Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Clinical experience using a tensor fascia lata flapin oncology patients
Akira Saito • Hidehiko Minakawa • Noriko Saito •
Kazuo Isu • Hiroaki Hiraga • Toshihisa Osanai
Received: 5 March 2012 / Accepted: 19 July 2013
� Springer Japan 2013
Abstract
Purpose The tensor fascia lata (TFL) flap is used to
reconstruct various anatomical structures in different
regions of the body. We herein describe the use of TFL
flaps for a variety of indications, and discuss the results of
such procedures with respect to postoperative complica-
tions in oncology patients.
Methods We reviewed 15 oncology patients who were
treated with TFL flaps.
Results The lesions were located in the groin in five patients,
the lower abdomen in five, and the buttocks, ischium, shoul-
der, thigh and upper abdomen in one patient each. Abdominal
wall reconstruction was performed in nine patients. Three
patients underwent resection of femoral vessels and the tumor
in the groin, followed by a vascular graft implant. In these
patients, the combined flaps were transferred to reconstruct
the defects. Nine patients developed complications. No total
flap loss occurred in any patient.
Conclusions Postoperative complications, such as necro-
sis in the distal part of the flap (33 %) and ventral hernias
(11 %) were seen, but these percentages were comparable
to those seen in previous reports. Our review shows that the
TFL flap is useful to reconstruct the defects in various
anatomical sites in oncology patients.
Keywords Tensor fascia lata flap � TFL flap �Reconstruction � Abdominal wall reconstruction �Oncologic patients
Introduction
The tensor fascia lata (TFL) flap is a versatile flap, and is used
both as a pedicled flap and as a free flap to reconstruct struc-
tures in various anatomical regions [1]. A TFL flap is the
preferred choice of pedicled flap used in the treatment of
pressure sores and inguinal and abdominal defects [2]. In
particular, the TFL flap is most commonly used for abdominal
wall reconstruction, since the flap undersurface is dense with a
strong sheet of fascia, the overlying skin is reliably supplied by
an anatomically constant vascular pedicle and it can offer
simultaneous fascia and skin replacement as a single unit [3].
This study aimed to show the use of TFL flaps for a
variety of indications and to discuss the postoperative
complications associated with these procedures in oncol-
ogy patients.
Patients
From 2001 to 2010, 15 oncology patients [seven (47 %)
males and eight (53 %) females] were treated with TFL
muscle flaps or myocutaneous flaps at the Hokkaido Cancer
Center, and these patients were included in a retrospective
chart review. Their mean age was 55.5 years (range
30–81 years). The mean follow-up time after surgery was
37 months (range 0–116 months).
A. Saito (&) � H. Minakawa
Division of Plastic and Reconstructive Surgery, Hokkaido
Cancer Center, Kikusui 4-2, Shiroishi-ku,
Sapporo 003-0804, Japan
e-mail: [email protected]
N. Saito
Department of Plastic and Reconstructive Surgery, Graduate
School of Medicine, Hokkaido University, Kita 15, Nishi 7,
Kita-ku, Sapporo 060-8638, Japan
K. Isu � H. Hiraga � T. Osanai
Division of Orthopaedics, Hokkaido Cancer Center, Kikusui 4-2,
Shiroishi-ku, Sapporo 003-0804, Japan
123
Surg Today
DOI 10.1007/s00595-013-0733-z

Results
The patient data are summarized in Table 1. Defects after the
resection of soft tissue sarcomas were the most common
precondition (n = 13), followed by radiation ulcers (n = 2).
The lesions were located in the groin in five patients, the
lower abdomen in five patients, and in the buttocks, ischium,
shoulder, thigh and upper abdomen in one patient each.
Among 13 patients presenting with manifest tumor disease,
10 underwent surgery for primary disease and three for
recurrent disease. Among all 15 patients, six patients had
been administered radiation therapy (44–66 Gy) at the
recipient site prior to the current operation.
