Embed Size (px)
Citation preview

48
Precision medicine is positioned to revolutionize the healthcare landscape, and the utilization of advanced
clinical development technologies is key to supporting precision medicine trials. These technologies can
harness a variety of disparate data sources at richer and greater volumes to build more accurate predictive
models for different patient subsets. We discuss briefly the nature of precision medicine, the FDA’s initiatives
encouraging the development of targeted therapies and the importance of the revolution in genomics for
precision medicine. We describe the five Vs of big data and the pivotal role of big data in precision medicine.
We present four clinical trial technologies that provide essential capabilities for precision medicine:
(1) Continuous collection, aggregation, and integration of myriad data sources; (2) Adaptive and iterative
study design and execution as new information becomes available; (3) Maintenance and management of data
throughout the study life cycle; and (4) Advanced analytics for research discovery. Precision medicine shows
great promise for developing exploratory hypotheses from its broad variety of data and iterative approach,
evaluating these hypotheses, and producing safer, more effective treatments for targeted patient subgroups
with advantageous benefit-risk profiles. The complexities of precision medicine study designs require
substantial planning, investment, and commitment from all stakeholders.
Clinical Trial Technologies for Precision Medicine: The Current State of the Art by Ruthanna Davi, Ph.D.,Therese Dolan, Jeffrey Wiser, and Steven Schwager, Ph.D.

1. Introduction
Precision medicine is an approach to medicinal
practice that tailors decisions to a patient’s
individual characteristics: genetic, anatomical,
physiological, environmental, and lifestyle.
Precision medicine is defined by the National
Academies of Science as “an emerging
approach for disease treatment and prevention
that takes into account individual variability
in genes, environment, and lifestyle for each
person” (National Academies of Science, 2017).
Individually tailored healthcare is a rapidly
developing, exciting alternative to the
traditional practices that are often described
as one-size-fits-all, based on the best course
of prevention or treatment for the general
population. In this approach, if an initial
treatment fails, the patient moves on to the
next standard treatment, again based on the
population. The challenge of this method
of practicing medicine have long been
recognized.
Clinicians and patients today have access to a
rapidly expanding range of data. Drug regula-
tory authorities and the practice of medicine
itself are adapting to this new information
era, which holds promise both to further our
understanding of disease etiology and to
deliver better patient care and optimal
outcomes (Heckman-Stoddard, 2014;
Woodcock, 2017).
Torkamani et al. (2017) recently expanded on
the concept of precision medicine by defining
high-definition medicine as “the data-driven
practice of medicine through the utilization of
highly detailed, longitudinal, and multi-para-
metric measures of the determinants of health
to modify disease risk factors, detect disease
processes early, drive precise and dynamically
adjusted interventions, and determine
preventative and therapeutic intervention
efficacy from real-world outcomes.” Establishing a
personal baseline through frequent assessment
of the determinants of health can enable early
detection and intervention, sometimes before
diseases manifest clinically.
The objective of this paper is to describe the
current state of affairs for sponsors who are
considering a precision medicine approach and
seeking to create a development path that will
maximize the chance of success.
1.1. Precision Medicine and the FDA
The U.S. Food and Drug Administration (FDA)
has embraced the possibilities offered by
precision medicine. This is reflected in a recent
New England Journal of Medicine article by
Janet Woodcock, director of FDA’s Center for
Drug Evaluation and Research (CDER), and Lisa
LaVange, director of the Office of Biostatistics
at CDER (Woodcock, 2017) that discusses the
need to capitalize on similarities among trials
(e.g., shared control group and recruiting
efforts) to gain efficiencies in drug development
using umbrella, basket, or platform trials and
cites I-SPY2 trial and Lung-Map as examples of
such innovation.
The FDA recently announced the Precision
Medicine Initiative (PMI), with the overarching
goals of facilitating the identification of genetic
drivers of disease and developing better
diagnostic tools and treatments (FDA, 2016).
The FDA has issued two PMI draft guidances
and established the precisionFDA portal
for oversight, analysis, and validation of
methodology related to next-generation
sequencing (NGS), also known as
high-throughput sequencing. NGS tests are
used to identify the genomic differences in
individuals (FDA, 2016) that are the basis of
the genetic component of precision medicine.
The FDA has fostered numerous initiatives that
encourage drug sponsors to develop targeted
therapies and has provided guidance on the
regulatory pathway for such medicines. FDA’s
Enrichment Guidance (FDA, 2012) describes
approaches to studying therapeutics when
the efficacy or safety of that therapeutic is
expected to vary across subgroups. The FDA
guidance on adaptive designs provides advice
for incorporating analyses of accumulating
data at prospectively planned time points
(FDA, 2010). Adaptations such as modifications
in the treatment randomization ratios,
dropping or adding an arm, or revising a
patient’s treatment based on their inadequate
response to an initial treatment are all
examples of how adaptive designs can fuel
precision medicine and are discussed in the
guidance. The Co-development Guidance
provides advice for obtaining contemporane-
ous marketing authorization for a therapeutic
product and its corresponding companion
diagnostic (FDA, 2016). And, expected soon is
the Complementary Diagnostics Guidance.
This guidance is expected to lay out a
framework that allows for a diagnostic device
that aids in the benefit-risk assessment of
the therapeutic product (but it is not essential
as with the companion diagnostic).
The FDA has approved an increasing number of
medicines that are indicated for defined subsets
of patients, including the first ever-approval
of a drug [Keytruda (pembrolizumab)] to treat
patients whose cancers have a specific genetic
feature, or biomarker, rather than being based
on the location of origin of the cancer.
Importantly, these precision medicine
approvals are not limited to oncology
indications. For instance, the FDA has approved
two products for treatment of severe asthma
in patients with an eosinophilic phenotype
[Cinqair (reslizumab), Nucala (mepolizumab)].
