Embed Size (px)
Citation preview
I-TECH Ethiopia ClASS Report March 2011 Page 1
Clinical Assessment for Systems Strengthening (ClASS)
ASSESSMENT REPORT For
International Training and Education Center for Health (I-TECH) Ethiopia 14-28 March 2011
Health Resources and Services Administration (HRSA)
HIV/AIDS Bureau—Global HIV/AIDS Program

I-TECH Ethiopia ClASS Report March 2011 Page 2
Table of Contents Abbreviations and Acronyms .................................................................................................................... 4
Executive Summary ................................................................................................................................... 5
International Partner ................................................................................................................................... 9
International Training and Education Center on Health (I-TECH) Ethiopia Office ............................ 10
Local Partner Treatment Facilities ........................................................................................................... 26
Debre-Birhan Referral Hospital ........................................................................................................... 27
Dessie Regional Referral Hospital ....................................................................................................... 33
Woldia Zonal Referral Hospital ........................................................................................................... 37
Dubti Hospital ...................................................................................................................................... 40
Asaita Health Center ............................................................................................................................ 44
Awash Health Center ........................................................................................................................... 48
St. Mary’s Axum Zonal Hospital ......................................................................................................... 57
Adwa District Hospital ........................................................................................................................ 61
Shire SuhulHospital ............................................................................................................................. 66
Mekelle Regional Referral Hospital .................................................................................................... 76
Mekelle University College of Health Sciences .................................................................................. 83
Ayder Hospital HIV Care & Treatment Centre ................................................................................... 83
Tigray Regional Health Bureau ........................................................................................................... 86
Tigray Regional Referral Laboratory ................................................................................................... 87
Appendices ............................................................................................................................................... 88
Appendix 1: ClASS Visit Participants ................................................................................................. 89
I-TECH Ethiopia ClASS Report March 2011 Page 3
Acknowledgments The Health Resources and Services Administration (HRSA) conducted the I-TECH Ethiopia assessment 14-28 March 2011 using the Clinical Assessment for System Strengthening (CLASS) model. The staffs of the US Embassy, Ethiopia, the Centers for Disease Control and Prevention, Global AIDS Program, Ethiopia and I-TECH Ethiopia provided transportation for the teams during the two week visit. I-TECH coordinated logistics and in-country flights. Both organizations shared in the planning and coordination of the assessment; their staff actively participated in all aspects of the visit. Many thanks for their contributions, support, feedback and membership on the review teams. Dr. Philippe Chiliade, the Track 1.0 lead and Dr. John Oguntomilade, Project Officer from the HRSA, HIV/AIDS Bureau, Global HIV/AIDS Program, led the team. Team members included Dr. Jeremy Penner and Dr. Angel Brana (clinical reviewers), Cheryl Nesbitt (administrative/program reviewer), and Juanita Farrow (financial reviewer) conducted the reviews and contributed to the contents of this report. The authors are solely responsible for any errors in representation and/or interpretation of the data sourced from interviews, observations and document review. We hope this report contributes to the strengthening of the PEPFAR program and builds on the successes that have been achieved by I-TECH Ethiopia.
I-TECH Ethiopia ClASS Report March 2011 Page 4
Abbreviations and Acronyms
ACM Adherence Case Manager AFB Acid-Fast Bacillus ALT Alanine Aminotransferase ART Antiretroviral Therapy ARV Antiretroviral AS Adherence Supporter CDC Centers for Disease Control and Prevention CEO Chief Executive Officer ClASS Clinical Assessment for Systems Strengthening CMO Chief Medical Officer COO Chief Operating Officer CQI Continuous Quality Improvement DQA Data Quality Assurance EQA External Quality Assurance FMOH Federal Ministry of Health FBS Fasting Blood Sugars FBTs Field Based Teams HANS HIV/AIDS Nurse Specialist HAART Highly-Active Antiretroviral Treatment HCT HIV Counseling and Testing HR Human Resources HRSA Health Resources Services Administration INH Isoniazid LTFU Lost-To-Follow-Up M&E Monitoring & Evaluation MDR-TB Multi-Drug Resistant Tuberculosis MDT Multi-Disciplinary Team MOU Memorandum of Understanding OPD Outpatient Department PEPFAR US President’s Emergency Plan for AIDS Relief PICT Provider-Initiated Counseling and Testing PDSA Plan-Do-Study-Act cycle PLWHA Persons Living with HIV/AIDS PMTCT Prevention of Mother-to-Child Transmission of HIV RHB Regional Health Bureau SI Strategic Information STI Sexually Transmitted Infections TA Technical Assistance TB Tuberculosis TOT Training of Trainers USG United States Government VCT Voluntary Counseling and Testing WHO World Health Organization
I-TECH Ethiopia ClASS Report March 2011 Page 5
Executive Summary The International Training and Education Center on Health (I-TECH), founded in 2002, is a collaboration between the University of Washington (located in Seattle, Washington) and the University of California, San Francisco. I-TECH was created to focus on global HIV/AIDS training needs by the Health Resources and Services Administration (HRSA) Global AIDS Program (GAP) in collaboration with the Centers for Disease Control and Prevention (CDC); the organization expanded in 2010 to cover a broader array of primary health care. I-TECH’s mission is to increase human and institutional capacity for care and treatment in countries hardest hit by the HIV and AIDS pandemic. I-TECH is the HRSA grantee of record for the PEPFAR program in Ethiopia. I-TECH has been working in Ethiopia since 2003 under a national mandate to provide technical assistance (TA) to build Ethiopian human resources and service delivery systems in HIV/AIDS care. As such, I-TECH has played a critical role both in the setting up and scale up of antiretroviral therapy (ART) clinics and care delivery systems and in health work force training. I-TECH staffs have significant experience and expertise in training, mentoring and implementation of service delivery systems. I-TECH’s activities are coordinated with the Federal Ministry of Health (FMOH), Federal HIV/AIDS Prevention and Control Office (FHAPCO), Regional Health Bureaus (RHBs), Regional HIV/AIDS Prevention and Control Office (RHAPCO), and participating government health facilities. On 27 October 2010, the Government of the Federal Democratic Republic of Ethiopia and Government of the United States committed to a “Five Year Partnership Framework in Support of the Ethiopia National Response to HIV/AIDS 2010-2014.” While Ethiopia’s 2009 HIV prevalence estimate of 2.3% is lower than many other Sub-Saharan African countries, there are still an estimated 1.1 million people living with HIV in the country. Ethiopia has a low-level generalized epidemic with wide urban and rural differences in prevalence (7.7% and 0.9% respectively) 1. The Government of Ethiopia (GOE) has doubled its budget for health over the last five years. Priorities in the abovementioned Partnership Frame work include promoting sustainability through a multi-sectorial approach, as well as targeting programming on the health needs of the most vulnerable populations. Currently, I-TECH is providing technical assistance (TA) to enhance prevention, care and ART service delivery through operational support, human resource development and quality improvement strategies to 42 facilities; the organization’s work spans eight program areas. I-TECH expects to add new facility programs (infection prevention and general and HIV pre-service training for medical doctors) under flat funding. More facilities, including private hospitals, will be added over the next few years. The three regions in which I-TECH provides services, Afar, Amhara and Tigray, account for 40% of the HIV burden in Ethiopia. Clinical Assessment for Systems Strengthening (ClASS) Methodology The Ethiopia CLASS visit took place from 14-28 March 2011. Meetings were held with CDC and I-TECH Ethiopia staff at their Addis Ababa offices. The purpose of the I-TECH Ethiopia
I-TECH Ethiopia ClASS Report March 2011 Page 6
ClASS visit was to:
Assess the administrative, clinical, and financial capacity of USG-supported HIV/AIDS programs;
Inform HRSA, CDC and other relevant partners of existing technical assistance needs; Identify available resources to address needs, and enable systems strengthening at the
Grantee and clinic site levels; and Determine the sustainability of Grantee efforts and inform HRSA and relevant partners.
The ClASS team divided into two groups to ensure more time to assess each site. The specific objectives of the assessment are as follows:
Assess the quality of comprehensive HIV services; Ensure that organizational systems, policies, and procedures are in place to accomplish
program goals and objectives at the Grantee and local facilities; and Determine the vision of the RHBs in supporting existing programs and identify needs to
better manage and sustain the funded services. The two teams visited hospitals, health centers and RHBs as indicated below. Team 1 Afar Regional Health Bureau Asaita Health Center Awash Health Center Debre-Birhan Referral Hospital Dessie Referral Hospital Dubti Hospital Woldia Hospital
Team 2 Adwa Hospital Axum Hospital Gondar University Hospital Mekelle Hospital Mekelle University Shire Suhul Hospital Tigray Regional Health Bureau Wukro Hospital
The team members consisted of the following HRSA staff and consultants:
• Laura Cheever, MD, HRSA, HAB, Deputy Associate Administrator, Team 2 • Philippe Chilliade, MD, HRSA, HAB, GAP Clinical Lead, Team 2 • John Oguntomilade, DDS, HRSA, HAB, GAP Project Officer, Team 1 • Angel Brana, MD, Clinical Reviewer, Team 1 • Jeremy Penner, MD, Clinical Reviewer, Team 2 • Cheryl Nesbitt, Administrative Reviewer, Team 2 • Juanita Farrow, Financial Reviewer, I-TECH Headquarters Review Team
The CDC Ethiopia staff participated with the teams throughout the visit as follows:
• Getahundt Sisay, Project Coordinator • Demmelash Birhanu, Cooperative Agreement Specialist

AIDSRelief-Tanzania ClASS Report-December 2010 Page 7
• Ribka Fantu, Project Coordinator for Tb/HIV, CDC-Ethiopia The following I-TECH managers from Addis Ababa traveled with the teams during the visit.
• Dr. Getachew Feleke, Clinical Director • Dr. Manuel Kassaye Sebhatu, Care and Treatment Director • Dr. Wubshet Mamo, Laboratory Director • Dr. Teklu Belay, Regional Programs Director • Dr. Eskinder Tesfaye, Senior Care and Treatment Advisor
Report Format The I-TECH ClASS report is divided into two sections. Part 1 provides an overview of the Addis Ababa Country Office management and programmatic functions while Part 2 offers specific reports on the hospitals, health centers, and the two regional health bureaus visited as part of the assessment. The reports do not contain the traditional clinical, administrative and financial management sections, but instead focus on management of the organization, program management (administrative and program oversight, monitoring and evaluation/strategic information), and clinical HIV services. No financial management reviews were conducted at the site, only at the I-TECH. Country Office. I-TECH Ethiopia strengths and areas for improvement are provided at the end of the overall report, while those for the hospitals and clinics are included with each site report. Conclusions The I-TECH Ethiopia program has made significant strides in helping to improve the quality of HIV care and treatment training for assigned hospitals and health centers in the Afar, Amhara, and Tigray regions. The sites and staff of the RHBs clearly value and desire the support from I-TECH to continue and expand as funding allows. However, many improvements are needed at the country, regional, and site levels, and particularly in the oversight and management of I-TECH clinical mentoring program. Increased documentation at all levels, the introduction of participant evaluation surveys, and the implementation of strategies to increase local ownership within each site will serve to strengthen quality improvement and ensure the sustainability of I-TECH’s clinical mentoring program. For general areas of improvement, the authors of this report recommend increasing the level of detail in mentoring plans and reports, and tracking findings and improvements within each site and region. There is also a need to evaluate the various components of the clinical mentoring program Clinical systems in Ethiopia should be reviewed. Several of the hospitals and clinics visited lack the space necessary to ensure patient confidentiality during interviews and physical examinations. In many locations at least two clinicians were found to share the same examination room and the same situation was also found in several instances for adherence case managers. Expanding available space to meet these needs is a key recommendation of this report. The irregular supply of laboratory reagents delays and/or prevents testing completion and clinician diagnosis. The breakdown of laboratory equipment and slow repair times are also contributing

AIDSRelief-Tanzania ClASS Report-December 2010 Page 8
factors. There are no standardized specimen transport protocols for viral load testing to ensure quality results. The division of the country between partners may be limiting how the MOH referral and support systems are able to assists hospitals and health centers and hospitals supporting health centers. Additional laboratory mentoring staffs, particularly those able to provide equipment maintenance, are needed to work directly with the sites. I-TECH has initiated strategic planning efforts for the management of the program’s pre-service and in-service components; however, the status and plans for the clinical mentoring program, particularly adherence case management and strategic information (SI), remain unclear. Visits to the RHBs revealed that direct capacity building and significant additional resources will be needed to improve management of both existing and future programs. I-TECH should develop a plan to transfer additional SI and monitoring and evaluation (M&E) staff to these areas and actively encourage their collaboration with local health management information systems (HMIS) staff. HRSA HAB GAP with the I-TECH Project Officer and I-TECH will determine upon review of the report where it will be appropriate to use internal versus external technical assistance, as well as in-country versus US-based resources.
AIDSRelief-Tanzania ClASS Report-December 2010 Page 9
International Partner
International Training & Education Center for Health (I-TECH)
I TECH Ethiopia CLASS Report July 2010 Page 10
INTERNATIONAL TRAINING AND EDUCATION CENTER ON HEALTH (I-TECH) ETHIOPIA OFFICE
March 14 and 24, 2011 Management I-TECH’s Addis Ababa office serves as the headquarters for the organization’s programs in Ethiopia. Its five primary management functions are: Organization Operations, Human Resources, Grants Management, Financial Management, and Program Monitoring. The Operations Director has been with the organization for four months. The Addis Ababa office also provides oversight for I-TECH’s three regional offices located in the Afar, Amhara and Tigray. At the time of the visit discussions were underway on how to decentralize maintenance and support functions for information management systems. Similarly, procurement of items under US$1,000 will also transfer to the regional offices. The country and regional offices are currently fully staffed as follows:
Region Staff # Afar 54
Amhara 92 Tigray 71
HQ-Addis Ababa 74 Each regional office is staffed by a Regional Manager; a Regional Planning, Monitoring and Evaluation Coordinator; and a Regional Administrative Manager. The Regional Manager manages and coordinates all I-TECH Ethiopia resources and activities in the region. The Regional Planning, Monitoring and Evaluation Coordinator is responsible for data entry and data management used to monitor program performance. The Regional Administrative Manager provides accounting oversight. Additional regional staff includes an administrative assistant, driver, and security staff. The regional offices also house the Field Based Teams (FBT) A and B. Pre-Service Training The ClASS team did not conduct a formal assessment of I-TECH’s support for pre-service training. This report includes areas for improvement based on discussions with faculty at Gondar University and Mekelle University regarding pre-service training. Gondar University began with a team training program, pre-dating the medical school, to train in the multidisciplinary team model and community based learning. The school built health center facilities to accommodate this training. In recent years, lack of funding caused the program to go into decline. In 2011, I-TECH assisted Gondar University with funding, resulting in significant improvement of the program. The Government of Ethiopia aims to address the country’s shortage of health care workers (HCWs) by increasing the number of students enrolled in health sciences programs. As a result, Gondar University has increased the average size of its medical school class from 60-70 to 180-200 students per year and may be told to enroll additional students. Due to this increase, there are
I TECH Ethiopia CLASS Report July 2010 Page 11
now 30 students per patient in the university’s pre-service program, limiting student opportunities for hands-on training. While staff are hopeful that the new Gondar University Hospital outpatient center will allow more learning opportunities, there are currently only 6 internists. I-TECH has intermittently supplied guest lecturers to the Gondar University medical student training program. Neither Mekelle University nor Gondar University has been able to implement a significant response to this situation yet, although they are considering potential solutions with the support of I-TECH. One solution currently under consideration is a clinical skills simulation lab which would allow students to practice procedures, examination techniques, and case scenarios without overwhelming the available patients in the hospitals. Another solution under consideration is a distributed learning model; under this model, zonal and district hospitals and health centers would serve as teaching sites for nurses and health officers. This model would require training physicians and other senior health care workers on adult education teaching skills and providing them with refresher courses on relevant focus areas, as well as incentives for assuming this added responsibility. Financial incentives and improved work environment may have the added benefit of increasing staff retention at peripheral health facilities as well. Video conferencing and web-based learning are potential cost effective tools to support the distributed learning model Currently I-TECH is supporting pre-service training in several ways, including: 1) Courses in Basic HIV Care and Treatment for pre-placement (internship-level) medical students and faculty members; 2) Trainings on Comprehensive HIV Care and Treatment, TB/HIV, prevention of mother-to-child transmission (PMTCT), and provider initiated counseling and testing (PICT) using the national curriculum for health officers and nurses, 3) Training on advanced HIV care and treatment for faculty members; 4) Training on advanced molecular laboratory techniques for faculty members; 5 ) Training clinical skills for hospital general practitioners and senior physicians; 6) Coordinating volunteer short-term faculty placements and guest lecturers within the universities; and 7) Improved faculty retention through joint appointments (which greatly increases the salary) and additional training and teaching opportunities. In-Service Training The ClASS team did not conduct a formal assessment of I-TECH Ethiopia’s support for in-service training. This report offers areas for improvement based on discussions with faculty at Gondar University and Mekelle University regarding in-service training. The University of Gondar is now responsible for regional in-service training on four program areas following national curricula: 1) Syndromic management of sexually transmitted infections; 2) Comprehensive HIV care and treatment; 3) Prevention of mother-to-child HIV transmission, and; 4) TB/HIV. The university coordinates and facilitates these trainings through funding and logistical support from I-TECH Similarly, I-TECH plans to transfer program responsibility and ownership for in-service HIV training to Mekelle University for the Tigray region. A formal impact assessment of I-TECH’s in-service training program has not yet been conducted. Mentoring Program
I TECH Ethiopia CLASS Report July 2010 Page 12
The I-TECH mentorship model uses Field Based Teams (FBT), each with specific site coverage. FBT-A is composed of mentors specific to clinicians/physicians, nurses, case management and infection prevention mentors (who are also nurses), and information management staff. Each FBT-A is responsible for four sites in the region, and they visit each site for three to five days each month. Each region has several FBT-As. FBT-B is composed of an internist, a pediatrician, a nurse mentor-of-mentors, and a laboratory mentor/supervisor. FBT-Bs spend two to three days per month at high volume sites in the region, and coordinate to ensure that there is some overlapping with the visits from the FBT-As. The overlap of the visits is critical to support/supervise the FBT-As. FBT-A and B are usually composed of full-time I-TECH staff. Teams operate under the direction of their respective Regional Program Manager, Clinical Team Lead and Program Advisor(s) based in I-TECH’s Addis Ababa office. Team “A” members consistently visit each site on a monthly basis regardless of the region. Some regional teams visit sites together as a rule, while others coordinate several visits per quarter, but are more flexible allowing members to address urgent issues of other sites in the region as needed. Mentors are expected to support site staff with information updates and feedback on the quality of care provision; mentors also work with support site staff to develop solutions to any barriers to effective patient care. The mentorship model at University of Gondar is slightly different. FBT-A has the same composition except that the physician team lead role is shared by four university employees as opposed to one I-TECH employee. Each of the four university doctors is responsible for one of the 4 FBT-A sites in the coverage area and spends one week per month at the site. The remainder of their time is spent at the university hospital. FBT-B also has university faculty. Two faculty pediatricians each spend 50% of their time supporting facilities in the FBT-A’s coverage area, spending one week at each site every month. One faculty internist spends 50% of his/her time supporting the same sites, visiting each site for a week every two months. The Nurse Mentor of Mentors and the Laboratory Advisor are full-time I-TECH employees. The same mentorship model is in effect at Debre Birhan Hospital, where experienced physicians on the Debre Birhan Hospital staff have taken on the Clinical Team Lead mentoring role for the Debre Birhan facility as well as at nearby hospitals. I-TECH is considering using this model with Mekelle University as well. The I-TECH mentoring handbook provides a detailed explanation of the overall mentoring process and expectations of mentors and the participating sites. All hospitals visited relayed the benefits of the multi-disciplinary team (MDT) meetings to the staff and management team. The handbook does not specify the frequency with and format in which information updates are to be provided to the staff. This area was most often identified as an area for improvement by hospital and clinic case management and information management staff. I-TECH should work with the Team Leads to develop minimum guidelines for information sharing and training templates. I-TECH should also provide sites with training overviews to ensure a clear understanding of criteria for training updates. This was an area of confusion for site staff. Several issues affecting the quality of care at facilities may be beyond I-TECH’s scope of work, such as shortage of space, the slow response time for laboratory equipment repairs, inconsistent supply of reagents and controls to sites, the low frequency of external quality assurance (EQA)
I TECH Ethiopia CLASS Report July 2010 Page 13
cycles (less than quarterly), and slow turn-around-time of EQA results. CDC Ethiopia may need to work with I-TECH if these are areas expected to be part of their scope of work Case Management, and Infection Prevention Mentors and Information Mentors Case Management and Infection Prevention mentors and Strategic Information/Data mentors walk a fine line between the mentorship role and that of a supervisor. At many of the sites Adherence Case Managers (ACMs), Data Clerks, and Information Technology Specialists identified the mentors as their supervisors or as the only persons from whom they receive feedback on work performance. While I-TECH clearly delineates the mentor role, more work needs to be done with site management to ensure involvement in non-clinical management components. Adherence counseling is provided to all newly enrolled clients and a more intensive effort is made to those that are identified as high risk for non-adherence based on pre-defined criteria. There appears to be inconsistency from one site to another on documentation requirements for patient charts for adherence counseling and the family matrix. I-TECH may want to revisit with mentors what level of documentation is appropriate for clinicians to know the status of adherence counseling discussions for patients. If documentation is kept separate, then opportunities for the sharing of this information will be critical between the clinicians and the ACMs. The Family Matrix was completed by the nurses until recently, but this extra duty was slowing the clinic process and this responsibility was shifted to the ACMs. Reviewers found that the Family Matrix is being completed at some sites for all HIV patients, but is not consistently used as a tool for locating partners and children who may require counseling and testing and enrollment into care. It appears that some mentors and ACMs have put their own interpretation on how “partner” should be defined, thus limiting prevention and education efforts. For example, sites in one region did not talk with or document information on a woman’s partner because he was not a husband while at another site in a different region, any partners were documented and interviewed. The latter definition of partner is the one intended from the MOH case management guidelines. A revised instruction sheet may be needed to clarify all appropriate partner options for use by ACMs and mentors. Mentoring reports and site reports are developed monthly by the HIV focal person and the assigned mentor. These separate reports are not compiled at the end of the year into a document that provides a clear picture of the issues, solutions shared and the end of year status of those issues. Such a document would give the site and mentors a clear picture of accomplishments and areas where support from the FBT ”B” may be needed. Four M&E mentor reports examined by reviewers showed a finding from their mentoring and site monitoring visits about a lack of completion of sections of the intake forms as part of the case management review. Despite a lack of improvement over several visits, the reports did not include any mention of corrective measures taken by the mentors with site staff toward improvement. This lack of detail raises concerns about internal I-TECH documentation of monitoring of program documentation and activities of mentors. SI/Data Clerk staff at sites are employees of I-TECH. While this initially served as a benefit, I-TECH should begin to shift their employment to the RHB responsible for the sites for better sustainability and ownership. One challenge shared by several sites was how to handle leave when
I TECH Ethiopia CLASS Report July 2010 Page 14
there are no additional staffs trained to perform the SI/Data Clerk duties. Mentors identified themselves as the back-up option, while site staff said they were told they could not take any leave because there was no one to take over their responsibilities. I-TECH Ethiopia should develop a written staffing back-up plan for each site on a yearly basis to identify primary and secondary replacement persons. Some sites need such a plan for ACMs as well as SI/Data Clerk staff. Human Resources I-TECH’s Addis Ababa office handles all hiring, though when reviewing candidates for the Field Based Teams the relevant regional office may participate in the interview process. However, lower- to mid-level positions (nurses, data clerks, information technicians, administrative/office staff), which are regionally based are interviewed and hired by regional office staff while paperwork is processed through headquarters. I-TECH began conducting performance reviews in 2010, however, merit increases (increases in wages achieved through superior performance on the job) were not issued due to ending of the HRSA contract period. Human resources (HR) staff is working with I-TECH managers to address common errors found during an internal process assessment after the implementation. Trainings are under development to assist managers in conducting performance reviews. I-TECH developed the case management model, which was subsequently adopted by the Federal Ministry of Health. I-TECH, therefore initially employed all of the Adherence Case Managers, Data Clerks, and Information Technicians. In 2010, following formal adoption as the national model and consistent with I-TECH’s sustainability ACM strategy, the ACMs were transferred from I-TECH employment to that of the local hospital with funding for salaries flowing through the RHBs. This process has not taken place for the data support staff due to the salaries of the FMOH positions and FMOH HMIS training requirements. The I-TECH staff bring significantly more experience than required for the FMOH positions, but the salaries would be significantly lower. I-TECH is waiting on the FMOH to make decisions on how and when the data staff positions are expected to transfer. Most FBT-B members are staff/consultants at either Gondar or Mekelle University. Others are full-time I-TECH staff seconded to the university and region as incentives to retain their expertise. Specifically, all eight Senior Clinical Advisors from FBT-B are seconded to four universities—University of Gondar, Mekelle University, Bahir Dar University, and Wollo University. MOUs were developed between I-TECH Ethiopia and the universities specific to the seconding of the consultant/faculty member. Two MOUs were reviewed for Dr. Abadi Leul and Dr. Senay Argawi, both full-time on the PEPFAR grant. There is relevant content in the MOU of Dr. Leul that should be added to that of Dr. Argawi. I-TECH should review both agreements and develop boilerplate formats and contents to be consistently used for future agreements. The MOU between I-TECH, Mekelle University, and Dr. Senay Argawi does not address expectations for documentation of Dr. Argawi’s time and effort while performing services at the university (95% university and 5% I-TECH). None of the MOU agreements discuss reporting requirements (level of detail and timeframes) for all activities performed for the university and I-TECH. The agreement for Dr. Leul does have a requirement for submission of a monthly workplan and performance report to the I-TECH regional office. Reviewers recognize the arrangements made to bring HIV expertise to the program and support the university and have no issue with ensuring these opportunities continue. The requirement for documentation of how and where time
I TECH Ethiopia CLASS Report July 2010 Page 15
is spent by persons paid with PEPFAR funds needs to be addressed by the consultants or the university and maintained by I-TECH Ethiopia. I-TECH should consider whether it is appropriate to reference participation in research activities in the MOU since PEPFAR cannot pay for any research-related activities. Grants Management The I-TECH Ethiopia office recently lost two staff in the Grants Management Department, the Sub-contract Manager and the Sub-contract Finance Coordinator about one month prior to the visit. These individuals served as liaisons between the Management, Program, Finance Departments in Ethiopia and their counterparts in Seattle. In the past, I-TECH Seattle has developed Requests for Proposals (RFPs) and scopes of work for sub-contractors. Plans are underway to decentralize some of these responsibilities to the Ethiopia office. I-TECH Ethiopia requires a current budget and workplan every year. Subcontractor reporting is submitted to the I-TECH Ethiopia office and then forwarded to I-TECH Seattle. The recently hired Operations Director in I-TECH’s Addis office is working to decentralize some of the maintenance support for SI and data management efforts. I-TECH Seattle should review all subcontract agreements to ensure that reporting requirements, particularly those on report submissions, are clear and consistent. Reporting requirements require that subcontractors submit reporting documents to the I-TECH Ethiopia Office for review prior to them being routed to I-TECH Seattle. I-TECH Ethiopia’s regional offices provide substantial support to RHBs in preparing the reporting documents. While this support is commendable, it raises concerns about the ability of the RHBs to meet reporting requirements in the future. It is also unclear how I-TECH is building capacity for the RHB to complete these efforts independently. Subcontract progress reports are submitted quarterly. Strengths: Management
• I-TECH transferred funding for the ACMs to the RHBs and some for Adherence Supporters (ASs) to local NGOs in support of increasing program sustainability.
