Embed Size (px)
Citation preview

Endodontics
Clinical evaluation of audiometric control root canaltreatment: A retrospective case study
Masaki Murakami, DDSVShintaro Inoue, DDS, PhDVNoboru Inoue, DDS, PhD, FICD^
Objective: The purpose of this study was to retrospectively assess the success of endodontic treatmentthat tiad been guided by audiometric (electronic) measurement. Method and materials: The lengths of66 infected root canals tbat demonstrated periapical patbosis were accurately measured by the Sono-Explorer before root canal obturation. Tbe results over time intervals ot 1 month to 20 years were evalu-ated on tbe basis of radiographie examinations. Results: Tbe rate of successful treatment was 90,4% forshort-filled root canals, 94.5% for flush-filled root canals, and a low 50.0% for long-filled root canals, Tberate of suocessful endodontic tberapy was 87,8% for restorations that did not exceed the apical foramenbut reached the apioal oonstriotion and 95,3% if cases in wbtcb tbe apical radiolucencies were disappear-ing were included as suocesses. If oases of uninlenlional long-filling (overextension) were excluded, thesucoess rate was as high as 98,4%, Conclusion: Tbe poor performance of overfilled root canals indicatestbat practitioners should not overextend these restorations. Use of the Sono-Explorer aided successfultreatment of infected root canals, (Quintessence Inl2002:33:465-^75)
Key words: apical limit, audiometric cotitrol, endodontic therapy, root canal, Sono-Explorer
CUNICAL RELEVANCE: Tbe electric (audiometric) rootcanal measurement metbod is more accurate than theradiograpbio measurement metbod, and an accuratemeasurement of root canal length is considered key tosuccessful endodontio treatment.
The success of endodontic treatment depends on anumber of factors, the most important of which is
the accurate measurement of root canal length. Manystudies have shown that a root canal has to be mea-sured carefully to determine an accurate workinglength for its treatment,'-** To proceed with treatmentwithout first obtaining an accurate measurement is notto apply due diligence in treatment. Guesswork insuch circumstances often resuh in underinstrumenta-tion or overinstrumentation, and underextension oroverextension. Care should fae taken not to waste timeand effort in this manner and to strive for the mostfavorable outcome.
'Staff, I roje Dental Clinic, Toltyo, Japan,
'Director, Inoue Dental Clinic, Tokyo, Japan; torme^iy. Visiting Protessor,Division ot Endodontics, Faculty of Dentistry, University of WesternOnrario, Lenden, Ontario, Canada,
Reprint requests ; Dr Noboru Incue, Inoue Dentai Clinic, Nisseki-Mitsjbishi Building B l , 1-3-12 Nishi-simbastii, Minato-kj, Tci<yo 1O5-0CC3,Japan, Fax; 813-3595-3599, E - mail ;se-i noue© siren, oon, ne.jp
Ideally, a practitioner should measure the rootcanal length up to the biologic apex. This measure-ment is then used as a basis for determining workinglength, the ideal length of instrumentation and filling.Studies have also shown the biologic apical foramen,or dentinocementum juncfion, is generally located 0,5to 1,0 mm or more short of the anatomic apex,'-^
Despite this knowledge, many practitioners haverepeatedly used the radiographie apex as a basis forclassification in conducting outcome research onendodontic therapy. In so doing, they classify a fillingthat reaches the radiographie apex as flush and anyfilling beyond or short of the apex as overfilled orunderfilled, respectively. Given the results of manyanatomic studies and knowledge of the function ofelectronic apex locators, the authors question theaccuracy of such a basis for classification,
Schilder' distinguished between the terms over-extension (exceeding the root apex on the radiograph)and underextension and the terms overfilling andunderfilling. Overfilling is achieved when root obtura-fion leads to a homogenous, dense filling of the rootcanal. Overextension and underextension thereforerefer solely to the vertical position of the root canalfilling, regardless of its volume. In overextension andunderextension, the filling may be grossly underfilled.This may give rise to the formation of large deadspaces or voids and hollows in the dental pulp cavity,resulting in exudation of tissue fluid and ultimately to
Quintessence Internationai465

• Murakami étal
Fig 1a Radiograpii for determining Itie working length witti ttieSo no-Explorer.
