Embed Size (px)
DESCRIPTION
Evolving Roles of GLP-1 Receptor Agonists
Citation preview

Clinical Updates in TYPE 2 DIABETESEvolving Roles of GLP-1 Receptor Agonists

Learning Objectives
• Describe the major pathologic deficits underlying T2DM development with a focus on relationships with incretin hormone signaling
• Individualize therapy for patients with T2DM based on disease severity, therapeutic goals, comorbidities, and treatment-related risks, including hypoglycemia
• Select appropriate patients with T2DM for treatment with short- or long-acting GLP-1 RAs
• Intensify antidiabetes regimens for various patient types to address poor fasting and/or postprandial glycemic control and other relevant clinical parameters
• Educate patients on lifestyle changes, the clinical profiles of GLP-1 RAs, and treatment adherence
GLP-1 RAs = glucagon-like peptide-1 receptor agonists; T2DM = type 2 diabetes mellitus.

Achieving Treatment GoalsRoom for Improvement in T2DM
*P <.01.N = 1497 (1988-1994) and 1447 (2007-2010) adults aged ≥20 years with a self-reported diagnosis of diabetes. Retrospective analysis of data obtained from the National Health and Nutrition Examination Surveys.A1C = glycated hemoglobin; BP = blood pressure; LDL-C = low-density lipoprotein cholesterol.Stark Casagrande S, et al. Diabetes Care. 2013;36:2271-2279.
0
Patie
nts
Ach
ievi
ng G
oal,
%
A1C <7.0% BP <130/80 mm Hg LDL-C <100 mg/dL A1C <7.0%,BP <130/80 mm Hg,
and LDL-C <100 mg/dL
1988-19942007-2010
40
50
60
70
30
20
10
* **
*

Goals Potential Benefits
• Establish a partnership based on exchange of information
• Discuss treatment options• Match therapies with patient
preferences• Prioritize actions required to fulfill
clinical decisions
• Individualized goals and therapy• Improved treatment outcomes• Mitigated behavioral risks and
psychosocial hurdles• Increased treatment adherence• Reduced inappropriate care and
healthcare costs
Shared Decision Making and Coordinated Care in T2DM
Barriers• Time constraints• Patient health literacy• Lack of clinician accessibility and availability• Patient/provider power imbalance
Solutions• Interprofessional care• Patient decision aids
O’Connor PJ, et al. Diabetes Care. 2011;34:1651-1659; Oshima Lee E, et al. N Engl J Med. 2013;368:6-8; Peek ME, et al. J Gen Intern Med. 2009;24:1135-1139; Shojania KG, et al. JAMA. 2006;296:427-440.

AliceAnnual Checkup
• 46-year-old Latina lawyer• Married with no children• BMI, 30.6 kg/m2 (obese)• BP, 141/92 mm Hg• Unhealthy lifestyle
– Little physical activity– Regularly consumes fried
food and red meat– Eats few fruits or
vegetables
• Family history– Father had T2DM
• Medical history– Hypertension diagnosis
5 years ago• Lisinopril 40 mg daily• Atenolol 50 mg daily
– Forgets BP medications at least once weekly
BMI = body mass index.

Screening Asymptomatic Persons for Diabetes
ADA
• Screen at least every 3 years if ≥45 years of age OR BMI ≥25 kg/m2 (≥23 kg/m2 for Asian Americans) with an additional risk factor• Screen more frequently based on results and risk status
AACE• Screen every 3 years if any risk factor is present• Screen annually if ≥2 risk factors are present
Alice’s risk factors
• Sedentary lifestyle • Obese• First-degree relative with T2DM• High-risk race or ethnic group (eg, black, Hispanic)• Hypertension (BP ≥140/90 mm Hg, or therapy)
AACE = American Association of Clinical Endocrinologists; ADA = American Diabetes Association.ADA. Diabetes Care. 2015;38(suppl 1):S1-S91; Handelsman Y, et al. Endocr Pract. 2015;21:1-87.

AliceWorkup and Diagnosis
• A1C, 8.5%• FPG, 225 mg/dL
– Second test 218 mg/dL• eGFR, 88 mL/min/1.73 m2
• ACR, 2.5 mg/mmol • Normal sensory
examination• Normal fundoscopic
examination
• Lipids– LDL-C, 121 mg/dL– HDL-C, 41 mg/dL– TG, 180 mg/dL– TC, 198 mg/dL
ACR = albumin/creatinine ratio; eGFR = estimated glomerular filtration rate; FPG = fasting plasma glucose; HDL-C = high-density lipoprotein cholesterol; TC = total cholesterol; TG = triglycerides.
Alice receives a diagnosis of T2DM

AliceSetting Glycemic Targets
Age, 46 yearsNewly diagnosed
BMI, 30.6 kg/m2 A1C, 8.5% Father treated for T2DM
Hypertension Mild dyslipidemia Normal renal function
Not adherent to other drug
therapies
What treatment goals would you target for Alice?

Reducing T2DM ComplicationsMultidimensional Treatment Goals
a2014 American College of Cardiology/American Heart Association guidelines: Patients aged 40-75 years with T2DM and initial LDL-C ≥70 mg/dL should receive high-intensity (lower LDL-C by ≥50% if 10-year ASCVD risk is ≥7.5%) or moderate-intensity (lower LDL-C 30%-50% if 10-year ASCVD risk is <7.5%) statin therapy.ASCVD = atherosclerotic CVD; CVD = cardiovascular disease.ADA. Diabetes Care. 2015;38(suppl 1):S1-S91; Handelsman Y, et al. Endocr Pract. 2015;21:1-87; Stone NJ, et al. Circulation. 2014;129(25 suppl 2):S1-S45.
Lifestyle modificationsHealthy diet, exercise, smoking cessation
BPADA
<140/90mm HgAACE
<130/80mm Hg
A1CADA
<7.0%AACE≤6.5%
Lipidsa
LDL-C: <100 mg/dL (<70 mg/dL with CVD)
HDL-C: >40 mg/dL (men)>50 mg/dL (women)
TG: <150 mg/dL
Comprehensive Diabetes Management
BMI<25 kg/m2

AliceInitial Treatment Planning
• Target A1C ≤6.5%• Alice and her clinician discuss lifestyle modifications• Clinician suggests a certified diabetes educator
– Patient education– Detailed dietary and exercise recommendations