Mentoring Program
• Mentoring handbook is a great “resource reference” for I-TECH staff, facility management and ART program staff.
• All levels of I-TECH Ethiopia participate in MDT and other site meetings when the mentoring teams share strengths and areas for improvements.
• Hospital HIV Committee meetings have helped create buy-in of the program from all levels.
• The comprehensive and intensive mentoring program is highly appreciated by all sites
I TECH Ethiopia CLASS Report July 2010 Page 16
• Mentors are knowledgeable and possess a strong understanding of HIV management and national HIV care and treatment guidelines. Mentors are also empathetic and respectful of mentees regardless of their experience or position.
• The length of time mentors spend at each site allows for assessment of gaps, technical assistance based on needs, and feedback to the hospital management. Systems are in place to document mentorship activities, track site-specific issues over time, and provide feedback to sites
• The majority of supported sites have high uptake of HIV testing at key service delivery points, strong linkage/referral to HIV care for those who test positive, integrated family planning at the HIV clinic, and overall good quality of care (based on documentation available).
• The University of Gondar and Debre Birhan Referral Hospital have demonstrated ownership of the FBT-A roles of the mentorship team for that region. The sharing of the physician lead role of FBT-A in Gondar and Debre Birhan allows staff to provide required services at the university hospital
• Case management and infection control mentors provide more than information and education while facility staff are overwhelmed with other responsibilities.
• Many of the supported sites use numerous strategies to verify the success of referrals for patients transferring to other sites (such as telephone calls, referral notes, catchment area meetings, etc).
• Modification of case management flow has taken place in many of the sites to ensure a broader social assessment at first visit.
Grants Management
• I-TECH Seattle provides strong support to the Addis Ababa office, including extended visits in the event of staffing shortages.
Areas for Improvement and Recommendations: Mentoring Program 1. Area for Improvement: There is no formal evaluation of mentees. Priority. Recommendation: I-TECH Ethiopia should implement assessments (at least twice per year) of mentees to allow mentors to identify gaps in knowledge to be addressed through on-going mentoring. 2. Area for Improvement: There is no formal evaluation of mentors with the exception of nurse mentors. Priority. Recommendation: The quality of mentorship provided to sites may vary between mentors. I-TECH Ethiopia should conduct assessments of mentors at least twice per year to identify gaps in knowledge, teaching skills, and mentorship techniques, and to provide targets for the mentors to improve and direction for efforts at building the capacity of mentors. 3. Area for Improvement: A. Site physicians should receive additional HIV training on advanced clinical issues (beyond the national curricula) to increase their competence and confidence, and these physicians should be incorporated into the supervision and monitoring visits that I-TECH performs for the HIV services at the site. B. HIV clinic staff are not reviewing each
I TECH Ethiopia CLASS Report July 2010 Page 17
other’s charts or reviewing the charts of patients who die; these functions are considered the responsibility of I-TECH. C. The majority of sites do not have formal case-based discussions or continuous medical education (CME) in the absence of the I-TECH team. Recommendations: 3A: Site physicians should receive additional HIV training on advanced clinical issues (beyond the national curricula) to increase their competence and confidence. This may require incentives and/or solutions for the workload barriers to hospital staff involvement. I-TECH should also strengthen the supervision and monitoring provided onsite. Recommendation 3B: Hospital physicians may need training on quality monitoring and the use of tools to guide the process. Chart audit tools could help guide HIV clinic staff through the process of regular peer chart reviews. Peer chart reviews serve to identify indicators for continuous quality improvement (CQI), case discussions, and CME, and foster peer support around adherence to standards of care. Recommendation 3C: To encourage facilities to develop an independent CME/case-based discussion program, I-TECH could train site staff on how to lead case-based teaching sessions and provide resources for weekly topics that the facility has identified and can lead even when the I-TECH team is not on site. 4. Area for Improvement: It is unclear if health facilities have the capacity to mentor new staff when they are posted to the HIV clinic, or if I-TECH is required to ensure new staff can provide quality care. Recommendation: For long-term sustainability each site should have the capacity to provide a certain level of mentorship to newly posted staff. This may require I-TECH Ethiopia to train HIV clinic staff on mentorship techniques and provide tools to guide the mentorship process and evaluate the progress of mentees. 5. Area for Improvement: FBTs currently visit the sites on a monthly basis. However, there are no clear criteria for assessing sites’ capacity or need for this intensity of support. Staff turnover may prevent a site from becoming fully independent, but there may be sites that are stable for periods of time. Recommendation: The I-TECH Ethiopia mentoring program should consider conducting twice annual needs assessments at each site. The program should then be tailored to meet the needs identified by the needs assessment. I-TECH Ethiopia should be open to modifying the time frames for mentoring visits depending on the results of the needs assessment. 6. Area for Improvement: There does not appear to be a written detailed annual plan for mentoring for each site based on the areas for improvement and gaps not addressed from the previous year. There does not appear to be an annual summary of accomplishments and outstanding issues from each mentor per site. Recommendation: I-TECH Ethiopia should consider developing a formalized mentoring plan for each site including the outstanding areas for improvement from the previous year. Advisors should become more involved if there appears to be no progress from mentor efforts. 7. Area for Improvement: Mentor written monthly reports reviewed (examples were from Axum mentors) do not provide sufficient information to facilitate follow-up on all areas for improvement. The MDT reports do not prioritize areas for improvement for the facility and do not provide sufficient detail for the site to fully understand and/or address any identified issues. Recommendation: I-TECH Ethiopia Team Mentors, Regional Coordinators and Program Managers should agree on the level of detail appropriate for the programs and managers to monitor the action plan accomplishments. The level of detail should also allow another team member to assume mentoring efforts when necessary.
I TECH Ethiopia CLASS Report July 2010 Page 18
8. Area for Improvement: I-TECH has not done an impact assessment of their mentorship model. Recommendation: I-TECH Ethiopia should conduct an impact assessment to document success and identify areas of weakness. 9. Area for Improvement: The success of the PMTCT program is limited by the low overall uptake of antenatal clinic visits and facility-based deliveries. Recommendation: To have an impact on vertical HIV transmission, I-TECH Ethiopia with the RHBs may need to introduce innovative approaches at health facilities to encourage attendance and mobilization within the community. Lessons learned may need to be drawn from other regions or countries and adapted to the local setting. 10. Area for Improvement: At Gondar University, the mentorship model has four university physicians sharing the physician lead role of FBT-A, yet there is no formal process or forum for them to share experiences/lessons/challenges from their respective sites. Recommendation: I-TECH Ethiopia with Gondar University should develop a process for sharing experiences between physicians, such as a monthly meeting and rotations at sites. 11. Area for Improvement: Referral and support systems between facilities were often weak. Facilities used catchment area meetings to share ideas of what has worked and not worked but in many cases it does not appear effective in identifying solutions to address issues of tracking referrals between sites or in using case management teams at other sites to support defaulter tracing of patients who reside near that facility. Few facilities provide technical/clinical support to lower-level satellite facilities. Recommendation: I-TECH Ethiopia with the RHBs should focus to improve referral and support systems between health facilities. Where partner mapping may be interfering with this process a strong collaborative effort at problem solving is required. 12. Area for Improvement: The long-term transition plan of the mentorship model to local ownership is not clear. Recommendation: I-TECH Ethiopia should work with the Federal Ministry of Health (FMOH), US Government, and other international partners to develop a common vision of how the mentorship and support of facilities can be sustained in the long term. The RHBs, Universities, and Regional Hospitals may each have key roles to play in supporting the theoretical FMOH model of each facility supporting the lower-level facilities around it. These roles need to be defined to allow for the assessment of transition readiness and provision of technical assistance based on the gaps identified. 13. Area for Improvement: Several sites are currently accessing HIV viral load testing at the regional referral laboratories where the test is being processed, however sites lack clear guidance on how to store and transport specimens in a manner that maintains specimen integrity. Priority. Recommendation: I-TECH is reportedly participating in a national-level working group tasked with developing guidelines on viral load lab networking. In the interim, I-TECH Ethiopia should develop a protocol to ensure that sites have access to valid and reliable results. 14. Area for Improvement: The FBT-B Laboratory Mentors supports a high number of sites and may not have the time necessary to provide direct mentorship of laboratory staff. Recommendation: I-TECH Ethiopia should consider dividing the Laboratory Mentors role into a

I TECH Ethiopia CLASS Report July 2010 Page 19
shared position with fewer sites per person to enable Lab Mentors to provide more direct mentorship to site laboratory staff. 15. Area for Improvement: None of the sites visited had the laboratory capacity to diagnose cryptococcal meningitis. Recommendation: If resources allow, I-TECH Ethiopia and FMOH should consider improving diagnosis of cryptococcal meningitis as a priority for the laboratory once the capacity for basic/routine investigations is established. Case Management/Infection Control Prevention
16. Area for Improvement: Case management staff at sites visited in the Tigray Region indicated refresher or update trainings have not been offered to them since their initial sessions. Recommendation: I-TECH Ethiopia should consider providing such regional sessions, if deemed appropriate. I-TECH and FMOH should consider how ACMs are expected to conduct adherence counseling if they are not provided similar information as nurses. Topics desired by ACMs included: how to talk with clients who have refused care; additional counseling options to help clients with adherence; and additional information on ART medications. 17. Area for Improvement: Family matrix forms are not being completed as required by case management guidelines. Forms are not dated nor is there space to clearly identify who completed the form, since either the nurse or the case manager can be responsible. Recommendation: I-TECH Ethiopia should consider providing refresher trainings for Case Management& Infection Prevention mentors who do not appear to be conducting chart reviews specific to the family matrix forms. I-TECH Ethiopia with FMOH should develop a checklist for this effort and orient CM/IP mentors.
18. Area for Improvement: Case management referral forms are stored in a binder, but are never included in the patient chart to offer the reasons for referral. Similarly, all case manager notes are not included in the patient chart. Recommendation: I-TECH Clinical Team Leads, Nurse Mentors, and Case Management and Infection Prevention mentors should develop a process for all forms to be stored in the patient medical chart. This will allow clinicians to have access to additional information, support staff to better complete required information, and ensure that support staff is held accountable for properly filling referral forms. 19. Area for Improvement: There is no formal mechanism for mentors to provide written feedback to Hospital Case Manager Supervisors for use during performance reviews. Recommendation: I-TECH, together with the RHB, should develop a feedback form and distribute it to hospital supervisors for use at least two times per year.
I TECH Ethiopia CLASS Report July 2010 Page 20
Strategic Information/Data Entry 20. Area for Improvement: I-TECH information managers and data clerks at all sites visited in Tigray region indicated that refresher or update trainings have not been offered to them since their initial sessions. Topics requested by sites include: software updates, basic equipment maintenance, and how to address challenges of using different software programs to collect HIV data in one facility. Recommendation: I-TECH should consider providing regional training and update sessions if deemed appropriate. I-TECH should also consider providing sessions at least twice per year for site staff to exchange lessons learned regarding data collection, entry, and analysis. 21. Area for Improvement: Four months of M&E mentor reports examined by reviewers identified a pattern of lack of completion of sections of the intake forms as a repeat issue at a site. Despite lack of improvement over time, the reports did not include any mention of corrective measures taken by the mentor with site staff. This lack of detail raises concerns about internal I-TECH monitoring of program documentation. Recommendation: I-TECH Ethiopia Clinical Leads may need additional oversight from the regional and/or Addis Ababa offices to ensure that reports are not “copied” from month to month and that corrective action is taken to prevent or remedy problems once identified. 22. Area for Improvement: M&E data backup is not consistently secured in a location separate from that of the database. Recommendation: I-TECH policies on data backup are clear, but should be amended to include a requirement for storing data backup in a separate location. I-TECH should also ensure that hospital and clinical management are reinforcing these policies. 23. Areas for improvement: Sites are not effectively using data for program improvement decision making as part of the MDT meetings, even though the data has been shared with the sites. Recommendation: I TECH Ethiopia could provide more technical support and mentorship on the utilization of data at site level for decision making to improve quality of services through identifying the problems and defining strategies to solve the identified problems Human Resources 24. Area for Improvement: The MOUs between I-TECH, Mekelle University, and Consultant Faculty do not address expectations for documentation and reporting requirements of time and effort while performing services at the university. Recommendation: I-TECH Ethiopia HR staff should work with the clinical mentoring program managers to develop a clear written policy, as well as examples of documentation demonstrating the desired level of detail to be provided immediately to all consultants. FINANCIAL REVIEW I-TECH Ethiopia has delivered technical assistance that enhances ART service delivery and human resources development since 2003. In addition to the Addis Office, there are regional offices operating in Afar, Amhara, and Tigray. Regional offices are minimally staffed for finance typically with an accountant and a cashier.
I TECH Ethiopia CLASS Report July 2010 Page 21
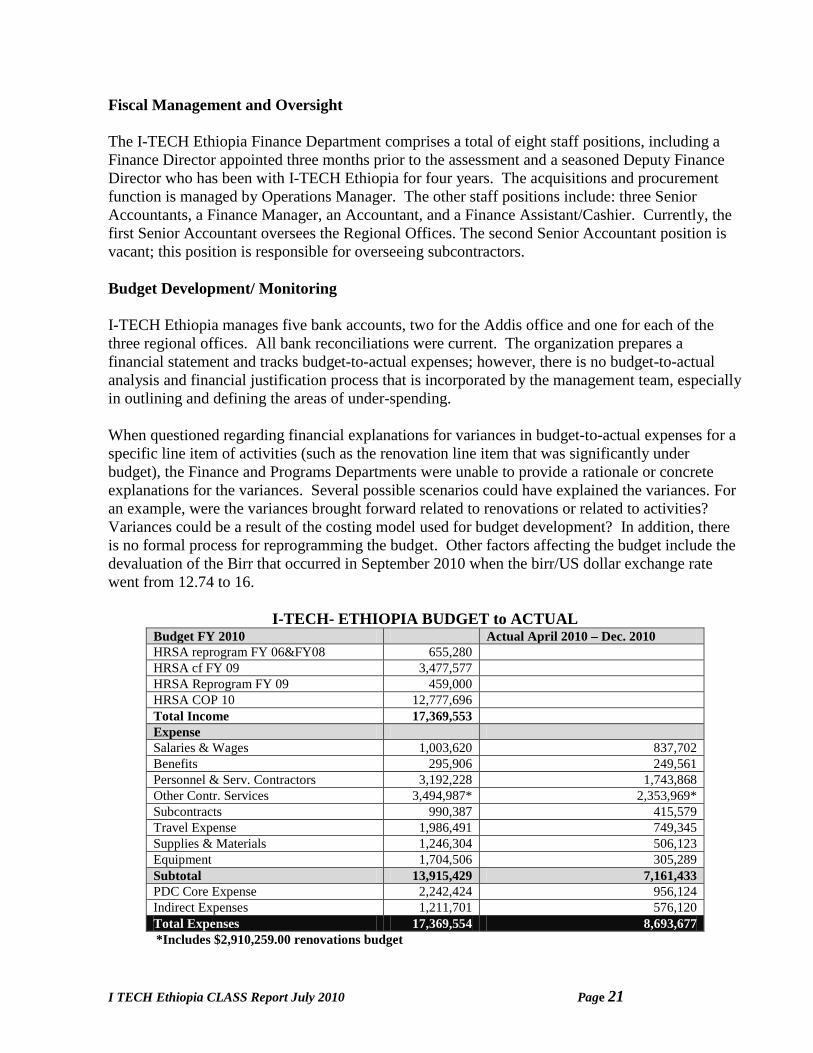
Fiscal Management and Oversight The I-TECH Ethiopia Finance Department comprises a total of eight staff positions, including a Finance Director appointed three months prior to the assessment and a seasoned Deputy Finance Director who has been with I-TECH Ethiopia for four years. The acquisitions and procurement function is managed by Operations Manager. The other staff positions include: three Senior Accountants, a Finance Manager, an Accountant, and a Finance Assistant/Cashier. Currently, the first Senior Accountant oversees the Regional Offices. The second Senior Accountant position is vacant; this position is responsible for overseeing subcontractors. Budget Development/ Monitoring I-TECH Ethiopia manages five bank accounts, two for the Addis office and one for each of the three regional offices. All bank reconciliations were current. The organization prepares a financial statement and tracks budget-to-actual expenses; however, there is no budget-to-actual analysis and financial justification process that is incorporated by the management team, especially in outlining and defining the areas of under-spending. When questioned regarding financial explanations for variances in budget-to-actual expenses for a specific line item of activities (such as the renovation line item that was significantly under budget), the Finance and Programs Departments were unable to provide a rationale or concrete explanations for the variances. Several possible scenarios could have explained the variances. For an example, were the variances brought forward related to renovations or related to activities? Variances could be a result of the costing model used for budget development? In addition, there is no formal process for reprogramming the budget. Other factors affecting the budget include the devaluation of the Birr that occurred in September 2010 when the birr/US dollar exchange rate went from 12.74 to 16.
I-TECH- ETHIOPIA BUDGET to ACTUAL Budget FY 2010 Actual April 2010 – Dec. 2010 HRSA reprogram FY 06&FY08 655,280 HRSA cf FY 09 3,477,577 HRSA Reprogram FY 09 459,000 HRSA COP 10 12,777,696 Total Income 17,369,553 Expense Salaries & Wages 1,003,620 837,702 Benefits 295,906 249,561 Personnel & Serv. Contractors 3,192,228 1,743,868 Other Contr. Services 3,494,987* 2,353,969* Subcontracts 990,387 415,579 Travel Expense 1,986,491 749,345 Supplies & Materials 1,246,304 506,123 Equipment 1,704,506 305,289 Subtotal 13,915,429 7,161,433 PDC Core Expense 2,242,424 956,124 Indirect Expenses 1,211,701 576,120 Total Expenses 17,369,554 8,693,677 *Includes $2,910,259.00 renovations budget

I TECH Ethiopia CLASS Report July 2010 Page 22
Accounting – Information System I-TECH Ethiopia uses the QuickBooks accounting system to track and report expenses. The Chart of Accounts used by the organization is a detailed listing of all the business transaction categories or sub-accounts in accordance to the organization’s General Ledger. This accounting structure specifically outlines and describes the classification and recording of all business transactions. The accounting team confirmed that based on the current chart of accounts it would be difficult to readily access information based on the activities of renovations and training. Therefore this information could not be obtained during the visit. Based on the interviews conducted the consultant found password security systems for the accounting system exposed. Password authorization and modification processes must be enhanced to secure and maintain system accountability at all times. To date, when an employee departs the organization, there is no formal process in place to immediately remove and delete the employee’s password information, leaving a breach in the system’s security and rendering the system exposed to vulnerable activity. An audit process to validate system security passwords must be implemented by an Information Security Officer or key security individual in accordance with I-TECH Ethiopia’s business structure and audit policy checkpoints. Policies and Procedures The organization uses the policies and procedures developed for the Regional Offices entitled “Regional Offices Financial Policy”. There was no reference by the staff to other policies and procedures provided by I-TECH Seattle, including I-TECH’s Global Operations Manual. The Global Operations Manual for Fiscal Operations is very comprehensive. Audits/Internal Reviews The most recent audit report for I-TECH Ethiopia dated 7 October 2010 was performed by A.A. Bromhead & Co. Chartered Accountants and UK Registered Auditor, for the year ending on 31 March 2010. The Balance Sheet as of 31 March 2010 provided by the Accountants revealed a current ratio of 1.53 (19,124,780 Birr in current assets/ 12,443,350 birr in current liabilities). This ratio indicates the ability of I-TECH Ethiopia to cover its debt obligations. The I-TECH Seattle office has recently introduced a policy of making quarterly onsite visits to the Addis Office. A comprehensive report documenting the findings of the quarterly visit was developed and accessible for this assessment. However, it was unclear how recommendations stemming from the quarterly onsite visits would be implemented by the Addis Office. While these quarterly visits by I-TECH Seattle to the Addis office will provide greater strategic insight and inform capacity planning, they should be viewed as a short-term measure to “ensure a sound organization” and not a long-term strategy due to the associated costs. The goal should be mentorship and capacity building in order to create the necessary ownership in-country. Payroll (Time & Effort) The organization uses timesheets to track and report time and effort. Timesheets are submitted by the employees to the Human Resources (HR) Department on a monthly basis. After HR approves the timesheets, HR forwards the timesheets to the Finance Department. However, the Finance
I TECH Ethiopia CLASS Report July 2010 Page 23
Department has not implemented a process to verify and validate employees’ hours worked and hours reported on the timesheets versus employees’ pay for a given month. Payroll is generated by the Finance Department based on the monthly pay rate of the employee. If there is a difference between the employee’s hours worked, HR will report the disparity to the Finance Department. The Finance Department will make the necessary pay adjustment in accordance to the areas for improvements of the employee’s actual hours worked, though this process is dependent on HR’s notification of the Finance Department. Acquisitions and Procurement The acquisition and procurement process is managed by the Operations Director. Requests from $1,000 to $11,000 require three written informal bids; requests over $11,000 require three formal bids. Formal bids must be advertised using social media and local papers. The Procurement Committee is composed of five individuals, with one representing the department that originated the request. There was no indication that members of the Procurement Committee have completed conflicts of interest declarations to disclose any potential conflicts of interest. Fiscal Strengths:
• I-TECH HQ is building capacity (at I-TECH Ethiopia) through quarterly on-site reviews on a short term basis.