All flaps were harvested unilaterally. One flap was
transferred as a free vascularized flap and the other as a
pedicle flap. The flaps were harvested as a myocutaneous
flap in seven patients, as a muscle flap in two, as a muscle
flap combined with the vastus lateralis (VL) muscle in
three, as a myocutaneous flap combined with the VL
muscle in one, as a myocutaneous flap combined with the
rectus femoris muscle in one and as a myocutaneous flap
combined with the posterior thigh fasciocutaneous flap in
one case.
In all nine patients treated with a myocutaneous flap, the
donor site required a skin graft. There were eight full-
thickness abdominal wall defects and one partial-thickness
abdominal wall defect (defects involving only the loss of
skin and subcutaneous tissue). Abdominal wall recon-
struction was performed in these patients. Among these nine
patients, one developed a ventral hernia postoperatively.
Overall, nine patients (60 %) developed complications.
None of the patients had total flap loss. Four patients had
Table 1 Patient summary
Case Age Sex Diagnosis Previous treatment Site of the
lesion
Free or
pedicled
Type of flap Vascular
graft
Abdominal
wall
reconstruction
Complication Revision
surgeryOperation RT
1 30 M Synovial
sarcoma
(-) (-) Shoulder Free TFL mc-flap (-) (-) Wound
infection
(?)
2 43 F Chondrosarcoma (-) (-) Lower
abdomen
Pedicled TFL m-flap ? VL
m-flap
(-) (?) Partial flap
necrosis
wound
infection
(?)
3 56 F Epithelioid
sarcoma
(?) 66 Gy Ischium Pedicled TFL-mc
flap ? Posterior
thigh flap
(-) (-) Wound
infection
(-)
4 64 F MFH (-) 50 Gy Groin Pedicled TFL-m flap ? VL
m-flap
Autologous
vessel
(?) (-) N/A
5 76 F Radiation ulcers (?) 57 Gy Buttock Pedicled TFL mc-flap (-) (-) Partial flap
necrosis
wound
infection
(-)
6 81 M MFH (-) 44 Gy Groin Pedicled TFL m-flap ? VL
m-flap
Prosthesis (?) (-) N/A
7 53 M Radiation ulcers (?) 59.4 Gy Thigh Pedicled TFL mc-
flap ? VL
m-flap
(-) (-) (-) N/A
8 61 M Fibrosarcoma (?) (-) Groin Pedicled TFL mc-flap (-) (?) Partial flap
necrosis
ventral
hernia
(-)
9 45 F Synovial
sarcoma
(-) 44 Gy Lower
abdomen
Pedicled TFL m-flap ? RF
m-flap
Prosthesis (?) (-) N/A
10 62 F MFH (-) (-) Lower
abdomen
Pedicled TFL mc-flap (-) (?) Wound
infection
(-)
11 72 F MFH (-) (-) Lower
abdomen
Pedicled TFL mc-flap (-) (?) Partial flap
necrosis
(?)
12 30 M Leiomyosarcoma (?) (-) Groin Pedicled TFL m-flap (-) (-) Wound
dehiscence
(-)
13 44 F MPNST (-) (-) Lower
abdomen
Pedicled TFL mc-flap (-) (?) (-) N/A
14 42 M Clear cell
sarcoma
(-) (-) Upper
abdomen
Pedicled TFL m-flap (-) (?) (-) N/A
15 74 M Liposarcoma (-) (-) Groin Pedicled TFL mc-flap (-) (-) Partial flap
necrosis
(?)
RT radiation therapy, MFH malignant fibrous histiocytoma, MPNST malignant peripheral nerve sheath tumor, TFL mc-flap tensor fascia lata myocutaneous flap, TFL m-flap
tensor fascia lata muscle flap, VL m-flap vastus lateralis muscle flap, RF m-flap rectus femoris muscle flap
Surg Today
123
distal necrosis of the skin paddle and one had distal
necrosis of the muscle flap. Five patients developed wound
infections, and one developed wound dehiscence. Among
the nine patients with complications, four required surgical
revisions. These procedures consisted of local wound
debridement, readvancement of the muscle flap, skin
grafting and the transfer of another flap. Delayed wound
healing occurred in five patients; however, no secondary
procedure was required in these patients.
