Embed Size (px)
Citation preview

Cocoon Formation in Patients With MidgutNeuroendocrine Tumors
A Rare and Unrecognized Final Pathway
Yi-Zarn Wang, DDS, MD, Heather King, MD, and Anne Diebold, BS
Objectives: Neuroendocrine tumors (NETs) are relatively rare withan indolent nature. As a result, treatment is often delayed and passive.The most commonly recognized disease progression leading to death isfrom the sequelae of bowel obstruction, ischemia, or liver failure sec-ondary to liver metastasis. We recently recognized a rare cocoon-likeformation in patients with metastatic gastroenteropancreatic NETs andhypothesize that this may be a distinct, final pathway for these patients.Methods: Ten patients with stage IV gastroenteropancreatic NETs,seen at our center between October 2008 and November 2011, whodeveloped a cocoon were identified. Patient’s charts, operative reports,pathology, and tumor markers were reviewed.Results: No discernable predictors were identified as precursors tothis condition. One patient survived 13 months after cocoon diagnosis,and the remaining 9 patients were all deceased within 5 months. Surgicaltreatment was attempted in 6 patients and was only partially successfulin 1 patient who had the earliest stage of cocoon formation (type 1).Conclusions: Cocoon-like formations in patients with stage IVgastroenteropancreatic NETs is rare and may be a terminal diseaseprogression that has not been previously recognized. The best treatmentoption remains unknown. Surgical treatment is not advisable, with theexception of type 1 abdominal cocoons.
Key Words: neuroendocrine tumor (NET), midgut, peritonitis
(Pancreas 2013;42: 944Y948)
An abdominal cocoon is a rare and generally benign condi-tion that leads to bowel obstruction. It is usually easily
treatable with a complete surgical excision of the encasingmembrane overlying the intestine and any other involved or-gans. Patients with this condition usually recover well aftersurgical intervention without risk of disease recurrence or anyother long-term sequelae.1
Foo et al2 first recognized the cocoon formation as a dis-ease process commonly affecting young adolescent girls intropical regions. The cause was hypothesized to stem fromretroperitoneal retrograde menstruation leading to inflamma-tory changes with subsequent fibrosis.2 Although the true eti-ology of the cocoon remains unclear, some recent descriptionshave attempted to classify the cocoon formation into primaryversus secondary etiologies. Primary causes include tuberculo-sis, endometriosis, gastrointestinal malignancy, and transplants.3,4
Secondary causes include prolonged peritoneal dialysis, practolol
use, and ventriculoperitoneal shunts.5 However, the distinctionof primary versus secondary cocoons has no merit in terms ofpatient care or management, and therefore, this terminology isnot widely accepted.
Most commonly, abdominal cocoons are classified as oneof 3 subtypes based on the degree of intestinal or organ encase-ment. Type 1 is segmental or partial bowel encasement, type 2implies encasement of the entire length of the small intestine,and type 3 includes entrapment of other organs in addition tothe small intestine.1 In addition, there is an ongoing debate inthe definition of an advanced and extensive encasing sheathformation, which has been named idiopathic encapsulatingperitoneal sclerosis.6 To resolve the dispute and confusion, wepropose to designate this advanced and extensive form of fibroticsheath formation as a type 4 abdominal cocoon, indicating theinvolvement of the entire abdominal peritoneal lining.
Neuroendocrine tumors (NETs) are rare with an estimatedincidence of 1 to 4.6 per 100,000 persons, most of which originatein the midgut.7 Most often, patients with midgut NETs have along history of vague abdominal symptoms with a substantialdelay before their eventual pathologic diagnosis. This diseaseis commonly associated with regional lymph node metastasisand distant metastasis to the liver and/or bone at the time ofdiagnosis.8
Midgut NETs are usually small with a characteristic fi-brotic and desmoplastic reaction of the surrounding tissues.Strangulation of the bowel because of mesenteric vessel encase-ment is not an uncommon intraoperative finding and massivereplacement of normal liver parenchyma by metastatic tumorscan eventually lead to liver failure and death.9
The fibrotic encasement of entire loops of bowel or thewhole abdominal peritoneum as a single cocoon-like forma-tion, to our knowledge, has not been previously described in aNET patient.