• Bank reconciliations for five accounts are current with appropriate signoff. • There is good fiscal segregation of duties among the finance team. • The transactions sampled revealed good support documentation. • The policies and procedures in existence are comprehensive.
Financial Areas for Improvement and Recommendations Budget Monitoring 1. Area for Improvement: While the Addis Office tracks budget to actual variances, the variances are not formally explained. There is also no formal process for the reprogramming of funds. Priority. Recommendation: Develop a policy to address documentation requirements to include: the explanation of budget variances and the reprogramming of funds. Accounting: Chart of Accounts 2. Area for Improvement: The current chart of accounts does not allow for efficient tracking of costs by activity. Through meetings and discussions with the Finance and Program Departments it became clear that there is no efficient way to track costs by activities. Tracking of costs by activity would provide a better understanding of the source or cause of variances. The Program Office has budgets developed for activities; however the tracking of activity costs in the QuickBooks system does not provide sufficient detail that would allow the program office to evaluate actual expenditures to budget. Recommendation: Update the chart of accounts by developing “class codes” to allow for more efficient tracking and reporting of activities in the General Ledger. Track program costs through Class codes which add the program tracking and can
I TECH Ethiopia CLASS Report July 2010 Page 24
be further detailed out by sub-activities. This will allow I-TECH Ethiopia to track activities based on allowable costs. Payroll 3. Area for Improvement: Employee’ timesheet verification and validation appears to be weak. The Finance Department pays employees based on the monthly pay rate. Timesheets are used to document time and effort and are sent to the Human Resources Department. Finance Department staff report any differences in time and effort, such as hours actually worked and hours reported by HR. The Finance Department does not have a validation process in place to ensure that the hours the employee was paid for correspond to the hours worked. Recommendation: There is a need for I-TECH Ethiopia to ensure validation of the time and effort for employees and consultants reported to the PEPFAR program. A formal process should be developed that compares the hours allocated, worked and paid to employees against the source documents (timesheets). In addition, I-TECH Ethiopia should periodically consider conducting productivity studies that reflects an employee’s document activities. This would allow the organization to determine whether the grant allocations are consistent with work activities. Compliance 4. Area for Improvement: There is a lack of clarity on USG fiscal compliance standards/requirements among staff in the Addis Ababa office Finance Department. Recommendation: I-TECH-Seattle training opportunities should be increased or made available for members of the department’s fiscal team to ensure a better understanding of USG fiscal compliance requirements. Acquisition and Procurement 5. Area for Improvement: I-TECH Ethiopia Procurement Committee members have not implemented conflict of interest policies and therefore engage in activities without clear guidance on the disclosure of potential conflicts of interest, including financial interests. Recommendation: I-TECH-Seattle should develop a policy requiring the disclosure of potential conflicts or financial interests by I-TECH Ethiopia Procurement Committee members. Accounts Payable 6. Area for Improvement: The Accounts Payable (AP) process does not allow for efficient tracking of invoices. Invoices are first received by the Operations Department and later forwarded to the Finance Department. There is no tracking currently being used by the QuickBooks accounting system. Recommendation: Invoices from sub-contractors should be received by the I-TECH Ethiopia Finance Department directly and entered into the finance system. This will allow for better tracking of AP and for the development of AP aging reports while the invoices are pending approval by the Operations and Program Departments.
I TECH Ethiopia CLASS Report July 2010 Page 25
Accounting- Information System 7. Area for Improvement: The I-TECH Ethiopia password security system appears weak. There is the lack of comprehensive processes for strengthening the password security for the accounting system. When an employee leaves the organization, there is no systematic way to delete the password information for that employee. In addition, passwords are not periodically changed to strengthen security. Recommendation: I-TECH Ethiopia should develop a formal process to ensure that passwords for departing employees are deleted. Also develop processes to strengthen information system security such as a process for changing passwords periodically. Audits and internal reviews 8. Area for Improvement: A formal process has been implemented to ensure that recommendations from external audits are addressed and executed. However, there is no comprehensive approach to ensure that internal audit and quarterly review findings, specifically areas for improvement and recommendations, are addressed in the same manner. Recommendation: I-TECH Ethiopia should develop a formal comprehensive system, including identification of responsible parties and timelines, to ensure that all areas for improvements and recommendations from internal audits and other reviews are addressed and implemented. Monitoring and Oversight 9. Area for Improvement: a) I-TECH Ethiopia Regional offices lack efficient systems for tracking expenses. QuickBooks has been implemented in some of the Regional Offices but is not fully operational in all of the offices. The Addis Office has been working on this. b) The system for validating time and effort for subcontract staff and consultants is inadequate. Recommendation(s): a) The I-TECH Ethiopia Addis Office should ensure that QuickBooks is fully operational in all three regional offices in order to strengthen their capacity, financial monitoring and oversight. b) I-TECH Seattle and Ethiopia should ensure that adequate time and effort tracking is in place for subcontract staff and consultants. Validation systems are needed to ensure that individuals paid with PEPFAR funds are performing PEPFAR activities. Documentation and verification of activities should demonstrate activities performed are related to the PEPFAR program.
I TECH Ethiopia CLASS Report July 2010 Page 26
Local Partner Treatment Facilities
Local Partner Treatment Facility Reports
Debre-Birhan Referral Hospital Dubti Zonal Referral Hospital Dessie Regional Referral Hospital Asaita Health Center Woldia Zonal Referral Hospital Awash Health Center
Page27
DEBRE-BIRHAN REFERRAL HOSPITAL 15 March 2011
Organization and Program Management Debre Birhan Referral Hospital (DBRH) is located in the North Shewa Zone ofAmhara National Regional State. As a government institution, DBRH operates under the general authorization and policies and procedures of Ethiopia’s Federal Ministry of Health and is undergoing the new national hospital reform process. DBRH serves a population of 2.2 million people. Since 2010, DBRH served as a referral hospital for 20 health centers and two hospitals in the vicinity. It operates Monday through Friday from 8:30AM-12:30PM and 1:30-5:30PM. Emergency services are available24 hours per day, seven days a week, including public holidays. The hospital has 128 beds and offers medical, surgical, obstetrical, gynecological, pediatric, dental, and ophthalmological services. The hospital is managed by a Chief Executive Officer (CEO), who reports to a Governing Board. The Governing Board reports to the Regional Health Bureau. The Chief Clinical Officer (CCO), heads of the Finance, Human Resources, Monitoring and Evaluation, and Audit Department and other administrative leads report to the CEO. DBRH also has a hospital-wide Multi-Disciplinary Team (MDT) that meets twice a month. The first monthly meeting addresses hospital-wide issues with specific department heads in attendance, including the Head of the HIV clinic. The second monthly meeting discusses issues specific to the HIV Clinic; all clinic staff are invited to attend. The Hospital Internist heads the HIV Clinic which is staffed by two general practice physicians and four nurses (no health officers). DBRH is organized around four case teams: the Outpatient, In-Patient, Delivery and Emergency teams. Clinical staff consists of: an internist (who oversees HIV services), nine general practitioners, nine health officers (mostly nurses) 92 nurses, 13 laboratory staff, 15 pharmacy staff, 14 midwives, a dentist and an ophthalmologist. DBRH refers patients for tertiary care to hospitals in Addis Ababa, 120 kilometers away. The hospital also serves as a training site for health officers and nurses. It houses a “learning and resource center” and a resource library for clinical capacity building. These two facilities receive support from the International Training and Education Center for Health (I-TECH) in the form of computers, and case therapeutic simulation (TheraSim program). The hospital CMO and department heads meet with I-TECH’s Amhara Regional Office to determine priority areas for purchases and renovation. The DBRH requests are also evaluated by I-TECH Ethiopia office to determine the level of support. In addition, I-TECH has supported DBRH in its renovation of the patient waiting area and a section of the lab building. Microscopes have also been purchased for DBRH by I-TECH. It was observed that I-TECH initially intended to renovate the entire lab building, was however requested by the hospital management to stop renovation and refocus renovation on another part of the hospital. The lab renovation remains incomplete. HIV Services DBRH, with technical and material support from I-TECH, has been providing HIV care and
Page28
treatment services since 2006. The laboratory has received significant material support from I-TECH in the form of furniture, refrigerators and microscopes. HIV care and treatment services are organized under the Outpatient Team. Services are offered daily during the hospital’s regular hours. DBRH adheres to the following national country guidelines on HIV care and treatment as defined by the Federal Ministry of Health, Federal HIV/AIDS Prevention and Control Office:
1. Guidelines for Pediatric HIV/AIDS Care and Treatment in Ethiopia (July 2008). 2. Guidelines For Prevention of Mother-to-Child Transmission of HIV in Ethiopia (July
2007) 3. National Pain Management Guideline (December 2008) 4. Guidelines for Implementation of HIV/AIDS Case Management in Ethiopia (June 2009) 5. Management of Opportunistic Infections and Antiretroviral Treatment in Adolescents and
Adults in Ethiopia (March 2008) 6. National Guidelines for the Management of Sexually Transmitted Infections Using
Syndromic Approach 7. Guidelines for Implementation of the Antiretroviral Therapy Program in Ethiopia
(September 2008) 8. National Guidelines for HIV/AIDS and Nutrition (September 2008) 9. Accelerated Access to HIV/AIDS Prevention, Care and Treatment in Ethiopia, Road Map
2007-2008/10 10. Pocket Guide, Adult HIV/AIDS 2008-09
HIV prevention, care and treatment services are provided in-house. These include counseling and testing, highly active antiretroviral therapy (HAART), prevention and treatment of opportunistic infections including TB/HIV, STI treatment, prevention of mother-to-children transmission of HIV (PMTCT), and palliative care. The following case management services are also provided: counseling and care planning for at-risk-for-adherence clients and house visits for lost to follow-up patients. Laboratory services include CD4 count, hematology, blood chemistry rapid test, acid-fast bacilli (AFB) stains; dry blood samples for early infant diagnosis are referred out to the Ethiopian Health and Nutrition Research Institute (EHNRI) for DNA-PCR. DBRH’s HIV care and treatment team is composed of: three physicians (two general practitioners and one internist), one health officer, two nurses, two adherence case managers, five adherence supporters and four mentor mothers. The team evaluates between 70-90 patients daily for medication pick-up, of which a physician evaluates 35-40 for complaints and/or specific follow-up. These appointments provide an opportunity for patients to relate any problem they may be experiencing, and for staff to question patients on clinical symptoms of tuberculosis and to counsel on adherence strategies. Chart Review DBRH maintains individual patient paper charts with unique identifiers for each patient. Patient information is documented at every visit on an HIV Care/ART Follow-Up Standardized Form (as per design by the Federal Ministry of Health). The form is comprehensive and facilitates the documentation of the patient’s care plan. The chart also contains additional HIV/Care /ART intake standardized forms: patient registration form, past medical / treatment history, general

Page29
condition / physical exam, clinical review, social assessment, ART adherence counseling and, ART assessment and plan. Laboratory results and referral documentation are kept in the chart. At the time of this visit, DBRH was serving 1,397 adult patients currently receiving ART(as of 3/8/2011); and over the course of COP year 2010 provided HIV testing to 2,579 women at ANC or L&D, of whom 69 were HIV-infected (59 mothers and 50 newborns received prophylaxis). A total of nine charts were reviewed (those of six adults including, three pregnant women on PMTCT and three children). The review was done with the assistance of Dr. Melat Sebsibie, a “junior” general practitioner who deserves special recognition for her thorough understanding and comprehensive knowledge of managing HIV care and treatment. All of the patients were generally followed in accordance with the country National Guidelines except for elements discussed below under chart review. The national guidelines are readily available for reference by clinicians. The care provided was documented by checking boxes on the standard medical chart forms. The completion by clinicians of the intake forms and of the flow chart is interpreted as a measure of quality depicting the continuum of care and adherence to the national guidelines. Several charts did not contain progress notes. It should be noted that given the large caseload of HIV patients at DBRH, time constraints limit clinicians’ ability to document the decision-making process.
Two charts contained referral documentation and provided follow up information on whether a consultation had occurred. This usually depended on the patient notifying the clinician about the event, or personal communication by the referring clinician with the referring source. All patient charts reviewed had a basic CD4 count and follow-up counts as per guidelines. All patients were properly staged when evaluated by the clinicians, all met criteria for HAART, and those who met the criteria had been prescribed prophylaxis. The therapeutic regimen prescribed in all cases appeared commensurate with the blood laboratory values; the patient adherence box was checked on all of the reviewed charts. All of them had increased their CD4 counts from the initial level when started on treatment. All charts had documented a base line complete blood count. Creatinine levels were not done. It was explained that creatinine testing was considered optional due to lack of reagents. All the patients had documented baseline and follow-up visit screening for tuberculosis. Screening for Hepatitis B and venereal disease laboratory test (VDRL) was done on all pregnant women as per national guidelines. Lipids, fasting blood sugar, and VDRL for men and children are done only as per indication by the clinician. Patient Support Services HIV/AIDS Case Management functions at DBRH are supported by a Case Management and Infection Prevention Mentor from I-TECH, two Adherence Case Managers (ACMs), five Adherence Supporters (ASs), and four Mother Mentors (MMs). The ACMs receive referrals from voluntary counseling and testing (VCT), provider-initiated testing and counseling (PITC) clinics & OPD. ACMs assess those at a high risk of not adhering to ART, refer those most at-risk to assistance, connect patients to adherence supporters (ASs), who are also PLWHAs, conduct home
Page30
visits to those that live further away from DBRH, and coordinate with MMs to support PMTCT activities. Monitoring and Evaluation M&E functions are supported by the Strategic Information Mentor (IM) from I-TECH FBT-A, an Information Technician (IT) and a Data Clerk (DC). The three M&E staff are hired directly by I-TECH. The DC and IT are stationed at DBRH. While the IM comes in once a month, the DC updates the pre-ART and ART registers in paper form and updates socio-demographic information and also sends referrals to the ACM. The IT updates information from registers on an Excel spreadsheet. The IT also updates information from patient charts after return visits and produces monthly reports. The IM reviews the Excel spreadsheets and assists in compiling monthly reports to be sent to the RHB. Quality Improvement DBRH’s quality assurance program is organized around infection prevention. I-TECH has introduced a continuous quality improvement (CQI) initiative through the plan–do–study–act (PDSA) cycle approach. Data is collected regularly for compliance with performance standards as per clinical guidelines; when elements are not in compliance, a PDSA cycle is implemented. Strengths
• DBRH can be considered a “one-stop” service delivery model where individuals are treated with respect, dignity and competence.
• DBRH has a very competent, dedicated, committed and cohesive staff that provide good quality care to their HIV clients.
• All ART patients had good immunological response based on CD4 counts. • The various forms of support I-TECH provides to DBRH – training, mentoring, and
material support - are highly regarded by staff at the hospital. • Patients who test HIV positive are escorted to a case manager for additional post-test
counseling and strong efforts are displayed towards partner testing. • I-TECH ACM and M&E mentors stationed in the region provide easy access to the
mentees (ACM mentors spend as much as two weeks out of the month at DBRH). • I-TECH has established adherence case systems to ensure that all cases are captured by the
use of ASs and MMs. • I-TECH M&E mentors support coordination of DBRH data with the RHB. • I-TECH mentors support hospitals with information updates and attendance at MDT
meetings. • I-TECH infrastructural support has been significant in the clinic, labs and resources center
at DBRH. Areas for Improvement and Recommendations Medical Records
Page31
1. Area for Improvement: The quality of care provided is documented by checking boxes on the standard medical chart forms. Leaving a box empty could be interpreted either as a “negative” or a “not asked” area. This presents problems in assessing whether an element was actually examined or evaluated. The form has no place to indicate if any one element changes how the initial entries are updated systematically. Recommendation: I-TECH Ethiopia should continue to educate clinical staff on writing synoptic notes to document their decision-making process and using progress notes to complement the follow-up form. Tracking of referrals 2. Area for Improvement: Clinicians rely on the patient to notify them of whether a referral was kept and to inform them of the outcome. There is often little or no personal communication by the referring clinician with the referring/receiving source. Recommendation: Tracking referrals and consultations is always a challenging task. The hospital should consider dedicating one staff member to record all details on the referral, coordinate the request directly with the receiving service, follow-up with the patient and/or referral facility, and ensure that the information about the service is documented in the chart. This process is labor and time intensive and given current staffing levels at DBRH it is unclear whether this coordination/linking could be accomplished. Quality Assurance/Improvement 3. Area for Improvement: It was unclear, whether an ongoing cycle of change and re-measurement was in operation at the hospital HIV clinic at the time of the assessment. Recommendation: While I-TECH is mentoring DBRH on correct use of the PDSA cycle for quality improvement, it was not clear how systematic issues are identified to be subjected to PDSA cycles. I-TECH should work with the hospital and consider restructuring the chart review activity as a multidisciplinary CQI activity incorporating the data sources mentioned above to create PDSA’s within a framework of peer review and continuing education. Baseline Laboratories 4. Area for Improvement: Many of the recommended baseline laboratory tests are not performed systematically as per the National Guidelines (i.e. alanine aminotransferase (ALT), creatinine, lipid profile, hepatitis B serology, fasting blood sugar (FBS), syphilis serology). Pregnant women, however, systematically receive VDRL and hepatitis B screening. It was explained that lack of laboratory reagents precluded more systematic testing. Recommendation: I-TECH and hospital management should develop strategies to ensure consistent access to required supplies in compliance with national Ethiopia and WHO guidelines for laboratory services. 5. Area for Improvement: The laboratory does not currently provide diagnostic testing for cryptococcal meningitis, such as India ink staining of cerebrospinal fluid, or serum cryptococcal antigen testing. Recommendation: Cryptococcal meningitis is reportedly a significant contributor to morbidity and mortality among patients with HIV in Ethiopia. Although not yet a required test in the national guidelines, if resources allow, I-TECH Ethiopia should assist in increasing laboratory capacity to aid in this diagnosis.
Page32
Patient Support Services 6. Area for Improvement: There is no established internal hospital forum for ACMs to review cases with attending physicians in support of a multi-disciplinary approach to patient care and treatment. Recommendation: I-TECH Ethiopia should decide if such a forum would be a valuable addition to the mentoring program. DRBH staff should assess the benefits of including all HIV clinic staff in patient care review meetings and ensure proper documentation of discussions and outcomes.
7. Area for Improvement: Patient data updated in Excel spread sheets does not seem to have adequate data quality tests. Recommendation: Updated software may be needed to perform DQA and identify follow-up information to inform physicians of tests that have been missed or results that are in consistent. I-TECH Ethiopia should determine if such software is needed and include RHBs and ZHBs in deciding how to fund for long-term sustainability.
8. Area for Improvement: HIV Program site staffs identified areas where they may need additional training to increase their capacity to do their jobs. Recommendation: DRBH should determine what continuing medical education is available within the hospital to fill these information and education gaps. The RHBs and ZHBs may also be sources for sessions in the area, regardless of funding source.
Page33
DESSIE REGIONAL REFERRAL HOSPITAL 17 March 2011
Organization Management Dessie Regional Referral Hospital (DRRH) has been serving the Amhara region (South Wollo Zone) for the past 50 years. The hospital serves a catchment area of 7 million people in five zones, and has 99,921 HIV patients cumulatively enrolled on ART treatment. As a government institution, DRRH operates under the general authorization and policies and procedures of the Ethiopia Federal Ministry of Health (FMOH) and is implementing the new national hospital reform process. As part of this reform and as a mechanism to increase collections and retain staff, the hospital serves private patients who can pay. Eighty five percent of the income generated through this initiative is shared with the staff in the form of incentives. DRRH operates Monday through Friday, 8:30AM-12:30PM and 1:30-5:30PM. Emergency services are covered 24 hours per day, seven days a week including on public holidays. The hospital has 200 beds and offers medical, surgical, obstetrical and gynecological, pediatric, and emergency services. Its clinical staff is composed of 24 physicians, 12 specialists and 12 General Practitioners. DRRH refers patients for tertiary care in Addis Ababa, 400 km away. The hospital also serves as a training site for physicians, health officers, pharmacy professionals, laboratory staff, nurses and nurses-midwives. DRRH also houses a “learning and resource center” and a library for clinical capacity building. The Chief Medical Officer (CMO) and Chief Operating Officer (COO) report directly to the Chief Executive Officer (CEO). All other departmental heads report to the CMO and COO. Senior management meetings are held weekly, departmental meetings occur bi-monthly and all-staff meetings are held monthly. DRRH also has a Multi-Disciplinary Team, chaired by the ART focal person that meets every 2 weeks to discuss priority issues in the operations of the ART clinic. DRRH recently conducted a Patient Satisfaction Survey and scored 67% in overall patient satisfaction, a marked improvement from previous performance surveys. Management recognized dissatisfaction as stemming primarily from the waiting time to obtain lab results. This has been addressed and it is believed that patients are more satisfied with the services provided. Leadership is very committed to quality improvement at DRRH. The hospital provides clinical training for medical students, nurses, pharmacy and X-ray technicians from nearby schools and colleges. The facility has a high clinical staff retention mostly based on an arrangement where physicians are allowed to spend some hours working in private hospitals. Clinical staff also share in the profits from the private wing of the hospital. The CEO and heads of hospital departments meet with the regional I-TECH staff to determine priority areas for purchase and renovation. The DRRH requests are evaluated by I-TECH to determine the level of support. I-TECH has supported the renovation of DRRH’s patient waiting areas, Tuberculosis and Dermatology Clinics, and ART laboratory. The laboratory has been equipped with microscopes, cabinets and other lab furniture. I-TECH Ethiopia has also been involved in updating the regional laboratory.
Page34
HIV Services DRRH, with technical and material support from I-TECH, has been providing HIV care and treatment services since 2006. The laboratory has received significant material support from I-TECH Ethiopia in the form of furniture, refrigerators and microscopes. Services are offered daily as during the hospital’s regular working hours.
DRRH’s HIV care and treatment team is composed by two general practitioners, one health officer, five nurses, two ACMs, eight ASs, and four mother mentors (MM). The team evaluates an average of 245 patients daily for medication pick-up, f which the physician evaluates 25-30 for complaints and or specific follow-up. These appointments provide an opportunity for patients to relate any problem they may be experiencing, and for staff to question patients on clinical symptoms of tuberculosis and to counsel on adherence strategies. The HIV Clinic has implemented effective plan-do-study-act (PDSA) cycles in dealing with lost-to-follow-up patients and developing strategies coordinated by the pharmacy staff and outreach workers. In addition, the CEO assesses patient satisfaction through comprehensive satisfaction surveys. Data is regularly collected for compliance with performance standards as per national HIV clinical guidelines; when elements are not in compliance, a PDSA cycle is implemented. The most recent survey demonstrated patients are mostly satisfied with DRRH’s laboratory services. DRRH maintains an individual patient paper chart with a unique identifier for each patient. Patient information is documented at every visit in an HIV Care/ART Follow-Up standardized form (as per design by the Federal Ministry of Health). The form is comprehensive and facilitates documentation of the patient’s care plan. The chart also contains additional HIV/Care /ART intake standardized forms, including: patient registration, past medical/treatment history, general condition/physical exam, clinical review, social assessment, ART adherence counseling and, ART assessment and plan forms. Laboratory results and referral documentation are kept in the chart. Referral documentation is also kept in patient charts. It was explained that consultation confirmation usually depends on the patient notifying the clinician about the event or personal communication by the referring clinician with the referring source. Chart Review The HIV clinic has served a cumulative total of 14,300 individuals of which 9,921 were prescribed ART. At the time of the visit 5,396 adult patients and 336 children were on ART, in addition, 2,445 patients were on prevention of mother-to-child transmission of HIV (PMCTC). Fourteen charts were reviewed, of which11 were of adults, including three pregnant women, and three of children. National care and treatment guidelines are readily available for reference by physicians. The care provided was documented by checking boxes on the standard medical chart forms. All of the patients had a baseline CD4 count and follow-up counts as per guidelines. All patients were properly staged when evaluated by the clinicians and all met criteria for highly active antiretroviral therapy (HAART), and those who met the criteria had been prescribed prophylaxis. The therapeutic regimen prescribed in all cases appeared commensurate with the blood laboratory values and all charts had the patient adherence box checked. All of them had increased their CD4
Page35
counts from the initial level when started on treatment and had documented a baseline completed blood count. Creatinine levels were found in all cases, as well as screening for tuberculosis. Screening for hepatitis B was not documented on any case, while venereal disease research laboratory (VDRL) testing was done on two female patients. Lipids and fasting blood sugars (FBS) are done only as per indication by the clinician. ACMs perform all of the standard requirements and additionally provide health education talks twice daily in the clinic. This service has also been extended to other government facilities, schools, prisons and support groups. Data is sent to the hospital Health Management Information Systems (HMIS) Department which then forwards it to the RHB. Strengths
• ACMs are hired by the RHB, through a subcontract mechanism from I-TECH. This will eventually ensure sustainability of the program.
