinical pharmacists in amanagement of depression by clinical pharmacists in aprimary care setting.primary care setting. FormularyFormulary,, 3434, 864^870., 864^870.
Finley, P., Rens, H., Pont, J.,Finley, P., Rens, H., Pont, J., et alet al (2003)(2003) Impact of aImpact of acollaborative care model on depression in a primarycollaborative care model on depression in a primarycare setting: a randomized controlled trial.care setting: a randomized controlled trial.PharmacotherapyPharmacotherapy,, 2323, 1175^1185., 1175^1185.
Furukawa,T., Barbui,C., Cipriani, A.,Furukawa,T., Barbui,C.,Cipriani, A., et alet al (2006)(2006)Imputing missing standard deviations in meta-analysesImputing missing standard deviations in meta-analysescan provide accurate results.can provide accurate results. Journal of ClinicalJournal of ClinicalEpidemiologyEpidemiology,, 5959, 7^10., 7^10.
Gilbody, S.,Whitty, P., Grimshaw, J.,Gilbody, S.,Whitty, P., Grimshaw, J., et alet al (2003)(2003)Educational and organisational interventions to improveEducational and organisational interventions to improvethe management of depression in primary care: athe management of depression in primary care: asystematic review.systematic review. JAMAJAMA,, 289289, 3145^3151., 3145^3151.
Higgins, J. & Thompson, S. (2004)Higgins, J. & Thompson, S. (2004) Controlling theControlling therisk of spurious findings frommeta-regression.risk of spurious findings frommeta-regression. StatisticsStatisticsin Medicinein Medicine,, 2323, 1663^1682., 1663^1682.
Higgins, J.,Thompson, S., Deeks, J.,Higgins, J.,Thompson, S., Deeks, J., et alet al (2003)(2003)Measuring inconsistency in meta-analyses.Measuring inconsistency in meta-analyses. BMJBMJ,, 327327,,557^560.557^560.
Hunkeler, E., Meresman, J., Hargreaves,W.,Hunkeler, E., Meresman, J., Hargreaves,W., et alet al(2000)(2000) Efficacy of nurse telehealth care and peerEfficacy of nurse telehealth care and peersupport in augmenting treatment of depression insupport in augmenting treatment of depression inprimary care.primary care. Archives of Family MedicineArchives of Family Medicine,, 99, 700^708., 700^708.
Katon,W.,Von Korff, M., Lin, E.,Katon,W.,Von Korff, M., Lin, E., et alet al (1995)(1995)Collaborative management to achieve treatmentCollaborative management to achieve treatmentguidelines: impact on depression in primary care.guidelines: impact on depression in primary care. JAMAJAMA,,273273, 1026^1031., 1026^1031.
Katon,W., Robinson, P.,Von Korff, M.,Katon,W., Robinson, P.,Von Korff, M., et alet al (1996)(1996)Amultifaceted intervention to improve treatment ofA multifaceted intervention to improve treatment ofdepression in primary care.depression in primary care. Archives of GeneralArchives of GeneralPsychiatryPsychiatry,, 5353, 924^932., 924^932.
Katon,W.,Von Korff, M., Lin, E.,Katon,W.,Von Korff, M., Lin, E., et alet al (1999)(1999) SteppedSteppedcollaborative care for primary care patients withcollaborative care for primary care patients withpersistent symptoms of depression: a randomized trial.persistent symptoms of depression: a randomized trial.Archives of General PsychiatryArchives of General Psychiatry,, 5656, 1109^1115., 1109^1115.
4 9 24 9 2
AppendixAppendix Initial intervention content variablesInitial intervention content variables
VariableVariable DescriptionDescription
SettingSetting What was the geographical location of the study?What was the geographical location of the study?Patient populationPatient population Did the population include all patients with depression, or was itDid the population include all patients with depression, or was it
restricted to patients who had depression and were currently taking,restricted to patients who had depression and were currently taking,or willing to take, antidepressants?or willing to take, antidepressants?
ScreeningScreening Were patients referred by their primary care providers, or systematicallyWere patients referred by their primary care providers, or systematicallyidentified (e.g. through screening)?identified (e.g. through screening)?
