Embed Size (px)
Citation preview

Clinical StudySingle Ascending Dose Safety and Pharmacokinetics ofCDRI-9778 First-in-Human Study of a Novel Antimalarial Drug
N Shafiq1 S Rajagopalan1 H N Kushwaha2 N Mittal1 N Chandurkar3
A Bhalla4 S Kaur1 P Pandhi1 G D Puri5 S Achuthan1 A Pareek3 S K Singh2
J S Srivastava6 S P S Gaur6 and S Malhotra1
1 Department of Pharmacology PGIMER Chandigarh India2 Pharmacokinetics and Metabolism Division Central Drug Research Institute Lucknow India3 IPCA Laboratories Ltd Mumbai Maharashtra India4Department of Internal Medicine PGIMER Chandigarh India5 Department of Anaesthesia Incharge Critical Care PGIMER Chandigarh India6Clinical and Experimental Medicine Central Drug research Institute Lucknow India
Correspondence should be addressed to S Malhotra samirmalhotra345yahoocom
Received 14 November 2013 Revised 13 January 2014 Accepted 17 January 2014 Published 27 March 2014
Academic Editor Neena Valecha
Copyright copy 2014 N Shafiq et alThis is an open access article distributed under the Creative CommonsAttribution License whichpermits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
Background CDRI 9778 has shown efficacy in animal models of falciparummalaria The present study is the first in-human phaseI trial in healthy volunteersMethods The study was conducted in 50 healthy volunteers in a single ascending dose randomizedplacebo-controlled double blind design The dose ranges evaluated were from 80mg to 700mg Volunteers were assessed forclinical biochemical haematological radiographic and electrocardiographic parameters for any adverse events in an in-housefacility After evaluation of safety study results another cohort of 16 participantswere administered a single oral dose of 200mgof thedrug and a detailed pharmacokinetic analysis was undertakenResultsThe compoundwas found to be well toleratedMTDwas notreachedThe few adverse events noted were of grade 2 severity not requiring intervention and not showing any dose response rela-tionshipThe laboratory and electrocardiographic parameters showed statistically significant differences but all werewithin the pre-defined normal rangeThese parameters were not associated with symptomssigns and hence regarded as clinically irrelevantMeanvalues of T
12 MRT and AUC
0minusinfinof the active metabolite 9763 were 1185 plusmn 194 h 1377 plusmn 205 h and 87874 plusmn 13315 ngsdot hmL
respectively Conclusion The novel 124 trioxane CDRI 9778 is safe and will be an asset in malarial therapy if results are replicatedin multiple dose studies and benefit is shown in confirmatory trials
1 Introduction
The global burden of malaria can be estimated from the factthat nearly 107 countries and territories are at risk of malariatransmission and the annual worldwide cases of acute illnessdue to malaria are estimated to be around 300ndash500 million[1] In the Southeastern Asian Region of the World HealthOrganization (WHO) 12 billion are exposed to the risk ofmalaria most of whom live in India [2] In many regionsincluding India multidrug resistant P falciparum is one ofthe important causative strains of malaria Falciparum mal-aria which was traditionally effectively treated by chloro-quine now commonly shows resistance to the drug [3] Till
date progress in malaria therapy has been made using theendoperoxide sesquiterpene artemisinin and its derivativeslike arteether artemether artesunate and so forthTheWorldHealth Organization (WHO) recommended artemisininbased therapies as first line of therapy for falciparummalaria[3 4]
A novel trioxane 9778 developed by Central DrugResearch Institute (CDRI) India has shown promisingantimalarial activity and is currently in clinical trials phase I9778 contains 124-trioxane nucleus similar to artemisininresponsible for their pharmacological activity [5ndash9](Figure 1) During the last 10 years antimalarials based oninhibition of plasmodial phospholipid metabolism were
Hindawi Publishing CorporationMalaria Research and TreatmentVolume 2014 Article ID 372521 10 pageshttpdxdoiorg1011552014372521
2 Malaria Research and Treatment
O
OO
OO
O
O
O
OO
OHO
HO
O
OHH
HO
O
H
97ndash78 parent compound
97ndash63 metabolite
CH3
CH3
H3C
OC2H5
IS (120572-Arteether)
Figure 1 Chemical structure of parent compound 9778 in vivoactive metabolites 9763 and IS (120572-arteether)
identified and developed by CDRI groups [5ndash8 10ndash17] Manycompounds have shown high efficacy against multidrugresistant Plasmodium falciparum strains [6 12 13 15 17] But9778 emerged as lead compound for excellent pharma-cological activity in both in vitro and in vivomalarial modelsAfter successful completion of regulatory preclinical studiescompound is currently in phase I clinical trials [18 19]
Potent antimalarial activity of these compounds may bedue to its capacity (i) to mimic the choline structure whichblocks phosphatidylcholine biosynthesis and (ii) to interactwith hemozoin the malarial hemoglobin-degradation pro-duct Compounds potency is also due to its high accumula-tion inside the infected erythrocytes This dual mechanismof action of 9778 should limit the risk of emergence ofresistance The chemical name of the compound isMono[2methyl2[3(1spiro[tricycle[331137]decane231015840-[1 24]trioxan] 61015840-yle thenyl) phenoxy] propyl] ester It has power-ful antimalarial activity against chloroquine resistant Pfalciparum in vitro chloroquine sensitive P berghei and mul-tidrug resistant P yoelii in mice and P cynomolgi in rhesusmonkeys It has been developed as a synthetic substitute forantimalarial peroxide artemisinin and its derivatives such asartemether arteether and artesunic acid The CDRI com-pound 9778 is effective by oral and intravenous routes andtherefore can be used by either route
Firstly 9763 was synthesized but due to its poor bioavail-ability it was resynthesized as a hemisuccinate derivative andcoded as 9778 Upon administration of 9778 it gets con-verted into its active in vivo metabolite 9763 The concen-trations of 9763 and 9778 can be measured by validatedLC-MSMS method [19] The preclinical testing for thiscompound included pharmacokinetic (PK) studies animal
pharmacology and toxicology male fertility studies femalereproduction and development toxicity studies and genotox-icity studies and the compound was taken up for evaluationin phase I study as it lacked any remarkable toxicity concernsin animal studies
The aim of this study was to calculate the maximumtolerated dose of the compound in healthy human volunteersalong with evaluation of PK profiles of 9778 and its in vivometabolite 9763 after oral administrations of 9778
2 Subjects and Methods
21 Subjects The study was approved by the Institutersquos EthicsCommitteeThe single ascending dose study and the pharma-cokinetic study are registered with Central Trial Registry ofIndia (CTRI201207002812 CTRI201207002832) Nor-mal healthy male volunteers in the age group of 18ndash45 yearswere invited to join the trial A detailed informed consentprocess of the volunteerswas undertaken and screening of thevolunteers was done after obtaining informed consent Theywere recruited through contacts and hospital employees wereexcluded The health status of the volunteers was determinedby taking medical history physical examination routinehaematology (haemoglobin total lymphocyte count differ-ential count and platelet count) clinical biochemistry (serumglutamic oxaloacetic transaminase (SGOT) serum glutamicpyruvic transaminase (SGPT) serum bilirubin serum crea-tinine blood urea serum electrolytes random blood sugartotal protein and serum lipid profile) and urine and stoolanalysis (routine examination and microscopy) The volun-teers were asked to report to the study site after 12 hours offasting for the blood tests Chest X-ray and 12-lead ECGwerealso taken The participants were also screened for humanimmunodeficiency virus (HIV) and hepatitis B
The volunteers were excluded if there was a history ofhaving donated blood in the past 3 months HIV or HBsAgpositivity history of any drug intake in the past 15 days his-tory of receiving any enzyme-inducing agent in the preceding15 days history of participating in any investigational newdrug (IND) study in the previous 6 months history of par-ticipating in any non-IND study in the preceding 3 monthshistory of allergy or hypersensitivity to any medication his-tory of peptic disorder chronic smoker gt6 cigarettesbeediesper day alcoholic (history of daily alcohol intake in the last 6months) history of any drug abuse tobacco user in any formhistory of any chronic disease and taking medication andhistory of taking nonallopathic drug in the past 6 months forany illness or history of any major illness in the past (namelymeningitis hepatitis tuberculosis epilepsy nephritis havingreceived treatment and presently asymptomatic)
The procedure for recruiting participants for single dosePK study was similar to the above The PK study was under-taken in 16 separate volunteers following the evaluation ofsafety data for phase I study and evaluation of pharmacody-namics study in animals
22 Design This was a single ascending dose placebo-controlled randomized double blind trial Randomization
Malaria Research and Treatment 3
was carried out by computer generated random numbersequence Randomization was carried out for the drug andthe placebo in a 3 1 ratio for each dose level The drugs weredispensed in sealed bottles with the randomization codewrit-ten on them Randomization codes were provided in sealedopaque envelopes with the protocol specification that thecodes may be opened by the investigator only in case of aserious or severe adverse event
23 Starting Dose and Dose Escalation The starting dose was80mg calculation of starting dose was based on the basis ofmaximum tolerated dose of 100mgkg obtained in rats Thiswas used to obtain a dose of 96mg for a 60 kg man The for-mulation which was available for a dose below this was of80mg and hence taking these factors into consideration astarting dose of 80mg was chosen The following dose levelswere evaluated 80 160 320 400 500 600 and 700mg Thestarting dose was calculated by allometric scaling from ani-mals At each dose level six volunteers received CDRI 9778and two received placebo except at 700mg where only twovolunteers were given this dose At each dose level volunteerswere assessed before proceeding to the next dose The deci-sion to dose only 2 volunteers was taken after analysis of dataof 600mg wherein no remarkable adverse events were noted
24 Stopping Rule The decision to stop the dose escalationwas based on the appearance of the dose limiting toxicity(DLT) which was defined as the dose at which any of thefollowing appeared severe nausea vomiting heartburnheadache remarkable change in vital parameters such asblood pressure heart rate respiratory rate or oxygen satura-tion of blood changes in QT interval or any event that in theopinion of the investigators required stopping of the trial
Maximum tolerated dose was defined as the dose beforewhich any of the components of DLT appeared at a signifi-cantly higher rate as compared to placebo In case this was notachieved it was planned not to dose volunteers beyond700mg
25 Study Procedure The volunteers after giving informedconsent were screenedThe screening process was done latestwithin 1 month of admission for dosing The volunteers whofulfilled the inclusionexclusion criteria were admitted inthe CPU the night before drug administration Standardizeddinner was served at 9 pm the night prior to dosing On day0 baseline blood sample for biochemical and haematologicalexamination and stool and urine samples for routine andmicroscopywere takenThey received the study drug accord-ing to the randomization sequence under supervision Theempty packaging was returned to the container The volun-teers received drug as per randomization Breakfast was givenhalf an hour after drug administration Subsequently stan-dardized lunch and dinner were served to the volunteers
For pharmacokinetic (PK) study eligible participantswere admitted and housed in the clinical pharmacology unitan evening prior to the PK study A standard dinner wasserved and a fasting condition for at least 10 hrs prior todosing and 4 hrs after dosing was ensured A peripheral
forearm veinwas cannulated for sampling for the PK analysis200mg of the study drug was administered with 300mL ofwater The time of actual dose administration to the nearestminute was recorded 25mL of blood was collected from theindwelling cannula at 0 (before dose) 025 05 075 1 15 24 6 8 12 18 24 48 72 96 120 and 144 hrs (after dose) 10mLof additional blood was collected at 0 (before dose) and 24 hr(after dose) for laboratory parameters for safety assessmentand PK control sample A time window of plusmn2 minutes waspermitted for collecting the post dose samples from thescheduled time for PK analysis
Plasmawas separated from blood sample intended for PKanalysis within 1 hour of blood sampling by centrifugationat 2000 rpm for 10min at 4∘C Samples were stored at minus80∘Cpending transportation Heparinised blood samples weretransported to the laboratory within 7 days of collection
26 Subject Monitoring The subjects were attached to a car-diac monitor and vital HR BP ECG oxygen saturation andRR were recorded Corrected QT interval using Fridericiarsquosformula was calculated Adverse events were assessed atspecific time points (05 1 2 4 6 8 12 and 24 hrs after med-ication) Unscheduled monitoring was undertaken wheneverit felt necessary The volunteers were discharged after 24 hrsand they had to return at 48 hrs and on the 7th day for follow-up At the end of the 7th day theywere said to have completedthe study Routine haematological and biochemical investiga-tionswere performed at 0 hr 24 hrs after drug administrationand on day 7 The study was monitored by a Data SafetyMonitoring Board
27 Pharmacokinetic Analysis Quantitative analyses of clin-ical phase ascending dose and single dose PKs samples weredone at GLP lab of Pharmacokinetics and Metabolism Divi-sion CDRI Lucknow India 120572-Arteether was used as aninternal standard and all the analyses were performed as perthe published method by Singh et al 2009 [19] Acceptancecriteria for analytical runs were fixed as per internationallyapproved guidelines [20] Data acquisition and quantitationwere performed using analyst software version 14 (AppliedBiosystems MDS SCIEX Toronto Canada) PK parameterswere estimated by using WinNonlin software (Version 15Pharsight Corporation Mountain View CA) Oral datawere best fitted in noncompartmental model The individualplasma concentration-time profiles were subjected to non-compartmental analysis to determine various PK parametersThe PK parameters included the terminal elimination half-life (119879
12) maximum plasma concentration (119862max) time to
reachmaximum plasma concentration (119879max) area under thecurve (AUC
0ndashinfin) and mean residence time (MRT)
28 Statistical Analysis Continuous data were presented asmean plusmn SD and categorical data were presented as 119899 () Forcomparison between the drug and placebo at each dose levelunpaired 119905-test was used for continuous variables and Fis-cherrsquos exact test for categorical variables For comparisonbetween various dose levels ANOVAwas used 119875 value lt005was considered significant
4 Malaria Research and Treatment
Table 1 Demographic characteristics of the volunteers included in the studies
Characteristic 80mg 160mg 320mg 400mg 500mg 600mg 700mg Placebo119873 = 6 119873 = 6 119873 = 6 119873 = 6 119873 = 6 119873 = 6 119873 = 2 119873 = 12
Age in years Mean (SD) 285 (1093) 275 (432) 250 (712) 252 (213) 213 (353) 252 (767) 230 (141) 254 (575)Height in cm Mean (SD) 1705 (533) 1675 (58) 1667 (644) 1673 (408) 1670 (357) 1702 (577) 1710 (141) 1713 (489)Weight in kg Mean (SD) 586 (972) 690 (1357) 566 (884) 616 (717) 596 (647) 613 (1267) 635 (212) 607 (843)BMI (kgm2) Mean (SD) 201 (304) 248 (589) 203 (214) 220 (235) 214 (25) 217 (036) 207 (275) 214 (34)
Table 2 Adverse events noted at various drug dosages of CDRI9778
Treatment group Type of adverse events No of events80mg CDRI 9778 Heaviness of head 1160mg CDRI 9778 None320mg CDRI 9778 Visual disturbance 1
400mg CDRI 9778Drowsiness 1Bradycardia 1Itching 1
500mg CDRI 9778 Sedation 1Nausea 1
600 and 700mg CDRI 9778 Sedation 1
Placebo
Sedation 1Drowsiness 1Nausea 1Retching 1Dizziness 1
Heaviness of head 1
3 Results
63 volunteers were screened out of whom 50 volunteersmatched the inclusionexclusion criteria andwere included inthe safety study (Figure 2) For the PK study 16 healthy malevolunteers were included after screening of 20 volunteers Asrequired by the study protocol all the volunteers were male(Figure 2) There was no significant difference in the demo-graphic parameters like age (119875 = 07) height (119875 = 05)weight (119875 = 05) and body mass index (119875 = 03) amongparticipants in various treatment groups (Table 1)
31 Adverse Events Adverse events that occurred during thestudy were few (Table 2) and largely of severity grade 1 to 2(Table 2)There was no significant difference in the incidenceof events in the drug and the placebo groups (119875 = 043)
Sedation was the most common adverse event reportedacross different groups (314 214) It was noted in 3 vol-unteers given 500mg CDRI 9778 600mg CDRI 9778 andplacebo about 2 hours after drug administration and lastedfor 1-2 hours It was grade 1-2 in severity spontaneous andcomplete recoverywas seen in all and no actionwas requiredThe other adverse events noted were mild drowsiness mildnausea slight heaviness of head bradycardia (56-57 bpm)visual disturbances and itching (Table 3)
Severe adverse event nausea and retching immediatelyafter drug administration was observed in one patient whichlasted for 10minutes the patient also complained of dizzinessand slight heaviness of head 1 hour after drug administrationOn decoding he was found to have received placebo Thesymptoms resolved spontaneously hence no further actionneeded to be taken
32 Clinical Parameters At baseline the different treatmentgroups were similar in terms of clinical parameters (pulserate blood pressure and respiratory rate) None of the treat-ment groups demonstrated a significant alteration in pulserate respiratory rate and systolic blood pressure at any timepoint compared to baseline However there was a significantchange in diastolic blood pressure in 600 and 700mg CDRI9778 group (7687plusmn 874 7837plusmn 886 7925plusmn 1346 6712plusmn649 7312plusmn1232 7587plusmn811 74plusmn11 and 75plusmn1003mmHgat 0 05 1 2 4 6 8 and 12 hours respectively 119875 = 002)although clinically significant declinewas not observed in anyof the volunteers Statistical significance was observed forbetween group comparison of systolic and diastolic bloodpressures 2 hours after drug administration The SBP for80mg 160mg 320mg 400mg 500mg 600mg 700mgand placebo groups were 11217 plusmn 624 1195 plusmn 517 1275 plusmn638 11183plusmn791 1145plusmn834 11283plusmn618 1155plusmn212 and11633 plusmn 877 respectively (119875 = 001) The DBP for 80mg160mg 320mg 400mg 500mg 600mg 700mg andplacebo groups were 73 plusmn 521 7717 plusmn 806 8233 plusmn 4687133plusmn819 7183plusmn781 665plusmn653 69plusmn848 and 7375plusmn824(119875 = 003) Respiratory rate was found to be significantlydifferent between treatment groups 4 6 and 8 hours afterdrug administration although this was not clinically relevant
There was no statistically or clinically significant dif-ference noted in the corrected QT interval within varioustreatment groups (119875 = 0656 0523 0901 0348 0809 and043 respectively for 80 160 320 400 500 and 600700mggroups)
33 Hematological Parameters Hemoglobin values demon-strated a statistically significant alteration during posttreat-ment period in the group receiving 400mg CDRI 9778(1425 plusmn 075 1492 plusmn 094 and 1435 plusmn 110 gm at baseline24 hr and 7th day respectively 119875 = 002) A statistically sig-nificant change in platelet counts was also observed in 320mgCDRI 9778 group (190 plusmn 68 190 plusmn 69 and 212 plusmn 66(times1012)L respectively 119875 = 004) All these values were wellwithin normal limits Other haematological parameterswhich showed statistically significant difference however
Malaria Research and Treatment 5
Table3Descriptio
nof
alladverse
eventsob
served
inthes
tudy
Nam
eofA
ETreatm
entg
roup
Treatm
entg
iven
Time(hrs)of
onset
after
drug
administratio
n
Durationof
AE
(min)
Spon
taneou
sreversal(yes
orno
)Re
versalcomplete
(yes
orno
)Severitygrade
Causalityassessment
Sedatio
n60
0mg
Non
e2
60Yes
Yes
1-2Po
ssible
Sedatio
n500mg
Non
e2
120
Yes
Yes
1-2Po
ssible
Sedatio
nPlacebo
Non
e2
120
Yes
Yes
1-2Not
drug
related
Drowsin
ess
400mg
Non
e2
60Yes
Yes
1Po
ssible
Drowsin
ess
Placebo
Non
e15
140
Yes
Yes
1Not
drug
related
Nausea
500mg
Non
e025
20Yes
Yes
1Po
ssible
Nausea
Placebo
Non
eIm
mediate
10Yes
Yes
3Not
drug
related
Heavinessof
head
80mg
Non
e025
15Yes
Yes
1Po
ssible
Heavinessof
head
Placebo
Non
e1
10Yes
Yes
1Not
drug
related
Visualdistu
rbances
320mg
Non
e36
2-3
Yes
Yes
1Re
mote
Bradycardia
400mg
Non
e1
60Yes
Yes
1Po
ssible
Retching
Placebo
Non
eIm
mediate
10Yes
Yes
3Not
drug
related
Itching
400mg
Non
e24
8Yes
Yes
1Po
ssible
Dizziness
Placebo
Non
e1
10Yes
Yes
3Not
drug
related
Severitygradingdo
neaccordingto
Com
mon
Term
inolog
yCr
iteria
forA
dverse
Eventsv40U
SDepartm
ento
fHealth
andHum
anServicesG
rade
1Mild
asymptom
aticor
mild
symptom
sclinicalord
iagn
ostic
observations
onlyinterventionno
tind
icatedG
rade
2Mod
erateminim
allocalor
noninvasiveinterventionindicatedGrade
3Severeor
medicallysig
nificantb
utno
timmediatelylife-threateningho
spita
lization
orprolon
gatio
nof
hospita
lizationindicateddisablingGrade
4Life-th
reateningconsequencesurgentinterventionindicatedGrade
5Death
relatedto
AE
Causality
assessmentNon
eremote(lt5
chance
ofbeingdrug
related)possib
le(gt5
butle
50chance
ofbeingdrug
relatedprobable(gt50chance
ofbeingdrug
related)
anddefin
ite
Grade
3severitymdash
volunteerw
ason
placebo
6 Malaria Research and Treatment
Excluded 13
Screened n = 63
Did not meet inclusionexclusion criteria n = 5
Refused consent n = 8
Randomized n = 50
Completed n = 12
Analyzed n = 50
Placebo n = 12 CDRI 9778 n = 38
Completed n = 38
Withdrawals n = 0
Dropouts n = 0
(a)
Flow of participants through the pharmacokinetic study
Enrolled and included in final
Screened (n = 20)
analysis (n = 16)
meet inclusion criteria n = 3
Refused consent n = 1 did not
(b)
Figure 2 Volunteer screening flowchart for ascending dose study 50 normal healthy human volunteers were screened from 63 volunteerswhile for single dose pharmacokinetics study 16 healthy volunteers were from 20 volunteers
remained well within normal range and did not demonstrateany dose response relationship were PCV total leukocyte andlymphocyte counts RBC counts and methemoglobin levels
34 Biochemical Parameters There was no significant differ-ence in serumbilirubin SGOT and SGPT at any time point ofmeasurement for intergroup comparisons The values ofserum alkaline phosphatase however were significantly dif-ferent between various groups at all pre- and postdrug mea-surements Post hoc analysis for this revealed that the resultswere significant for comparisons between lowest (80mgCDRI 9778) and higher doses (500 and 600mgCDRI 9778)although none of the groups was significantly differentfrom placebo All the values remained within normal range(Table 4) The other biochemical parameters which showedsignificant changes between groups were serum albumin
