Embed Size (px)
Citation preview

Clinical Conference 15 Dec 04
George P. Topulos, M.D.
Department of Anesthesia and Perioperative Medicine
Brigham & Women’s Hospital
Case Presentation - 1
60 yof o/w well - breast lumpectomy and axillary node mapping
Uneventful iv induction and oral ETTVentilator on, O2/N2O/Desflurane/fentanylNo NMB at request of surgeonPatient movement and BP, Desflurane
Several minutes go byReservoir bag is collapsedNo alarms (I think)
What would you do now?

Case Presentation - 2
Switch to bag (manual) ventilation
What would you do now?
Unable to ventilate or fill reservoir bag despite O2 FGF up to max.
Wake up patient and cancel surgery?
Call for help

Case Presentation - 3
Switch to manual resuscitator (ambu bag) for ventilation
What would you do now?
What if you could not find manual resuscitator?
Connect to O2 and capnograph!
Total iv anesthesia
Patient starts to move around

Clinical Problem SolvingRecognize
Best guess at Diagnosis
Temporize
Mechanism Context
Specific Therapy
Evaluate Success of Therapy
Re-evaluateDiagnosis
How bad is it?
Crisis Management - 1
Assign someone to take care of the patient and
nothing else!
They ignore the equipment problem.

Show Simulator Movie

Crisis Management - 2
Don’t panic – do not stare at the anesthesia machine.
Don’t ignore it either. “It would be unthinkably awful if this were true so it must not be real.”
While you are thinking have the nurse call your staff and say you want them NOW. This is no time for YOU to be on the phone.
Do not fixate on a single measurement or monitor look at the other vital signs.
Look at the patient and the surgical field.
Life is not a multiple-choice test, do all of this in 30 seconds.
Make sure you have not forgotten something you did.