Fig 1b Radiograph after root canal obturation. The gutta-percinafills the entire root canal spaoe. Because this tooth is in torsiver-sion. the image shows a mesioeocentric projection.
Fig 2a Radiograph revealing a bent H file in the canai. The fiiewas removed with ultrasonic vibration
Fig 2b Radiograph attef root canal obturation The root canalhas been tilled by the laterovertical oondensation method, ensur-ing signitioant dispersal of restorative material to the accessorychannels and lateral oanals.
failure of the surgical procedure. Schilder' thereforeargued that overfilling may be permitted.
In contrast to this view, the authors are of the opin-ion that overfilling is best avoided, because it is ourexperience that, when gutta-percha leaks outside ofthe apical foramen, lesions wii! arise in the apical peri-odontium. In addition, obturation of the apical fora-men witb cementum as tbe ideal stop is difficult toachieve; it may take considerable time to absorb, andbiologic healing may be difficult.
Tbe authors have tried a spatial obturation tecb-nique in wbicb the root canal space is filled so tbatgutta-percha does not leak outside tbe root apex. Inthis metbod, tbe precise position of the apical foramenis measured witb a Sono-Explorer {DentalElectronics), and an apical stop is formed approxi-mately 0.5 mm short of tbe foramen. The main gutta-percha is coated witb sealer, an extremely small
amount of eucapercba is applied to tbe gutta-percha,and it is first fixed by lateral condensation to preventthe gutta-percha tip from protruding outside tbe apicalforamen. A plug is tbus formed in the root apex. Tberoot canal space is automatically softened by tberino-mecbanical condensation witb a McSpaddetiCompactor (Ranson & Randolpb) and N.T. Condenser(Analytic Endodontics), and vertical compaction isapplied to provide spatial obturation of tbe root canalThe name used by tbe autbors to describe this proce-dure is tbe laterovertical condensation method, wbichis currently under investigation (Figs 1 to 4).
It is evident tbat this method does not lend itself tothe phenomena described by Schilder' as overexten-sion and underextension, not to mention overfilling.Because this metbod can also manage tbe lateralcanal, it can certainly be regarded as a biologic obtu-ration tecbnique.
466

• Murakami et al
Fig 3a Radiograph tor determining the working lenglh wilh theSono-Explorer. The tooth is in torsiversion. Fig 3b Radiograph after root canal obturalion. Lateroverlical
condensation has completely filled Ihe canal and ensured disper-sion of the restorative material to accessory channels and lateralcanals.
Furthermore, tbe location of tbe anatomic apicalforamen and apical constriction do not always coin-cide clinically^-'" (Figs 5 to 7). This fact was tbe basisfor developing an electronic device to apply to thetneasurement of root canal length, instead of having torely solely on the radiographie method."-^'
Measurement of the root canal length with an elec-tronic device ensures accuracy, despite the differencesin the locations of the anatomic apex and the apicalforamen. The method is also an effective way toreduce a patient's exposure to x-ray radiation. Theelectronic apex locator meets Ingle and Bakiand's cri-teria'* for measuring working length with an effectiveendodontic device. These criteria are (1) accuracy ofmeasurement, (2) ease of operation, and (3) repro-ducibility of results.
To test the long-term efficacy of endodontic treat-ment, outcomes were analyzed in a sample of patientswho received endodontic treatment that was guidedby the clinical results of electrical root canal lengthtneasurement.
METHOD AND MATERIALS
A clinical outcome study was done on patients aged20 to 65 years who had received root canal treatmentat the Inoue Dental Clinic between 1970 and 1990,Sixty-six endodontically treated teeth were selected fora follow-up examination. In the sample there were 25incisors, 13 premolars, and 13 molars, all exhihitingapical pathoses before clinical examination. The Sono-Explorer had been used to measure the root canallength in all 66 cases. Based on these measurements,the infected root canals were treated, prepared andfilled. The patients were divided into two groups,based on the filling material used. There was no differ-
Fig 4 Radiograph after roo[ canai ooturation. ihie sealer wasplaced and canals were obturated by the lateroverlicat condensa-tion of gutta-percha The material is dispersed to the accessorychannels and lateral canals.
ence in the ages or health of the patients in the twosample groups.