Primary care providersPrimary care providersPCP professional groupPCP professional group What was the professional background of the primary care providers?What was the professional background of the primary care providers?PCP training and educationPCP training and education What training and education did the primary care providers receive?What training and education did the primary care providers receive?PCP EBM guidelines?PCP EBM guidelines? Did the primary care providers receive an evidence-based guideline?Did the primary care providers receive an evidence-based guideline?PCP T+E timePCP T+E time Howmuch timewas involved in the training of the primary care providers?Howmuch timewas involved in the training of the primary care providers?PCP T+E materialsPCP T+E materials What other materials were used in the training of the primary careWhat other materials were used in the training of the primary care
providers?providers?Case managersCase managers
CM professional groupCM professional group What was the professional background of the case managers?What was the professional background of the case managers?CM training and educationCM training and education What training and education did the case managers receive?What training and education did the case managers receive?CM T+E timeCM T+E time Howmuch time was involved in the training of the case managers?How much time was involved in the training of the case managers?CM T+E materialsCM T+E materials What other materials were used in the training of the case managers?What other materials were used in the training of the case managers?CM session number plannedCM session number planned Howmany case management sessions were planned?How many case management sessions were planned?CM session frequency plannedCM session frequency planned How often were case management sessions designed to be delivered?How often were case management sessions designed to be delivered?CM session duration plannedCM session duration planned What was the planned duration of case management sessions?What was the planned duration of case management sessions?CM total time plannedCM total time planned What was the total planned time for the case management?What was the total planned time for the case management?CM session number deliveredCM session number delivered Howmany case management sessions were delivered?How many case management sessions were delivered?CM session frequency deliveredCM session frequency delivered How often were case management sessions delivered?How often were case management sessions delivered?CM session duration deliveredCM session duration delivered What was the actual duration of case management sessions?What was the actual duration of case management sessions?CM total time deliveredCM total time delivered What was the actual total time for the case management?What was the actual total time for the case management?CM intervention contentCM intervention content What was the content of the case management sessions?What was the content of the case management sessions?CM intervention patientCM intervention patientmaterialsmaterials
What patient materials were used in the case management session?What patient materials were used in the case management session?
CM liaison with PCPCM liaison with PCP How did the case manager liaise with the primary care provider?How did the case manager liaise with the primary care provider?Specialist careSpecialist care
Specialist professional groupSpecialist professional group What was the professional background of the specialist?What was the professional background of the specialist?Specialist training and educationSpecialist training and education What training and education did the specialist receive?What training and education did the specialist receive?Specialist liaison with PCPSpecialist liaison with PCP How did the specialist liaise with the primary care provider?How did the specialist liaise with the primary care provider?Specialist liaison with CMSpecialist liaison with CM How did the specialist liaise with the case manager?How did the specialist liaise with the case manager?
CM, case manager; EBM, evidence-based medicine; PCP, primary care provider;T+E, training and education.CM, case manager; EBM, evidence-based medicine; PCP, primary care provider;T+E, training and education.

COLLABORATIVE CARE FOR DEPRES S IONCOLLABORATIVE CARE FOR DEPRES S ION
Katon,W., Rutter,C., Ludman, E.,Katon,W., Rutter,C., Ludman, E., et alet al (2001(2001aa)) AArandomized trial of relapse prevention of depression inrandomized trial of relapse prevention of depression inprimary care.primary care. Archives of General PsychiatryArchives of General Psychiatry,, 5858, 241^247., 241^247.
Katon,W.,Von Korff, M., Lin, E.,Katon,W.,Von Korff, M., Lin, E., et alet al (2001(2001bb))Rethinking practitioner roles in chronic illness: theRethinking practitioner roles in chronic illness: thespecialist, primary care physician and the practice nurse.specialist, primary care physician and the practice nurse.General Hospital PsychiatryGeneral Hospital Psychiatry,, 2323, 138^144., 138^144.
Katon,W.,Von Korff, M., Lin, E.,Katon,W.,Von Korff, M., Lin, E., et alet al (2003)(2003)Improving primary care treatment of depression amongImproving primary care treatment of depression amongpatients with diabetes mellitus: the design of thepatients with diabetes mellitus: the design of thepathways study.pathways study.General Hospital PsychiatryGeneral Hospital Psychiatry,, 2525, 158^168., 158^168.
Katon,W.,Von Korff, M., Lin, E.,Katon,W.,Von Korff, M., Lin, E., et alet al (2004)(2004) TheThePathways Study: a randomized trial of collaborative carePathways Study: a randomized trial of collaborative carein patients with diabetes and depression.in patients with diabetes and depression. Archives ofArchives ofGeneral PsychiatryGeneral Psychiatry,, 6161, 1042^1049., 1042^1049.
