Embed Size (px)
Citation preview

Progress and Challenges to approve a drug based on data from global clinical trials: PMDA’s experience
Dr Yoshiaki Uyama
Pharmaceuticals & Medical Devices Agency (PMDA)Visiting Professor, Graduate School of Advanced Clinical Science, Chiba University
Visiting Professor, Graduate School of Medicine, Nagoya University
Disclaimer• The views and opinions expressed in the following PowerPoint slides
are those of the individual presenter and should not be attributed to
Pharmaceuticals and Medical Devices Agency (PMDA), Drug
Information Association, Inc. (“DIA”), its directors, officers, employees,
volunteers, members, chapters, councils, Communities or affiliates, or
any organization with which the presenter is employed or affiliated.
• Drug Information Association, Drug Information Association Inc., DIA
and DIA logo are registered trademarks. All other trademarks are the
property of their respective owners.
2

Globalization of Drug Developments
Nature Rev Drug Discovery, 7: 13, 2008
Japan
15.7; 10.3%
3

APEC MRCT Road Map
-Gap Analysis-
4
• Target Economies:
– Canada, Chinese Taipei, Indonesia, Japan, Malaysia, Mexico, Peru, Singapore, Korea, Thailand, and the United States
• Period : October 2013 ~ April 2014
• Methodology : Questionnaire by e-mail
• Responses received : 8 regions
• Collection rate : 72.7 % (8/11 regions)
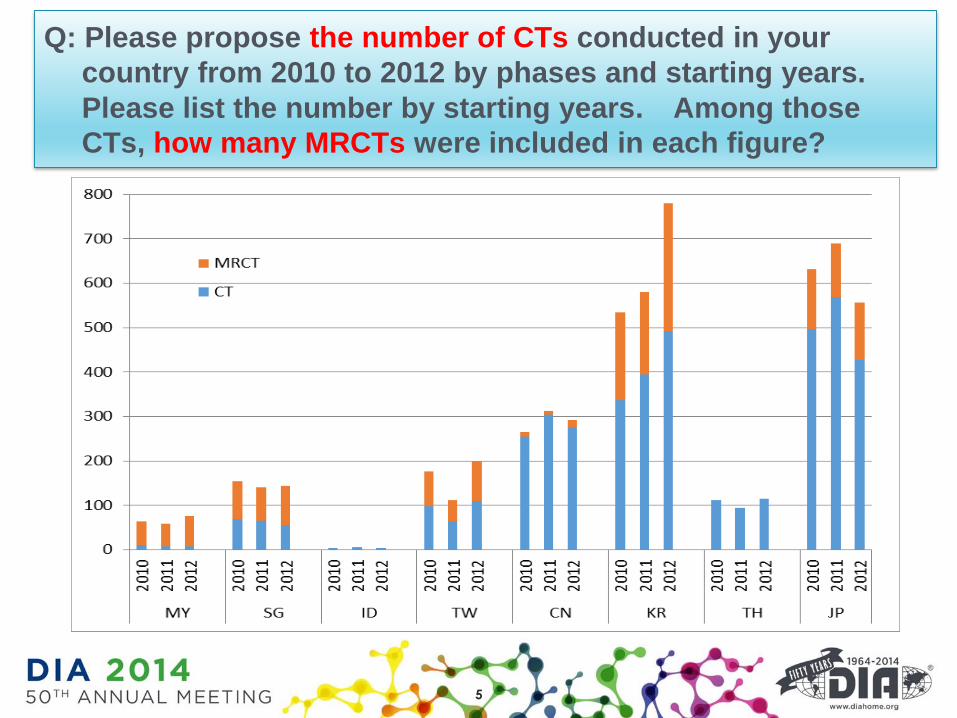
Q: Please propose the number of CTs conducted in your
country from 2010 to 2012 by phases and starting years.
Please list the number by starting years. Among those
CTs, how many MRCTs were included in each figure?
5

