Embed Size (px)
Citation preview

www.ccnonline.org CriticalCareNurse Vol 29, No. 5, OCTOBER 2009 45
Congenital completeatrioventricular block(CCAVB) occurs fromfetal age to young adult-hood in a person who
has had no other cardiac arrhythmiadetected before the heart block andno other history or signs and symp-toms of generalized disease.1 In thisarticle, I present the etiology ofCCAVB, risk factors, electrophysi-ology, pathophysiology, clinical features, diagnostic test findings,treatment, a case study, implicationsfor nurses, and teaching topics forpatients with pacemakers. Increasedawareness of suspecting an atrioven-tricular heart block, in children andyoung adults undergoing a physicalexamination or who are hospitalizedfor unrelated problems and then
Congenital CompleteAtrioventricular Block in aYoung Man: A Case Study
This article has been designated for CE credit. Aclosed-book, multiple-choice examination followsthis article, which tests your knowledge of the fol-lowing objectives:
1. Discuss the pathophysiology of completecongenital atrioventricular block
2. Identify the clinical features of completecongenital atrioventricular block
3. Describe 3 teaching points for a patientwith a pacemaker
CEContinuing Education
found to have a slow heart rate, willensure earlier recognition of thisproblem. Early recognition can helpprevent cardiac decompensationand sudden cardiac death in theseyoung persons.
Diagnostic criteria for CCAVB inchildren include occurrence of com-plete atrioventricular block (CAVB)in utero or at birth as indicated byechocardiographic or electrocardio-graphic (ECG) findings or CAVBwith some evidence of a slow pulseat a fairly early age with no historyof myocarditis that might havecaused the condition after birth.2
The estimated incidence of CCAVBis 1 in 20000 live births,2-4 but in astudy by Siren et al,5 the incidencein Finland during the 1990s hadincreased to 1 in 11000 births. Thisincrease may be due to improvedtechnological advances and increasedprenatal care. CCAVB affects malesand females equally and has beenassociated with familial clustering.1,4
The common occurrence of heartblock in older patients lowers expec-tations of CAVB in younger patients.CAVB most often occurs in patientswho are older (>70 years) who mayhave injury to or degeneration ofthe fibers in the conduction system.
Connie S. Chronister, RN, MSN, CCRN
Clinical Article
PRIME POINTS
• Health care profession-als performing physicalassessments should sus-pect the possibility of anunderlying heart conditionin young adults and chil-dren with slow heart rates.
• Arrhythmias associatedwith a slow heart rate caneasily be missed during aphysical assessment if anECG is not obtained.
• Patients with congenitalcomplete atrioventricularheart block can be totallyasymptomatic or can havesubtle signs and symp-toms that can easily beattributed to other causes.
©2009 American Association of Critical-Care Nurses doi: 10.4037/ccn2009297
by AACN on May 10, 2018http://ccn.aacnjournals.org/Downloaded from

Etiology and Risk FactorsCCAVB is thought to be caused
by destruction of the conductionsystem by myocarditis2 and is associ-ated with maternal autoimmune dis-ease,6 structural heart disease, and,when diagnosed in utero, neonatallupus syndrome.7 CCAVB is stronglyassociated with maternal connectivetissue disorders (CTDs), especiallythose involving autoantibodies toRo/SS-A, which have been detectedin maternal sera in up to 98% of casesof CCAVB. These auto antibodies arethought to cause damage to the car-diac conduction system. CCAVB mayoccur in association with destruc-tion of the normal conduction sys-tem by maternal autoantibodies tothe nuclear antigens Ro/SS-A andLa in CTDs such as systemic lupuserythematosus (SLE), which triggersimmune-mediated inflammation ofthe atrioventricular nodal and myo -cardial tissues in a susceptible fetus.Viral infections and long-QT syn-drome might be responsible for casesin which these autoantibodies arenot detected in the mother.8 CCAVBis thought to be primarily the resultof maternal CTDs such as Sjögrensyndrome, SLE, and rheumatoidarthritis. In SLE, small-vessel vas-culitis and fibrous tissue infiltrationare the major causes of dysfunctionof the sinus or atrioventricular node.9
These conditions are thought to causea placental transfer of antibodies toRo/SS-A and La that damage the
fetal conduction system.9 Whentested for CTD, 75% of motherswho had a child with CCAVB hadno signs and symptoms of CTDbut had antibodies to Ro/SS-A.2
Other causes of CCAVB (25%-33%),10 which may or may not havean inherited component, includestructural cardiac abnormalitiessuch as L-transposition of greatarteries, ventricular inversion, andatrioventricular septal defect inwhich the atrioventricular nodeends blindly.4 CCAVB patients withstructural heart disease have highermortality than do those withoutstructural heart disease.2
Neonatal lupus is rare and maylead to CCAVB due to transplacen-tal transfer of autoantibodies frommothers who are positive for anti-bodies to Ro/SS-A and La, butCCAVB in patients with neonatallupus is thought to occur in only 3%of infants with antibody-positivemothers.9 Neonatal lupus syndromehas a 12% to 41% first-year mortality
rate6 and is rarely responsible forpreviously asymptomatic CCAVBthat occurs in childhood or youngadulthood.6 Jaeggi et al11 reportedthat the mechanism of heart blockmay differ between CCAVB diag-nosed in utero or during the neona-tal period (<28 days) and CCAVBdiagnosed in childhood. This find-ing suggests that the mechanism ofheart block is not due to autoimmunedestruction of the conduction sys-tem in these patients because CCAVBdiagnosed in childhood has a lessdire prognosis.
