Embed Size (px)
Citation preview

Closing the Abdomen
Mary Theophilus
Specialists Without BordersSeminar in Surgery
Rwanda, September 2010

www.specialistswithoutborders.org
Outline• Factors influencing type of abdominal closure• Post-operative wound dehiscence• Principles of abdominal closure• Abdominal Compartment Syndrome• Laparostomy = temporary closure• Closure post-laparostomy

www.specialistswithoutborders.org
What type of closure? Factors influencing type of abdominal closure
• Patient factors – diabetes, steroids, obesity, malnutrition etc…
• Operative factors– Risk of wound infection…contamination?– Unable to close abdomen– Weak or frayed fascia
• Planned re-operation(s)?

• Signs– Excessive serous discharge from wound– Palpable defect in fascia– Bowel on view !
• A full thickness wound dehiscence involving bowel requires urgent closure– herniated bowel will develop an overlying layer of
granulation tissue (peritonealised) making future hernia repair impossible.
www.specialistswithoutborders.org
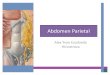
Post-operative Wound Dehiscence

www.specialistswithoutborders.org
Post-operative Wound Dehiscence
Small bowel in the base of the wound has been covered by granulation tissue, making primary closure of the wound impossible. The wound was treated with dressings.
2 weeks post-laparotomy for perforated appendicitis

• No tension !• Single layer closure
– Incorporating fascia and no muscle
• Jenkins’ Rule of 4– 2cm by 2cm
• Continuous vs Interrupted– If high risk of wound infection - use interrupted
www.specialistswithoutborders.org
Principles of Abdominal Closure

www.specialistswithoutborders.org
Tension Sutures

• Back to first principles – NO TENSION• Abdominal Compartment Syndrome
• = Laparostomy with later primary or mesh closure
www.specialistswithoutborders.org
If it will not close!

• Organ dysfunction caused by intraabdominal hypertension
• Normal pressure – 5-7mmHg , Hypertension - >12mmHg
• Respiratory, renal and GI tract impairment• Intravesical pressure measurement• NG tube, empty gut, diuretics• = Laparostomy with later primary or mesh
closure
www.specialistswithoutborders.org
Abdominal Compartment Syndrome

• Protects small bowel from fascial adhesions• Avoids fascial retraction and loss of domain• Allows tissue oedema to settle and the
abdomen to close without tension• Useful if further planned re-operation
www.specialistswithoutborders.org
Laparostomy - Temporary ClosureAdvantages

• Fraying of the fascia (if sutured) compromising subsequent definitive closure
• Long term laparostomy can lead to shortening of the rectus abdominis muscles– Especially in the obese– Makes definitive closure difficult– Relaxation incisions maybe required
www.specialistswithoutborders.org
Laparostomy - Temporary ClosureDisadvantages

• Rapid closure• Protects intra-abdominal organs• Prevents peritoneal contamination• Addresses peritoneal fluid• Allows reoperation with minimal tissue
damage• Allows timely and easy closure with low rate
of ensuing wound complications
www.specialistswithoutborders.org
Good technique

• Bogota bag• Towel clip closure• Zip closure• Mesh (absorbable, non-absorbable,
composite)• Vac dressing
www.specialistswithoutborders.org
Laparostomy Techniques

• Bogota bag
www.specialistswithoutborders.org
Laparostomy Techniques

• Towel clip closure
www.specialistswithoutborders.org
Laparostomy Techniques

• Vac Dressing
www.specialistswithoutborders.org
Laparostomy Techniques

• Suction dressing
www.specialistswithoutborders.org
Laparostomy Techniques

www.specialistswithoutborders.org
• Ideal• May be closed serially• May require other techniques to facilitate :Relaxing incisions in the fascia
Primary closure post laparostomy

www.specialistswithoutborders.org
Component Separation Technique

• Non absorbable• Absorbable• Composite• Bilayer• Organic
www.specialistswithoutborders.org
Mesh closure post Laparostomy

Close skin if possible, else vac dressings, skin
grafting, tissue flaps
www.specialistswithoutborders.org

www.specialistswithoutborders.org
ConclusionsPrimary closure best but only if NO TENSION
Abdominal compartment syndrome should be avoided and treated with laparostomy
Good laparostomy techniques enable early secondary closure and help avoid late wound complications

• Finding the best Abdominal Closure: An evidence based review of the Literature, Ceydeli A, Rucinsk J, Wise L; Current Surgery 2005 vol 62:2, 220-225
• Temporary abdominal closure with the Vacuum pack technique, Ozguc H, Paksoy E,Ozturk E; Acta Chir Belg 2008, 108 (414-419)
www.specialistswithoutborders.org
References

www.specialistswithoutborders.org

Thank You!
www.specialistswithoutborders.org

![0165-0183 – Theophilus Antiochenus – Ad Autolycum ......[I venture to assign to Theophilus a conjectural date of birth, circiter A.D. 115.524] 89 THEOPHILUS TO AUTOLYCUS. Book](https://img.dokumen.tips/doc/110x75/610d2985826db564063a4250/0165-0183-a-theophilus-antiochenus-a-ad-autolycum-i-venture-to-assign.jpg)