0
100
200
300
400
500
600
700
Phase I
Non MRCT MRCT
Q: Please propose the number of CTs conducted in your
country from 2010 to 2012 by phases and starting years.
Please list the number by starting years. Among those
CTs, how many MRCTs were included in each figure?
0
50
100
150
200
250
300
350
400
450
500
Phase II
Non MRCT MRCT
0
100
200
300
400
500
600
700
800
900
Phase III
Non MRCT MRCT
6

Q: Please describe the annual number of new
drugs approved in your country from 2010 to 2012.
0
20
40
60
80
100
120
140
160
2010 2011 2012
New Drug Approved
CAN IDN KOR MYS SGP TWN THA JPN
7

Japanese:http://www.pmda.go.jp/operations/notice/2007/file/0928010.pdf
English:http://www.pmda.go.jp/operations/notice/2007/file/0928010-e.pdf
Japanese version English version
Basic principles on Global Clinical Trials
8

9
Trend of new drug application approvals
in Japan
FY2007 FY2008 FY2009 FY2010 FY2011 FY2012 FY2013
0
5
10
15
% o
f G
CT
% of GCT
% of Bridging
Total 81 79 107 114 130 134 133
MRCT 1 0 4 7 12 18 21
Bridging 4 2 3 6 2 3 1
(Year)

Approved new drugs based on GCT
in Japan
10
2006~2009 20112010 2012
Tolterodine
Losartan
Trastuzumab
Insulin -
Glulisine
Tadalafil
Peramivir
Everolimus
Panitumumab
Travoprost/
Timolol
Temsirolimus
Laninamivir
Nilotinib
Dabigatran
Trastuzumab
Pramipexole
Edoxaban
Dasatinib
Indacaterol
Linagliptin
Gefitinib
Everolimus
Denosumab
Aripiprazole
Olanzapine
Exenatide
Crizotinib
Budesonide/
Formoterol
Formoterol
Esomeprazole
Axitinib
Budesonide/
Formoterol
Atomoxetine
Aflibercept
Insulin -
Degludec
Glycopyrronium
Pazopanib
• 59 applications were approved as of March 1, 2014
Red: Asian Clinical Trial
Everolimus
Fesoterodine
Everolimus
Apixaban
Insulin-
Degludec+Aspart
Paclitaxel
Pregabalin
Tofacitinib
Regorafenib
2013
Guidance
Guidance: “Basic Principles on Global Clinical Trials”
Guidance RC
Guidance RC: “Basic Principles on Global Clinical
Trials –
Reference Cases”
2014
Bevacizumab
Pertuzumab
Lixisenatide
Regorafenib
Indacaterol/
Glycopyrronium
Paliperidone
Vilanterol/
Fluticasone
Bevacizumab
Aflibercept
Riociguat
Tadalafil
Afatinib
Turoctocog alfa
Ranibizumab

• New active ingredient indicated for the treatment of
persistent/recurrent Chronic Thromboembolic
Pulmonary Hypertension (CTEPH)
• Soluble guanylate cyclase (sGC) stimulator
• Orphan drug
• Application date: Feb 2013 (US/EU)
May 2013 (JP)
Riociguat: Example of GCT (1)
11
http://www.info.pmda.go.jp/shinyaku/P201300173/630004000_22600AMX00013000_A100_2.pdf
http://www.info.pmda.go.jp/shinyaku/P201300173/index.html