The overall mortality rate forCCAVB is 4% to 29%2 (Table 1). Thegeneral population potentiallyincludes a small percentage of indi-viduals who have grown to youngadulthood with CCAVB that has notbeen diagnosed. The exact incidenceof this problem in individuals whoare now young adults is unknownbecause CCAVB may not have beenrecognized when they were youngerand their bodies were able to com-pensate for the slow heart rate.
CCAVB is associated with manypotential cardiac complications(Table 2). The main causes of earlydeath due to CCAVB are cardiac fail-ure associated with cardiomyopathy6
and sudden cardiac death. Thesecardiac complications account for
Connie S. Chronister is a clinical instructor at the University of Akron in Akron, a doctoralstudent in nursing practice at Case Western Reserve University in Cleveland, and a staffnurse at Medina General Hospital in Medina, Ohio.Corresponding author: Connie S. Chronister, RN, MSN, CCRN, 2824 Sharon Copley Rd, Medina, OH 44256 (e-mail: [email protected]).
To purchase electronic or print reprints, contact The InnoVision Group, 101 Columbia, Aliso Viejo, CA 92656.Phone, (800) 899-1712 or (949) 362-2050 (ext 532); fax, (949) 362-2049; e-mail, [email protected].
Author
Table 1 Mortality rates associated with congenital complete atrioventricularblock (CCAVB)a
Population
Children with isolated CCAVB
Infants with isolated CCAVB
Infants with associated structural heart disease
Children with associated structural heart disease
Adults with isolated CCAVB who were asymptomatic duringinfancy and childhood
Estimated mortality rate, %
6-8
4-8
29
10
5
a Based on data from Balmer et al2 and Michaelsson et al.29
46 CriticalCareNurse Vol 29, No. 5, OCTOBER 2009 www.ccnonline.org
by AACN on May 10, 2018http://ccn.aacnjournals.org/Downloaded from

up to 14% of deaths in patients withCCAVB.5 Adams-Stokes attacks andheart failure may develop at any agein children with CCAVB.15 Patientswith CCAVB can appear healthy,especially when they have no othercardiovascular problems, but it isclearly established that the firstmanifestation of CCAVB can besudden death.10
Electrophysiology of CAVBCAVB is characterized by a com-
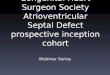
plete absence of conduction of elec-trical impulses from the atria to theventricles; the cardiac conductionsystem (Figure 1) is interrupted atthe level of the atrioventricular node,bundle of His, or bundle branches.16
Because of the dissociation of theatria and ventricles, patients withCAVB have a ventricular heart ratethat is slower than the atrial rate.The atrial and ventricular chambersbeat independently of each otherbecause no communication existsbetween the chambers. This lack ofcommunication results in a con-duction block at the level of theatrioventricular node. For example,the atrial rate may be 80/min andthe ventricular rate 40/min. A regu-lar P-P interval may be visible, orthe interval may appear to changebecause of nonvisible P waves that
may be hidden in the QRS complexor the T waves. Importantly, althoughthe PR intervals vary widely, the PRmeasurement in complete heart blockis meaningless because no relation-ship exists between atrial conductionand ventricular conduction; they areindependent of each other. Table 3
indicates differences in types ofheart block and provides examplesof ECG findings.