serum globulin and blood glucose and serum HDL levelsHowever they remained within the normal laboratory rangeand did not cause any sign or symptoms and there was nodose response relationship noted
35 Serum Electrolyte Levels The groups demonstrated sig-nificant variation in serum sodium and serum potassiumvalues at all time points of measurements None of the volun-teers had values outside the normal physiological ranges norpresented with any signs or symptoms of dyselectrolytemiaso these findings were considered clinically irrelevant
36 Pharmacokinetic Analysis Following oral administrationat 200mg compound 9778 was rapidly absorbed getsimmediately converted into active metabolite 9763 andis eliminated from the systemic circulation within 48 h
Malaria Research and Treatment 7
Table4Com
paris
onof
liver
functio
ntests
betweenvario
ustre
atmentg
roup
sonrepeated
observations
atbaselin
e24
hoursa
ndday7
Treatm
entg
roup
sTo
talserum
bilirub
inSerum
SGOT
Serum
SGPT
Serum
Alkalinep
hosphatase
Baselin
e24
hour
Day
7Ba
selin
e24
hour
Day
7Ba
selin
e24
hour
Day
7Ba
selin
e24
hour
Day
780
mg(119899=6)082plusmn024073plusmn024064plusmn0232215plusmn632348plusmn288277plusmn612188plusmn100262plusmn66218plusmn37955plusmn26651025plusmn300910683plusmn3712
160m
g(119899=6)076plusmn039055plusmn00706plusmn0063418plusmn7893398plusmn9693833plusmn8913721plusmn4163943plusmn808445plusmn11642115plusmn6865212plusmn6720717plusmn6103
320m
g(119899=6)073plusmn05208plusmn04087plusmn0593283plusmn5153417plusmn77635plusmn8533383plusmn9093733plusmn8873833plusmn1384242plusmn45242225plusmn345523583plusmn3249
400m
g(119899=6)052plusmn004053plusmn005055plusmn0082667plusmn662315plusmn453233plusmn88729plusmn5443517plusmn41238plusmn129523283plusmn4225167plusmn475924283plusmn3482
500m
g(119899=6)052plusmn004052plusmn004053plusmn0053133plusmn876315plusmn60234plusmn6003283plusmn1153483plusmn11073533plusmn105632117plusmn151313plusmn124533967plusmn18425
600m
g(119899=6)08plusmn05408plusmn059082plusmn0593117plusmn633033plusmn6743133plusmn57830plusmn716305plusmn8463317plusmn10532725plusmn667127583plusmn6129274plusmn7517
700m
g(119899=2)06plusmn01406plusmn014055plusmn007355plusmn07140plusmn424345plusmn07146plusmn566465plusmn49540plusmn11312615plusmn502254plusmn56572605plusmn4455
Placebo(119899=12)055plusmn007056plusmn006055plusmn0123191plusmn9673117plusmn918305plusmn8153708plusmn18113858plusmn19563583plusmn1811208plusmn6823208plusmn655620858plusmn7223
ANOVA119865
1114
1308
1105
1701
1631
114
162
1097
1435
4545
5103
3802
df49
4949
4949
4949
4949
4949
49119875
037
027
038
013
015
036
016
038
022
lt0001lowast
lt0001lowastlowast
0002
lowast119875=0002for5
00mgcomparedto
80mgdrug
and119875=002for6
00mgcomparedto
80mgdrug
(Scheffersquos
test)
lowastlowast119875=0001and000
6for8
0mgdrug
comparedto
500and60
0mgdrug
respectiv
ely(Scheffersquos
test)
119875=0006forc
omparis
onbetween80
and500m
gdrug
grou
ps(Scheffersquos
test)
Nodifferencefrom
placeboin
anycomparis
on
8 Malaria Research and Treatment
Table 5 Pharmacokinetic parameters of converted active metabolite 9763 after oral administration of 9778 at 200mg single dose to malehealthy human volunteers (119873 = 16)
PKparameter
Converted in vivometabolite 9763Mean plusmn SEMMale healthy human volunteers (119873 = 16)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16119862max(ngmL) 172 201 373 187 149 355 426 202 609 295 474 504 654 105 55 123 14393 plusmn 2832
119879max (h) 15 4 1 2 15 2 4 4 4 2 2 2 15 15 2 15 228 plusmn 02711987912
(h) 1389 217 478 220 388 2127 300 894 780 1163 2426 1450 1010 1773 2451 1890 1185 plusmn 194AUC0minusinfin
(ngsdothmL) 7887 1048 1644 6026 785 15226 2079 16049 5117 18989 935 3561 5836 6968 8331 9841 87874plusmn13315
MRT (h) 1257 572 137 353 538 1425 642 1413 928 976 3072 1453 1126 1837 3220 1852 1377 plusmn 205
Mea
n pl
asm
a con
sn (
ngm
L)
158
138
118
98
78
58
38
18
minus2minus2 8 18 28 38 48 58 68 78
Time (h)
Converted active metabolite 97ndash63
Figure 3 Mean plasma concentration-time profile of in vivo activemetabolite 9763 after oral administration of 9778 at 200mg singledose to male healthy human volunteers (119873 = 16)
except in two volunteers (72 h) as observed from plasmaconcentration-time profile (Figure 3) PK parameters gener-ated in individual volunteers have been shown in Table 5119879max of active metabolite 9763 was found to be 228 plusmn 027 hwith 119862max of 14393 plusmn 2832 Mean values of 119879
12 MRT and
AUC0ndashinfin of 9763were 505plusmn057 h 973plusmn106 h and 84522plusmn
14296 ngsdothmL respectively Active metabolite 9763 wasquantified from 05 h and up to 48 h in healthy volunteerswith exception to two volunteers in whom it was observed upto 72 h No additional metabolite peaks were observed duringanalysis except 9763 In most of the volunteers parentmolecule 9778was below the limit of quantitationMoreoververy low concentrations of 9778were observed in some volu-nteers but these were not sufficient for generating the PKparameters
4 Discussion
This was a first-in-human study conducted on healthy malevolunteers for a new antimalarial drug CDRI 9778 Overallthe drug was found to be safe
Few adverse events were reported which were of mildnature and were probable in causality But the adverse eventswere neither clinically nor statistically significant The 14adverse events reported in this trial occurred in various treat-ment groups over a large time frame Hence it cannot be said
definitelywhether theywere due to the drug or notMoreoversimilar adverse events were also seen in the placebo groupEven the statistically significant alteration in blood pressurewas not associated with signs and symptoms of altered bloodpressure and the values fell within normal ranges
For none of the adverse events any intervention in theform of drug administration fluid substitution and resusci-tation was required All the reported events continued to beobserved and resolved spontaneously
The severity of the adverse events was at best graded at 2No serious adverse events were reported The NCE underevaluation is a derivative of artemisinin compound which israrely associatedwith any SAEHowever structural similarityis just an indicator for predicting adverse effect profile of anovel compound A future possibility of such reactions com-ing into light always remains
Hence theMTD could not be determinedThough deter-mination of MTD was the main purpose of the study thiscould not be achieved This is a definite possibility in phase Istudies as has been seen previously [21 22] For the determi-nation of dose for multiple ascending dose study data frompreclinical efficacy studies will be used which is found to liewell within the highest dose evaluated in the present study
Therewere some haematological and biochemical param-eters which showed statistically significant values when com-pared to placebo but the differences were not clinically sig-nificant as most of them stayed within the normal laboratoryrange Further the absence of dose response relationshiphighlighted the fact that they were innocuous Nonclinicaltoxicity data serves as a guide to the monitoring of adversedrug events once the studies are conducted in healthy volun-teers Though there were no specific concerns raised in non-clinical toxicity a thorough evaluation of haematological andbiochemical parameters was undertaken Statistically signif-icant differences should be interpreted with caution keepingin mind the clinical relevance [23 24]
Since structurally the compound was similar to arte-misinin which has been reported to prolong QTc interval[25] a careful evaluation of QT interval was also undertakenThiswas also undertaken for assessing a future need to under-take a thoroughQT study No clinicallymeaningful alterationofQT interval as laid down in E 14 guidance document forQTevaluation [26] was observed
Malaria Research and Treatment 9
5 Conclusion
In conclusion we can say that the new compound CDRI9778 appears to be a safe and tolerable drug Its safety can befurther tested in multiple dose studies and if found tolerablecan be a good therapeutic option for malaria especiallymalaria resistant to available drugs
Conflict of Interests
The investigators did not receive any money for the conductof the study The study was sponsored by the Central DrugResearch Institute India The Innovator Institute a govern-ment organization had tied up with IPCA Ltd for the man-ufacture of the drug The drugs were supplied by IPCA LtdThey had no role in data collection recording and reportingTwo of the authors Dr Nitin Chandorkar and Dr AnilPareek are employees of IPCA Their role was in designingand conducting the study All the analyses were done inde-pendently by the investigatorsrsquo team
Acknowledgments
The authors would like to acknowledge the efforts of MrOnkar Rathod for helping in the execution of the study andMr Mitesh Sharma for giving his inputs for statistical analy-sis The research was funded by Central Drug Research Insti-tute (CSIR) Lucknow India This is a government organiza-tion
References
[1] ldquoWorldMalaria Reportrdquo 2005 httpwwwrollbackmalariaorgwmr2005
[2] A V Kondrashin ldquoMalaria in theWHOSoutheast Asia regionrdquoIndian Journal of Malariology vol 29 no 3 pp 129ndash160 1992
[3] U Arora G S Sonal G P S Dhillon andH GThakor ldquoEmer-gence of drug resistance in Indiardquo Journal of the Indian MedicalAssociation vol 106 no 10 pp 678ndash681 2008
[4] B M Greenwood D A Fidock D E Kyle et al ldquoMalaria pro-gress perils and prospects for eradicationrdquo Journal of ClinicalInvestigation vol 118 no 4 pp 1266ndash1276 2008
[5] C Singh and S K Puri ldquoSubstituted 124-trioxanes as anti-malarial agents and a process of producing the substituted 124-trioxanerdquo US Patent no 6316493 B1 2001
[6] C Singh N Gupta and S K Puri ldquoPhoto-oxygenation of ger-aniol synthesis of a novel series of hydroxy-functionalized anti-malarial 124-trioxanesrdquo Bioorganic and Medicinal ChemistryLetters vol 12 no 15 pp 1913ndash1916 2002
[7] C Singh N Gupta and S K Puri ldquoGeraniol-derived 124-trioxanes with potent in-vivo antimalarial activityrdquo Bioorganicand Medicinal Chemistry Letters vol 13 no 20 pp 3447ndash34502003
[8] C Singh N C Srivastav and S K Puri ldquoSynthesis and anti-malarial activity of 6-cycloalkylvinyl substituted 124-tri-oxanesrdquo Bioorganic andMedicinal Chemistry vol 12 no 22 pp5745ndash5752 2004
[9] A G Griesbeck T T El-Idreesy L-O Hoinck J Lex and RBrun ldquoNovel spiroanellated 124-trioxanes with high in vitro
antimalarial activitiesrdquo Bioorganic and Medicinal ChemistryLetters vol 15 no 3 pp 595ndash597 2005
[10] C Singh H Malik and S K Puri ldquoOrally active amino func-tionalized antimalarial 124-trioxanesrdquo Bioorganic and Medici-nal Chemistry Letters vol 14 no 2 pp 459ndash462 2004
[11] C SinghNGupta and S K Puri ldquoPhotooxygenation of 3-aryl-2-cyclohexenols synthesis of a new series of antimalarial 124-trioxanesrdquo Tetrahedron Letters vol 46 no 2 pp 205ndash207 2005
[12] C Singh HMalik and S K Puri ldquoOrally active 124-trioxanessynthesis and antimalarial assessment of a new series of 9-functionalized 3-(1-arylvinyl)-125-trioxaspiro[55]undecanesagainst multi-drug-resistant Plasmodium yoelii nigeriensis inmicerdquo Journal of Medicinal Chemistry vol 49 no 9 pp 2794ndash2803 2006
[13] C Singh S Chaudhary and S K Puri ldquoNew orally active deri-vatives of artemisinin with high efficacy against multidrug-resistant malaria in micerdquo Journal of Medicinal Chemistry vol49 no 24 pp 7227ndash7233 2006
[14] C Singh U Sharma G Saxena and S K Puri ldquoOrally activeantimalarials synthesis and bioevaluation of a new series ofsteroid-based 124-trioxanes against multi-drug resistantmalaria in micerdquo Bioorganic and Medicinal Chemistry Lettersvol 17 no 15 pp 4097ndash4101 2007
[15] C Singh R Kanchan U Sharma and S K Puri ldquoNewadamantane-based spiro 124-trioxanes orally effective againstrodent and simianmalariardquo Journal ofMedicinal Chemistry vol50 no 3 pp 521ndash527 2007
[16] C Singh S Chaudhary RKanchan and SK Puri ldquoConversionof antimalarial drug artemisinin to a new series of tricyclic 124-trioxanesrdquo Organic Letters vol 9 no 21 pp 4327ndash4329 2007
[17] C Singh V P Verma N K Naikade A S Singh M Hassamand S K Puri ldquoNovel bis- and tris-124-trioxanes synthesis andantimalarial activity against multidrug-resistant Plasmodiumyoelii in swiss micerdquo Journal of Medicinal Chemistry vol 51 no23 pp 7581ndash7592 2008
[18] R P Singh S Sabarinath N Gautam R C Gupta and S KSingh ldquoPharmacokinetic study of the novel synthetic trioxaneantimalarial compound 97-78 in rats using an LC-MSMSmethod for quantificationrdquo Arzneimittel-Forschung vol 61 no2 pp 120ndash125 2011
[19] R P Singh S Sabarinath N Gautam R C Gupta and S KSingh ldquoLiquid chromatographic tandem mass spectrometricassay for quantification of 9778 and its metabolite 9763 apromising trioxane antimalarial in monkey plasmardquo Journal ofChromatography B vol 877 no 22 pp 2074ndash2080 2009
[20] V P Shah K K Midha J W A Findlay et al ldquoBioanalyticalmethod validationmdasha revisit with a decade of progressrdquo Phar-maceutical Research vol 17 no 12 pp 1551ndash1557 2000
[21] E RGerstner A F Eichler S R Plotkin et al ldquoPhase I trial withbiomarker studies of vatalanib (PTK787) in patients with newlydiagnosed glioblastoma treated with enzyme inducing anti-epileptic drugs and standard radiation and temozolomiderdquoJournal of Neuro-Oncology vol 103 no 2 pp 325ndash332 2011
[22] A Forero-Torres J Shah TWood et al ldquoPhase I trial of weeklytigatuzumab an agonistic humanizedmonoclonal antibody tar-geting death receptor 5 (DR5)rdquo Cancer Biotherapy and Radio-pharmaceuticals vol 25 no 1 pp 13ndash19 2010
[23] R C Kane ldquoThe clinical significance of statistical significancerdquoOncologist vol 13 no 11 pp 1129ndash1133 2008
[24] M J Hayat ldquoUnderstanding statistical significancerdquo NursingResearch vol 59 no 3 pp 219ndash223 2010
10 Malaria Research and Treatment
[25] I R Ribeiro and P Olliaro ldquoSafety of artemisinin and its deriva-tives A review of published and unpublished clinical trialsrdquoMedecine Tropicale vol 58 no 3 supplement pp 50ndash53 1998
[26] 2013 httpwwwfdagovdownloadsDrugsGuidanceCompli-anceRegulatoryInformationGuidancesucm073161pdf
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 Malaria Research and Treatment
O
OO
OO
O
O
O
OO
OHO
HO
O
OHH
HO
O
H
97ndash78 parent compound
97ndash63 metabolite
CH3
CH3
H3C
OC2H5
IS (120572-Arteether)
Figure 1 Chemical structure of parent compound 9778 in vivoactive metabolites 9763 and IS (120572-arteether)
identified and developed by CDRI groups [5ndash8 10ndash17] Manycompounds have shown high efficacy against multidrugresistant Plasmodium falciparum strains [6 12 13 15 17] But9778 emerged as lead compound for excellent pharma-cological activity in both in vitro and in vivomalarial modelsAfter successful completion of regulatory preclinical studiescompound is currently in phase I clinical trials [18 19]
Potent antimalarial activity of these compounds may bedue to its capacity (i) to mimic the choline structure whichblocks phosphatidylcholine biosynthesis and (ii) to interactwith hemozoin the malarial hemoglobin-degradation pro-duct Compounds potency is also due to its high accumula-tion inside the infected erythrocytes This dual mechanismof action of 9778 should limit the risk of emergence ofresistance The chemical name of the compound isMono[2methyl2[3(1spiro[tricycle[331137]decane231015840-[1 24]trioxan] 61015840-yle thenyl) phenoxy] propyl] ester It has power-ful antimalarial activity against chloroquine resistant Pfalciparum in vitro chloroquine sensitive P berghei and mul-tidrug resistant P yoelii in mice and P cynomolgi in rhesusmonkeys It has been developed as a synthetic substitute forantimalarial peroxide artemisinin and its derivatives such asartemether arteether and artesunic acid The CDRI com-pound 9778 is effective by oral and intravenous routes andtherefore can be used by either route
Firstly 9763 was synthesized but due to its poor bioavail-ability it was resynthesized as a hemisuccinate derivative andcoded as 9778 Upon administration of 9778 it gets con-verted into its active in vivo metabolite 9763 The concen-trations of 9763 and 9778 can be measured by validatedLC-MSMS method [19] The preclinical testing for thiscompound included pharmacokinetic (PK) studies animal
pharmacology and toxicology male fertility studies femalereproduction and development toxicity studies and genotox-icity studies and the compound was taken up for evaluationin phase I study as it lacked any remarkable toxicity concernsin animal studies
The aim of this study was to calculate the maximumtolerated dose of the compound in healthy human volunteersalong with evaluation of PK profiles of 9778 and its in vivometabolite 9763 after oral administrations of 9778
2 Subjects and Methods
21 Subjects The study was approved by the Institutersquos EthicsCommitteeThe single ascending dose study and the pharma-cokinetic study are registered with Central Trial Registry ofIndia (CTRI201207002812 CTRI201207002832) Nor-mal healthy male volunteers in the age group of 18ndash45 yearswere invited to join the trial A detailed informed consentprocess of the volunteerswas undertaken and screening of thevolunteers was done after obtaining informed consent Theywere recruited through contacts and hospital employees wereexcluded The health status of the volunteers was determinedby taking medical history physical examination routinehaematology (haemoglobin total lymphocyte count differ-ential count and platelet count) clinical biochemistry (serumglutamic oxaloacetic transaminase (SGOT) serum glutamicpyruvic transaminase (SGPT) serum bilirubin serum crea-tinine blood urea serum electrolytes random blood sugartotal protein and serum lipid profile) and urine and stoolanalysis (routine examination and microscopy) The volun-teers were asked to report to the study site after 12 hours offasting for the blood tests Chest X-ray and 12-lead ECGwerealso taken The participants were also screened for humanimmunodeficiency virus (HIV) and hepatitis B
The volunteers were excluded if there was a history ofhaving donated blood in the past 3 months HIV or HBsAgpositivity history of any drug intake in the past 15 days his-tory of receiving any enzyme-inducing agent in the preceding15 days history of participating in any investigational newdrug (IND) study in the previous 6 months history of par-ticipating in any non-IND study in the preceding 3 monthshistory of allergy or hypersensitivity to any medication his-tory of peptic disorder chronic smoker gt6 cigarettesbeediesper day alcoholic (history of daily alcohol intake in the last 6months) history of any drug abuse tobacco user in any formhistory of any chronic disease and taking medication andhistory of taking nonallopathic drug in the past 6 months forany illness or history of any major illness in the past (namelymeningitis hepatitis tuberculosis epilepsy nephritis havingreceived treatment and presently asymptomatic)
The procedure for recruiting participants for single dosePK study was similar to the above The PK study was under-taken in 16 separate volunteers following the evaluation ofsafety data for phase I study and evaluation of pharmacody-namics study in animals
22 Design This was a single ascending dose placebo-controlled randomized double blind trial Randomization
Malaria Research and Treatment 3
was carried out by computer generated random numbersequence Randomization was carried out for the drug andthe placebo in a 3 1 ratio for each dose level The drugs weredispensed in sealed bottles with the randomization codewrit-ten on them Randomization codes were provided in sealedopaque envelopes with the protocol specification that thecodes may be opened by the investigator only in case of aserious or severe adverse event
23 Starting Dose and Dose Escalation The starting dose was80mg calculation of starting dose was based on the basis ofmaximum tolerated dose of 100mgkg obtained in rats Thiswas used to obtain a dose of 96mg for a 60 kg man The for-mulation which was available for a dose below this was of80mg and hence taking these factors into consideration astarting dose of 80mg was chosen The following dose levelswere evaluated 80 160 320 400 500 600 and 700mg Thestarting dose was calculated by allometric scaling from ani-mals At each dose level six volunteers received CDRI 9778and two received placebo except at 700mg where only twovolunteers were given this dose At each dose level volunteerswere assessed before proceeding to the next dose The deci-sion to dose only 2 volunteers was taken after analysis of dataof 600mg wherein no remarkable adverse events were noted
24 Stopping Rule The decision to stop the dose escalationwas based on the appearance of the dose limiting toxicity(DLT) which was defined as the dose at which any of thefollowing appeared severe nausea vomiting heartburnheadache remarkable change in vital parameters such asblood pressure heart rate respiratory rate or oxygen satura-tion of blood changes in QT interval or any event that in theopinion of the investigators required stopping of the trial
Maximum tolerated dose was defined as the dose beforewhich any of the components of DLT appeared at a signifi-cantly higher rate as compared to placebo In case this was notachieved it was planned not to dose volunteers beyond700mg
25 Study Procedure The volunteers after giving informedconsent were screenedThe screening process was done latestwithin 1 month of admission for dosing The volunteers whofulfilled the inclusionexclusion criteria were admitted inthe CPU the night before drug administration Standardizeddinner was served at 9 pm the night prior to dosing On day0 baseline blood sample for biochemical and haematologicalexamination and stool and urine samples for routine andmicroscopywere takenThey received the study drug accord-ing to the randomization sequence under supervision Theempty packaging was returned to the container The volun-teers received drug as per randomization Breakfast was givenhalf an hour after drug administration Subsequently stan-dardized lunch and dinner were served to the volunteers
For pharmacokinetic (PK) study eligible participantswere admitted and housed in the clinical pharmacology unitan evening prior to the PK study A standard dinner wasserved and a fasting condition for at least 10 hrs prior todosing and 4 hrs after dosing was ensured A peripheral
forearm veinwas cannulated for sampling for the PK analysis200mg of the study drug was administered with 300mL ofwater The time of actual dose administration to the nearestminute was recorded 25mL of blood was collected from theindwelling cannula at 0 (before dose) 025 05 075 1 15 24 6 8 12 18 24 48 72 96 120 and 144 hrs (after dose) 10mLof additional blood was collected at 0 (before dose) and 24 hr(after dose) for laboratory parameters for safety assessmentand PK control sample A time window of plusmn2 minutes waspermitted for collecting the post dose samples from thescheduled time for PK analysis
Plasmawas separated from blood sample intended for PKanalysis within 1 hour of blood sampling by centrifugationat 2000 rpm for 10min at 4∘C Samples were stored at minus80∘Cpending transportation Heparinised blood samples weretransported to the laboratory within 7 days of collection