In March 2017, FDA concurrently approved a
drug [Zejula (niraparib)] and a complementary
diagnostic test [BRACAnalysis CDx] to identify
patients with germline BRCA mutations, the
subset of patients expected to benefit most
from Zejula. A complementary diagnostic test
is defined as one that aids in the benefit-risk
decision(s) related to a particular therapeutic
product but is not essential to the safe and
effective use of the product, as is the case with
a companion diagnostic. Draft guidance on the
topic of therapeutic products developed with
a complementary diagnostic test is expected
from the FDA soon (Mansfield, 2015). Overall, the
FDA continues to solidify a workable regulato-
ry platform that encourages innovation while
maintaining efficacy and safety as priorities.
49
PR
EC
ISIO
N T
OO
LS

51
PR
EC
ISIO
N T
OO
LS
1.2. Genomic Data and the Current State of
Precision Medicine
The ongoing revolution in genomics and
molecular biology continues to improve our
fundamental understanding of human biology
and disease; at the same time, it presents new
opportunities for precision medicine. For
example, not long ago, breast cancer was
largely defined as a single disease. Today,
based on molecular subtyping, breast cancer
is recognized to consist of several distinct
molecular subtypes (Bartlett, 2017). The
biomarkers that distinguish these molecular
subtypes or influence the risk of cancer
development have been translated into
targeted clinical practice (Marchina, 2010;
Godet, 2017; Slamon, 2001). Similarly, the
clinical phenotype of depression has long
been known to encompass several subtypes
(e.g., major depressive disorder, bipolar
disorder, and atypical depression) and to
show high variability regarding treatment
response. This has often made the diagnosis
As precision medicine continues to propagate
into clinical practice, it is increasingly impor-
tant for clinicians to be trained to understand
precision medicine and to use it effectively
for the benefit of their patients. The National
Human Genome Research Institute (a research
institute of the National Institutes of Health
(NIH)) recently awarded several training grants
that will instruct medical doctors in applying
computational tools to disease-gene discovery,
patient genome interpretation, and big data
management in research and clinical settings
(National Human Genome Research Institute,
2016).
Drug developers may view precision medicine
as a daunting and uncertain task, and utilizing
large datasets (i.e., big data) effectively for
precision medicine requires careful planning,
investment, and discussion among stakehold-
ers. Establishing the appropriate infrastructure
is a crucial step in dealing with huge volumes
of information and the complexities of
adaptive precision medicine study designs.
and treatment of depression challenging for
clinicians. However, exciting new biomarker
data may soon aid clinical practice by providing-
molecular insights to guide accurate diagnosis
and prediction of treatment response (Buzuk,
2016; McIntyre, 2016; Strawbridge, 2017; Yue,
2016).
Increasingly, precision medicine is transitioning
from a specialized treatment approach to an
aspect of standard clinical practice. As of
September 2017, approximately 179 studies
(~50% actively recruiting) were listed in
clinicaltrials.gov as search returns for the term
“precision medicine,” with approximately
21% of these trials being funded by industry.
This is a gross underestimate of the actual
number of trials that can be deemed precision
medicine trials, because most of these
trials are not explicitly labeled as such in
clinicaltrials.gov. Based on combinations
of keywords related to biomarkers, next
generation sequencing and synonymous
terms, we can roughly suggest that this
number is an order of magnitude greater.

52
To predict outcomes accurately in a patient
subgroup, precision medicine demands large
volumes of data from often disparate data
streams, some of which are generated
continuously. One challenge for drug
developers is how to seamlessly ingest,
aggregate, integrate, and analyze these
datasets in an easy-to-use workflow that
can help uncover meaningful relationships
resulting in improved patient outcomes.
Precision medicine is an exploratory and
iterative journey, so the data platform of
choice must be flexible enough to adapt to
emerging data and to allow investigators to
redefine – in real time – patient clusters into
more precise subsets and to redesign studies
to enable refined hypothesis testing. A useful
starting point is to adopt a flexible, integrated,
and intelligent clinical development platform
as the engine that will drive the precision
medicine program. These are crucial features
in an optimized precision medicine approach.
The remainder of this paper discusses the
relevance of big data to precision medicine
trials and some key clinical development
technologies that can facilitate the
development of targeted therapies.
“ Phenotypic data, drug interaction data, family history data. Making sense of that data is a huge challenge, The key is to teach physicians to effectively use the new tools to tackle big data.”(National Human Genome Research Institute, 2016)
The ability to redefine patient clusters and adapt study designs in real time are key attributes of a platform to support a precision medicine approach.
“As drugs become more precise and trials become more complex, it will be increasingly important to exploit optimized clinical trial technologies.The platform should seamlessly ingest, aggregate, integrate, and facilitate analysis of disparate data types so that the ideal target patient population can be identified quickly and reliably.”

53
PR
EC
ISIO
N T
OO
LS
2. Big Data and the Path to Precision Medicine
A precision medicine approach to drug
development relies on large datasets to cluster
patients into increasingly more precise subsets.
This requires that investigators measure
patients on numerous attributes of many
different types, ranging from genotype to
phenotype and beyond (Beckmann, 2016;
Dinov, 2016; Dumitrescu, 2017). Simply
ingesting and managing data of such scope
and complexity are formidable tasks, and
conceiving, executing, and interpreting
appropriate analyses are even more formidable.
However, we must meet these challenges in
order to achieve the tremendous gains that
precision medicine promises over one-size-
fits-all population-based medicine.
The precision medicine approach generates a
unique and comprehensive patient profile by
integrating a wide range of medical data.
Taken in the aggregate, these data encompass
enormous volume, velocity, variety, veracity,
and value. We can describe these attributes –
the five Vs of big data – briefly as:
Volume — Enormous amounts of data are
generated by many data streams of different
types, including over 3 billion nucleotides
in the human genome; hundreds or thousands
of laboratory test results and vital signs;
wearable sensor readings of dozens of kinds;
environmental data on dozens or hundreds
of relevant biological, chemical, and
meteorological features; medical imaging
data containing many thousands or millions
of pixels per image; and more.
The utility of genetic information to drive
precision medicine has been clearly
demonstrated (e.g., trastuzumab (Herceptin)
for women with HER-2 positive breast cancer).