Diabetes Education and Lifestyle Modifications
Skills-Based Diabetes Education• Disease process and treatment options• Blood glucose monitoring • Medication safety (eg, hypoglycemia)• Strategies to promote behavior change
Individualized Dietary Recommendations• Dehydration and nutritional deficits• Discuss macronutrient content and eating patterns • Monitor carbohydrate intake• Reduce calories to achieve weight loss
− Initial moderate calorie restriction (500-1000 kcal/d)
Physical Activity• At least 150 min/wk of moderate activity • Aerobic, resistance, flexibility
ADA. Diabetes Care. 2015;38(suppl 1):S1-S91; Evert AB, et al. Diabetes Care. 2014;37(suppl 1):S120-S143; Jensen MD, et al. Circulation. 2014;129(25 suppl 2):S102-S138; Haas L, et al. Diabetes Care. 2014;37(suppl 1):S144-S153.
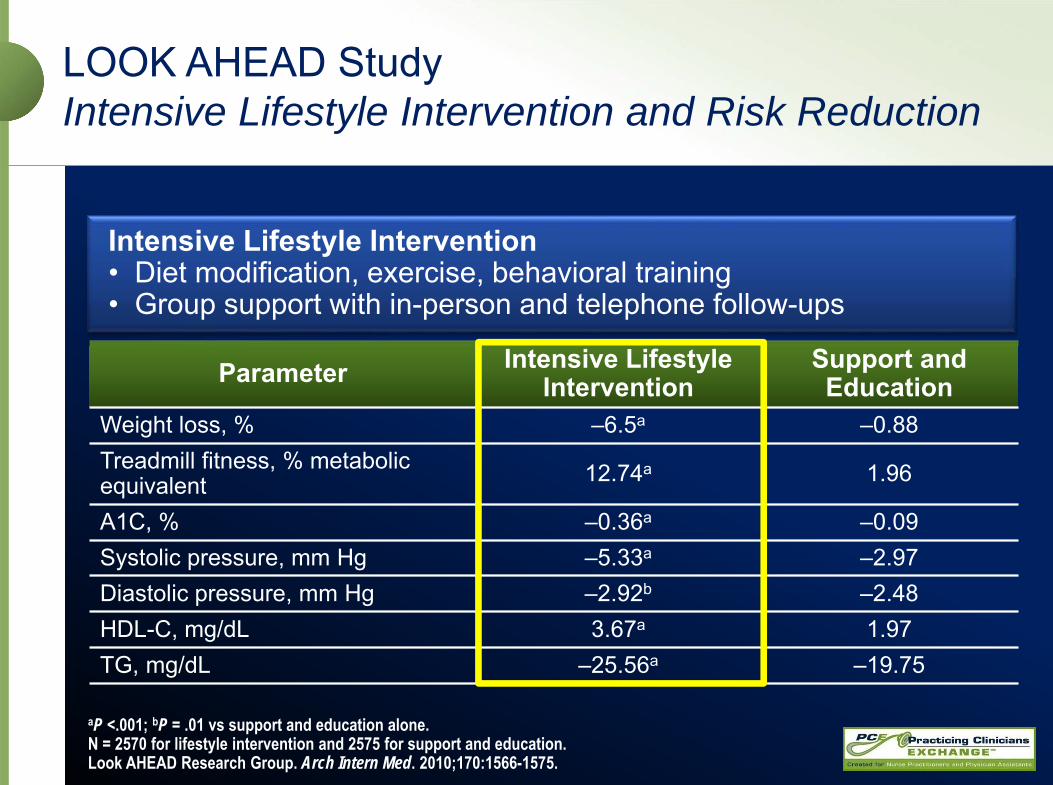
aP <.001; bP = .01 vs support and education alone.N = 2570 for lifestyle intervention and 2575 for support and education.Look AHEAD Research Group. Arch Intern Med. 2010;170:1566-1575.
Parameter Intensive Lifestyle Intervention
Support and Education
Weight loss, % –6.5a –0.88Treadmill fitness, % metabolic equivalent 12.74a 1.96
A1C, % –0.36a –0.09Systolic pressure, mm Hg –5.33a –2.97Diastolic pressure, mm Hg –2.92b –2.48HDL-C, mg/dL 3.67a 1.97TG, mg/dL –25.56a –19.75
LOOK AHEAD StudyIntensive Lifestyle Intervention and Risk Reduction
Intensive Lifestyle Intervention • Diet modification, exercise, behavioral training• Group support with in-person and telephone follow-ups

Look AHEADIntensive Lifestyle Intervention and Diabetes Remission
Years of Continuous Remission (Partial or Complete)
Remission Prevalence Remission Duration
Year
0
4
8
12
16
Prev
alen
ce, %
1 2 3 4
Intensive lifestyle interventionDiabetes support and education
0
4
8
12
20
Estim
ate,
%
≥1 ≥2 ≥3 4
Intensive lifestyle interventionDiabetes support and education
16
N = 4503 adults with T2DM and BMI ≥25 kg/m2.Gregg EW, et al. JAMA. 2012;308:2489-2496.

AliceOverview
• 46-year-old Latina woman with an unhealthy lifestyle
• BMI, 30.6 kg/m2 (obese)• BP, 141/92 mm Hg• A1C, 8.5%
– Target A1C, ≤6.5%• FPG, 225 mg/dL• eGFR, 88 mL/min/1.73 m2
• ACR, 2.5 mg/mmol • Normal sensory and fundoscopic exams
• Lipids– LDL-C, 121 mg/dL– HDL-C, 41 mg/dL– TG, 180 mg/dL– TC, 198 mg/dL
• Father had T2DM• Medical history
– Hypertension• Lisinopril and atenolol• Often forgets medications
What medication(s) would you initially consider for Alice?

AACE/ACE Algorithm for Glycemic Control
Lifestyle Modification
Entry A1C <7.5% Entry A1C ≥7.5% Entry A1C >9.0%
Monotherapya Dual therapya
MetforminGLP-1 RASGLT2 inhibitorDPP-4 inhibitorAG inhibitorTZDSU/GLN
If not at goal in 3 months, proceed to
dual therapy
GLP-1 RASGLT2 inhibitorDPP-4 inhibitorTZDBasal insulinColesevelamBromocriptine QRAG inhibitorSU/GLN
METF
ORMI
N or
othe
r firs
t-line
agen
t Dual therapy
ORtriple
therapy
Insulin ±other
agents
Add or intensify insulinPossible benefits or few adverse eventsUse with caution
aMedications listed in order of suggested hierarchy of usage.ACE = American College of Endocrinology; AG = α-glucosidase; DPP-4 = dipeptidyl peptidase-4; GLN = glinide; QR = quick release; SGLT2 = sodium-glucose cotransporter-2; SU = sulfonylurea; TZD = thiazolidinedione.Garber AJ, et al. Endocr Pract. 2015;21:438-447.
If not at goal in 3 months, proceed to triple therapy
Symptoms
NO YES

AliceTreatment Initiation and Follow-up
• Prescribed metformin 500 mg twice daily – Titrated up to 1000 mg twice daily after 1 week
• At 1-month follow-up appointment– A1C, 7.9%
• Previous value, 8.5%• Target value, ≤6.5%
– FPG, 125 mg/dL• Previous value, 225 mg/dL
– PPG, 219 mg/dL (2-hours postmeal)– No significant changes in any other clinical parameters
PPG = postprandial glucose.
Clinician suggests adding a GLP-1 RA.Should the 2nd agent have been initiated with metformin?

Effects of Incretin Hormones
• GLP-1 and GIP stimulate insulin release in response to food intake• Reduced incretin effect is an early sign of T2DM development• GLP-1 and GIP are rapidly degraded by DPP-4
– Incretin-based therapies include degradation-resistant GLP-1 RAs and inhibitors of DPP-4
N = 8 metabolically healthy control subjects. GIP = gastric inhibitory polypeptide. Elrick H, et al. J Clin Endocrinol Metab. 1964;24:1076-1082; Grunberger G. J Diabetes. 2013;5:241-253; Holst JJ, et al. Diabetes Care. 2011;34 (suppl 2):S251-S257; Nauck M, et al. Diabetologia. 1986;29:46-52; Russell S. Int J Clin Pharm. 2013;35:159-172.
Time, min
15
Insu
lin, m
U/L
60
Oral glucose load (50 g)Intravenous glucose infusion10
5
0–10 –5 120 180
Incretin Effect