The ventricular rate in CAVB isslow because the atrioventricular(junctional) or ventricular pace-maker takes over to pace the heartat a rate much slower than theintrinsic sinus node rate. The inher-ent rate of automaticity of the atri-oventricular pacemaker is 40/minto 60/min, with a narrow QRS com-plex; the inherent rate of automatic-ity of the ventricular pacemaker is20/min to 40/min, with a wideQRS complex.19 However, escaperhythms such as accelerated junc-tional or accelerated idioventricularrhythms are common. The morphol-ogy of the escape rhythm may help
Table 2 Cardiac complications associated with congenital complete atrioven-tricular blocka
Complication
Dilated cardiomyopathy, heart failure (more common in patients <4 years old)
Syncope or Adams-Stokes attacks (more common in patients >4 years old)
Mitral valve insufficiency in adults
Sudden deathIn newbornsIn adults
% of cases
3-4
40
10
2010
a Based on data from Esscher,1 Kertesz et al,3 Gordon,6 Beaufort-Krol et al,13 and Michaelsson and Jonzon.14
Figure 1 Cardiac conduction system.Reprinted with permission of SensorMedics.
Atrioventricular bundle(bundle of His)
Right bundlebranch
Atrioventricularnode
Sinoatrialnode/pacemaker
Leftbundlebranch
www.ccnonline.org CriticalCareNurse Vol 29, No. 5, OCTOBER 2009 47
by AACN on May 10, 2018http://ccn.aacnjournals.org/Downloaded from

distinguish its origin. A narrow com-plex (<120 ms) indicates a block inthe atrioventricular node with theescape pacemaker at the atrioven-tricular junction, a condition that is
considered “stable” and usuallydoes not progress to asystole.20 Awide QRS (>120 ms), signifies a dis-tal or infrahisian block (in the lowerpart of the bundle of His or in the
bundle branches) and is inherentlyless stable, with a risk of asystole orpolymorphic ventricular tachycar-dia20 (Figure 2). A wide QRS com-plex (>120 ms) may also occur if the
Table 3 Differences between first-degree, second-degree, and complete heart blocka
Type of heart block
Feature First degree Second degree, Mobitz type 1 (Wenckebach)
Electrocardiographic appearanceb
Rate Generally at intrinsic rate of 60/min to 100/minMay be slower
Atrial rate generally at intrinsic rate of 60/min to100/min
Ventricular rate depends on number of impulsesconducted through atrioventricular node; will beslower than atrial rate
Regularity of atrial rhythm Regular Regular
Regularity of ventricular rhythm Regular Regularly irregular
P wave P to P wave is constant P to P wave is constant
P:QRS ratio 1:1 1:1 until block occurs, then a P wave with apause absent of a QRS complex, then cyclerestarts with a P wave and associated QRScomplex
PR interval (the primary clue to thedegree of heart block)
Constant PR interval but prolonged >0.20 s or200 ms
Variable: PR interval progressively lengthens untila QRS complex is dropped
A pause follows the dropped QRS complex, thenPR interval resets to shorter interval and thecycle repeats, very cyclic
QRS width Normal, <0.12 s Normal <0.12 s
Dropped QRS complexes/pauses None Yes: pattern of progressive lengthening of theinterval from QRS to QRS until a QRS is droppedafter a P wave; then a pause occurs, and theinterval resets
a Adapted from Huff17 and Garcia and Holtz.18
b Images of second-degree and complete heart block are reprinted from Huszar,19 with permission. Copyright Elsevier 2002.
48 CriticalCareNurse Vol 29, No. 5, OCTOBER 2009 www.ccnonline.org
by AACN on May 10, 2018http://ccn.aacnjournals.org/Downloaded from

atrioventricular junction pacemakerdischarges before both the bundlebranches have completely repolar-ized, thus causing the electricalimpulse to be conducted down one
bundle branch (usually the left one)and blocked in the other branch(usually the right one).19 CAVB mostoften occurs in patients who areolder (>70 years) who may have
degeneration of the fibers in theconduction system. CAVB is com-mon in patients with ischemic heartdisease, including patients with acuteinferior or right ventricular myocar-dial infarctions, digitalis poisoning(because the sodium and potassiumchannels in the action potential arealtered), or chronic degenerativechanges in the conduction system.16,19
The common occurrence of heartblocks in older patients may lower apractitioner’s awareness of the pos-sibility of CAVB in younger patients.
