Embed Size (px)
Citation preview

Clinical Updates Novel Agents for the Treatment of Metastatic Melanoma
Future Directions: Opportunities for Targeting B-RAF and Other Targets in
Melanoma Management
Keith T. Flaherty, MDAssistant Professor of MedicineAbramson Cancer Center of the
University of PennsylvaniaPhiladelphia, PA

Novel Cytotoxics

Albumin-bound paclitaxel
• Established superiority to conventional paclitaxel in metastatic breast cancer
• Phase II trial in metastatic melanoma
• 35 patients with chemotherapy-naïve metastatic melanoma received ABI-007 100 mg/m2 IV weekly for 3 out of 4 weeks
• Objective response rate 26%
• Median PFS 4 months
• Phase III trial being conducted compared to dacarbazine

Altering the Threshold for Chemotherapy-induced Apoptosis

STA-4783 Induces Programmed Cell Death via
the Intrinsic Mitochondrial Apoptotic Pathway
STA-4783
TARGET
↑ ROSMitochondria
Cytochrome c release
APOPTOSISCaspase 9activation
STA-4783 induces ROS which accumulate in the mitochondria
Cytochrome c activates caspase 9 which then activates caspase 3/7 leading to apoptosis
ROS elevation leads to the oxidation of cardiolipin, a mitochondrial phospholipid which holds cytochrome c in the mitochondria. Oxidation of cardiolipin leads to the release of cytochrome c
Cytochrome c exits the mitochondria through pores which are created by pro-apoptotic members of the Bcl2 family and are dependent upon elevated ROS

STA-4783 in Metastatic MelanomaStudy Design
Coordinating investigator: Steven O’Day, MD, The Angeles Clinic and Research Institute
(81 patients were enrolled from December 2004 to September 2005)
• Double-blind, randomized, controlled; 21 centers in United States
• Treatment: 3 weekly treatments per each 4-week cycle, until PD
• Assessment: at baseline and every other cycle thereafter (RECIST)
• Cross-over for paclitaxel-alone arm after PD
Paclitaxel: 80 mg/m2
+STA-4783 213 mg/m2
(N=53)
Study Population
Stage IV 0-1 prior
Chemo for Metastatic disease
ECOG 0-2 No brain mets
Paclitaxel: 80 mg/m2
(N=28)
Randomization2:1
(N=81)
Primary Endpoint
Progression-freeSurvival
1/week for 3 weeks; 1 week off

Kaplan-Meier Plot of Progression-free Survival
Hazard Ratio= .583
P= 0.035*
* The P-value is from a 2-sided log-rank test.
6 Month PFS
STA-4783 + Paclitaxel
35%
Paclitaxel 15%

Genasense Drug Substance (Oblimersen Sodium, G3139)
• 18-base DNA oligonucleotide
• TCTCCCAGCGTGCGCCAT
• Phosphorothioate backbone
• Selectively targets Bcl-2 RNA
• Decreases Bcl-2 protein
• Other MOAs possible
O BaseO
BaseO
BaseO
OP
S O
-O
OP
-O O
S
OP
S O
-O

GM301 Study Design
• Primary endpoint: overall survival
• Secondary endpoints: response rate, progression free survival
• Sample size: N = 771
• Cycles every 21 days (maximum of 8): no cross-over
• Radiologic assessment every 2 cycles
• Minimum follow-up: 2 years
DTIC 1000 mg/m²
G3139 7 mg/kg/d x 5 days DTIC 1000 mg/m²
Stratification/
Randomization

1.0
0.4
0.2
0.0
0 20 24
0.8
0.6
4 8 12 16
Months
Pro
po
rtio
n S
urv
ivin
g
G+DTIC DTIC
Median (mos) 9.0 7.8
Hazard Ratio 0.87
Logrank p 0.077
Overall Survival (24-Month)Intent-to-treat Population; N=771