GLP-1 RAs Effects on Human Physiology
1. Holst JJ, et al. Trends Mol Med. 2008;14:161-168; 2. Flint A, et al. Adv Ther. 2011;28:213-226; 3. Degn K, et al. Diabetes. 2004;53:1187-1194; 4. Baggio LL, Drucker DJ. Gastroenterology. 2007;132:2131-2157; 5. Horowitz M, et al. Diabetes Res Clin Pract. 2012;97:258-266; 6. Vilsbøll T, et al. BMJ. 2012;344:d7771; 7. Niswender K, et al. Diabetes Obes Metab. 2013;15:42-54; 8. Fonseca V, et al. Diabetes. 2010;59(suppl 1):A79(296-OR).
Brain5-7
Body weightSatietyEnergy intake
Pancreas1-4
Insulin secretion (glucose-dependent)and β-cell sensitivity Insulin synthesisGlucagon secretion (glucose-dependent)
CV System8
Systolic BP
Liver4
Hepatic glucose output
Stomach1,4
Gastric emptying

FDA-Approved GLP-1 RAsDaily Formulations
Medication Dosage Forms
Adverse Eventsa Dosing
Exenatide twicedaily1
• 5 μg/dose in 1.2-mL prefilled pen
• 10 μg/dose in 2.4-mL prefilled pen
Nausea, vomiting, dyspepsia
1. Start at 5 μg twice daily (1 hour before morning and evening meals)
2. Increase to 10 μg twice daily after 1 month
Liraglutide2 • Prefilled, multidose pen that delivers doses of 0.6 mg, 1.2 mg, or 1.8 mg
Nausea, diarrhea,vomiting,
constipation, headache
1. Initiate at 0.6 mg once daily, regardless of meals
2. After 1 week, increasedose to 1.2 mg
3. If glycemic control is not acceptable, dose can beincreased to 1.8 mg
aTreatment-emergent adverse reactions with ≥5% incidence in clinical trials with drug as monotherapy (excluding hypoglycemia). FDA = Food and Drug Administration.1. Drugs@FDA. www.accessdata.fda.gov/drugsatfda_docs/label/2011/021773s029s030lbl.pdf. Accessed May 29, 2015; 2. Drugs@FDA. www.accessdata.fda.gov/drugsatfda_docs/label/2013/022341s020lbl.pdf. Accessed May 29, 2015.
Shor
t Act
ing
Long
Act
ing

FDA-Approved GLP-1 RAsWeekly Formulations
Medication Dosage Forms Adverse Eventsa Dosing
Exenatide once weekly1
• Single-dose tray with 2-mg vial
• Single-dose 2-mg prefilled pen
Nausea, diarrhea,injection-site nodule, constipation,headache, dyspepsia
1. Administer at 2 mg once every 7 days (weekly), independent of meals
Albiglutide2 • 30-mg or 50-mg lyophilized powder in single-dose pen for reconstitution
Upper respiratory tract infection, diarrhea,nausea, injection-site reaction, cough, back pain, arthralgia, sinusitis, influenza
1. Administer at 30 mg once every 7 days (weekly), regardless of meals
2. If glycemic control is not acceptable, dose can increaseto 50 mg
Dulaglutide3 • Single-dose pen in 0.75-mg or 1.5-mg doses
• Prefilled, single-dose syringe in 0.75-mg or 1.5-mg doses
Nausea, diarrhea, vomiting, abdominal pain, and decreased appetite
1. Initiate at 0.75 mg weekly, regardless of meals or time of day; dose can be increased to 1.5 mg
2. If dose is missed, missed dose must be taken within 3 days
aTreatment-emergent adverse reactions with ≥5% incidence in clinical trials with drug as monotherapy (excluding hypoglycemia).1. Drugs@FDA. www.accessdata.fda.gov/drugsatfda_docs/label/2014/022200s008lbl.pdf). Accessed May 29, 2015;2. Albiglutide prescribing information. www.gsksource.com/pharma/content/dam/GlaxoSmithKline/US/en/Prescribing_Information/Tanzeum/pdf/TANZEUM-PI-MG-IFU-COMBINED.PDF. Accessed May 29, 2015; 3. Dulaglutide prescribing information. http://pi.lilly.com/us/trulicity-uspi.pdf. Accessed May 29, 2015.
Long
Act
ing
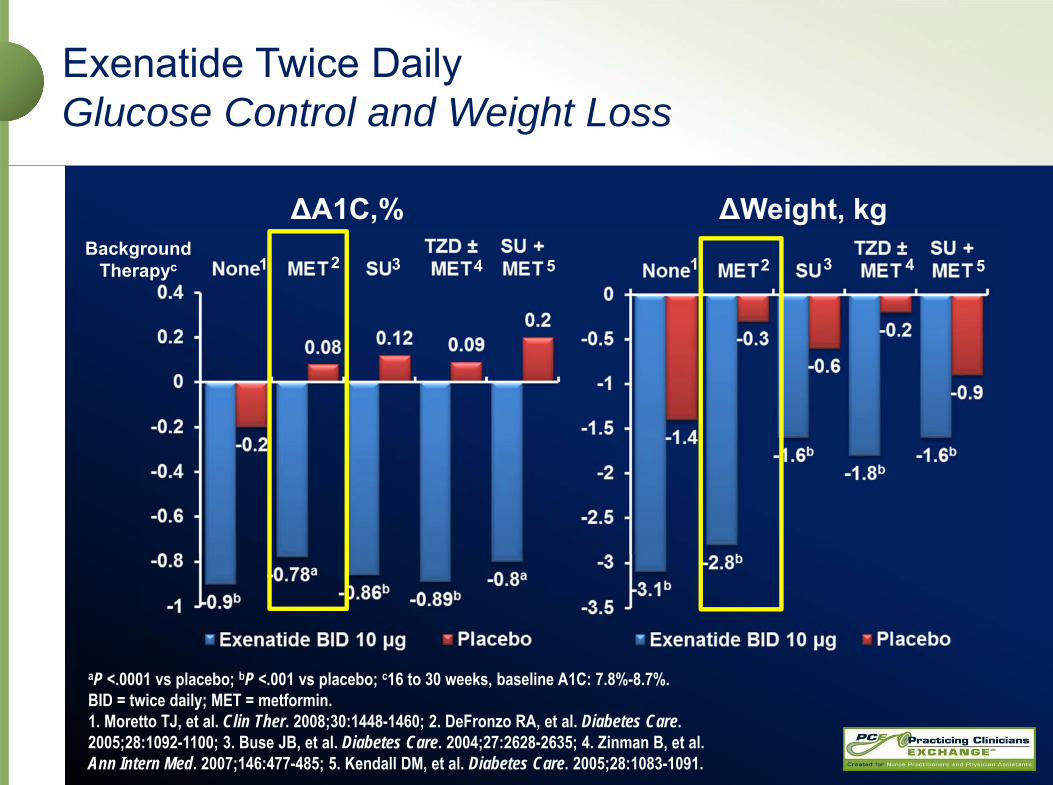
Exenatide Twice DailyGlucose Control and Weight Loss
aP <.0001 vs placebo; bP <.001 vs placebo; c16 to 30 weeks, baseline A1C: 7.8%-8.7%. BID = twice daily; MET = metformin.1. Moretto TJ, et al. Clin Ther. 2008;30:1448-1460; 2. DeFronzo RA, et al. Diabetes Care. 2005;28:1092-1100; 3. Buse JB, et al. Diabetes Care. 2004;27:2628-2635; 4. Zinman B, et al. Ann Intern Med. 2007;146:477-485; 5. Kendall DM, et al. Diabetes Care. 2005;28:1083-1091.
ΔA1C,% ΔWeight, kg1 2 3 34 45 521
BackgroundTherapyc