Katzelnick, D., Simon,G., Pearson, S.,Katzelnick, D., Simon,G., Pearson, S., et alet al (2000)(2000)Randomized trial of a depression management programRandomized trial of a depression management programin high utilizers of medical care.in high utilizers of medical care. Archives of FamilyArchives of FamilyMedicineMedicine,, 99, 345^351., 345^351.
Lambert, P., Sutton, A., Abrams, K.,Lambert, P., Sutton, A., Abrams, K., et alet al (2002)(2002) AAcomparison of summary patient-level covariates in meta-comparison of summary patient-level covariates in meta-regression with individual patient data meta-analysis.regression with individual patient data meta-analysis.Journal of Clinical EpidemiologyJournal of Clinical Epidemiology,, 5555, 86^94., 86^94.
Lipsey, M. & Wilson, D. (2001)Lipsey, M. & Wilson, D. (2001) Practical Meta-AnalysisPractical Meta-Analysis..Thousand Oaks,CA: Sage.Thousand Oaks,CA: Sage.
Loeb, M. (2002)Loeb, M. (2002) Application of the development stagesApplication of the development stagesof a cluster randomized trial to a framework forof a cluster randomized trial to a framework forevaluating complex health interventions.evaluating complex health interventions. BMC HealthBMC HealthServices ResearchServices Research,, 22, 13., 13.
Mann, A., Blizard, R., Murray, J.,Mann, A., Blizard, R., Murray, J., et alet al (1998)(1998) AnAnevaluation of practice nurses working with generalevaluation of practice nurses working with generalpractitioners to treat people with depression.practitioners to treat people with depression. BritishBritishJournal of General PracticeJournal of General Practice,, 4848, 875^879., 875^879.
Marshall, M. & Creed, F. (2000)Marshall, M. & Creed, F. (2000) Assertive communityAssertive communitytreatment ^ is it the future of community care in thetreatment ^ is it the future of community care in theUK?UK? International Review of PsychiatryInternational Review of Psychiatry,, 1212, 191^196., 191^196.
Marshall, M., Lockwood, A., Lewis, S.,Marshall, M., Lockwood, A., Lewis, S., et alet al (2004)(2004)Essential elements of an early intervention service forEssential elements of an early intervention service forpsychosis: the opinions of expert clinicians.psychosis: the opinions of expert clinicians. BMCBMCPsychiatryPsychiatry,, 44, 17., 17.
Medical Research Council (2000)Medical Research Council (2000) A Framework forA Framework forDevelopment and Evaluation of RCTs for ComplexDevelopment and Evaluation of RCTs for ComplexInterventions to Improve HealthInterventions to Improve Health. London: MRC.. London:MRC.
Moher, D.,Cook, D., Eastwood, S.,Moher, D., Cook, D., Eastwood, S., et alet al (1999)(1999)Improving the quality of reports of meta-analyses ofImproving the quality of reports of meta-analyses ofrandomised controlled trials: the QUORUM statement.randomised controlled trials: the QUORUM statement.LancetLancet,, 354354, 1896^1900., 1896^1900.
Moher, D., Schutz, K. & Altman, D. (2001)Moher, D., Schutz, K. & Altman, D. (2001) TheTheCONSORTstatement: revised recommendations forCONSORTstatement: revised recommendations forimproving the quality of reports of parallel-groupimproving the quality of reports of parallel-grouprandomised trials.randomised trials. LancetLancet,, 354354, 1896^1900., 1896^1900.
Oslin, D., Sayers, S., Ross, J.,Oslin, D., Sayers, S., Ross, J., et alet al (2003)(2003) DiseaseDiseasemanagement for depression and at risk drinking viamanagement for depression and at risk drinking viatelephone in an older population of veterans.telephone in an older population of veterans.Psychosomatic MedicinePsychosomatic Medicine,, 6565, 931^937., 931^937.
Peveler, R.,George,C., Kinmonth, A.,Peveler, R., George,C., Kinmonth, A., et alet al (1999)(1999)Effect of antidepressant drug counselling and informationEffect of antidepressant drug counselling and informationleaflets on adherence to drug treatment in primary care:leaflets on adherence to drug treatment in primary care:randomised controlled trial.randomised controlled trial. BMJBMJ,, 319319, 612^615., 612^615.
Pildal, J., Chan, A.,Hrobjartsson, A.,Pildal, J., Chan, A.,Hrobjartsson, A., et alet al (2005)(2005)Comparisons of descriptions of allocation concealment inComparisons of descriptions of allocation concealment intrial protocols and published reports: cohort study.trial protocols and published reports: cohort study. BMJBMJ,,330330, 1049., 1049.