0 2 6 10 14 18 20 244 8 12 16 22
1.0
0.4
0.2
0.0
0.8
0.6
Months
Pro
port
ion
Su
rviv
ing
G+DTIC DTIC
Median (mos) 12.3 9.9
Hazard Ratio 0.64
Logrank P 0.0009
Overall SurvivalBaseline LDH < 0.8 x ULN; N=274

AGENDA (GM307) Study Design
• Co-Primary Endpoints: PFS/Overall survival
• Secondary endpoints: overall response rate, durable response rate, duration of response
• Sample size: N = 300
• Cycles every 21 days (maximum of 8): no cross-over
• Radiologic assessment every 42 days
• Minimum follow-up: 2 years
Genasense 7 mg/kg/d CIV x 5 days DTIC 1000 mg/m²
Stratification/
RandomizationMatching PCBO CIV x 5 days DTIC 1000 mg/m²

Signal Transduction & Angiogenesis Inhibitors
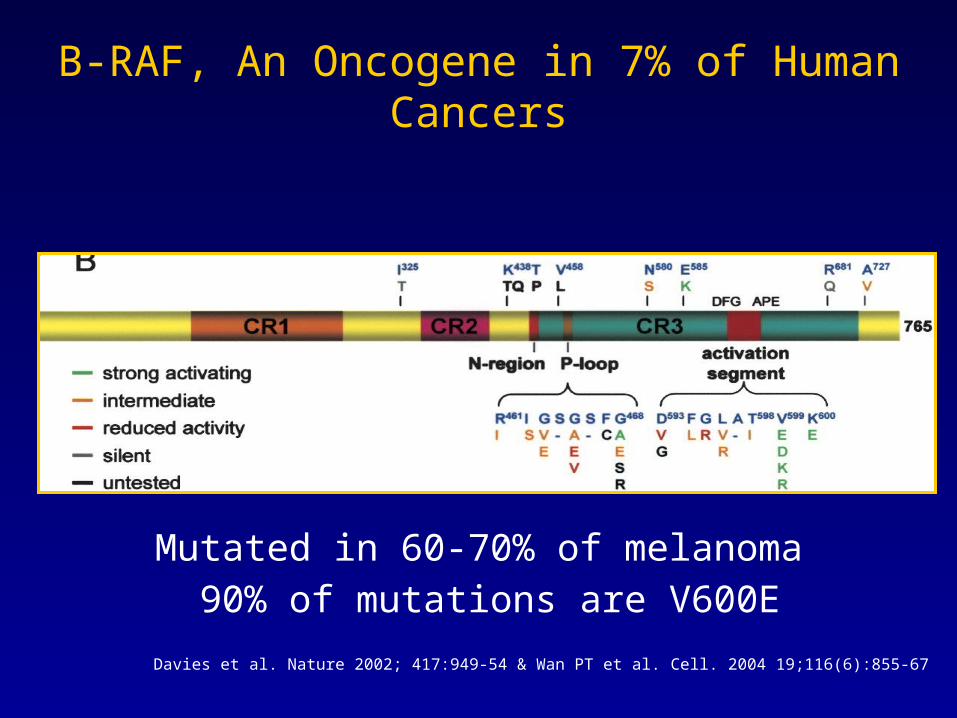
Mutated in 60-70% of melanoma 90% of mutations are V600E
Davies et al. Nature 2002; 417:949-54 & Wan PT et al. Cell. 2004 19;116(6):855-67
B-RAF, An Oncogene in 7% of Human Cancers

Response Rates & B-RAF Mutation Status
combination chemotherapy response rate
Wild type B-RAF 33%
Mutant B-RAF 11%
Chang et al. J Transl Med. 2004 Dec 21;2(1):46.

NRASB-RAF
MEK
ERK
MAP kinase pathway inhibitors in melanoma
PD0325901 ARRY-142886
BAY 43-9006/sorafenib
CHR-265
PLX4032
SB-590885

Sorafenib
Kinase assays IC50
C-Raf 2 nM
mVEGFR2, VEGFR3 6-10 nM
wt B-Raf, V599E B-Raf 20–40 nM
p38, PDGFrβ 28–38 nM
FLT-3, c-KIT 40–80 nM
EGFR, PKC, MEK, ERK Inactive at 10 mM
Wilhelm S et al. Cancer Res. 2004;64:7099-109
NH
NH
OO
N
NH
OCF3
Cl

Sorafenib Spectrum vs. Whole Kinome
Fabian, M.A. et al. Nat Biotechnol, 2005. 23(3):329-36.