LiraglutideGlucose Control and Weight Loss
aP <.0001 vs comparator; bP <.001 vs comparator; cP <.01 vs comparator; d26 weeks (except 52 weeks for monotherapy), mean baseline A1C: 8.2%-8.6%.1. Garber A, et al. Lancet. 2009;373:473-481; 2. Nauck M, et al. Diabetes Care. 2009;32:84-90; 3. Marre M, et al. Diabet Med. 2009;26:268-278; 4. Zinman B, et al. Diabetes Care. 2009;32:1224-1230; 5. Russell-Jones D, et al. Diabetologia. 2009;52:2046-2055.
ΔA1C,% ΔWeight, kg
Liraglutide 1.8 mg Placebo Sulfonylurea
1 2 3 34 45 521Background
Therapyd
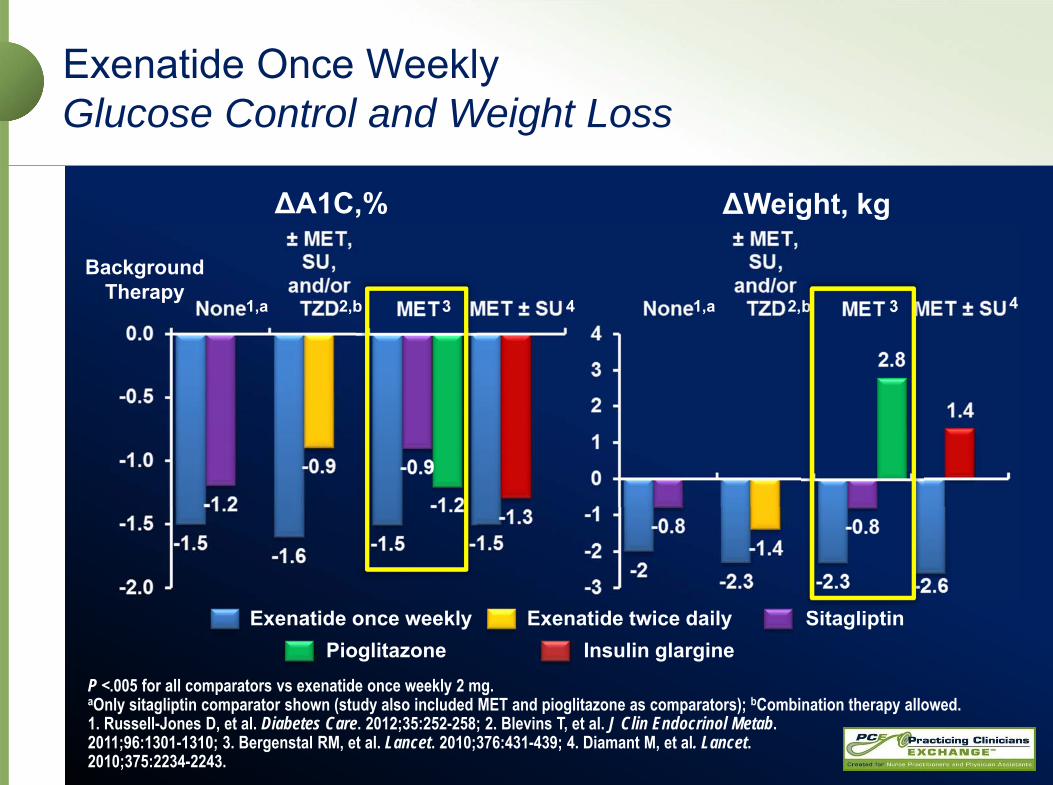
Exenatide Once WeeklyGlucose Control and Weight Loss
P <.005 for all comparators vs exenatide once weekly 2 mg.aOnly sitagliptin comparator shown (study also included MET and pioglitazone as comparators); bCombination therapy allowed.1. Russell-Jones D, et al. Diabetes Care. 2012;35:252-258; 2. Blevins T, et al. J Clin Endocrinol Metab. 2011;96:1301-1310; 3. Bergenstal RM, et al. Lancet. 2010;376:431-439; 4. Diamant M, et al. Lancet. 2010;375:2234-2243.
ΔA1C,% ΔWeight, kg
Exenatide once weekly Exenatide twice daily SitagliptinPioglitazone Insulin glargine
1,a 2,b 3 34 41,a 2,b
BackgroundTherapy

AlbiglutideGlucose Control and Weight Loss
aP <.0001 vs comparator; bP <.001 vs comparator; cP = .0086 vs insulin glargine and met noninferiority margin; dData represent only patients treated with albiglutide 50 mg; eData represent only patients treated with albiglutide 30 mg. 1. Reinhardt R, et al. 49th Annual Meeting EASD, 2013. ePoster #903; 2. Ahrén B, et al. Diabetes Care. 2014;37:2141-2148; 3. Reusch J, et al. Diabetes Obes Metab. 2014;16:1257-1264; 4. Weissman PN, et al. Diabetologia. 2014;57:2475-2484.
ΔA1C,% ΔWeight, kg
Albiglutide 30 mg or 50 mg Placebo Insulin glargine
1 2 3 3 44 21
BackgroundTherapy

DulaglutideGlucose Control and Weight Loss
aP <.05 vs comparator and met superiority margin; bP <.001 vs comparator and met superiority margin; cMet superiority margin vs comparator; dData shown are for weeks 26 or 52; eComparators added to insulin lispro and background conventional insulin therapy.GLIM = glimepiride; INS = insulin; PIO = pioglitazone.1. Umpierrez G, et al. Diabetes Care. 2014;37:2168-2176; 2. Nauck M, et al. Diabetes Care. 2014;37:2149-2158; 3. Wysham C, et al. Diabetes Care. 2014;37:2159-2167; 4. Giorgino F, et al. 74th ADA Scientific Sessions, 2014. Abstract 330-OR; 5. Jendle J, et al. 74th ADA Scientific Sessions, 2014. Abstract 962-P.
ΔA1C,% ΔWeight, kgBackground
Therapyd
Dulaglutide 1.5 mg Exenatide twice daily SitagliptinInsulin glargine Metformin
1 2 3 4 5,e 1 2 3 4 5,e

Long-Term Efficacy and Safety5-Year Data for Exenatide Once Weekly
• Significant improvements in FPG, body weight, lipid levels, and diastolic BP• Nausea and injection-site reactions decreased vs initial 30-week trial• No major hypoglycemia or new safety signals
N = 153 of 258 extension-phase patients (59.3%) who completed 5 years of treatment (exenatide once weekly2 mg or exenatide twice daily 10 μg for 30 weeks ± oral antidiabetes drugs, followed by 4.4 years on exenatide once weekly 2 mg ± oral drugs). DURATION = Diabetes therapy Utilization: Researching changes in A1C, weight and other factors Through Intervention with exenatide ONce weekly; SE = standard error. Wysham CH, et al. Mayo Clin Proc. 2015;90:356-365.
Open-Ended, Uncontrolled Extension of 30-Week DURATION-1Baseline A1C, 8.1%
32.7
43.9
0
10
20
30
40
50
≤6.5% <7.0%A1C Targets
Prop
ortio
n of
Pa
tient
s, %
Year
Mea
n A
1C (S
E), %
6.56.8 6.8 6.9 7
6
6.5
7
7.5
8
8.5
0 1 2 3 4 5

In an 82-week exenatide completer cohort, weight loss was 1) similar across degrees of nausea, 2) progressive despite stable
nausea incidence, and 3) unlikely to be driven by nausea.3
Weight Loss With GLP-1 RAsNot Driven by Gastrointestinal Adverse Events
aP <.05 vs baseline; bP <.05 vs placebo. EXN = exenatide; LIRA = liraglutide; NVD = nausea, vomiting, diarrhea; PBO = placebo; QW = once weekly.1. Russell-Jones D, et al. 70th ADA Scientific Sessions, 2010;1886-P; 2. Drucker DJ, et al. Lancet. 2008;372:1240-1250; 3. Blonde L, et al. Diabetes Obes Metab. 2006;8:436-447.