PathophysiologyCCAVB is thought to be due to
maternal autoantibodies associatedwith autoimmune disease that crossthe placenta during fetal develop-ment, causing a myocarditis thatdamages the atrioventricular nodeand bundle of His region of thecardiac conduction system.2 Themyocarditis leads to inflammationand scarring of the atrioventricularnode and bundle of His areas,resulting in delayed and blockedconduction through these areas.ECG features of CCAVB are a per-sistently low ventricular rate, a pro-longed QT interval, and a wideQRS complex. Because of incom-plete ventricular emptying, mitralregurgitation and left ventriculardilatation are also associated withCCAVB. Cardiac output = strokevolume × heart rate. To maintaincardiac output, the stroke volumeincreases, and the increased forceof contraction contributes to ven-tricular hypertrophy. This processcombined with increased left ven-tricular end-diastolic volume21 canresult in dilated cardiomyopathy.13
Cardiac dilatation as a compensatorymechanism may also predispose
Type of heart block
Second degree, Mobitz type 2 Complete or third degree
Atrial rate generally at intrinsic rate of 60/minto 100/min
Ventricular rate depends on number of impulsesconducted through atrioventricular node:may intermittently be the same as atrial ratewhen impulses are being conducted
Ventricular rate will be slower than atrial ratewhen impulses are blocked
Atrial rate and the ventricular rate are alwaysdifferent; atrial is faster than ventricular
Regular Regular
Regularly irregular or irregularly irregular Regular with ventricular rate slower than atrialrate
May become irregular as heart becomesischemic
P to P wave is constant P to P wave is constant but P waves may bedifficult to see if buried in the QRS complexor T wave
1:1 until block occurs, then 2 or more P wavesthat are followed by a pause without QRScomplexes
1:1 conduction may recur or may progress toventricular asystole or complete heart block
Variable, more P waves than QRS complexes
PR interval remains constant until a blockoccurs and the QRS complex is dropped,resulting in a pause
When or if conduction resumes, the PR interval remains constant
PR interval is not consistent
Impulses are not conducted from the atria tothe ventricles
Visually the PR interval is not constant anddoes not progressively lengthen, “no pattern”
Normal if block is at level of bundle of His
Wide (≥0.12 s) if block in bundle branches
Normal or wide
Normal (<0.12 s) if block at level of atrioven-tricular node or bundle of His
Wide (≥0.12 s) if block in bundle of His
Yes: QRS-QRS rate is constant until a QRScomplex is dropped and a pause occurs
None
www.ccnonline.org CriticalCareNurse Vol 29, No. 5, OCTOBER 2009 49
by AACN on May 10, 2018http://ccn.aacnjournals.org/Downloaded from

patients to ventricular ectopy similarto the way atrial dilatation predis-poses patients to atrial dysrhyth-mias.21 Risk of sudden cardiac deathmay increase in patients with a pro-longed QT interval, which predis-poses them to development of theventricular arrhythmia torsades depointes. Age and resting heart rateare also factors implicated in therisk for sudden cardiac death. Therisk for sudden death is increasedin infancy, decreases in childhood,and then increases again later in life.21
Clinical FeaturesThe signs and symptoms of
patients with CCAVB depend onthe baseline ventricular rate andunderlying structural defects. Patientsmay be asymptomatic until cardiacdecompensation begins to occur inadulthood. Slow heart rates and faint-ing or Adams-Stokes attacks, definedas abrupt loss of consciousness
without warning,22 and near-fainting(dizzy) spells or presyncopal episodesare common overt indications. Othersigns and symptoms of low cardiacoutput and exercise intolerance aresometimes subtle and often areattributed to other causes. Many
children and young adults adopt asedentary lifestyle as an adaptivemechanism.1 Table 4 lists overt andsubtle signs and symptoms of lowcardiac output.
Signs and symptoms, includingthe first Adams-Stokes attack, developin adulthood in approximately 50%of adults with CCAVB who wereasymptomatic in childhood andadolescence, and 10% die prema-turely.3 Also, heart rate decreasesprogressively in adults with CCAVBas they become older, a change thatdoes not occur in healthy adults.15
A physiological explanation forincreased signs and symptoms ofdecompensation in older patientswith CAVB is related to the deterio-ration of physiological compensa-tory mechanisms.6
Signs and symptoms in CCAVBare due to a slow heart rate withresultant low cardiac output. Parox-ysmal nocturnal dyspnea, a suddenattack of dyspnea that occurs duringsleep, is related to CCAVB becausethe heart rate slows more severelyduring sleep. Cardiac output is then
Figure 2 Close-up of atrioventricular node.Adapted from Garcia and Holtz,18 with permission.