Pyne, J., Smith, J., Fortney, J.,Pyne, J., Smith, J., Fortney, J., et alet al (2003)(2003) Cost-Cost-effectiveness of a primary care intervention foreffectiveness of a primary care intervention fordepressed females.depressed females. Journal of Affective DisordersJournal of Affective Disorders,, 7474,,23^32.23^32.
Rickles, N. (2003)Rickles, N. (2003) A Randomized Controlled StudyA Randomized Controlled StudyEvaluating the Impact of an Antidepressant MonitoringEvaluating the Impact of an Antidepressant Monitoring
Program on Consumer OutcomesProgram on Consumer Outcomes. PhDThesis,University. PhDThesis,Universityof Wisconsin,Madison.of Wisconsin,Madison.
Rost, K.,Nutting, P., Smith, J.,Rost, K.,Nutting, P., Smith, J., et alet al (2000)(2000) DesigningDesigningand implementing a primary care intervention trial toand implementing a primary care intervention trial toimprove the quality and outcome of care for majorimprove the quality and outcome of care for majordepression.depression.General Hospital PsychiatryGeneral Hospital Psychiatry,, 2222, 66^77., 66^77.
Rost, K.,Nutting, P., Smith, J.,Rost, K.,Nutting, P., Smith, J., et alet al (2001)(2001) ImprovingImprovingdepression outcomes in community primary caredepression outcomes in community primary carepractice: a randomized trial of the QuEST intervention.practice: a randomized trial of the QuEST intervention.Journal of General Internal MedicineJournal of General Internal Medicine,, 1616, 143^149., 143^149.
Schoenbaum, M.,Unutzer, J., Sherbourne,C.,Schoenbaum, M.,Unutzer, J., Sherbourne,C., et alet al(2001)(2001) Cost-effectiveness of practice-initiated qualityCost-effectiveness of practice-initiated qualityimprovement for depression: results of a randomizedimprovement for depression: results of a randomizedcontrolled trial.controlled trial. JAMAJAMA,, 286286, 1325^1330., 1325^1330.
Schulz, K. & Grimes, D. (2002)Schulz, K. & Grimes, D. (2002) AllocationAllocationconcealment in randomised trials: defending againstconcealment in randomised trials: defending againstdeciphering.deciphering. LancetLancet,, 359359, 614^618., 614^618.
Sherbourne,C.,Wells, K., Duan,N.,Sherbourne,C.,Wells, K., Duan, N., et alet al (2001)(2001)Long-term effectiveness of disseminating qualityLong-term effectiveness of disseminating qualityimprovement for depression in primary care.improvement for depression in primary care. Archives ofArchives ofGeneral PsychiatryGeneral Psychiatry,, 5858, 696^703., 696^703.
Simon,G. & Von Korff, M. (1995)Simon,G. & Von Korff, M. (1995) Recognition,Recognition,management and outcomes of depression in primarymanagement and outcomes of depression in primarycare.care. Archives of Family MedicineArchives of Family Medicine,, 44, 99^105., 99^105.
Simon,G.,Von Korff, M., Rutter,C.,Simon,G.,Von Korff, M., Rutter,C., et alet al (2000)(2000)Randomised trial of monitoring, feedback andRandomised trial of monitoring, feedback andmanagement of care by telephone to improve treatmentmanagement of care by telephone to improve treatmentof depression in primary care.of depression in primary care. BMJBMJ,, 320320, 550^554., 550^554.
Simon,G., Katon,W.,Von Korff, M.,Simon,G., Katon,W.,Von Korff, M., et alet al (2001(2001aa))Cost-effectiveness of a collaborative care program forCost-effectiveness of a collaborative care program forprimary care patients with persistent depression.primary care patients with persistent depression.American Journal of PsychiatryAmerican Journal of Psychiatry,, 158158, 1638^1644., 1638^1644.
Simon,G., Manning,W., Katzelnick, D.,Simon,G., Manning,W., Katzelnick, D., et alet al (2001(2001bb))Cost-effectiveness of systematic depression treatmentCost-effectiveness of systematic depression treatmentfor high utilisers of general medical care.for high utilisers of general medical care. Archives ofArchives ofGeneral PsychiatryGeneral Psychiatry,, 5858, 181^187., 181^187.