In a number of the 66 treatments, a combination offilling techniques using siiver point and gutta-percbawere used. Neodain (Neo Dental Cbemical Products}was used as the root canal sealer. The laterovertical con-densation method was used as the obturation procedure.
Teetb treated witb silver point-type root fillingmaterial were classified as group 1, because tbis typeof filling is electroconductive, and the lengtb of thefilling can he measured and reexamined accuratelywith the Sono-Explorer at the time the point is seated.
The remaining treatments used only gutta-perchafilling material with the endodontic sealer cementDentalis (KEZ, Neo Dental Chemical Products) as theroot canal sealer. Again, obturation was completed witbthe laterovertical condensation method. Teeth treatedwith this type of root filling were classified as group 2.
Quintessence International 467

Fig 5a (ieft) Radiograph tor determiningfhe working lengtfi with the Sono-Expfore;,Efectronic measuring shows an apioai fora-men mat is shorter than the radiographieroot ape«.
Fig 5b (right) Radiograph after rooi canaiobturation. The canai was filied wifh gutta-peroha, buf restoration resuited in overex-tension because the apicai stop wasincompiefe.
Fig 5c (left) Postsurgicai radiograph.Alter thG exoess gutta-percha was surgi-caiiy scraped out of the canai apex, it wasconfirmed that the apical foramen was afIhe same position as it was at the time otthe eiectronio measurement.
Fig 5d (rigiit) Extracted tooth from a dif-ferent patient, reveafing that the anatomicapex (A) and the position of the apicaf fora-men (B) may be remari<abiy different.
For group 2, the Sono-Explorer was used to obtainthe exact root canal length down to the apical fora-men, and this measurement was confirmed with radio-graphs. An apical stop was then formed 0.5 mmshorter than the measurement of the root canal length,and the canal was filled carefully so that the materialdid not go beyond the apical constriction,''
In subsequent follow-up examinations, the degreeof apical healing was assessed with radiographs.Radiographs taken at the follow-up examination werecompared with the radiographs taken at the titne ofobturation. The radiographs were specifically exam-
ined for changes in the apical radiolucency and thecondition of the trabecular bone. Close attention waspaid to identify the lamina dura and the periodontalmembrane space. The results of these radiographieexaminations were classified according to the changein radiolucency: (1) no change, (2) smaller or healing,and (3) disappeared or healed. In no instance was thelesion larger.
To allow comparison with other endodontic follow-up examinations reported by other practitioners, thelengths of root canal fillings were classified accordingto a system previously described by Bender et aV^

• Murakami et al
Fig 6a Badiograoti for determining the working length with theSono-Explorer. The position of the reamer stiows that Ihe workingiergth is shorter than the radiographie root apex.
Fig6b Raacgrr-r.- .-.••••••.-:•-;•-. ciuration. Tiie sealer, whichwas placea in the ¿a.-i.e locaüún ¿s (he lip ot the reamer, hasexpressed out, confirming the presenoe oí an apical foramen.
Fig 6e Raoiograpn at the 10-year recall. The radioluoenoy hascompletely aisappeared and healed well.
Heling," and Seltzer'^: According to their classifica-tion, a flush filling is a root canal ending 0.0 to 1-5 mmshort of the radiographie apex, a short filling is a fill-ing ending 1.6 mm to 3.0 mm short of the radio-graphic apex, and a long filling is any filling ending 0.1mra or more beyond the radiographie apex.
Because of variations in patient compliance, thefollow-up examinations were not always performedover the same time period. For this reason, the timesof follow-up examinations after root canal treatmentwere rounded off to 1, 2, and 3 months and 1, 3, 7, 10,15. and 20 years.
RESULTS
None of the patients experienced spontaneous pain orpercussion pain during the follow-up period. From aclitiical standpoint, the treatment had restored theteeth to normal function.