Sinoatrial node
Atrioventricular node
Infrahisian region
Suprahisian region
Bundle of His(intrahisian region)
Table 4 Overt and subtle signs and symptoms of low cardiac output associatedwith slow heart rate in older childrena
Overt
Fainting or dizzy spells (Adams-Stokes attacks)
Syncope
Exercise intolerance (dyspnea with exertion, diaphoresis)
Sudden death
Subtle
Sedentary lifestyle, avoidance of physical workor play
Postural nocturnal dyspnea
Shortness of breath with activity
Long naps or sleep intervals
Irritability
Insomnia (related to diaphoresis, posturalnocturnal dyspnea)
Headaches
Intolerance to heat
a Based on data from Beaufort-Krol et al.23
50 CriticalCareNurse Vol 29, No. 5, OCTOBER 2009 www.ccnonline.org
by AACN on May 10, 2018http://ccn.aacnjournals.org/Downloaded from

further compromised, decreasingoxygen delivery to the tissues, caus-ing dyspnea. Paroxysmal nocturnaldyspnea disturbs sleep, and theperson awakens with a feeling ofextreme suffocation that resolveswhen he or she sits upright. Ini-tially, the experience may be inter-preted as awakening from a baddream.24 Cardiac fatigue is mani-fested as tiredness that occurs laterin the day, with a resultant need fornaps. Exercise intolerance leads toexercise avoidance and adaptivemechanisms such as moving slowlyand resting frequently. Irritability,fatigue, and headaches in adoles-cents can also be associated withheart failure; cardiac output is notsufficient to perfuse the brain andorgans because the ventricular ratecannot increase.
Diagnostic Test FindingsPatients with CCAVB may
undergo routine 12-lead ECG,echocardiography, Holter monitor-ing, electrophysiology studies, andtreadmill testing to determine theeffects of the disease process. Theresults of diagnostic tests are notpredictive of who will die fromCCAVB, but the results do indicaterisk factors and can be used todetermine which patients shouldreceive a pacemaker. Resting heartrate decreases with age in patientswith CCAVB during infancy andchildhood, and heart rates less than50/min are associated with signs andsymptoms and increasing mortality.14
In ECG evaluations, the widthof the QRS complex is used to inferwhether hemodynamically unstablecardiac rhythms may develop.14 Aventricular rhythm with a wide com-plex (>120 ms) and a prolonged
QTc (>450 ms) in patients withCCAVB is an unfavorable prognos-tic sign because it may be related tounderlying myocardial damage.14
A prolonged QTc is associated withCCAVB and occurs in approxi-mately 15% to 22% of patients.3 Inmultiple studies,1,10,14 a greater per-centage of patients with CCAVBand QTc prolongation greater than450 ms had signs and symptomsrelated to the CCAVB or suddenlydied than did CCAVB patientswithout QTc prolongation.
The results of Holter monitor-ing in CCAVB have not been exten-sively studied, but patients who hada heart rate less than 50/min had anincreased risk for syncope or sud-den cardiac death.3,15
Treadmill exercise testing is donemainly to evaluate functional capac-ity.10 In patients with CCAVB with-out structural heart disease, up to90% have normal results in exercisetreadmill tests.3,14 During exercisetesting, ventricular ectopy occurs in50% to 70% of patients, but its impor-tance in sudden cardiac death hasnot been determined. Patients whosepeak exercise or target heart rateswere less than 123/min had morecardiac deaths and/or pacemakerinsertions than did patients withhigher rates.10
Before treadmill exercise testing,the patient’s target heart rate is cal-culated. The target rate is usually85% of the maximum predicted rate.(In order to obtain the target rate,22
the patient’s age is subtracted from220, and the new number is multi-plied by 0.85.) Because of heart block,patients with CCAVB may not attaintheir target heart rate during exer-cise. In the electrophysiology labo-ratory, the location of the block inthe bundle of His can be determined(Figure 1). Suprahisian block is themost common, but the location ofthe block is not predictive of syncopeor sudden death.4 The terms supra(above) and infra (below) refer tothe location of the block within thebundle of His; intrahisian (within)is a general term referring to thebundle of His. Table 5 lists typesof diagnostic tests used to diagnoseCCAVB.