Simon,G.,Von Korff, M., Ludman, E.,Simon,G.,Von Korff, M., Ludman, E., et alet al (2002)(2002)Cost-effectiveness of a program to prevent depressionCost-effectiveness of a program to prevent depressionrelapse in primary care.relapse in primary care. Medical CareMedical Care,, 4040, 941^950., 941^950.
Simon,G., Ludman, E.,Tutty, S.,Simon,G., Ludman, E.,Tutty, S., et alet al (2004)(2004)Telephone psychotherapy and telephone careTelephone psychotherapy and telephone caremanagement for primary care patients startingmanagement for primary care patients startingantidepressant treatment: a randomized controlled trial.antidepressant treatment: a randomized controlled trial.JAMAJAMA,, 292292, 935^942., 935^942.
Soares,H., Daniels, S., Kumar, A.,Soares, H., Daniels, S., Kumar, A., et alet al (2004)(2004) BadBadreporting does not mean bad methods for randomisedreporting does not mean bad methods for randomisedtrials: observational study of randomised controlledtrials: observational study of randomised controlledtrials performed by the RadiationTherapy Oncologytrials performed by the RadiationTherapy OncologyGroup.Group. BMJBMJ,, 328328, 22^25., 22^25.
Sutton, A., Abrams, K., Jones, D.,Sutton, A., Abrams, K., Jones, D., et alet al (1998)(1998)Systematic reviews of trials and other studies.Systematic reviews of trials and other studies. HealthHealthTechnology AssessmentTechnology Assessment,, 22, 1^276., 1^276.
Swindle, R., Rao, J., Helmy, A.,Swindle, R., Rao, J., Helmy, A., et alet al (2003)(2003)Integrating clinical nurse specialists into the treatment ofIntegrating clinical nurse specialists into the treatment ofprimary care patients with depression.primary care patients with depression. InternationalInternationalJournal of Psychiatry in MedicineJournal of Psychiatry in Medicine,, 3333, 17^37., 17^37.
Tabachnick, B. & Fidell, L. (2001)Tabachnick, B. & Fidell, L. (2001) Using MultivariateUsing MultivariateStatisticsStatistics. Boston: Allyn & Bacon..Boston: Allyn & Bacon.
Thompson, S. & Higgins, J. (2002)Thompson, S. & Higgins, J. (2002) How should meta-How should meta-regression analyses be undertaken and interpreted?regression analyses be undertaken and interpreted?Statistics in MedicineStatistics in Medicine,, 2121, 1559^1573., 1559^1573.
Unutzer, J., Katon,W.,Williams, J.,Unutzer, J., Katon,W.,Williams, J., et alet al (2001(2001aa))Improving primary care for depression in late life: theImproving primary care for depression in late life: thedesign of a multicenter randomized trial.design of a multicenter randomized trial. Medical CareMedical Care,,3939, 785^799., 785^799.
Unutzer, J., Rubenstein, L., Katon,W.,Unutzer, J., Rubenstein, L., Katon,W., et alet al (2001(2001bb))Two-year effects of quality improvement programs onTwo-year effects of quality improvement programs onmedication management for depression.medication management for depression. Archives ofArchives ofGeneral PsychiatryGeneral Psychiatry,, 5858, 935^942., 935^942.
Unutzer, J., Katon,W.,Callahan,C.,Unutzer, J., Katon,W.,Callahan,C., et alet al (2003)(2003)Collaborative care management of late-life depression inCollaborative care management of late-life depression inthe primary care setting: a randomized controlled trial.the primary care setting: a randomized controlled trial.JAMAJAMA,, 288288, 2836^2845., 2836^2845.
Vergouwen, A., Bakker, A., Burger,H.,Vergouwen, A., Bakker, A., Burger,H., et alet al (2005)(2005)A cluster randomized trial comparing two interventionsA cluster randomized trial comparing two interventionsto improve treatment of major depression in primaryto improve treatment of major depression in primarycare.care. Psychological MedicinePsychological Medicine,, 3535, 25^35., 25^35.
Von Korff, M. & Goldberg, D. (2001)Von Korff, M. & Goldberg, D. (2001) ImprovingImprovingoutcomes in depression.outcomes in depression. BMJBMJ,, 323323, 948^949., 948^949.
Von Korff, M, Katon,W., Bush,T.,Von Korff, M, Katon,W., Bush,T., et alet al (1998)(1998)Treatment costs, cost offset, and cost effectiveness ofTreatment costs, cost offset, and cost effectiveness ofcollaborative management of depression.collaborative management of depression. PsychosomaticPsychosomaticMedicineMedicine,, 6060, 143^149., 143^149.