26 Subject Monitoring The subjects were attached to a car-diac monitor and vital HR BP ECG oxygen saturation andRR were recorded Corrected QT interval using Fridericiarsquosformula was calculated Adverse events were assessed atspecific time points (05 1 2 4 6 8 12 and 24 hrs after med-ication) Unscheduled monitoring was undertaken wheneverit felt necessary The volunteers were discharged after 24 hrsand they had to return at 48 hrs and on the 7th day for follow-up At the end of the 7th day theywere said to have completedthe study Routine haematological and biochemical investiga-tionswere performed at 0 hr 24 hrs after drug administrationand on day 7 The study was monitored by a Data SafetyMonitoring Board
27 Pharmacokinetic Analysis Quantitative analyses of clin-ical phase ascending dose and single dose PKs samples weredone at GLP lab of Pharmacokinetics and Metabolism Divi-sion CDRI Lucknow India 120572-Arteether was used as aninternal standard and all the analyses were performed as perthe published method by Singh et al 2009 [19] Acceptancecriteria for analytical runs were fixed as per internationallyapproved guidelines [20] Data acquisition and quantitationwere performed using analyst software version 14 (AppliedBiosystems MDS SCIEX Toronto Canada) PK parameterswere estimated by using WinNonlin software (Version 15Pharsight Corporation Mountain View CA) Oral datawere best fitted in noncompartmental model The individualplasma concentration-time profiles were subjected to non-compartmental analysis to determine various PK parametersThe PK parameters included the terminal elimination half-life (119879
12) maximum plasma concentration (119862max) time to
reachmaximum plasma concentration (119879max) area under thecurve (AUC
0ndashinfin) and mean residence time (MRT)
28 Statistical Analysis Continuous data were presented asmean plusmn SD and categorical data were presented as 119899 () Forcomparison between the drug and placebo at each dose levelunpaired 119905-test was used for continuous variables and Fis-cherrsquos exact test for categorical variables For comparisonbetween various dose levels ANOVAwas used 119875 value lt005was considered significant
4 Malaria Research and Treatment
Table 1 Demographic characteristics of the volunteers included in the studies
Characteristic 80mg 160mg 320mg 400mg 500mg 600mg 700mg Placebo119873 = 6 119873 = 6 119873 = 6 119873 = 6 119873 = 6 119873 = 6 119873 = 2 119873 = 12
Age in years Mean (SD) 285 (1093) 275 (432) 250 (712) 252 (213) 213 (353) 252 (767) 230 (141) 254 (575)Height in cm Mean (SD) 1705 (533) 1675 (58) 1667 (644) 1673 (408) 1670 (357) 1702 (577) 1710 (141) 1713 (489)Weight in kg Mean (SD) 586 (972) 690 (1357) 566 (884) 616 (717) 596 (647) 613 (1267) 635 (212) 607 (843)BMI (kgm2) Mean (SD) 201 (304) 248 (589) 203 (214) 220 (235) 214 (25) 217 (036) 207 (275) 214 (34)
Table 2 Adverse events noted at various drug dosages of CDRI9778
Treatment group Type of adverse events No of events80mg CDRI 9778 Heaviness of head 1160mg CDRI 9778 None320mg CDRI 9778 Visual disturbance 1
400mg CDRI 9778Drowsiness 1Bradycardia 1Itching 1
500mg CDRI 9778 Sedation 1Nausea 1
600 and 700mg CDRI 9778 Sedation 1
Placebo
Sedation 1Drowsiness 1Nausea 1Retching 1Dizziness 1
Heaviness of head 1
3 Results
63 volunteers were screened out of whom 50 volunteersmatched the inclusionexclusion criteria andwere included inthe safety study (Figure 2) For the PK study 16 healthy malevolunteers were included after screening of 20 volunteers Asrequired by the study protocol all the volunteers were male(Figure 2) There was no significant difference in the demo-graphic parameters like age (119875 = 07) height (119875 = 05)weight (119875 = 05) and body mass index (119875 = 03) amongparticipants in various treatment groups (Table 1)
31 Adverse Events Adverse events that occurred during thestudy were few (Table 2) and largely of severity grade 1 to 2(Table 2)There was no significant difference in the incidenceof events in the drug and the placebo groups (119875 = 043)
Sedation was the most common adverse event reportedacross different groups (314 214) It was noted in 3 vol-unteers given 500mg CDRI 9778 600mg CDRI 9778 andplacebo about 2 hours after drug administration and lastedfor 1-2 hours It was grade 1-2 in severity spontaneous andcomplete recoverywas seen in all and no actionwas requiredThe other adverse events noted were mild drowsiness mildnausea slight heaviness of head bradycardia (56-57 bpm)visual disturbances and itching (Table 3)
Severe adverse event nausea and retching immediatelyafter drug administration was observed in one patient whichlasted for 10minutes the patient also complained of dizzinessand slight heaviness of head 1 hour after drug administrationOn decoding he was found to have received placebo Thesymptoms resolved spontaneously hence no further actionneeded to be taken
32 Clinical Parameters At baseline the different treatmentgroups were similar in terms of clinical parameters (pulserate blood pressure and respiratory rate) None of the treat-ment groups demonstrated a significant alteration in pulserate respiratory rate and systolic blood pressure at any timepoint compared to baseline However there was a significantchange in diastolic blood pressure in 600 and 700mg CDRI9778 group (7687plusmn 874 7837plusmn 886 7925plusmn 1346 6712plusmn649 7312plusmn1232 7587plusmn811 74plusmn11 and 75plusmn1003mmHgat 0 05 1 2 4 6 8 and 12 hours respectively 119875 = 002)although clinically significant declinewas not observed in anyof the volunteers Statistical significance was observed forbetween group comparison of systolic and diastolic bloodpressures 2 hours after drug administration The SBP for80mg 160mg 320mg 400mg 500mg 600mg 700mgand placebo groups were 11217 plusmn 624 1195 plusmn 517 1275 plusmn638 11183plusmn791 1145plusmn834 11283plusmn618 1155plusmn212 and11633 plusmn 877 respectively (119875 = 001) The DBP for 80mg160mg 320mg 400mg 500mg 600mg 700mg andplacebo groups were 73 plusmn 521 7717 plusmn 806 8233 plusmn 4687133plusmn819 7183plusmn781 665plusmn653 69plusmn848 and 7375plusmn824(119875 = 003) Respiratory rate was found to be significantlydifferent between treatment groups 4 6 and 8 hours afterdrug administration although this was not clinically relevant
There was no statistically or clinically significant dif-ference noted in the corrected QT interval within varioustreatment groups (119875 = 0656 0523 0901 0348 0809 and043 respectively for 80 160 320 400 500 and 600700mggroups)
33 Hematological Parameters Hemoglobin values demon-strated a statistically significant alteration during posttreat-ment period in the group receiving 400mg CDRI 9778(1425 plusmn 075 1492 plusmn 094 and 1435 plusmn 110 gm at baseline24 hr and 7th day respectively 119875 = 002) A statistically sig-nificant change in platelet counts was also observed in 320mgCDRI 9778 group (190 plusmn 68 190 plusmn 69 and 212 plusmn 66(times1012)L respectively 119875 = 004) All these values were wellwithin normal limits Other haematological parameterswhich showed statistically significant difference however
Malaria Research and Treatment 5
Table3Descriptio
nof
alladverse
eventsob
served
inthes
tudy
Nam
eofA
ETreatm
entg
roup
Treatm
entg
iven
Time(hrs)of
onset
after
drug
administratio
n
Durationof
AE
(min)
Spon
taneou
sreversal(yes
orno
)Re
versalcomplete
(yes
orno
)Severitygrade
Causalityassessment
Sedatio
n60
0mg
Non
e2
60Yes
Yes
1-2Po
ssible
Sedatio
n500mg
Non
e2
120
Yes
Yes
1-2Po
ssible
Sedatio
nPlacebo
Non
e2
120
Yes
Yes
1-2Not
drug
related
Drowsin
ess
400mg
Non
e2
60Yes
Yes
1Po
ssible
Drowsin
ess
Placebo
Non
e15
140
Yes
Yes
1Not
drug
related
Nausea
500mg
Non
e025
20Yes
Yes
1Po
ssible
Nausea
Placebo
Non
eIm
mediate
10Yes
Yes
3Not
drug
related
Heavinessof
head
80mg
Non
e025
15Yes
Yes
1Po
ssible
Heavinessof
head
Placebo
Non
e1
10Yes
Yes
1Not
drug
related
Visualdistu
rbances
320mg
Non
e36
2-3
Yes
Yes
1Re
mote
Bradycardia
400mg
Non
e1
60Yes
Yes
1Po
ssible
Retching
Placebo
Non
eIm
mediate
10Yes
Yes
3Not
drug
related
Itching
400mg
Non
e24
8Yes
Yes
1Po
ssible
Dizziness
Placebo
Non
e1
10Yes
Yes
3Not
drug
related
Severitygradingdo
neaccordingto
Com
mon
Term
inolog
yCr
iteria
forA
dverse
Eventsv40U
SDepartm
ento
fHealth
andHum
anServicesG
rade
1Mild
asymptom
aticor
mild
symptom
sclinicalord
iagn
ostic
observations
onlyinterventionno
tind
icatedG
rade
2Mod
erateminim
allocalor
noninvasiveinterventionindicatedGrade
3Severeor
medicallysig
nificantb
utno
timmediatelylife-threateningho
spita
lization
orprolon
gatio
nof
hospita
lizationindicateddisablingGrade
4Life-th
reateningconsequencesurgentinterventionindicatedGrade
5Death
relatedto
AE
Causality
assessmentNon
eremote(lt5
chance
ofbeingdrug
related)possib
le(gt5
butle
50chance
ofbeingdrug
relatedprobable(gt50chance
ofbeingdrug
related)
anddefin
ite
Grade
3severitymdash
volunteerw
ason
placebo
6 Malaria Research and Treatment
Excluded 13
Screened n = 63
Did not meet inclusionexclusion criteria n = 5
Refused consent n = 8
Randomized n = 50
Completed n = 12
Analyzed n = 50
Placebo n = 12 CDRI 9778 n = 38
Completed n = 38
Withdrawals n = 0
Dropouts n = 0
(a)
Flow of participants through the pharmacokinetic study
Enrolled and included in final
Screened (n = 20)
analysis (n = 16)
meet inclusion criteria n = 3
Refused consent n = 1 did not
(b)
Figure 2 Volunteer screening flowchart for ascending dose study 50 normal healthy human volunteers were screened from 63 volunteerswhile for single dose pharmacokinetics study 16 healthy volunteers were from 20 volunteers
remained well within normal range and did not demonstrateany dose response relationship were PCV total leukocyte andlymphocyte counts RBC counts and methemoglobin levels
34 Biochemical Parameters There was no significant differ-ence in serumbilirubin SGOT and SGPT at any time point ofmeasurement for intergroup comparisons The values ofserum alkaline phosphatase however were significantly dif-ferent between various groups at all pre- and postdrug mea-surements Post hoc analysis for this revealed that the resultswere significant for comparisons between lowest (80mgCDRI 9778) and higher doses (500 and 600mgCDRI 9778)although none of the groups was significantly differentfrom placebo All the values remained within normal range(Table 4) The other biochemical parameters which showedsignificant changes between groups were serum albumin
serum globulin and blood glucose and serum HDL levelsHowever they remained within the normal laboratory rangeand did not cause any sign or symptoms and there was nodose response relationship noted
35 Serum Electrolyte Levels The groups demonstrated sig-nificant variation in serum sodium and serum potassiumvalues at all time points of measurements None of the volun-teers had values outside the normal physiological ranges norpresented with any signs or symptoms of dyselectrolytemiaso these findings were considered clinically irrelevant
36 Pharmacokinetic Analysis Following oral administrationat 200mg compound 9778 was rapidly absorbed getsimmediately converted into active metabolite 9763 andis eliminated from the systemic circulation within 48 h
Malaria Research and Treatment 7
Table4Com
paris
onof
liver
functio
ntests
betweenvario
ustre
atmentg
roup
sonrepeated
observations
atbaselin
e24
hoursa
ndday7
Treatm
entg
roup
sTo
talserum
bilirub
inSerum
SGOT
Serum
SGPT
Serum
Alkalinep
hosphatase
Baselin
e24
hour
Day
7Ba
selin
e24
hour
Day
7Ba
selin
e24
hour
Day
7Ba
selin
e24
hour
Day
780
mg(119899=6)082plusmn024073plusmn024064plusmn0232215plusmn632348plusmn288277plusmn612188plusmn100262plusmn66218plusmn37955plusmn26651025plusmn300910683plusmn3712
160m
g(119899=6)076plusmn039055plusmn00706plusmn0063418plusmn7893398plusmn9693833plusmn8913721plusmn4163943plusmn808445plusmn11642115plusmn6865212plusmn6720717plusmn6103
320m
g(119899=6)073plusmn05208plusmn04087plusmn0593283plusmn5153417plusmn77635plusmn8533383plusmn9093733plusmn8873833plusmn1384242plusmn45242225plusmn345523583plusmn3249
400m
g(119899=6)052plusmn004053plusmn005055plusmn0082667plusmn662315plusmn453233plusmn88729plusmn5443517plusmn41238plusmn129523283plusmn4225167plusmn475924283plusmn3482
500m
g(119899=6)052plusmn004052plusmn004053plusmn0053133plusmn876315plusmn60234plusmn6003283plusmn1153483plusmn11073533plusmn105632117plusmn151313plusmn124533967plusmn18425
600m
g(119899=6)08plusmn05408plusmn059082plusmn0593117plusmn633033plusmn6743133plusmn57830plusmn716305plusmn8463317plusmn10532725plusmn667127583plusmn6129274plusmn7517
700m
g(119899=2)06plusmn01406plusmn014055plusmn007355plusmn07140plusmn424345plusmn07146plusmn566465plusmn49540plusmn11312615plusmn502254plusmn56572605plusmn4455
Placebo(119899=12)055plusmn007056plusmn006055plusmn0123191plusmn9673117plusmn918305plusmn8153708plusmn18113858plusmn19563583plusmn1811208plusmn6823208plusmn655620858plusmn7223
ANOVA119865
1114
1308
1105
1701
1631
114
162
1097
1435
4545
5103
3802
df49
4949
4949
4949
4949
4949
49119875
037
027
038
013
015
036
016
038
022
lt0001lowast
lt0001lowastlowast
0002
lowast119875=0002for5
00mgcomparedto
80mgdrug
and119875=002for6
00mgcomparedto
80mgdrug
(Scheffersquos
test)
lowastlowast119875=0001and000
6for8
0mgdrug
comparedto
500and60
0mgdrug
respectiv
ely(Scheffersquos
test)
119875=0006forc
omparis
onbetween80
and500m
gdrug
grou
ps(Scheffersquos
test)
Nodifferencefrom
placeboin
anycomparis
on
8 Malaria Research and Treatment
Table 5 Pharmacokinetic parameters of converted active metabolite 9763 after oral administration of 9778 at 200mg single dose to malehealthy human volunteers (119873 = 16)
PKparameter
Converted in vivometabolite 9763Mean plusmn SEMMale healthy human volunteers (119873 = 16)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16119862max(ngmL) 172 201 373 187 149 355 426 202 609 295 474 504 654 105 55 123 14393 plusmn 2832
119879max (h) 15 4 1 2 15 2 4 4 4 2 2 2 15 15 2 15 228 plusmn 02711987912
(h) 1389 217 478 220 388 2127 300 894 780 1163 2426 1450 1010 1773 2451 1890 1185 plusmn 194AUC0minusinfin
(ngsdothmL) 7887 1048 1644 6026 785 15226 2079 16049 5117 18989 935 3561 5836 6968 8331 9841 87874plusmn13315
MRT (h) 1257 572 137 353 538 1425 642 1413 928 976 3072 1453 1126 1837 3220 1852 1377 plusmn 205
Mea
n pl
asm
a con
sn (
ngm
L)
158
138
118
98
78
58
38
18
minus2minus2 8 18 28 38 48 58 68 78
Time (h)
Converted active metabolite 97ndash63
Figure 3 Mean plasma concentration-time profile of in vivo activemetabolite 9763 after oral administration of 9778 at 200mg singledose to male healthy human volunteers (119873 = 16)
except in two volunteers (72 h) as observed from plasmaconcentration-time profile (Figure 3) PK parameters gener-ated in individual volunteers have been shown in Table 5119879max of active metabolite 9763 was found to be 228 plusmn 027 hwith 119862max of 14393 plusmn 2832 Mean values of 119879
12 MRT and
AUC0ndashinfin of 9763were 505plusmn057 h 973plusmn106 h and 84522plusmn
14296 ngsdothmL respectively Active metabolite 9763 wasquantified from 05 h and up to 48 h in healthy volunteerswith exception to two volunteers in whom it was observed upto 72 h No additional metabolite peaks were observed duringanalysis except 9763 In most of the volunteers parentmolecule 9778was below the limit of quantitationMoreoververy low concentrations of 9778were observed in some volu-nteers but these were not sufficient for generating the PKparameters
4 Discussion
This was a first-in-human study conducted on healthy malevolunteers for a new antimalarial drug CDRI 9778 Overallthe drug was found to be safe
Few adverse events were reported which were of mildnature and were probable in causality But the adverse eventswere neither clinically nor statistically significant The 14adverse events reported in this trial occurred in various treat-ment groups over a large time frame Hence it cannot be said
definitelywhether theywere due to the drug or notMoreoversimilar adverse events were also seen in the placebo groupEven the statistically significant alteration in blood pressurewas not associated with signs and symptoms of altered bloodpressure and the values fell within normal ranges
For none of the adverse events any intervention in theform of drug administration fluid substitution and resusci-tation was required All the reported events continued to beobserved and resolved spontaneously
The severity of the adverse events was at best graded at 2No serious adverse events were reported The NCE underevaluation is a derivative of artemisinin compound which israrely associatedwith any SAEHowever structural similarityis just an indicator for predicting adverse effect profile of anovel compound A future possibility of such reactions com-ing into light always remains
Hence theMTD could not be determinedThough deter-mination of MTD was the main purpose of the study thiscould not be achieved This is a definite possibility in phase Istudies as has been seen previously [21 22] For the determi-nation of dose for multiple ascending dose study data frompreclinical efficacy studies will be used which is found to liewell within the highest dose evaluated in the present study
Therewere some haematological and biochemical param-eters which showed statistically significant values when com-pared to placebo but the differences were not clinically sig-nificant as most of them stayed within the normal laboratoryrange Further the absence of dose response relationshiphighlighted the fact that they were innocuous Nonclinicaltoxicity data serves as a guide to the monitoring of adversedrug events once the studies are conducted in healthy volun-teers Though there were no specific concerns raised in non-clinical toxicity a thorough evaluation of haematological andbiochemical parameters was undertaken Statistically signif-icant differences should be interpreted with caution keepingin mind the clinical relevance [23 24]
Since structurally the compound was similar to arte-misinin which has been reported to prolong QTc interval[25] a careful evaluation of QT interval was also undertakenThiswas also undertaken for assessing a future need to under-take a thoroughQT study No clinicallymeaningful alterationofQT interval as laid down in E 14 guidance document forQTevaluation [26] was observed
Malaria Research and Treatment 9
5 Conclusion
In conclusion we can say that the new compound CDRI9778 appears to be a safe and tolerable drug Its safety can befurther tested in multiple dose studies and if found tolerablecan be a good therapeutic option for malaria especiallymalaria resistant to available drugs
Conflict of Interests
The investigators did not receive any money for the conductof the study The study was sponsored by the Central DrugResearch Institute India The Innovator Institute a govern-ment organization had tied up with IPCA Ltd for the man-ufacture of the drug The drugs were supplied by IPCA LtdThey had no role in data collection recording and reportingTwo of the authors Dr Nitin Chandorkar and Dr AnilPareek are employees of IPCA Their role was in designingand conducting the study All the analyses were done inde-pendently by the investigatorsrsquo team
Acknowledgments
The authors would like to acknowledge the efforts of MrOnkar Rathod for helping in the execution of the study andMr Mitesh Sharma for giving his inputs for statistical analy-sis The research was funded by Central Drug Research Insti-tute (CSIR) Lucknow India This is a government organiza-tion
References
[1] ldquoWorldMalaria Reportrdquo 2005 httpwwwrollbackmalariaorgwmr2005
[2] A V Kondrashin ldquoMalaria in theWHOSoutheast Asia regionrdquoIndian Journal of Malariology vol 29 no 3 pp 129ndash160 1992
[3] U Arora G S Sonal G P S Dhillon andH GThakor ldquoEmer-gence of drug resistance in Indiardquo Journal of the Indian MedicalAssociation vol 106 no 10 pp 678ndash681 2008
[4] B M Greenwood D A Fidock D E Kyle et al ldquoMalaria pro-gress perils and prospects for eradicationrdquo Journal of ClinicalInvestigation vol 118 no 4 pp 1266ndash1276 2008
[5] C Singh and S K Puri ldquoSubstituted 124-trioxanes as anti-malarial agents and a process of producing the substituted 124-trioxanerdquo US Patent no 6316493 B1 2001
[6] C Singh N Gupta and S K Puri ldquoPhoto-oxygenation of ger-aniol synthesis of a novel series of hydroxy-functionalized anti-malarial 124-trioxanesrdquo Bioorganic and Medicinal ChemistryLetters vol 12 no 15 pp 1913ndash1916 2002
[7] C Singh N Gupta and S K Puri ldquoGeraniol-derived 124-trioxanes with potent in-vivo antimalarial activityrdquo Bioorganicand Medicinal Chemistry Letters vol 13 no 20 pp 3447ndash34502003
[8] C Singh N C Srivastav and S K Puri ldquoSynthesis and anti-malarial activity of 6-cycloalkylvinyl substituted 124-tri-oxanesrdquo Bioorganic andMedicinal Chemistry vol 12 no 22 pp5745ndash5752 2004
[9] A G Griesbeck T T El-Idreesy L-O Hoinck J Lex and RBrun ldquoNovel spiroanellated 124-trioxanes with high in vitro
antimalarial activitiesrdquo Bioorganic and Medicinal ChemistryLetters vol 15 no 3 pp 595ndash597 2005
[10] C Singh H Malik and S K Puri ldquoOrally active amino func-tionalized antimalarial 124-trioxanesrdquo Bioorganic and Medici-nal Chemistry Letters vol 14 no 2 pp 459ndash462 2004
[11] C SinghNGupta and S K Puri ldquoPhotooxygenation of 3-aryl-2-cyclohexenols synthesis of a new series of antimalarial 124-trioxanesrdquo Tetrahedron Letters vol 46 no 2 pp 205ndash207 2005
[12] C Singh HMalik and S K Puri ldquoOrally active 124-trioxanessynthesis and antimalarial assessment of a new series of 9-functionalized 3-(1-arylvinyl)-125-trioxaspiro[55]undecanesagainst multi-drug-resistant Plasmodium yoelii nigeriensis inmicerdquo Journal of Medicinal Chemistry vol 49 no 9 pp 2794ndash2803 2006
[13] C Singh S Chaudhary and S K Puri ldquoNew orally active deri-vatives of artemisinin with high efficacy against multidrug-resistant malaria in micerdquo Journal of Medicinal Chemistry vol49 no 24 pp 7227ndash7233 2006
[14] C Singh U Sharma G Saxena and S K Puri ldquoOrally activeantimalarials synthesis and bioevaluation of a new series ofsteroid-based 124-trioxanes against multi-drug resistantmalaria in micerdquo Bioorganic and Medicinal Chemistry Lettersvol 17 no 15 pp 4097ndash4101 2007
[15] C Singh R Kanchan U Sharma and S K Puri ldquoNewadamantane-based spiro 124-trioxanes orally effective againstrodent and simianmalariardquo Journal ofMedicinal Chemistry vol50 no 3 pp 521ndash527 2007
[16] C Singh S Chaudhary RKanchan and SK Puri ldquoConversionof antimalarial drug artemisinin to a new series of tricyclic 124-trioxanesrdquo Organic Letters vol 9 no 21 pp 4327ndash4329 2007
[17] C Singh V P Verma N K Naikade A S Singh M Hassamand S K Puri ldquoNovel bis- and tris-124-trioxanes synthesis andantimalarial activity against multidrug-resistant Plasmodiumyoelii in swiss micerdquo Journal of Medicinal Chemistry vol 51 no23 pp 7581ndash7592 2008
[18] R P Singh S Sabarinath N Gautam R C Gupta and S KSingh ldquoPharmacokinetic study of the novel synthetic trioxaneantimalarial compound 97-78 in rats using an LC-MSMSmethod for quantificationrdquo Arzneimittel-Forschung vol 61 no2 pp 120ndash125 2011
[19] R P Singh S Sabarinath N Gautam R C Gupta and S KSingh ldquoLiquid chromatographic tandem mass spectrometricassay for quantification of 9778 and its metabolite 9763 apromising trioxane antimalarial in monkey plasmardquo Journal ofChromatography B vol 877 no 22 pp 2074ndash2080 2009
[20] V P Shah K K Midha J W A Findlay et al ldquoBioanalyticalmethod validationmdasha revisit with a decade of progressrdquo Phar-maceutical Research vol 17 no 12 pp 1551ndash1557 2000