The medical history of the 15 patients was acquired
from the patient charts. Of these patients, five died because
of their malignant disease and one had died the day after
the operation, but the cause of that one death was unknown.
Case report
Case 13
A 44-year-old female presented with a tumor in the left
groin. A needle biopsy had confirmed the diagnosis of
sarcoma at her previous hospital, and she was referred to
the division of Orthopaedics, Hokkaido Cancer Center, for
treatment. The tumor was approximately 5 9 5 cm in size
(Fig. 1). She underwent a wide local excision of the tumor,
including part of the rectus abdominis muscle and the
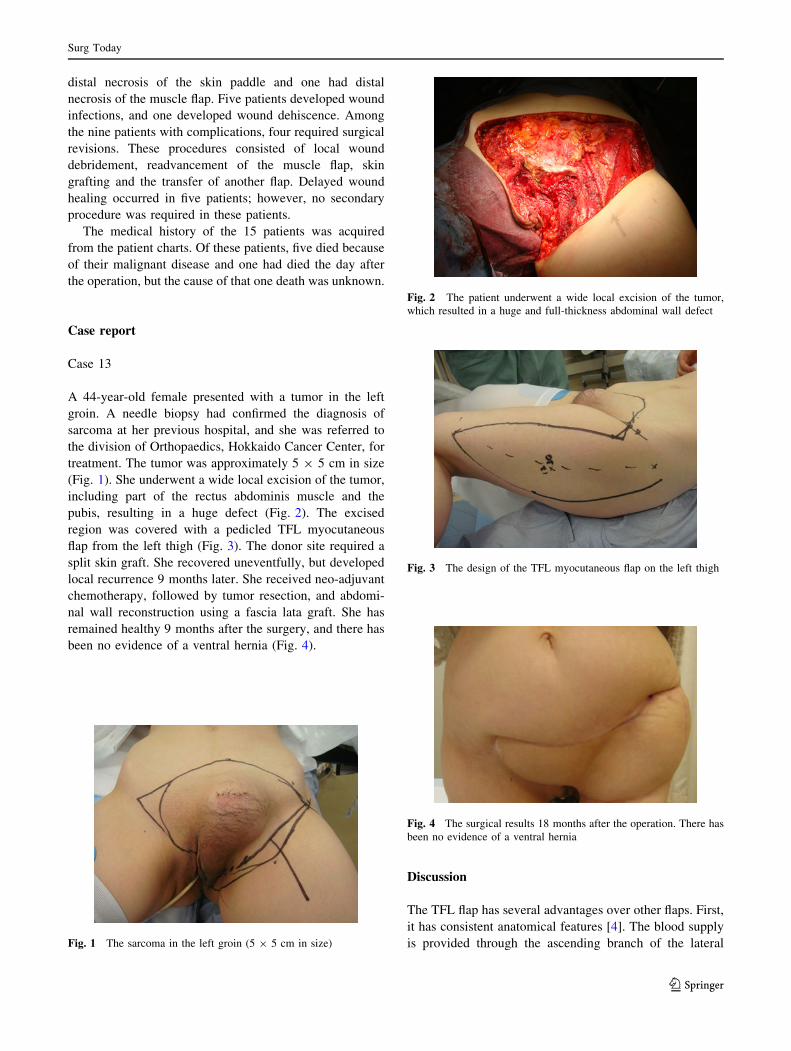
pubis, resulting in a huge defect (Fig. 2). The excised
region was covered with a pedicled TFL myocutaneous
flap from the left thigh (Fig. 3). The donor site required a
split skin graft. She recovered uneventfully, but developed
local recurrence 9 months later. She received neo-adjuvant
chemotherapy, followed by tumor resection, and abdomi-
nal wall reconstruction using a fascia lata graft. She has
remained healthy 9 months after the surgery, and there has
been no evidence of a ventral hernia (Fig. 4).