Single-agent Sorafenib in Melanoma
• 39 patients with metastatic melanoma
– 1 responder
– 7 patients with stable disease at 12 weeks
• 22 patients with metastatic melanoma
– 1 partial response
– 12 with stable disease
Median progression-free survival: 3 months

Sorafenib with Chemotherapy
Single arm phase II trials
N ORR PFS
Dacarbazine 30 17% 3.6 mo.
Temozolomide 76 24% 6.0 mo.
Carboplatin & paclitaxel 105 26% 8.8 mo.

1ST 2ND
DTIC/temozolomide randomized phase II
Carboplatin/paclitaxel E2603 phase III OS PFS
Line of therapyChemotherapy
backbone
Randomized Trials in Metastatic Melanoma

Eligibility criteria• No prior chemotherapy,
one prior immunotherapy allowed
• Measurable disease by RECIST
• No active brain metastases, screening brain MRI required
Stratified: AJCC stage• Unresectable stage III• Stage IV-M1a, M1b• Stage IV-M1cECOG PS• 0• 1
Group A: DTIC, 1000 mg/m2 IV q3wSorafenib 400 mg po bid
Group B: DTIC, 1000 mg/m2 IV q3wPlacebo 2 tablets po bid
Sorafenib in Melanoma: Randomized Phase II Sorafenib + DTIC Trial Design
Ran
do
miz
atio
n
(N=
98)
• 1° end point: PFS
• 2° end point: OS
• 3° end points: TTP, tumor response rate, duration of response, EQ-5D QoL
Data on file. Bayer HealthCare.

Phase II Dacarbazine ± Sorafenib
1.00
0.75
0.50
0.25
0.000 100 200 300 400 500
Days From Randomization
Pro
gres
sion
-Fre
e S
urvi
val P
roba
bilit
y
600
Hazard Ratio = 0.67; P = 0.068
Sorafenib + DTIC (39 events)Median: 2.7 mo.
Placebo + DTIC (42 events) Median: 4.9 mo.
ORR
24%
12%

Sorafenib in Melanoma: PRISMPhase III Paclitaxel + Carboplatin ± Sorafenib
Agarwala SS, et al. Proc Am Soc Clin Oncol. 2007;25:474s. Abstract 8510.
N=270
Primary endpoint: progression-free survival (by independent assessment)
Secondary and tertiary endpoints: time to progression, objective response rate, duration of response, overall survival
Carboplatin AUC 6 IV Day 1Paclitaxel 225 mg/m2 IV Day 1
Sorafenib 400 mg po bid Days 2-19Cycles repeated every 21 days
Stratified by:
AJCC stage: Unresectable stage III Stage IV – M1a, M1b Stage IV – M1c
ECOG PS: 0 vs 1
Key Eligibility: Progresses on DTIC/TMZ No active brain Metastases Measurable disease by RECIST Carboplatin AUC 6 IV Day 1
Paclitaxel 225 mg/m2 IV Day 1Placebo 2 tablets po bid Days 2-19
Cycles repeated every 21 days
RRAANNDDOOMMIIZZAATTIIOONN
Mandatory dose reduction after cycle 4 to paclitaxel 175 mg/m2 and
carboplatin AUC 5

Phase III Carboplatin/Paclitaxel ± Sorafenib
Hazard Ratio = 0.91; P = 0.492
Sorafenib + C/P (97 events)
Median: 4.0 mo.
Placebo + C/P (100 events)
Median: 4.1 mo.
1.00
0.75
0.50
0.25
0.00
Pro
babi
lity
of P
rogr
essi
on-F
ree
Sur
viva
l
0 14 29 43 57 71
Weeks From Randomization
ORR
11%
10%
Agarwala SS, et al. Proc Am Soc Clin Oncol. 2007;25:474s. Abstract 8510.