• I-TECH infrastructural support has been significant in the clinic and labs. • Quality of care is good. • DRRH staff regards highly the support I-TECH provides them, both in training and
mentoring and in material support. • DRRH has implemented effective PDSA cycles in which different departments and staff
are involved. • The use of comprehensive patient’s satisfaction surveys could be adopted at other hospitals
and health centers as a “best practice” for continued quality improvement (CQI).
Areas for Improvement and Recommendations Medical Records 1. Area for Improvement: The quality of care provided is documented by checking boxes on the standard medical chart forms. Leaving a box empty could be interpreted as a “negative” or as a “not asked” area. This presents problems in assessing whether an element was actually examined or evaluated. The form has no place to indicate if any one element changes how the initial entries are updated systematically. Recommendation: I-TECH should continue to educate DRRH clinical staff on how to write synoptic notes to document their decision-making process and how to use the progress notes to complement the follow-up form. Quality Assurance/Improvement 2. Area for Improvement: It was not clear that an ongoing cycle of change and re-measurement is in operation as part of the quality assurance improvement process. Recommendation: Patient satisfaction surveys, suggestions and complaints by patient and staff, patient flow analysis, and primary chart reviews could well serve as other primary sources for DRRH on how the clinical/administrative processes affect the overall HIV health care system and how work flow affects patient care. I-TECH could restructure the chart review activity as a
Page36
multidisciplinary CQI activity that incorporates the data sources mentioned above to create PDSA’s within a framework of peer review and continuing education. Baseline Laboratories 3. Area for Improvement: Many of the baseline laboratory tests recommended are not done systematically as per guidelines on the patient stage of the disease (i.e. ALT, creatinine, lipid profile, hepatitis B and C serology, FBS, syphilis serology). Exceptions to this are the pregnant women that systematically receive VDRL and hepatitis B screening. It was explained that lack or laboratory reagents precluded doing these screening systematically. Recommendation: I-TECH and hospital management should determine how to ensure consistent access to required supplies in compliance with the national Ethiopia and WHO guidelines for laboratory services. 4. Area for Improvement: The laboratory does not have diagnostic testing for cryptococcal meningitis, such as India ink staining of cerebrospinal fluid, or serum cryptococcal antigen testing. Recommendation: Cryptococcal meningitis is reportedly a significant contributor to morbidity and mortality among patients with HIV in Ethiopia. Although not yet a required test in the national guidelines, if resources allow, I-TECH Ethiopia should assist in increasing laboratory capacity to aid in this diagnosis. Support Services 5. Area for Improvement: There is no established forum for ACM to review cases with attending physicians in support of a multi-disciplinary approach. Recommendation: I-TECH should decide if should be a requirement for participation in the mentoring program. DRRH staff should determine the benefits of including all HIV clinic staff in patient care review meetings and be sure there is documentation of discussions and outcomes. 6. Area for Improvement: Patient data reviewed in Excel spreadsheets does not appear to have adequate data quality assessments (DQA). Recommendation: A software update may be needed to perform DQA and identify follow-up information to inform physicians of missing tests or inconsistent results. I-TECH Ethiopia with the FMOH should determine how or if this recommendation should be implemented.
Page37
WOLDIA ZONAL REFERRAL HOSPITAL 18 March 2011
Organization Management Woldia Zonal Referral Hospital (WZRH) was established in 1961; it serves 16 districts and a catchment area of 1.5 million people. WZRH has 2,400 patients cumulatively enrolled in HIV treatment. Hospital departments are referred to as Case Teams and are headed by a Manager. The hospital serves as a referral site for 15 health centers in the vicinity. Emergency services are covered 24 hours per day, seven days a week, including public holidays. The hospital offers medical, surgical, obstetrical and gynecological, ophthalmological and pediatrics services. Its clinical staff are composed of one Head Physician, one surgeon, one obstetrician-gynecologist, one ophthalmologist, four general practitioners and several nurses. The hospital also serves as a training site for nurses and nurse-midwives. HIV services are organized under the Outpatient Case Team. Services are offered daily as per the regular schedule of the hospital. HIV Services HIV services have been provided since 2006. The HIV clinic operates Monday through Friday, 8:30AM-12:30PM and 1:30-5:30PM. Antiretroviral therapy (ART) multi-disciplinary team (MDT) meetings are held monthly to discuss issues related to the ART departments. The I-TECH FMT-Bs also present at these meetings. The Chief Executive Officer (CEO) and some senior leadership attend and present at the catchment area meetings. WZRH also provides clinical training for nurses and midwives from four different colleges. The CEO and heads of hospital meet with the I-TECH FBT lead and I-TECH Regional Manager to determine priority areas for purchase and renovation. WZRH requests are also evaluated by I-TECH Country Office to determine the level of support. I-TECH has supported the renovation of two patient waiting areas at WZRH. The ART lab has been renovated. The lab has been equipped with microscopes, cabinets and other lab furniture. WZRH’s HIV clinical care and treatment team is led by the Medical Director and consists of: one physician and four nurses, two adherence case managers, six adherence supporters and four mother mentors. The team evaluates 60-70 patients daily for medication pick-up, complaints and or specific follow-up. These appointments provide an opportunity for patients to relate any problem they may be experiencing, and for staff to question patients on clinical symptoms of tuberculosis and to counsel on adherence strategies. Adherence Case Managers (ACMs) recently conducted a patient referral audit: the ACMs compiled a list of hospitals and health centers in the region and their phone numbers, and called to confirm that patients claiming to transfer to others locations have been received and started treatment. This audit served to ensure that patients who claim to have transferred are not lost-to-follow-up (LTFU). Adherence Supporters (ASs) are assigned to cover specific catchment areas. The number of patients assigned and reached by ASs’ every 5 months are demonstrated on a chart and displayed in the office to track AS progress and provide healthy motivation. ACMs and ASs also conduct fundraising and seek donor organizations to ensure that funding is sufficient to
Page38
continue to support patients in ART adherence. Current LTFU in WH is 1.7%.The WZRH adherence care program exhibits some best practices that may be adopted by other programs Quality Improvement WZRH’s quality assurance program is organized around infection prevention. I-TECH has introduced a continue quality improvement (CQI) initiative through the plan–do–study–act (PDSA) cycle approach. Data is collected regularly for compliance with performance standards as per clinical guidelines; when elements are not in compliance, a PDSA cycle is implemented. Medical Records WZRH maintains an individual patient paper chart with a unique identifier for each patient. Patient’s information is documented at every visit in an HIV Care/ART Follow-Up standardized form (as per design by the Federal Ministry of Health). The form is comprehensive and facilitates the documentation of the care plan of the patient. The chart also contains additional HIV/Care /ART intake standardized forms, including: patient registration, past medical/treatment history, general condition/physical exam, clinical review, social assessment, ART adherence counseling, and ART assessment and plan forms. Laboratory results and referral documentation is kept in the chart. At the time of this visit, WZRH is serving 2,878,878 patients for ART (as of 3/8/11) and had cumulatively enrolled 7,110 pre-ART patients. Fifteen charts were reviewed (those of nine adults, including three of pregnant women on PMCTC, and six children). The review was done with the assistance of WZRH’s ART Coordinator, Abduilhafiz Hassen. All of the patients were generally followed in accordance with the National Guidelines except for elements discussed below. The national guidelines are readily available for reference by clinicians. The care provided was documented by checking boxes on the standard medical chart forms. The completion by clinicians of the intake forms and of the flow chart is interpreted as a measure of quality depicting the continuum of care and the adherence to the national guidelines.
One chart had referral documentation (transfer-in). In relation to referrals and consultations, it was explained that the process was personally coordinated by the adherence case managers contacting the receiving organizations to assure patients had attended appointments. All of the patients had a basic CD4 count and follow up counts as per guidelines. All patients were properly staged when evaluated by the clinicians, all met criteria for highly active antiretroviral therapy (HAART), and those who met criteria where prescribed prophylaxis. The therapeutic regimens prescribed in all cases appeared commensurate with the blood laboratory values; every patient charts reviewed had the patient adherence box checked. All demonstrated an increase in CD4 counts following the initiation of treatment. All had documented a baseline complete blood count. Creatinine levels were not done. It was explained that this testing was considered optional due to lack of reagents. Every patient chart reviewed documented baseline and follow-up visit screening for tuberculosis. Lipids, fasting blood sugar, and venereal disease research laboratory (VDRL) tests for men and children are done only as per indication by the clinician. I-TECH infrastructural support has been significant in the ART Clinic, labs and the patient waiting areas. ACM activities have been able to demonstrate good patient referral audits.
Page39
Strengths:
• All patients were properly staged when evaluated by the clinicians. • Patients who test positive are escorted to case manager for additional post-test counseling
and, strong efforts are displayed towards partner testing. • Screening for hepatitis B and VDRL was done on all pregnant women as per guidelines. • M&E team performs monthly cohort analysis which is shared with MDTs to ensure
adequate interventions in the event of unfavorable results. Area for Improvement and Recommendations:
1. Area for Improvement: There are no clear policies and procedures between I-TECH and WZRH outlining how to address and resolve unsatisfactory renovations. One of the waiting areas renovated by I-TECH approximately 12 months earlier bears a structural defect yet no corrective action has been taken and the waiting area poses a potential risk for patients. Recommendation: I-TECH needs to review the contract language with hospitals on the processes that must be followed once renovations are started. New guidelines on who must approve any changes in the contract must be clear and I-TECH legal counsel should be present for discussions with facilities when changes are desired once renovations have been started.
Page40
DUBTI HOSPITAL 21 March 2011
Organization and Program Management Dubti Hospital was established in 1958 for agricultural workers. In 1995, the hospital was handed over to the Afar Regional Health Bureau. The hospital provides outpatient adult services through four departments: the Psychiatric, Dental, Ophthalmology, and Surgical Referral Department. There are a total of 90 beds divided as follows: medical and TB isolation-38 bed capacity, Surgical-20 bed capacity, gynecology and obstetrics-18 bed capacity, delivery ward -3 couches, and pediatric ward-10 bed capacity. The abovementioned services are supported by the hospital’s laboratory services which include hematology, blood chemistry, enzyme-linked immunosorbent assay (ELISA) and CD4 testing. The Medical Director (MD), who heads the hospital, oversees the departments and reports to the Afar RHB. Dubti’s management structure is currently undergoing a reorganization to improve coordination with other referral hospitals. Currently, the technical arm and the administrative arms of Dubti report to the MD. The hospital has 58 full-time paid health workers and 147 administrative and supporting staff. The hospital serves a catchment area of 1.4 million and is the only referral hospital for 15 health centers in the vicinity. Three levels of management meetings include the following:
• Weekly (Monday and Thursday) meetings of general Clinical Staff
• Multi-disciplinary group meetings meet every two weeks (on Wednesdays)
• General staff meeting are held every two weeks (on Fridays)
Catchment area meetings are held in the region on a quarterly basis. These meetings include a total of six sites comprised of two hospitals and four health centers and serve as forums for discussions on challenges, performance and coordination of HIV services. I-TECH staff participate in these meetings. The hospital supports the training of nurses, lab technicians, pharmacy technicians and midwives. The ART clinic has 2,581 patients cumulatively enrolled in care, 1,769 cumulatively on treatment and 1,012 currently on treatment. Facility The Medical Director prepares a priority list of support needs and sends it to the RHB for concurrence. I-TECH has supported the renovation of the antiretroviral therapy lab, including the modification, partitioning and painting of the laboratory structure, and the purchase of appropriate work benches, table, chairs and shelves. New air conditioners and refrigerators were also installed along with a sample mixer, a CD4 machine and an automated machine for hematology and blood chemistry. I-TECH also updated the general lab and provided computers, books and some furniture for the resource center/library in collaboration with other organizations.
Page41
HIV Services Dubti Hospital has been providing voluntary counseling and testing (VCT) services since 2004. The hospital has provided HIV care and treatment since 2006 through the Global Fund and PEPFAR fund. As of 1 April 2011, 2,548 patients were receiving HIV services. Approximately 20 HIV+ patients are seen daily, with an additional 40 receiving medication refills. During 2010, Dubti provided HIV counseling and testing services to 747 pregnant women, of which the prevalence rate was 3.88 %. The hospital provides prevention services, HIV counseling and testing (HCT), adult care and treatment, prevention of mother-to-child transmission of HIV (PMTCT), tuberculosis (TB) services, sexually transmitted infection (STI) services, and laboratory services. A total of 386 patients have been referred for ART to the catchment area health center. The national comprehensive HIV training workshops were attended in the last year by the 4 clinicians and the 5 nurses are scheduled to attend in 2011. The current lost-to-follow-up (LTFU) for the HIV clinic is 18%.
The ART team evaluates approximately 50 patients daily for medication pick-up, of which the physician evaluates 20-30 for complaints and/or specific follow-up. These appointments provide an opportunity for patients to share any problem they may be experiencing, for staff to question patients on clinical symptoms of tuberculosis and to counsel on adherence strategies. Patient Support Services The adherence case management function is supported by one Adherence Case Manager (ACM), three Adherence Supporters (ASs) and three Mother Mentors (MMs). ACMs coordinate with MMs who support mothers in PMTCT activities by organizing coffee meetings and providing health education information. The ACMs have been able to conduct a patient referral audit. ASs are assigned to cover patients they are familiar with and not according to specific areas/districts. All of the ASs and MMs are people living with HIV/AIDS PLWHA at this hospital. Monitoring and evaluation (M&E) functions are supported by the Information Mentor (IM) from I-TECH, an Information Technician (IT) and a Data Clerk (DC). Chart Review At the time of this visit, the clinic had approximately 1,680 adult patients enrolled on ART. A total of 14 charts were reviewed (those of 11adults, including four pregnant women on PMCTC, and three children). All of the patients were treated in accordance with the National HIV Guidelines. The care provided is documented by checking boxes on the standard medical chart forms. All of the patients had a basic CD4 count and follow up counts as per guidelines. All patients were properly staged when evaluated by the clinicians, all met criteria for highly active antiretroviral therapy (HAART), and those who met the criteria had been prescribed prophylaxis. The therapeutic regimen prescribed in all cases appeared commensurate with the blood laboratory values and all the charts had the patient adherence box checked. All patient charts demonstrated an increase in CD4 counts from the initial pre-treatment levels. All the charts had documented a baseline complete blood count. Creatinine levels were not done at the initial visit in all but two of the patients. Screening for hepatitis B and venereal disease research laboratory (VDRL) testing was not documented on all pregnant women. Lipids and VDRL for men and children are done only
Page42
as per indication by the clinician and none of the charts had it documented. Fasting blood sugar was documented on six of the charts. On two of the charts cotrimoxazole was prescribed without indication for it. It was explained that frequently it is prescribed for as long as two weeks to assess patient compliance when the patient is determined to need HAART. By the second week, depending on the blood laboratory results, the medication and the patient’s compliance, they will decide to either prescribe or discontinue the drug. Strengths:
• There was a high level of compliance with documenting in the HIV CARE/ART follow-up forms.
• Management levels of support and participation in HIV program activities is commendable. • Hospital management has been able to recruit and retain “junior” general practitioners
interested in HIV care. • I-TECH mentors have made considerable contributions to service delivery.
Area for Improvement and Recommendations: Management
1. Area for Improvement: There is no formal process to solicit and document the ongoing training needs of HIV clinic staff. Recommendation: The hospital Human Resources (HR) should conduct regular assessments of staff training needs; when these needs are determined to be HIV specific, HR should coordinate with I-TECH mentors to develop appropriate training. Strong documentation processes need to be implemented by all involved.
Patient Support Services
2. Area for Improvement: The LTFU rate was high at 18%. There was no indication of progression tracking to inform management decisions for appropriate intervention. Recommendation: I-TECH should work with Dubti M&E staff to provide data monthly to show how outreach is supporting the return of patients. This should also generate discussions on whether other strategies may be more affective.
Medical Records 3. Area for Improvement: Some charts did not contain progress notes, presenting a challenge for any other clinician to provide appropriate care for the patient. Recommendation: Hospital management should support the addition of extra pages to patient charts for notes and encourage clinicians to add more to the chart to help support care delivery when there is no specific restriction against it. I-TECH should continue to educate clinical staff on how to write synoptic notes to document their decision-making process and how to use progress notes to complement the follow-up form. In particular, the prescribing of cotrimoxazole to assess patient’s ability to comply with a future regime should be reviewed.

Page43
Tracking of referrals 4. Area for Improvement: There is no formal process for receiving confirmation of whether a consultation has occurred other than relying on the patient. Recommendation: The hospital and ART clinic management together with I-TECH should develop a process to allow a staff person to regularly speak with or visit referral locations to accurately document the outcome of referrals. Laboratory testing 5. Area for Improvement: The laboratory does not have diagnostic testing for cryptococcal meningitis, such as India ink staining of cerebrospinal fluid, or serum cryptococcal antigen testing. Recommendation: Cryptococcal meningitis is reportedly a significant contributor to morbidity and mortality among patients with HIV in Ethiopia. Although not yet a required test in the national guidelines, if resources allow, I-TECH Ethiopia should assist in increasing laboratory capacity to aid in this diagnosis.
Page44
ASAITA HEALTH CENTER 22 March 2011
Organization and Program Management Established in 1972, Asaita Health Center (AHC) currently serves seven health posts with a population of 52,470. AHC is supported by an NGO with the construction of additional clinic buildings to upgrade AHC to the status of a general hospital. AHC referrals are sent to Dubti Hospital. AHC is staffed with 1 general practice physician, 5 Health Officers, 17 Nurses, 1 midwife, 2 pharmacists, 2 pharmacy technicians, 2 lab technicians and 2 lab technologists. AHC is led by a Medical Director. Management staff includes the Heads of the Nursing, Administration, Laboratory, PMTCT, Pharmacy and Antiretroviral therapy (ART) units. General staff meetings are held once a month. Two multi-disciplinary team (MDT) meetings are held monthly, one of which focuses specifically on the ART program. I-TECH’s Field Based Team (FBT) is present at this meeting. Quarterly catchment area meetings were implemented around June of 2010.
AHC is located in the Asaita town, Afar Region. AHC provides outpatient and laboratory services. As a nucleus health center it also supports a smaller health center, Afambo Health Center, and seven health posts (small health access points that serve approximately 5,000 people) in the vicinity. AHC refers patients for secondary /tertiary care to Dubti Zone Referral Hospital. The center also serves as a training site for nurses, nurse midwifes and laboratory technicians. AHC is currently in the process of being upgraded to a hospital as part of the implementation by the Federal Ministry of Health’s new national hospital reform process. HIV Services AHC has received Global Fund PEPFAR funds since 2006. AHC has been providing HIV care and treatment services with technical and material support (furniture, medical supplies) from I-TECH. Four health officers and two nurses provide HIV care and treatment services. The other house staff physician, a general practitioner, supervises these clinicians. The laboratory has received significant material support from I-TECH in the form of furniture, refrigerators and microscopes. Services are offered daily as per the center’s regular schedule. Chart Review As of the date of this site visit AHC had an active caseload of approximately 421 adult patients on ART, and 1,107 patients on PMTCT. A total of 16 charts were reviewed: those of eleven of adults, five on ART, one on pre-ART and five pregnant women and five of children. The review was done with the assistance of Solomon Wango, Health Officer; Sister Rukiya Ahmed, Clinical Nurse, and; Dr. Eyob Gebrehawariaz, Clinical Team Leader for I-TECH Ethiopia. The chart reviews demonstrated that patients were treated in accordance with National Guidelines on HIV care and treatment, except for several elements discussed below. The national guidelines are readily available to the clinicians for reference. The care provided was documented by
Page45
checking boxes on the standard medical chart forms. The completion by clinicians of the intake forms and of the flow chart is interpreted as a measure of quality depicting the continuum of care and the adherence to the national guidelines.
Four of the charts reviewed had referral documentation for “transfer-in” and one had referral documentation for both “transfer in” and transfer-out”. It was explained that the confirmation of transfers primarily depends on the patient carrying the documents. On the other hand, one of the charts reviewed contained clear documentation on both transfer-in and transfer-out referrals and one can infer that the clinicians are systematically following standard operating procedure. This has to be understood within the context of the Afar region being extraordinarily isolated with very few resources in all respects. All of the patients had a basic CD4 count and follow up counts as per guidelines. All patients were properly staged when evaluated by the clinicians, all met criteria for highly active antiretroviral therapy (HAART), and those who met criteria were prescribed prophylaxis. All patients who qualified for isoniazid (INH) prophylaxis received it as per guidelines. Acid-fast bacillus smear (ABFS) results were found in the charts. The therapeutic regimen prescribed in all cases appeared commensurate with the blood laboratory values; all charts reviewed had the patient adherence box checked. All but one patient had increased their CD4 counts from the initial level when started on treatment. It was not clear that immunological failure is being recognized. Creatinine level test results were available in only six of the fourteen patient files that could have had it. It was explained that creatinine testing was considered optional due to frequent lack of reagents. All the patients had documented baseline screening for tuberculosis and on follow up visits AFBS were properly documented. Screening for hepatitis B and venereal disease research laboratory (VDRL) tests were not performed on pregnant women as per guidelines. Lipids, fasting blood sugar, and VDRL for men and children are done only as per indication by the clinician. One patient had high blood sugar consistent with a diagnosis of diabetes mellitus but no follow up/evaluation was done. One pregnant woman had only been seen once for antenatal care three months following an HIV positive diagnosis; though she had attended ART visits three times during that period. None of the children that were of age for growth monitoring had the growth charts plotted.
Strengths:
• I-TECH Adherence and M&E mentors stationed in the region provide easy access to mentees.
• ACMs are hired by the RHB, through a subcontract mechanism with I-TECH. This is an important step towards ensuring local ownership and the sustainability of the clinical mentoring program in the Afar region program.
• I-TECH has established adherence case systems that ensure all cases are captured by the use of Adherence Supporters (ASs) and MMs.
• I-TECH supports the process for sending data to the district (Woreda) level authorities who will update the RHB with the data.
• AHC can be considered a “one-stop” service delivery model where individuals are treated with respect, dignity and competence.
Page46
• Considering that the staff at AHC is primarily health officers, the level of completeness and appropriateness of care is reasonable.
• AHC staff highly regards the support – training, mentoring and material support – that I-TECH provides the center.
Areas of Improvement and Recommendations: Medical Record Documentation 1. Area for Improvement: Some charts did not contain progress notes. Recommendation: AHC ART clinic management should determine how much additional information is realistic to expect clinicians to documents to get a “true” picture of care provided. I-TECH should continue to educate clinical staff on writing synoptic notes to document their decision-making process and using the progress notes to complement the follow-up form. Preventive health care: Antenatal care 2. Area for Improvement: One pregnant woman had only been seen once for antenatal care three months after an HIV diagnosis, though she attended ART visits three times during that same period. Recommendation: AHC clinicians should be more attentive to patients who miss follow up appointments in other service areas. Providing joint appointments for antenatal care and ART is one strategy to avoid missed appointments. Clinical and immunological failure 3. Area for Improvement: One patient experienced a decline in CD4 counts following the initiation of treatment, it was not clear that immunological failures are identified and acted upon. Recommendation(s): I-TECH could help build capacity in identifying clinical /immunological failure. A clear protocol for action can be adopted for potential treatment failures for example evaluating adherence assessment, case discussions in multi-disciplinary team (MDT) meetings, etc. Baseline Laboratories 4. Area for Improvement: Many of the recommended baseline laboratory tests are not systematically performed as per stage of the disease (i.e. tests for alanine amino transferase (ALT), creatinine, lipid profile, hepatitis B and C serology, fasting blood sugars (FBS), syphilis serology). Not all pregnant women received venereal disease research laboratory (VDRL) and hepatitis B screenings. It was explained that lack of laboratory reagents precluded doing these screening systematically. Recommendation: I-TECH Ethiopia with the RHB should help determine how compliance with the national and WHO guidelines for laboratory services should be “conciliated” with the availability of local resources.