GLP-1 RAs and CV Outcomes Ongoing Trials
Trial Agent Patients (N)
Duration (y)
Patient-Years
Estimated Completion
REWIND(NCT01394952) Dulaglutide 9622 6.5 62,543 2019
EXSCEL(NCT01144338)
Exenatide once weekly 14,000 7.5 105,000 2018
LEADER(NCT01179048) Liraglutide 9340 5 46,700 2015
ELIXA(NCT01147250) Lixisenatide 6075 3.9 23,693 2015
SUSTAIN 6(NCT01720446) Semaglutide 3297 2.8 9232 2016
National Institutes of Health. www.clinicaltrials.gov. Accessed May 29, 2015.

Safety Concerns With Antidiabetic Therapies Hypoglycemia
aIncludes saxagliptin, linagliptin, and sitagliptin; bIncludes canagliflozin, dapagliflozin, and empagliflozin; cIncludes NPH insulin, insulin glargine, and insulin detemir; dHypoglycemia risk is higher when used with sulfonylurea or insulin. NPH = neutral protamine Hagedorn.1. Drugs@FDA. www.accessdata.fda.gov/drugsatfda_docs/label/2011/021773s029s030lbl.pdf. Accessed May 29, 2015; 2. Drugs@FDA. www.accessdata.fda.gov/drugsatfda_docs/label/2014/022200s008lbl.pdf. Accessed May 29, 2015; 3. Drugs@FDA. www.accessdata.fda.gov/drugsatfda_docs/label/2013/022341s020lbl.pdf. Accessed May 29, 2015; 4. Albiglutide prescribing information. www.gsksource.com/pharma/content/dam/GlaxoSmithKline/US/en/Prescribing_Information/Tanzeum/pdf/TANZEUM-PI-MG-IFU-COMBINED.PDF. Accessed May 29, 2015; 5. Dulaglutide prescribing information. http://pi.lilly.com/us/trulicity-uspi.pdf. Accessed May 29, 2015; 6. Boland CL, et al. Ann Pharmacother. 2013;47:490-505; 7. Nauck MA. Drug Des Devel Ther. 2014;8:1335-1380.
Drug A1C Reduction, % Hypoglycemia Incidence, %
Exenatide twice daily1 0.5-0.7 3.8-10.7d
Exenatide once weekly2 1.6 0-3.7d
Liraglutide3 0.8-1.1 3.7-10.9d
Albiglutide4 0.8-1.0 2-3d
Dulaglutide5 0.7-0.8 2.6-5.6d
DPP-4 inhibitors6,a 0.4-0.8 0.3-5SGLT2 inhibitors7,b 0.7 0-6d
Sulfonylureas6 1-2 18-30Pioglitazone6 0.5-1.4 0-3.7Basal Insulin6,c 1.5-3.5 29.9-61.2
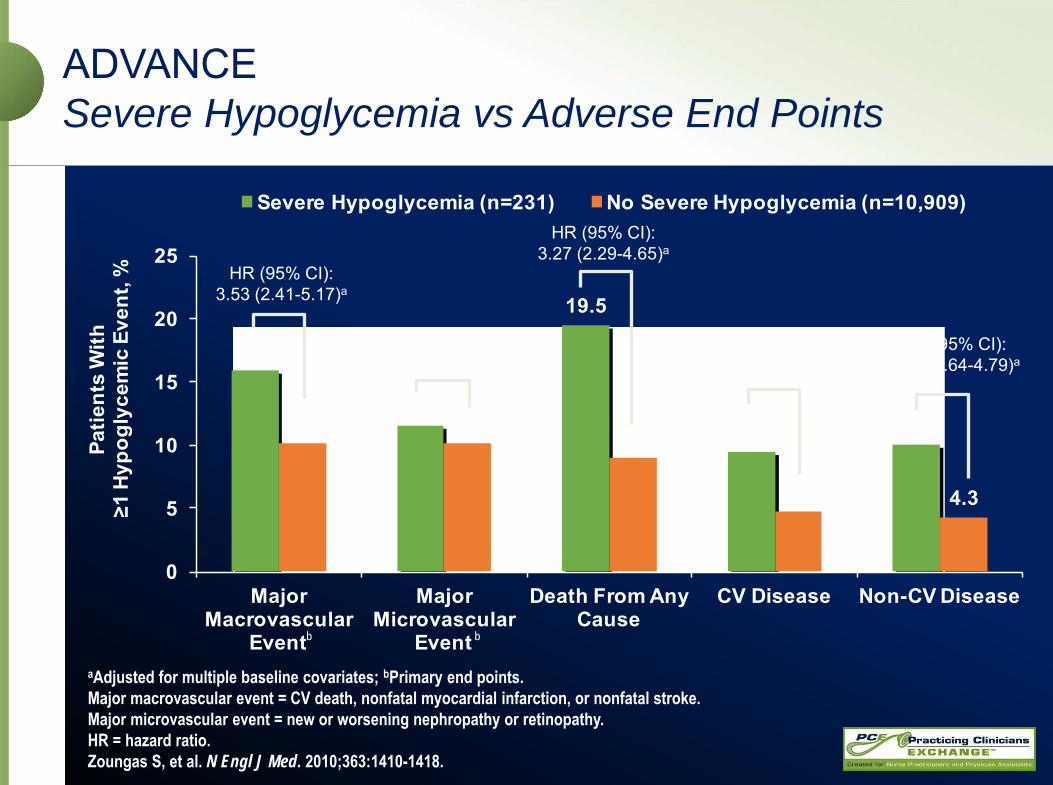
ADVANCESevere Hypoglycemia vs Adverse End Points
aAdjusted for multiple baseline covariates; bPrimary end points. Major macrovascular event = CV death, nonfatal myocardial infarction, or nonfatal stroke.Major microvascular event = new or worsening nephropathy or retinopathy.HR = hazard ratio.Zoungas S, et al. N Engl J Med. 2010;363:1410-1418.
15.9
11.5
19.5
9.5 10.010.2 10.1 9.0
4.8 4.3
0
5
10
15
20
25
Major Macrovascular
Event
Major Microvascular
Event
Death From Any Cause
CV Disease Non-CV Disease
Patie
nts
With
≥1
Hyp
ogly
cem
ic E
vent
, %
Severe Hypoglycemia (n=231) No Severe Hypoglycemia (n=10,909)
HR (95% CI):3.53 (2.41-5.17)a
HR (95% CI):2.19 (1.40-3.45)a
HR (95% CI):3.27 (2.29-4.65)a
HR (95% CI):3.79 (2.36-6.08)a
HR (95% CI):2.80 (1.64-4.79)a
b b
Safe Prescribing With GLP-1 RAsAcute Pancreatitis
Precautions1-5
• Cases of pancreatitis have been reported
• Consider treatments other than GLP-1 RAs in patients with history of pancreatitis
Recommendations1-5
• Ask about pancreatitis history• Discontinue promptly if
pancreatitis symptoms occur • If acute pancreatitis develops,
do not restart GLP-1 RA• Report cases of pancreatitis to
www.fda.gov/medwatch
1. Drugs@FDA. www.accessdata.fda.gov/drugsatfda_docs/label/2011/021773s029s030lbl.pdf. Accessed May 29, 2015; 2. Drugs@FDA. www.accessdata.fda.gov/drugsatfda_docs/label/2014/022200s008lbl.pdf. Accessed May 29, 2015; 3. Drugs@FDA. www.accessdata.fda.gov/drugsatfda_docs/label/2013/022341s020lbl.pdf. Accessed May 29, 2015; 4. Albiglutide prescribing information. www.gsksource.com/pharma/content/dam/GlaxoSmithKline/US/en/Prescribing_Information/Tanzeum/pdf/TANZEUM-PI-MG-IFU-COMBINED.PDF. Accessed May 29, 2015; 5. Dulaglutide prescribing information. http://pi.lilly.com/us/trulicity-uspi.pdf. Accessed May 29, 2015.