Discussion
The TFL flap has several advantages over other flaps. First,
it has consistent anatomical features [4]. The blood supply
is provided through the ascending branch of the lateralFig. 1 The sarcoma in the left groin (5 9 5 cm in size)
Fig. 2 The patient underwent a wide local excision of the tumor,
which resulted in a huge and full-thickness abdominal wall defect
Fig. 3 The design of the TFL myocutaneous flap on the left thigh
Fig. 4 The surgical results 18 months after the operation. There has
been no evidence of a ventral hernia
Surg Today
123

femoral circumflex artery [5], which arises from the pro-
fundus femoris in 80 % of patients, or alternately, from the
common femoral or medial circumflex arteries [1]. Raising
the TFL flap is an uncomplicated procedure, and an ade-
quate-sized flap can be obtained [6]. Moreover, donor-site
morbidity is not critical [7, 8]. The donor sites for flaps up
to 10 or 12 cm in size can be closed directly [7].
Using a TFL flap is a reconstructive option for the
treatment of defects in various anatomical regions,
including the head, neck, trunk, upper limb and lower limb.
The flap can be used as either a pedicled flap or a free flap.
The TFL flap is most commonly used as a pedicled flap for
the treatment of pressure sores and groin and abdominal
wall defects [2]. In particular, this flap seems to be well
suited for abdominal wall reconstruction, as it structurally
resembles the strong and dense fascia and the thin skin
paddle of the abdominal wall [3, 8]. As a free flap, the TFL
is used for reconstructing large abdominal wall defects, as
well as head and neck, composite extremity and perineal
defects [9].
In this series, 14 out of 15 flaps were used as pedicled
flaps and only one flap was used for functional recon-
struction of a shoulder defect following tumor ablation; the
pedicled flap is frequently modified for reconstruction in
the groin and the lower abdomen. To reconstruct larger
defects, the TFL flap can be combined and used with other
flaps like the rectus femoris muscle flap [10], anterolateral
thigh flap [11] or VL muscle flap [12, 13]. We used
combined flaps in six patients; a muscle flap combined with
the VL muscle in three patients, a myocutaneous flap
combined with the VL muscle in one, a myocutaneous flap
combined with the rectus femoris muscle in one and a
myocutaneous flap combined with the posterior thigh fas-
ciocutaneous flap in one case.
All the flaps required a relatively large volume of tissue
for transfer because of the large defects following tumor
resection or debridement of irradiated tissue.
The groin is believed to be the most common site of
distal extremity graft infection [14]. The incidence of
prosthetic vascular graft infections is 1–6 % [14]. The use
of a muscle flap to cover exposed native vessels or to
salvage prosthetic material used in arterial reconstruction
has also been advocated [15]. A muscle provides bulk to
obliterate any dead space, thus diminishing the possibility
of recurrent infection [14]. The flap options include the
sartorius muscle, rectus femoris muscle, rectus abdominis
muscle, gracilis muscle and omental flaps [14, 16].
In oncology patients, it is necessary to not only cover the
vessels, but also reconstruct the skin and soft tissue defects.
In this series, three patients underwent the resection of
femoral vessels, together with the tumor in the groin
region, followed by vascular grafting. In all of these
patients, the combined flaps were transferred to reconstruct
the skin and soft tissue defects and to obliterate the dead
space around the grafts. One patient with an autologous
vessel graft died the day after the operation, but the cause
of death was unknown. Two patients received prosthetic
grafts. One of them had tumor recurrence that caused
occlusion of the femoral artery, and this patient died of
sepsis 20 months after the operation. In another patient, no
infection was observed at the 30-month follow-up.
Although the TFL flap is said to have consistent ana-
tomical features [4], distal necrosis of the TFL flap has
been frequently reported [13, 17–19]. Gosain et al. [20]
evaluated the perfusion of an extended TFL flap raised to
include the skin as far as the lateral aspect of the knee.
They described that the flap usually becomes unreliable
about 8–10 cm proximal to the knee joint. Muramatsu et al.
[17] have reported that one of 10 patients in their study
developed partial necrosis. Agarwal et al. [13] have
reported two cases of marginal flap necrosis among 15
cases studied. Rifaat et al. [18] have reported that distal flap
necrosis occurred in four out of 12 patients. Similarly, de
Vries Reilingh et al. [19] described that partial flap necrosis
can be expected in 10–50 % of patients. In this study, no
total flap loss occurred, but there were five cases of distal
necrosis (33 %), which was comparable to that docu-
mented in other reports.