According to the aforementioned classification'^'^using radiography, there were 21 cases of underfilling(31.8%), 37 cases of fiush filling (56.0%), and eightcases of overfilling (overextension) (12.1%) in thesample. This distribution was almost identical to sam-ples in previous endodontic clinical studies conducted
Quintessence International 469
íiurakami et al
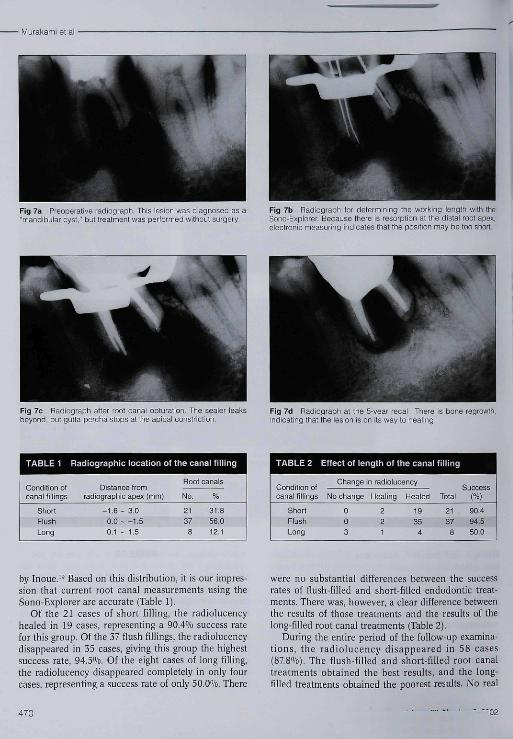
Fig 7a Preoperative radiograph. This lésion was diagnosed as a"mandibular cyst," but treatment was performed without surgery
Fig 7b Radiograph lor determining the wofi<ing length with theSono-Explorer, Because there is résorption at the distal root ape:*,electronic measuring indicates that the position may be too short.
Fig 7c Raaiograph atter root canal obturation. The sealer ieaksbeyond, but gutta-percha slops at the apicai oonstnction
Fig 7d Radiograph at the 5-year recall. There is bone regrowth,indicating that the lesion is on its way to healing
TABLE 1 Radiographie location of the canal filling
Condition otcanal fillings
ShortFlushLong
Distance I romradiographie apex (mm]
-1,6 - 3,00 , 0 - -1,50.1 ~ 1,5
Root canals
No, %
31.856,012,1
TABLE 2
Condition otcanal fillings
ShortFlushLong
Effect of length of the canal fiMinc
Change
No change
003
n radioiucency
Healing
221
Healed
19354
Total
21378
Success(%)
90.494,550,0
by Inoue,'^ Based on this distribution, it is our impres-sion that current root canal measurements using theSono-Explorer are accurate (Table 1).
Of the 21 cases of short filling, the radiolucencyhealed in 19 cases, representing a 90,4% success ratefor this group. Of the 37 flush fillings, the radiolucencydisappeared in 35 cases, giving this group the highestsuccess rate, 94,5%, Of the eight cases of long filling,the radiolucency disappeared completely in only fourcases, represenfing a success rate of only 50,0%, There
were no substanfial differences between the successrates of fiush-fiUed and short-filled endodontic treat-ments. There was, however, a clear difference betweenthe results of those treatments and the results of thelong-filled root canal treatments (Table 2),
During the entire period of the follow-up examina-tions, the radiolucency disappeared in 58 cases(87,8%), The flush-filled and short-filled root canaltreatments obtained the best results, and the long-filled treatments obtained the poorest results. No real
470

• Muraiíami et al
TABLE 3 Radiographie condition ot the canal fillings and finalresults versus rate of disappearance of radiolucency
Change inradiolucency
No change
Healing
Healed
Total
Condition ofcanal filiing
ShortFlushLongShortFlushLongShortFlushLong
Silver point
No, %
0
0 581
1
0 5.80
5
10 88.20
17
Gutta-percha
No. %
0
0 4,02
1
2 8.01
14
25 87,74
49
No
0
0
3
2
2
1
19
35
4
66
Totai
%
4.5
7.5
87 8
100 0
differences could be observed between tbe resultsobtained witb silver point (group 1) and gutta-percba(group 2) üllings (Table 3). Despite tbe long 20-yearperiod of some teetb in tbe follow-up examination,there was no incidence of relapse, and a 95.3''/o suc-cess rate was recorded overall. Tbis includes theoccurrence of cases with radiolucency still in theprocess of healing. When two cases of unintentionaloverfilling (overextension) were excluded, the successrate reacbed 98.4%.