NChange from
baseline to last visita
Difference between
groups b
All regionRiociguat 173 42.0 (-376, 335)
45.69 [ 24.74, 66.63] Placebo 88 5.0 (-389, 226)
JapanRiociguat 11 64.0 (-376, 217)
-Placebo 5 14.0 (6, 85)
Primary endpoint: 6MWD (m)
Change from baseline: Median (Min, Max), Difference between groups: LS mean [ 95 CI]
a:Last observed value (not including follow-up) for subjects who completed the study or withdrew, except imputed worst
value in case of death or clinical worsening without a termination visit or a measurement at that termination visit.
b:ANCOVA model with baseline value, treatment group, and region as fixed effects
PIII: Efficacy
NChange from
baseline to last visit
Difference between
groups b
All regionRiociguat 151 -175.94 (-1753.2, 511.0)
-246.43 [-303.33, -189.53] Placebo 82 14.89 (-679.6, 969.2)
JapanRiociguat 9 -159.16 (-291.5, 146.8)
-Placebo 5 -14.18 (-125.6, 205.1)
Secondary endpoint: PVR (dyn∙sec∙cm-5)
12
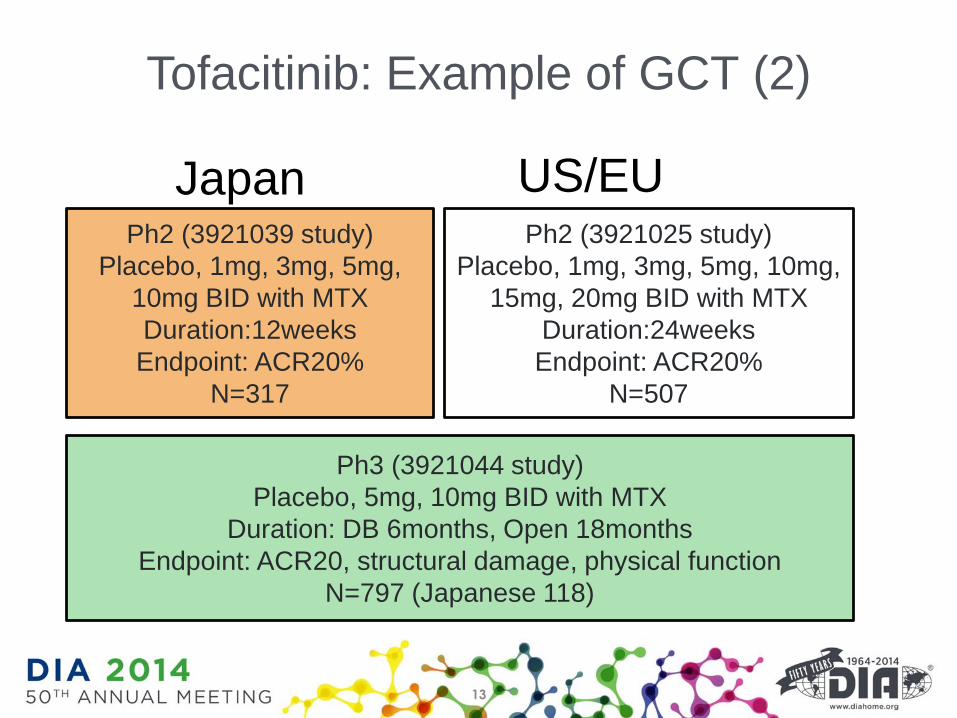
Ph2 (3921039 study)
Placebo, 1mg, 3mg, 5mg,
10mg BID with MTX
Duration:12weeks
Endpoint: ACR20%
N=317
Ph3 (3921044 study)
Placebo, 5mg, 10mg BID with MTX
Duration: DB 6months, Open 18months
Endpoint: ACR20, structural damage, physical function
N=797 (Japanese 118)
Japan US/EUPh2 (3921025 study)
Placebo, 1mg, 3mg, 5mg, 10mg,
15mg, 20mg BID with MTX
Duration:24weeks
Endpoint: ACR20%
N=507
13
Tofacitinib: Example of GCT (2)

-3
-2.5
-2
-1.5
-1
-0.5
0
0.5
5mg
N=277
10mg
N=2905mg
N=44
10mg
N=44
JapaneseFAS
Dose response of tofacitinib
0
10
20
30
40
50
60
70ACR20 ACR50 ACR70
FAS JapaneseModified Total Sharp Score (vs placebo)
14
Average & 95%CI

Review experiences of GCT data
• Ethnic factor consideration is important even in AsianGCTs
• Extrinsic ethnic factors such as concomitant therapiessometimes have impacts on data evaluation
• PPK data are useful for ethnic factor consideration
• Confirming efficacy in overall population and consistencyevaluation in Japanese sub-population– limitation in evaluating data when sample size of Japanese was
so small
• Differences in adverse event rate are not uncommon;partly due to difference on categorization or datacollection process of adverse events in GCTs
15