Paclitaxel/Carboplatin ± Sorafenib in Advanced Melanoma E2603 Phase III Trial
Arm ACarboplatin AUC 6 IV Day 1Paclitaxel 225 mg/m2 IV Day 1Placebo 2 tablets po bid Days 2-19 Q3WStratified by:
AJCC Stage ECOG PS Prior Therapy
Arm BCarboplatin AUC 6 IV Day 1Paclitaxel 225 mg/m2 IV Day 1Sorafenib 400 mg po bid Days 2-19 Q3W
RRAANNDDOOMMIIZZEE
Carboplatin and paclitaxel with or without sorafenib in treating patients with unresectable stage III or stage IV melanoma.
Available at: www.clinicaltrials.gov/ct/show/NCT0010019?order=1. Accessed September 17, 2007.
800 patients with metastatic melanoma and no prior chemotherapy; primary endpoint - OS

BIM
p27Kip
-actin
pMEK
MEK
RAF265 Sorafenib
Vehicle
10 mg/kg q2d RAF26530 mg/kg q2d RAF265 100 mg/kg q2d RAF265
Mea
n T
um
or
Vo
lum
e (m
m3)(
+/-
SE
)
0
400
800
1200
1600
2000
2400
0 4 8 12 16 20
Days Post Staging
MEXF 276 (B-RafV600E)
RAF265 Causes Tumor Regression in Xenografts of V600E B-RAF Human Melanoma
Tumor Regressions (N=8/group)
PR / CR
1 / 08 / 08 / 0
100 mg/kg qd Sorafenib
0 / 0
0 / 0
Courtesy of Darrin Stuart, Novartis
-
Vehicle
-
Vehicle
-
Vehicle 10 mg/kg 30 mg/kg 100 mg/kg
Vehicle 10 mg/kg 30 mg/kg 100 mg/kg
-
Vehicle 10 mg/kg 30 mg/kg 100 mg/kg
Vehicle 10 mg/kg 30 mg/kg 100 mg/kg

RAF-265-MEL01 Study Design
40-60 B-RAFWT
40-60 B-RAFMUT
• Dose escalate to MTD without regard to B-RAF status using Bayesian methodology
• Assess Safety, PK, PD
• Expand at MTD and stratify based on B-RAF mutation status
• Assess PFS, ORR
Phase I
MTD
Serial biopsies once target drug exposure achieved
Phase II expansion

Selectivity of PLX4032 in vivo
N-RasMUT B-RafMUT
Lee J et al. 2006 NCI/AACR/EORTC

PLX4032 Dose Escalation Study
Dose level 1
Dose level 2
Dose level 3
Dose level 4
Maximum tolerated dose
3-6pts
3-6pts
3-6pts
3-6pts
3-6pts
Target AUC 6 patients with V600E+ melanoma
Serial biopsies
6 patients with V600E+ melanoma

AZD6244 Suppresses the Growth of 1205Lu Melanoma Xenograft (B-RAF mutant)
K Smalley et al, NCI/AACR/EORTC 2006

Lorusso et al. ASCO 2005, abstract 3011
Tumor pERK Suppression in Individual Patients MEK Inhibitor (PD0325901)

Phase II Trials with MEK Inhibitors
• ARRY-142886/AZ6244 (AstraZeneca)
– Randomized phase II: ARRY-142886 vs. temozolomide
– N = 182
– Archival, paraffin-embedded tissue collection
– Sample size allows allows exploration of effect in patients with a B-RAF or N-RAS mutation
• PD0325901 (Pfizer)
– Single-arm phase II