Treatment of CCAVBInsertion of a pacemaker is rec-
ommended for patients with symp-tomatic bradycardia,3 and treatmentof CCAVB centers on temporary andpermanent pacing.21 Prevention ofsudden cardiac death and an increasein functional capacity are the pri-mary goals of pacemaker insertion.Implantation is indicated in most
Table 5 Diagnostic testing for congenital complete atrioventricular blocka
Test
Electrocardiography
Electrophysiology studies
Treadmill stress testing
Holter monitoring
Echocardiography
Purpose
Diagnose arrhythmia, type of heart block
Locate level block in conduction system
Evaluate functional capacity
Determine how heart rate and rhythm vary with activities ofdaily living
Diagnose structural problems
a Based on data from Vukomanovic et al15 and Dewey et al.25
www.ccnonline.org CriticalCareNurse Vol 29, No. 5, OCTOBER 2009 51
by AACN on May 10, 2018http://ccn.aacnjournals.org/Downloaded from

patients with isolated CCAVB26
(Table 6). Symptomatic patients orpatients with congestive heart fail-ure who are in complete heart blockshould be treated with an atrioven-tricular sequential (or dual chamber)pacemaker to maintain normal syn-chrony of the heart and physiologi-cal rate response. If sinus nodefunction is normal in a child oryoung adult with CCAVB, then asingle-lead ventricle dual-chamberpacemaker can be safely implanted.This type is preferred over dual-chamber pacing because of the longperiod of pacing ahead for young
Table 6 Indications for pacemaker implantation in children and adults withcongenital complete atrioventricular blocka
Children
Congestive heart failure
Syncope
Dilatation of the left ventricle
Ventricular arrhythmia
Changing (widening) QRS morphology or abruptpauses in ventricular rate that are 2-3 times longerthan the preceding RR interval and bradycardia(heart rate, 50/min to 55/min) with QTc prolongation
Mitral regurgitation
Ventricular rate <60/min
Adults
Congestive heart failure
Repeated episodes of syncope
Exertional dyspnea
Fatigue
Ventricular and supraventricularectopic beats during exercisetests
Mitral regurgitation
Ventricular rate <50/min
Dizziness
a Based on data from Balmer et al,2 Siren et al,5 Michaelsson and Jonzon,14 and Dewey et al.25
CASE STUDY
A 30-year-old man came to the emergency depart-ment because of shortness of breath, dry persist-
ent cough, and midsternal chest pain. His temperaturewas 40ºC (103ºF) orally, and his heart rate was 40/min.Cardiac monitoring indicated CAVB with narrow QRScomplexes. The diagnosis was bronchitis and completeheart block, which was verified by findings on a 12-leadECG (Figure 3). He left the emergency department againstmedical advice because he was “late to work.” He wastold that he might need a pacemaker and that he shouldsee a cardiologist.
At a follow-up appointment with a cardiologist, thepatient said that he had been told since childhood, dur-ing his school physicals, that he had a “slow heart beat,”but he had not asked questions about it. No subsequentfollow-up testing or ECG had been done. In retrospect,the patient had had signs and symptoms of low cardiacoutput throughout adolescence, but they were so subtlethat the association with the slow heart beat was notrecognized even by his mother, who was a nurse in anintensive care unit.
A resting ECG showed CAVB with a junctional escaperhythm of 41/min. The QRS duration was 98 ms (normal,80-120 ms), and the QT interval and the QTc were 524and 432 ms, respectively (normal range, QTc >450 ms).19
An echocardiogram completed during this workupshowed normal left ventricular systolic function and an
ejection fraction of 72% (normal range, 50%-70%), indi-cating strong heart muscle function. The echocardio-gram showed no left ventricular hypertrophy, normalright ventricle, and normal right and left atria. All valvesappeared normal except the pulmonary valve, whichwas not visualized.
On a stress test, the baseline ECG finding was com-plete atrioventricular dissociation with a resting heartrate of 38/min. Total exercise time was 10 minutes and33 seconds with a heart rate response of only 58%. Bloodpressure response was somewhat abnormal, with a sys-tolic pressure of 180 mm Hg. No ST-segment abnormal-ities occurred during the stress testing. The patientremained in second-degree heart block Mobitz type IIduring the test and at peak exercise appeared to be insinus tachycardia, with a heart rate of 111/min. Then,less than 1 minute after exercise, the rhythm changedto complete heart block, with a resting ventricular rateof 38/min. The stress test was inconclusive because thepatient did not achieve his calculated target heart rate.