Other important data streams also offer vast
possibilities for additional lines of investiga-
tion. Electronic health records (EHRs) are an
example of big data that can help inform a
precision medicine approach. A recent article
by Dumitrescu et al. (2017) concluded that
current and new EHR technology will provide
international standards for applications that
facilitate precision medicine using the
complex healthcare information in health,
social, economic, behavioral, and environmental
data. This article reported the results of a
genome-wide association study for resistant
hypertension linked to EHRs and genotypes.
The authors demonstrated the utility of DNA
biobanks linked to EHRs for classifying
resistant hypertension cases and controls
and for performing large-scale genome-wide
association studies. Evans (2016) utilized an
algorithm based on a combination of billing
codes, laboratory values, text queries, and
prescription records. A study by Szlosek (2016)
reported the use of machine learning and
natural processing algorithms to automate the
evaluation of clinical decision support in EHR
systems. The authors showed that a machine
learning algorithm can be used to identify
abnormal head CT scans in free-text health
care data with a high degree of accuracy.
These examples demonstrate that using big
data to support a precision medicine approach
has moved beyond a conceptual framework.
These and other well-documented studies
showcase how big data technology can
enable precision medicine. However, it is our
experience that some drug developers are not
prepared to handle the complexities inherent
in the five Vs of big data, which can quickly
overwhelm the clinical development platform
and the supporting business processes not
designed for them.
Velocity
Many data streams produce new data at
rates of dozens or hundreds of points per
second (e.g., sensor data, environmental
data, imaging data).
Variety
The information collected for a patient
includes structured and unstructured data
from vital signs, laboratory tests,
genomic sequencing, patient behaviors,
social media, wearable sensor readings,
point-of-care notes, photos, medical
images, and more.
Veracity
It is critical for precision medicine trials
to have high-quality data. Missing and
inaccurate observations can rarely be
completely eliminated, but every effort
must be made to minimize their occur-
rence. Poor data quality will produce
errors in data interpretation and the
analyses required for precision medicine.
Value
The impressive scope of big data is
not an end in itself, but a means to the
end of valuable results: better therapeutic
and preventative treatments. Precision
medicine must manage the volume,
velocity, and variety of big data and
maximize the veracity of the data;
however, to be successful, precision
medicine must extract value from the
data with analytical algorithms whose
results yield improved treatments for
patients.
In precision medicine as well as traditional
medicine, data quality is a wide-ranging,
serious issue that poses a grave threat to the
validity of clinical research. Poor planning
often results in poorly standardized data,
missing or incomplete clinical datasets,
incompatible conceptualizations of data
types and elements, and infrastructure that is
inadequate for processing robust healthcare
data (Anderson, 2014; Field & Sansone, 2016;
Mead, 2006; Richesson, 2007).
The following section highlights clinical trial
technologies that make precision medicine
possible, not only by enabling the efficient
collection, aggregation, and integration of
data, but by empowering the exploratory and
iterative processes that drive the precision
medicine approach via powerful analytics.
3. Clinical Trial Technologies to Facilitate
Precision Medicine
Advanced clinical trial technologies allow
investigators to seamlessly collect and integrate
massive amounts of data from sources across
the clinical care continuum. An adaptable
system can leverage both historical datasets
and in-study datasets to update and optimize
models that allow for re-running the cohort
selection, risk stratification, and subsequent
intervention assignment. Further, advanced
predictive analytics enable the development
of new treatment models that can adapt to
new information as it is uncovered, with
subsequent forecasts and trials becoming
increasingly accurate as the volume of data
expands.
As discussed earlier, an important first step to
achieving a precision medicine approach is
to utilize a clinical technology platform that
ingests a wide variety of phenotypic data,
integrates the data into standardized data
models, and unifies these data models with
analytic technologies. This is a key determinant
of an optimized precision medicine approach.
Huge volumes of data, poorly standardized data
models, or integration challenges between data
models and analytical technologies can quickly
overwhelm ill-equipped data centers and
business processes, and without an adequate
infrastructure in place, the entire platform can
collapse, leading to lost time, money, and even
valuable data.
The platform should provide these capabilities,
which we list and then discuss in more detail:
l Continuous collection, aggregation, and
integration of myriad data sources.
l Adaptive and iterative study design and
execution as new information is made
available.
l Maintenance and management of data
throughout the study life cycle.
l Advanced analytics for research discovery
during the study and post-study.
3.1. Continuous Collection, Aggregation, and
Integration of Myriad Data Sources
To benefit fully from insights available with a
big data approach, massive amounts of data
must be collected, aggregated, and integrated,
either in real time (e.g., sensor data) or from
archives (e.g., unstructured data such as
point-of-care notes, histological images,
and photos). By capturing a wider variety of
non-traditional data derived as close to the
source as possible, big data offers amazing
opportunities for precision medicine. Below
are brief descriptions of the types of data that
are integral to informing a precision medicine
approach.
Laboratory data and vital signs continue to
serve as crucial data points. These data provide
temporally important insights; for example,
blood work can evaluate the status of a
biomarker to aid in diagnosis or prognosis of
a disease.
With the advent of NGS, genetic analyses can
have increasing impact on precision medicine;
NGS can simultaneously target hundreds of
genes that are known to be important for a
disease (Roychowdhury, 2016). The genetic
testing firm Concert Genetics estimates that
there are more than 65,000 genetic testing
products available on the market, with 10 new
products introduced per day. As additional
genetic data are verified, this will allow for
the definition of more precise stratification
of patient subsets and better assessments of
interactions between genotypes and clinical
phenotypes derived from biobank data (Azimi,
2016). New high-quality genome assemblies
are increasingly offering ethnicity-specific
reference sequences that can be used to
improve precision medicine studies in certain
populations, such as Asians (e.g., Seo, 2016;
Qiao, 2016; Shi, 2016).
Imaging data are a medically rich source that
can also be a resource-intense burden. Much
of the available technology is unable to analyze
these data effectively without careful deep
learning or neural network techniques (Dinov,
2016; Geraci, 2017). Continual advances in this
realm are generating new ways to use technol-
ogy to evaluate and even interpret images.