[21] E RGerstner A F Eichler S R Plotkin et al ldquoPhase I trial withbiomarker studies of vatalanib (PTK787) in patients with newlydiagnosed glioblastoma treated with enzyme inducing anti-epileptic drugs and standard radiation and temozolomiderdquoJournal of Neuro-Oncology vol 103 no 2 pp 325ndash332 2011
[22] A Forero-Torres J Shah TWood et al ldquoPhase I trial of weeklytigatuzumab an agonistic humanizedmonoclonal antibody tar-geting death receptor 5 (DR5)rdquo Cancer Biotherapy and Radio-pharmaceuticals vol 25 no 1 pp 13ndash19 2010
[23] R C Kane ldquoThe clinical significance of statistical significancerdquoOncologist vol 13 no 11 pp 1129ndash1133 2008
[24] M J Hayat ldquoUnderstanding statistical significancerdquo NursingResearch vol 59 no 3 pp 219ndash223 2010
10 Malaria Research and Treatment
[25] I R Ribeiro and P Olliaro ldquoSafety of artemisinin and its deriva-tives A review of published and unpublished clinical trialsrdquoMedecine Tropicale vol 58 no 3 supplement pp 50ndash53 1998
[26] 2013 httpwwwfdagovdownloadsDrugsGuidanceCompli-anceRegulatoryInformationGuidancesucm073161pdf
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Malaria Research and Treatment 3
was carried out by computer generated random numbersequence Randomization was carried out for the drug andthe placebo in a 3 1 ratio for each dose level The drugs weredispensed in sealed bottles with the randomization codewrit-ten on them Randomization codes were provided in sealedopaque envelopes with the protocol specification that thecodes may be opened by the investigator only in case of aserious or severe adverse event
23 Starting Dose and Dose Escalation The starting dose was80mg calculation of starting dose was based on the basis ofmaximum tolerated dose of 100mgkg obtained in rats Thiswas used to obtain a dose of 96mg for a 60 kg man The for-mulation which was available for a dose below this was of80mg and hence taking these factors into consideration astarting dose of 80mg was chosen The following dose levelswere evaluated 80 160 320 400 500 600 and 700mg Thestarting dose was calculated by allometric scaling from ani-mals At each dose level six volunteers received CDRI 9778and two received placebo except at 700mg where only twovolunteers were given this dose At each dose level volunteerswere assessed before proceeding to the next dose The deci-sion to dose only 2 volunteers was taken after analysis of dataof 600mg wherein no remarkable adverse events were noted
24 Stopping Rule The decision to stop the dose escalationwas based on the appearance of the dose limiting toxicity(DLT) which was defined as the dose at which any of thefollowing appeared severe nausea vomiting heartburnheadache remarkable change in vital parameters such asblood pressure heart rate respiratory rate or oxygen satura-tion of blood changes in QT interval or any event that in theopinion of the investigators required stopping of the trial
Maximum tolerated dose was defined as the dose beforewhich any of the components of DLT appeared at a signifi-cantly higher rate as compared to placebo In case this was notachieved it was planned not to dose volunteers beyond700mg
25 Study Procedure The volunteers after giving informedconsent were screenedThe screening process was done latestwithin 1 month of admission for dosing The volunteers whofulfilled the inclusionexclusion criteria were admitted inthe CPU the night before drug administration Standardizeddinner was served at 9 pm the night prior to dosing On day0 baseline blood sample for biochemical and haematologicalexamination and stool and urine samples for routine andmicroscopywere takenThey received the study drug accord-ing to the randomization sequence under supervision Theempty packaging was returned to the container The volun-teers received drug as per randomization Breakfast was givenhalf an hour after drug administration Subsequently stan-dardized lunch and dinner were served to the volunteers
For pharmacokinetic (PK) study eligible participantswere admitted and housed in the clinical pharmacology unitan evening prior to the PK study A standard dinner wasserved and a fasting condition for at least 10 hrs prior todosing and 4 hrs after dosing was ensured A peripheral
forearm veinwas cannulated for sampling for the PK analysis200mg of the study drug was administered with 300mL ofwater The time of actual dose administration to the nearestminute was recorded 25mL of blood was collected from theindwelling cannula at 0 (before dose) 025 05 075 1 15 24 6 8 12 18 24 48 72 96 120 and 144 hrs (after dose) 10mLof additional blood was collected at 0 (before dose) and 24 hr(after dose) for laboratory parameters for safety assessmentand PK control sample A time window of plusmn2 minutes waspermitted for collecting the post dose samples from thescheduled time for PK analysis
Plasmawas separated from blood sample intended for PKanalysis within 1 hour of blood sampling by centrifugationat 2000 rpm for 10min at 4∘C Samples were stored at minus80∘Cpending transportation Heparinised blood samples weretransported to the laboratory within 7 days of collection
26 Subject Monitoring The subjects were attached to a car-diac monitor and vital HR BP ECG oxygen saturation andRR were recorded Corrected QT interval using Fridericiarsquosformula was calculated Adverse events were assessed atspecific time points (05 1 2 4 6 8 12 and 24 hrs after med-ication) Unscheduled monitoring was undertaken wheneverit felt necessary The volunteers were discharged after 24 hrsand they had to return at 48 hrs and on the 7th day for follow-up At the end of the 7th day theywere said to have completedthe study Routine haematological and biochemical investiga-tionswere performed at 0 hr 24 hrs after drug administrationand on day 7 The study was monitored by a Data SafetyMonitoring Board
27 Pharmacokinetic Analysis Quantitative analyses of clin-ical phase ascending dose and single dose PKs samples weredone at GLP lab of Pharmacokinetics and Metabolism Divi-sion CDRI Lucknow India 120572-Arteether was used as aninternal standard and all the analyses were performed as perthe published method by Singh et al 2009 [19] Acceptancecriteria for analytical runs were fixed as per internationallyapproved guidelines [20] Data acquisition and quantitationwere performed using analyst software version 14 (AppliedBiosystems MDS SCIEX Toronto Canada) PK parameterswere estimated by using WinNonlin software (Version 15Pharsight Corporation Mountain View CA) Oral datawere best fitted in noncompartmental model The individualplasma concentration-time profiles were subjected to non-compartmental analysis to determine various PK parametersThe PK parameters included the terminal elimination half-life (119879
12) maximum plasma concentration (119862max) time to
reachmaximum plasma concentration (119879max) area under thecurve (AUC
0ndashinfin) and mean residence time (MRT)
28 Statistical Analysis Continuous data were presented asmean plusmn SD and categorical data were presented as 119899 () Forcomparison between the drug and placebo at each dose levelunpaired 119905-test was used for continuous variables and Fis-cherrsquos exact test for categorical variables For comparisonbetween various dose levels ANOVAwas used 119875 value lt005was considered significant
4 Malaria Research and Treatment
Table 1 Demographic characteristics of the volunteers included in the studies
Characteristic 80mg 160mg 320mg 400mg 500mg 600mg 700mg Placebo119873 = 6 119873 = 6 119873 = 6 119873 = 6 119873 = 6 119873 = 6 119873 = 2 119873 = 12
Age in years Mean (SD) 285 (1093) 275 (432) 250 (712) 252 (213) 213 (353) 252 (767) 230 (141) 254 (575)Height in cm Mean (SD) 1705 (533) 1675 (58) 1667 (644) 1673 (408) 1670 (357) 1702 (577) 1710 (141) 1713 (489)Weight in kg Mean (SD) 586 (972) 690 (1357) 566 (884) 616 (717) 596 (647) 613 (1267) 635 (212) 607 (843)BMI (kgm2) Mean (SD) 201 (304) 248 (589) 203 (214) 220 (235) 214 (25) 217 (036) 207 (275) 214 (34)
Table 2 Adverse events noted at various drug dosages of CDRI9778
Treatment group Type of adverse events No of events80mg CDRI 9778 Heaviness of head 1160mg CDRI 9778 None320mg CDRI 9778 Visual disturbance 1
400mg CDRI 9778Drowsiness 1Bradycardia 1Itching 1
500mg CDRI 9778 Sedation 1Nausea 1
600 and 700mg CDRI 9778 Sedation 1
Placebo
Sedation 1Drowsiness 1Nausea 1Retching 1Dizziness 1
Heaviness of head 1
3 Results
63 volunteers were screened out of whom 50 volunteersmatched the inclusionexclusion criteria andwere included inthe safety study (Figure 2) For the PK study 16 healthy malevolunteers were included after screening of 20 volunteers Asrequired by the study protocol all the volunteers were male(Figure 2) There was no significant difference in the demo-graphic parameters like age (119875 = 07) height (119875 = 05)weight (119875 = 05) and body mass index (119875 = 03) amongparticipants in various treatment groups (Table 1)
31 Adverse Events Adverse events that occurred during thestudy were few (Table 2) and largely of severity grade 1 to 2(Table 2)There was no significant difference in the incidenceof events in the drug and the placebo groups (119875 = 043)
Sedation was the most common adverse event reportedacross different groups (314 214) It was noted in 3 vol-unteers given 500mg CDRI 9778 600mg CDRI 9778 andplacebo about 2 hours after drug administration and lastedfor 1-2 hours It was grade 1-2 in severity spontaneous andcomplete recoverywas seen in all and no actionwas requiredThe other adverse events noted were mild drowsiness mildnausea slight heaviness of head bradycardia (56-57 bpm)visual disturbances and itching (Table 3)
Severe adverse event nausea and retching immediatelyafter drug administration was observed in one patient whichlasted for 10minutes the patient also complained of dizzinessand slight heaviness of head 1 hour after drug administrationOn decoding he was found to have received placebo Thesymptoms resolved spontaneously hence no further actionneeded to be taken
32 Clinical Parameters At baseline the different treatmentgroups were similar in terms of clinical parameters (pulserate blood pressure and respiratory rate) None of the treat-ment groups demonstrated a significant alteration in pulserate respiratory rate and systolic blood pressure at any timepoint compared to baseline However there was a significantchange in diastolic blood pressure in 600 and 700mg CDRI9778 group (7687plusmn 874 7837plusmn 886 7925plusmn 1346 6712plusmn649 7312plusmn1232 7587plusmn811 74plusmn11 and 75plusmn1003mmHgat 0 05 1 2 4 6 8 and 12 hours respectively 119875 = 002)although clinically significant declinewas not observed in anyof the volunteers Statistical significance was observed forbetween group comparison of systolic and diastolic bloodpressures 2 hours after drug administration The SBP for80mg 160mg 320mg 400mg 500mg 600mg 700mgand placebo groups were 11217 plusmn 624 1195 plusmn 517 1275 plusmn638 11183plusmn791 1145plusmn834 11283plusmn618 1155plusmn212 and11633 plusmn 877 respectively (119875 = 001) The DBP for 80mg160mg 320mg 400mg 500mg 600mg 700mg andplacebo groups were 73 plusmn 521 7717 plusmn 806 8233 plusmn 4687133plusmn819 7183plusmn781 665plusmn653 69plusmn848 and 7375plusmn824(119875 = 003) Respiratory rate was found to be significantlydifferent between treatment groups 4 6 and 8 hours afterdrug administration although this was not clinically relevant
There was no statistically or clinically significant dif-ference noted in the corrected QT interval within varioustreatment groups (119875 = 0656 0523 0901 0348 0809 and043 respectively for 80 160 320 400 500 and 600700mggroups)
33 Hematological Parameters Hemoglobin values demon-strated a statistically significant alteration during posttreat-ment period in the group receiving 400mg CDRI 9778(1425 plusmn 075 1492 plusmn 094 and 1435 plusmn 110 gm at baseline24 hr and 7th day respectively 119875 = 002) A statistically sig-nificant change in platelet counts was also observed in 320mgCDRI 9778 group (190 plusmn 68 190 plusmn 69 and 212 plusmn 66(times1012)L respectively 119875 = 004) All these values were wellwithin normal limits Other haematological parameterswhich showed statistically significant difference however
Malaria Research and Treatment 5
Table3Descriptio
nof
alladverse
eventsob
served
inthes
tudy
Nam
eofA
ETreatm
entg
roup
Treatm
entg
iven
Time(hrs)of
onset
after
drug
administratio
n
Durationof
AE
(min)
Spon
taneou
sreversal(yes
orno
)Re
versalcomplete
(yes
orno
)Severitygrade
Causalityassessment
Sedatio
n60
0mg
Non
e2
60Yes
Yes
1-2Po
ssible
Sedatio
n500mg
Non
e2
120
Yes
Yes
1-2Po
ssible
Sedatio
nPlacebo
Non
e2
120
Yes
Yes
1-2Not
drug
related
Drowsin
ess
400mg
Non
e2
60Yes
Yes
1Po
ssible
Drowsin
ess
Placebo
Non
e15
140
Yes
Yes
1Not
drug
related
Nausea
500mg
Non
e025
20Yes
Yes
1Po
ssible
Nausea
Placebo
Non
eIm
mediate
10Yes
Yes
3Not
drug
related
Heavinessof
head
80mg
Non
e025
15Yes
Yes
1Po
ssible
Heavinessof
head
Placebo
Non
e1
10Yes
Yes
1Not
drug
related
Visualdistu
rbances
320mg
Non
e36
2-3
Yes
Yes
1Re
mote
Bradycardia
400mg
Non
e1
60Yes
Yes
1Po
ssible
Retching
Placebo
Non
eIm
mediate
10Yes
Yes
3Not
drug
related
Itching
400mg
Non
e24
8Yes
Yes
1Po
ssible
Dizziness
Placebo
Non
e1
10Yes
Yes
3Not
drug
related
Severitygradingdo
neaccordingto
Com
mon
Term
inolog
yCr
iteria
forA
dverse
Eventsv40U
SDepartm
ento
fHealth
andHum
anServicesG
rade
1Mild
asymptom
aticor
mild
symptom
sclinicalord
iagn
ostic
observations
onlyinterventionno
tind
icatedG
rade
2Mod
erateminim
allocalor
noninvasiveinterventionindicatedGrade
3Severeor
medicallysig
nificantb
utno
timmediatelylife-threateningho
spita
lization
orprolon
gatio
nof
hospita
lizationindicateddisablingGrade
4Life-th
reateningconsequencesurgentinterventionindicatedGrade
5Death
relatedto
AE
Causality
assessmentNon
eremote(lt5
chance
ofbeingdrug
related)possib
le(gt5
butle
50chance
ofbeingdrug
relatedprobable(gt50chance
ofbeingdrug
related)
anddefin
ite
Grade
3severitymdash
volunteerw
ason
placebo
6 Malaria Research and Treatment
Excluded 13
Screened n = 63
Did not meet inclusionexclusion criteria n = 5
Refused consent n = 8
Randomized n = 50
Completed n = 12
Analyzed n = 50
Placebo n = 12 CDRI 9778 n = 38
Completed n = 38
Withdrawals n = 0
Dropouts n = 0
(a)
Flow of participants through the pharmacokinetic study
Enrolled and included in final
Screened (n = 20)
analysis (n = 16)
meet inclusion criteria n = 3
Refused consent n = 1 did not
(b)
Figure 2 Volunteer screening flowchart for ascending dose study 50 normal healthy human volunteers were screened from 63 volunteerswhile for single dose pharmacokinetics study 16 healthy volunteers were from 20 volunteers
remained well within normal range and did not demonstrateany dose response relationship were PCV total leukocyte andlymphocyte counts RBC counts and methemoglobin levels
34 Biochemical Parameters There was no significant differ-ence in serumbilirubin SGOT and SGPT at any time point ofmeasurement for intergroup comparisons The values ofserum alkaline phosphatase however were significantly dif-ferent between various groups at all pre- and postdrug mea-surements Post hoc analysis for this revealed that the resultswere significant for comparisons between lowest (80mgCDRI 9778) and higher doses (500 and 600mgCDRI 9778)although none of the groups was significantly differentfrom placebo All the values remained within normal range(Table 4) The other biochemical parameters which showedsignificant changes between groups were serum albumin
serum globulin and blood glucose and serum HDL levelsHowever they remained within the normal laboratory rangeand did not cause any sign or symptoms and there was nodose response relationship noted
35 Serum Electrolyte Levels The groups demonstrated sig-nificant variation in serum sodium and serum potassiumvalues at all time points of measurements None of the volun-teers had values outside the normal physiological ranges norpresented with any signs or symptoms of dyselectrolytemiaso these findings were considered clinically irrelevant
36 Pharmacokinetic Analysis Following oral administrationat 200mg compound 9778 was rapidly absorbed getsimmediately converted into active metabolite 9763 andis eliminated from the systemic circulation within 48 h
Malaria Research and Treatment 7
Table4Com
paris
onof
liver
functio
ntests
betweenvario
ustre
atmentg
roup
sonrepeated
observations
atbaselin
e24
hoursa
ndday7
Treatm
entg
roup
sTo
talserum
bilirub
inSerum
SGOT
Serum
SGPT
Serum
Alkalinep
hosphatase
Baselin
e24
hour
Day
7Ba
selin
e24
hour
Day
7Ba
selin
e24
hour
Day
7Ba
selin
e24
hour
Day
780
mg(119899=6)082plusmn024073plusmn024064plusmn0232215plusmn632348plusmn288277plusmn612188plusmn100262plusmn66218plusmn37955plusmn26651025plusmn300910683plusmn3712
160m
g(119899=6)076plusmn039055plusmn00706plusmn0063418plusmn7893398plusmn9693833plusmn8913721plusmn4163943plusmn808445plusmn11642115plusmn6865212plusmn6720717plusmn6103
320m
g(119899=6)073plusmn05208plusmn04087plusmn0593283plusmn5153417plusmn77635plusmn8533383plusmn9093733plusmn8873833plusmn1384242plusmn45242225plusmn345523583plusmn3249
400m
g(119899=6)052plusmn004053plusmn005055plusmn0082667plusmn662315plusmn453233plusmn88729plusmn5443517plusmn41238plusmn129523283plusmn4225167plusmn475924283plusmn3482
500m
g(119899=6)052plusmn004052plusmn004053plusmn0053133plusmn876315plusmn60234plusmn6003283plusmn1153483plusmn11073533plusmn105632117plusmn151313plusmn124533967plusmn18425
600m
g(119899=6)08plusmn05408plusmn059082plusmn0593117plusmn633033plusmn6743133plusmn57830plusmn716305plusmn8463317plusmn10532725plusmn667127583plusmn6129274plusmn7517
700m
g(119899=2)06plusmn01406plusmn014055plusmn007355plusmn07140plusmn424345plusmn07146plusmn566465plusmn49540plusmn11312615plusmn502254plusmn56572605plusmn4455
Placebo(119899=12)055plusmn007056plusmn006055plusmn0123191plusmn9673117plusmn918305plusmn8153708plusmn18113858plusmn19563583plusmn1811208plusmn6823208plusmn655620858plusmn7223
ANOVA119865
1114
1308
1105
1701
1631
114
162
1097
1435
4545
5103
3802
df49
4949
4949
4949
4949
4949
49119875
037
027
038
013
015
036
016
038
022
lt0001lowast
lt0001lowastlowast
0002
lowast119875=0002for5
00mgcomparedto
80mgdrug
and119875=002for6
00mgcomparedto
80mgdrug
(Scheffersquos
test)
lowastlowast119875=0001and000
6for8
0mgdrug
comparedto
500and60
0mgdrug
respectiv
ely(Scheffersquos
test)
119875=0006forc
omparis
onbetween80
and500m
gdrug
grou
ps(Scheffersquos
test)
Nodifferencefrom
placeboin
anycomparis
on
8 Malaria Research and Treatment
Table 5 Pharmacokinetic parameters of converted active metabolite 9763 after oral administration of 9778 at 200mg single dose to malehealthy human volunteers (119873 = 16)
PKparameter
Converted in vivometabolite 9763Mean plusmn SEMMale healthy human volunteers (119873 = 16)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16119862max(ngmL) 172 201 373 187 149 355 426 202 609 295 474 504 654 105 55 123 14393 plusmn 2832
119879max (h) 15 4 1 2 15 2 4 4 4 2 2 2 15 15 2 15 228 plusmn 02711987912
(h) 1389 217 478 220 388 2127 300 894 780 1163 2426 1450 1010 1773 2451 1890 1185 plusmn 194AUC0minusinfin
(ngsdothmL) 7887 1048 1644 6026 785 15226 2079 16049 5117 18989 935 3561 5836 6968 8331 9841 87874plusmn13315
MRT (h) 1257 572 137 353 538 1425 642 1413 928 976 3072 1453 1126 1837 3220 1852 1377 plusmn 205
Mea
n pl
asm
a con
sn (
ngm
L)
158
138
118
98
78
58
38
18
minus2minus2 8 18 28 38 48 58 68 78
Time (h)
Converted active metabolite 97ndash63
Figure 3 Mean plasma concentration-time profile of in vivo activemetabolite 9763 after oral administration of 9778 at 200mg singledose to male healthy human volunteers (119873 = 16)
except in two volunteers (72 h) as observed from plasmaconcentration-time profile (Figure 3) PK parameters gener-ated in individual volunteers have been shown in Table 5119879max of active metabolite 9763 was found to be 228 plusmn 027 hwith 119862max of 14393 plusmn 2832 Mean values of 119879
12 MRT and
AUC0ndashinfin of 9763were 505plusmn057 h 973plusmn106 h and 84522plusmn
14296 ngsdothmL respectively Active metabolite 9763 wasquantified from 05 h and up to 48 h in healthy volunteerswith exception to two volunteers in whom it was observed upto 72 h No additional metabolite peaks were observed duringanalysis except 9763 In most of the volunteers parentmolecule 9778was below the limit of quantitationMoreoververy low concentrations of 9778were observed in some volu-nteers but these were not sufficient for generating the PKparameters
4 Discussion
This was a first-in-human study conducted on healthy malevolunteers for a new antimalarial drug CDRI 9778 Overallthe drug was found to be safe
Few adverse events were reported which were of mildnature and were probable in causality But the adverse eventswere neither clinically nor statistically significant The 14adverse events reported in this trial occurred in various treat-ment groups over a large time frame Hence it cannot be said
definitelywhether theywere due to the drug or notMoreoversimilar adverse events were also seen in the placebo groupEven the statistically significant alteration in blood pressurewas not associated with signs and symptoms of altered bloodpressure and the values fell within normal ranges
For none of the adverse events any intervention in theform of drug administration fluid substitution and resusci-tation was required All the reported events continued to beobserved and resolved spontaneously
The severity of the adverse events was at best graded at 2No serious adverse events were reported The NCE underevaluation is a derivative of artemisinin compound which israrely associatedwith any SAEHowever structural similarityis just an indicator for predicting adverse effect profile of anovel compound A future possibility of such reactions com-ing into light always remains
Hence theMTD could not be determinedThough deter-mination of MTD was the main purpose of the study thiscould not be achieved This is a definite possibility in phase Istudies as has been seen previously [21 22] For the determi-nation of dose for multiple ascending dose study data frompreclinical efficacy studies will be used which is found to liewell within the highest dose evaluated in the present study
Therewere some haematological and biochemical param-eters which showed statistically significant values when com-pared to placebo but the differences were not clinically sig-nificant as most of them stayed within the normal laboratoryrange Further the absence of dose response relationshiphighlighted the fact that they were innocuous Nonclinicaltoxicity data serves as a guide to the monitoring of adversedrug events once the studies are conducted in healthy volun-teers Though there were no specific concerns raised in non-clinical toxicity a thorough evaluation of haematological andbiochemical parameters was undertaken Statistically signif-icant differences should be interpreted with caution keepingin mind the clinical relevance [23 24]
Since structurally the compound was similar to arte-misinin which has been reported to prolong QTc interval[25] a careful evaluation of QT interval was also undertakenThiswas also undertaken for assessing a future need to under-take a thoroughQT study No clinicallymeaningful alterationofQT interval as laid down in E 14 guidance document forQTevaluation [26] was observed
Malaria Research and Treatment 9
5 Conclusion
In conclusion we can say that the new compound CDRI9778 appears to be a safe and tolerable drug Its safety can befurther tested in multiple dose studies and if found tolerablecan be a good therapeutic option for malaria especiallymalaria resistant to available drugs
