Embed Size (px)
DESCRIPTION
Coccidia 10 -11.ppt
Citation preview

TISSUE COCCIDIA
Dr. Devika Iddawela
Department of Parasitology
10/11

ObjectivesTo be able to-
• Name the Tissue coccidia that cause human disease and state the habitats of each • State the source (s) of infection, entry to and exit of agent from humans • Describe the life cycle with stages and events• Identify the stages that cause pathogenic effects• Outline laboratory methods of identification of organism• Identify points in the life cycle where preventive measures are applicable
• Describe the pathogenicity•List the clinical features•Describe transmission, prevention and control of toxoplasmosis

COCCIDIAIntracellular protozoans; alternation of asexual & asexual Development in epithelial cells (usually gut) of the definitive host
TISSUE COCCIDIA
INTESTINAL COCCIDIA-
Tissue coccidia Toxoplasma gondii Sarcocystis spp.

Toxoplasma gondii

Toxoplasma gondii
• Coccidian parasite • Cats ONLY known DEFINITIVE HOST• INTERMEDIATE HOSTS: widespread in birds & mammals

TOXOPLASMOSISWorld wide distribution; most prevalent parasitic infection of humans-• on serological assays, rates vary in communities 4-90%
Sri Lanka > 50% healthy adults have Ab.Many animals (dogs, cats, rodents are positive; cats 24% )

•obligate intracellular parasite of all nucleated cells
• Latent infection is common
• It is an important opportunistic parasite
• Causes fatal infections in the immuno-compromised eg.AIDS

Morphology – There are 3 forms:
1. Tachyzoites (endozoites) and pseudocysts– Crescent shape, 4 – 8 µm with single nucleus
found in macrophages (pseudocyst) or any nucleated cell . Multiply rapidly (tachyzoites) . Pseudocysts can cross the placenta
Characteristic form is crescentic shaped trophozoite

2. Bradyzoites ( cystozoites) and true cysts – can be found in any part of the body Organs commonly affected are brain, eye, heart.Cyst wall is by the parasite and host. Zoites in true cysts multiply slowly (bradyzoites)

3.Oocyst – formed in the small intestine of the cat and passed in cat faeces. Each sporulated oocyst contains 02 sporocysts and each sporocyst has 04 sporozoitesNOT FOUND IN HUMANS and other intermediate hosts

Definitive host
Life cycle
Only known definitive hosts for Toxoplasma gondii are members of family Felidae (domestic cats and their relatives)
Unsporulated oocysts are shed in the cat’s faeces
Oocysts take 2-5 days to sporulate in the environment and become infective.

Toxoplasma in Definitive host–Gut epithelial cells of cat
SCHIZOGONY(asexual multiplication)
GAMETOGONYmale gametocytesfemale gametocytesZygote
SPOROGONY oocystoutside environment- (sporozoites)

Pathogenesis
• Tachyzoites actively invade the cells• Multiply rapidly• Form intracellulaer pseudocyst• This leads to cellular disruption, released tachyzoites infect adjacent cells• As the host immunity develops,Tissue true cyst form, containing bradyzoitesPeriodic excystation can occur

clinical disease
majority asymptomatic except in Neonatesimmunocompromised
eg. Transplant surgery, AIDS

fever, painless cervical lymphadenopathy+ rash
Immunocompromised- organtransplant,AIDS
Severe disease- multiple tissue/organ involvement
Symptomatic toxoplasmosis n normal patients ( immuno-competant)

In Immunodeficient patients- mostly due to reactivationCommon _ central nervous system (CNS) disease – encephalitis
In patients with AIDS, toxoplasmic encephalitis is the most common cause of intracerebral mass lesions
but may have retinochoroiditis, pneumonitis, or other systemic disease.

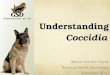
Ocular toxoplasmosis
Most common cause of infectious posterior Uveitis
Due to• periodic reactivation of congenital toxoplasmosis or• acquired acute infection
Clinical features• Floaters• Blurred vision
• Usually unilateral• Active lesion is whitish with ill-define margins ( cotton –wool appearance) and pigmented when quiescent Involves macular in majority

CONGENITAL TOXOPLASMOSISoccurs generally with acute (1ry) infection in Mother –(endometrial reactivation reported))
Placental infection Zoites transmittedto foetus
Risk of infection increases with duration of pregnancy
but foetal damage severe during early pregnancy- abortion, intra uterine death

diagnosis
The diagnosis of toxoplasmosis is typically made by serologic testing.
Indirect
Detection of IgM, IgA or low avidity IgG , rising IgG titreindicate acute infection,IgG – Past infection

Serological tests available1.Sabin-Felman dye test – Gold standard2.IFAT3. IHA4. ELISA

•Use live tachyzoites
• live tachyzoites stain blue with alkaline methylene blue dye
• If antibodies to T gondii are present in the patient's serum, they will damage the organisms
• damaged organisms will not take up the dye and appear as pale "ghosts" compared to undamaged organisms.
• The test needs live tachyzoites and is difficult to perform, so other serological tests are typically used. However, the test is very sensitive and specific and remains the reference method.
Sabin-Felman dye test