Safe Prescribing With GLP-1 RAsPossible Thyroid and Endocrine Risk
• Recommendations• Counsel patients regarding MTC risk and symptoms of thyroid tumors• Value of routine calcitonin and/or ultrasound monitoring is uncertain; such monitoring may
lead to unnecessary procedures• Patients with thyroid nodules or elevated serum calcitonin levels identified for other reasons
should be sent to an endocrinologist• Report MTC to state cancer registry, regardless of treatment
http://www.naaccr.org/Membership/MembershipDirectory.aspx
Contraindications1-5 Albiglutide Dulaglutide Exenatide Twice Daily
Exenatide Once Weekly Liraglutide
Do not use if personal/ family history of MTC or presence of multiple endocrine neoplasia syndrome type 2
X X X X
MTC = medullary thyroid carcinoma.1. Drugs@FDA. www.accessdata.fda.gov/drugsatfda_docs/label/2011/021773s029s030lbl.pdf. Accessed May 29, 2015; 2. Drugs@FDA. www.accessdata.fda.gov/drugsatfda_docs/label/2014/022200s008lbl.pdf. Accessed May 29, 2015; 3. Drugs@FDA. www.accessdata.fda.gov/drugsatfda_docs/label/2013/022341s020lbl.pdf. Accessed May 29, 2015; 4. Albiglutide prescribing information. www.gsksource.com/pharma/content/dam/GlaxoSmithKline/US/en/Prescribing_Information/Tanzeum/pdf/TANZEUM-PI-MG-IFU-COMBINED.PDF. Accessed May 29, 2015; 5. Dulaglutide prescribing information. http://pi.lilly.com/us/trulicity-uspi.pdf. Accessed May 29, 2015.
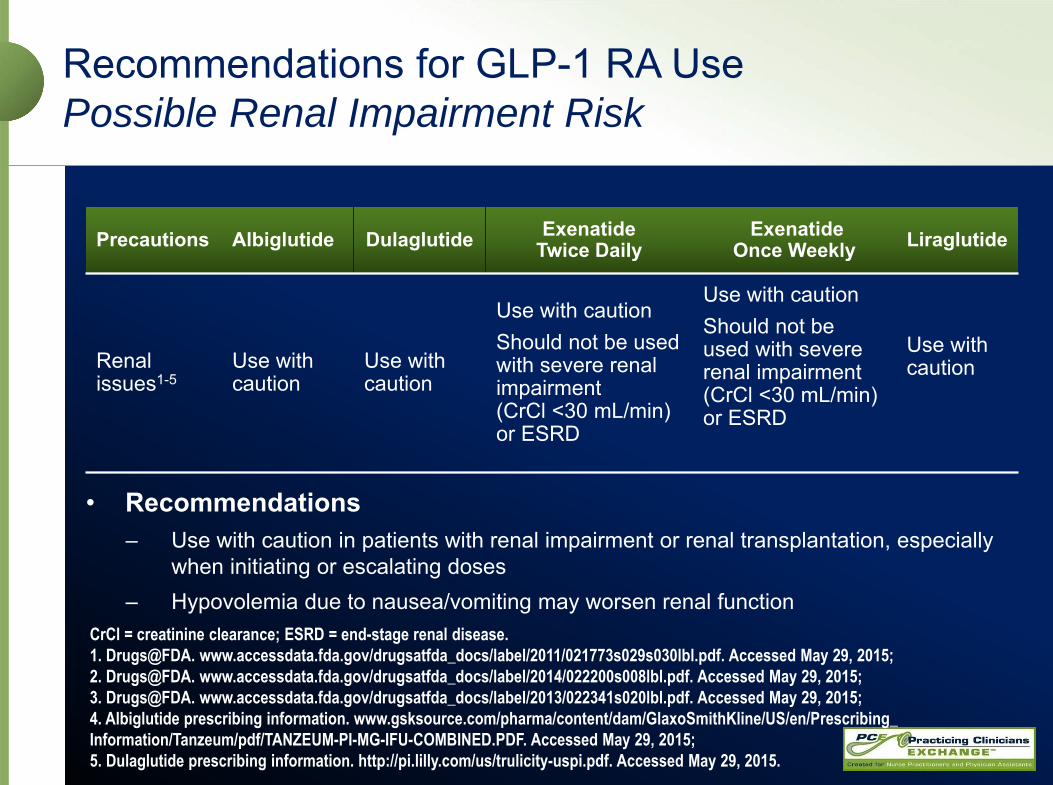
Recommendations for GLP-1 RA UsePossible Renal Impairment Risk
• Recommendations– Use with caution in patients with renal impairment or renal transplantation, especially
when initiating or escalating doses– Hypovolemia due to nausea/vomiting may worsen renal function
Precautions Albiglutide Dulaglutide Exenatide Twice Daily
Exenatide Once Weekly Liraglutide
Renal issues1-5
Use with caution
Use with caution
Use with cautionShould not be used with severe renal impairment (CrCl <30 mL/min) or ESRD
Use with cautionShould not be used with severe renal impairment (CrCl <30 mL/min)or ESRD
Use with caution
CrCl = creatinine clearance; ESRD = end-stage renal disease.1. Drugs@FDA. www.accessdata.fda.gov/drugsatfda_docs/label/2011/021773s029s030lbl.pdf. Accessed May 29, 2015; 2. Drugs@FDA. www.accessdata.fda.gov/drugsatfda_docs/label/2014/022200s008lbl.pdf. Accessed May 29, 2015; 3. Drugs@FDA. www.accessdata.fda.gov/drugsatfda_docs/label/2013/022341s020lbl.pdf. Accessed May 29, 2015; 4. Albiglutide prescribing information. www.gsksource.com/pharma/content/dam/GlaxoSmithKline/US/en/Prescribing_Information/Tanzeum/pdf/TANZEUM-PI-MG-IFU-COMBINED.PDF. Accessed May 29, 2015; 5. Dulaglutide prescribing information. http://pi.lilly.com/us/trulicity-uspi.pdf. Accessed May 29, 2015.