New Guidance (Sep 5th 2012): Basic principles on Global Clinical Trials
(Reference Cases)
Japanese:http://www.pmda.go.jp/regulatory/file/guideline/new_drug/GCT_jirei.pdf
English:http://www.pmda.go.jp/regulatory/file/english_guideline/new_drug/GCT-jirei_en.pdf
16
17
Future Drug Development

Regulatory Perspective: PMDA and FDA
Clin Pharmacol Ther. 2013;94:230-42.Clin Pharmacol Ther. 2013;94:195-8.
18
US FDA PMDA
Ueno, T et al, Clin Pharmacol Ther 95, 533-41 (2014).
Honig, P.K. Clin Pharmacol Ther 95, 467-9 (2014).
19

GCTs can contribute to reducing the lag
in drug development
20
Clinical development strategy
0
500
1000
1500
2000
2500
3000
3500
4000
4500
5000
5500
6000
6500
7000
The
lag
in d
rug
deve
lopm
ent
(day
s)
1111 days
Local
trial
(n = 69)
Local and
foreign trials
(n = 59)
Bridging
study
(n = 19)
Global
clinical
trial
(n = 18)
Foreign
trial
(n = 13)
No
efficacy/safety
trial (n = 5)
***
**

• Simultaneous global drug development is a
useful strategy to provide a drug earlier to
Japanese patients
• But, we are facing some challenges in the future
drug development
21

• Effects of ethnic factors on drug efficacy/safety
should be more characterized
• Methods for planning/evaluation should be
established
– Sample size calculation, consistency evaluation
etc.
• Regulatory harmonization
22
Challenges for better GCTs
Advancing regulatory science

PMDA GCT Project Team
• 12 members as a representative from various offices
(New drug, Biologics, Conformity audit)
• Discuss various regulatory issues relating to GCTs
• Responsible for a guideline relating to GCTs
• Periodically hold meetings with industries for discussion
23
Promoting conduct of GCTs more appropriately
for drug approval

PMDA’s New Initiative: Advanced workflow of review/consultation
More rational & effective
evaluation process for
regulatory decision
Giving additional
scientific value to
submitted data Regulatory Science
e-Submission
of study data
Each reviewer utilizes innovative
assessment techniques
Sophisticated review
Advanced evaluation methods
Active utilization of Modeling &
Simulation Disease model
Objective B/R assessment
Identifying AE-related factors etc.
NDA
etc.
• More predictable
efficacy/safety after approval
• Reduction of applicant’s
work load
• More scientific regulatory
decision
• Epoch-making proposal
leading the world
• Proactive publication of
guideline More evidence-based consultation
Sophisticated Consultation
Cross-Products Analysis
Cooperation with
Academia
Practical use of Innovative
Medical Products Analysis by PMDA
More effective and high quality
Review
More efficient and Successful
Development Database
Data
Accumulation
24

25
Possible Development Strategy
Japan
Other
Asia
US/EU
PK,
Safety
Exploratory,
Dose-FindingConfirmatoryPOC
Japan only
West only
J/W
GCT
J/W
GCTJapan/West
W/J/E
GCT
W/J/E
GCTWest/Japan/
Asia
Asian
GCT
Asian
GCT Asia
Asian
GCT
Asian
GCTEarly
Asia
Asian
GCT
W/J/E
GCT
W/J/E
GCT
Asia
LeadingEast
Asian
GCT
Asian
GCT
Asian
GCTReal
Asia
Asian
GCT
Asian
GCT
J/W
GCT
J/W
GCT
Early
Japan/West
J/W
GCT

26
PMDA’s proposal: New ICH guideline on MRCTs

EU North America
USA
Canada
Asia
Drugs from Asia to the world
Cooperation for better drug development
27

28
Information
• HOMEPAGE (English)
http://www.pmda.go.jp/english/index.html
• Regulatory Science Page
http://www.pmda.go.jp/regulatory/index.html
• E-mail:
Thank you for your attention





