Page47
Growth charts 5. Area for Improvement: None of the children that were of age for growth monitoring had the growth charts plotted.in the medical charts reviewed. Recommendation: AHC should ensure that growth charts are incorporated into every pediatric file and should be regularly updated. Poor growth trends should be used for WHO staging as per the national guidelines.

Page48
AWASH HEALTH CENTER 24 March 2011
Organization and Program Management Awash Health Center (AWHC) is the only health center in the zone that provides antiretroviral therapy (ART) treatment. It serves a catchment population of 32,068. The town of Awash and surrounding areas are primarily rural and of low socioeconomic status. The health center may be upgraded to the status of a general hospital soon. AWHC also serves three clinics and four health posts in the vicinity. It also receives sample referrals from nearby facilities (Werer Health Center, Gewane Health Center and National Hospital) to perform CD4, hematology and blood chemistry tests. AWHC staff includes one general practice physician, three health officers, 11 nurses, two midwives, three pharmacy staff and four lab staff. AWHC is led by a Medical Director. General staff meetings are held once a month. Two multi-disciplinary team (MDT) meetings are held monthly where catchment area HIV service providers meet about care and treatment issues with the RHB and funding representatives. One MDT meeting focuses on the ART program and the I-TECH Field Based Team (FBT) is present at this meeting. Other meetings, including the catchment area meetings, are held quarterly. AWHC staff consists of 24 health care providers: one physician, three health officers, 12 nurses, four laboratory technicians, four pharmacy technicians and 20 administrative & supporting staff. The HIV care and treatment team is composed of: one physician, one health officer, three nurses, one adherence case managers, five adherence supporters and four mentor mothers (MMs). HIV Services The ART clinic has 766 patients cumulatively enrolled in care, 500 cumulatively on treatment and 267 currently on treatment. The center offers inpatient services only on an emergency basis. The team evaluates approximately 20 patients daily for medication pick-up, of which five or six are evaluated for complaints and or specific follow-up. These appointments provide an opportunity for patients to relate any problem they may be experiencing, and for staff to question patients on clinical symptoms of tuberculosis and to counsel on adherence strategies. AWHC, with the technical and material support of I-TECH (furniture and medical supplies), has been providing HIV care and treatment services since 2006. The laboratory has received significant material support from I-TECH in the form of furniture, refrigerators and microscopes. I-TECH infrastructural support includes renovation of the labs and waiting areas, and purchase of furniture and lab equipment (microscopes). AWHC’s quality assurance program is organized around infection prevention. I-TECH has introduced a continue quality improvement (CQI) initiative through the plan–do–study–act (PDSA) cycle approach. Data is collected regularly for compliance with performance standards as per clinical guidelines and when there are elements not in compliance a PDSA cycle is implemented.
Page49
AWHC maintains an individual patient paper chart with a unique identifier for each patient. Patient’s information is documented at every visit in an HIV Care/ART Follow-Up standardized form (as per design by the Federal Ministry of Health). The form is comprehensive and facilitates the documentation of the care plan of the patient. The chart also contains other HIV/Care/ART intake standardized forms: patient registration form, past medical / treatment history, general condition / physical exam, clinical review, social assessment, ART adherence counseling and, ART assessment and plan. Laboratory results and referrals documentation is kept in the chart. Chart Review At the time of this visit, AHC is providing approximately 260 positive patients with ART. A total of twelve charts were reviewed (seven adults, including four pregnant women on PMCTC, and five of children). The review was done with the assistance of AWHC Nurse Abdella Kedir. All but one of the patient charts reviewed contained a baseline CD4 count and follow up counts as per national HIV care and treatment guidelines. All other patients were properly staged when evaluated by the clinicians, all met criteria for highly active antiretroviral therapy (HAART), and those who met criteria for prophylaxis had been prescribed it. The one patient that did not have the CD4 count was a girl of eight years whose laboratory had been ordered in various occasions but it was not clear why the blood had not been drawn, or, if drawn, what had happened to the sample. She was asymptomatic and was receiving cotrimoxazole. The therapeutic regimen prescribed in all cases appeared commensurate with the blood laboratory values and all the charts had the patient adherence box checked. All, but the eight year old girl, had increased their CD4 counts from the initial level when started on treatment. Creatinine level testing was not performed. It was explained that this testing was considered optional due to lack of reagents. Strengths:
1. AHC can be considered a “one-stop” service delivery model where individuals are treated with respect, dignity and competence.
2. Except for the lack of laboratory testing, quality of care is reasonably good; assuming that good documentation in the medical chart standards forms is a measure of quality. All of the patients (except the asymptomatic eight years girl without the CD4 count) had good immunological response based on CD4 counts.
3. AHC staff regards highly the support I-TECH provides them, both in training and mentoring and in material support.
Areas for Improvement and Recommendations: Tracking of referrals 1. Area for Improvement: The confirmation of whether a consultation actually took place depends on the patient notifying the clinician about the event or personal communication rather than some official communication with the referring/receiving source. Recommendation: I-TECH should work with the FMOH and RHB to develop a referral verification process that can used by all facilities since this was found to be a repeat issue at many sites.

Page50
Quality Assurance/Improvement 2. Area for Improvement: Monitoring performance data is a measure of quality which serves to inform changes in care. It was unclear, however, whether an ongoing cycle of change and re-measurement was in operation at the time of the assessment. Recommendation: I-TECH should ensure that site staff are deciding what topics are appropriate for the PDSAs and coordinate all aspects of the cycle, not just the mentors. 3. Area for Improvement: AWHC did not have the laboratory capacity - India ink staining of cerebrospinal fluid or serum cryptococcal antigen testing - to test for cryptococcal meningitis, Recommendation: Cryptococcal meningitis is reportedly a significant contributor to morbidity and mortality among patients with HIV in Ethiopia. Although not yet a required test in the national guidelines, if resources allow, I-TECH Ethiopia should assist in increasing laboratory capacity to aid in this diagnosis.
Page51
Meeting with Afar Regional Health Bureau March 23, 2011
Regional Health Bureau staff shared their feedback on the work I-TECH has accomplished date. Their remarks are summarized below:
• I-TECH’s work in the region is well appreciated
• I-TECH’s work spreads across to some of the most challenging places
• I-TECH is the main NGO in the region supporting HIV programs
• There has been good communication and coordination with I-TECH’s regional team
• RHB heads and I-TECH regional teams often drive to the catchment area meetings together
• I-TECH has been involved in training 250 health extension workers and assisting in infrastructural support for the region especially the renovation of the regional health labs
• I-TECH has supported the coordination of health facility data with the Regional Health Bureau
The RHB requested further assistance from I-TECH in the following areas:
• Support in training more health extension workers. About 750 health extension workers need training.
• Flexibility to support more programs; including their Media Outreaches and health awareness programs
• Support in prevention activities of other diseases such as malaria
• Greater coverage of PMTCT activities across the region
• Supports programs that eliminate female genital mutilation (circumcision) and infection control
• Sustainability plans for in-country ownership of I-TECH functions and I-TECH supported staff
Page52
Team 2 ClASS Reports
Page53
GONDAR UNIVERSITY HOSPITAL 15 March 2011
Gondar University Hospital (GUH) is an HIV care and treatment site supported by the Federal Ministry of Health (FMOH) through the Amhara RHB. Governance of GUH is shared between the FMOH and Ministry of Education. Based on feedback from the community and patients, a new Board was recruited and resulted in a change in the senior management coordinators. The new CEO proposed additional changes to improve staff retention and quality of care services. GUH HIV program has enrolled 8,950 patients (as of 3/8/11), of whom 5,975 were started on ART, of which 3,548 are currently on ART, with approximately 2,000 on pre-ART. The HIV program sees from 60-70 patients daily and processes 70-100 ART refills per day. Organization and Program Management The GUH HIV program is staffed with one Health Officer, two registered pediatric nurses, four registered nurses trained on adult HIV/ART care and treatment, three ACMs, eight ASs, and four Mother’s Mentors (MMs). The ASs and MMs are generally persons living with HIV/AIDS (PLWHA) who conduct patient follow-up and education along with their other duties. Some receive a stipend and others are volunteers, and both are responsible for community outreach. Staff shared how they were able to work with some of the priests in the community to help them understand that holy water can be used while the patient continues to take their medication. Some priests had been telling patients to stop medication and allow holy water to cure them. The GUH HIV program is well organized with the ART pharmacy, laboratory, waiting areas and patient care rooms all located on the same floor. Space is at a premium for the entire hospital as the tour of the facility illustrated. Space issues should be resolved within one year with the completion of a new hospital facility a few miles away. Two clinicians share a room, reducing the likelihood of physical examinations and patient confidentiality. During the visit there was shuffling of departments to new space that would allow the Chronic Care Clinic to move and provide the entire floor of space to the HIV clinic. The waiting area is not well ventilated. There is a treatment renewal room for three staff to use with patients. While there are windows in the room, there was no movement of air through the space. HIV Services GUH offers inpatient and outpatient HIV prevention, care, and treatment services. HIV counseling and testing (HCT) is offered at the Voluntary HIV Counseling and Testing (VCT) clinic, which is located beside the HIV clinic. HCT is also offered as a routine service for all pregnant women and all patients with tuberculosis (TB); it is offered based on provider discretion in the general Outpatient Department and inpatient wards. Once a patient tests HIV positive they are escorted to the HIV clinic for registration or referral to another facility. Outpatient adult and pediatric HIV care and treatment are offered in separate clinics, with children being seen at the Pediatric Outpatient Clinic. The clinics are open Monday to Friday, but they are
Page54
considering re-starting their Saturday clinic. All patients see a nurse for routine clinic appointments, and can be referred to a health officer or general practitioner at the nurse’s discretion. The hospital, with I-TECH’s support, has recently opened a TB isolation ward with four negative pressure rooms for multi-drug-resistant tuberculosis (MDR-TB). HIV care and treatment is not integrated with other services – e.g., the Mother and Child Health (MCH) clinic, the TB clinic - and relies on patient referrals and patients scheduling multiple appointments for the different services. Every attempt is made to schedule visits on the same day for the different departments to help facilitate transportation. The HIV clinic dispensing pharmacy and the HIV laboratory are also independent of the main hospital dispensing pharmacy and laboratory, respectively. The pharmacy experiences periodic low stock levels of antiretroviral drugs (ARVs). The laboratory has a FACS Caliber machine for CD4 enumeration, with a FACS Count for back-up. The lab experiences inconsistent supplies of reagents (at the time of this visit they had no FACS Caliber reagents) and slow response time for equipment repair (they have been waiting for repair of the chemistry machine for over a year now). Patient Support Services In January 2011, I-TECH recognized that Adherence Case Managers (ACMs) were not being fully utilized and changed their clinic processes to require that all new patients see an ACM during their initial visits. This has significantly increased the volume of patients seen by the ACMs. Staff identified that general patient referrals did not work well because there are no capable facilities in the area where patients can be referred out, all referrals are within the university hospital. HIV care referrals work better because Gondar staff has worked with the health centers to build their capacity to manage more complicated patients. Staff identified that many patients who could be seen at their local health center continue to prefer a facility where they are not known or recognized. Patients who live outside of the catchment area pose a problem for the ASs and MMs to track due to lack of funding and transportation support. ACMs reported delays in payments through the RHB since the transfer from I-TECH. MMs work with the women enrolled in prevention of mother-to-child transmission of HIV (PMTCT). Monitoring and Evaluation Six Monitoring and Evaluation (M&E) staff support the GUH HIV program, but they share a single office space. Charts are pulled monthly to conduct data quality assurance assessments. While the hospital has a Health Management Information Systems (HMIS) Department, there is no coordination or sharing of information with I-TECH M&E staff. The primary area for improvement desired by staff is for training updates. Mentors are tasked with updating staff, but it was shared that time constraints do not always allow for the level of detail needed and desired. Staff appreciated the support of the Mentors in preparations for data review meetings conducted in the region. GUH is using the Johns Hopkins database, but this is not a software platform for which I-TECH has technical expertise resulting in challenges for staff when problems arise. The CD-drives of the I-TECH computers do not work, so data is backed up on a thumb drive. This drive is used to send the data to the I-TECH Addis office, but is also carried around by the mentor. There is no back-up kept at GUH should the mentor be unavailable. A back-up power source for
Page55
the computers has not worked since it was provided several years ago, but has yet to be replaced; an extended power outage would seriously compromise the site. Strengths:
• The hospital and university have been responsive to internal and external requests for change and improvements.
• The new hospital management has an excellent knowledge of the HIV program and proposed expansions. New health care financing options are being considered to help increase funds.
• The institution identified TB/MDR-TB management as a problem and worked with I-TECH to implement a solution
• There is effective task shifting of clinical care at the HIV clinic • The HIV laboratory supports several other health facilities in the region • There is a vision for the laboratory to move towards WHO accreditation • Measurement and evaluation team members are current on data entry. • Adherence case managers keep detailed documentation of discussions with patients and
have worked with religious leaders to support prevention efforts. • Adherence supporters are providing significant time to conduct contact tracing and patients
prior to and after identified as lost. • Hospital management has arranged to allocate additional space to the ART program within
a month of the assessment. Areas for Improvement and Recommendations: HIV Services 1. Area for Improvement: The site is not using patient/facility-level data to identify areas for improvement, guide solutions, and monitor the impact of efforts towards improvement. Recommendation: GUH HIV program staff should form a continuous quality improvement (CQI) team, and with support from I-TECH, use facility data to conduct a formal CQI process. 2. Area for Improvement: Frequency of patient appointments does not seem to be based on a standardized protocol. Recommendation: GUH HIV program staff should develop and implement clear criteria for determining the frequency of appointment visits, which will then reduce workload. 3. Area for Improvement: With less than 2% of ART patients on second-line treatment, clinical and immunological failure is potentially being missed or not acted upon. Recommendation(s): With the support of I-TECH, GUH HIV program staff should work with health care workers to build their capacity to identify clinical/immunological failure. Develop a clear protocol for action to be taken once potential treatment failure is identified (e.g., adherence assessment, multi-disciplinary team (MDT) meetings, viral load testing). Consider implementing a viral load specimen transport system so patients can access this test at the nearest providing laboratory. Consider using the patient-level data at the facility to flag patients with immunological failure.
Page56
4. Area for Improvement: ARV supply shortages are limiting the length of prescription a patient can receive, and thus affect appointment frequency and workload. Recommendation: GUH management and FMOH should identify all potential contributing factors to ARV supply shortages and develop strategies to address the issues that are within the university’s scope of influence. Laboratory 5. Area for Improvement: The HIV laboratory is not integrated with hospital laboratory. Recommendation: GUH should determine if it may be more efficient to have an integrated laboratory for HIV and non-HIV investigations. 6. Area for Improvement: The FACS Count machine is used as a back-up when the FACS Caliber is not in use (as in the current situation), however the FACS Count machine failed the most recent external quality assurance (EQA) cycle. Recommendation: GUH should act upon EQA results to ensure this back-up CD4 machine is providing accurate results. Monitoring and Evaluation 7. Area for Improvement: Data is not being stored effectively and no copy is currently kept at the university hospital. Recommendation: I-TECH Ethiopia should annually assess the status of all equipment as well as any equipment requests that have not been addressed. Refresher sessions are needed with mentors to review acceptable data back-up options. This is a priority area.
8. Area for Improvement: University staff have not been included in data analysis or informed of how to access data for CQI efforts. Recommendation: I-TECH regional M&E staff and the M&E mentor should meet with the University HMIS department and determine how staff can support each other, particularly in the area of equipment maintenance.
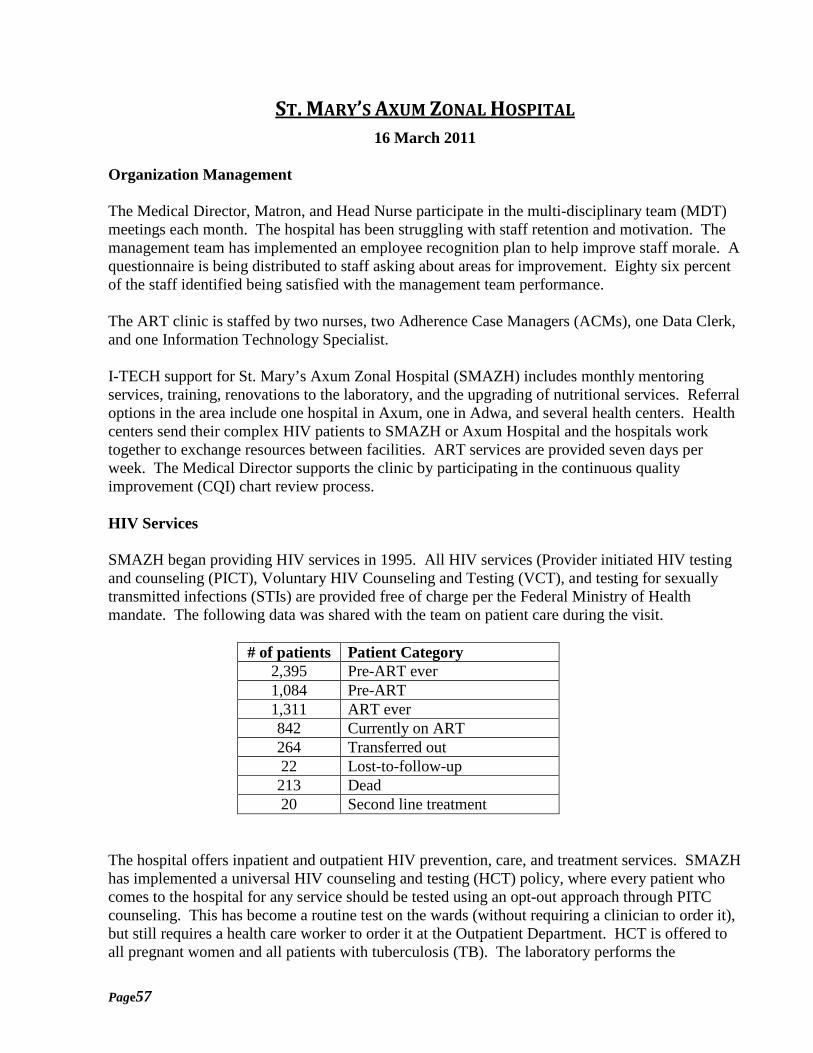
Page57
ST. MARY’S AXUM ZONAL HOSPITAL 16 March 2011
Organization Management The Medical Director, Matron, and Head Nurse participate in the multi-disciplinary team (MDT) meetings each month. The hospital has been struggling with staff retention and motivation. The management team has implemented an employee recognition plan to help improve staff morale. A questionnaire is being distributed to staff asking about areas for improvement. Eighty six percent of the staff identified being satisfied with the management team performance. The ART clinic is staffed by two nurses, two Adherence Case Managers (ACMs), one Data Clerk, and one Information Technology Specialist. I-TECH support for St. Mary’s Axum Zonal Hospital (SMAZH) includes monthly mentoring services, training, renovations to the laboratory, and the upgrading of nutritional services. Referral options in the area include one hospital in Axum, one in Adwa, and several health centers. Health centers send their complex HIV patients to SMAZH or Axum Hospital and the hospitals work together to exchange resources between facilities. ART services are provided seven days per week. The Medical Director supports the clinic by participating in the continuous quality improvement (CQI) chart review process. HIV Services SMAZH began providing HIV services in 1995. All HIV services (Provider initiated HIV testing and counseling (PICT), Voluntary HIV Counseling and Testing (VCT), and testing for sexually transmitted infections (STIs) are provided free of charge per the Federal Ministry of Health mandate. The following data was shared with the team on patient care during the visit.
# of patients Patient Category 2,395 Pre-ART ever 1,084 Pre-ART 1,311 ART ever 842 Currently on ART 264 Transferred out 22 Lost-to-follow-up 213 Dead 20 Second line treatment
The hospital offers inpatient and outpatient HIV prevention, care, and treatment services. SMAZH has implemented a universal HIV counseling and testing (HCT) policy, where every patient who comes to the hospital for any service should be tested using an opt-out approach through PITC counseling. This has become a routine test on the wards (without requiring a clinician to order it), but still requires a health care worker to order it at the Outpatient Department. HCT is offered to all pregnant women and all patients with tuberculosis (TB). The laboratory performs the
Page58
confirmatory HIV test for those who initially test positive through PICT. HCT is also offered at the VCT Clinic, which is located in the HIV Clinic block. Once a patient tests positive they are escorted to the HIV Clinic for registration or referral to another facility. Outpatient adult and pediatric HIV care and treatment are offered together at the HIV clinic (separate from the general Outpatient Department), which is open seven days per week. All patients are seen by the HIV/ART Nurse Specialist (HANS) for routine clinic appointments, who can consult with the internist/medical director on any complicated issues. HIV care and treatment is not integrated with other services (e.g., the Mother and Child Health (MCH) Clinic, the TB Clinic) and relies on patient referrals and patients scheduling multiple appointments for the different services. HIV medical records are integrated with the general hospital medical records. The HIV Clinic Dispensing Pharmacy is independent of the main hospital dispensing pharmacy. The pharmacy experiences periodic low stock levels of antiretroviral drugs (ARVs); at the time of this visit, the pharmacy was facing an inadequate supply of ARV syrups. The hospital has a basic laboratory for the HIV/Chronic Care Clinic for phlebotomy, dipstick tests, and microscopy. The main hospital laboratory performs all automated tests, and has a FACS Count machine for CD4 enumeration. The laboratory experiences inconsistent supply of reagents and slow response time for equipment repair. At the time of this visit, the laboratory had a shortage of hematology reagents and controls. The FMOH case management checklist is used by clinicians to identify those patients in care who require a referral for adherence or other referrals. ACMs have established strong relationships with the other health facilities in the area to be able to verify transfer out and patient deaths. Support staff identified that there are resource/referral books for the region listing all known resources, but the hospitals do not have enough for each program to have its own copy. ACMs reported sharing a single book between several departments. The once per month visit by ACMs and monitoring and evaluation (M&E) mentors was identified as insufficient for building capacity and providing training. Adherence case managers indicated that no formal training has been provided to them since their initial orientation and training. One or two hours of listening to someone refer to an article or meeting they attended did not “train” them to do something new. Staff did appreciate the mentor sitting in on counseling and adherence sessions and providing immediate feedback on how to ask better questions and provide additional strategies to promote ART adherence. I-TECH is supporting the data management of the HIV program and the hospital health management information systems (HMIS). Strengths:
• The hospital CEO and senior management have been with the organization for a long time and are actively involved with the ART program.
• Management conducts internal assessments every six months with staff to gather areas for improvement.
Page59
• The hospital will be developing performance-based recognition program to motive staff and reduce staff turnover.
• The Medical Director is an experienced physician and is actively involved in the HIV services at the hospital
• Multi-disciplinary team (MDT) meetings are being used to identify areas for improvement and develop action plans (e.g., to reduce the lost to follow-up rates)
• Adherence case managers follow the national guidelines and maintain detailed documentation on the services they provide.