AliceTreatment Tailoring
• Treated with metformin 1000 mg twice daily • A1C, 7.9%
– Target value, <6.5%• FPG, 125 mg/dL• PPG, 219 mg/dL (2-hours postmeal)• Alice expresses some concerns about GLP-1 RAs
– Worried that the injections will be painful– Has read comments online about cancer risks
Her clinician discusses the available options for GLP-1 RA medications
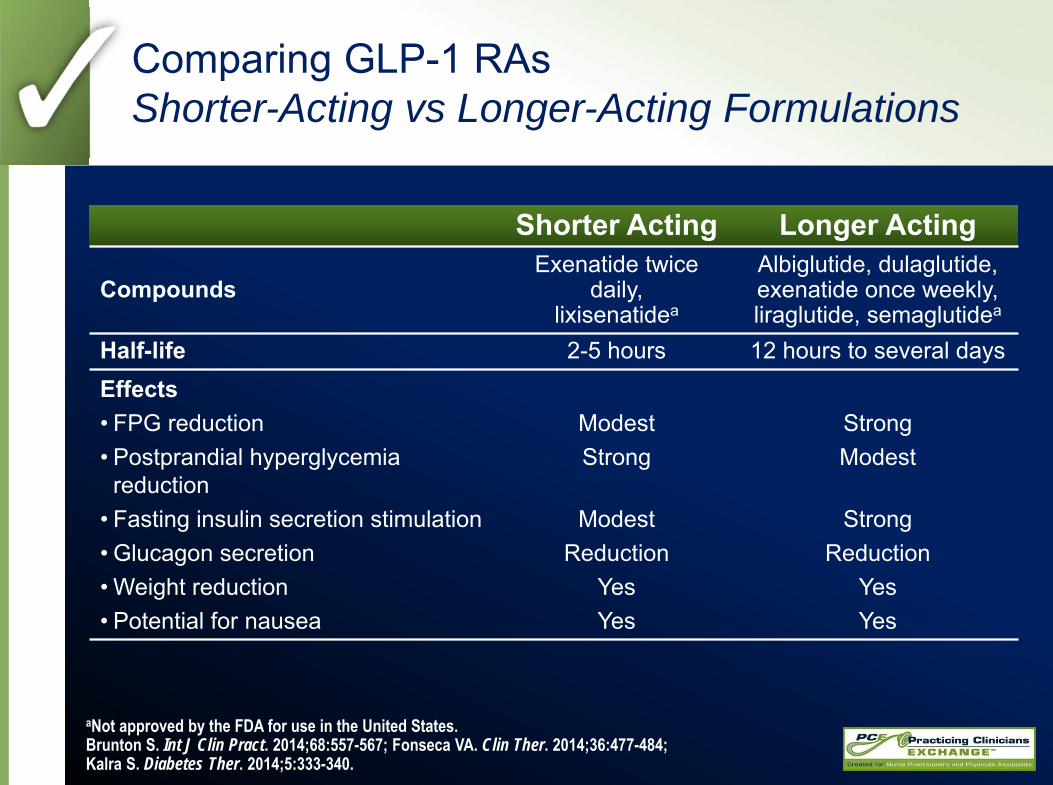
Comparing GLP-1 RAsShorter-Acting vs Longer-Acting Formulations
aNot approved by the FDA for use in the United States.Brunton S. Int J Clin Pract. 2014;68:557-567; Fonseca VA. Clin Ther. 2014;36:477-484; Kalra S. Diabetes Ther. 2014;5:333-340.
Shorter Acting Longer Acting
CompoundsExenatide twice
daily, lixisenatidea
Albiglutide, dulaglutide, exenatide once weekly, liraglutide, semaglutidea
Half-life 2-5 hours 12 hours to several daysEffects• FPG reduction• Postprandial hyperglycemia
reduction• Fasting insulin secretion stimulation• Glucagon secretion• Weight reduction• Potential for nausea
ModestStrong
ModestReduction
YesYes
StrongModest
StrongReduction
YesYes
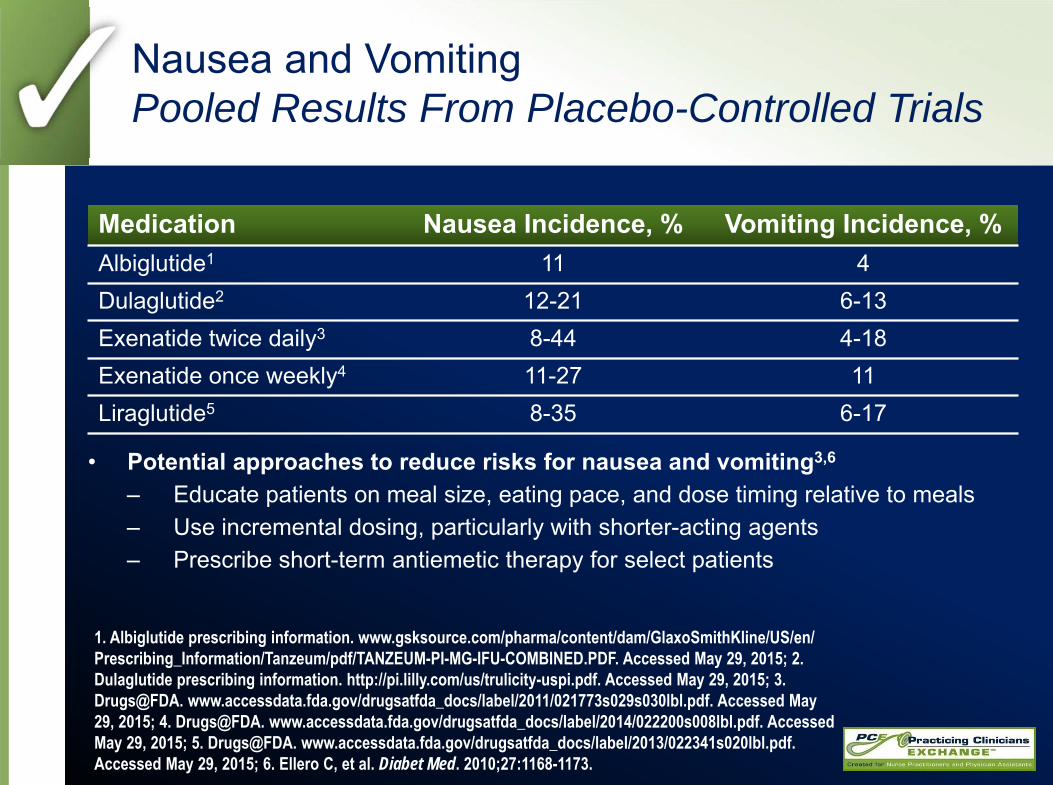
Nausea and VomitingPooled Results From Placebo-Controlled Trials
• Potential approaches to reduce risks for nausea and vomiting3,6
– Educate patients on meal size, eating pace, and dose timing relative to meals– Use incremental dosing, particularly with shorter-acting agents– Prescribe short-term antiemetic therapy for select patients
1. Albiglutide prescribing information. www.gsksource.com/pharma/content/dam/GlaxoSmithKline/US/en/Prescribing_Information/Tanzeum/pdf/TANZEUM-PI-MG-IFU-COMBINED.PDF. Accessed May 29, 2015; 2. Dulaglutide prescribing information. http://pi.lilly.com/us/trulicity-uspi.pdf. Accessed May 29, 2015; 3. Drugs@FDA. www.accessdata.fda.gov/drugsatfda_docs/label/2011/021773s029s030lbl.pdf. Accessed May 29, 2015; 4. Drugs@FDA. www.accessdata.fda.gov/drugsatfda_docs/label/2014/022200s008lbl.pdf. Accessed May 29, 2015; 5. Drugs@FDA. www.accessdata.fda.gov/drugsatfda_docs/label/2013/022341s020lbl.pdf. Accessed May 29, 2015; 6. Ellero C, et al. Diabet Med. 2010;27:1168-1173.
Medication Nausea Incidence, % Vomiting Incidence, %Albiglutide1 11 4Dulaglutide2 12-21 6-13Exenatide twice daily3 8-44 4-18Exenatide once weekly4 11-27 11Liraglutide5 8-35 6-17

