Embed Size (px)
Citation preview


Clinical Decision Making Process
Universal Patient Management Guide
Connie Blow, MS, PTKyle Gibson, PT, MA, OCS
University of Missouri-Columbia
© 2007
1
5
6
2
34

Examination
5
6
2
34
Components of Clinical Decision Making

Examination Documentation Template
• Begins with………
• Patient Demographics• Reason for Referral
– Current Pathoanatomical or Pathophysiological conditions
• Past Medical History• Systems Review• Tests and Measures
Patient Demographics

DemographicsPatient Name
Date of Birth
Chronological Age
Adjusted Chronological Age
Date of Exam
Referring Physician
Other??
Reason for Referral
• Client/Patient Preferred Outcome– Patient’s motivation expected outcome for seeking
services.– This information encourages the therapist to keep
patient centered examination, intervention and outcome measurement at the forefront of their minds.
• Current Pathoanatomical or Pathophysiological Condition– Gives a medical, anatomical or phathophysiological
context to the examination

Past Medical History• Health History Questionnaire
• Review of recordsPast health statusCurrent health statusPrevious therapeutic interventions and outcomes
Structured Patient/Client Interview– Red/yellow flags– Current Medications– Previous/Current Functional Level
Social History– Work Status– Cultural Preferences
Systems Review
• Identification of issues requiring referrals or consultations
• Status of:– Cardiopulmonary– Integumentary– Musculoskeletal– Neuromuscular– Cognitive/Arousal

Systems Review
Blood Pressure
Edema
Heart Rate
Respiratory Rate
Must memorize normal and exercise values for BP, HR, RR
Betty Gail Phenomenon
“I am fine………just a little dizzy”
“I don’t know…..it’s probably the weather….what are we doing first today?
“My sugar this morning? …..it was OK yesterday afternoon”
“Oh, that bump on my heel? It’s nothing…..I just have to be careful when I first stand up on it”
Quick Check
• What is the normal blood pressure, heart rate and respiration rate for an 8 month old infant?
• Blood Pressure 87-105/53-66 mm Hg
• Heart Rate 100-160 bpm
• Respiration Rate 30-60 breaths per minute

Quick Check
• What are four signs of increased ICP in an 8 month old infant?
• Irritability• Vomiting (projectile)• Sunset Eyes• Increased Tone (change in tone)• Difficult to arouse• Increase Strabismus • Changes in feeding• Seizures

Tests and Measures
• Reliability
• Validity
• Appropriate Population
• What are you wanting to measure and why?

Quick Check
• Where and the categories of tests and measures be found quickly?
• Guide to PT Practice
Categories of Tests and Measures
• Disability– Ability to fulfill life roles in school, work, recreation,
social
• Functional Status– Mobility, transfers, play skills, self care
• Impairments– Pain, ROM, strength, endurance, circulation
• Pathophysiological – Often same as medical diagnosis
• Disease, trauma, metabolic imbalance

Examination
5
6
Evaluation
34
Components of Clinical Decision Making

Examination
5
6
Evaluation
PT Diagnosis4
Quick Check
• PT Diagnosis is the same as the Practice Patterns found in the Guide to PT Practice.
• False
Diagnosis “Guide Language”
“Both the process and the end result of evaluating examination data, which the physical therapist organizes into clusters, syndromes or categories to help determine the prognosis (including plan of care) and the most appropriate intervention strategies.”
APTA Guide to Physical Therapy Practice
Enhanced Mizzou Language
• Statement that minimally links impairments to functional deficits. Include pathoanatomical or pathophysiological classification as it affects prognosis or plan of care. – Conclusion of the evaluative process– Helps determine the prognosis– Required to develop plan of care

•This sounds like a call for a template!

Documentation of PT Diagnosis
• “Patient……
• “with an inability to…….(Disability)
• “as a result of difficulty in performing…(Linking Disability to FL’s)
• “secondary to....... (Linking FL’s to Impairments)
• “in the presence of signs and symptoms consistent with specific pathologies

Example
• Patient is a 23 year old male with an inability to work as a carpenter due to difficulty reaching/working overhead secondary to right rotator cuff weakness with glenohumeral hypomobility. These impairments are consistent with a possible right shoulder rotator cuff impingement and tendonitis.

Model
• Patient is a 23 year old male with an inability to work as a carpenter due to difficulty reaching/working overhead secondary to right rotator cuff weakness with glenohumeral hypomobility. These impairments are consistent with a possible right shoulder rotator cuff impingement and tendonitis.
• “Patient……• “with an inability to…….
(Disability)• “as a result of difficulty in
performing…(Linking Disability to FL’s)
• “secondary to....... (Linking FL’s to Impairments)
• “in the presence of signs and symptoms consistent with specific pathologies IF it affects prognosis or plan of care.