• ACMs are verifying patients who transfer out with visits to the identified facilities. • Uptake of HIV testing is excellent throughout the hospital • The HIV clinic is very accessible, open seven days per week • There is effective task shifting of clinical care at the HIV Clinic • The retention of the HIV/AIDS Nurse Specialists is excellent • There is a formalized system for making referrals/transfers to other facilities and for
tracking the completion of referrals Areas for Improvement and Recommendations: HIV Services 1. Area for Improvement: The hospital regularly holds MDT meeting to address issues, however, the hospital does not have a formal process for using patient/facility-level data to identify areas for improvement, guide solutions, and monitor the impact of efforts towards improvement. Recommendation: The Axum ART program staff should form a continuous quality improvement (CQI) team, and with support from I-TECH, use facility data to conduct a formal CQI process. 2. Area for Improvement: At the Child Welfare Clinic (CWC) it appeared that all children are being tested for HIV when they come for their month nine immunizations and after the mother is tested, as part of the hospital’s universal HIV testing policy (there may have been a misunderstanding about this due to a language barrier). Recommendation: The hospital should confirm the HIV testing policy at the CWC. It is unnecessary to routinely test children of mothers who test negative unless there is a different route of HIV exposure. Patient Support Services 3. Area for Improvement: The Family Matrix tool was not in the majority of patient files reviewed and is not being fully utilized by health care workers. Recommendation(s): The partners and children of patients already enrolled in HIV care are at high-risk for HIV so family member testing is a critical entry point for identifying people infected with HIV and is an important opportunity for reinforcing prevention messages for those that are negative. The Family Matrix tool has a high potential for facilitating this process. Hospital ACMs and other clinic staff need to ensure the tool is used for all patients at enrollment and that it is referred to and updated at every visit until all family members at risk have been tested and those who are positive have been enrolled into care. The tool should be used as a reminder to work with patients through the entire process of family member testing, which starts with disclosure. An individualized plan should be developed with each patient on how they will disclose, and strategies for having family members
Page60
tested and enrolled into care. The tool should be kept in a location in the patient file (e.g., inside the front cover) to help staff remember to use it. 4. Area for Improvement: With only 2.4% of ART patients on 2nd line, clinical and immunological failure is potentially being missed or not acted upon. Recommendation(s): I-TECH Ethiopia should work with health care workers to build their capacity to identify clinical/immunological failure. I-TECH Ethiopia with ART focal person should develop a clear protocol for action to be taken once potential treatment failure is identified (e.g. adherence assessment, multi-disciplinary team (MDT) meeting, and viral load). Consider using the patient-level data at the facility to flag patients with immunological failure. 5. Area for Improvement: Of the total pediatric patients ever started on ART, only 60% are currently active on ART. Recommendation: The hospital HIV team should review files from pediatric patients who have dropped out from ART to identify any systems issues that may be resulting in this high drop off rate. 6. Area for Improvement: There is a high rate of LTFU among pre-ART patients. Recommendation: The hospital HIV team should try to identify reasons for the high LTFU rate among pre-ART patients to develop targeted strategies to improve retention. Laboratory 7. Area for Improvement: Viral load specimens are being transported to the Tigray Regional Referral Laboratory in Mekelle, however the specimen storage and transportation chain may not be maintaining specimen integrity. Recommendation: The hospital HIV team should, with the support of I-TECH, should develop a protocol for specimen storage and transportation that assures valid and reliable results. 8. Area for Improvement: The laboratory does not have diagnostic testing for cryptococcal meningitis, such as India ink staining of cerebrospinal fluid, or serum cryptococcal antigen testing. Recommendation: Cryptococcal meningitis is reportedly a significant contributor to morbidity and mortality among patients with HIV in Ethiopia, so if resources allow, I-TECH Ethiopia should assist in increasing laboratory capacity to aid in this diagnosis. 9. Area for Improvement: The laboratory is participating in EQA for biochemistry but is not able to interpret the results. Recommendation: The hospital laboratory should work with I-TECH Ethiopia and EHNRI to ensure that laboratory staff is able to correctly interpret the results of all EQA cycles.
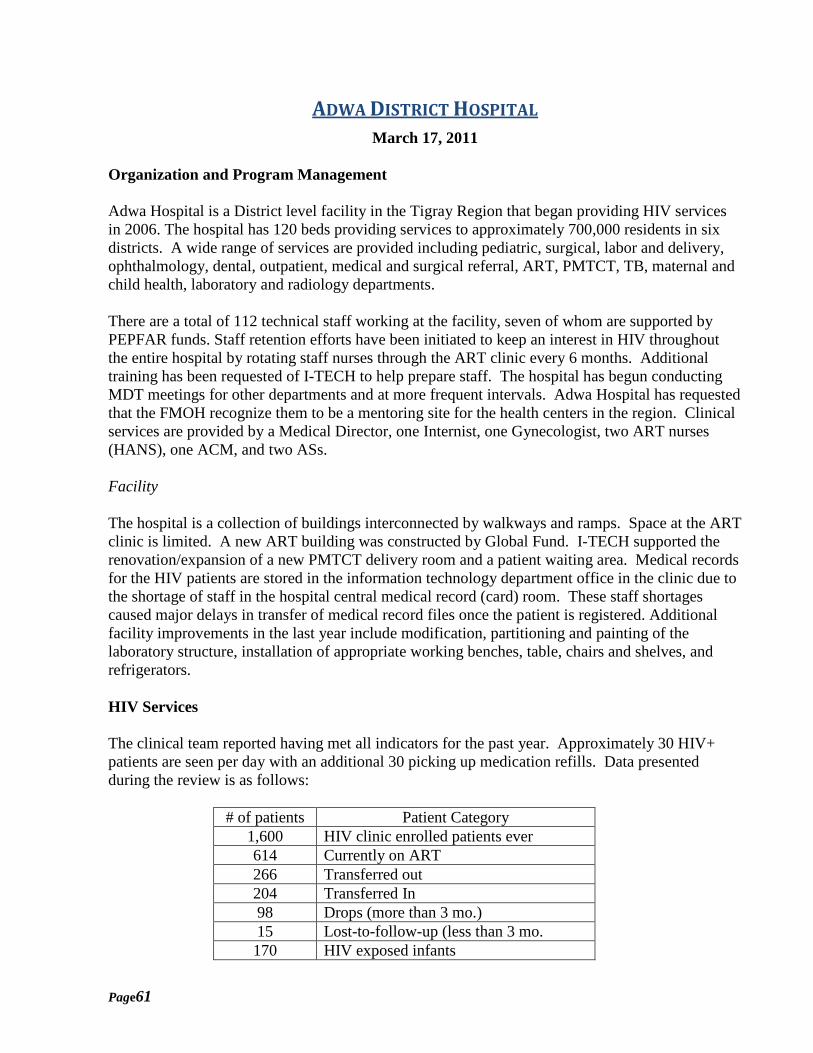
Page61
ADWA DISTRICT HOSPITAL March 17, 2011
Organization and Program Management Adwa Hospital is a District level facility in the Tigray Region that began providing HIV services in 2006. The hospital has 120 beds providing services to approximately 700,000 residents in six districts. A wide range of services are provided including pediatric, surgical, labor and delivery, ophthalmology, dental, outpatient, medical and surgical referral, ART, PMTCT, TB, maternal and child health, laboratory and radiology departments. There are a total of 112 technical staff working at the facility, seven of whom are supported by PEPFAR funds. Staff retention efforts have been initiated to keep an interest in HIV throughout the entire hospital by rotating staff nurses through the ART clinic every 6 months. Additional training has been requested of I-TECH to help prepare staff. The hospital has begun conducting MDT meetings for other departments and at more frequent intervals. Adwa Hospital has requested that the FMOH recognize them to be a mentoring site for the health centers in the region. Clinical services are provided by a Medical Director, one Internist, one Gynecologist, two ART nurses (HANS), one ACM, and two ASs. Facility The hospital is a collection of buildings interconnected by walkways and ramps. Space at the ART clinic is limited. A new ART building was constructed by Global Fund. I-TECH supported the renovation/expansion of a new PMTCT delivery room and a patient waiting area. Medical records for the HIV patients are stored in the information technology department office in the clinic due to the shortage of staff in the hospital central medical record (card) room. These staff shortages caused major delays in transfer of medical record files once the patient is registered. Additional facility improvements in the last year include modification, partitioning and painting of the laboratory structure, installation of appropriate working benches, table, chairs and shelves, and refrigerators. HIV Services The clinical team reported having met all indicators for the past year. Approximately 30 HIV+ patients are seen per day with an additional 30 picking up medication refills. Data presented during the review is as follows:
# of patients Patient Category 1,600 HIV clinic enrolled patients ever 614 Currently on ART 266 Transferred out 204 Transferred In 98 Drops (more than 3 mo.) 15 Lost-to-follow-up (less than 3 mo. 170 HIV exposed infants
Page62
The hospital offers inpatient and outpatient HIV prevention, care, and treatment services. HIV counseling and testing (HCT) is offered at the Voluntary HIV Counseling and Testing (VCT) clinic, which is located at the general outpatient department (OPD). HCT is also offered as a routine service for all pregnant women and all patients with TB, and based on provider discretion in the general outpatient department and the inpatient wards. Once a patient tests positive they are escorted to the HIV clinic for registration or referral to another facility, and they always see the case manager for counseling before being referred out. Outpatient adult and pediatric HIV care and treatment are offered together at the HIV clinic, which is located next to the chronic care clinic. The HIV clinic is open Monday to Friday. All patients are seen by the HANS Nurse for routine clinic appointments. For complex clinical issues the HANS consult the physician at the chronic care clinic or the I-TECH mentors. HIV care and treatment is integrated at the mother-child health (MCH) clinic. Once a pregnant woman tests positive she goes to the HIV clinic for registration, but then receives all of her antenatal and postnatal care (including ARVs) at the MCH along with the HIV exposed infant, until 6 weeks post-partum. The TB clinic is located adjacent to the HIV clinic so relies on patient referrals and patients having dual appointments for HIV and TB services. The HIV and chronic care clinic dispensing pharmacy is independent of the main hospital dispensing pharmacy. The pharmacy experiences periodic low stock levels of ARVs. The hospital has an integrated laboratory for HIV and non-HIV services, and has a FACS Count machine for CD4 enumeration. They send samples for HIV viral load testing to Tigray Regional Referral Laboratory in Mekelle. They experience inconsistent supply of reagents (currently no hematology reagents) and slow response time for equipment repair (chemistry and FACS Count currently waiting for repair). Patient Support Services HIV clinic staff provides telephone and on-site consultation for difficult patients. Currently there are only five patients with treatment failure that are on second line therapy. The ACM is the first point of contact for new patients at this facility. The intake is done by the Data Technician who then refers the patient to the HANS Nurse for a clinical assessment. If the patient declines enrollment on the first visit, a second visit is still scheduled to allow other program staff to speak with the patient. It was reported that very few patients refuse care. Four Mother’s Mentors (MMs) also called Moms for Moms (MOMs) at some facilities support the program working with patients of PMTCT. Two of the MMs work at the site and two conduct community visits. The MMs conduct follow-up for patients missing appointments, LTFU or decline to enroll for care. All of the support staff identified a need for more specific training updates. One employee noted that she had worked in the position for two years, but had not been to any other training. Topics of most need were identified as specific counseling skills for the ACMs, more information on new treatment medications and side-effects, and new strategies for conducting risk assessments. The ACMs have asked to attend some of the clinical updates, but have been told they are not clinicians, yet they are the ones primarily responsible for developing and working with patients on adherence issues. This is an issue that I-TECH needs to consider to ensure that staff are able to perform their duties.
Page63
Change Life is an NGO providing people with HIV counseling and support services. This group works with the ASs and Outreach Workers (ORWs). Missionaries of Charity is another organization providing housing and food support. Monitoring and Evaluation M&E staff report consistently being current with data entry. There are weekly ART team meetings where any data challenges are reported. Twice a month the HIV Committee meets and program data is made available. Incomplete registration forms are a significant problem that delays data entry in all parts of the hospital. The hospital has a HMIS department compiling data for the entire hospital. HIV program M&E staff meets regularly with HMIS to share gaps in the registers. Strengths:
• Hospital support of the ART program is strong. • Hospital management is conducting in-services for all clinical staff on HIV and using
rotation every 6 months as a way to retain staff. • ART MDT meetings are being used to identify areas for improvement and develop action
plans • The Maternal-Child Health (MCH) clinic offers integrated HIV care and treatment
services, with 100% testing uptake, mother support groups, and partner testing • There is a high level of engagement of all patients who test HIV positive at the hospital.
Even patients who are not enrolling into HIV care at the site are escorted to the ACM for HIV education/counseling, and may even be scheduled for follow-up counseling
• There is effective task shifting of clinical care at the HIV clinic • Based on review of the TB screening register it appears nearly all patients attending the
HIV clinic are being screened for TB at every visit • Family planning services are integrated with the HIV care • There is a formalized process for verifying if transfer-out patients complete the referral to
the new facility (if within the catchment region) • Patients attending the HIV/Chronic care clinic have on-site phlebotomy instead of having
to walk to the central laboratory • Linkages and relationship to support organizations are meeting the patient needs. • ACMs and ASs are using multiple options to track and bring patients back into care. • MMs are filling a key role in educating and supporting clients.
Areas for Improvement and Recommendations: HIV Services 1. Area for Improvement: Physicians at the hospital are available to the HIV clinic staff for consultation but play a minimal role in ongoing mentorship of the staff or in monitoring the quality of the care provided. The responsibility of quality oversight is left to the I-TECH team. Recommendation: If staffing time allows, the hospital physicians should participate in monitoring
Page64
the quality of care at the HIV clinic. This could be done through periodic chart reviews and observation of clinical encounters. 2. Area for Improvement: Although the hospital has a regular MDT meeting to address issues, they do not have a formal process for using patient/facility-level data to identify areas for improvement, guide solutions, and monitor the impact of efforts towards improvement. Recommendation: Hospital and ART program management should form a continuous quality improvement (CQI) team, and with support from I-TECH use facility data for a formal CQI process. 3. Area for Improvement: The hospital has adopted an “opt-out” policy for HIV counseling and testing, however the health care workers (HCW) interviewed who is offering PITC at the out-patient department was using language consistent with “opt-in” testing. Recommendation: Hospital and I-TECH staff agreed that they should be using an opt-out approach to HIV testing. Language to be used when presenting the test to the patient should be scripted and agreed to by all appropriate entities since subtle differences may affect test acceptance rates. 4. Area for Improvement: Frequency of patient appointments does not seem to be based on a standardized protocol. Recommendation: ART program management should develop and implement clear criteria for determining the frequency of appointment visits, which will then reduce workload. 5. Area for Improvement: During the chart review we found one child who had a positive HIV polymerase chain reaction (PCR) test but was not started on ART as per the national guidelines. There was a misunderstanding among the clinical staff that this was not a definitive diagnosis for HIV and they needed to wait until a follow-up anti-body test was done. Recommendation: I-TECH mentors and ART focal person should review the Early Infant Diagnosis algorithm with all health care workers at the MCH and HIV clinic to ensure that all children with positive PCR begin ART as per the national guidelines. 6. Area for Improvement: Only a few of the ART patients are on 2nd line, which may indicate that clinical and immunological failure is being missed or not acted upon. Recommendation: With the support of I-TECH, Mentors should work with HCWs to build their capacity to identify clinical/immunological failure. I-TECH should develop a clear protocol for action to be taken once potential treatment failure is identified (e.g., adherence assessment, multi-disciplinary team (MDT) meeting, viral load, etc.). Consider using the patient-level data at the facility to flag patients with immunological failure. 7. Area for Improvement: There has been a shortage of ARV syrups for pediatrics. Recommendation: I-TECH, with the RHB, should identify all potential contributing factors to ARV supply shortages and develop strategies to address the issues that are within the hospital’s scope of influence. 8. Area for Improvement: The Chronic Care Clinic pharmacy had expired drugs on the shelves because staff thought they should wait until the stock review period before removing any drugs. Recommendation: I-TECH Mentors should work with the hospital management to develop a policy that will help avoid the possibility of dispensing expired drugs. The policy should state
Page65
that all expired drugs should be removed from the dispensing pharmacy as of the date of expiration. 9. Area for Improvement: A few viral load specimens have been transported to the Tigray Regional Referral Laboratory in Mekelle, however the specimen storage and transportation chain may not be maintaining specimen integrity. Recommendation: With the support of I-TECH, hospital management and the ART focal person should develop a protocol for specimen storage and transportation that assures valid and reliable results. Management 1. Area for Improvement: There are single staff persons filling the Data Entry and ACM positions and no formal options for coverage to take annual leave. Recommendation: The hospital and ART management with I-TECH should develop a succession plan for any position where there is a single staff person responsible for a program area. Adherence Case Management 2. Area for Improvement: Detailed notes from the ACM are included in the medical chart for clients identified as needing “Intensive” support, but not for those only receiving “Regular” support. Recommendation: ART program management should determine if there is any significant information in the ACM notes critical for the clinican to know. Develop policies to cover as needed. Measurement and Evaluation 3. Area for Improvement: The M&E data for the ART program is backed up on CD, but the hospital copy is kept in the desk drawer of the M&E office. Recommendation: The hospital backed-up copy should be kept with the Medical Director or Hospital CEO when their offices are in a different building.
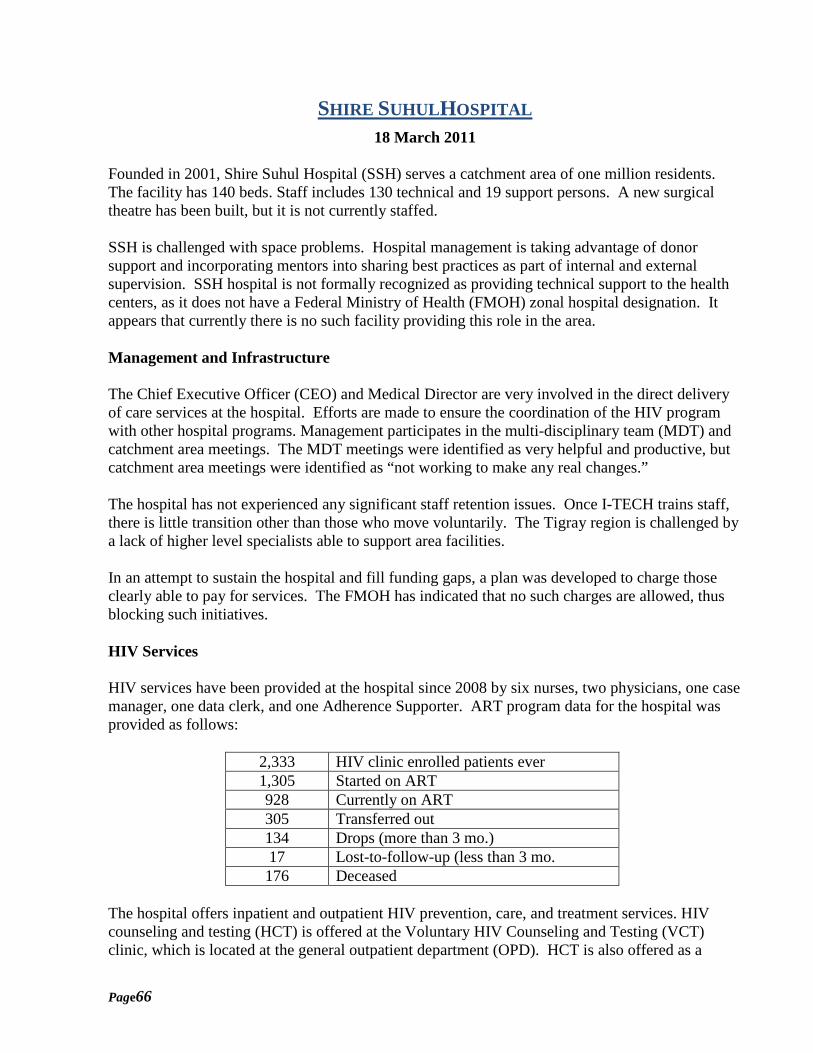
Page66
SHIRE SUHULHOSPITAL 18 March 2011
Founded in 2001, Shire Suhul Hospital (SSH) serves a catchment area of one million residents. The facility has 140 beds. Staff includes 130 technical and 19 support persons. A new surgical theatre has been built, but it is not currently staffed. SSH is challenged with space problems. Hospital management is taking advantage of donor support and incorporating mentors into sharing best practices as part of internal and external supervision. SSH hospital is not formally recognized as providing technical support to the health centers, as it does not have a Federal Ministry of Health (FMOH) zonal hospital designation. It appears that currently there is no such facility providing this role in the area. Management and Infrastructure The Chief Executive Officer (CEO) and Medical Director are very involved in the direct delivery of care services at the hospital. Efforts are made to ensure the coordination of the HIV program with other hospital programs. Management participates in the multi-disciplinary team (MDT) and catchment area meetings. The MDT meetings were identified as very helpful and productive, but catchment area meetings were identified as “not working to make any real changes.” The hospital has not experienced any significant staff retention issues. Once I-TECH trains staff, there is little transition other than those who move voluntarily. The Tigray region is challenged by a lack of higher level specialists able to support area facilities. In an attempt to sustain the hospital and fill funding gaps, a plan was developed to charge those clearly able to pay for services. The FMOH has indicated that no such charges are allowed, thus blocking such initiatives. HIV Services HIV services have been provided at the hospital since 2008 by six nurses, two physicians, one case manager, one data clerk, and one Adherence Supporter. ART program data for the hospital was provided as follows:
2,333 HIV clinic enrolled patients ever 1,305 Started on ART 928 Currently on ART 305 Transferred out 134 Drops (more than 3 mo.) 17 Lost-to-follow-up (less than 3 mo. 176 Deceased
The hospital offers inpatient and outpatient HIV prevention, care, and treatment services. HIV counseling and testing (HCT) is offered at the Voluntary HIV Counseling and Testing (VCT) clinic, which is located at the general outpatient department (OPD). HCT is also offered as a
Page67
routine service for all pregnant women and all patients with TB, and based on provider discretion in the general outpatient department and the inpatient wards. Once a patient tests positive they are only escorted to the HIV clinic if they are going to enroll at Shire. If not, they are referred to the facility of their choice directly from the testing point. Outpatient adult and pediatric HIV care and treatment are offered together at the HIV clinic, which is located in its own building. The HIV clinic is open Monday to Friday. All patients are seen by the HANS nurse for routine clinic appointments. For complex clinical issues the HANS nurse consults the general practitioners at the OPD or the internist. They rarely consult the I-TECH mentors except when the mentorship team is on site. The TB clinic is integrated with the HIV clinic. HIV care and treatment is not integrated with the mother-child health (MCH) clinic so relies on patient referrals and patients having dual appointments for the two services if they qualify for HAART. Sixty to seventy patients are seen each day in the ART clinic. The HIV clinic dispensing pharmacy is independent of the main hospital dispensing pharmacy. The pharmacy experiences periodic low stock levels of ARVs (currently inadequate supply of ARV syrups). The hospital has an integrated laboratory for HIV and non-HIV services, and has a FACS Count machine for CD4 enumeration. The hospital laboratory is able to conduct CD4 and hematocrit tests, but viral load tests must be sent to Mekelle. Patient Support Services Adherence Case Managers (ACM) were previously I-TECH employees. In 2010 the funds for these positions was sub-contracted to the RHB. It was apparent from the questions asked by the ACM that the transfer of the positions to the RHB had not been clearly explained and had not been put in writing by I-TECH to prevent misunderstandings. The ACMs and ASs report that adherence is a major problem for the patients. Many of the reasons shared with case managers are stigma, discontinuation of meds when well, transient, belief that holy water is better than medication, and lack of understanding of treatment failure. The Medical Director indicated that staffs need more training on how to better explain treatment failure with patients, co-infection of HIV and TB, and opportunistic infection treatment when there is not a consistent supply of medications. The ACM has no telephone or computer. Notes from patient discussions are kept manually by date. This means that there is no single source to find all counseling provided to a single patient over time. Recently, notes have been typed on the computer of the pharmacy technician. None of this documentation is kept in the medical chart if the patient is not identified as “Intensive.” Care plans are to be completed for all patients, but many were found to be blank or incomplete for the adherence sections. Four hundred forty-one (441) counseling sessions were conducted from April 2010 to February 2011. There were 244 patients counseled who were not enrolled in HIV care. The Adherence Supporters are employed by Save Generation Tigray, an association of people living with HIV/AIDS.