Conflict of Interests
The investigators did not receive any money for the conductof the study The study was sponsored by the Central DrugResearch Institute India The Innovator Institute a govern-ment organization had tied up with IPCA Ltd for the man-ufacture of the drug The drugs were supplied by IPCA LtdThey had no role in data collection recording and reportingTwo of the authors Dr Nitin Chandorkar and Dr AnilPareek are employees of IPCA Their role was in designingand conducting the study All the analyses were done inde-pendently by the investigatorsrsquo team
Acknowledgments
The authors would like to acknowledge the efforts of MrOnkar Rathod for helping in the execution of the study andMr Mitesh Sharma for giving his inputs for statistical analy-sis The research was funded by Central Drug Research Insti-tute (CSIR) Lucknow India This is a government organiza-tion
References
[1] ldquoWorldMalaria Reportrdquo 2005 httpwwwrollbackmalariaorgwmr2005
[2] A V Kondrashin ldquoMalaria in theWHOSoutheast Asia regionrdquoIndian Journal of Malariology vol 29 no 3 pp 129ndash160 1992
[3] U Arora G S Sonal G P S Dhillon andH GThakor ldquoEmer-gence of drug resistance in Indiardquo Journal of the Indian MedicalAssociation vol 106 no 10 pp 678ndash681 2008
[4] B M Greenwood D A Fidock D E Kyle et al ldquoMalaria pro-gress perils and prospects for eradicationrdquo Journal of ClinicalInvestigation vol 118 no 4 pp 1266ndash1276 2008
[5] C Singh and S K Puri ldquoSubstituted 124-trioxanes as anti-malarial agents and a process of producing the substituted 124-trioxanerdquo US Patent no 6316493 B1 2001
[6] C Singh N Gupta and S K Puri ldquoPhoto-oxygenation of ger-aniol synthesis of a novel series of hydroxy-functionalized anti-malarial 124-trioxanesrdquo Bioorganic and Medicinal ChemistryLetters vol 12 no 15 pp 1913ndash1916 2002
[7] C Singh N Gupta and S K Puri ldquoGeraniol-derived 124-trioxanes with potent in-vivo antimalarial activityrdquo Bioorganicand Medicinal Chemistry Letters vol 13 no 20 pp 3447ndash34502003
[8] C Singh N C Srivastav and S K Puri ldquoSynthesis and anti-malarial activity of 6-cycloalkylvinyl substituted 124-tri-oxanesrdquo Bioorganic andMedicinal Chemistry vol 12 no 22 pp5745ndash5752 2004
[9] A G Griesbeck T T El-Idreesy L-O Hoinck J Lex and RBrun ldquoNovel spiroanellated 124-trioxanes with high in vitro
antimalarial activitiesrdquo Bioorganic and Medicinal ChemistryLetters vol 15 no 3 pp 595ndash597 2005
[10] C Singh H Malik and S K Puri ldquoOrally active amino func-tionalized antimalarial 124-trioxanesrdquo Bioorganic and Medici-nal Chemistry Letters vol 14 no 2 pp 459ndash462 2004
[11] C SinghNGupta and S K Puri ldquoPhotooxygenation of 3-aryl-2-cyclohexenols synthesis of a new series of antimalarial 124-trioxanesrdquo Tetrahedron Letters vol 46 no 2 pp 205ndash207 2005
[12] C Singh HMalik and S K Puri ldquoOrally active 124-trioxanessynthesis and antimalarial assessment of a new series of 9-functionalized 3-(1-arylvinyl)-125-trioxaspiro[55]undecanesagainst multi-drug-resistant Plasmodium yoelii nigeriensis inmicerdquo Journal of Medicinal Chemistry vol 49 no 9 pp 2794ndash2803 2006
[13] C Singh S Chaudhary and S K Puri ldquoNew orally active deri-vatives of artemisinin with high efficacy against multidrug-resistant malaria in micerdquo Journal of Medicinal Chemistry vol49 no 24 pp 7227ndash7233 2006
[14] C Singh U Sharma G Saxena and S K Puri ldquoOrally activeantimalarials synthesis and bioevaluation of a new series ofsteroid-based 124-trioxanes against multi-drug resistantmalaria in micerdquo Bioorganic and Medicinal Chemistry Lettersvol 17 no 15 pp 4097ndash4101 2007
[15] C Singh R Kanchan U Sharma and S K Puri ldquoNewadamantane-based spiro 124-trioxanes orally effective againstrodent and simianmalariardquo Journal ofMedicinal Chemistry vol50 no 3 pp 521ndash527 2007
[16] C Singh S Chaudhary RKanchan and SK Puri ldquoConversionof antimalarial drug artemisinin to a new series of tricyclic 124-trioxanesrdquo Organic Letters vol 9 no 21 pp 4327ndash4329 2007
[17] C Singh V P Verma N K Naikade A S Singh M Hassamand S K Puri ldquoNovel bis- and tris-124-trioxanes synthesis andantimalarial activity against multidrug-resistant Plasmodiumyoelii in swiss micerdquo Journal of Medicinal Chemistry vol 51 no23 pp 7581ndash7592 2008
[18] R P Singh S Sabarinath N Gautam R C Gupta and S KSingh ldquoPharmacokinetic study of the novel synthetic trioxaneantimalarial compound 97-78 in rats using an LC-MSMSmethod for quantificationrdquo Arzneimittel-Forschung vol 61 no2 pp 120ndash125 2011
[19] R P Singh S Sabarinath N Gautam R C Gupta and S KSingh ldquoLiquid chromatographic tandem mass spectrometricassay for quantification of 9778 and its metabolite 9763 apromising trioxane antimalarial in monkey plasmardquo Journal ofChromatography B vol 877 no 22 pp 2074ndash2080 2009
[20] V P Shah K K Midha J W A Findlay et al ldquoBioanalyticalmethod validationmdasha revisit with a decade of progressrdquo Phar-maceutical Research vol 17 no 12 pp 1551ndash1557 2000
[21] E RGerstner A F Eichler S R Plotkin et al ldquoPhase I trial withbiomarker studies of vatalanib (PTK787) in patients with newlydiagnosed glioblastoma treated with enzyme inducing anti-epileptic drugs and standard radiation and temozolomiderdquoJournal of Neuro-Oncology vol 103 no 2 pp 325ndash332 2011
[22] A Forero-Torres J Shah TWood et al ldquoPhase I trial of weeklytigatuzumab an agonistic humanizedmonoclonal antibody tar-geting death receptor 5 (DR5)rdquo Cancer Biotherapy and Radio-pharmaceuticals vol 25 no 1 pp 13ndash19 2010
[23] R C Kane ldquoThe clinical significance of statistical significancerdquoOncologist vol 13 no 11 pp 1129ndash1133 2008
[24] M J Hayat ldquoUnderstanding statistical significancerdquo NursingResearch vol 59 no 3 pp 219ndash223 2010
10 Malaria Research and Treatment
[25] I R Ribeiro and P Olliaro ldquoSafety of artemisinin and its deriva-tives A review of published and unpublished clinical trialsrdquoMedecine Tropicale vol 58 no 3 supplement pp 50ndash53 1998
[26] 2013 httpwwwfdagovdownloadsDrugsGuidanceCompli-anceRegulatoryInformationGuidancesucm073161pdf
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
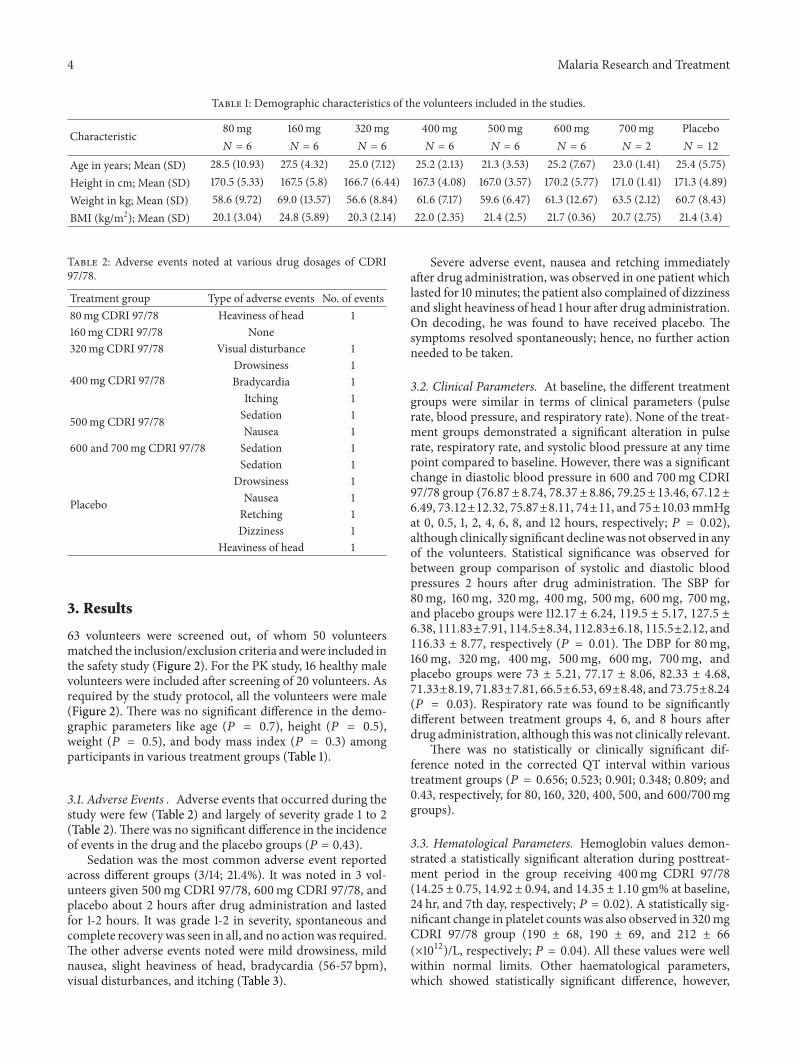
4 Malaria Research and Treatment
Table 1 Demographic characteristics of the volunteers included in the studies
Characteristic 80mg 160mg 320mg 400mg 500mg 600mg 700mg Placebo119873 = 6 119873 = 6 119873 = 6 119873 = 6 119873 = 6 119873 = 6 119873 = 2 119873 = 12
Age in years Mean (SD) 285 (1093) 275 (432) 250 (712) 252 (213) 213 (353) 252 (767) 230 (141) 254 (575)Height in cm Mean (SD) 1705 (533) 1675 (58) 1667 (644) 1673 (408) 1670 (357) 1702 (577) 1710 (141) 1713 (489)Weight in kg Mean (SD) 586 (972) 690 (1357) 566 (884) 616 (717) 596 (647) 613 (1267) 635 (212) 607 (843)BMI (kgm2) Mean (SD) 201 (304) 248 (589) 203 (214) 220 (235) 214 (25) 217 (036) 207 (275) 214 (34)
Table 2 Adverse events noted at various drug dosages of CDRI9778
Treatment group Type of adverse events No of events80mg CDRI 9778 Heaviness of head 1160mg CDRI 9778 None320mg CDRI 9778 Visual disturbance 1
400mg CDRI 9778Drowsiness 1Bradycardia 1Itching 1
500mg CDRI 9778 Sedation 1Nausea 1
600 and 700mg CDRI 9778 Sedation 1
Placebo
Sedation 1Drowsiness 1Nausea 1Retching 1Dizziness 1
Heaviness of head 1
3 Results
63 volunteers were screened out of whom 50 volunteersmatched the inclusionexclusion criteria andwere included inthe safety study (Figure 2) For the PK study 16 healthy malevolunteers were included after screening of 20 volunteers Asrequired by the study protocol all the volunteers were male(Figure 2) There was no significant difference in the demo-graphic parameters like age (119875 = 07) height (119875 = 05)weight (119875 = 05) and body mass index (119875 = 03) amongparticipants in various treatment groups (Table 1)
31 Adverse Events Adverse events that occurred during thestudy were few (Table 2) and largely of severity grade 1 to 2(Table 2)There was no significant difference in the incidenceof events in the drug and the placebo groups (119875 = 043)
Sedation was the most common adverse event reportedacross different groups (314 214) It was noted in 3 vol-unteers given 500mg CDRI 9778 600mg CDRI 9778 andplacebo about 2 hours after drug administration and lastedfor 1-2 hours It was grade 1-2 in severity spontaneous andcomplete recoverywas seen in all and no actionwas requiredThe other adverse events noted were mild drowsiness mildnausea slight heaviness of head bradycardia (56-57 bpm)visual disturbances and itching (Table 3)
Severe adverse event nausea and retching immediatelyafter drug administration was observed in one patient whichlasted for 10minutes the patient also complained of dizzinessand slight heaviness of head 1 hour after drug administrationOn decoding he was found to have received placebo Thesymptoms resolved spontaneously hence no further actionneeded to be taken
32 Clinical Parameters At baseline the different treatmentgroups were similar in terms of clinical parameters (pulserate blood pressure and respiratory rate) None of the treat-ment groups demonstrated a significant alteration in pulserate respiratory rate and systolic blood pressure at any timepoint compared to baseline However there was a significantchange in diastolic blood pressure in 600 and 700mg CDRI9778 group (7687plusmn 874 7837plusmn 886 7925plusmn 1346 6712plusmn649 7312plusmn1232 7587plusmn811 74plusmn11 and 75plusmn1003mmHgat 0 05 1 2 4 6 8 and 12 hours respectively 119875 = 002)although clinically significant declinewas not observed in anyof the volunteers Statistical significance was observed forbetween group comparison of systolic and diastolic bloodpressures 2 hours after drug administration The SBP for80mg 160mg 320mg 400mg 500mg 600mg 700mgand placebo groups were 11217 plusmn 624 1195 plusmn 517 1275 plusmn638 11183plusmn791 1145plusmn834 11283plusmn618 1155plusmn212 and11633 plusmn 877 respectively (119875 = 001) The DBP for 80mg160mg 320mg 400mg 500mg 600mg 700mg andplacebo groups were 73 plusmn 521 7717 plusmn 806 8233 plusmn 4687133plusmn819 7183plusmn781 665plusmn653 69plusmn848 and 7375plusmn824(119875 = 003) Respiratory rate was found to be significantlydifferent between treatment groups 4 6 and 8 hours afterdrug administration although this was not clinically relevant
There was no statistically or clinically significant dif-ference noted in the corrected QT interval within varioustreatment groups (119875 = 0656 0523 0901 0348 0809 and043 respectively for 80 160 320 400 500 and 600700mggroups)
33 Hematological Parameters Hemoglobin values demon-strated a statistically significant alteration during posttreat-ment period in the group receiving 400mg CDRI 9778(1425 plusmn 075 1492 plusmn 094 and 1435 plusmn 110 gm at baseline24 hr and 7th day respectively 119875 = 002) A statistically sig-nificant change in platelet counts was also observed in 320mgCDRI 9778 group (190 plusmn 68 190 plusmn 69 and 212 plusmn 66(times1012)L respectively 119875 = 004) All these values were wellwithin normal limits Other haematological parameterswhich showed statistically significant difference however
Malaria Research and Treatment 5
Table3Descriptio
nof
alladverse
eventsob
served
inthes
tudy
Nam
eofA
ETreatm
entg
roup
Treatm
entg
iven
Time(hrs)of
onset
after
drug
administratio
n
Durationof
AE
(min)
Spon
taneou
sreversal(yes
orno
)Re
versalcomplete
(yes
orno
)Severitygrade
Causalityassessment
Sedatio
n60
0mg
Non
e2
60Yes
Yes
1-2Po
ssible
Sedatio
n500mg
Non
e2
120
Yes
Yes
1-2Po
ssible
Sedatio
nPlacebo
Non
e2
120
Yes
Yes
1-2Not
drug
related
Drowsin
ess
400mg
Non
e2
60Yes
Yes
1Po
ssible
Drowsin
ess
Placebo
Non
e15
140
Yes
Yes
1Not
drug
related
Nausea
500mg
Non
e025
20Yes
Yes
1Po
ssible
Nausea
Placebo
Non
eIm
mediate
10Yes
Yes
3Not
drug
related
Heavinessof
head
80mg
Non
e025
15Yes
Yes
1Po
ssible
Heavinessof
head
Placebo
Non
e1
10Yes
Yes
1Not
drug
related
Visualdistu
rbances
320mg
Non
e36
2-3
Yes
Yes
1Re
mote
Bradycardia
400mg
Non
e1
60Yes
Yes
1Po
ssible
Retching
Placebo
Non
eIm
mediate
10Yes
Yes
3Not
drug
related
Itching
400mg
Non
e24
8Yes
Yes
1Po
ssible
Dizziness
Placebo
Non
e1
10Yes
Yes
3Not
drug
related
Severitygradingdo
neaccordingto
Com
mon
Term
inolog
yCr
iteria
forA
dverse
Eventsv40U
SDepartm
ento
fHealth
andHum
anServicesG
rade
1Mild
asymptom
aticor
mild
symptom
sclinicalord
iagn
ostic
observations
onlyinterventionno
tind
icatedG
rade
2Mod
erateminim
allocalor
noninvasiveinterventionindicatedGrade
3Severeor
medicallysig
nificantb
utno
timmediatelylife-threateningho
spita
lization
orprolon
gatio
nof
hospita
lizationindicateddisablingGrade
4Life-th
reateningconsequencesurgentinterventionindicatedGrade
5Death
relatedto
AE
Causality
assessmentNon
eremote(lt5
chance
ofbeingdrug
related)possib
le(gt5
butle
50chance
ofbeingdrug
relatedprobable(gt50chance
ofbeingdrug
related)
anddefin
ite
Grade
3severitymdash
volunteerw
ason
placebo
6 Malaria Research and Treatment
Excluded 13
Screened n = 63
Did not meet inclusionexclusion criteria n = 5
Refused consent n = 8
Randomized n = 50
Completed n = 12
Analyzed n = 50
Placebo n = 12 CDRI 9778 n = 38
Completed n = 38
Withdrawals n = 0
Dropouts n = 0
(a)
Flow of participants through the pharmacokinetic study
Enrolled and included in final
Screened (n = 20)
analysis (n = 16)
meet inclusion criteria n = 3
Refused consent n = 1 did not
(b)
Figure 2 Volunteer screening flowchart for ascending dose study 50 normal healthy human volunteers were screened from 63 volunteerswhile for single dose pharmacokinetics study 16 healthy volunteers were from 20 volunteers
remained well within normal range and did not demonstrateany dose response relationship were PCV total leukocyte andlymphocyte counts RBC counts and methemoglobin levels
34 Biochemical Parameters There was no significant differ-ence in serumbilirubin SGOT and SGPT at any time point ofmeasurement for intergroup comparisons The values ofserum alkaline phosphatase however were significantly dif-ferent between various groups at all pre- and postdrug mea-surements Post hoc analysis for this revealed that the resultswere significant for comparisons between lowest (80mgCDRI 9778) and higher doses (500 and 600mgCDRI 9778)although none of the groups was significantly differentfrom placebo All the values remained within normal range(Table 4) The other biochemical parameters which showedsignificant changes between groups were serum albumin
serum globulin and blood glucose and serum HDL levelsHowever they remained within the normal laboratory rangeand did not cause any sign or symptoms and there was nodose response relationship noted
35 Serum Electrolyte Levels The groups demonstrated sig-nificant variation in serum sodium and serum potassiumvalues at all time points of measurements None of the volun-teers had values outside the normal physiological ranges norpresented with any signs or symptoms of dyselectrolytemiaso these findings were considered clinically irrelevant
36 Pharmacokinetic Analysis Following oral administrationat 200mg compound 9778 was rapidly absorbed getsimmediately converted into active metabolite 9763 andis eliminated from the systemic circulation within 48 h
Malaria Research and Treatment 7
Table4Com
paris
onof
liver
functio
ntests
betweenvario
ustre
atmentg
roup
sonrepeated
observations
atbaselin
e24
hoursa
ndday7
Treatm
entg
roup
sTo
talserum
bilirub
inSerum
SGOT
Serum
SGPT
Serum
Alkalinep
hosphatase
Baselin
e24
hour
Day
7Ba
selin
e24
hour
Day
7Ba
selin
e24
hour
Day
7Ba
selin
e24
hour
Day
780
mg(119899=6)082plusmn024073plusmn024064plusmn0232215plusmn632348plusmn288277plusmn612188plusmn100262plusmn66218plusmn37955plusmn26651025plusmn300910683plusmn3712
160m
g(119899=6)076plusmn039055plusmn00706plusmn0063418plusmn7893398plusmn9693833plusmn8913721plusmn4163943plusmn808445plusmn11642115plusmn6865212plusmn6720717plusmn6103
320m
g(119899=6)073plusmn05208plusmn04087plusmn0593283plusmn5153417plusmn77635plusmn8533383plusmn9093733plusmn8873833plusmn1384242plusmn45242225plusmn345523583plusmn3249
400m
g(119899=6)052plusmn004053plusmn005055plusmn0082667plusmn662315plusmn453233plusmn88729plusmn5443517plusmn41238plusmn129523283plusmn4225167plusmn475924283plusmn3482
500m
g(119899=6)052plusmn004052plusmn004053plusmn0053133plusmn876315plusmn60234plusmn6003283plusmn1153483plusmn11073533plusmn105632117plusmn151313plusmn124533967plusmn18425
600m
g(119899=6)08plusmn05408plusmn059082plusmn0593117plusmn633033plusmn6743133plusmn57830plusmn716305plusmn8463317plusmn10532725plusmn667127583plusmn6129274plusmn7517
700m
g(119899=2)06plusmn01406plusmn014055plusmn007355plusmn07140plusmn424345plusmn07146plusmn566465plusmn49540plusmn11312615plusmn502254plusmn56572605plusmn4455
Placebo(119899=12)055plusmn007056plusmn006055plusmn0123191plusmn9673117plusmn918305plusmn8153708plusmn18113858plusmn19563583plusmn1811208plusmn6823208plusmn655620858plusmn7223
ANOVA119865
1114
1308
1105
1701
1631
114
162
1097
1435
4545
5103
3802
df49
4949
4949
4949
4949
4949
49119875
037
027
038
013
015
036
016
038
022
lt0001lowast
lt0001lowastlowast
0002
lowast119875=0002for5
00mgcomparedto
80mgdrug
and119875=002for6
00mgcomparedto
80mgdrug
(Scheffersquos
test)
lowastlowast119875=0001and000
6for8
0mgdrug
comparedto
500and60
0mgdrug
respectiv
ely(Scheffersquos
test)
119875=0006forc
omparis
onbetween80
and500m
gdrug
grou
ps(Scheffersquos
test)
Nodifferencefrom
placeboin
anycomparis
on
8 Malaria Research and Treatment
Table 5 Pharmacokinetic parameters of converted active metabolite 9763 after oral administration of 9778 at 200mg single dose to malehealthy human volunteers (119873 = 16)
PKparameter
Converted in vivometabolite 9763Mean plusmn SEMMale healthy human volunteers (119873 = 16)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16119862max(ngmL) 172 201 373 187 149 355 426 202 609 295 474 504 654 105 55 123 14393 plusmn 2832
119879max (h) 15 4 1 2 15 2 4 4 4 2 2 2 15 15 2 15 228 plusmn 02711987912
(h) 1389 217 478 220 388 2127 300 894 780 1163 2426 1450 1010 1773 2451 1890 1185 plusmn 194AUC0minusinfin
(ngsdothmL) 7887 1048 1644 6026 785 15226 2079 16049 5117 18989 935 3561 5836 6968 8331 9841 87874plusmn13315
MRT (h) 1257 572 137 353 538 1425 642 1413 928 976 3072 1453 1126 1837 3220 1852 1377 plusmn 205
Mea
n pl
asm
a con
sn (
ngm
L)
158
138
118
98
78
58
38
18
minus2minus2 8 18 28 38 48 58 68 78
Time (h)
Converted active metabolite 97ndash63
Figure 3 Mean plasma concentration-time profile of in vivo activemetabolite 9763 after oral administration of 9778 at 200mg singledose to male healthy human volunteers (119873 = 16)
except in two volunteers (72 h) as observed from plasmaconcentration-time profile (Figure 3) PK parameters gener-ated in individual volunteers have been shown in Table 5119879max of active metabolite 9763 was found to be 228 plusmn 027 hwith 119862max of 14393 plusmn 2832 Mean values of 119879
12 MRT and
AUC0ndashinfin of 9763were 505plusmn057 h 973plusmn106 h and 84522plusmn
14296 ngsdothmL respectively Active metabolite 9763 wasquantified from 05 h and up to 48 h in healthy volunteerswith exception to two volunteers in whom it was observed upto 72 h No additional metabolite peaks were observed duringanalysis except 9763 In most of the volunteers parentmolecule 9778was below the limit of quantitationMoreoververy low concentrations of 9778were observed in some volu-nteers but these were not sufficient for generating the PKparameters
4 Discussion
This was a first-in-human study conducted on healthy malevolunteers for a new antimalarial drug CDRI 9778 Overallthe drug was found to be safe
Few adverse events were reported which were of mildnature and were probable in causality But the adverse eventswere neither clinically nor statistically significant The 14adverse events reported in this trial occurred in various treat-ment groups over a large time frame Hence it cannot be said
definitelywhether theywere due to the drug or notMoreoversimilar adverse events were also seen in the placebo groupEven the statistically significant alteration in blood pressurewas not associated with signs and symptoms of altered bloodpressure and the values fell within normal ranges
For none of the adverse events any intervention in theform of drug administration fluid substitution and resusci-tation was required All the reported events continued to beobserved and resolved spontaneously
The severity of the adverse events was at best graded at 2No serious adverse events were reported The NCE underevaluation is a derivative of artemisinin compound which israrely associatedwith any SAEHowever structural similarityis just an indicator for predicting adverse effect profile of anovel compound A future possibility of such reactions com-ing into light always remains
Hence theMTD could not be determinedThough deter-mination of MTD was the main purpose of the study thiscould not be achieved This is a definite possibility in phase Istudies as has been seen previously [21 22] For the determi-nation of dose for multiple ascending dose study data frompreclinical efficacy studies will be used which is found to liewell within the highest dose evaluated in the present study
Therewere some haematological and biochemical param-eters which showed statistically significant values when com-pared to placebo but the differences were not clinically sig-nificant as most of them stayed within the normal laboratoryrange Further the absence of dose response relationshiphighlighted the fact that they were innocuous Nonclinicaltoxicity data serves as a guide to the monitoring of adversedrug events once the studies are conducted in healthy volun-teers Though there were no specific concerns raised in non-clinical toxicity a thorough evaluation of haematological andbiochemical parameters was undertaken Statistically signif-icant differences should be interpreted with caution keepingin mind the clinical relevance [23 24]
Since structurally the compound was similar to arte-misinin which has been reported to prolong QTc interval[25] a careful evaluation of QT interval was also undertakenThiswas also undertaken for assessing a future need to under-take a thoroughQT study No clinicallymeaningful alterationofQT interval as laid down in E 14 guidance document forQTevaluation [26] was observed
Malaria Research and Treatment 9
5 Conclusion
In conclusion we can say that the new compound CDRI9778 appears to be a safe and tolerable drug Its safety can befurther tested in multiple dose studies and if found tolerablecan be a good therapeutic option for malaria especiallymalaria resistant to available drugs
Conflict of Interests
The investigators did not receive any money for the conductof the study The study was sponsored by the Central DrugResearch Institute India The Innovator Institute a govern-ment organization had tied up with IPCA Ltd for the man-ufacture of the drug The drugs were supplied by IPCA LtdThey had no role in data collection recording and reportingTwo of the authors Dr Nitin Chandorkar and Dr AnilPareek are employees of IPCA Their role was in designingand conducting the study All the analyses were done inde-pendently by the investigatorsrsquo team
Acknowledgments
The authors would like to acknowledge the efforts of MrOnkar Rathod for helping in the execution of the study andMr Mitesh Sharma for giving his inputs for statistical analy-sis The research was funded by Central Drug Research Insti-tute (CSIR) Lucknow India This is a government organiza-tion
References
[1] ldquoWorldMalaria Reportrdquo 2005 httpwwwrollbackmalariaorgwmr2005