Case Presentation - 4
Unable to find leak, clinical engineers, another attending who happened in.
Automatic "leak test" OK (and was before case).
Disconnect from patient and still a big circuit leak.
Switch anesthesia machines?
If so how when and with what help? if could not get another anesthesia machine use an ICU vent and iv anesthesia.
Causes of Circuit Leaks
Involve Patient
NG tube
Cuff leak
ETT out
Lung leak
Do Not involve Patient
Circuit disconnect
CO2 canister
Vaporizer leak
OR Biomedical Engineering Machine Post-Mortum
Jim Philip and OR Biomed TeamPage 3-1055 or call 3-1987
Vaporizer - worked without problem on another FabiusAnother Vaporizer in same slot created leak on this FabiusNo leak with Vaporizer offBig leak with Vaporizer onWhy?What happens when the Vaporizer is turned on?
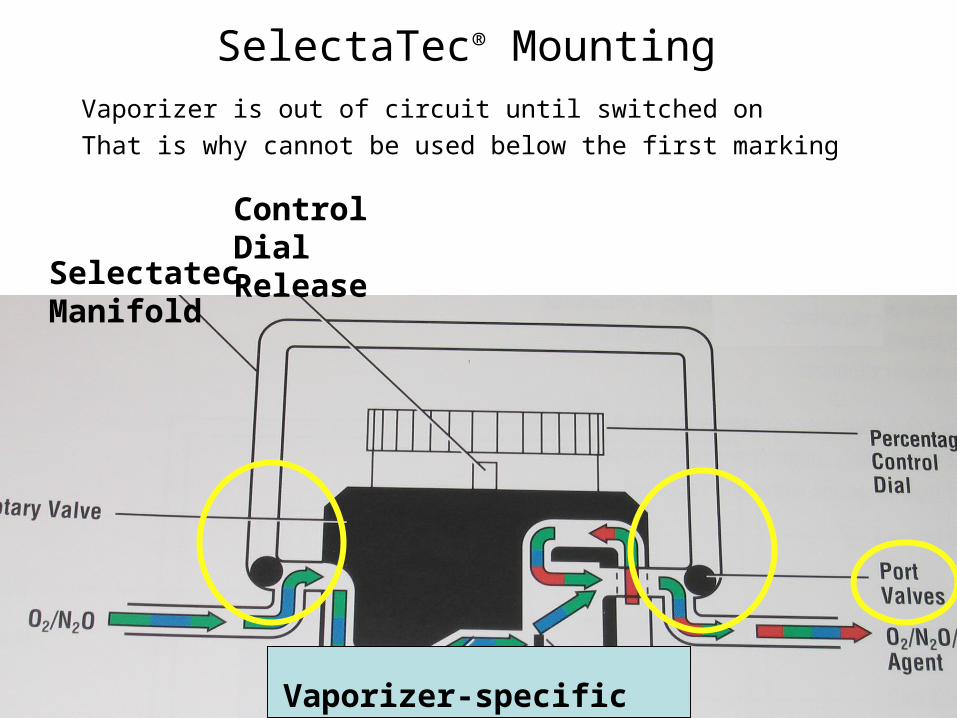
SelectaTec® Mounting
Vaporizer is out of circuit until switched on
That is why cannot be used below the first marking
SelectatecManifold
Control DialRelease
Vaporizer-specific innards
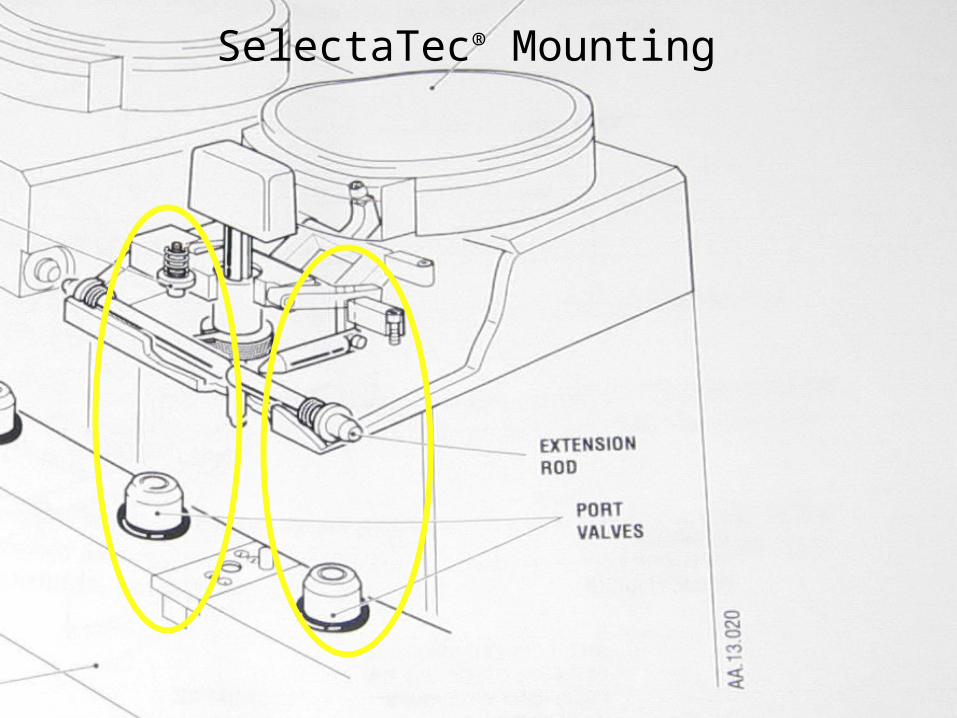
SelectaTec® Mounting