DISCUSSION
In 1972, Inoue^" first described the concept of tbeSono-Expiorer, a sound-activated root canal-measur-ing device. Since its debut in 1972, tbe Sono-Explorerhas evolved from tbe original to the Mark II, Mark III,and Mark IV models, undergoing many developmentalimprovements. In the 29 years since the product wasfirst introduced, many researchers and cliniciansworldwide''-^* have used tbe Sono-Explorer, andmany clinical studies have demonstrated its acctu'acyand reliability.
In addition to tbe Sono-Explorer, tbe Endex"-'^and the Root-ZX*'̂ -'-' are new methods that use twodifferent frequencies, but tbere are few long-term clini-cal studies to demonstrate tbeir accuracy.
Many reports bave been made on the accuracy ofthe Sono-Explorer (Table 4), In 1977, Inoue'^ measuredroot canal lengtb in vivo electronically, and tben veri-fied tbe measurements by direct observation after tbetootb was extracted. Of tbose cases wbere tbe apicalforamen and tbe tip of the measuring device coincided,a comparison was made of the preoperative appearanceof the radio^pbic apex, and a discrepancy was noted.
In the present retrospective study, tbe radiolucentlesion disappeared in 19 of tbe 21 teeth with under-filled root canals, 35 of 37 teeth with flush-filled rootcanals, and only 4 of 8 teeth with overfilled rootcanals (see Table 2). Wben tbese results are comparedwitb tbose obtained by Bender et al,'^ Heling," andSeltzer,'' tbe present success rates for short- and flusb-filled canals are higher, while the results for long-filledcanals are less successful (Table 5).
This high success rate may be possibly due to theinclusion of numerous root canals tbat were filled totbe biologic apical foramen or apical constriction andtbat were actually tbought to be underfilled accordingto tbe radiographie images (see Figs 6 and 7). It isimportant to note tbat tbe designation of underfillingor overfilling was based on tbe appearance of tbe radi-ograpbic image and tbus was not necessarily an accu-rate representation of wbether tbe obturating materialwas actually long of or short of the apical foramen orapical constriction. To make an accurate decision ofwhether it is a long or shortfilling. it is suggested tbattbe lengtb of tbe root canal be measured electronically.
In tbe present study, there were no major differ-ences in tbe success rates of the flush-filled and theshort-filled root canals. This may be because all under-fillings were defined by the apical foramen or apicaiconstriction. Tbe overfilled root canals experiencedpoorer bealing (Table 5 and Figs 8a to 8c).