We have recently recognized this rare ‘‘cocoon’’ formationin patients with stage IV gastroenteropancreatic NETs and hy-pothesize that this may be a distinct final pathway for patientswith metastatic NETs patient .
MATERIALS AND METHODSAbdominal cocoon-like formations were identified in 10
of 489 patients with pathologically confirmed, metastatic(stage IV) gastroenteropancreatic NETs (lung and unknownprimaries excluded). All patients were seen in our NET clinicbetween October 1, 2008 (first cocoon-like identification), andNovember 1, 2011 (most recent cocoon-like identification).Patients’ clinical courses, laboratory results, pathologic infor-mation, and tumor markers were reviewed. An effort was madeto identify any existing predictors or preconditions that mightresult in a ‘‘cocoon’’ formation (chemoresistance assays, bio-markers, comorbid conditions, previous surgeries/therapies).We reviewed our operative experiences in the 6 (6/10) patientswho were operated on. In addition, a review of the literature
ORIGINAL ARTICLE
944 www.pancreasjournal.com Pancreas & Volume 42, Number 6, August 2013
From the Department of Surgery, Louisiana State University Health SciencesCenter, New Orleans, LA.Received for publication July 11, 2012; accepted November 26, 2012.Reprints: Yi-Zarn Wang DDS, MD, Department of Surgery, Louisiana State
University Health Sciences Center, Rm 747, 1542 Tulane Ave,New Orleans, LA 70112 (e-mail: [email protected]).
Financial support: none.The authors declare no conflicts of interest.Copyright * 2013 by Lippincott Williams & Wilkins
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

TABLE
1.Pa
tient
Dem
ograph
ics
Patient
No.
Sex
Race
Primary
NET
Age
atNET
Diagn
osis,y
Diagn
osis
toCocoo
nDevelop
ment
(mo)
Cocoo
nto
Death
(mo)
Significan
tCom
orbid
Con
ditions
PrimaryPreviou
sly
Resected(Total
No.
Previou
sSurgeries)
Surgeryfor
Cocoo
n?(Typ
eof
Cocoo
n)
Therap
ies
BeforeCocoo
nDevelop
ment
San
dostatin(R
)(O
ctreotide,East
Han
over,NJ)
Therap
y
1M
White
Smallbowel
5549
13Basalcell
carcinom
a;IVCsyndrome
Yes
(3)
Yes
(typ
e1)
Nexavar
(R)(Sorafenib;
OnyxPh
arma&
Bayer
Health
Care,Pittsburgh,PA
);Xeloda(R)(Capecitabine;
Genentech,S
anFrancisco,
Calif)+Temodar(R)
(Tem
ozolam
ide;Merck,
WhitehouseStation,
NJ)
Intolerant
2M
White
Smallbowel
4330
2Non
eYes
(2)
Yes
(typ
e2)
Afinitor(R)(Everolim
us,
RAD00
1;Novartis,
EastHanover,NJ)
40mg/2wk;
rescue
shots
asneeded
3F
White
Smallbowel
6111
33
Non
eYes
(2)
Yes
(typ
e2)
WeeklyPEG
interferon
30mg/mo
4M
African
American
Pancreas
4678
1Carcino
matosis
Yes
(2)
Yes
(typ
e4)
MIBG
therapy(�
2);
Xelod
a60
mg/mo
5F
White
Smallbowel
(atypical)
5738
5Carcino
matosis
Yes
(4)
Yes
(typ
e4)
Non
e30
mg/mo
6F
White
Smallbowel
5712
53
IVCsynd
rome/
thrombo
sis
Yes
(3)
Yes
(aborted;
type
4)Non
e30
mg/mo
7F
White
Smallbowel
4714
24
Invasive
ductal
carcinom
aYes
(4)
No
Xelodawith
concurrent
radiationtherapy
(�3wk);Y-90
microspheres(�
2)
Sub
cutaneou
s2.40
mg
pump/24
h
8F
White
Rectum
4283
4Basal
cell
carcinom
a;lip
oma
Yes
(3)
No
Radiatio
n(�
15);Y-90
microspheres(�
2);
PRRT(�
2)
Non
e
9M
White
Smallbowel
5620
2Non
eYes
(2)
No
Y-90
microspheres(�
2);
Etoposide
+Carboplatin;
Afinitor
30mg/mo
10F
White
Smallbowel
7044
1Carcino
matosis
Yes
(2)
No
Y-90
microspheres(�
2)30
mg/mo
Findicatesfemale;
IVC,inferior
vena
cava;M,m
ale;
MIBG,M
eta-Iodo-Benzyl-Guanidine;PEG,p
ercutaneousendoscopicgastrostom
y;PRRT,
peptidereceptor
radion
ucleotidetherapy.