Serological test for toxoplasmosis: FAT
positive negative

Direct – Demonstration of Parasite
1. Observation of parasites in patient specimens, such as bronchoalveolar lavage material from immunocompromised patients, or lymph node biopsy2. Isolation of parasites from blood or other body fluids, by intraperitoneal inoculation into mice or tissue culture mice should be tested for the presence of Toxoplasma organisms in the peritoneal fluid 6 to 10 days post inoculation;
if no organisms are found – serology 4 -6 weeks post innoculation,

• especially in detecting congenital infections in utero. Amniotic Fluid - parasite DNA by PCRPrenatal diagnosis:•Fetal US - calcifications / hydrocephalus
•Isolation of parasite placenta, amniotic fluid, foetal blood
Detection of parasite genetic material by PCR,

Amniocentesis• Done around 16th week of pregnancy• A long needle is inserted into the Amniotic sac and
amniotic fluid is drawn.

Transmission
Parasitic stages that can be transmitted to humans
• Oocysts
• Tachyzoites or pseudocysts
• Bradyzoites or true cysts

Transmission
a) oocysts via contaminated Vegetables, fruits and water
Food and water borne

• Accidental ingestion of oocysts after cleaning a cat's litter box when the cat has shed Toxoplasma in its faeces
• Accidental ingestion of oocysts after touching or ingesting anything that has come into contact with a cat's faeces that contain Toxoplasma
• Accidental ingestion of oocysts in contaminated soil (e.g. not washing hands after gardening)
• Drinking water contaminated with the Toxoplasma oocysts
Animal-to-human (zoonotic) transmission

true cysts (bradyzoites)• eating uncooked or undercooked meat of infected animal
• Eating food that was contaminated by knives, utensils, cutting boards, or other foods that had contact with raw, contaminated meat
•Organ transplant recipients can become infected by receiving an organ from a Toxoplasma-positive donor.
Rarely
•Accidental ingestion of undercooked, contaminated meat after handling it and not washing hands thoroughly (Toxoplasma cannot be absorbed through intact skin)

Mother-to-foetus (congenital) transmission
• A woman who is newly infected with Toxoplasma during pregnancy can pass the infection to her unborn child (congenital infection).
Tachyzoites or pseudocysts
•Laboratory workers who handle infected blood can also acquire infection through accidental inoculation. • Entering body through abrasions
(butchers, veterinarians),• Blood transfusion

PREVENTION Reduce Risk of Toxoplasmosis from Food
Avoid eating raw/undercooked meat-15 C for 3 days-65 C 4-5 minutes-4 C persists for months
salt/nitrates kills cysts,

•Avoid eating raw/undercooked meats
-
Wash foods such as green salads leaves and fruits, especially if it is to be eaten uncooked.
•Wash cutting boards, dishes, counters, utensils, and hands with hot soapy water after contact with raw meat, poultry, seafood, or unwashed fruits or vegetables.
To reduce risk from food

Reduce Risk of Toxoplasmosis from the Environment
• Wear gloves when gardening and during any contact with soil or sand
•Keep outdoor sandboxes covered.
• Wash hands after contact with soil

•Feed cats only canned or dried commercial food or well-cooked food, not raw or undercooked meats.
•
•Change the litter box daily . •The Toxoplasma parasite does not become infectious until 2 to 5 days after it is shed in a cat's faeces
To reduce environmental contamination

High risk: pregnancy, immunocompromised- •Avoid contact with cats/gardening
• Avoid changing cat litter

• Keep cats indoors.
• Do not adopt or handle stray cats, especially kittens.

SARCOSPORIDIOSIS / SARCOCYSTOSIS
Two types - Intestinal sarcocystosis
Muscle sarcocystosis
Organism - Sarcocystis spp. many species present
coccidian parasite, tissue protozoan
Life cycle - requires two hosts ; a definitive host & an intermediate host
man can be the definitive host for some species and an intermediate host for some other species
In the definitive host - sporogony in intestinal mucosae with the production of sporocysts (infective stage)
In the intermediate host-sarcocysts or Meischer’s tubes in muscle (intermediate stage)

Muscle sarcocystosis
• Man act as the intermediate host
• Definitive host may be a carnivore; monkey, dog
• Sarcocysts are found in muscles andconnective tissues of man
• Sarcocysts vary in size from few µm to 5 mm.
• These contain cystozoites. Similar to Toxoplasma zoites but larger; banana shaped.
Cysts in the muscles can cause myositis and muscle necrosis.

True/ false regarding toxoplasmosis
Cats act as definitive hosts
Oocysts could be found in human faeces
True cysts can be transmitted by blood transfusion
Tachyzoites can be transmitted by mosquito bite
Risk of congenital infection increase with duration of pregnancy
If the mother get infected during the later part of pregnancy, foetal damage is sever
Known to cause life- threatening infections in immuno-compromized patients

Can cause sever disease in pregnancy
Serology is diagnosis of choice
Detection of IgM indicate a past infection
Prenatal diagnosis is usually rely on serology
Washing hands after going to toilet is good method of preventing infection
Oocysts are infective as soon as it pass in the faeces