Physical Therapy Diagnosis Key Concepts
Not the same as PT Practice Pattern More than an ICD Code Linking…NOT Listing
– Linkage between functional limitations and impairments always required
– Linking functional limitations to disability is required when disability is present
– Inclusion of suspected pathoanatomical or pathophysiological classification is included as it affects prognosis or plan.

Examination
5
6
Evaluation
PT DiagnosisPrognosis
Plan of Care
Prognosis
Determination of the ability to meet Client/Patient Preferred
Outcome
Total Time Needed to Reach Optimal Level of Functioning
Based on Guide to PT Practice and Available Evidence
Written as:
Who, Will Do What, Under What Conditions, How Well, and By When
Long Term Goals/Outcomes: generally address remediation of functional limitations & disabilityShort Term Goals:
generally address remediation of impairments that have been linked to FL
Patient Centered

Examination
ImplementationPOC
6
Evaluation
PT DiagnosisPrognosis
Plan of Care

Documentation of Interventions
• Described such that it reflects “skilled PT”– “Gait training”…..not sufficient– “Gait training utilizing manual and verbal cues
for proper weight shift and symmetry of stride length.”
Show link to outcome measuresEvidence basedSpecific enough to guide careDocument Patient/Family Consent and
Understanding

Examination
ImplementationPOC
OutcomesRe-examination
Evaluation
PT DiagnosisPrognosis
Plan of Care

Outcome Measures and Re-examination
Efficacy of Treatment
Goals and Objectives Reasonable?
Appropriate Interventions for Impairments?
Patient Motivation?
Goals Patient Centered?
Constraining Factors?
Discharge?
Revise Goals and Objectives?
Quick Check
• At what points in the Client Management Model do we base decisions on the best evidence?
• Every One!
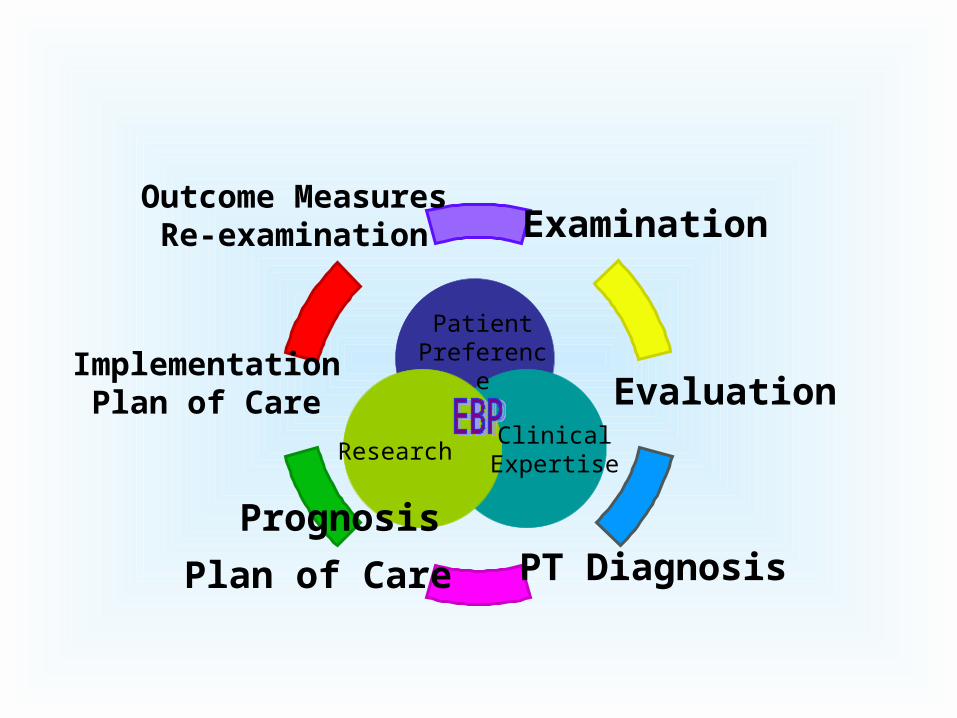
Examination
ImplementationPlan of Care
Outcome MeasuresRe-examination
Evaluation
PT DiagnosisPlan of Care
Prognosis
Patient Preference
ResearchClinical
Expertise

References
• O’Sullivan SB, Schmitz TJ, Physical Rehabilitation Assessment and Treatment 4th ed. Philadelphia, PA 2001
• Guide to Physical Therapist Practice. Rev 2nd ed. Alexandria, Va: American Physical Therapy Association;2001
• Using the Guide for Pediatric Practice, Chiarello, LA October 2000 CSM Presentation
• Quinn L, Gordon J, Functional Outcomes – Documentation for Rehabilitation. Saunders, Philadelphia PA 2003





