Pancreas & Volume 42, Number 6, August 2013 Cocoon Formation in Patients With Midgut NET
* 2013 Lippincott Williams & Wilkins www.pancreasjournal.com 945
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

was conducted to compare and contrast the different clinicalimplications of this cocoon-like formation in patients withgastroenteropancreatic NETs versus those with other etiologies.
RESULTSAbdominal cocoon-like formations were identified in 10
(2%) of 489 patients with NETs. The charts of these 10 patientswere reviewed. There were 6 women and 4 men; 9 Caucasian’sand 1 African American. The mean age at time of NET diag-nosis was 53 years with a range from 42 to 70 years. The meantime between the diagnosis of a NET and the cocoon formationwas 72.2months. Themean time between the diagnosis of cocoonand death was 3.8 months, with a single outlier of 13 months(Table 1).
The 4 different tumor markers we routinely obtain for pa-tients with NETs [urinary 5-hydroxyindoleacetic acid (5-HIAA),chromogranin A, pancreastatin, and neurokinin A] were reviewedto determine if the levels at the time of their carcinoid diagnosisand their ‘‘cocoon’’ formation were different. There was widevariability in the marker levels between patients, with no reliableindicator that could be used as a predictor of disease progres-sion toward ‘‘cocoon’’ formation. The only noted trend was anonparallel increase in chromogranin A and pancreastatin levels.
Of the 10 patients, 6 underwent surgical intervention.Only 1 patient benefited from surgery, and only for a periodof 5 months. The last surgical patient was diagnosed at explo-ration upon entering the abdomen, and the procedure wasaborted (patient 7). Of the 10 patients, 8 had small bowel pri-maries, 1 had a rectal primary, and 1 had a pancreatic primary.All pathology was consistent with the diagnosis of a NET. Onesmall bowel primary had atypical features on final pathology(patient 5), and the 1 pancreatic islet cell patient presented withcarcinomatosis clinically (patient 4). Chemoresistance assays ofthe surgically removed tumors are routinely conducted in ourpatients. The initial primary tumors of all 10 patients showed avariable resistance profile to different chemotherapeutic agentswith no discernable trend.
Six patients were explored for recurrent or persistent bowelobstruction and ischemic symptoms. Only 1 patient was defin-itively diagnosed with a cocoon-like formation preoperatively(patient 3), although in 3 patients, high clinical suspicion wasraised prior to their surgical explorations (patients 4, 5, 6). Thefinal 4 patients were diagnosed clinically, and no surgical in-tervention was offered.
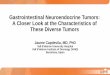
The first operative patient was surgically explored forpersistent bowel obstruction and inferior vena cava syndrome.At surgery, a fibrotic sheath encasing the terminal ileum andright colon was identified, which was treated with segmental enbloc resection as a recurrent tumor mass (Fig. 1). The diagnosisas a type 1 ‘‘cocoon’’ was established retrospectively after thefinal pathology report became available. An isolated area ofretroperitoneal fibrotic membrane encasement of cava wasalso noted intraoperatively, which was incised to release thecava compression. The final pathology revealed nonmalignantcells within the fibrotic membrane sheath but an abundanceof fibroblasts. Patient 1’s symptoms improved for approxi-mately 5 months but then rapidly deteriorated. The patient died13 months after surgery.