GLP-1 RAs vs Basal Insulin
Buse JB, et al. Diabetes Obes Metab. 2015;17:145-151; Diamant M. Lancet Diabetes Endocrinol. 2014;2:464-473; Russell-Jones D, et al. Diabetologia. 2009;52:2046-2055.
-0.8-1.2 -1.3
-2.3
-0.6-0.9
-1.3
-2.1
-4
-3
-2
-1
01st 2nd 3rd 4th
Exenatide QWGlargine
Cha
nge
in A
1CFr
om B
asel
ine,
% -0.9 -1.1-1.4
-1.8
-0.5-0.9
-1.2-1.5
-4
-3
-2
-1
01st 2nd 3rd 4th
LiraglutideGlargine
Baseline A1C, % 7.1 7.1 7.7 7.8 8.4 8.5 9.9 9.8
End of TrialA1C, % 6.4 6.6 6.6 6.8 7.1 7.1 7.5 7.7
n 55 49 54 59 59 59 60 53
7.2 7.1 7.9 7.9 8.5 8.6 9.5 9.4
6.3 6.6 6.8 7.0 7.2 7.4 7.7 7.9
61 63 55 69 49 44 59 49
Patient Quartiles Based on Baseline A1C

Combining GLP-1 RA and Basal Insulin
aPercenatge achieving <7% across baseline A1C quartiles for liraglutide and exenatide once weekly vs insulin glargine.Buse JB, et al. Diabetes Obes Metab. 2015;17:145-151; Holst JJ, Vilsbøll T. Diabetes Obes Metab. 2013;15:3-14; Vora J, et al. Diabetes Metab. 2013;39:6-15.
• Simple to initiate• Can control FPG and PPG• Do not impair α-cell response
to hypoglycemia (reduce risks of severe hypoglycemia)
• Weight-lowering• Achieve A1C target in ~60%a
• Simple to initiate• Control nocturnal hyperglycemia
and FPG• Lower hypoglycemia risk than NPH• Can cause weight gain• Achieve A1C target in ~50%a
Potential for better overall A1C control
Basal insulin analogs GLP-1 RAs
Additive effects
Complementary actions
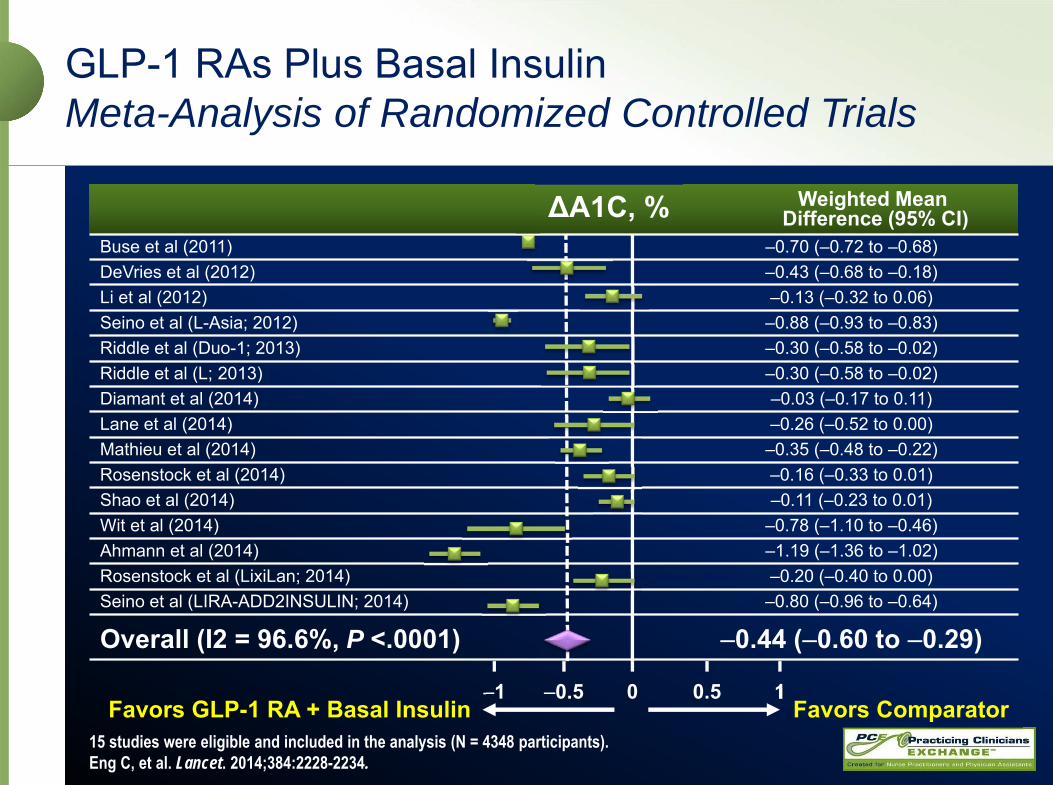
Weighted Mean Difference (95% CI)
Buse et al (2011) –0.70 (–0.72 to –0.68)DeVries et al (2012) –0.43 (–0.68 to –0.18)Li et al (2012) –0.13 (–0.32 to 0.06)Seino et al (L-Asia; 2012) –0.88 (–0.93 to –0.83)Riddle et al (Duo-1; 2013) –0.30 (–0.58 to –0.02)Riddle et al (L; 2013) –0.30 (–0.58 to –0.02)Diamant et al (2014) –0.03 (–0.17 to 0.11)Lane et al (2014) –0.26 (–0.52 to 0.00)Mathieu et al (2014) –0.35 (–0.48 to –0.22)Rosenstock et al (2014) –0.16 (–0.33 to 0.01)Shao et al (2014) –0.11 (–0.23 to 0.01)Wit et al (2014) –0.78 (–1.10 to –0.46)Ahmann et al (2014) –1.19 (–1.36 to –1.02)Rosenstock et al (LixiLan; 2014) –0.20 (–0.40 to 0.00)Seino et al (LIRA-ADD2INSULIN; 2014) –0.80 (–0.96 to –0.64)
Overall (I2 = 96.6%, P <.0001) –0.44 (–0.60 to –0.29)
GLP-1 RAs Plus Basal InsulinMeta-Analysis of Randomized Controlled Trials
15 studies were eligible and included in the analysis (N = 4348 participants).Eng C, et al. Lancet. 2014;384:2228-2234.
–1 –0.5 0 0.5 1Favors GLP-1 RA + Basal Insulin Favors Comparator
ΔA1C, %
AliceKey Points
• Individualize goals and treatment intensity for T2DM– Consider comorbidities– Address psychosocial factors – Take steps to reduce risk of hypoglycemia
• Monitor multiple metabolic targets for comprehensive management and reduction of CV risk– A1C, lipids, BP
• Consider appropriate roles of GLP-1 RAs– Clinically relevant reductions in A1C– Relatively low risks of hypoglycemia– Potential for weight loss and other CV benefits

PCE Action Plan
Routinely screen for T2DM with a frequency that reflects patient age, family history, and other risk factors
Ensure lifestyle modifications are the foundation of any treatment regimen for T2DM
Counsel patients about the risks, signs, and symptoms of pancreatitis before initiating treatment with a GLP-1 RA
Select GLP-1 RAs for T2DM based on the patient’s hyperglycemia profile and preferences
Recommend that patients eat smaller meals and more slowly when initiating treatment with a GLP-1 RA





