It is usually assumed that the donor sites for flaps up to
10 or 12 cm in size can be closed directly [7]. However, the
most common problem of the TFL flap is reported to be
excessive tension and eventual suture separation at the
confluence of the donor site flaps and the TFL flap [21]. In
our series, the donor site required a skin graft in all nine
patients with a myocutaneous flap to prevent suture sepa-
ration, even though the flap was less than 10 cm in width
for some patients.
The TFL flap can be used to reconstruct the musculo-
fascial layer of the abdominal wall to prevent postoperative
hernia formation; however, a hernia can still be a possible
complication. Rifaat et al. [18] have reported that one out
of five patients developed a ventral hernia after undergoing
abdominal wall reconstruction with the TFL flap. Tukiai-
nen and Leppaniemi [9] have reported that a ventral hernia
occurred in one among 20 patients who underwent
abdominal wall reconstruction with a free TFL flap. Tang
et al. [22] have recommended enforcing repair with a
synthetic or biological mesh to minimize the incidence of
ventral hernia. In our series, one among the nine patients
developed a ventral hernia, but a synthetic or biological
mesh had not been used for repair.
Radiation therapy is a treatment modality used for the
pre- or postoperative local control of malignant disease
[23]. Radiation damage is known to delay healing and
increase the risk of wound infection [24], and it is rea-
sonable to choose muscle or myocutaneous flaps for an
Surg Today
123

irradiated field, since they may be more resistant to bac-
terial infection or may not cause residual infection [23].
In this study, six patients had undergone preoperative
radiation therapy, and two patients developed complica-
tions (33 %). A wound infection developed in one of these
patients, and distal flap necrosis along with wound infec-
tion developed in another.
Conclusion
The TFL flap has proven to be versatile, and is associated
with several advantages, including consistent anatomical
features, an ease of elevation and simple donor-site repair.
In this study, we reviewed our clinical experiences using
TFL flaps in oncology patients. Postoperative complica-
tions such as distal necrosis of the flap developed in 33 %
of patients and a ventral hernia developed in 11 %, but
these incidences were comparable to those reported in
previous studies.
The number of patients in this series is very small, but
our review shows that the TFL flap is useful to reconstruct
the defects in various anatomical sites, because there were
no total flap loss or donor-site complications.
Conflict of interest None.
References
1. Bulstrode NW, Kotronakis I, Baldwin MA. Free tensor fasciae
latae musculofasciocutaneous flap in reconstructive surgery: a
series of 85 cases. J Plast Reconstr Aesthet Surg. 2006;59:130–6.
2. Koshima I, Urushibara K, Inagawa K, Moriguchi T. Free tensor
fasciae latae perforator flap for the reconstruction of defects in the
extremities. Plast Reconstr Surg. 2001;107:1759–65.
3. Caffee HH. Reconstruction of the abdominal wall by variations of
the tensor fasciae latae flap. Plast Reconstr Surg. 1983;71:
348–53.
4. Hill HL, Nahai F, Vasconez LO. The tensor fascia lata myocu-
taneous free flap. Plast Reconstr Surg. 1978;61:517–22.
5. Hubmer MG, Schwaiger N, Windisch G, Feigl G, Koch H, Haas
FM, et al. The vascular anatomy of the tensor fasciae latae per-
forator flap. Plast Reconstr Surg. 2009;124:181–9.
6. Ohno Y, Tanaka K, Kanematsu T, Noguchi M, Okada M, Ka-
mitamari A, et al. Reconstruction of a pelvic floor defect using a
pedicled tensor fascia lata flap: a new technique to prevent
radiation injury for pediatric patients with advanced pelvic
tumors. J Pediatr Surg. 2008;43:947–50.
7. Nahai F, Hill L, Hester TR. Experiences with the tensor fascia
lata flap. Plast Reconstr Surg. 1979;63:788–99.