[2] A V Kondrashin ldquoMalaria in theWHOSoutheast Asia regionrdquoIndian Journal of Malariology vol 29 no 3 pp 129ndash160 1992
[3] U Arora G S Sonal G P S Dhillon andH GThakor ldquoEmer-gence of drug resistance in Indiardquo Journal of the Indian MedicalAssociation vol 106 no 10 pp 678ndash681 2008
[4] B M Greenwood D A Fidock D E Kyle et al ldquoMalaria pro-gress perils and prospects for eradicationrdquo Journal of ClinicalInvestigation vol 118 no 4 pp 1266ndash1276 2008
[5] C Singh and S K Puri ldquoSubstituted 124-trioxanes as anti-malarial agents and a process of producing the substituted 124-trioxanerdquo US Patent no 6316493 B1 2001
[6] C Singh N Gupta and S K Puri ldquoPhoto-oxygenation of ger-aniol synthesis of a novel series of hydroxy-functionalized anti-malarial 124-trioxanesrdquo Bioorganic and Medicinal ChemistryLetters vol 12 no 15 pp 1913ndash1916 2002
[7] C Singh N Gupta and S K Puri ldquoGeraniol-derived 124-trioxanes with potent in-vivo antimalarial activityrdquo Bioorganicand Medicinal Chemistry Letters vol 13 no 20 pp 3447ndash34502003
[8] C Singh N C Srivastav and S K Puri ldquoSynthesis and anti-malarial activity of 6-cycloalkylvinyl substituted 124-tri-oxanesrdquo Bioorganic andMedicinal Chemistry vol 12 no 22 pp5745ndash5752 2004
[9] A G Griesbeck T T El-Idreesy L-O Hoinck J Lex and RBrun ldquoNovel spiroanellated 124-trioxanes with high in vitro
antimalarial activitiesrdquo Bioorganic and Medicinal ChemistryLetters vol 15 no 3 pp 595ndash597 2005
[10] C Singh H Malik and S K Puri ldquoOrally active amino func-tionalized antimalarial 124-trioxanesrdquo Bioorganic and Medici-nal Chemistry Letters vol 14 no 2 pp 459ndash462 2004
[11] C SinghNGupta and S K Puri ldquoPhotooxygenation of 3-aryl-2-cyclohexenols synthesis of a new series of antimalarial 124-trioxanesrdquo Tetrahedron Letters vol 46 no 2 pp 205ndash207 2005
[12] C Singh HMalik and S K Puri ldquoOrally active 124-trioxanessynthesis and antimalarial assessment of a new series of 9-functionalized 3-(1-arylvinyl)-125-trioxaspiro[55]undecanesagainst multi-drug-resistant Plasmodium yoelii nigeriensis inmicerdquo Journal of Medicinal Chemistry vol 49 no 9 pp 2794ndash2803 2006
[13] C Singh S Chaudhary and S K Puri ldquoNew orally active deri-vatives of artemisinin with high efficacy against multidrug-resistant malaria in micerdquo Journal of Medicinal Chemistry vol49 no 24 pp 7227ndash7233 2006
[14] C Singh U Sharma G Saxena and S K Puri ldquoOrally activeantimalarials synthesis and bioevaluation of a new series ofsteroid-based 124-trioxanes against multi-drug resistantmalaria in micerdquo Bioorganic and Medicinal Chemistry Lettersvol 17 no 15 pp 4097ndash4101 2007
[15] C Singh R Kanchan U Sharma and S K Puri ldquoNewadamantane-based spiro 124-trioxanes orally effective againstrodent and simianmalariardquo Journal ofMedicinal Chemistry vol50 no 3 pp 521ndash527 2007
[16] C Singh S Chaudhary RKanchan and SK Puri ldquoConversionof antimalarial drug artemisinin to a new series of tricyclic 124-trioxanesrdquo Organic Letters vol 9 no 21 pp 4327ndash4329 2007
[17] C Singh V P Verma N K Naikade A S Singh M Hassamand S K Puri ldquoNovel bis- and tris-124-trioxanes synthesis andantimalarial activity against multidrug-resistant Plasmodiumyoelii in swiss micerdquo Journal of Medicinal Chemistry vol 51 no23 pp 7581ndash7592 2008
[18] R P Singh S Sabarinath N Gautam R C Gupta and S KSingh ldquoPharmacokinetic study of the novel synthetic trioxaneantimalarial compound 97-78 in rats using an LC-MSMSmethod for quantificationrdquo Arzneimittel-Forschung vol 61 no2 pp 120ndash125 2011
[19] R P Singh S Sabarinath N Gautam R C Gupta and S KSingh ldquoLiquid chromatographic tandem mass spectrometricassay for quantification of 9778 and its metabolite 9763 apromising trioxane antimalarial in monkey plasmardquo Journal ofChromatography B vol 877 no 22 pp 2074ndash2080 2009
[20] V P Shah K K Midha J W A Findlay et al ldquoBioanalyticalmethod validationmdasha revisit with a decade of progressrdquo Phar-maceutical Research vol 17 no 12 pp 1551ndash1557 2000
[21] E RGerstner A F Eichler S R Plotkin et al ldquoPhase I trial withbiomarker studies of vatalanib (PTK787) in patients with newlydiagnosed glioblastoma treated with enzyme inducing anti-epileptic drugs and standard radiation and temozolomiderdquoJournal of Neuro-Oncology vol 103 no 2 pp 325ndash332 2011
[22] A Forero-Torres J Shah TWood et al ldquoPhase I trial of weeklytigatuzumab an agonistic humanizedmonoclonal antibody tar-geting death receptor 5 (DR5)rdquo Cancer Biotherapy and Radio-pharmaceuticals vol 25 no 1 pp 13ndash19 2010
[23] R C Kane ldquoThe clinical significance of statistical significancerdquoOncologist vol 13 no 11 pp 1129ndash1133 2008
[24] M J Hayat ldquoUnderstanding statistical significancerdquo NursingResearch vol 59 no 3 pp 219ndash223 2010
10 Malaria Research and Treatment
[25] I R Ribeiro and P Olliaro ldquoSafety of artemisinin and its deriva-tives A review of published and unpublished clinical trialsrdquoMedecine Tropicale vol 58 no 3 supplement pp 50ndash53 1998
[26] 2013 httpwwwfdagovdownloadsDrugsGuidanceCompli-anceRegulatoryInformationGuidancesucm073161pdf
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Malaria Research and Treatment 5
Table3Descriptio
nof
alladverse
eventsob
served
inthes
tudy
Nam
eofA
ETreatm
entg
roup
Treatm
entg
iven
Time(hrs)of
onset
after
drug
administratio
n
Durationof
AE
(min)
Spon
taneou
sreversal(yes
orno
)Re
versalcomplete
(yes
orno
)Severitygrade
Causalityassessment
Sedatio
n60
0mg
Non
e2
60Yes
Yes
1-2Po
ssible
Sedatio
n500mg
Non
e2
120
Yes
Yes
1-2Po
ssible
Sedatio
nPlacebo
Non
e2
120
Yes
Yes
1-2Not
drug
related
Drowsin
ess
400mg
Non
e2
60Yes
Yes
1Po
ssible
Drowsin
ess
Placebo
Non
e15
140
Yes
Yes
1Not
drug
related
Nausea
500mg
Non
e025
20Yes
Yes
1Po
ssible
Nausea
Placebo
Non
eIm
mediate
10Yes
Yes
3Not
drug
related
Heavinessof
head
80mg
Non
e025
15Yes
Yes
1Po
ssible
Heavinessof
head
Placebo
Non
e1
10Yes
Yes
1Not
drug
related
Visualdistu
rbances
320mg
Non
e36
2-3
Yes
Yes
1Re
mote
Bradycardia
400mg
Non
e1
60Yes
Yes
1Po
ssible
Retching
Placebo
Non
eIm
mediate
10Yes
Yes
3Not
drug
related
Itching
400mg
Non
e24
8Yes
Yes
1Po
ssible
Dizziness
Placebo
Non
e1
10Yes
Yes
3Not
drug
related
Severitygradingdo
neaccordingto
Com
mon
Term
inolog
yCr
iteria
forA
dverse
Eventsv40U
SDepartm
ento
fHealth
andHum
anServicesG
rade
1Mild
asymptom
aticor
mild
symptom
sclinicalord
iagn
ostic
observations
onlyinterventionno
tind
icatedG
rade
2Mod
erateminim
allocalor
noninvasiveinterventionindicatedGrade
3Severeor
medicallysig
nificantb
utno
timmediatelylife-threateningho
spita
lization
orprolon
gatio
nof
hospita
lizationindicateddisablingGrade
4Life-th
reateningconsequencesurgentinterventionindicatedGrade
5Death
relatedto
AE
Causality
assessmentNon
eremote(lt5
chance
ofbeingdrug
related)possib
le(gt5
butle
50chance
ofbeingdrug
relatedprobable(gt50chance
ofbeingdrug
related)
anddefin
ite
Grade
3severitymdash
volunteerw
ason
placebo
6 Malaria Research and Treatment
Excluded 13
Screened n = 63
Did not meet inclusionexclusion criteria n = 5
Refused consent n = 8
Randomized n = 50
Completed n = 12
Analyzed n = 50
Placebo n = 12 CDRI 9778 n = 38
Completed n = 38
Withdrawals n = 0
Dropouts n = 0
(a)
Flow of participants through the pharmacokinetic study
Enrolled and included in final
Screened (n = 20)
analysis (n = 16)
meet inclusion criteria n = 3
Refused consent n = 1 did not
(b)
Figure 2 Volunteer screening flowchart for ascending dose study 50 normal healthy human volunteers were screened from 63 volunteerswhile for single dose pharmacokinetics study 16 healthy volunteers were from 20 volunteers
remained well within normal range and did not demonstrateany dose response relationship were PCV total leukocyte andlymphocyte counts RBC counts and methemoglobin levels
34 Biochemical Parameters There was no significant differ-ence in serumbilirubin SGOT and SGPT at any time point ofmeasurement for intergroup comparisons The values ofserum alkaline phosphatase however were significantly dif-ferent between various groups at all pre- and postdrug mea-surements Post hoc analysis for this revealed that the resultswere significant for comparisons between lowest (80mgCDRI 9778) and higher doses (500 and 600mgCDRI 9778)although none of the groups was significantly differentfrom placebo All the values remained within normal range(Table 4) The other biochemical parameters which showedsignificant changes between groups were serum albumin
serum globulin and blood glucose and serum HDL levelsHowever they remained within the normal laboratory rangeand did not cause any sign or symptoms and there was nodose response relationship noted
35 Serum Electrolyte Levels The groups demonstrated sig-nificant variation in serum sodium and serum potassiumvalues at all time points of measurements None of the volun-teers had values outside the normal physiological ranges norpresented with any signs or symptoms of dyselectrolytemiaso these findings were considered clinically irrelevant
36 Pharmacokinetic Analysis Following oral administrationat 200mg compound 9778 was rapidly absorbed getsimmediately converted into active metabolite 9763 andis eliminated from the systemic circulation within 48 h
Malaria Research and Treatment 7
Table4Com
paris
onof
liver
functio
ntests
betweenvario
ustre
atmentg
roup
sonrepeated
observations
atbaselin
e24
hoursa
ndday7
Treatm
entg
roup
sTo
talserum
bilirub
inSerum
SGOT
Serum
SGPT
Serum
Alkalinep
hosphatase
Baselin
e24
hour
Day
7Ba
selin
e24
hour
Day
7Ba
selin
e24
hour
Day
7Ba
selin
e24
hour
Day
780
mg(119899=6)082plusmn024073plusmn024064plusmn0232215plusmn632348plusmn288277plusmn612188plusmn100262plusmn66218plusmn37955plusmn26651025plusmn300910683plusmn3712
160m
g(119899=6)076plusmn039055plusmn00706plusmn0063418plusmn7893398plusmn9693833plusmn8913721plusmn4163943plusmn808445plusmn11642115plusmn6865212plusmn6720717plusmn6103
320m
g(119899=6)073plusmn05208plusmn04087plusmn0593283plusmn5153417plusmn77635plusmn8533383plusmn9093733plusmn8873833plusmn1384242plusmn45242225plusmn345523583plusmn3249
400m
g(119899=6)052plusmn004053plusmn005055plusmn0082667plusmn662315plusmn453233plusmn88729plusmn5443517plusmn41238plusmn129523283plusmn4225167plusmn475924283plusmn3482
500m
g(119899=6)052plusmn004052plusmn004053plusmn0053133plusmn876315plusmn60234plusmn6003283plusmn1153483plusmn11073533plusmn105632117plusmn151313plusmn124533967plusmn18425
600m
g(119899=6)08plusmn05408plusmn059082plusmn0593117plusmn633033plusmn6743133plusmn57830plusmn716305plusmn8463317plusmn10532725plusmn667127583plusmn6129274plusmn7517
700m
g(119899=2)06plusmn01406plusmn014055plusmn007355plusmn07140plusmn424345plusmn07146plusmn566465plusmn49540plusmn11312615plusmn502254plusmn56572605plusmn4455
Placebo(119899=12)055plusmn007056plusmn006055plusmn0123191plusmn9673117plusmn918305plusmn8153708plusmn18113858plusmn19563583plusmn1811208plusmn6823208plusmn655620858plusmn7223
ANOVA119865
1114
1308
1105
1701
1631
114
162
1097
1435
4545
5103
3802
df49
4949
4949
4949
4949
4949
49119875
037
027
038
013
015
036
016
038
022
lt0001lowast
lt0001lowastlowast
0002
lowast119875=0002for5
00mgcomparedto
80mgdrug
and119875=002for6
00mgcomparedto
80mgdrug
(Scheffersquos
test)
lowastlowast119875=0001and000
6for8
0mgdrug
comparedto
500and60
0mgdrug
respectiv
ely(Scheffersquos
test)
119875=0006forc
omparis
onbetween80
and500m
gdrug
grou
ps(Scheffersquos
test)
Nodifferencefrom
placeboin
anycomparis
on
8 Malaria Research and Treatment
Table 5 Pharmacokinetic parameters of converted active metabolite 9763 after oral administration of 9778 at 200mg single dose to malehealthy human volunteers (119873 = 16)
PKparameter
Converted in vivometabolite 9763Mean plusmn SEMMale healthy human volunteers (119873 = 16)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16119862max(ngmL) 172 201 373 187 149 355 426 202 609 295 474 504 654 105 55 123 14393 plusmn 2832
119879max (h) 15 4 1 2 15 2 4 4 4 2 2 2 15 15 2 15 228 plusmn 02711987912
(h) 1389 217 478 220 388 2127 300 894 780 1163 2426 1450 1010 1773 2451 1890 1185 plusmn 194AUC0minusinfin
(ngsdothmL) 7887 1048 1644 6026 785 15226 2079 16049 5117 18989 935 3561 5836 6968 8331 9841 87874plusmn13315
MRT (h) 1257 572 137 353 538 1425 642 1413 928 976 3072 1453 1126 1837 3220 1852 1377 plusmn 205
Mea
n pl
asm
a con
sn (
ngm
L)
158
138
118
98
78
58
38
18
minus2minus2 8 18 28 38 48 58 68 78
Time (h)
Converted active metabolite 97ndash63
Figure 3 Mean plasma concentration-time profile of in vivo activemetabolite 9763 after oral administration of 9778 at 200mg singledose to male healthy human volunteers (119873 = 16)
except in two volunteers (72 h) as observed from plasmaconcentration-time profile (Figure 3) PK parameters gener-ated in individual volunteers have been shown in Table 5119879max of active metabolite 9763 was found to be 228 plusmn 027 hwith 119862max of 14393 plusmn 2832 Mean values of 119879
12 MRT and
AUC0ndashinfin of 9763were 505plusmn057 h 973plusmn106 h and 84522plusmn
14296 ngsdothmL respectively Active metabolite 9763 wasquantified from 05 h and up to 48 h in healthy volunteerswith exception to two volunteers in whom it was observed upto 72 h No additional metabolite peaks were observed duringanalysis except 9763 In most of the volunteers parentmolecule 9778was below the limit of quantitationMoreoververy low concentrations of 9778were observed in some volu-nteers but these were not sufficient for generating the PKparameters
4 Discussion
This was a first-in-human study conducted on healthy malevolunteers for a new antimalarial drug CDRI 9778 Overallthe drug was found to be safe
Few adverse events were reported which were of mildnature and were probable in causality But the adverse eventswere neither clinically nor statistically significant The 14adverse events reported in this trial occurred in various treat-ment groups over a large time frame Hence it cannot be said
definitelywhether theywere due to the drug or notMoreoversimilar adverse events were also seen in the placebo groupEven the statistically significant alteration in blood pressurewas not associated with signs and symptoms of altered bloodpressure and the values fell within normal ranges
For none of the adverse events any intervention in theform of drug administration fluid substitution and resusci-tation was required All the reported events continued to beobserved and resolved spontaneously
The severity of the adverse events was at best graded at 2No serious adverse events were reported The NCE underevaluation is a derivative of artemisinin compound which israrely associatedwith any SAEHowever structural similarityis just an indicator for predicting adverse effect profile of anovel compound A future possibility of such reactions com-ing into light always remains
Hence theMTD could not be determinedThough deter-mination of MTD was the main purpose of the study thiscould not be achieved This is a definite possibility in phase Istudies as has been seen previously [21 22] For the determi-nation of dose for multiple ascending dose study data frompreclinical efficacy studies will be used which is found to liewell within the highest dose evaluated in the present study
Therewere some haematological and biochemical param-eters which showed statistically significant values when com-pared to placebo but the differences were not clinically sig-nificant as most of them stayed within the normal laboratoryrange Further the absence of dose response relationshiphighlighted the fact that they were innocuous Nonclinicaltoxicity data serves as a guide to the monitoring of adversedrug events once the studies are conducted in healthy volun-teers Though there were no specific concerns raised in non-clinical toxicity a thorough evaluation of haematological andbiochemical parameters was undertaken Statistically signif-icant differences should be interpreted with caution keepingin mind the clinical relevance [23 24]
Since structurally the compound was similar to arte-misinin which has been reported to prolong QTc interval[25] a careful evaluation of QT interval was also undertakenThiswas also undertaken for assessing a future need to under-take a thoroughQT study No clinicallymeaningful alterationofQT interval as laid down in E 14 guidance document forQTevaluation [26] was observed
Malaria Research and Treatment 9
5 Conclusion
In conclusion we can say that the new compound CDRI9778 appears to be a safe and tolerable drug Its safety can befurther tested in multiple dose studies and if found tolerablecan be a good therapeutic option for malaria especiallymalaria resistant to available drugs
Conflict of Interests
The investigators did not receive any money for the conductof the study The study was sponsored by the Central DrugResearch Institute India The Innovator Institute a govern-ment organization had tied up with IPCA Ltd for the man-ufacture of the drug The drugs were supplied by IPCA LtdThey had no role in data collection recording and reportingTwo of the authors Dr Nitin Chandorkar and Dr AnilPareek are employees of IPCA Their role was in designingand conducting the study All the analyses were done inde-pendently by the investigatorsrsquo team
Acknowledgments
The authors would like to acknowledge the efforts of MrOnkar Rathod for helping in the execution of the study andMr Mitesh Sharma for giving his inputs for statistical analy-sis The research was funded by Central Drug Research Insti-tute (CSIR) Lucknow India This is a government organiza-tion
References
[1] ldquoWorldMalaria Reportrdquo 2005 httpwwwrollbackmalariaorgwmr2005
[2] A V Kondrashin ldquoMalaria in theWHOSoutheast Asia regionrdquoIndian Journal of Malariology vol 29 no 3 pp 129ndash160 1992
[3] U Arora G S Sonal G P S Dhillon andH GThakor ldquoEmer-gence of drug resistance in Indiardquo Journal of the Indian MedicalAssociation vol 106 no 10 pp 678ndash681 2008
[4] B M Greenwood D A Fidock D E Kyle et al ldquoMalaria pro-gress perils and prospects for eradicationrdquo Journal of ClinicalInvestigation vol 118 no 4 pp 1266ndash1276 2008
[5] C Singh and S K Puri ldquoSubstituted 124-trioxanes as anti-malarial agents and a process of producing the substituted 124-trioxanerdquo US Patent no 6316493 B1 2001
[6] C Singh N Gupta and S K Puri ldquoPhoto-oxygenation of ger-aniol synthesis of a novel series of hydroxy-functionalized anti-malarial 124-trioxanesrdquo Bioorganic and Medicinal ChemistryLetters vol 12 no 15 pp 1913ndash1916 2002
[7] C Singh N Gupta and S K Puri ldquoGeraniol-derived 124-trioxanes with potent in-vivo antimalarial activityrdquo Bioorganicand Medicinal Chemistry Letters vol 13 no 20 pp 3447ndash34502003
[8] C Singh N C Srivastav and S K Puri ldquoSynthesis and anti-malarial activity of 6-cycloalkylvinyl substituted 124-tri-oxanesrdquo Bioorganic andMedicinal Chemistry vol 12 no 22 pp5745ndash5752 2004
[9] A G Griesbeck T T El-Idreesy L-O Hoinck J Lex and RBrun ldquoNovel spiroanellated 124-trioxanes with high in vitro
antimalarial activitiesrdquo Bioorganic and Medicinal ChemistryLetters vol 15 no 3 pp 595ndash597 2005
[10] C Singh H Malik and S K Puri ldquoOrally active amino func-tionalized antimalarial 124-trioxanesrdquo Bioorganic and Medici-nal Chemistry Letters vol 14 no 2 pp 459ndash462 2004
[11] C SinghNGupta and S K Puri ldquoPhotooxygenation of 3-aryl-2-cyclohexenols synthesis of a new series of antimalarial 124-trioxanesrdquo Tetrahedron Letters vol 46 no 2 pp 205ndash207 2005
[12] C Singh HMalik and S K Puri ldquoOrally active 124-trioxanessynthesis and antimalarial assessment of a new series of 9-functionalized 3-(1-arylvinyl)-125-trioxaspiro[55]undecanesagainst multi-drug-resistant Plasmodium yoelii nigeriensis inmicerdquo Journal of Medicinal Chemistry vol 49 no 9 pp 2794ndash2803 2006
[13] C Singh S Chaudhary and S K Puri ldquoNew orally active deri-vatives of artemisinin with high efficacy against multidrug-resistant malaria in micerdquo Journal of Medicinal Chemistry vol49 no 24 pp 7227ndash7233 2006
[14] C Singh U Sharma G Saxena and S K Puri ldquoOrally activeantimalarials synthesis and bioevaluation of a new series ofsteroid-based 124-trioxanes against multi-drug resistantmalaria in micerdquo Bioorganic and Medicinal Chemistry Lettersvol 17 no 15 pp 4097ndash4101 2007
[15] C Singh R Kanchan U Sharma and S K Puri ldquoNewadamantane-based spiro 124-trioxanes orally effective againstrodent and simianmalariardquo Journal ofMedicinal Chemistry vol50 no 3 pp 521ndash527 2007
[16] C Singh S Chaudhary RKanchan and SK Puri ldquoConversionof antimalarial drug artemisinin to a new series of tricyclic 124-trioxanesrdquo Organic Letters vol 9 no 21 pp 4327ndash4329 2007
[17] C Singh V P Verma N K Naikade A S Singh M Hassamand S K Puri ldquoNovel bis- and tris-124-trioxanes synthesis andantimalarial activity against multidrug-resistant Plasmodiumyoelii in swiss micerdquo Journal of Medicinal Chemistry vol 51 no23 pp 7581ndash7592 2008
[18] R P Singh S Sabarinath N Gautam R C Gupta and S KSingh ldquoPharmacokinetic study of the novel synthetic trioxaneantimalarial compound 97-78 in rats using an LC-MSMSmethod for quantificationrdquo Arzneimittel-Forschung vol 61 no2 pp 120ndash125 2011
[19] R P Singh S Sabarinath N Gautam R C Gupta and S KSingh ldquoLiquid chromatographic tandem mass spectrometricassay for quantification of 9778 and its metabolite 9763 apromising trioxane antimalarial in monkey plasmardquo Journal ofChromatography B vol 877 no 22 pp 2074ndash2080 2009
[20] V P Shah K K Midha J W A Findlay et al ldquoBioanalyticalmethod validationmdasha revisit with a decade of progressrdquo Phar-maceutical Research vol 17 no 12 pp 1551ndash1557 2000
[21] E RGerstner A F Eichler S R Plotkin et al ldquoPhase I trial withbiomarker studies of vatalanib (PTK787) in patients with newlydiagnosed glioblastoma treated with enzyme inducing anti-epileptic drugs and standard radiation and temozolomiderdquoJournal of Neuro-Oncology vol 103 no 2 pp 325ndash332 2011
[22] A Forero-Torres J Shah TWood et al ldquoPhase I trial of weeklytigatuzumab an agonistic humanizedmonoclonal antibody tar-geting death receptor 5 (DR5)rdquo Cancer Biotherapy and Radio-pharmaceuticals vol 25 no 1 pp 13ndash19 2010
[23] R C Kane ldquoThe clinical significance of statistical significancerdquoOncologist vol 13 no 11 pp 1129ndash1133 2008
[24] M J Hayat ldquoUnderstanding statistical significancerdquo NursingResearch vol 59 no 3 pp 219ndash223 2010
10 Malaria Research and Treatment
[25] I R Ribeiro and P Olliaro ldquoSafety of artemisinin and its deriva-tives A review of published and unpublished clinical trialsrdquoMedecine Tropicale vol 58 no 3 supplement pp 50ndash53 1998
[26] 2013 httpwwwfdagovdownloadsDrugsGuidanceCompli-anceRegulatoryInformationGuidancesucm073161pdf
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

6 Malaria Research and Treatment
Excluded 13
Screened n = 63
Did not meet inclusionexclusion criteria n = 5
Refused consent n = 8
Randomized n = 50
Completed n = 12
Analyzed n = 50
Placebo n = 12 CDRI 9778 n = 38
Completed n = 38
Withdrawals n = 0
Dropouts n = 0
(a)
Flow of participants through the pharmacokinetic study
Enrolled and included in final
Screened (n = 20)
analysis (n = 16)
meet inclusion criteria n = 3
Refused consent n = 1 did not
(b)
Figure 2 Volunteer screening flowchart for ascending dose study 50 normal healthy human volunteers were screened from 63 volunteerswhile for single dose pharmacokinetics study 16 healthy volunteers were from 20 volunteers