In histology, for instance, much of the routine
work of diagnosis follows algorithmic decision
trees. Recent studies have reported success in
using deep learning to increase the accuracy
and efficiency of histopathological diagnoses
(Djuric, 2017; Litjens, 2016). In another example,
deep convolutional neural networks were
shown to have potential for general and highly
variable tasks across many fine-grained object
categories: investigators demonstrated artificial
intelligence (AI) to be capable of classifying
skin cancer with a level of competence
comparable to dermatologists (Esteva, 2017).
Digital biomarkers represent a valuable stream
of citizen-generated data from sensors
embedded in a variety of devices (e.g.,
wearables, implantables, and smartphones).
These digital biomarkers can play a vital role
55
PR
EC
ISIO
N T
OO
LS

56
in helping to identify more precise subsets
of patients, based on their ability to provide
longitudinal data in on a real-world setting (as
opposed to a single snapshot in time in
a doctor’s office). More advanced intuitive
designs in microelectromechanical systems
are providing researchers with abundant data
to aid the precision medicine efforts for a
variety of phenotypes of interest (Redmond,
2014). In addition to health-related data, a
variety of behavioral and social data can also
be used to explore social networks and social
determinants of health for patient outcomes.
Prior to initiating a precision medicine trial,
sponsors must develop their study designs
based on the types of data that will be
collected. Sponsors must also be prepared to
address data quality deficiencies that result
from aggregating disparate data sources with
varying degrees of structure, and they must
be able to integrate data quality assessment
functionality to ensure the ongoing validity
and reproducibility of findings. Developments
in AI are expected to make data collection and
integration even more efficient in the near
future. For example, AI is actively being used
in the form of chatbots for patient triage (e.g.,
Microsoft’s Health bot), and this technology is
also being explored to support the burdensome
process of creating clinical notes and pheno-
typing disease (Deliberato, 2017; Geraci, 2017).
As data streams become increasingly structured
and streamed in real time, the precision
medicine approach will become even more
efficient and accelerated.
3.2. Adaptive and Iterative Study Design
and Execution as New Information is Made
Available
Precision medicine studies must offer
investigators the capability to adapt study
designs throughout the life cycle of the study,
based on newly added information or
newly discovered relationships in the data.
The precision medicine approach is initially
exploratory, and it requires iteration to
redefine patient clusters into more precise
subsets and to redesign studies to enable
refined hypothesis testing.
Investigators must find the right balance
of the number of initial hypotheses that
will be tested (i.e., exploratory analyses),
since too many hypotheses can be viewed
as unfavorable and lacking a defined research
objective. Likewise, too many post hoc
analyses constitute data dredging. While,
understanding causal relationships in data
to surface actionable insights that are truly
governing improvements can have a significant
impact. There is a need to use appropriate
methods, avoiding model misspecifications,
and careful selection of data to avoid issues
of endogeneity, which can manifest from rate
dependence or state dependence.
Methodological innovations in trial design
include the ability to evaluate multiple
treatments in more than one patient type or
disease within the same overall trial structure
(Woodcock, 2017). The key to this approach
is to generate a master protocol, a single
overarching protocol designed to answer
multiple questions (e.g., studies involving
multiple drugs and/or diseases) and to enable
the use of “innovative statistical approaches to
study designs and analysis, enabling a broader
set of objectives to be met more effectively
than would be possible in independent trials”
(Woodcock, 2017). The master protocol can
accommodate different clinical trial designs,
including umbrella, basket, and platform trials
(Woodcock, 2017).
Key tasks in designing a precision
medicine study:
l Generate the protocol — establish solid
scientific foundation for predictive
precision medicine trial via pre-protocol
literature research to derive several initial
hypotheses to be tested (may result in
generating a new master protocol or
capitalizing on existing trial infrastructures).
l Plan adequately for the complex trial
designs and real-time decision making that
is the foundation of precision medicine
trials, including a basis for decisions about
treatments to pursue and those to
discontinue.
l Consider a wide array of data types and
depth to be measured, based on the range
of relevant factors and outcomes.
l Construct the infrastructure required to
handle data flow, data quality, data sharing,
trial logistics, and real-time ability to analyze
trial data and redesign trials according to
new information.
l Evaluate innovative methods for analyses
and recognize the care required to interpret
results.
After the study objectives and measurable
outcomes have been finalized in the
protocol, downstream analyses may
leverage some of these clinical trial
designs:
l Longitudinal cohort studies: Precision
medicine cohorts can be created to
evaluate the relationships between genotype
and phenotype over time, such as the NIH
sponsored program All of Us (Collins, 2015;
National Institutes of Health, 2017).

l Basket trials: Enable a larger recruitment
pool, since this design tests whether a drug is
effective in patients characterized by a single
genetic alteration and whether patients may
have tumors of different histologic types and
tissue of origin (Simon, 2017; Redig, 2015;
American Society of Clinical Oncology, 2017).
For instance, the National Cancer Institute
Molecular Analysis for Therapy Choice
(NCI-Match) is a Phase II clinical trial in
which patients who share a common genetic
mutation for a given cancer are sorted into
“baskets,” or treatment arms, regardless of
cancer type.
l Umbrella trials: Assign patients to a
particular treatment arm based on their
cancer type and genetic marker. This design
can have many treatment arms. The Lung
Master Protocol (Lung-MAP) study aims to
rapidly identify drug therapies for particular
cancer types, making it a useful design for
cancers with wide genetic heterogeneity
(Woodcock, 2017).
l N-of-1 studies: In these trials, which are
often used in evaluation of musculoskeletal
or pulmonary conditions, a patient serves
as both control and experimental treatment.
Although seemingly counterintuitive to the
goal of precision medicine, which typically
harnesses large amounts of data, this design is
especially useful for low-frequency, rare
conditions (Schork, 2015; Duan, 2013; Lillie,
2011).
l Adaptive trials: Investigators can adapt study
goals based on emerging data, thus provoking
a revision of hypotheses to be tested
(Heckman-Stoddard, 2014). Treatment arms
can be altered or biomarker strategies adjusted
depending on drug efficacy data (Woodcock,
2017). This paradigm is potentially conducive
to more rapid drug approvals for precision
medicine (Printz, 2013).
Figure: Schematic highlighting the flow of umbrella and basket trials (Redrawn from Woodcock, 2017).