Single-agent Bevacizumab or Bevacizumab/IFN in Melanoma
• Randomized phase II trial:
– bevacizumab 15 mg/kg IV every 2 weeks vs.
– bevacizumab 15 mg/kg IV every 2 weeks + 1 MIU IFNα SQ QD
• 17 patients accrued as of preliminary analysis
– 44% with lymph node/skin metastases (M1a)
• 1 CR, 1 PR both on combination arm, both with M1a disease
• 4 SD > 24 weeks (3 on bevacizumab alone)
• Not published
Carson W et al. ASCO 2003, abstract 2873

Randomized Phase II Trial of Carboplatin/Paclitaxel ± Bevacizumab
RRAANNDDOOM M IIZZEE
Arm A
Carboplatin AUC 5 IV q 21dPaclitaxel 175 mg/m2 IV q21d Placebo
Arm B
Carboplatin AUC 5 IV q21dPaclitaxel 175 mg/m2 IV q21dBevacizumab 15 mg/kg IV q 21d
Stratify:
AJCC stage
ECOG PS
N = 200 patients with previously untreated metastatic melanoma
Primary endpoint = progression-free survival

Current Phase I or II Melanoma Trials with Angiogenesis Inhibitors
• AG-013736 (VEGFR & PDGFR)
– Single arm phase II
• CHR-258 (VEGFR & FGFR)
– Phase I in melanoma
• Sunitinib
– Phase I with temozolomide in melanoma
• Sorafenib/bevacizumab
• Sorafenib/temsirolimus
• Bevacizumab/temsirolimus
NCI/CTEP sponsored phase II