Tbe final results of the root canal filling length, asjudged by the radiographie images were as follows:Three of 66 lesions (4.5%) were unchanged, primarilyall in tbe overfilled group. Five of 66 lesions (7,5%)were smaller or sbowing signs of bealing. Tbeseincluded two underfilled, two flusb-filled, and oneoverfilled tootb. Tbe remaining 58 of 66 apical radio-lucencies (95,3%) were healed, and they included
Quintessence International 471
• Murakami et al
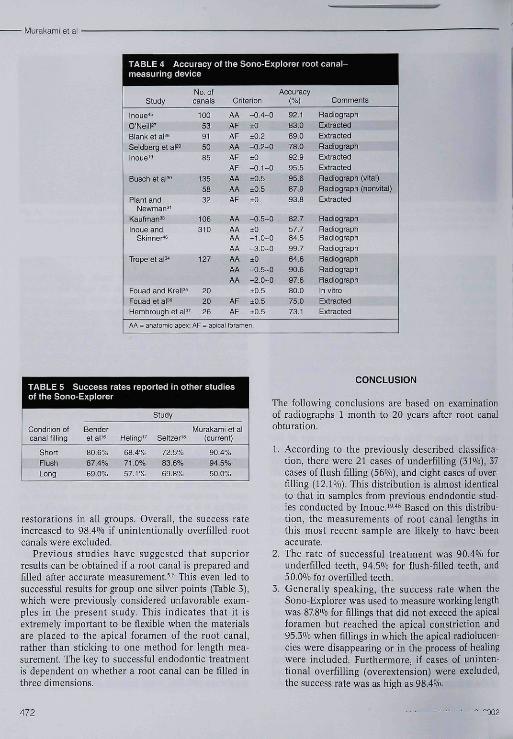
TABLE 4 Accuracy of the Sono-Explorer root canal-measuring device
Study
Incue's
O'Neill^'Blank et al=*Seidberg et aPInoue"
Busch et aP"
Plant andNewman '̂'
Kautman^^Inoue and
Skinner"
Trope et aP
Fouad and KrelP^Fouad et al^'Hembrough et al=
A A ̂ anatomic apex
No, ofcanals
100
53
91
50
35
135
5S
32
106
310
127
20
20
26
Criterion
AA
AF
AF
AA
AF
AF
AA
AA
AF
AA
AAAA
AA
AA
AA
AA
AF
AF
AF = apical foram
-0.4-0±0
±0.2-0.2-0±0
-0,1-0±0,5±0.5±0
-0.5-0±0-1.0-0-3.0-0±0
-0.5-0-2.0-0+0.5±0.5±0.5
en.
Accuracy(%)
92.183.Q89.078.092.995.595,6B7.993.a
82.757.784.599.764.690.697.680.075.073,1
Comments
RadiographExtraotBdExtractedRadiographExtractedExtractedRadiograph (vital)Radiograph (nonvital)Extracted
RadiographRadiographRadicgraphRadiographRadicgraphRadiographRadiographIn vitroExtractedExtracted
TABLE 5 Success rates reported in other studiesot the Sono-Explorer
Condition otcanal filling
ShortFlushLcng
Benderet al'«
80.6%87.4%69.0%
Hei ing"
68.4%71.0%57.1%
Study
Seltzer'ä
72.5%83.6%69.8%
Vlurakami et al(current)
90.4%94.5%50.0%
restorations in all groups. Overall, the success rateincreased to 98.4% if unintentionally overfilled rootcanals were excluded.
Previous studies have suggested that superiorresults can be obtained if a root canal is prepared andfilled after accurate measurement.̂ -^ Tbis even led tosuccessful results for group one silver points (Table 3),which were previously considered unfavorable exam-ples in tbe present study. This indicates that it isextremely important to be fiexible wben the materialsare placed to tbe apical foramen of the root canal,rather than sticking to one method for length mea-surement. The key to successful endodontic treatmentis dependent on whether a root canal can be filled inthree dimensions.
CONCLUSION
The following conclusions are based on examinationof radiographs 1 montb to 20 years after root canalobturation.
1. According to the previously described classifica-tion, there were 21 cases of underfilling (31%), 37cases of fiush filling (56%), and eight cases of over-filling (12.P/0). This distribution is almost identicalto that in samples from previous endodontic stud-ies conducted by Inoue.'̂ '** Based on this distribu-tion, the measurements of root canal lengths inthis most recent sample are likely to have beenaccurate,
2. The rate of successful treatment was 90.4% forunderfilled teeth, 94.5̂ /0 for fiush-filled teeth, and50.0% for overfilled teeth.
3. Generally speaking, the success rate when theSono-Explorer was used to measure working lengthwas 87.8% for fillings that did not exceed the apicalforamen but reached the apical constriction and95.3% when fillings in which the apical radiolucen-cics were disappearing or in the process of healingwere included. Furthermore, if cases of uninten-tional overfilling (overextension) were excluded,the success rate was as high as 98.4%.