Page68
Monitoring and Evaluation Two Data Clerks and one Information Management specialist work at the hospital. The Data Clerk completes the registry and some of the registration forms. The Excel spreadsheets used at the sites for I-TECH data collection do not allow for an electronic quality assurance review. Access to the internet is through dial-up and is very slow. This phone line is the one expected to be used by the ACM to reach patients. Mentors visit once per month for 5 days. They have helped to develop new indicators, generate new reports to support them, assess data entered in the system, and how to use formulas to analyze data. Strengths:
• The CEO, Medical Director, and HIV ART focal person have a great working relationship,
open communication, and have responded to improve ART services. • Senior leadership of the hospital is actively involved in the MDT meetings and issue
solutions. • Multiple options are used to gather feedback from hospital staff on areas for improvements. • The ART program has strong linkages with the People Living with HIV association
bringing additional resources for the clients. • MDT meetings are being used to identify areas for improvement and develop action plans • Patients who refuse to enroll in HIV care after testing positive are linked with a physician
for additional discussion/counseling • There is effective task shifting of clinical care at the HIV clinic • The Adherence Case Manager has been with the program for two years. • Outreach/Adherence Supporters do a great job of educating, locating and reestablishing
links with patients who default Areas for Improvement and Recommendations: 1. Area for Improvement: Physicians at the hospital are available to the HIV clinic staff for consultation but play a minimal role in ongoing mentorship of the staff or in monitoring or overseeing the quality of the care provided. The responsibility of quality oversight is left to the I-TECH team. Recommendation: If staffing time allows, the hospital physicians should participate in monitoring the quality of care at the HIV clinic. This could be done through periodic chart reviews and observation of clinical encounters. 2. Area for Improvement: Although the hospital has a regular MDT meeting to address issues, they do not have a formal process for using patient/facility-level data to identify areas for improvement, guide solutions, and monitor the impact of efforts towards improvement. Recommendation(s): Hospital ART program staff should form a continuous quality improvement (CQI) team, and with support from I-TECH use facility data to conduct a formal CQI process.
Page69
3. Area for Improvement: The current space being used for VCT is not a confidential environment and has inadequate lighting. Recommendation: Hospital management with the ART program staff should reconsider the location for VCT. 4. Area for Improvement: Some of the HIV test kits currently being used were within a week of expiry. The health care workers at the testing points did not seem aware of this. Recommendation: The hospital laboratory management should develop and follow a protocol for monitoring the expiration date of HIV test kits, for communicating expiry information to users, and for recalling test kits for disposal by the date of expiry. 5. Area for Improvement: The hospital has adopted an “opt-out” policy for HIV counseling and testing, however the health care worker interviewed who is offering PITC at the out-patient department was using language consistent with “opt-in” testing. Recommendation: There was general agreement amongst hospital and I-TECH staff that they should and were using an opt-out approach to HIV testing, so the hospital team probably just needs to clarify the exact words to be used when presenting the test to the patient since subtle differences may affect test acceptance rates. 6. Area for Improvement: The HIV clinic health care workers do not routinely review each other’s charts or review the charts for patients who died. Recommendation: Peer chart reviews (where health care workers take a few charts seen by another health care worker that day, and review for any gaps in quality) and mortality reviews are potential ways to identify quality gaps and clinical systems that need strengthening, and clinical topics that require additional reinforcement. These processes can be used to generate issues for CQI and topics for Continuous Medical Education (CME) and case-based discussions. The hospital HIV clinic team should adopt a schedule for these activities, with support from I-TECH Ethiopia for guidelines and tools to assist. 7. Area for Improvement: Based on a review of patient files it was noted that growth charts are not being used consistently for pediatric patients. Recommendation: The HIV clinic team should ensure that growth charts should be incorporated into every pediatric file. The growth charts should be updated regularly and health care workers should pay attention to trends. Poor growth trends should be used for WHO staging as per the national guidelines. 8. Area for Improvement: CD4 was not consistently done every 6 months for the patient files reviewed, and was not consistently updated on the follow-up forms. Recommendation: Routine CD4 as per the national guidelines should be ordered by clinical staff and documented on the follow-up forms. Monitoring CD4 trends on the follow-up form is essential for identifying immunological treatment failure. 9. Area for Improvement: Only a few of the ART patients are on 2nd line, which may indicate that clinical and immunological failure is being missed or not acted upon. Recommendation: With the support of I-TECH, the hospital HIV clinical team should work with health care workers to build their capacity to identify clinical/immunological failure. They should develop a clear protocol for action to be taken once potential treatment failure is identified (adherence assessment, multi-disciplinary team (MDT) meeting, viral load). The HIV clinical team should consider implementing a viral load specimen transport system so patients can access this test at the Tigray
Page70
Regional Referral Laboratory in Mekelle. The HIV clinic team should consider using the patient-level data at the facility to flag patients with immunological failure. 10. Area for Improvement: Based on a review of the TB screening register, all patients at the HIV clinic are not consistently being screened for TB at every visit. Recommendation: TB is an important contributor to morbidity and mortality for patients with HIV. To identify TB early, clinical staff should screen every patient at every visit as per the national guidelines. 11. Area for Improvement: Of the total pediatric patients ever started on ART, less than 50% are currently active on ART. Recommendation: The HIV clinic team should review files from pediatric patients who have dropped out from ART to identify any systems issues that may be resulting in this high drop off rate. 12. Area for Improvement: Expired drugs were being stored in the HIV dispensing pharmacy. Expiration dates were not recorded on bin cards in the dispensing pharmacy and it was not clear if the central pharmacy database was being used to monitor the expiration of drugs at the dispensing pharmacy. Recommendations: To avoid the possibility of dispensing expired drugs, the pharmacy team should remove all expired drugs from the dispensing pharmacy before the date of expiry. The system for monitoring drug expiration at the dispensing pharmacy should be reviewed by the pharmacy team to ensure there is coordination/utilization of the central pharmacy database. 13. Area for Improvement: The laboratory did not have a fume hood for processing TB specimens. Recommendation: The hospital should procure a fume hood to reduce the risk of TB transmission to laboratory staff. 14. Area for Improvement: When internal quality control exercises showed a failed test there was no documentation of a repeat test being done the same day. Recommendation: The laboratory team should develop and implement a policy to guide action taken after a failed quality control cycle and documentation of action. 15. Area for Improvement: The HIV clinic team does not engage in CME sessions or formal case-based discussions except when the I-TECH team is on site. Recommendation: The facility could start an internal CME program to increase clinical expertise and knowledge. Topics could be generated from areas of concern identified during chart reviews.
16. Area for Improvement: The Family Matrix is expected to be completed for each patient on the first visit and updated on each following visit. This form was found in only one of 11 medical charts reviewed by the clinical team. Recommendation: The nurses and case manager should develop an immediate process to ensure forms are completed for all patients on their next visit. The ART program may want to consider making this a PDSA project. The tool should be used as a reminder to work with patients through the entire process of family member testing, which starts with disclosure. An individualized plan should be developed with each patient on how they will disclose, and strategies for having family members tested and enrolled into care. The tool should be kept in a promote location in the patient file (inside the front cover) to help staff remember to use it.
Page71
17. Area for Improvement: The FMOH case management guidelines expect the first level of follow-up for clients who have missed appointments to be a telephone call when an option. The ART clinic does not have a telephone that is available for the case manager use to conduct patient follow-up. Recommendation: The hospital with the Regional Health Bureau should determine how the minimum tools needed to perform the case manager duties can be provided. 18. Area for Improvement: The Outreach/Adherence Supporters are expected to conduct follow-up at clinics and hospitals where clients have transferred out. Many of these facilities will not speak with the staff because they have no form of identification validating their job. Recommendation: The Outreach/Adherence Supporters are employees of the persons living with HIV association. The hospital and ART program management should work with the organization to provide this basic tool for conducting their duties.
Page72
Wukro District Hospital 22 March 2011
Management Wukro Hospital was upgraded from a health center in 1993. The hospital serves for more than a half million population coming from six district areas seeing 50,000-60,000 patients per year. The facility provides outpatient comprehensive HIV/AIDS, inpatient (90 beds), laboratory, pharmacy, imaging, and emergency services. There are a total of 187 staff, with 98 technical, 3 physicians, 4 Health Officers (including 1 emergency surgeon), 3 BSC nurses, 2 Pharmacists, 4 Laboratory technologists, and 50 clinical nurses. Motivation activities (ceremonies, certificates, and experience sharing) have had significant impact on staff retention. HIV Services The hospital offers inpatient and outpatient HIV prevention, care, and treatment services. HIV counseling and testing (HCT) is offered at the Voluntary HIV Counseling and Testing (VCT) clinic, which is located near the HIV clinic. HCT is also offered as a routine service for all pregnant women and all patients with TB, and based on provider discretion in the general outpatient department (OPD) and the inpatient wards. There are 11 point of care testing sites throughout the hospital. Once a patient tests positive they are escorted to the HIV clinic for registration or they are referred to another facility of their choice. Outpatient adult and pediatric HIV care and treatment are offered together at the chronic care block (separate from the general OPD), which is open Monday to Friday. Routine adult pre-ART and ART patients are seen by the HANS or BSc nurse, Pediatric patients (including HIV-exposed infants) are seen by the HANS. The health officer (HO) sees all new patients and patients initiating ARVs, and takes consultations from the HANS and BSc nurse. The Health Officer consults the I-TECH mentors or the hospital physicians for complex cases. HIV care and treatment is not integrated with other services (mother-child health (MCH) clinic, TB clinic) so relies on patient referrals and patients having multiple appointments for the different services. The HIV medical records are integrated with the general hospital medical records. The hospital has an integrated laboratory for HIV and non-HIV services, and has a FACS Count machine for CD4 enumeration. They experience inconsistent supply of reagents and controls (currently there is a shortage of hematology controls). The partners and children of patients already enrolled in HIV care are at high-risk for HIV so family member testing is a critical entry point for identifying people infected with HIV and is an important opportunity for reinforcing prevention messages for those that are negative. The Family Matrix tool has a high potential for facilitating this process. The tool should be kept in a promote location in the patient file (inside the front cover) to help staff remember to use it.
Page73
Strengths:
• There has been a successful transition from a health center to a hospital. • The Medical Director provides oversight of the ART program and is involved in hospital
CQI. • There are hospital-wide CQI efforts that include the ART program. • Hand-washing stations have been implemented throughout the facility. • The hospital has made major improvements to facility infrastructure and patient flow, and
has documented improvements in patient satisfaction. • MDT meetings are being used to identify areas for improvement and develop action plans. • The uptake of HIV testing at MCH, the TB clinic, and amongst patients with STIs is
excellent. • The HIV medical records are integrated with the main hospital card room. • The HIV clinic team meets daily to discuss and address areas of concern. • Patients receive their CD4 results on the same day as the sample is drawn. • Retention of pediatrics on ART is excellent. • Based on review of the TB screening register it appears nearly all patients attending the
HIV clinic are being screened for TB at every visit. • The laboratory has excellent results for CD4 and hematology EQA. • The laboratory supports CD4 specimen networking from 4 other health facilities. • The Pharmacy store and the dispensary are models of excellence for other facilities.
Areas for Improvement and Recommendations: 1. Area for Improvement: Care plans are not documenting all intensive adherence encounters. All appropriate areas for which the patient received counseling did not appear to be documented. Recommendation: The I-TECH case management mentor should develop a chart review for use on each visit 2. Area for Improvement: The Family Matrix is expected to be completed for each patient on the first visit and updated on each following visit. The Family Matrix tool was not in the majority of patient files reviewed and is not being fully utilized by health care workers. Case managers are only completing the form for ART patients with a wife or husband or child. This limited use of the matrix is not consistent with the FMOH guidelines and is reducing identification of “at risk” partners. Matrix forms have no space for a date or signature of the person completing it. Recommendation: Adherence case managers and health care workers need to ensure the tool is used for all patients at enrollment and that it is referred to and updated at every visit until all family members at risk have been tested and those who are positive have been enrolled into care. The tool should be kept in a promote location in the patient file (e.g. inside the front cover) to help staff remember to use it. The tool should also be used as a reminder to work with patients through the entire process of family member testing, which starts with disclosure. An individualized plan should be developed with each patient on how they will disclose, and strategies for having family members tested and enrolled into care. a. The nurses and case manager should develop an immediate process to ensure forms are completed for all patients on their next visit. The ART program may want to consider making this a PDSA project. b. Consider adding identifying information on the person completing the form and the date(s) of completion.
Page74
3. Area for Improvement: The hospital is not maximizing use of the FMOH resources to help find patients outside of the catchment area who have missed appointments or are lost to follow-up. Recommendation: I-TECH Ethiopia should work with CDC-Ethiopia and the FMOH to determine how the Health Extension workers can be used to extend the lost-to follow-up reach. 4. Area for Improvement: Physicians at the hospital are available to the HIV clinic staff for consultation but play a minimal role in ongoing mentorship of the staff overseeing or the quality of the care provided. The responsibility of quality oversight is left to the I-TECH team. Recommendation: If staffing time allows, the hospital physicians should participate in monitoring the quality of care at the HIV clinic. This could be done through periodic chart reviews and observation of clinical encounters. 5. Area for Improvement: The HIV clinic health care workers do not routinely review each other’s charts or review the charts for patients who died. Recommendation(s): Peer chart reviews (where health care workers take a few charts seen by another health care worker that day, and review for any gaps in quality) and mortality reviews are potential ways to identify quality gaps and clinical systems that need strengthening, and clinical topics that require additional reinforcement. These processes can be used to generate issues for CQI and topics for Continuous Medical Education (CME) and case-based discussions. The hospital HIV clinic team should adopt a schedule for these activities, with support from I-TECH Ethiopia for guidelines and tools to assist. 6. Area for Improvement: The HIV clinic team does not engage in CME sessions or formal case-based discussions except when the I-TECH team is on site. Recommendation: The facility could start an internal CME program to increase clinical expertise and knowledge. Topics could be generated from areas of concern identified during chart reviews. 7. Area for Improvement: The VCT session includes routine TB screening; however the VCT counselor did not have a job aid available to ensure standardization of the TB screening process. Recommendation: The hospital should place a TB screening job aid in the VCT room. 8. Area for Improvement: Approximately 40% of patients who test positive at VCT choose to enroll into HIV care at a health facility other than Wukro Hospital, yet there is not a formalized process for tracking the success of referrals or documenting the process. Recommendation: The HIV clinic team and VCT counselors should develop a system for tracking referrals to other health facilities. 9. Area for Improvement: The patient file does not have any paper allowing for documentation of clinical issues. Recommendation: The HIV clinic team should add additional sheets of paper to the patient file (such as the out-patient progress/history sheet) so that clinical issues and decision-making processes beyond routine follow-up can be documented for future reference by other health care workers. 10. Area for Improvement: Only a few of the ART patients are on 2nd line, which may indicate that clinical and immunological failure is being missed or not acted upon. Recommendation(s): With the support of I-TECH, the HIV clinic teams should work with health care workers to build
Page75
their capacity to identify clinical/immunological failure. They should develop a clear protocol for action to be taken once potential treatment failure is identified (adherence assessment, multi-disciplinary team (MDT) meeting, viral load). They should consider implementing a viral load specimen transport system so patients can access this test at the Tigray Regional Referral Laboratory in Mekelle (currently patients are being sent for viral load, instead of transporting samples). They should consider using the patient-level data at the facility to flag patients with immunological failure. 11. Area for Improvement: The laboratory does not have diagnostic testing for cryptococcal meningitis, such as India ink staining of cerebrospinal fluid, or serum cryptococcal antigen testing. Recommendation: Cryptococcal meningitis is reportedly a significant contributor to morbidity and mortality among patients with HIV in Ethiopia. Although not yet a required test in the national guidelines, if resources allow I-TECH Ethiopia should assist in increasing laboratory capacity to aid in this diagnosis. 12. Area for Improvement: Internal quality control (IQC) for point-of-care HIV testing in the hospital is very intensive, occurring 2-3 times per week. Recommendation: The hospital could adopt an adequate but less intensive schedule for IQC of HIV testing, such as monthly or quarterly. 13. Area for Improvement: External quality assurance (EQA) has not yet been initiated for AFB smears or HIV antibody testing. Recommendation: The hospital laboratory team should work with the I-TECH laboratory mentor to join an EQA program for these investigations.
Page76
MEKELLE REGIONAL REFERRAL HOSPITAL 21 March 2011
Mekelle Regional Hospital has been providing PEPFAR funded HIV services for the last six years. The facility has 180 beds and services are provided by seven specialists, four general practitioners, eighty-three nurses, eight health officers, and twelve midwives. The hospital provides the second largest number of club feet surgeries in the country. New equipment has also been purchased to upgrade the quality of services. As part of the upgrade, 25 cleaners were hired on a contractual basis to improve the infection control while head nurses conduct hand-washing and other sanitation education sessions during each shift. The hospital is a training center for radiographers. Health education media technology has been added to the wards to help improve patient education. Patient record management has also been upgraded. A new client satisfaction process has been implemented and 95% of the respondents in the last six months have expressed the hospital is meeting its objectives. The hospital’s greatest challenges are the loss of revenue by having so many services restricted by the FMOH as “waived.” There is no pharmacy store, poor sewage, an x-ray machine that is almost 20 years old and costs more to fix than replace, and a shortage of diagnostic equipment. The hospital is clearly used as a referral option by every other level of facility. Many patients bypass going to the health centers and health posts and come directly to Mekelle without waiting for a referral in the region, but are also sent referrals from Afar and Tigray regions. Organization and Program Management Hospital management has been instrumental in securing facility renovations for the surgical theatre, labor and delivery wards and laboratory. The hospital is accountable to the Regional Health Bureau (RHB) and receives supportive supervision visits twice per year. The hospital management is not always included in planning activities at the regional level that will impact the use of staff and funds at the facility. One of the hospitals greatest challenges is not being able to move funds from prevention to care delivery. The CEO facilitates the monthly MDT and quarterly catchment area meetings. Issues that continue to arise at the meetings with no resolution to date include maintenance of laboratory equipment, empowerment and funding for the health centers, funds to better support the Adherence Supporters and Outreach workers, and support to help patients who are missing appointments due to transportation issues. The hospital created a new space for the HIV services that includes TB and pharmacy next door. The case manager offices are in the back of the hospital. The ART focal person has partitioned some of a second waiting area for the case managers to meet with clients in the clinic area. This is a great temporary option, but there is no privacy to ensure that discussions cannot be heard by those in the first and second waiting rooms. There is also a third waiting room designated for coughing patients or those known to have TB and has no ventilation. There are four examinations rooms to be used by six clinicians.
Page77
HIV Services ART services have been decentralized from the hospital to make use of the health centers. Approximately 3,000 patients have been referred from the hospital to these facilities. The hospital offers inpatient and outpatient HIV prevention, care, and treatment services. HIV counseling and testing (HCT) is offered at the Voluntary HIV Counseling and Testing (VCT) clinic, which is located at the HIV/chronic care clinic. HCT is also offered as a routine service (utilizing an opt-out approach to assure patients the opportunity to decline) for all pregnant women, all patients with TB, and all patients seen in general outpatient department and the inpatient wards. Once a patient tests positive they are escorted to the HIV clinic for registration or referral to another facility, and they always see the case manager for counseling before being referred out. Outpatient adult and pediatric HIV care and treatment are offered together at the HIV clinic, which is located next to the chronic care clinic. The HIV clinic is open Monday to Friday. All pre-ART patients are seen by the health officer (HO) or BSc nurse. All pediatric patients are seen by the BSc nurse. Other patients are seen by the HANS for routine clinic appointments, and then by the HO or BSc nurse if it is a new patient (for WHO staging and physical exam), for initiation of ARVs, or for any clinical complaints. For complex clinical issues the HANS consult the HO or a BSc nurse, who in turn usually consults the I-TECH mentors when they have questions (the general practitioners at the hospital are usually very busy at the OPD, and the hospital does not have a pediatrician or internist). HIV care and treatment is not integrated with other services (mother-child health (MCH) clinic, TB clinic) so relies on patient referrals and patients having multiple appointments for the different services. The HIV clinic dispensing pharmacy is independent of the main hospital dispensing pharmacy. The hospital has an integrated laboratory for HIV and non-HIV services, with a FACS Caliber machine for CD4 enumeration and a FACS Count for back-up. They do not receive controls for the FACS Caliber machine, and experience slow response time for equipment repairs. Patient Support Services Referral forms are used to identify existing patients needing adherence support services. Care plans are completed for all patients referred for this service and progress forms are filled out only for those identified as “Intensive.” ACMs and ASs conduct verification visits to agencies when a patient indicates they have transferred out of care. This has posed a challenge for some of the ASs who do not have an identification card. ACMs serve as the supervisors for the ASs and Outreach workers and conduct outreach activities with them at least twice per month. Every Friday the ACMs, ASs, and outreach workers meet to discuss challenges and areas for improvement. ACMs face problems being able to make telephone calls to locate patients when this is the same telephone used for the data staff to access the internet. ACMs at this site also conduct health education on a daily basis in the waiting room. These presentations are often the way for ACMs to show the mentors they have learned and understood some new information shared with them. The ASs are employees of Safe Generation, an organization for people living with HIV in the region that receives funds from I-TECH. The case managers serve as the “on-site” supervisors. Outreach workers identified that they are following up on patients who have not been to the
Page78
hospital for services in the last 4-5 years. Most have moved and the staff wondered about the logic of allocating resources in this area. Monitoring and Evaluation The ART program is supported by two Data Entry Clerks and two Information Technicians. This office serves as the HMIS for the ART program and for the hospital. Data cleaning processes are completed monthly. Monthly, the data is presented at the ART meetings and quarterly to the entire hospital. Data quality is a key concern at this site since the actual charts are never used to enter or verify data. Data Clerks manually copy information from the chart onto a spreadsheet that is used to enter data into the Johns Hopkins data base. When data quality reviews are conducted, they rely on the spreadsheets making the assumption that initial information transfer was correct. Staff experience delays in getting data reports completed. Particularly when they are waiting on software updates for the system. There is no training provided to staff on the updates also resulting in delays as staff must learn on their own the differences. Back-up of the data system is made to a CD twice per week and stored in a locked cabinet in the same office. Strengths:
• Senior hospital leadership provides significant support to the ART program. • Hospital has under taken diverse options to raise funds to support programs and services. • Several new strategies are being implemented to help with staff retention. • MDT meetings are being used to identify areas for improvement and develop action plans. • The hospital has introduced an innovative “mini media” program to teach in-patients about
use of latrines and the importance of hand washing. • There is an established link with Mekelle University for training of staff and sharing certain
resources. • Uptake of HIV testing is excellent through-out the hospital. • VCT services and the HIV outpatient clinic are accessible with a Saturday clinic every
week. • Based on review of the TB screening register it appears nearly all patients attending the
HIV clinic are being screened for TB at every visit. • Patients have access to free cervical cancer screening using the visual inspection with
acetic acid method. • Patients receive their CD4 results on the same day as the sample is drawn. • The HIV clinic has a routine process for clinical case discussions and the HANS focal
person does a peer review of other clinicians’ charts. • There is a functional FACS Caliber machine for CD4 enumeration, with a FACS Count
machine for back-up. • Client satisfaction surveys have been implemented hospital wide and data is used in the
hospital CQI. • The hospital and ART program have strong linkages with support organizations in the city.
Page79
• Formal MOUs exist with a local family planning organization and one working with children with club feet.