Novel Immunologics

Dendritic Cell/T Cell Activating Therapies in Clinical Development
Dendritic cell T cell
+T cell
receptorMHC
CD28
B7-1 (CD80)
CTLA4
B7-2 (CD86)
-
PD-L1 (B7-H1)
PD-1
-
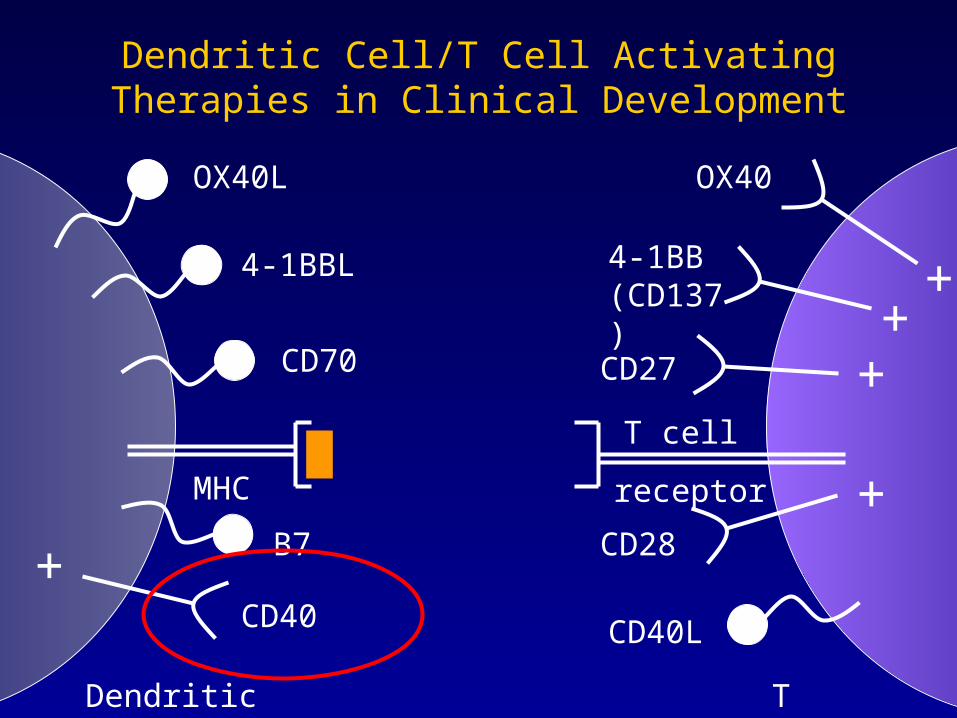
Dendritic Cell/T Cell Activating Therapies in Clinical Development
Dendritic cell T cell
OX40L OX40
4-1BBL 4-1BB (CD137)
CD40LCD40
+
+
CD70 CD27
+
+T cell
receptorMHC
CD28B7
+
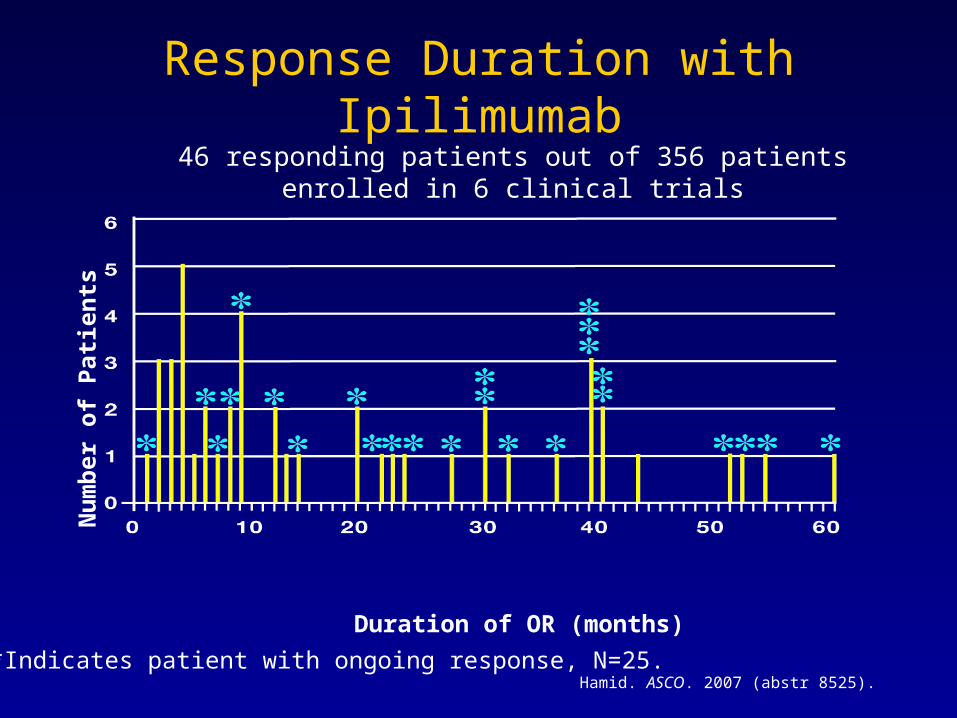
Hamid. ASCO. 2007 (abstr 8525).
46 responding patients out of 356 patientsenrolled in 6 clinical trials
*Indicates patient with ongoing response, N=25.
Duration of OR (months)
Nu
mb
er o
f P
atie
nts
Response Duration with Ipilimumab

Phase I Trial of CP-870,893• 29 patients with advanced solid tumors; 15 with melanoma
evaluated by RECIST
– 4 Partial Responses
– 7 Stable Disease
• All partial responses were in patients with melanoma
– Regression of lesions in liver, skin, lymph nodes, lung, muscle
– All PRs at 0.2 mg/kg or 0.3 mg/kg
• One melanoma patient (0.2 mg/kg) had a near CR for 18 months, then isolated LN recurrence, underwent surgery, now CR for 18 additional months
UPIN 1017 (melanoma)

Future Directions in Melanoma
• Diverse mechanisms currently being explored in melanoma
– Novel cytotoxics, signal transduction inhibitors, anti-angiogenic & novel immunotherapies
• Critical for new therapies to establish which subpopulation derives the greatest benefit




![Case Report A Rare Case of Metastatic Malignant Melanoma ...downloads.hindawi.com/journals/crigm/2014/312902.pdf · metastatic malignant melanoma of the GI tract [ ]. In fact, Wysocki](https://img.dokumen.tips/doc/110x75/5f9b841cf1457c0af634448c/case-report-a-rare-case-of-metastatic-malignant-melanoma-metastatic-malignant.jpg)