57
PR
EC
ISIO
N T
OO
LS
59
PR
EC
ISIO
N T
OO
LS
The precision medicine approach requires
rigorous pre-trial discussion between sponsors,
clinical trial management firms, and the
governing regulatory agency to ensure
alignment with the protocol; therapeutic
approaches that will be tested to improve
patient outcomes; and timing of regulatory
submission filing (Woodcock, 2017;
Schwaederle, 2015).
Precision medicine trials necessitate a steadfast
approach with considerable advance planning,
because the protocols and trial designs can be
quite complex.
3.3. Maintenance and Management of
Data Throughout the Study Life Cycle
The complexities underlying precision
medicine trials require substantial planning
for data maintenance and management over
the entire life cycle of the study. The highly
adaptive nature of precision medicine trials
demands that high-quality data be maintained
throughout the trial.
“The use of a single system for clinical data management will enable shorter start-up times as the protocol is expanded to incorporate new investigations. The use of a single central randomization system facilitates the addition of new therapies with minimal disruption. Real-time access to the genomic, proteomic, pathological, and imaging data streams is requisite for the adaptive features of I-S P Y 2 [Neoadjuvant and Personalized Adaptive Novel Agents to Treat Breast Cancer].”(Woodcock, 2017)
The infrastructure for logistical efficiencies
that establish optimal data quality is a
necessary component for the success of a
precision medicine trial. Engaging in early
discussions with experts in clinical trial
technologies can help establish the trajectory
for success.
3.4. Advanced Analytics for Research
Discovery During the Study and Post-study
Precision medicine trials rely heavily on
clinicians and researchers to consider emerging
data in new ways and to develop innovative
strategies to fully leverage the massive body
of data generated.
Promoting high-quality data relies on stringent,
consistently applied definitions of data quality
as well as quality assurance and control
procedures to ensure the validity of the
incoming data and reproducibility of results.
Data standards should be maintained to assess
quality on a variety of dimensions (Kahn, 2016;
Weiskopf, 2013). The breadth of information
generated in precision medicine often warrants
the development of procedures and statistical
models and algorithms to ensure rapid and
uninterrupted data flow (Woodcock, 2017;
Garraway, 2013).
60
“The collection and processing of biomarker samples is extremely important to the integrity and validity of the genetic data used in a precision medicine trial. Optimized clinical trial
technologies use a combination of risk indicators and advanced pattern detection, to identify sites that may be lacking in the
collection and processing of samples according to defined protocol procedures. The faster any quality issue with
biomarker samples can be identified, the faster mitigation strategies can be deployed.”
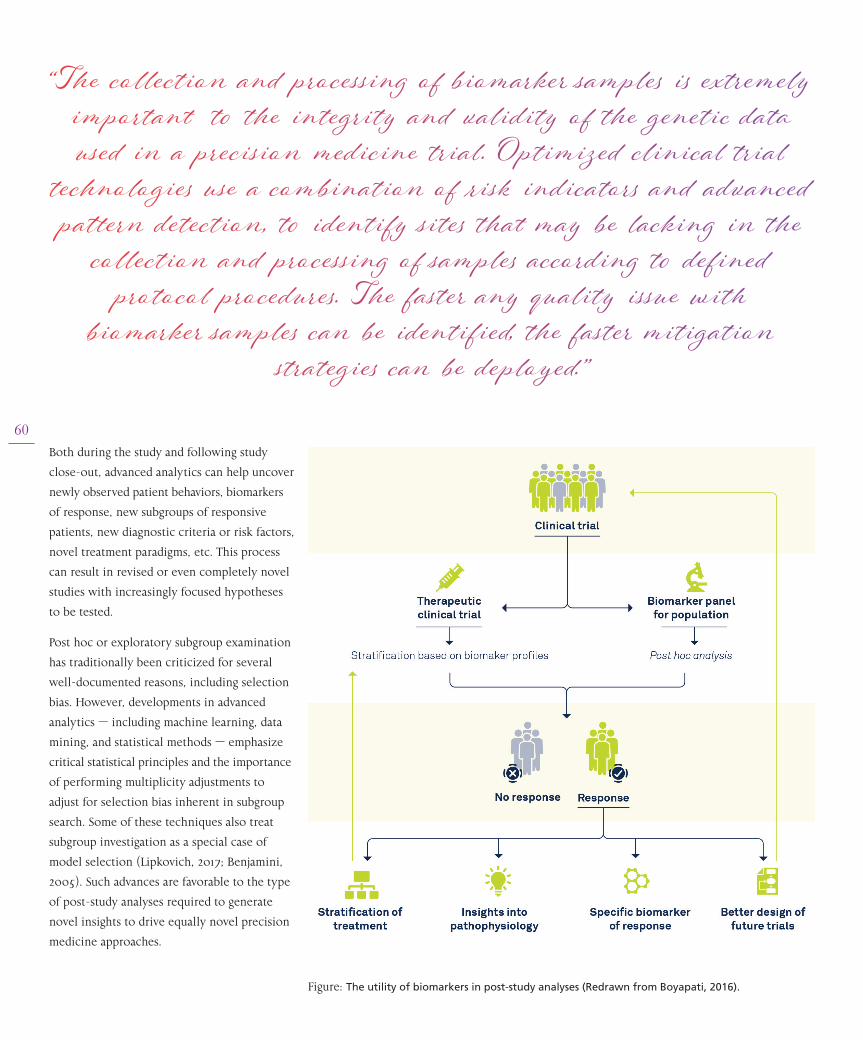
Both during the study and following study
close-out, advanced analytics can help uncover
newly observed patient behaviors, biomarkers
of response, new subgroups of responsive
patients, new diagnostic criteria or risk factors,
novel treatment paradigms, etc. This process
can result in revised or even completely novel
studies with increasingly focused hypotheses
to be tested.