A 24-hour recording from Holter monitoring indi-cated predominantly complete block with intermittentsecond-degree heart block Mobitz type II at a meanheart rate of 42/min. The ventricular rate varied from alow of 29/min to a high of 78/min. A single sinus pauseof 3.7 seconds was evident, with rare asymptomaticventricular and supraventricular ectopy.
The cardiologist diagnosed CCAVB on the basis ofa history of slow heart rates, which were noted during
52 CriticalCareNurse Vol 29, No. 5, OCTOBER 2009 www.ccnonline.org
by AACN on May 10, 2018http://ccn.aacnjournals.org/Downloaded from

patients with CCAVB. Early implan-tation of a pacemaker may reduceor eliminate mor bidity by prevent-ing complications such as mitralvalve insufficiency.2
Implications for NursesAdvanced practice and school
nurses who perform physical assess-ments on children or young adultsand discover a heart rate less than55/min should use a cardiac moni-tor to determine the patient’s heartrhythm. Health care professionalsshould suspect a heart block untilproven otherwise when the heart
rate is slow. Of note, patients bornbefore the advent of routine fetalultrasound testing may grow toadulthood without this cardiac prob-lem being detected. They may beginto manifest signs and symptoms ofcardiac decompensation later in life.
In this case study, the patienthad been told during routine physi-cals that he had a slow heart ratebut did not know to ask how slowor to suspect that his fatigue, insom-nia, and other signs and symptomsmight have been related to a slowheart rate, and he never mentionedthe information to anyone. A parent
should accompany adolescents totheir physical examinations andsports physicals so that he or shecan be available to ask questionsand obtain information from thepractitioner. Although routine sportsphysical forms include questionsabout a history of long QT syndromeand abnormal heart rhythms, theseproblems may not have been diag-nosed or a family history of theseproblems may not be known. Patientswith slow heart rates should have aECG, and the PR interval, QRScomplex, and QT interval shouldbe measured and documented.
sports physicals in adolescence but attributed to an“athletic heart.” One cannot be completely certain thata complete heart block in a young adult is congenitalunless the block is noted at birth.1 In this case, the diag-nosis was attributed to the previous lack of diagnosticcapabilities when the patient was an infant and the fact
that his slow heart rate was overlooked because heappeared healthy. Also supporting the diagnosis was afamily history of great-uncles and uncles on the pater-nal side who died unexpectedly in their 40s of “heartproblems.” The patient’s mother had had tests for SLE;the results indicated no SLE, although no assays for
Figure 3 12-Lead electrocardiogram shows complete heart block.
I
II
III aVF
aVL
aVR V1
V2
V3 V6
V5
V4
www.ccnonline.org CriticalCareNurse Vol 29, No. 5, OCTOBER 2009 53
by AACN on May 10, 2018http://ccn.aacnjournals.org/Downloaded from

Medical/surgical, emergency,and pediatric nurses should alsoconsider the possibility of cardiacproblems in patients who have heartrates less than 55/min even thoughthe patients may have no symptomsof bradycardia. A high fever in apatient with a slow heart rate shouldbe a red flag because fever usuallycauses tachycardia.16 Health careproviders should not assume that apatient with a slow heart rate is ath-letic and physically fit; the patientshould be questioned about his orher involvement in and tolerance ofphysical activities.
Patient Teaching Patients who are receiving pace-
makers to treat CCAVB or sometype of heart block and the patients’families should be taught how tomeasure a radial or carotid pulse.The patients should carry a card
with them at all times that has theirpacemaker information. Commonly,patients with CCAVB are pacemakerdependent because of their inher-ently slow heart rate. Family mem-bers of any patient who is pacemakerdependent or has CCAVB shouldlearn cardiopulmonary resuscitation.Patients who are pacemaker depend-ent or at risk for syncope or cardiacarrest should be encouraged to obtaina medical identification bracelet.27
Nurses should also be aware ofthe psychosocial issues involvedwhen a young adult needs a pace-maker. Patients may deny the needfor a pacemaker because it is asso-ciated with something old peopleneed and may resist the surgery forpacemaker implantation because ofa fear of scars and visibility of theimplanted device. In addition, con-tact sports must be avoided, a situ-ation that may influence the child
or adolescent’s fear of social isola-tion or of “being different.” A com-prehensive team approach withnurses, physicians, patients’ familymembers, and sometimes referralto professional counseling may bebeneficial.27
Gradual resumption of activitiesshould be encouraged after implan-tation of a permanent pacemaker.Activities that a child or adolescentmay perform should not overstretchor overextend the arm or shoulderon the side of the pacemaker, becausedoing so can cause lead dislodge-ment. For example, if a patient hasa pacemaker on the left side, he orshe may play tennis with the rightarm but should avoid playing withthe left arm. Noncontact sportsshould be encouraged to promoteself-esteem and improve or main-tain circulatory status. Patients andtheir family members should be
antibodies to Ro were done. The patient had a paternalgreat-grandmother who had severe rheumatic arthritis.