8. Safak T, Klebuc MJ, Kecik A, Shenaq SM. The subcutaneous
pedicle tensor fascia lata flap. Plast Reconstr Surg. 1996;97:
765–74.
9. Tukiainen E, Leppaniemi A. Reconstruction of extensive
abdominal wall defects with microvascular tensor fasciae latae
flap. Br J Surg. 2011;98:880–4.
10. Koshima I, Moriguchi T, Inagawa K, Urushibara K. Dynamic
reconstruction of the abdominal wall using a reinnervated free
rectus femoris muscle transfer. Ann Plast Surg. 1999;43:199–203.
11. Sasaki K, Nozaki M, Nakazawa H, Kikuchi Y, Huang T.
Reconstruction of a large abdominal wall defect using combined
free tensor fasciae latae musculocutaneous flap and anterolateral
thigh flap. Plast Reconstr Surg. 1998;102:2244–52.
12. Lin MT, Chang KP, Lin SD, Lai CS, Yang YL. Tensor fasciae
latae combined with tangentially split vastus lateralis musculo-
cutaneous flap for the reconstruction of pressure sores. Ann Plast
Surg. 2004;53:343–7.
13. Agarwal AK, Gupta S, Bhattacharya N, Guha G, Agarwal A.
Tensor fascia lata flap reconstruction in groin malignancy. Singap
Med J. 2009;50:781–4.
14. Seify H, Moyer HR, Jones GE, Busquets A, Brown K, Salam A,
et al. The role of muscle flaps in wound salvage after vascular
graft infections: the emory experience. Plast Reconstr Surg.
2006;117:1325–33.
15. Morasch MD, Sam AD 2nd, Kibbe MR, Hijjawi J, Dumanian
GA. Early results with use of gracilis muscle flap coverage of
infected groin wounds after vascular surgery. J Vasc Surg.
2004;39:1277–83.
16. Alkon JD, Smith A, Losee JE, Illig KA, Green RM, Serletti JM.
Management of complex groin wounds: preferred use of the
rectus femoris muscle flap. Plast Reconstr Surg. 2005;115:
776–83 (discussion 84–5).
17. Muramatsu K, Ihara K, Taguchi T. Selection of myocutaneous
flaps for reconstruction following oncologic resection of sarcoma.
Ann Plast Surg. 2010;64:307–10.
18. Rifaat MA, Abdel Gawad WS. The use of tensor fascia lata
pedicled flap in reconstructing full thickness abdominal wall
defects and groin defects following tumor ablation. J Egypt Natl
Canc Inst. 2005;17:139–48.
19. de Vries Reilingh TS, Bodegom ME, van Goor H, Hartman EH,
van der Wilt GJ, Bleichrodt RP. Autologous tissue repair of large
abdominal wall defects. Br J Surg. 2007;94:791–803.
20. Gosain AK, Yan JG, Aydin MA, Das DK, Sanger JR. The vas-
cular supply of the extended tensor fasciae latae flap: how far can
the skin paddle extend? Plast Reconstr Surg. 2002;110:1655–61
(discussion 62–3).
21. Aslan G, Tuncali D, Bingul F, Ates L, Yavuz N. The ‘‘duck’’
modification of the tensor fascia lata flap. Ann Plast Surg.
2005;54:637–9.
22. Tang R, Gu Y, Gong DQ, Qian YL. Immediate repair of major
abdominal wall defect after extensive tumor excision in patients
with abdominal wall neoplasm: a prospective review of 27 cases.
Ann Surg Oncol. 2009;16:2895–907.
23. Kurul S, Dincer M, Kizir A, Uzunismail A, Darendeliler E.
Plastic surgery in irradiated areas: analysis of 200 consecutive
cases. Eur J Surg Oncol. 1997;23:48–53.
24. Staiano JJ, Wong L, Butler J, Searle AE, Barton DP, Harris PA.
Flap reconstruction following gynaecological tumour resection
for advanced and recurrent disease–a 12 year experience. J Plast
Reconstr Aesthet Surg. 2009;62:346–51.
Surg Today
123





