Post hoc or exploratory subgroup examination
has traditionally been criticized for several
well-documented reasons, including selection
bias. However, developments in advanced
analytics — including machine learning, data
mining, and statistical methods — emphasize
critical statistical principles and the importance
of performing multiplicity adjustments to
adjust for selection bias inherent in subgroup
search. Some of these techniques also treat
subgroup investigation as a special case of
model selection (Lipkovich, 2017; Benjamini,
2005). Such advances are favorable to the type
of post-study analyses required to generate
novel insights to drive equally novel precision
medicine approaches.
Figure: The utility of biomarkers in post-study analyses (Redrawn from Boyapati, 2016).
62
“Machine learning algorithms have invigorated post-study analyses by minimizing biases while allowing
for novel insights that can be subsequently tested in a prospective trial.”
In planning a precision medicine trial, proper
consideration must be given to the clinical
development software platform that will be
used for post-study analytics. The software
should be user-friendly and integrated with
the existing trial infrastructure, to provide
for seamless workflows and to avoid the hefty
costs and extra work required to integrate
disparate solutions and adjusting to the various
environments.
4. Summary
Precision medicine is positioned to revolutionize
the healthcare landscape, and the utilization
of advanced clinical development technologies
is key to supporting precision medicine trials.
These technologies can harness a variety of
disparate data sources at richer and greater
volumes to build more accurate predictive
models for different patient subsets.
As the number of data streams increases across
the continuum of clinical care, the promise
is that precision medicines will become
increasingly targeted. However, the complexities
associated with evolving study designs are
substantial, and the precision medicine
approach demands solid planning, investment,
and commitment from all stakeholders.
An integrative platform should be designed
to house the clinical data; streamline
standardized workflow in data collection,
analysis, and iterative hypothesis testing; and
provide a satisfactory clinical user experience.
Our need to evaluate exploratory hypothesis
testing requires the thoughtful construction
of innovative clinical trials that are adaptive
to data generated in real time. A platform that
allows an iterative research process increases
the likelihood of success for sponsors
embarking on a precision medicine approach.
The promise of safer, more effective treatments
through targeting of specific patient subgroups
with the most advantageous benefit-risk profile
is what propels researchers on the precision
medicine journey.
References
American Society of Clinical Oncology, 2017. Clinical Trial Design and Methodology. [Online] Available at: https://www.asco.org/research-progress/clinical-trials/clini-cal-trial-resources/clinical-trial-design-and-methodology [Accessed August 24 2017].Anderson, V. H., Weintraub, W. S., Radfod, M. J., Kremers, M. S., Roe, M. T., Shaw, R. E., … Tcheng, J. E. (2014). Standardized Cardiovascular Data for Clinical Research, Registries, and Patient Care: A Report from the Data Stand-ards Workgroup of the National Cardiovascular Research Infrastructure Project. A collaboration of the Duke Clinical Research Institute and th, 61(18), 1835–1846. https://doi.org/10.1016/j.jacc.2012.12.047.StandardizedAzimi, M., Schmaus, K., Greger, V., Neitzel, D., Rochelle, R., & Dinh, T. (2016). Carrier screening by next-generation se-quencing: health benefits and cost effectiveness. Molecular Genetics & Genomic Medicine, 4(3), 292–302. https://doi.org/10.1002/mgg3.204Bartlett, J. M. S., & Parelukar, W. (2017). Breast cancers are rare diseases—and must be treated as such. NPJ Breast Cancer, 3, 11. https://doi.org/10.1038/s41523-017-0013-yBeckmann, J. S., & Lew, D. (2016). Reconciling evi-dence-based medicine and precision medicine in the era of big data: challenges and opportunities. Genome Medicine, 8, 134. https://doi.org/10.1186/s13073-016-0388-7Benjamini, Y., & Leshno, M. (2005). Statistical methods for data mining. In Data Mining and Knowledge Discovery Handbook (pp. 565-587). Springer US.Boyapati, R. K., Kalla, R., Satsangi, J., & Ho, G. T. (2016). Biomarkers in search of precision medicine in IBD. The American journal of gastroenterology, 111(12), 1682-1690.Buzuk, G., Lojko, D., Ow, M., & Ru, M. (2016). Depression with atypical features in various types of affective disor-ders, 50(4), 827–838.Collins, F. S., & Varmus, H. (2015). A New Initiative on Pre-cision Medicine. New England Journal of Medicine, 372(9), 793–795. https://doi.org/10.1056/NEJMp1500523Deliberato, O. R., Celi, A. L., & Stone, J. D. Clinical Note Creation, Binning, and Artificial Intelligence. JMIR Med Inform, 5(3), e24. https://doi.org/10.2196/medinform.7627Dinov, I. D. (2016). Methodological challenges and analytic opportunities for modeling and interpreting Big Healthcare Data. GigaScience, 5(1), 12. https://doi.org/10.1186/s13742-016-0117-6Djuric, U., Zadeh, G., Aldape, K., & Diamandis, P. (2017). Precision histology: how deep learning is poised to revi-talize histomorphology for personalized cancer care. npj Precision Oncology (Vol. 1). https://doi.org/10.1038/s41698-017-0022-1Duan, N., Kravitz, R. L., & Schmid, C. H. (2013). Single-pa-tient (n-of-1) trials: a pragmatic clinical decision meth-odology for patient-centered comparative effectiveness research. Journal of clinical epidemiology, 66(8), S21-S28. Dumitrescu, L., Ritchie, M. D., Denny, J. C., El Rouby, N. M., McDonough, C. W., Bradford, Y., … Crawford, D. C. (2017). Genome-wide study of resistant hypertensionidentified from electronic health records. PLoS ONE, 12(2), e0171745. https://doi.org/10.1371/journal.pone.0171745Esteva, A., Kuprel, B., Novoa, R. A., Ko, J., Swetter, S. M., Blau, H. M., & Thrun, S. (2017). Dermatologist-level classification of skin cancer with deep neural networks. Nature,542(7639), 115–118. https://doi.org/10.1038/nature21056Evans, R. S. (2016). Electronic Health Records: Then, Now, and in the Future. Yearbook of Medical Informatics, Suppl 1, S48-61. https://doi.org/10.15265/IYS-2016-s006