Weaver,T.,Tyrer, P., Ritchie, J.,Weaver,T.,Tyrer, P., Ritchie, J., et alet al (2003)(2003) AssessingAssessingthe value of assertive outreach: qualitative study ofthe value of assertive outreach: qualitative study ofprocess and outcome generation in the UK700 trial.process and outcome generation in the UK700 trial.British Journal of PsychiatryBritish Journal of Psychiatry,, 183183, 437^445., 437^445.
Weingarten, S., Henning, J., Badamgarav, E.,Weingarten, S.,Henning, J., Badamgarav, E., et alet al(2002)(2002) Interventions used in disease managementInterventions used in disease managementprogrammes for patients with chronic illnesses ^ whichprogrammes for patients with chronic illnesses ^ whichones work? Meta-analysis of published reports.ones work? Meta-analysis of published reports. BMJBMJ,,325325, 925., 925.
Wells, K., Sherbourne,C., Schoenbaum, M.,Wells, K., Sherbourne,C., Schoenbaum, M., et alet al(2000)(2000) Impact of disseminating quality improvementImpact of disseminating quality improvementprograms for depression in managed primary care: aprograms for depression in managed primary care: arandomized controlled trial.randomized controlled trial. JAMAJAMA,, 283283, 212^220., 212^220.
Wells, K., Sherbourne,C., Schoenbaum, M.,Wells, K., Sherbourne,C., Schoenbaum, M., et alet al(2004)(2004) Five year impact of quality improvement forFive year impact of quality improvement fordepression: results of a group-level randomizeddepression: results of a group-level randomizedcontrolled trial.controlled trial. Archives of General PsychiatryArchives of General Psychiatry,, 6161,,378^386.378^386.
Whitty, P. & Gilbody, S. (2005)Whitty, P. & Gilbody, S. (2005) NICE, but will theyNICE, but will theyhelp people with depression? The new Nationalhelp people with depression? The new NationalInstitute for Clinical Excellence depression guidelines.Institute for Clinical Excellence depression guidelines.British Journal of PsychiatryBritish Journal of Psychiatry,, 186186, 177^178., 177^178.
Whooley, M., Stone, B. & Soghikian, K. (2000)Whooley, M., Stone, B. & Soghikian, K. (2000)Randomized trial of case-finding for depression inRandomized trial of case-finding for depression inelderly primary care patients.elderly primary care patients. Journal of General InternalJournal of General InternalMedicineMedicine,, 1515, 293^300., 293^300.
Wilkinson,G., Allen, P., Marshall, E.,Wilkinson,G., Allen, P., Marshall, E., et alet al (1993)(1993) TheTherole of the practice nurse in the management ofrole of the practice nurse in the management ofdepression in general practice: treatment adherence todepression in general practice: treatment adherence toantidepressant medication.antidepressant medication. Psychological MedicinePsychological Medicine,, 2323,,229^237.229^237.
4 934 93
PETER BOWER, PhD,National Primary Care Research and Development Centre,University of Manchester;PETER BOWER, PhD,National Primary Care Research and Development Centre,University of Manchester;SIMONGILBODY,DPhil, MRCPsych,DAVID RICHARDS, PhD,Department of Health Sciences,University ofSIMONGILBODY,DPhil, MRCPsych,DAVID RICHARDS, PhD,Department of Health Sciences,University ofYork; JANINE FLETCHER,MRes,Department of Nursing,Midwifery and HealthVisiting,University ofYork; JANINE FLETCHER,MRes,Department of Nursing,Midwifery and HealthVisiting,University ofManchester; ALEX SUTTON, PhD,Department of Health Sciences,University of Leicester,UKManchester; ALEX SUTTON, PhD,Department of Health Sciences,University of Leicester,UK
Correspondence:Dr Peter Bower,National Primary Care Research and Development Centre,Correspondence:Dr Peter Bower,National Primary Care Research and Development Centre,University of Manchester,Manchester M13 9PL,UK. Email: peter.bowerUniversity of Manchester,Manchester M13 9PL,UK.Email: peter.bower@@manchester.ac.ukmanchester.ac.uk
(First received 28 February 2006, final revision 10 May 2006, accepted 2 June 2006)(First received 28 February 2006, final revision 10 May 2006, accepted 2 June 2006)





