472

• Murakami et al
Fig 8a Radiograph 1 month after roof canaf obturafion. The dis-tai canaf is overiiiied with gutta-peroha. The mesiai canals arefiiied with siiver point as indicated by ftie Sono-Expforer
Fig 8b Radiograph at the B-month recaif. The repair process isadvancing.
Electronic (audiometric) measurement of root canallength appears to be more accurate than the meth-ods using radiographie measurement. Accuratemeasurement of root canal lengths, to preventextension of filling material beyond the apical fora-men, was considered a key to successful endodontictreatment in these patients.
ACKNOWLEDGMENTS
The autho:5 thank Dr W. H, Christie, Associate Professor. SectionHead of Endodontology, Department of Restorative Dentistry,faculty of Dentistry, University' of Manitoba, Winnipeg, Manitoba.Canada, and Dr Jonathan Suzufii. Vancouver, British Columbia,Canada, for assistance with the translation of tfie manuscript. Wewonld also like to thank Dr F, S. Weine. Professor Emeritus, Loyofa[Jiiiversity. Chicago, who has made many vafuahie suggestions toimprove the Sono-Expforer.
REFERENCES
1. Grossmati LI. Endodontic Practice, ed 8. Philadelphia: LeaÄFebiger, 1974:201,
2. Cohen S, Bums RC, Pathways of the Puip, ed 7. St Louis:Mosby, 1998:209-211.
3. Weine FS, Endodontic Therapy, ed 4, St Louis: Mosby,1989:288-298.
4. Paltner MJ, Weine FS. Healey H). Position of the apicalforamen in relation to endodontic therapy. J Can DentAssoc 1971:37:305-308.
5 Ricucci D. Apical limit of root canal instrumentation andobturation. 1. Literature review. Int Endod J 1998:31:384-393.
6. Ricucci D, Langeland K. Apical hmit of root canal instru-mentation and obturation. 2. A histological study. IntEndodJ 1998:31:394-409.
7. Schilder H. Filling root canal in three dimensions. DentClin North Am 1967:1:723-744.
Fig Be Radiograph at ttie 2-year recafi The radiofucenoy of themesial canals has tiealed completely, but a smafi radiolucenoypersists ¡n the distaf canal (arrow).
8. Kuttler Y. Microscopic investigation of root apexes. ] AmDent Assoc 1955:50:544-552.
9. Green DA. A storeomicroscopic study of 700 root apices ofmaxillary and mandibular posterior teeth. Oral Surg!960;13:728-733.
10. Green DA. A stereomicroscopic study of apices of 400 max-illary and mandibular anterior teeth. Oral Surg 1956:9:1224-1233.
11. Suzuki K. Experimental study on iontophoresis. J JpnStomatol Soc 1942:16:411-417
12. Sunada 1, New method for tneasuring working length ofroot canal, J Dent Res 1962:41:375-378
13. Cash PW. Electronic measurement of root canals. DentSurv 1972;48:19-20.
14. Ingle J!, Bakland LK. Endodontics, vol 1, ed 4. Philadel-phia: Lea & Febiger, 1994191.
15. Cailleteau fG, Mullaney TP. Prevalence of teaching apicalpatency and various instrumentation and obturatioti tech-niques in United States dental schools. [ Endod 1997;13:394-396,
QtJintessence fnter nations I473
íturakami et si
16. Bender !B, Seltzer S, Turenkopf S. To culture or not to cul-ture? Oral Surg Oral Med Oral Pathol 1964;18:527.
17. Heling B. Evaluation of the success of endodonticallytreated teeth. Oral Surg Oral Med Oral Pathoi 1970;30:533-536.
18. Seltzer S. En do do nto logy. New York: McGraw-Hill, 1971:323.
19. Inoue N. A clinico-anatomical study for the determiningroot canal length by use of a novelty low-frequency oscilla-tion device. Bull Tokyo Dent Coll 1977;18:71-89.
20. Inoue N. Instrument of probing tbe length of root canal ofthe tooth. US patent 3,660. 1972.
21. Färber )P, Nygaard-Ostby B, Berk HL, and Salzberg M.Defend root canal measuring accuracy of Sono-Explorer[letter]. J Am Dent Assoc 1975:91:732.