FDA. (2010). Guidance for Industry Adaptive Design Clin-ical Trials Guidance for Industry Adaptive Design Clinical Trials. Available at: https://www.fda.gov/downloads/drugs/guidances/ucm201790.pdf FDA. (2016). Precision Medicine Initiative. [Online] Availa-ble at: https://www.fda.gov/scienceresearch/specialtopics/precisionmedicine/default.htm [Accessed August 22 2017].Field, D., & Sansone, S. (2006). A Special Issue on Data Standards. OMICS: A Journal of Integrative Biology, 10(2), 84–93.Ford, E., Carroll, J. A., Smith, H. E., Scott, D., & Cassell, J. A. (2016). Extracting information from the text of electron-ic medical records to improve case detection: a systematic review. Journal of the American Medical Informatics Asso-ciation : JAMIA, 23(5), 1007–1015. https://doi.org/10.1093/jamia/ocv180Garraway, L. A., Verweij, J., & Ballman, K. V. (2013). Preci-sion Oncology: An Overview. Journal of Clinical Oncology, 31(15), 1803–1805. https://doi.org/10.1200/JCO.2013.49.4799Geraci, J., Wilansky, P., de Luca, V., Roy, A., Kennedy, J. L., & Strauss, J. (2017). Applying deep neural networks to unstructured text notes in electronic medical records for phenotyping youth depression. Evidence-Based Mental Health. https://doi.org/10.1136/eb-2017-102688Godet, I., & Gilkes, D. M. (2017). BRCA1 and BRCA2 muta-tions and treatment strategies for breast cancer. Integrative cancer science and therapeutics, 4(1). Heckman-Stoddard, B. M., & Smith, J. J. (2014). Precision medicine clinical trials: defining new treatment strategies. Seminars in Oncology Nursing, 30(2), 109–116. https://doi.org/10.1016/j.soncn.2014.03.004Kahn, M. G., Callahan, T. J., Barnard, J., Bauck, A. E., Brown, J., Davidson, B. N., ... & Liaw, S. T. (2016). A harmonized data quality assessment terminology and framework for the secondary use of electronic health record data. eGEMs, 4(1).Lillie, E. O., Patay, B., Diamant, J., Issell, B., Topol, E. J., & Schork, N. J. (2011). The n-of-1 clinical trial: the ultimate strategy for individualizing medicine?. Personalized medi-cine, 8(2), 161-173.Lipkovich, I., & Dmitrienko, A. (2017). Tutorial in biosta-tistics: data‐driven subgroup identification and analysis in clinical trials. Statistics in medicine, 36(1), 136-196. Litjens, G., Sánchez, C. I., Timofeeva, N., Hermsen, M., Nagtegaal, I., Kovacs, I., … van der Laak, J. (2016). Deep learning as a tool for increased accuracy and efficiency of histopathological diagnosis, 6, 26286. Retrieved from http://dx.doi.org/10.1038/srep26286Marchina, E., Fontana, M. G., Speziani, M., Salvi, A., Ricca, G., Di Lorenzo, D., … Barlati, S. (2010). BRCA1 and BRCA2 genetic test in high risk patients and families: counselling and management. Oncology Reports, 24(6), 1661–1667.Mansfield, E. Precision Medicine at the FDA [PDF docu-ment]. Retrieved from FDA Web site available at: https://www.fda.gov/downloads/advisorycommittees/commit-teesmeetingmaterials/scienceboardtothefoodanddrugad-ministration/ucm473506.pdf McIntyre, R. S. (2016). Implementing treatment strategies for different types of depression. The Journal of Clinical Psychiatry, 77 Suppl 1, 9–15. https://doi.org/10.4088/JCP.14077su1c.02Mead, C. N. (2006). Data interchange standards in health-care IT--computable semantic interoperability: now possi-ble but still difficult, do we really need a better mousetrap? Journal of Healthcare Information Management : JHIM, 20(1), 71–78.

National Academies of Science. (2017). EnabliNational Insti-tutes of Health, 2017. All of Us. [Online] Available at: https://allofus.nih.gov/ [Accessed August 23, 2017].Phillips, K. A., Deverka, P. A., Sox, H. C., Khoury, M. J., Sandy, L. G., Ginsburg, G. S., … Douglas, M. P. (2017). Making genomic medicine evidence-based and patient- centered : a structured review and landscape analysis of comparative effec-tiveness research, (April). https://doi.org/10.1038/gim.2017.21Printz, C. (2013). I-SPY 2 may change how clinical trials are conducted. Cancer, 119(11), 1925–1927. https://doi.org/10.1002/cncr.28172Qiao, W., Yang, Y., Sebra, R., Mendiratta, G., Gaedigk, A., Desnick, R. J., & Scott, S. A. (2016). Long‐read single molecule real‐time full gene sequencing of cytochrome P450‐2D6. Human mutation, 37(3), 315-323.Redig, A. J., & Jänne, P. A. (2015). Basket Trials and the Evolu-tion of Clinical Trial Design in an Era of Genomic Medicine. Journal of Clinical Oncology, 33(9), 975–977. https://doi.org/10.1200/JCO.2014.59.8433ng Precision Medicine: The Role of Genetics in Clinical Drug Development: Proceedings of a Workshop. Washington (DC): The National Academies Press. https://doi.org/10.17226/24829National Human Genome Research Institute, 2016. New train-ing grants prime doctors to tackle genomic medicine. [Online] Available at: https://www.genome.gov/27565602/2016-news-feature-new-training-grants-prime-doctors-to-tackle-genom-ic-medicine/ [Accessed August 21, 2017].Redmond, S. J., Lovell, N. H., Yang, G. Z., Horsch, A., Lukow-icz, P., Murrugarra, L., & Marschollek, M. (2014). What Does Big Data Mean for Wearable Sensor Systems?: Contribution of the IMIA Wearable Sensors in Healthcare WG. Yearbook of Medical Informatics, 9(1), 135–142. https://doi.org/10.15265/IY-2014-0019Richesson, R. L., & Krischer, J. (2007). Data Standards in Clinical Research: Gaps, Overlaps, Challenges and Future Directions. Journal of the American Medical Informatics Asso-ciation, 14(6), 687–696. https://doi.org/10.1197/jamia.M2470Roychowdhury, S., & Chinnaiyan, A. M. (2016). Translating cancer genomes and transcriptomes for precision oncology. CA: a cancer journal