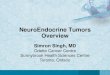
The second operative patient had a type 2 cocoon with aclassic preoperative computed tomographic (CT) finding (recog-nized postoperatively; Fig. 2). Upon exploration, the entire smallbowel was noted to be encased within a sac that moved as a singleunit. There were also extensive carcinoid deposits throughoutthe entire abdomen. Attempts at releasing the fibrotic sheathfrom the underlying bowel failed because of its incredibly ad-herent nature. Patient 2 died 2 months postoperatively.
The third operative patient was diagnosed preoperatively bya palpable mass and a classic CT finding (Fig. 3). As in patient 2,at exploration, a type 2 cocoon that freely moved as a single unitwas identified (Fig. 4). Attempts to peel or incise the sheath wereeventually aborted. Postoperatively, the patient developed a mul-tiple enterocutaneous fistula from the attempted resection sites,which persisted until death, 3 months postoperatively.
The fourth operative patient was explored for a persis-tent partial bowel obstruction with a preoperative suspicion ofcocoon. After 3 recurrent admissions for small bowel obstruc-tions in 5 weeks, we undertook a surgical exploration. A cocooncompletely encasing all abdominal contents (type 4) was identi-fied, and attempts to free the bowel were quickly aborted basedon our previous experience. The patient’s postoperative coursewas complicated with acute renal failure and aspiration pneumo-nia, eventually resulting in death during the postoperative periodof the same admission.
FIGURE 1. Postoperative image of a resected cocoon frompatient 1.
FIGURE 2. Computed tomographic scan image from patient 2depicting the small bowel contained in a ‘‘second abdomen.’’
Wang et al Pancreas & Volume 42, Number 6, August 2013
946 www.pancreasjournal.com * 2013 Lippincott Williams & Wilkins
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

The fifth operative patient was explored for a bowel ob-struction with a preoperative CT scan suggestive of type 4cocoon. Minimal freeing of the mesenteric vessels was under-taken. The patient experienced a transient improvement insymptoms but, nevertheless, died within 5 months.
The sixth operative patient was suspected of having atype 4 cocoon based on recurrent and persistent bowel ob-structions and the gradual development of inferior vena cavasyndrome. Initially, the patient was not offered the option forsurgical intervention. However, with a nondiagnostic pre-operative CT and persistent requests from the patient, an ex-ploration was undertaken. A type 4 cocoon was immediatelydiagnosed upon entering the abdomen, and the surgery wasthen aborted. The patient was discharged to hospice care andexpired within 3 months of the diagnosis.
The other 4 patients in this series were diagnosed by ra-diographic images and symptomatology alone (clinical pre-sentation of recurrent small bowel obstructions). No surgicalintervention was offered. All 4 of these patients were treatedwith decompressive percutaneous endoscopic gastrostomy tubeplacement and discharged to hospice care. Patients 7 and 8 eachdied 4 months after their ‘‘cocoon’’ diagnosis, patient 9 died2 months after the diagnosis, and patient 10 died within 1 monthof the diagnosis during the same hospital admission (Fig. 5).