22. Kerkes K, Nygaard-Ostby B. Locating the apical foramenwith the electronic apparatus Forameter. Swed Dent J1974;66:899-902.
23. Kerkes K, Nygaard-Ostby B. Electric measurement of lengthoftbe root canal Swed Dent J 1976j68:851-856.
24. Becker GJ. Lankelma P, Wesselink PR, Thoden van VelzcnSK. Electronic determination of root canal length. | Endod1980:6:876-880.
25. Auld CM. Conventional VS electronic endodontic measure-ment the Sono-Explorer. J Hawaii Dent Assoc 1982;13:24-25.
26. Berman LH, Eleischman SB Evaluation of the accuracy ofNeosono-D Eelectronic apes locator. J Endod 1994;10:164-167
27. O'Neill LJ. A clinical evaluation of electronic root canalmeasurement. Oral Surg Oral Med Oral Pathol 1974;38:469-473.
28. Blanlc LW, Tenca JI, Pclieu BG Jr. Rehability of electronicmeasuring device in endodontic therapy. J Endod 1975;1:141-145.
29. Seidberg BH, Alibarndi BV. Fine H, Logue B. Clinical inves-tigation of measuring working length of root canal witb anelectronic device and with digital-tactile sense. J Am DentAssoc 1975;90:379-386.
30. Busch LR, Chiat LR. Goldstein LO, Held SA, RosenbergPA. Determination of accuracy of the Sono-Explorer forestablishing endodontic measurement control. J Endod1976;2;295-297-
31. Plant JJ, Newman RF. Clinical evaluation of the Sono-Explorer. J Endod 1976:2:215-216.
32. Kaufman AY, Hehng B, Sechaiek M. What apex does theSonO'Explorcr really read? Quintessence Int 1979:10(12):63-71.
33. Kaufman AY. The Sono-Explorer as auxiliary device inendodontics. Isr ) Dent Med 1976:25:27-31.
34. Trope M, Rabie G, Tronstad L. Accuracy of electronic apexlocator under controlled clinical conditions. Endod DentTraumatol 1985;1:142-145.
35. Fouad AF, Krell KV, An vitro comparison of five root canallength measuring instruments. J Endod 1989;15:573-577
36. Fouad AF, Iirell KV, Mckendry DJ, Koorbusch GF, OlsonRA. A clinical evaluation of five electronic root canal lengthmeasuring instruments. J Endod 1990;16:446-449.
37. Hembrough JH, Weine SF, Pisano JV, Eskos N. Accuracy cfan electronic apes locator: A clinical evaluation in maxil-lary molars. J Endod 1993:19:242-246.
38. Fouad AF, Rivera EM, Krell KV. Accuracy of the Endexwith variation in canal irrigants and foramen size. J Endod1993:19:63-67
39. Yamaoka M, Yamaahita Y, Saito T. Electrical Root CanalMeasuring Instrument Based on a New Principle [thesis].Tokyo: Nihon University School of Dentistry, 1989.
40. Frank AL, Torabinejad M. An in vivo evaluation of Endexelectronic apex locator J Endod 1993:19:177-179.
41. Mayeda DL, Simon JH, Aimer DF, Finley K. In vivo mea-surement accuracy in vital and necrotic canal with theEndex apex locator. J Endod I993;19:545-548.
42. Kobayashi C, Suda H. New electronic canal measuringdevice based on the ratio method. J Endod 1994:20:111-114.
43. Christie WH, Peikoff MD, Hav/rish CE. Clinical observationon a newly designed electronic apex locator. J Can DentAssoc 1993:59:765-772.
44. Kaufma AV, Katz A. Reliability of Root ZX apex locator testby an in vitro model [Research Seminars, abstract 69].) Endod 1993:19:201.
45. Inoue N. An audiometric method for determining the lengthof root canals. J Can Dent Assoc 1973;39:630-656.
46. Inoue N, Skinner DH. A simple and accurate way of mea-suring root canal length. ] Endod 1985;ll:421-427
474 "02





