remained well within normal range and did not demonstrateany dose response relationship were PCV total leukocyte andlymphocyte counts RBC counts and methemoglobin levels
34 Biochemical Parameters There was no significant differ-ence in serumbilirubin SGOT and SGPT at any time point ofmeasurement for intergroup comparisons The values ofserum alkaline phosphatase however were significantly dif-ferent between various groups at all pre- and postdrug mea-surements Post hoc analysis for this revealed that the resultswere significant for comparisons between lowest (80mgCDRI 9778) and higher doses (500 and 600mgCDRI 9778)although none of the groups was significantly differentfrom placebo All the values remained within normal range(Table 4) The other biochemical parameters which showedsignificant changes between groups were serum albumin
serum globulin and blood glucose and serum HDL levelsHowever they remained within the normal laboratory rangeand did not cause any sign or symptoms and there was nodose response relationship noted
35 Serum Electrolyte Levels The groups demonstrated sig-nificant variation in serum sodium and serum potassiumvalues at all time points of measurements None of the volun-teers had values outside the normal physiological ranges norpresented with any signs or symptoms of dyselectrolytemiaso these findings were considered clinically irrelevant
36 Pharmacokinetic Analysis Following oral administrationat 200mg compound 9778 was rapidly absorbed getsimmediately converted into active metabolite 9763 andis eliminated from the systemic circulation within 48 h
Malaria Research and Treatment 7
Table4Com
paris
onof
liver
functio
ntests
betweenvario
ustre
atmentg
roup
sonrepeated
observations
atbaselin
e24
hoursa
ndday7
Treatm
entg
roup
sTo
talserum
bilirub
inSerum
SGOT
Serum
SGPT
Serum
Alkalinep
hosphatase
Baselin
e24
hour
Day
7Ba
selin
e24
hour
Day
7Ba
selin
e24
hour
Day
7Ba
selin
e24
hour
Day
780
mg(119899=6)082plusmn024073plusmn024064plusmn0232215plusmn632348plusmn288277plusmn612188plusmn100262plusmn66218plusmn37955plusmn26651025plusmn300910683plusmn3712
160m
g(119899=6)076plusmn039055plusmn00706plusmn0063418plusmn7893398plusmn9693833plusmn8913721plusmn4163943plusmn808445plusmn11642115plusmn6865212plusmn6720717plusmn6103
320m
g(119899=6)073plusmn05208plusmn04087plusmn0593283plusmn5153417plusmn77635plusmn8533383plusmn9093733plusmn8873833plusmn1384242plusmn45242225plusmn345523583plusmn3249
400m
g(119899=6)052plusmn004053plusmn005055plusmn0082667plusmn662315plusmn453233plusmn88729plusmn5443517plusmn41238plusmn129523283plusmn4225167plusmn475924283plusmn3482
500m
g(119899=6)052plusmn004052plusmn004053plusmn0053133plusmn876315plusmn60234plusmn6003283plusmn1153483plusmn11073533plusmn105632117plusmn151313plusmn124533967plusmn18425
600m
g(119899=6)08plusmn05408plusmn059082plusmn0593117plusmn633033plusmn6743133plusmn57830plusmn716305plusmn8463317plusmn10532725plusmn667127583plusmn6129274plusmn7517
700m
g(119899=2)06plusmn01406plusmn014055plusmn007355plusmn07140plusmn424345plusmn07146plusmn566465plusmn49540plusmn11312615plusmn502254plusmn56572605plusmn4455
Placebo(119899=12)055plusmn007056plusmn006055plusmn0123191plusmn9673117plusmn918305plusmn8153708plusmn18113858plusmn19563583plusmn1811208plusmn6823208plusmn655620858plusmn7223
ANOVA119865
1114
1308
1105
1701
1631
114
162
1097
1435
4545
5103
3802
df49
4949
4949
4949
4949
4949
49119875
037
027
038
013
015
036
016
038
022
lt0001lowast
lt0001lowastlowast
0002
lowast119875=0002for5
00mgcomparedto
80mgdrug
and119875=002for6
00mgcomparedto
80mgdrug
(Scheffersquos
test)
lowastlowast119875=0001and000
6for8
0mgdrug
comparedto
500and60
0mgdrug
respectiv
ely(Scheffersquos
test)
119875=0006forc
omparis
onbetween80
and500m
gdrug
grou
ps(Scheffersquos
test)
Nodifferencefrom
placeboin
anycomparis
on
8 Malaria Research and Treatment
Table 5 Pharmacokinetic parameters of converted active metabolite 9763 after oral administration of 9778 at 200mg single dose to malehealthy human volunteers (119873 = 16)
PKparameter
Converted in vivometabolite 9763Mean plusmn SEMMale healthy human volunteers (119873 = 16)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16119862max(ngmL) 172 201 373 187 149 355 426 202 609 295 474 504 654 105 55 123 14393 plusmn 2832
119879max (h) 15 4 1 2 15 2 4 4 4 2 2 2 15 15 2 15 228 plusmn 02711987912
(h) 1389 217 478 220 388 2127 300 894 780 1163 2426 1450 1010 1773 2451 1890 1185 plusmn 194AUC0minusinfin
(ngsdothmL) 7887 1048 1644 6026 785 15226 2079 16049 5117 18989 935 3561 5836 6968 8331 9841 87874plusmn13315
MRT (h) 1257 572 137 353 538 1425 642 1413 928 976 3072 1453 1126 1837 3220 1852 1377 plusmn 205
Mea
n pl
asm
a con
sn (
ngm
L)
158
138
118
98
78
58
38
18
minus2minus2 8 18 28 38 48 58 68 78
Time (h)
Converted active metabolite 97ndash63
Figure 3 Mean plasma concentration-time profile of in vivo activemetabolite 9763 after oral administration of 9778 at 200mg singledose to male healthy human volunteers (119873 = 16)
except in two volunteers (72 h) as observed from plasmaconcentration-time profile (Figure 3) PK parameters gener-ated in individual volunteers have been shown in Table 5119879max of active metabolite 9763 was found to be 228 plusmn 027 hwith 119862max of 14393 plusmn 2832 Mean values of 119879
12 MRT and
AUC0ndashinfin of 9763were 505plusmn057 h 973plusmn106 h and 84522plusmn
14296 ngsdothmL respectively Active metabolite 9763 wasquantified from 05 h and up to 48 h in healthy volunteerswith exception to two volunteers in whom it was observed upto 72 h No additional metabolite peaks were observed duringanalysis except 9763 In most of the volunteers parentmolecule 9778was below the limit of quantitationMoreoververy low concentrations of 9778were observed in some volu-nteers but these were not sufficient for generating the PKparameters
4 Discussion
This was a first-in-human study conducted on healthy malevolunteers for a new antimalarial drug CDRI 9778 Overallthe drug was found to be safe
Few adverse events were reported which were of mildnature and were probable in causality But the adverse eventswere neither clinically nor statistically significant The 14adverse events reported in this trial occurred in various treat-ment groups over a large time frame Hence it cannot be said
definitelywhether theywere due to the drug or notMoreoversimilar adverse events were also seen in the placebo groupEven the statistically significant alteration in blood pressurewas not associated with signs and symptoms of altered bloodpressure and the values fell within normal ranges
For none of the adverse events any intervention in theform of drug administration fluid substitution and resusci-tation was required All the reported events continued to beobserved and resolved spontaneously
The severity of the adverse events was at best graded at 2No serious adverse events were reported The NCE underevaluation is a derivative of artemisinin compound which israrely associatedwith any SAEHowever structural similarityis just an indicator for predicting adverse effect profile of anovel compound A future possibility of such reactions com-ing into light always remains
Hence theMTD could not be determinedThough deter-mination of MTD was the main purpose of the study thiscould not be achieved This is a definite possibility in phase Istudies as has been seen previously [21 22] For the determi-nation of dose for multiple ascending dose study data frompreclinical efficacy studies will be used which is found to liewell within the highest dose evaluated in the present study
Therewere some haematological and biochemical param-eters which showed statistically significant values when com-pared to placebo but the differences were not clinically sig-nificant as most of them stayed within the normal laboratoryrange Further the absence of dose response relationshiphighlighted the fact that they were innocuous Nonclinicaltoxicity data serves as a guide to the monitoring of adversedrug events once the studies are conducted in healthy volun-teers Though there were no specific concerns raised in non-clinical toxicity a thorough evaluation of haematological andbiochemical parameters was undertaken Statistically signif-icant differences should be interpreted with caution keepingin mind the clinical relevance [23 24]
Since structurally the compound was similar to arte-misinin which has been reported to prolong QTc interval[25] a careful evaluation of QT interval was also undertakenThiswas also undertaken for assessing a future need to under-take a thoroughQT study No clinicallymeaningful alterationofQT interval as laid down in E 14 guidance document forQTevaluation [26] was observed
Malaria Research and Treatment 9
5 Conclusion
In conclusion we can say that the new compound CDRI9778 appears to be a safe and tolerable drug Its safety can befurther tested in multiple dose studies and if found tolerablecan be a good therapeutic option for malaria especiallymalaria resistant to available drugs
Conflict of Interests
The investigators did not receive any money for the conductof the study The study was sponsored by the Central DrugResearch Institute India The Innovator Institute a govern-ment organization had tied up with IPCA Ltd for the man-ufacture of the drug The drugs were supplied by IPCA LtdThey had no role in data collection recording and reportingTwo of the authors Dr Nitin Chandorkar and Dr AnilPareek are employees of IPCA Their role was in designingand conducting the study All the analyses were done inde-pendently by the investigatorsrsquo team
Acknowledgments
The authors would like to acknowledge the efforts of MrOnkar Rathod for helping in the execution of the study andMr Mitesh Sharma for giving his inputs for statistical analy-sis The research was funded by Central Drug Research Insti-tute (CSIR) Lucknow India This is a government organiza-tion
References
[1] ldquoWorldMalaria Reportrdquo 2005 httpwwwrollbackmalariaorgwmr2005
[2] A V Kondrashin ldquoMalaria in theWHOSoutheast Asia regionrdquoIndian Journal of Malariology vol 29 no 3 pp 129ndash160 1992
[3] U Arora G S Sonal G P S Dhillon andH GThakor ldquoEmer-gence of drug resistance in Indiardquo Journal of the Indian MedicalAssociation vol 106 no 10 pp 678ndash681 2008
[4] B M Greenwood D A Fidock D E Kyle et al ldquoMalaria pro-gress perils and prospects for eradicationrdquo Journal of ClinicalInvestigation vol 118 no 4 pp 1266ndash1276 2008
[5] C Singh and S K Puri ldquoSubstituted 124-trioxanes as anti-malarial agents and a process of producing the substituted 124-trioxanerdquo US Patent no 6316493 B1 2001
[6] C Singh N Gupta and S K Puri ldquoPhoto-oxygenation of ger-aniol synthesis of a novel series of hydroxy-functionalized anti-malarial 124-trioxanesrdquo Bioorganic and Medicinal ChemistryLetters vol 12 no 15 pp 1913ndash1916 2002
[7] C Singh N Gupta and S K Puri ldquoGeraniol-derived 124-trioxanes with potent in-vivo antimalarial activityrdquo Bioorganicand Medicinal Chemistry Letters vol 13 no 20 pp 3447ndash34502003
[8] C Singh N C Srivastav and S K Puri ldquoSynthesis and anti-malarial activity of 6-cycloalkylvinyl substituted 124-tri-oxanesrdquo Bioorganic andMedicinal Chemistry vol 12 no 22 pp5745ndash5752 2004
[9] A G Griesbeck T T El-Idreesy L-O Hoinck J Lex and RBrun ldquoNovel spiroanellated 124-trioxanes with high in vitro
antimalarial activitiesrdquo Bioorganic and Medicinal ChemistryLetters vol 15 no 3 pp 595ndash597 2005
[10] C Singh H Malik and S K Puri ldquoOrally active amino func-tionalized antimalarial 124-trioxanesrdquo Bioorganic and Medici-nal Chemistry Letters vol 14 no 2 pp 459ndash462 2004
[11] C SinghNGupta and S K Puri ldquoPhotooxygenation of 3-aryl-2-cyclohexenols synthesis of a new series of antimalarial 124-trioxanesrdquo Tetrahedron Letters vol 46 no 2 pp 205ndash207 2005
[12] C Singh HMalik and S K Puri ldquoOrally active 124-trioxanessynthesis and antimalarial assessment of a new series of 9-functionalized 3-(1-arylvinyl)-125-trioxaspiro[55]undecanesagainst multi-drug-resistant Plasmodium yoelii nigeriensis inmicerdquo Journal of Medicinal Chemistry vol 49 no 9 pp 2794ndash2803 2006
[13] C Singh S Chaudhary and S K Puri ldquoNew orally active deri-vatives of artemisinin with high efficacy against multidrug-resistant malaria in micerdquo Journal of Medicinal Chemistry vol49 no 24 pp 7227ndash7233 2006
[14] C Singh U Sharma G Saxena and S K Puri ldquoOrally activeantimalarials synthesis and bioevaluation of a new series ofsteroid-based 124-trioxanes against multi-drug resistantmalaria in micerdquo Bioorganic and Medicinal Chemistry Lettersvol 17 no 15 pp 4097ndash4101 2007
[15] C Singh R Kanchan U Sharma and S K Puri ldquoNewadamantane-based spiro 124-trioxanes orally effective againstrodent and simianmalariardquo Journal ofMedicinal Chemistry vol50 no 3 pp 521ndash527 2007
[16] C Singh S Chaudhary RKanchan and SK Puri ldquoConversionof antimalarial drug artemisinin to a new series of tricyclic 124-trioxanesrdquo Organic Letters vol 9 no 21 pp 4327ndash4329 2007
[17] C Singh V P Verma N K Naikade A S Singh M Hassamand S K Puri ldquoNovel bis- and tris-124-trioxanes synthesis andantimalarial activity against multidrug-resistant Plasmodiumyoelii in swiss micerdquo Journal of Medicinal Chemistry vol 51 no23 pp 7581ndash7592 2008
[18] R P Singh S Sabarinath N Gautam R C Gupta and S KSingh ldquoPharmacokinetic study of the novel synthetic trioxaneantimalarial compound 97-78 in rats using an LC-MSMSmethod for quantificationrdquo Arzneimittel-Forschung vol 61 no2 pp 120ndash125 2011
[19] R P Singh S Sabarinath N Gautam R C Gupta and S KSingh ldquoLiquid chromatographic tandem mass spectrometricassay for quantification of 9778 and its metabolite 9763 apromising trioxane antimalarial in monkey plasmardquo Journal ofChromatography B vol 877 no 22 pp 2074ndash2080 2009
[20] V P Shah K K Midha J W A Findlay et al ldquoBioanalyticalmethod validationmdasha revisit with a decade of progressrdquo Phar-maceutical Research vol 17 no 12 pp 1551ndash1557 2000
[21] E RGerstner A F Eichler S R Plotkin et al ldquoPhase I trial withbiomarker studies of vatalanib (PTK787) in patients with newlydiagnosed glioblastoma treated with enzyme inducing anti-epileptic drugs and standard radiation and temozolomiderdquoJournal of Neuro-Oncology vol 103 no 2 pp 325ndash332 2011
[22] A Forero-Torres J Shah TWood et al ldquoPhase I trial of weeklytigatuzumab an agonistic humanizedmonoclonal antibody tar-geting death receptor 5 (DR5)rdquo Cancer Biotherapy and Radio-pharmaceuticals vol 25 no 1 pp 13ndash19 2010
[23] R C Kane ldquoThe clinical significance of statistical significancerdquoOncologist vol 13 no 11 pp 1129ndash1133 2008
[24] M J Hayat ldquoUnderstanding statistical significancerdquo NursingResearch vol 59 no 3 pp 219ndash223 2010
10 Malaria Research and Treatment
[25] I R Ribeiro and P Olliaro ldquoSafety of artemisinin and its deriva-tives A review of published and unpublished clinical trialsrdquoMedecine Tropicale vol 58 no 3 supplement pp 50ndash53 1998
[26] 2013 httpwwwfdagovdownloadsDrugsGuidanceCompli-anceRegulatoryInformationGuidancesucm073161pdf
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Malaria Research and Treatment 7
Table4Com
paris
onof
liver
functio
ntests
betweenvario
ustre
atmentg
roup
sonrepeated
observations
atbaselin
e24
hoursa
ndday7
Treatm
entg
roup
sTo
talserum
bilirub
inSerum
SGOT
Serum
SGPT
Serum
Alkalinep
hosphatase
Baselin
e24
hour
Day
7Ba
selin
e24
hour
Day
7Ba
selin
e24
hour
Day
7Ba
selin
e24
hour
Day
780
mg(119899=6)082plusmn024073plusmn024064plusmn0232215plusmn632348plusmn288277plusmn612188plusmn100262plusmn66218plusmn37955plusmn26651025plusmn300910683plusmn3712
160m
g(119899=6)076plusmn039055plusmn00706plusmn0063418plusmn7893398plusmn9693833plusmn8913721plusmn4163943plusmn808445plusmn11642115plusmn6865212plusmn6720717plusmn6103
320m
g(119899=6)073plusmn05208plusmn04087plusmn0593283plusmn5153417plusmn77635plusmn8533383plusmn9093733plusmn8873833plusmn1384242plusmn45242225plusmn345523583plusmn3249
400m
g(119899=6)052plusmn004053plusmn005055plusmn0082667plusmn662315plusmn453233plusmn88729plusmn5443517plusmn41238plusmn129523283plusmn4225167plusmn475924283plusmn3482
500m
g(119899=6)052plusmn004052plusmn004053plusmn0053133plusmn876315plusmn60234plusmn6003283plusmn1153483plusmn11073533plusmn105632117plusmn151313plusmn124533967plusmn18425
600m
g(119899=6)08plusmn05408plusmn059082plusmn0593117plusmn633033plusmn6743133plusmn57830plusmn716305plusmn8463317plusmn10532725plusmn667127583plusmn6129274plusmn7517
700m
g(119899=2)06plusmn01406plusmn014055plusmn007355plusmn07140plusmn424345plusmn07146plusmn566465plusmn49540plusmn11312615plusmn502254plusmn56572605plusmn4455
Placebo(119899=12)055plusmn007056plusmn006055plusmn0123191plusmn9673117plusmn918305plusmn8153708plusmn18113858plusmn19563583plusmn1811208plusmn6823208plusmn655620858plusmn7223
ANOVA119865
1114
1308
1105
1701
1631
114
162
1097
1435
4545
5103
3802
df49
4949
4949
4949
4949
4949
49119875
037
027
038
013
015
036
016
038
022
lt0001lowast
lt0001lowastlowast
0002
lowast119875=0002for5
00mgcomparedto
80mgdrug
and119875=002for6
00mgcomparedto
80mgdrug
(Scheffersquos
test)
lowastlowast119875=0001and000
6for8
0mgdrug
comparedto
500and60
0mgdrug
respectiv
ely(Scheffersquos
test)
119875=0006forc
omparis
onbetween80
and500m
gdrug
grou
ps(Scheffersquos
test)
Nodifferencefrom
placeboin
anycomparis
on
8 Malaria Research and Treatment
Table 5 Pharmacokinetic parameters of converted active metabolite 9763 after oral administration of 9778 at 200mg single dose to malehealthy human volunteers (119873 = 16)
PKparameter
Converted in vivometabolite 9763Mean plusmn SEMMale healthy human volunteers (119873 = 16)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16119862max(ngmL) 172 201 373 187 149 355 426 202 609 295 474 504 654 105 55 123 14393 plusmn 2832
119879max (h) 15 4 1 2 15 2 4 4 4 2 2 2 15 15 2 15 228 plusmn 02711987912
(h) 1389 217 478 220 388 2127 300 894 780 1163 2426 1450 1010 1773 2451 1890 1185 plusmn 194AUC0minusinfin
(ngsdothmL) 7887 1048 1644 6026 785 15226 2079 16049 5117 18989 935 3561 5836 6968 8331 9841 87874plusmn13315
MRT (h) 1257 572 137 353 538 1425 642 1413 928 976 3072 1453 1126 1837 3220 1852 1377 plusmn 205
Mea
n pl
asm
a con
sn (
ngm
L)
158
138
118
98
78
58
38
18
minus2minus2 8 18 28 38 48 58 68 78
Time (h)
Converted active metabolite 97ndash63
Figure 3 Mean plasma concentration-time profile of in vivo activemetabolite 9763 after oral administration of 9778 at 200mg singledose to male healthy human volunteers (119873 = 16)
except in two volunteers (72 h) as observed from plasmaconcentration-time profile (Figure 3) PK parameters gener-ated in individual volunteers have been shown in Table 5119879max of active metabolite 9763 was found to be 228 plusmn 027 hwith 119862max of 14393 plusmn 2832 Mean values of 119879
12 MRT and
AUC0ndashinfin of 9763were 505plusmn057 h 973plusmn106 h and 84522plusmn
14296 ngsdothmL respectively Active metabolite 9763 wasquantified from 05 h and up to 48 h in healthy volunteerswith exception to two volunteers in whom it was observed upto 72 h No additional metabolite peaks were observed duringanalysis except 9763 In most of the volunteers parentmolecule 9778was below the limit of quantitationMoreoververy low concentrations of 9778were observed in some volu-nteers but these were not sufficient for generating the PKparameters
4 Discussion
This was a first-in-human study conducted on healthy malevolunteers for a new antimalarial drug CDRI 9778 Overallthe drug was found to be safe
Few adverse events were reported which were of mildnature and were probable in causality But the adverse eventswere neither clinically nor statistically significant The 14adverse events reported in this trial occurred in various treat-ment groups over a large time frame Hence it cannot be said
definitelywhether theywere due to the drug or notMoreoversimilar adverse events were also seen in the placebo groupEven the statistically significant alteration in blood pressurewas not associated with signs and symptoms of altered bloodpressure and the values fell within normal ranges
For none of the adverse events any intervention in theform of drug administration fluid substitution and resusci-tation was required All the reported events continued to beobserved and resolved spontaneously
The severity of the adverse events was at best graded at 2No serious adverse events were reported The NCE underevaluation is a derivative of artemisinin compound which israrely associatedwith any SAEHowever structural similarityis just an indicator for predicting adverse effect profile of anovel compound A future possibility of such reactions com-ing into light always remains
Hence theMTD could not be determinedThough deter-mination of MTD was the main purpose of the study thiscould not be achieved This is a definite possibility in phase Istudies as has been seen previously [21 22] For the determi-nation of dose for multiple ascending dose study data frompreclinical efficacy studies will be used which is found to liewell within the highest dose evaluated in the present study
Therewere some haematological and biochemical param-eters which showed statistically significant values when com-pared to placebo but the differences were not clinically sig-nificant as most of them stayed within the normal laboratoryrange Further the absence of dose response relationshiphighlighted the fact that they were innocuous Nonclinicaltoxicity data serves as a guide to the monitoring of adversedrug events once the studies are conducted in healthy volun-teers Though there were no specific concerns raised in non-clinical toxicity a thorough evaluation of haematological andbiochemical parameters was undertaken Statistically signif-icant differences should be interpreted with caution keepingin mind the clinical relevance [23 24]
Since structurally the compound was similar to arte-misinin which has been reported to prolong QTc interval[25] a careful evaluation of QT interval was also undertakenThiswas also undertaken for assessing a future need to under-take a thoroughQT study No clinicallymeaningful alterationofQT interval as laid down in E 14 guidance document forQTevaluation [26] was observed
Malaria Research and Treatment 9
5 Conclusion
In conclusion we can say that the new compound CDRI9778 appears to be a safe and tolerable drug Its safety can befurther tested in multiple dose studies and if found tolerablecan be a good therapeutic option for malaria especiallymalaria resistant to available drugs
Conflict of Interests
The investigators did not receive any money for the conductof the study The study was sponsored by the Central DrugResearch Institute India The Innovator Institute a govern-ment organization had tied up with IPCA Ltd for the man-ufacture of the drug The drugs were supplied by IPCA LtdThey had no role in data collection recording and reportingTwo of the authors Dr Nitin Chandorkar and Dr AnilPareek are employees of IPCA Their role was in designingand conducting the study All the analyses were done inde-pendently by the investigatorsrsquo team
Acknowledgments
The authors would like to acknowledge the efforts of MrOnkar Rathod for helping in the execution of the study andMr Mitesh Sharma for giving his inputs for statistical analy-sis The research was funded by Central Drug Research Insti-tute (CSIR) Lucknow India This is a government organiza-tion
References
[1] ldquoWorldMalaria Reportrdquo 2005 httpwwwrollbackmalariaorgwmr2005