Areas for Improvement and Recommendations: HIV Services
1. Area for Improvement: Physicians at the hospital are not currently involved in the HIV outpatient services, for consultations, ongoing mentorship of the staff, or monitoring/overseeing the quality of the care provided. The responsibility of quality oversight is left to the I-TECH team. Recommendation: If staffing time allows, the hospital physicians should be available for clinical consultations and participate in monitoring the quality of care at the HIV clinic. This could be done through periodic chart reviews and observation of clinical encounters. 2. Area for Improvement: Although the hospital has a regular MDT meeting to address issues, and are using some facility-level data to monitor improvements (such as waiting times and patient satisfaction), this process has not been implemented specifically for the HIV services. Recommendation: The HIV clinic team should form a continuous quality improvement (CQI) team, and with support from I-TECH use facility data for a formal CQI process for the quality of HIV services. 3. Area for Improvement: The hospital has adopted an “opt-out” policy for HIV counseling and testing, however the health care worker interviewed who is offering Provider-Initiated HIV Testing and Counseling (PITC) at the out-patient department was using language consistent with “opt-in” testing. Recommendation: There was general agreement amongst hospital and I-TECH staff that they should and were using an opt-out approach to HIV testing, so the hospital team probably just needs to clarify the exact words to be used when presenting the test to the patient since subtle differences may affect test acceptance rates. 4. Area for Improvement: The HIV clinic health care workers do not routinely review each other’s charts (other than the HANS focal person) or review the charts for patients who died. Recommendation: Peer chart reviews (where health care workers take a few charts seen by another health care worker that day, and review for any gaps in quality) and mortality reviews are potential ways to identify quality gaps and clinical systems that need strengthening, and clinical topics that require additional reinforcement. These processes can be used to generate issues for CQI and topics for Continuous Medical Education (CME) and case-based discussions. The hospital HIV clinic team should adopt a schedule for these activities, with support from I-TECH Ethiopia for guidelines and tools to assist. 5. Area for Improvement: The HIV clinic team does not engage in CME sessions and rarely have formal case-based discussions except when the I-TECH team is on site. Recommendation: The facility could start an internal CME program to increase clinical expertise and knowledge. Topics could be generated from areas of concern identified during chart reviews. 6. Area for Improvement: Frequency of patient appointments does not seem to be based on a standardized protocol. Recommendation: The HIV clinic team should develop and implement
Page80
clear criteria for determining the frequency of appointment visits, which will then reduce workload. 7. Area for Improvement: The waiting area for coughing patients (also the VCT waiting area) is poorly ventilated. Recommendation: The hospital management should ensure that coughing patients wait in a well-ventilated waiting area away from other patients. 8. Area for Improvement: Based on a review of patient files it was noted that growth charts have recently been incorporated into pediatric patient files, but are not consistently being used to document trends and for WHO staging. Recommendation(s): The growth charts should be updated regularly by clinical staff to monitor trends. Poor growth trends should be used for WHO staging as per the national guidelines. 9. Area for Improvement: Based on a review of patient files and on the number of patients currently on 2nd line, it appears that clinical and immunological failure is being missed or not acted upon. Recommendation(s): With the support of I-TECH, the HIV clinic teams should work with health care workers to build their capacity to identify clinical/immunological failure. They should develop a clear protocol for action to be taken once potential treatment failure is identified (eg adherence assessment, multi-disciplinary team (MDT) meeting, viral load, etc). They should consider implementing a viral load specimen transport system so patients can access this test at the Tigray Regional Referral Laboratory in Mekelle (with the specimen being sent rather than the patient traveling to the referral lab). They should consider using the patient-level data at the facility to flag patients with immunological failure. 10. Area for Improvement: Physical exam areas for improvements were not routinely documented on the intake forms. Recommendation: The clinical staff should perform a complete physical exam on all newly enrolling patients, and document this on the intake form. 11. Area for Improvement: Expired drugs were being stored in the HIV dispensing pharmacy. Some drugs did not have legible expiry dates because of water damage and we did not see bin cards in use at the dispensing pharmacy and the database on site did not contain expiry information. The HIV dispensing pharmacy was crowded and not optimally organized for the work flow. Recommendation: To avoid the possibility of dispensing expired drugs, the pharmacy team should remove all expired drugs from the dispensing pharmacy before the date of expiry. The system for monitoring drug expiration at the dispensing pharmacy should be reviewed by the pharmacy team to ensure that expired drugs are identified and removed in a timely manner. The pharmacy team should improve the organization of the pharmacy to create more usable space for working. 12. Area for Improvement: The water distillation machine is not functioning. Recommendation: The hospital should do a cost-analysis to see if repairing the machine will result in a cost savings from not having to purchase distilled water. 13. Area for Improvement: The laboratory does not have diagnostic testing for cryptococcal meningitis, such as India ink staining of cerebrospinal fluid, or serum cryptococcal antigen testing. Recommendation: Cryptococcal meningitis is reportedly a significant contributor to morbidity
Page81
and mortality among patients with HIV in Ethiopia, so if resources allow I-TECH Ethiopia should assist in increasing laboratory capacity to aid in this diagnosis. 14. Area for Improvement: The laboratory is using the FACS Count machine to validate results from the FACS Caliber instead of running controls for the FACS Caliber, because of shortage of controls. Recommendation(s): The hospital laboratory team should work with EHNRI to access FACS Caliber controls. Measurement and Evaluation/HMIS 15 Area for Improvement: Back-ups for the M&E/SI and the hospital HMIS data is maintained in the same office providing limited protection of information. Recommendation: The M&E team should identify an option to store the CD back-ups in the Medical Director or CEO office in another building. Adherence Case Management 16. Area for Improvement: The Family Matrix tool was not completed or updated in the majority of patient files reviewed and is not being fully utilized by health care workers. The Family Matrix is only being used to capture the primary patients “legal” family (children, wife/husband). Girlfriends/boyfriends and partners are not being identified to determine if counseling and testing is needed. Recommendation(s): Mentors and ART program staff should review the language of the FMOH case management guidelines and modify use of the matrix to maximize all opportunities to identify persons with HIV. Adherence case managers and health care workers need to ensure the tool is used for all patients at enrolment and that it is referred to and updated at every visit until all family members at risk have been tested and those who are positive have been enrolled into care. The tool should be used as a reminder to work with patients through the entire process of family member testing, which starts with disclosure. An individualized plan should be developed with each patient on how they will disclose, and strategies for having family members tested and enrolled into care. The tool should be kept in a promote location in the patient file (e.g. inside the front cover) to help staff remember to use it. Facility 17. Area for Improvement: The second and third waiting rooms have limited ventilation. Adherence Case Managers see patients in the second room and TB patients or those with coughs wait in the third room. Recommendation: The hospital management should determine if the windows in the rooms can be opened. 18. Area for Improvement: Two clinical providers are sharing a single room restricting the ability to do physical exams with patients and reducing patient confidentiality. Recommendation: When additional space is available, the hospital management should ensure that each provider should have a separate area in which to see patients. 19. Area for Improvement: Poor sanitation in several areas being used by staff and clients could be creating infection control issues, particularly for ART patients. Recommendation: Hospital management and I-TECH infection prevention mentors should conduct visual reviews of
Page82
all locations that may be used by ART and other patients on a monthly basis to identify locations where additional cleaning and sanitation is needed. 20. Area for Improvement: The ART card room (which is separate from the central medical record unit) is locked in the evenings and weekends. This prevents hospital physicians from accessing patient medical records information if they come for emergency services during this time. Recommendation: The hospital management should consider integrating the HIV clinic patient records with the central medical records unit, which is open 24 hours every day. An interim solution could be to make a key to the ART patient files available to the medical director in the evenings and Sunday while changes are being made to the hospital card room that will allow both sets of charts to be combined. Adherence Supporters/Outreach Workers 21. Area for Improvement: The hospital is not maximizing use of the FMOH resources to help find patients outside of the catchment area who have missed appointments or are lost to follow-up. Recommendation: I-TECH Ethiopia should work with CDC-Ethiopia and the FMOH to determine how the Health Extension workers can be used to extend the lost-to follow-up reach.
Page83
MEKELLE UNIVERSITY COLLEGE OF HEALTH SCIENCES AYDER HOSPITAL HIV CARE & TREATMENT CENTRE
23 March 2011 The Ayder Hospital HIV Care and Treatment Centre was assessed briefly by one clinical reviewer while the rest of the team was at the Regional Health Bureau. The HIV Care and Treatment Centre has been operating for approximately two years, with I-TECH support for the past year. Five hundred and twenty-six patients have ever been enrolled (31 pediatric), and 287 ever started on highly active antiretroviral therapy (HAART), (19 pediatric) while 237 are currently on HAART (12 pediatric). Clinical Overview The university hospital offers inpatient and outpatient HIV prevention, care, and treatment services. HIV counseling and testing (HCT) is offered at the Voluntary HIV Counseling and Testing (VCT) clinic, which is located at the HIV clinic. HCT is also offered based on provider discretion in TB clinic, mother-child health (MCH) clinic, the general outpatient department (OPD), and the inpatient wards. Once a patient tests positive they are escorted to the HIV clinic for registration or referral to another facility. Outpatient adult and pediatric HIV care and treatment are offered together at the HIV clinic, which is located in a separate wing of the hospital. The HIV clinic is open Monday to Friday. All patients see the HANS or BSc nurse for routine clinical care. For complex clinical issues they call a hospital internist or pediatrician who comes to see the patient at the HIV clinic. If the internist/pediatrician is not available then they escort the patient to the OPD to be seen by a general practitioner. They rarely consult the I-TECH mentors except when the mentorship team is on site. HIV care and treatment is not integrated with other services (mother-child health (MCH) clinic, TB clinic) so relies on patient referrals and patients having multiple appointments for the different services. The HIV clinic dispensing pharmacy is independent of the main hospital dispensing pharmacy. The hospital has an integrated laboratory for HIV and non-HIV services. They experience inconsistent supply of reagents and slow response time for equipment repairs. Strengths
• An internist and pediatrician are available for clinical consultations at the HIV clinic. • The medical records for the HIV clinic are integrated with the general hospital record/card
room. • Clinical issues are documented on a separate piece of paper in the patient records (a history
sheet). • The laboratory for HIV services is integrated with the general hospital laboratory. • HIV viral load testing is available at the Regional Referral Laboratory which is on the
hospital grounds.
Page84
Areas for Improvement and Recommendations: 1. Area for Improvement: Physicians at the hospital are available to the HIV clinic staff for consultation but play a minimal role in ongoing mentorship of the staff or in monitoring the quality of the care provided. The responsibility of quality oversight is left to the I-TECH team. Recommendation: The University’s College of Health Sciences has expressed interest in taking on some of the mentorship responsibilities that I-TECH’s field based teams are currently doing. Taking on more responsibility for mentorship and oversight of the quality of care at their own HIV clinic would be a method of demonstrating this interest and capacity. 2. Area for Improvement: Uptake of testing at all entry points is low (MCH, only 83% tested; TB clinic, only 81% tested; pediatric ward, only 50% offered a test with only 55% acceptance; adult out-patient department, only 50% offered a test with only 33% acceptance). Recommendation: Hospital service delivery points are a key opportunity for identifying patients with HIV and enrolling them into care. The hospital should consider implementing universal PITC for all patients with a hospital encounter using an opt-out approach. At a minimum, the MCH and TB clinics need to urgently identify strategies to improve uptake of HIV testing. 3. Area for Improvement: There is no computer available for the data clerk at the HIV clinic, so no database or electronic medical records are being maintained. Recommendation: The hospital management or I-TECH Ethiopia should avail equipment for an electronic record in order to make reporting easier and provide data for CQI. 4. Area for Improvement: The HIV clinic health care workers do not routinely review each other’s charts or review the charts for patients who died. Recommendation(s): Peer chart reviews (where health care workers take a few charts seen by another health care worker that day, and review for any gaps in quality) and mortality reviews are potential ways to identify quality gaps and clinical systems that need strengthening, and clinical topics that require additional reinforcement. These processes can be used to generate issues for CQI and topics for Continuous Medical Education (CME) and case-based discussions. The hospital HIV clinic team should adopt a schedule for these activities, with support from I-TECH Ethiopia for guidelines and tools to assist. 5. Area for Improvement: The HIV clinic team does not engage in CME sessions or formal case-based discussions except when the I-TECH team is on site. Recommendation: The facility could start an internal CME program to increase clinical expertise and knowledge. Topics could be generated from areas of concern identified during chart reviews. 6. Area for Improvement: From a limited chart review and interview with health care workers at the site, it does not seem like the Family Matrix tool is being fully utilized by health care workers or updated regularly. Recommendation(s): The partners and children of patients already enrolled in HIV care are at high-risk for HIV so family member testing is a critical entry point for identifying people infected with HIV and is an important opportunity for reinforcing prevention messages for those that are negative. The Family Matrix tool has a high potential for facilitating this process. Adherence case managers and health care workers need to ensure the tool is used for all patients at enrolment and that it is referred to and updated at every visit until all family members at risk have been tested and those who are positive have been enrolled into care.
Page85
The tool should be used as a reminder to work with patients through the entire process of family member testing, which starts with disclosure. An individualized plan should be developed with each patient on how they will disclose, and strategies for having family members tested and enrolled into care. The tool should be kept in a promote location in the patient file (e.g. inside the front cover) to help staff remember to use it. 7. Area for Improvement: Only 2% of the ART patients are on 2nd line, which may indicate that clinical and immunological failure is being missed or not acted upon. Recommendation(s): With the support of I-TECH, the HIV clinic team should work with health care workers to build their capacity to identify clinical/immunological failure. They should develop a clear protocol for action to be taken once potential treatment failure is identified (e.g. adherence assessment, multi-disciplinary team (MDT) meeting, viral load). 8. Area for Improvement: Family planning services are only available to patients at the HIV clinic through referral to the OB/GYN clinic. Recommendation: The hospital management should consider training staff at the HIV clinic on family planning, and avail the necessary commodities so that patients can access family planning without moving to a different service delivery point in the hospital. 9. Area for Improvement: Staff report screening all patients for TB at every visit but they are not using the standard TB screening register/log-book. Recommendation: Documentation of TB screening will make it easier to verify that this is being done as per the national guidelines, and will reinforce the importance of TB screening for patients with HIV. The HIV clinic team should use a standardized register for documenting routine TB screening. 10. Area for Improvement: As a university hospital there will be an expectation that the HIV clinic is a centre of excellence with the capacity to manage the most complex patients in the region. It is not currently functioning in that capacity, and is not currently receiving the technical oversight from faculty members to raise it to that level. Recommendation(s): A vision for the HIV clinic’s role as a university hospital clinic and referral site needs to be developed by the hospital management and resources identified to meet that vision. If there is a clear capacity building plan and faculty commitment, the hospital HIV clinic could potentially offload complicated patients from the Mekelle Regional Hospital HIV clinic and be a teaching centre for advanced HIV care. Learners could rotate to other facilities for exposure to routine HIV care.
Page86
TIGRAY REGIONAL HEALTH BUREAU 23 March 2011
Strengths:
• Case team specifically designated to provide supportive supervision for ART programs. • Health extension workers posted in rural communities to help facilitate locating patients
with missed appointments and lost-to-follow-up near health centers and health posts (outside of the hospital catchment area).
• RHB Director and Case teams have identified areas of need to facilitate future transition options.
• Many of the site supportive supervision and program monitoring is done collaboratively with donor partners in the region.
• RHB staff is active participants in the catchment Area meetings.
Areas for Improvement and Recommendations: Patient Tracking 1. Area for Improvement: Many hospitals in the region do not appear to be using the Health Extension Coordinator and workers to facilitate tracking patients outside of the catchment area. Recommendation: Case team members should use the catchment Area meetings to share resources and improve these linkage relationships. Measurement and Evaluation
2. Area for Improvement: The M&E staff at the RHB office are 100% I-TECH funded. The RHB has not picked up any portion of these staff salaries to take ownership of the information management processes and data analysis. Recommendation: The RHB should determine the time frame for beginning to transition some of the M&E I-TECH staff. In preparation for this, the RHB should also assess what resources will be needed to fully accommodate the needs of these staff. Supportive Supervision and Program Monitoring 3. Area for Improvement: The Case team does not have access to the basic resources needed to conduct their responsibilities on behalf of the RHB. Recommendation: The RHB management with the FMOH should determine how transportation can be a minimum tool available to support the team to visit sites where I-TECH nor MSH are providing capacity building.
Page87
TIGRAY REGIONAL REFERRAL LABORATORY 23 March 2011
The assessment team briefly visited the Referral Laboratory as part of our visit to the University Hospital. The laboratory is in the early stages of working towards WHO accreditation. The Polymerase Chain Reaction (PCR) laboratory is funded by PEPFAR for Early Infant Diagnosis of HIV. It currently has the capacity to run 60 PCR samples per week, operating at 3 days per week (the shared extraction/amplification room is used 2 days per week for running HIV viral load samples). The PCR laboratory has gone through four EQA cycles with samples sent from CDC-Atlanta and passed at 100%. The laboratory has been running HIV viral load tests for approximately 2 months, and has processed 72 samples by the time of this visit. They have the capacity to run 36 samples per week operating 2 days per week (sharing the extraction/amplification room for PCR processing on the other days). The lower limit for detection is 75 viral copies per ml. They have not yet started EQA for viral load.
Page88
Appendices
Page89
APPENDIX 1: CLASS VISIT PARTICIPANTS HRSA ClASS Team 1 Members
1. John Oguntomilade, HRSA Team Leader 2. Angel R. Braña, MD, MPH, Clinical Consultant
HRSA ClASS Team 2 Members
1. Laura Cheever, MD, HAB Deputy Associate Director 2. Philippe Chiliade, MD, Medical Officer and Track 1 Lead 3. Juanita Farrow, MSA, Financial Reviewer 4. Cheryl Nesbitt, Administrative Reviewer 5. Jeremy Penner, MD Clinical Reviewer
Centers for Disease Control and Prevention - Ethiopia
1. Abubaker Bedir, Program Manager 2. Demmelash Birhanu, Cooperative Agreement Specialist 3. Ribka Fantu, Project Coordinator for TB/HIV 4. Julie Jenks, PMG Advisor 5. Getahundt Sisay, Project Coordinator 6. Seymour Williams, Care and Treatment Associate Director
I-TECH-Seattle Headquarters
1. Thomas Heller, Senior Clinical Advisor 2. Wesen Kifetew, Program Manager
I-TECH Ethiopia
1. Girma Abraham, Clinical Team Lead 2. Hamza Adus, Training Director 3. Ishmael Ahmed, Case Management Coordinator 4. Firkte Assaye, Case Management & Infection Prevention Mentor 5. Teklu Belay, MD, Regional Programs Director 6. Tadale Birhanu, Information Mentor 7. Meheret Elias, Care and Support Advisor 8. Getachu Feleke, MD, Clinical Director 9. Nega Gebreyesus, Deputy Country Director 10. Samson Getachew, Regional Laboratory Coordinator 11. Adhanom Girmay, Regional Manager 12. William Graham, Country Director 13. Hirut Haile, Field Based Nurse 14. Murida Kemal, Senior Program Manager
Page90
15. Kidanu Lilay, Data Clerk 16. Dr. Wubshet Mamo, Laboratory Director 17. Shimels Negash, Nurse Mentor and Team Lead 18. Manuel Kassaye Sebhatu, MD; Care and Treatment Director 19. Fidaku Shumi, Case Management and Infection Prevention Mentor 20. Kibrom Tadesse, Case Management & Infection Prevention Mentor 21. Adunga Tafa, Operations Manager 22. Yonas Taffesse, M&E Director 23. Asfaw Tesaye, Human Resources Director 24. Eskinder Tesfaya, Senior Clinical Care and Treatment Advisor 25. Ayele Tiyou, Monitoring and Evaluation Officer
Adwa Hospital
1. Dr. Gottom Gigar, CEO 2. Dr. Ataklti Tsegay, Medical Director 3. GebretsadikTsegay, Pharmacy Head 4. Tihut Bekele, ART Focal Person 5. Sister Rahel Hagos, TB Clinic Focal Person 6. Dr. Temesoen Asoedom, Gynecologic Department Head 7. Afera Meresa, Team Head 8. Marta Kenday, Case Manager 9. Abret Abseyed, Adherence Supporter 10. TirhasTeklu, ART staff 11. Ataklti Haills, Laboratory Focal Person 12. Gemet Aregano, Pediatric Focal Person 13. Trihas Odesta, Department Head 14. Seite Zeslasie, Pharmacy 15. Atalelti Welay, HMIS 16. Ferewasu Fetuw, PMTCT 17. Dr. Kitiom Tsegy, Clinician
Mekele Hospital
1. Bizayene Hadush, CEO 2. Dr. Mamute Mussie, Medical Director 3. Sister Eleni Abay, Ob/Gyn Case Team Leader 4. Shimaye Abrahm, HIV Clinic 5. Ferweyni Fisum, Case Manager 6. Alem Glyesus, Information Technician
Shire Shulu Hospital
1. Brook Dantechu, Medical Director 2. Dr. Amsalann Biten, Internist 3. Esayas Tiezasu, OPD Coordinator
Page91
4. Wigerima Tesfey, Pharmacist 5. Yemane Wibriel, Community Counselor 6. Fisehun Kindane, HIV/TB Nurse 7. TirhasTesta, ART Nurse 8. Aesanesh Glumedhim, Case Manager 9. Emebidi Hailu, Pharmacy/Data Clerk 10. Belai Hailu, Outreach Worker 11. Asranigh Abor, Outreach Worker 12. Shumuye Bahta, Community Counselor 13. Tirtu Hagos, Laboratory Coordinator 14. Asya Bert, Mothers Supporter 15. Sister Sedi Kemu, PMTCT Nurse 16. Fatima Amein, Mothers Supporter 17. Abelesh Meleti, Mothers Supporter 18. Rishan Tsipe, Mothers Supporter
Wukro Hospital
1. Aseye Bothru, Mothers Supporter
DebreBirhan Referral Hospital
1. Melat Sebsibie, MD: General Practitioner 2. Daniel Argaw, Pharmacist 3. Ermias Hailu, Head Laboratory Head 4. Tseganesh Biable 5. Lemma Negash, Human Resources Head 6. Fitsum Desalgn, Planning and Programming 7. Bekalu Mossie, Information Technician 8. Simegn Molla, Case Manager 9. Ruta Kidane, Data Clerk 10. Genet Waldekidan, Registered Nurse 11. Woinshet Kebede, Registered Nurse 12. Mehabw Fentie, HIV/AIDS Nurse Specialist
Dessie Regional Referral Hospital
1. Seid Tesfaw, CEO 2. Firehinot Tafete, MD-GP 3. Kedir Ali, MD-Internal Medicine 4. Yalew, Kesto, MD-Pediatrician 5. Mengstie Migussie, ART Head 6. FissehaYihenew, Drugist 7. Esayas Seyoum, Regional Laboratory Coordinator 8. Belet Eshet, PMTCT Head
Page92
9. Aklilu Abera, Nurse 10. Slr Negist Glgrogis, Nurse 11. Marta Bexlhun, Case Manager 12. Tehay Mohamed, Case Manager 13. Tigist Achenif, Information Mentor 14. ShunigeGigaw, MD-GP 15. Derbe Sitotaw Dessie, Senior Health Officer
WoldiaZonal Hospital
1. Ayalew Yimer, CEO 2. Abduilhafiz Hassen, Nurse, ART Coordinator 3. Eleni Asfawasen, Case Manager 4. Arega Abay, Information Mentor 5. Gezahagen Belay, Lab Manager 6. Amare Gedamis, Adherence Supporter 7. Solomon Guesh, Nurse Mentor 8. Seada Seid, Information Technician
Fisseha Damtie, Clinical Team Leader
Dubti Zonal Referral Hospital
1. Mohamed Ahmed, HO, Acting Medical Director 2. Seid Aseresu, ENV-Health (IP Focal) 3. Kebede Bezabih, Case Manager 4. Tesfye Gudissa, Pediatrician 5. Mevon Tadesse, Case Manager, IP Mentor 6. Bink Tadesse, Information Mentor 7. Hatsey Abrha, MD-ART Focal 8. Haimenot Manaye, Information Technician 9. Slr Elsabeth Aberha, HO- MCH Focal 10. Slr Foctuma Bekeao N/S VCT 11. Slr Aster Degu, Nurse TB/HIV 12. Ocjmun Alimeu, Nurse-Matron 13. Abdulhay Abdushehim, Drugist 14. Fitsume Kibret, MD, Regional Manager 15. Eyob Gebrehawariat, MD, Clinical Team Leader 16. Shegaw Denebe, HAN Specialist 17. Ibrahim Alemu, Nurse MoM
Aysaita Health Center
1. Fireweyen Yilema, Health Center Head, 2. Solomon Olango, HO 3. Sister Rukiya Ahmed, Nurse
Page93
4. Tiruwork Ali, IP/PMCTC 5. Abubeker Indris, TB/HIV Head Nurse 6. Issei Mohammed, CM 7. Mohammed Siraj, HCT Focal 8. Mohammed Hassen, STI Focal 9. KelemWorke 10. Bihan Legesse, Laboratory Head 11. Anteneh Abebe, Pharmacy Head 12. Birhan, Tessema, IT 13. Fitsume Kibret, MD, Regional Manager 14. BirukTadesse, Information Mentor 15. Birhan, Tessema, Information Technician 16. ShegahDeneke, HANS Mentor 17. Ibrahim Alemu, Nurse Mentor
18. Eyob, Gebrehawariaz, MD, Clinical Team Leader Awash Health Center
Site Participants
1. Abdella Kedir, Nurse, ART 2. Habib Ebrahim, Nurse 3. Berhane Takw, Information technician 4. Alemanyew Tefera, Health Officer, Medical Director 5. Shemsiya Mohammed, Lab Technician 6. Hailu Lechisa, Nurse Mentor 7. Hassen Mohammed, CM, IP Mentor 8. Mebese Bernenie, Information Mentor 9. Eshetu Abdissa, General Practitioner. Clinical Team Leader





