DISCUSSIONAn abdominal cocoon is an unusual etiology for small
bowel obstruction, and patients may present with chronic oracute obstructions. The cocoon itself is a dense fibrous sheathencasing segments or loops of the bowel, the entirety of theintestines, or with more advanced disease, it can progress toencase other intra-abdominal organs. This condition was firstobserved by Owtschinnikow in 1907 who named it peritonitischronica fibrosa incapsulata.10 The term sclerosing encapsu-lating peritonitis was coined by Foo et al2 in 1978. The termidiopathic encapsulating peritoneal sclerosis has also beenused to describe a thickened parietal peritoneum that encasesthe entire peritoneal cavity, although these authors questionedwhether this finding was a true abdominal cocoon.1,11
The cocoon is a rare disease process, with only a few smallseries ever reported in the literature.1,2,6,11 Most patients with anabdominal cocoon present with acute or more commonly, re-current relapsing chronic bowel obstructions.1,3,6,11 Consistentwith our experience, preoperative diagnosis is usually difficult.Different imaging modalities have had some success. Barium orcontrast studies with small bowel follow-through show a charac-teristic ‘‘cauliflower sign’’ (Fig. 5) and slow transit through theaffected area.6,12,13 Computed tomographic scans may reveal thatthe small intestines are contained in a thickened sac or sheathmimicking a second abdomen (Fig. 2) or thickening of the peri-toneal lining in some patients (Fig. 3).1,6,12,14 An indurated andfirm abdominal wall, asymmetrical distension of the abdomen,and occasionally, a mass that can be palpated on physical exam-ination, should raise suspicion of a cocoon.15 Recurrent and/orpersistent bowel obstruction, especially with a concurrent pro-gressive worsening of an inferior vena cava syndrome, is highlysuggestive of a type 4 cocoon. Nevertheless, even with an exten-sive workup, a definitive diagnosis is usually made at the time oflaparotomy and is therefore indicated in patients presenting withmultiple small bowel obstructions.
For the general surgical patient, an abdominal cocoon isbenign in nature. The treatment is simply a complete excisionof the membrane to release the trapped bowel and any other
FIGURE 3. Computed tomographic scan image from patient 3depicting a thickened peritoneal lining.
FIGURE 4. Intraoperative image of an unresectable cocoon frompatient 3.
FIGURE 5. Contrast study of patient 10 demonstrating theclassic cocoon ‘‘cauliflower sign.’’
Pancreas & Volume 42, Number 6, August 2013 Cocoon Formation in Patients With Midgut NET
* 2013 Lippincott Williams & Wilkins www.pancreasjournal.com 947
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

involved organs. This membrane is a dense and fibrotic sheathcomposed of fibroblasts and collagen.1,6,8,12 Most case reportsdescribe complete resolution of symptoms with release of theobstruction via excision of the sheath. Patients typically re-cover well without complications or recurrent disease.
In this series, we reported on this rare condition affecting ap-proximately 2% of patients with stage IV gastroenteropancreaticNETs. To our knowledge, this condition has never been recognizedas a terminal pathway for patients with gastroenteropancreaticNETs. A characteristic feature of NETs is the development offibrosis, which occurs as a result of the production of bioactiveagents. However, the mechanism of fibrosis remains largelyunknown. Extensive fibrosis of the mesentery can lead tobowel obstructions, mesenteric ischemia, and intestinal perfo-rations. At a very advanced stage, fibrosis can result in an ab-dominal cocoon for which there is currently no viable treatmentoption.16 Unfortunately, there are no reliable predictors that canalert the treating physician of this lethal disease progression.Even with a careful review of preoperative imaging, a thoroughhistory and physical examination, in our experience, the di-agnosis was made only at the time of surgical exploration andwas followed shortly thereafter by death.
In contrast to the excellent prognosis for abdominal co-coon patients without NETs, treatment options for NET patientswith a ‘‘cocoon’’ are extremely limited. In our series, the only‘‘successful’’ treatment was a complete excision of the encap-sulated bowel in a patient with a type 1 cocoon. However, thispatient only survived for 13 months after the ‘‘cocoon’’ di-agnosis. An attempt to peel or remove the fibrotic sheath isextremely difficult and can lead to enterotomies and fistula for-mations. Medical treatment to inhibit the overwhelming fibro-blastic activity and the tenacious collagen formation seems to bethe only viable option for these patients.17 Because the funda-mental pathology of this condition is thickening and encasementof the intra-abdominal organs, a multivisceral organ transplantmay be the optimal resolution for patients without any evidence ofcoexisting extraperitoneal disease.18
CONCLUSIONSAn abdominal ‘‘cocoon’’ in patients with stage IV
gastroenteropancreatic NETs has not been previously reportedand may be a rare and unrecognized final pathway for thesepatients. There are no useful tumor markers to predict its for-mation, and surgical intervention can only provide short-termrelief during the cocoon’s earliest stage of development. Withan advanced cocoon formation, routine decompressive surgicalintervention leads to complications that may hasten the patient’sdemise and, thus, should be avoided. Multivisceral organtransplant may be an option for these patients. However, further
studies are needed to determine any factors that may predisposea NET patient to develop a ‘‘cocoon’’ and to determine the besttreatment options for these patients.