[2] A V Kondrashin ldquoMalaria in theWHOSoutheast Asia regionrdquoIndian Journal of Malariology vol 29 no 3 pp 129ndash160 1992
[3] U Arora G S Sonal G P S Dhillon andH GThakor ldquoEmer-gence of drug resistance in Indiardquo Journal of the Indian MedicalAssociation vol 106 no 10 pp 678ndash681 2008
[4] B M Greenwood D A Fidock D E Kyle et al ldquoMalaria pro-gress perils and prospects for eradicationrdquo Journal of ClinicalInvestigation vol 118 no 4 pp 1266ndash1276 2008
[5] C Singh and S K Puri ldquoSubstituted 124-trioxanes as anti-malarial agents and a process of producing the substituted 124-trioxanerdquo US Patent no 6316493 B1 2001
[6] C Singh N Gupta and S K Puri ldquoPhoto-oxygenation of ger-aniol synthesis of a novel series of hydroxy-functionalized anti-malarial 124-trioxanesrdquo Bioorganic and Medicinal ChemistryLetters vol 12 no 15 pp 1913ndash1916 2002
[7] C Singh N Gupta and S K Puri ldquoGeraniol-derived 124-trioxanes with potent in-vivo antimalarial activityrdquo Bioorganicand Medicinal Chemistry Letters vol 13 no 20 pp 3447ndash34502003
[8] C Singh N C Srivastav and S K Puri ldquoSynthesis and anti-malarial activity of 6-cycloalkylvinyl substituted 124-tri-oxanesrdquo Bioorganic andMedicinal Chemistry vol 12 no 22 pp5745ndash5752 2004
[9] A G Griesbeck T T El-Idreesy L-O Hoinck J Lex and RBrun ldquoNovel spiroanellated 124-trioxanes with high in vitro
antimalarial activitiesrdquo Bioorganic and Medicinal ChemistryLetters vol 15 no 3 pp 595ndash597 2005
[10] C Singh H Malik and S K Puri ldquoOrally active amino func-tionalized antimalarial 124-trioxanesrdquo Bioorganic and Medici-nal Chemistry Letters vol 14 no 2 pp 459ndash462 2004
[11] C SinghNGupta and S K Puri ldquoPhotooxygenation of 3-aryl-2-cyclohexenols synthesis of a new series of antimalarial 124-trioxanesrdquo Tetrahedron Letters vol 46 no 2 pp 205ndash207 2005
[12] C Singh HMalik and S K Puri ldquoOrally active 124-trioxanessynthesis and antimalarial assessment of a new series of 9-functionalized 3-(1-arylvinyl)-125-trioxaspiro[55]undecanesagainst multi-drug-resistant Plasmodium yoelii nigeriensis inmicerdquo Journal of Medicinal Chemistry vol 49 no 9 pp 2794ndash2803 2006
[13] C Singh S Chaudhary and S K Puri ldquoNew orally active deri-vatives of artemisinin with high efficacy against multidrug-resistant malaria in micerdquo Journal of Medicinal Chemistry vol49 no 24 pp 7227ndash7233 2006
[14] C Singh U Sharma G Saxena and S K Puri ldquoOrally activeantimalarials synthesis and bioevaluation of a new series ofsteroid-based 124-trioxanes against multi-drug resistantmalaria in micerdquo Bioorganic and Medicinal Chemistry Lettersvol 17 no 15 pp 4097ndash4101 2007
[15] C Singh R Kanchan U Sharma and S K Puri ldquoNewadamantane-based spiro 124-trioxanes orally effective againstrodent and simianmalariardquo Journal ofMedicinal Chemistry vol50 no 3 pp 521ndash527 2007
[16] C Singh S Chaudhary RKanchan and SK Puri ldquoConversionof antimalarial drug artemisinin to a new series of tricyclic 124-trioxanesrdquo Organic Letters vol 9 no 21 pp 4327ndash4329 2007
[17] C Singh V P Verma N K Naikade A S Singh M Hassamand S K Puri ldquoNovel bis- and tris-124-trioxanes synthesis andantimalarial activity against multidrug-resistant Plasmodiumyoelii in swiss micerdquo Journal of Medicinal Chemistry vol 51 no23 pp 7581ndash7592 2008
[18] R P Singh S Sabarinath N Gautam R C Gupta and S KSingh ldquoPharmacokinetic study of the novel synthetic trioxaneantimalarial compound 97-78 in rats using an LC-MSMSmethod for quantificationrdquo Arzneimittel-Forschung vol 61 no2 pp 120ndash125 2011
[19] R P Singh S Sabarinath N Gautam R C Gupta and S KSingh ldquoLiquid chromatographic tandem mass spectrometricassay for quantification of 9778 and its metabolite 9763 apromising trioxane antimalarial in monkey plasmardquo Journal ofChromatography B vol 877 no 22 pp 2074ndash2080 2009
[20] V P Shah K K Midha J W A Findlay et al ldquoBioanalyticalmethod validationmdasha revisit with a decade of progressrdquo Phar-maceutical Research vol 17 no 12 pp 1551ndash1557 2000
[21] E RGerstner A F Eichler S R Plotkin et al ldquoPhase I trial withbiomarker studies of vatalanib (PTK787) in patients with newlydiagnosed glioblastoma treated with enzyme inducing anti-epileptic drugs and standard radiation and temozolomiderdquoJournal of Neuro-Oncology vol 103 no 2 pp 325ndash332 2011
[22] A Forero-Torres J Shah TWood et al ldquoPhase I trial of weeklytigatuzumab an agonistic humanizedmonoclonal antibody tar-geting death receptor 5 (DR5)rdquo Cancer Biotherapy and Radio-pharmaceuticals vol 25 no 1 pp 13ndash19 2010
[23] R C Kane ldquoThe clinical significance of statistical significancerdquoOncologist vol 13 no 11 pp 1129ndash1133 2008
[24] M J Hayat ldquoUnderstanding statistical significancerdquo NursingResearch vol 59 no 3 pp 219ndash223 2010
10 Malaria Research and Treatment
[25] I R Ribeiro and P Olliaro ldquoSafety of artemisinin and its deriva-tives A review of published and unpublished clinical trialsrdquoMedecine Tropicale vol 58 no 3 supplement pp 50ndash53 1998
[26] 2013 httpwwwfdagovdownloadsDrugsGuidanceCompli-anceRegulatoryInformationGuidancesucm073161pdf
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

8 Malaria Research and Treatment
Table 5 Pharmacokinetic parameters of converted active metabolite 9763 after oral administration of 9778 at 200mg single dose to malehealthy human volunteers (119873 = 16)
PKparameter
Converted in vivometabolite 9763Mean plusmn SEMMale healthy human volunteers (119873 = 16)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16119862max(ngmL) 172 201 373 187 149 355 426 202 609 295 474 504 654 105 55 123 14393 plusmn 2832
119879max (h) 15 4 1 2 15 2 4 4 4 2 2 2 15 15 2 15 228 plusmn 02711987912
(h) 1389 217 478 220 388 2127 300 894 780 1163 2426 1450 1010 1773 2451 1890 1185 plusmn 194AUC0minusinfin
(ngsdothmL) 7887 1048 1644 6026 785 15226 2079 16049 5117 18989 935 3561 5836 6968 8331 9841 87874plusmn13315
MRT (h) 1257 572 137 353 538 1425 642 1413 928 976 3072 1453 1126 1837 3220 1852 1377 plusmn 205
Mea
n pl
asm
a con
sn (
ngm
L)
158
138
118
98
78
58
38
18
minus2minus2 8 18 28 38 48 58 68 78
Time (h)
Converted active metabolite 97ndash63
Figure 3 Mean plasma concentration-time profile of in vivo activemetabolite 9763 after oral administration of 9778 at 200mg singledose to male healthy human volunteers (119873 = 16)
except in two volunteers (72 h) as observed from plasmaconcentration-time profile (Figure 3) PK parameters gener-ated in individual volunteers have been shown in Table 5119879max of active metabolite 9763 was found to be 228 plusmn 027 hwith 119862max of 14393 plusmn 2832 Mean values of 119879
12 MRT and
AUC0ndashinfin of 9763were 505plusmn057 h 973plusmn106 h and 84522plusmn
14296 ngsdothmL respectively Active metabolite 9763 wasquantified from 05 h and up to 48 h in healthy volunteerswith exception to two volunteers in whom it was observed upto 72 h No additional metabolite peaks were observed duringanalysis except 9763 In most of the volunteers parentmolecule 9778was below the limit of quantitationMoreoververy low concentrations of 9778were observed in some volu-nteers but these were not sufficient for generating the PKparameters
4 Discussion
This was a first-in-human study conducted on healthy malevolunteers for a new antimalarial drug CDRI 9778 Overallthe drug was found to be safe
Few adverse events were reported which were of mildnature and were probable in causality But the adverse eventswere neither clinically nor statistically significant The 14adverse events reported in this trial occurred in various treat-ment groups over a large time frame Hence it cannot be said
definitelywhether theywere due to the drug or notMoreoversimilar adverse events were also seen in the placebo groupEven the statistically significant alteration in blood pressurewas not associated with signs and symptoms of altered bloodpressure and the values fell within normal ranges
For none of the adverse events any intervention in theform of drug administration fluid substitution and resusci-tation was required All the reported events continued to beobserved and resolved spontaneously
The severity of the adverse events was at best graded at 2No serious adverse events were reported The NCE underevaluation is a derivative of artemisinin compound which israrely associatedwith any SAEHowever structural similarityis just an indicator for predicting adverse effect profile of anovel compound A future possibility of such reactions com-ing into light always remains
Hence theMTD could not be determinedThough deter-mination of MTD was the main purpose of the study thiscould not be achieved This is a definite possibility in phase Istudies as has been seen previously [21 22] For the determi-nation of dose for multiple ascending dose study data frompreclinical efficacy studies will be used which is found to liewell within the highest dose evaluated in the present study
Therewere some haematological and biochemical param-eters which showed statistically significant values when com-pared to placebo but the differences were not clinically sig-nificant as most of them stayed within the normal laboratoryrange Further the absence of dose response relationshiphighlighted the fact that they were innocuous Nonclinicaltoxicity data serves as a guide to the monitoring of adversedrug events once the studies are conducted in healthy volun-teers Though there were no specific concerns raised in non-clinical toxicity a thorough evaluation of haematological andbiochemical parameters was undertaken Statistically signif-icant differences should be interpreted with caution keepingin mind the clinical relevance [23 24]
Since structurally the compound was similar to arte-misinin which has been reported to prolong QTc interval[25] a careful evaluation of QT interval was also undertakenThiswas also undertaken for assessing a future need to under-take a thoroughQT study No clinicallymeaningful alterationofQT interval as laid down in E 14 guidance document forQTevaluation [26] was observed
Malaria Research and Treatment 9
5 Conclusion
In conclusion we can say that the new compound CDRI9778 appears to be a safe and tolerable drug Its safety can befurther tested in multiple dose studies and if found tolerablecan be a good therapeutic option for malaria especiallymalaria resistant to available drugs
Conflict of Interests
The investigators did not receive any money for the conductof the study The study was sponsored by the Central DrugResearch Institute India The Innovator Institute a govern-ment organization had tied up with IPCA Ltd for the man-ufacture of the drug The drugs were supplied by IPCA LtdThey had no role in data collection recording and reportingTwo of the authors Dr Nitin Chandorkar and Dr AnilPareek are employees of IPCA Their role was in designingand conducting the study All the analyses were done inde-pendently by the investigatorsrsquo team
Acknowledgments
The authors would like to acknowledge the efforts of MrOnkar Rathod for helping in the execution of the study andMr Mitesh Sharma for giving his inputs for statistical analy-sis The research was funded by Central Drug Research Insti-tute (CSIR) Lucknow India This is a government organiza-tion
References
[1] ldquoWorldMalaria Reportrdquo 2005 httpwwwrollbackmalariaorgwmr2005
[2] A V Kondrashin ldquoMalaria in theWHOSoutheast Asia regionrdquoIndian Journal of Malariology vol 29 no 3 pp 129ndash160 1992
[3] U Arora G S Sonal G P S Dhillon andH GThakor ldquoEmer-gence of drug resistance in Indiardquo Journal of the Indian MedicalAssociation vol 106 no 10 pp 678ndash681 2008
[4] B M Greenwood D A Fidock D E Kyle et al ldquoMalaria pro-gress perils and prospects for eradicationrdquo Journal of ClinicalInvestigation vol 118 no 4 pp 1266ndash1276 2008
[5] C Singh and S K Puri ldquoSubstituted 124-trioxanes as anti-malarial agents and a process of producing the substituted 124-trioxanerdquo US Patent no 6316493 B1 2001
[6] C Singh N Gupta and S K Puri ldquoPhoto-oxygenation of ger-aniol synthesis of a novel series of hydroxy-functionalized anti-malarial 124-trioxanesrdquo Bioorganic and Medicinal ChemistryLetters vol 12 no 15 pp 1913ndash1916 2002
[7] C Singh N Gupta and S K Puri ldquoGeraniol-derived 124-trioxanes with potent in-vivo antimalarial activityrdquo Bioorganicand Medicinal Chemistry Letters vol 13 no 20 pp 3447ndash34502003
[8] C Singh N C Srivastav and S K Puri ldquoSynthesis and anti-malarial activity of 6-cycloalkylvinyl substituted 124-tri-oxanesrdquo Bioorganic andMedicinal Chemistry vol 12 no 22 pp5745ndash5752 2004
[9] A G Griesbeck T T El-Idreesy L-O Hoinck J Lex and RBrun ldquoNovel spiroanellated 124-trioxanes with high in vitro
antimalarial activitiesrdquo Bioorganic and Medicinal ChemistryLetters vol 15 no 3 pp 595ndash597 2005
[10] C Singh H Malik and S K Puri ldquoOrally active amino func-tionalized antimalarial 124-trioxanesrdquo Bioorganic and Medici-nal Chemistry Letters vol 14 no 2 pp 459ndash462 2004
[11] C SinghNGupta and S K Puri ldquoPhotooxygenation of 3-aryl-2-cyclohexenols synthesis of a new series of antimalarial 124-trioxanesrdquo Tetrahedron Letters vol 46 no 2 pp 205ndash207 2005
[12] C Singh HMalik and S K Puri ldquoOrally active 124-trioxanessynthesis and antimalarial assessment of a new series of 9-functionalized 3-(1-arylvinyl)-125-trioxaspiro[55]undecanesagainst multi-drug-resistant Plasmodium yoelii nigeriensis inmicerdquo Journal of Medicinal Chemistry vol 49 no 9 pp 2794ndash2803 2006
[13] C Singh S Chaudhary and S K Puri ldquoNew orally active deri-vatives of artemisinin with high efficacy against multidrug-resistant malaria in micerdquo Journal of Medicinal Chemistry vol49 no 24 pp 7227ndash7233 2006
[14] C Singh U Sharma G Saxena and S K Puri ldquoOrally activeantimalarials synthesis and bioevaluation of a new series ofsteroid-based 124-trioxanes against multi-drug resistantmalaria in micerdquo Bioorganic and Medicinal Chemistry Lettersvol 17 no 15 pp 4097ndash4101 2007
[15] C Singh R Kanchan U Sharma and S K Puri ldquoNewadamantane-based spiro 124-trioxanes orally effective againstrodent and simianmalariardquo Journal ofMedicinal Chemistry vol50 no 3 pp 521ndash527 2007
[16] C Singh S Chaudhary RKanchan and SK Puri ldquoConversionof antimalarial drug artemisinin to a new series of tricyclic 124-trioxanesrdquo Organic Letters vol 9 no 21 pp 4327ndash4329 2007
[17] C Singh V P Verma N K Naikade A S Singh M Hassamand S K Puri ldquoNovel bis- and tris-124-trioxanes synthesis andantimalarial activity against multidrug-resistant Plasmodiumyoelii in swiss micerdquo Journal of Medicinal Chemistry vol 51 no23 pp 7581ndash7592 2008
[18] R P Singh S Sabarinath N Gautam R C Gupta and S KSingh ldquoPharmacokinetic study of the novel synthetic trioxaneantimalarial compound 97-78 in rats using an LC-MSMSmethod for quantificationrdquo Arzneimittel-Forschung vol 61 no2 pp 120ndash125 2011
[19] R P Singh S Sabarinath N Gautam R C Gupta and S KSingh ldquoLiquid chromatographic tandem mass spectrometricassay for quantification of 9778 and its metabolite 9763 apromising trioxane antimalarial in monkey plasmardquo Journal ofChromatography B vol 877 no 22 pp 2074ndash2080 2009
[20] V P Shah K K Midha J W A Findlay et al ldquoBioanalyticalmethod validationmdasha revisit with a decade of progressrdquo Phar-maceutical Research vol 17 no 12 pp 1551ndash1557 2000
[21] E RGerstner A F Eichler S R Plotkin et al ldquoPhase I trial withbiomarker studies of vatalanib (PTK787) in patients with newlydiagnosed glioblastoma treated with enzyme inducing anti-epileptic drugs and standard radiation and temozolomiderdquoJournal of Neuro-Oncology vol 103 no 2 pp 325ndash332 2011
[22] A Forero-Torres J Shah TWood et al ldquoPhase I trial of weeklytigatuzumab an agonistic humanizedmonoclonal antibody tar-geting death receptor 5 (DR5)rdquo Cancer Biotherapy and Radio-pharmaceuticals vol 25 no 1 pp 13ndash19 2010
[23] R C Kane ldquoThe clinical significance of statistical significancerdquoOncologist vol 13 no 11 pp 1129ndash1133 2008
[24] M J Hayat ldquoUnderstanding statistical significancerdquo NursingResearch vol 59 no 3 pp 219ndash223 2010
10 Malaria Research and Treatment
[25] I R Ribeiro and P Olliaro ldquoSafety of artemisinin and its deriva-tives A review of published and unpublished clinical trialsrdquoMedecine Tropicale vol 58 no 3 supplement pp 50ndash53 1998
[26] 2013 httpwwwfdagovdownloadsDrugsGuidanceCompli-anceRegulatoryInformationGuidancesucm073161pdf
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Malaria Research and Treatment 9
5 Conclusion
In conclusion we can say that the new compound CDRI9778 appears to be a safe and tolerable drug Its safety can befurther tested in multiple dose studies and if found tolerablecan be a good therapeutic option for malaria especiallymalaria resistant to available drugs
Conflict of Interests
The investigators did not receive any money for the conductof the study The study was sponsored by the Central DrugResearch Institute India The Innovator Institute a govern-ment organization had tied up with IPCA Ltd for the man-ufacture of the drug The drugs were supplied by IPCA LtdThey had no role in data collection recording and reportingTwo of the authors Dr Nitin Chandorkar and Dr AnilPareek are employees of IPCA Their role was in designingand conducting the study All the analyses were done inde-pendently by the investigatorsrsquo team
Acknowledgments
The authors would like to acknowledge the efforts of MrOnkar Rathod for helping in the execution of the study andMr Mitesh Sharma for giving his inputs for statistical analy-sis The research was funded by Central Drug Research Insti-tute (CSIR) Lucknow India This is a government organiza-tion
References
[1] ldquoWorldMalaria Reportrdquo 2005 httpwwwrollbackmalariaorgwmr2005
[2] A V Kondrashin ldquoMalaria in theWHOSoutheast Asia regionrdquoIndian Journal of Malariology vol 29 no 3 pp 129ndash160 1992
[3] U Arora G S Sonal G P S Dhillon andH GThakor ldquoEmer-gence of drug resistance in Indiardquo Journal of the Indian MedicalAssociation vol 106 no 10 pp 678ndash681 2008
[4] B M Greenwood D A Fidock D E Kyle et al ldquoMalaria pro-gress perils and prospects for eradicationrdquo Journal of ClinicalInvestigation vol 118 no 4 pp 1266ndash1276 2008
[5] C Singh and S K Puri ldquoSubstituted 124-trioxanes as anti-malarial agents and a process of producing the substituted 124-trioxanerdquo US Patent no 6316493 B1 2001
[6] C Singh N Gupta and S K Puri ldquoPhoto-oxygenation of ger-aniol synthesis of a novel series of hydroxy-functionalized anti-malarial 124-trioxanesrdquo Bioorganic and Medicinal ChemistryLetters vol 12 no 15 pp 1913ndash1916 2002
[7] C Singh N Gupta and S K Puri ldquoGeraniol-derived 124-trioxanes with potent in-vivo antimalarial activityrdquo Bioorganicand Medicinal Chemistry Letters vol 13 no 20 pp 3447ndash34502003
[8] C Singh N C Srivastav and S K Puri ldquoSynthesis and anti-malarial activity of 6-cycloalkylvinyl substituted 124-tri-oxanesrdquo Bioorganic andMedicinal Chemistry vol 12 no 22 pp5745ndash5752 2004
[9] A G Griesbeck T T El-Idreesy L-O Hoinck J Lex and RBrun ldquoNovel spiroanellated 124-trioxanes with high in vitro
antimalarial activitiesrdquo Bioorganic and Medicinal ChemistryLetters vol 15 no 3 pp 595ndash597 2005
[10] C Singh H Malik and S K Puri ldquoOrally active amino func-tionalized antimalarial 124-trioxanesrdquo Bioorganic and Medici-nal Chemistry Letters vol 14 no 2 pp 459ndash462 2004
[11] C SinghNGupta and S K Puri ldquoPhotooxygenation of 3-aryl-2-cyclohexenols synthesis of a new series of antimalarial 124-trioxanesrdquo Tetrahedron Letters vol 46 no 2 pp 205ndash207 2005
[12] C Singh HMalik and S K Puri ldquoOrally active 124-trioxanessynthesis and antimalarial assessment of a new series of 9-functionalized 3-(1-arylvinyl)-125-trioxaspiro[55]undecanesagainst multi-drug-resistant Plasmodium yoelii nigeriensis inmicerdquo Journal of Medicinal Chemistry vol 49 no 9 pp 2794ndash2803 2006
[13] C Singh S Chaudhary and S K Puri ldquoNew orally active deri-vatives of artemisinin with high efficacy against multidrug-resistant malaria in micerdquo Journal of Medicinal Chemistry vol49 no 24 pp 7227ndash7233 2006
[14] C Singh U Sharma G Saxena and S K Puri ldquoOrally activeantimalarials synthesis and bioevaluation of a new series ofsteroid-based 124-trioxanes against multi-drug resistantmalaria in micerdquo Bioorganic and Medicinal Chemistry Lettersvol 17 no 15 pp 4097ndash4101 2007
[15] C Singh R Kanchan U Sharma and S K Puri ldquoNewadamantane-based spiro 124-trioxanes orally effective againstrodent and simianmalariardquo Journal ofMedicinal Chemistry vol50 no 3 pp 521ndash527 2007
[16] C Singh S Chaudhary RKanchan and SK Puri ldquoConversionof antimalarial drug artemisinin to a new series of tricyclic 124-trioxanesrdquo Organic Letters vol 9 no 21 pp 4327ndash4329 2007
[17] C Singh V P Verma N K Naikade A S Singh M Hassamand S K Puri ldquoNovel bis- and tris-124-trioxanes synthesis andantimalarial activity against multidrug-resistant Plasmodiumyoelii in swiss micerdquo Journal of Medicinal Chemistry vol 51 no23 pp 7581ndash7592 2008
[18] R P Singh S Sabarinath N Gautam R C Gupta and S KSingh ldquoPharmacokinetic study of the novel synthetic trioxaneantimalarial compound 97-78 in rats using an LC-MSMSmethod for quantificationrdquo Arzneimittel-Forschung vol 61 no2 pp 120ndash125 2011
[19] R P Singh S Sabarinath N Gautam R C Gupta and S KSingh ldquoLiquid chromatographic tandem mass spectrometricassay for quantification of 9778 and its metabolite 9763 apromising trioxane antimalarial in monkey plasmardquo Journal ofChromatography B vol 877 no 22 pp 2074ndash2080 2009
[20] V P Shah K K Midha J W A Findlay et al ldquoBioanalyticalmethod validationmdasha revisit with a decade of progressrdquo Phar-maceutical Research vol 17 no 12 pp 1551ndash1557 2000
[21] E RGerstner A F Eichler S R Plotkin et al ldquoPhase I trial withbiomarker studies of vatalanib (PTK787) in patients with newlydiagnosed glioblastoma treated with enzyme inducing anti-epileptic drugs and standard radiation and temozolomiderdquoJournal of Neuro-Oncology vol 103 no 2 pp 325ndash332 2011
[22] A Forero-Torres J Shah TWood et al ldquoPhase I trial of weeklytigatuzumab an agonistic humanizedmonoclonal antibody tar-geting death receptor 5 (DR5)rdquo Cancer Biotherapy and Radio-pharmaceuticals vol 25 no 1 pp 13ndash19 2010
[23] R C Kane ldquoThe clinical significance of statistical significancerdquoOncologist vol 13 no 11 pp 1129ndash1133 2008
[24] M J Hayat ldquoUnderstanding statistical significancerdquo NursingResearch vol 59 no 3 pp 219ndash223 2010
10 Malaria Research and Treatment
[25] I R Ribeiro and P Olliaro ldquoSafety of artemisinin and its deriva-tives A review of published and unpublished clinical trialsrdquoMedecine Tropicale vol 58 no 3 supplement pp 50ndash53 1998
[26] 2013 httpwwwfdagovdownloadsDrugsGuidanceCompli-anceRegulatoryInformationGuidancesucm073161pdf
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
10 Malaria Research and Treatment
[25] I R Ribeiro and P Olliaro ldquoSafety of artemisinin and its deriva-tives A review of published and unpublished clinical trialsrdquoMedecine Tropicale vol 58 no 3 supplement pp 50ndash53 1998
[26] 2013 httpwwwfdagovdownloadsDrugsGuidanceCompli-anceRegulatoryInformationGuidancesucm073161pdf
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom





