for clinicians, 66(1), 75-88. Schork, N. J. (2015). Personalized medicine: time for one-person trials. Nature, 520(7549), 609-611.Schwaederle, M., Zhao, M., Lee, J. J., Eggermont, A. M., Schilsky, R. L., Mendelsohn, J., … Kurzrock, R. (2015). Impact of Precision Medicine in Diverse Cancers: A Meta-Analysis of Phase II Clinical Trials. Journal of Clinical Oncology, 33(32), 3817–3825. https://doi.org/10.1200/JCO.2015.61.5997Seo JS, Rhie A, Kim J, Lee S, Sohn MH, Kim CU, …, Kim C. (2016). De novo assembly and phasing of a Korean human genome. Nature. Oct 13;538(7624):243-247.Shi, L., Guo, Y., Dong, C., Huddleston, J., Yang, H., Han, X., ... & Lintner, K. E. (2016). Long-read sequencing and de novo assembly of a Chinese genome. Nature communications, 7. Simon, R. (2017). Clinical Trials in Precision Medicine. In Verma, M. & Barh, D. Editors, Progress and Challenges in Precision Medicine (209-2015). New York: Elsevier.Slamon, D. J., Leyland-Jones, B., Shak, S., Fuchs, H., Paton, V., Bajamonde, A., … Norton, L. (2001). Use of Chemotherapy plus a Monoclonal Antibody against HER2 for Metastatic Breast Cancer That Overexpresses HER2. New England Journal of Medicine, 344(11), 783–792. https://doi.org/10.1056/NEJM200103153441101Strawbridge, R., Young, A. H., & Cleare, A. J. (2017). Biomark-ers for depression: recent insights, current challenges and future prospects. Neuropsychiatric Disease and Treatment, 13, 1245–1262. https://doi.org/10.2147/NDT.S114542Szlosek, D. A., & Ferrett, J. (2016). Using Machine Learning and Natural Language Processing Algorithms to Automate the Evaluation of Clinical Decision Support in Electronic Medical Record Systems. eGEMs, 4(3), 1222. https://doi.org/10.13063/2327-9214.1222Torkamani, A., Andersen, K. G., Steinhubl, S. R., & Topol, E. J. (2017). High-Definition Medicine. Cell, 170(5), 828-843.Woodcock, J., & LaVange, L. M. (2017). Master Protocols to Study Multiple Therapies, Multiple Diseases, or Both. New England Journal of Medicine, 377(1), 62-70. http:// 10.1056/NEJMra1510062Yue, Y., Jiang, H., Yin, Y., Zhang, Y., Liang, J., Li, S., … Yuan, Y. (2016). The Role of Neuropeptide Y mRNA Expression Level in Distinguishing Different Types of Depression. Frontiers in Aging Neuroscience, 8, 323. https://doi.org/10.3389/fnagi.2016.00323
Steven Schwager, PhD, is a Research Principal in the
Data Science group at Medidata Solutions and a Professor
Emeritus of Statistics and Biological Statistics at Cornell
University. He joined the faculty at Cornell after earning
his PhD in statistics at Yale University. His research
includes statistical methodology and theory and
collaborative projects in a wide range of biological
and physical sciences and other fields. He works at
Medidata on developing statistical and analytical
methods for improving the design, execution, and
analysis of clinical trials, including Clinical Trial
Genomics, operational analytics, and synthetic control
arms.
Jeffery Wiser, recently joined Medidata as Genomics
Portfolio Director to grow the new Clinical Trial Genomics
(CTG) product. Jeff has spent his 20 year career leading
the development of life sciences software with a focus
on the integration of clinical and ‘omics’ data. For the
last 10 years, he has served as the Program Manager or
Co-Investigator on multiple National Institute of Health
funded projects, most notably the ImmPort project, a
public/private partnership with UCSF and Stanford
University. ImmPort serves as a repository for the
collection, QC, curation and sharing of clinical and
mechanistic assay results generated by researchers
funded by the National Institute of Allergy and Infectious
Diseases (NIAID), and was recently designated a Nature
Scientific Data recommended repository for immunology
and cytometry. Previously, Jeff served for 9 years in
management roles at Gene Logic Inc. building clinical
data capture, biobanking, LIMS, and gene expression
analysis software for what was at the time the largest
microarray gene expression database in the world. He
holds a MSE from the Unversity of Pennsylvania in
Bioengineering and a BS from Cornell University in
Mechanical Engineering.
Therese Dolan is a Global Marketing Director
overseeing Precision Medicine and Study Conduct
for Medidata Solutions. She joined Medidata after
spending most of her 20 year career in Life Sciences
working in global marketing for the Commercial and
the Licensing Divisions for Merck & Co. Therese has
had the opportunity to work with some of the leading
scientific experts in the field for multiple disease states
discussing the future state of science in terms of study
and treatment, which often included some strand of
what has now become the topic of Precision Medicine.
The passion behind these discussions have carried
forward as Therese works towards supporting the
industry in achieving its vision of Precision Medicine
through use of technology for clinical trials.
Ruthie Davi, PhD. has worked in the area of
pharmaceutical product development, and specifically
the FDA, over 20 years. In her current position as a
Director in Data Science at Medidata Solutions , she
is part of a team focused on providing centralized
systematic monitoring and other novel clinical trial
tools. Ruthie has held numerous positions within the
FDA, including Statistical Reviewer, Team Leader, and
Deputy Director, where she implemented innovative
statistical methods and made recommendations for
clinical trial designs tailored to the regulatory setting.
She has conducted the statistical review, represented
the Agency at Advisory Committee meetings, and
provided recommendations regarding FDA marketing
approval for numerous New Drug and Biologic Licensing
Applications. With a particular interest in pediatric
clinical trials, she was an active member of FDA’s
Pediatric Review Committee. Ruthie holds a Ph.D. in
biostatistics from George Washington University.
63
PR
EC
ISIO
N T
OO
LS





