REFERENCES
1. Wei B, Wei HB, Guo WP, et al. Diagnosis and treatment of abdominalcocoon: a report of 24 cases. Am J Surg. 2009;198:348Y353.
2. Foo KT, Ng KC, Rauff A, et al. Unusual small intestinal obstruction inadolescent girls: the abdominal cocoon. Br J Surg. 1978;65:427Y430.
3. Kaushik R, Punia RP, Mohan H, et al. Tuberculous abdominalcocoonVa report of 6 cases and review of the literature. World J Emerg
Surg. 2006;1:18.4. Santos VM, Barbosa ER Jr, Lima SH, et al. Abdominal cocoon
associated with endometriosis. Singapore Med J. 2007;48:e240Ye242.5. Alscher DM, Reimold F. New facts about encapsulating peritoneal
sclerosis as a sequel of long-term peritoneal dialysisVwhat can we do?Minerva Urol Nefrol. 2007;59:269Y279. Review.
6. Xu P, Chen LH, Li YM. Idiopathic sclerosing encapsulating peritonitis(or abdominal cocoon): a report of 5 cases. World J Gastroenterol.2007;13:3649Y3651.
7. Modlin IM, Sandor A. An analysis of 8305 cases of carcinoid tumors.Cancer. 1997;79:813Y829.
8. Modlin IM, Champaneria MC, Chan AKC, et al. A three-decadeanalysis of 3,911 small intestinal neuroendocrine tumors: the rapid paceof no progress. Am J Gastroenterol. 2007;102:1464Y1473.
9. Wang YZ, Joseph S, Lindholm E, et al. Lymphatic mapping helps todefine resection margins for midgut carcinoids. Surgery.2009;146:993Y997.
10. Owtschinnikow PJ. Peritonitis chronic fibrosa incapsulata. Arch Klin
Chir. 1907;83:623Y624.11. Devay AO, Gomceli I, Korukluoglu B, et al. An unusual and difficult
diagnosis of intestinal obstruction: the abdominal cocoon. Case reportand review of the literature. World J Emerg Surg. 2008;3:36.
12. Mohanty D, Jain BK, Agrawal J, et al. Abdominal cocoon: clinicalpresentation, diagnosis, and management. J Gastrointest Surg.2009;13:1160Y1162.
13. Raju GS. Abdominal cocoon due to primary peritonitis: barium mealis valuable in diagnosis. Trop Gastroenterol. 2004;25:80Y81.
14. Gupta S, Shirahatti RG, Anand J. CT findings of an abdominal cocoon.AJR Am J Roentgenol. 2004;183:1658Y1660.
15. Narasynsingh V, Maharaj D, Singh M, et al. Peritoneal encapsulation: apreoperative diagnosis is possible. Postgrad Med J. 2001;77:725Y726.
16. Modlin IM, Moss SF, Chung DC, et al. Priorities for Improving theManagement of gastroenteropancreatic neuroendocrine tumors.J Natl Cancer Inst. 2008;100:1282Y1289.
17. Chan JA, Kulke MH. New treatment options for patients with advancedneuroendocrine tumors. Curr Treat Options Oncol. 2011;12:136Y148.
18. Vianna RM, Mangus RS, Tector AJ. Current status of small bowel andmultivisceral transplantation. Adv Surg. 2008;42:129Y150.
Wang et al Pancreas & Volume 42, Number 6, August 2013
948 www.pancreasjournal.com * 2013 Lippincott Williams & Wilkins
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.