SelectaTec® Mounting
Vaporizer leak will be missed during pre-use checkUnless it is turned on
Loose vaporizer will leak at connectionOnly when it is switched on
Misalignment of Vaporizer will cause the leak observedAny anterior or posterior movement will do thisAlignment peg creates correct alignment
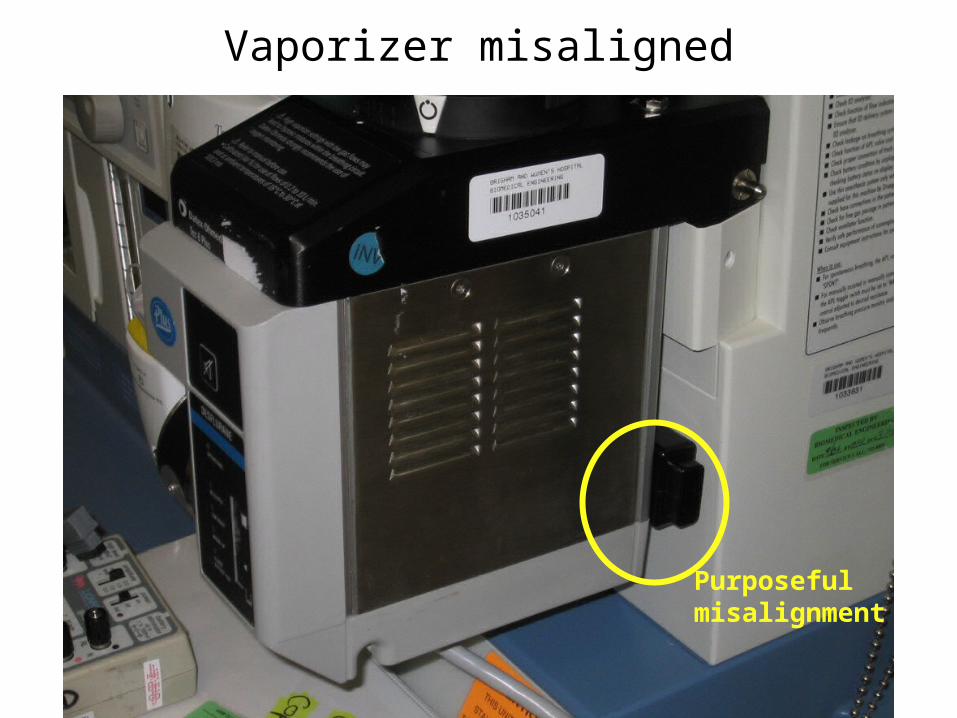
Vaporizer misaligned
Purposefulmisalignment
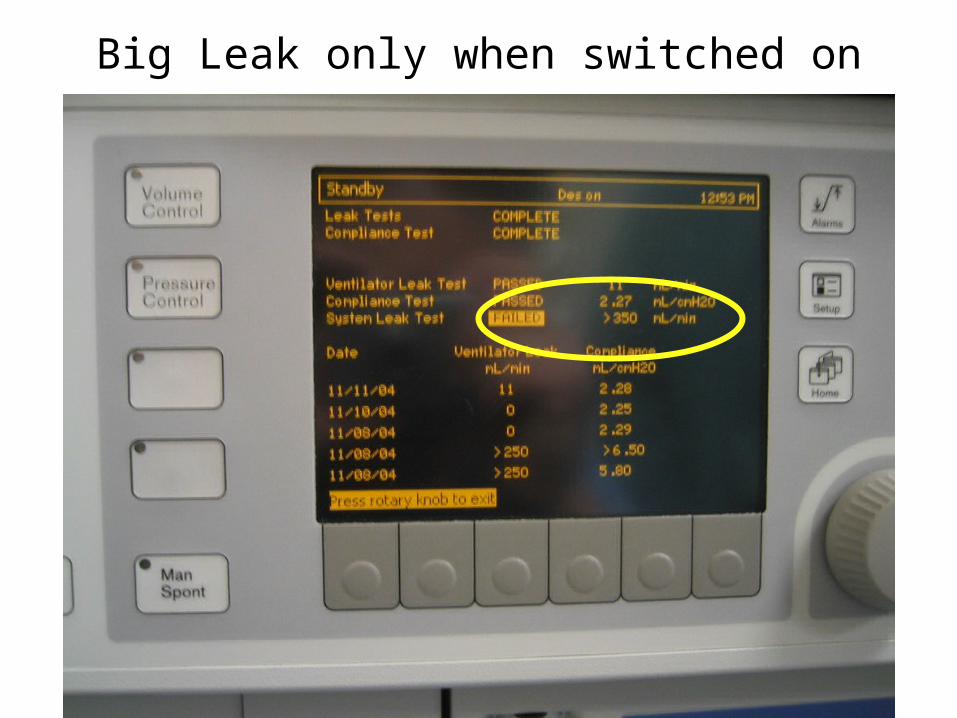
Big Leak only when switched on
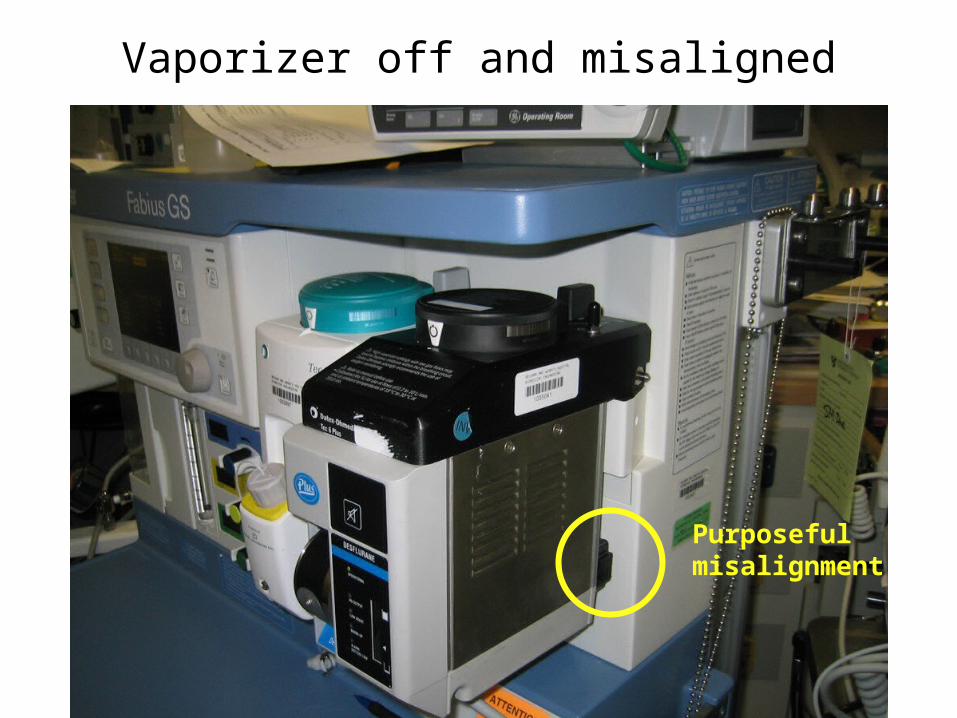
Vaporizer off and misaligned
Purposefulmisalignment
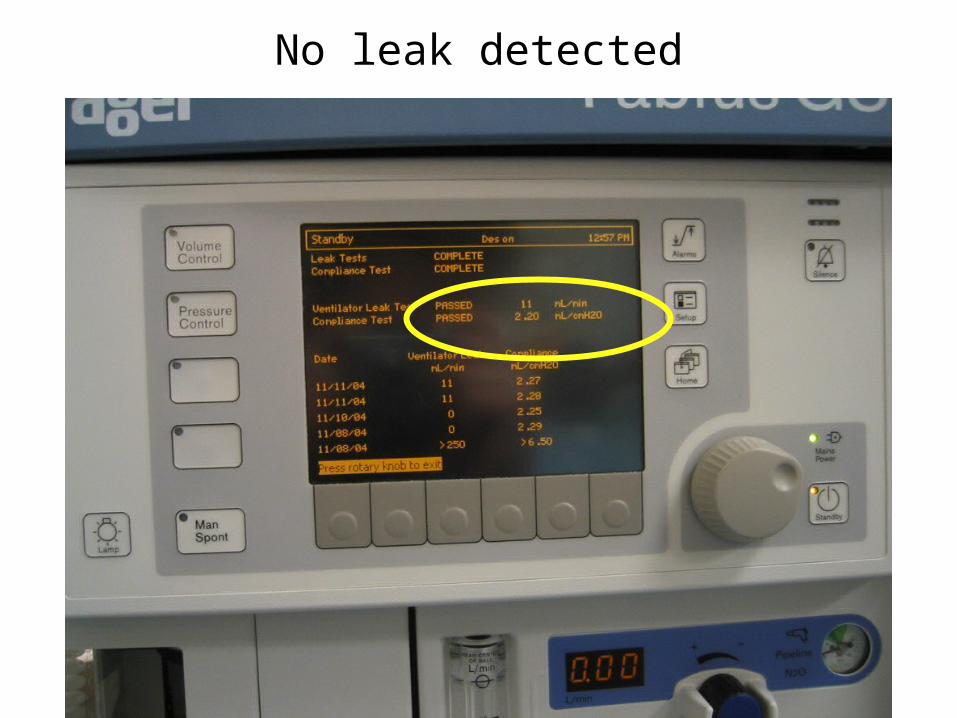
No leak detected

Followup
Manufacturer (Draeger) informed of “Failure of Pre-use Check”
Understood to be interaction of SelectaTec Vaporizers and back bar withDraeger “No Fresh Gas Hose” design
Resolution by Manufacturer?
Resolution at BWHInspect vaporizer mounting
Perform additional or primary leak testWith desired Vaporizer on
Black Slide
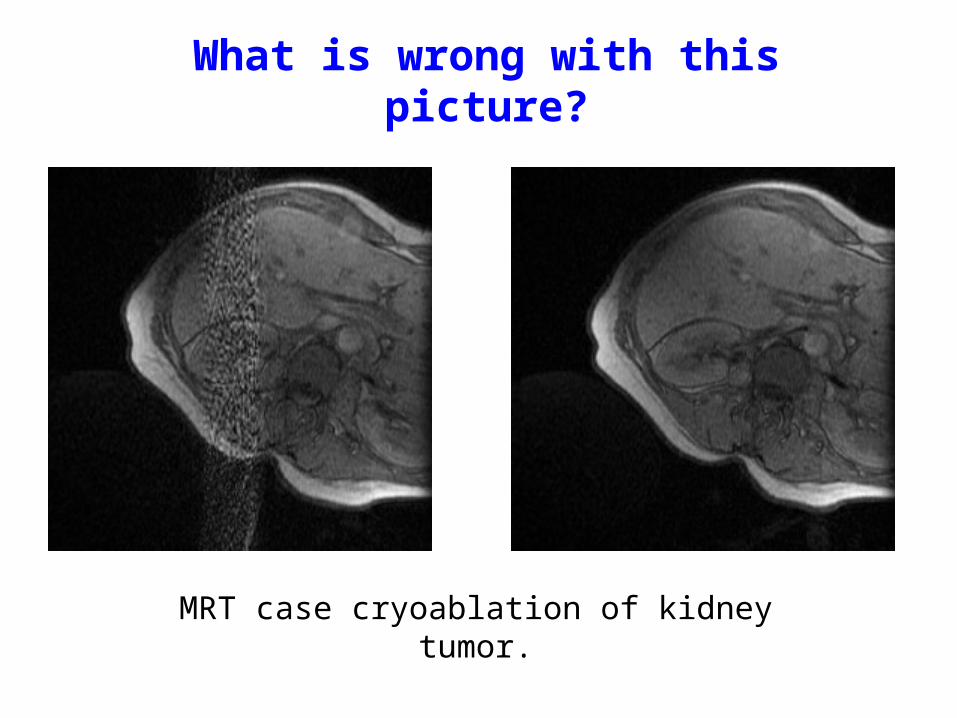
What is wrong with this picture?
MRT case cryoablation of kidney tumor.





