The patient reluctantly had placement of an atrioven-tricular sequential permanent pacemaker with the lowrate limit set at 60/min. He was initially resistant to hisneed for a pacemaker, feeling that the device was some-thing only needed by “old people.” A larger than normalgenerator was inserted because he needed the pacemaker100% of the time for atrial and ventricular pacing. Immedi-ately after receiving the pacemaker, he began to feel better.He described having “more energy” and stated days afterthe pacemaker insertion, “The way I feel now compared tobefore, I don’t think I would have been alive in five years.”
This patient was a full-term and healthy infant buthad a cesarean birth because of a slow heart rate, whichwas attributed to fetal distress. His childhood medicalhistory was notable for a poor sleep pattern that includednight terrors, heat intolerance, and activity intolerance.The activity intolerance was attributed to “laziness” byhis parents. According to his mother, his childhood wasbasically normal except that he had one speed: “slow.”
When he was about 13 years old, he became moodyand irritable and complained of insomnia and night-mares. These problems were attributed by his parentsto poor eating habits, not enough exercise, and justbeing a teenager who listened to heavy metal music. He also complained of headaches, which were attributedto stress at school and not sleeping. Unfortunately, hedropped out of high school in his junior year, partlybecause he had missed so much school because of hisfatigue. Again these symptoms were attributed to “teenagerebellion.” The patient had actually received a detentionat school for “walking too slow” when getting off theschool bus. This patient also reported near-faintingspells that occurred occasionally when he would changefrom a sitting position to a standing position and pro-fuse diaphoresis with light work. Despite having no overtsigns or symptoms of cardiac problems in childhood, at30 years old, the patient was beginning to have signs andsymptoms of cardiac decompensation. He would quicklybecome short of breath and profusely diaphoretic withminimal exertion.
54 CriticalCareNurse Vol 29, No. 5, OCTOBER 2009 www.ccnonline.org
by AACN on May 10, 2018http://ccn.aacnjournals.org/Downloaded from

instructed to call 911 if syncope orcardiac arrest occurs.
According to the American HeartAssociation,28 patients with pace-makers should be taught to avoiddevices that have strong magneticfields because the magnetic fieldscan interfere with the pacemaker.Most electromagnetic fields in thehome environment rarely affectpacemaker function. Most house-hold and workplace appliances,tools, and equipment can be usedwithout precautions. As a generalrule, patients with pacemakersshould avoid activities that causevibration because such movementcan dislodge the leads. Any patientwith a pacemaker who begins tofeel faint or dizzy or begins to havepalpitations when around any equip-ment should move farther awayfrom the equipment because it maybe interfering with the pacemaker.
Examples of devices with strongmagnetic fields that should beavoided because they cause electro-magnetic interference and can inter-fere with pacemaker function areairport scanners and handheld metaldetectors, magnetic resonance imag-ing machines (although some centerscan reprogram the pacemaker andthen perform low-energy imaging),arc-welding equipment, and electro-cautery sources commonly used insurgery. Items containing magnetsshould be kept at least 15 cm (6 in)from a pacemaker because mostpacemakers have a magnetically acti-vated switch built into the electronics
that closes, altering function andcausing the pacemaker to change toa preset rate.29 A magnet may be usedto monitor and test the pacemakerduring follow-up visits to a physi-cian’s office or during telephonemonitoring. Removing the magnetreturns the pacemaker back to theprevious settings and functioning.
In the United States, patientswith pacemakers who use cell phoneswith a power less than 3 W needtake no special precautions becausethe phones do not appear to dam-age pulse generators or affect howthe pacemakers work.30 Electromag-netic shielding has been incorpo-rated into the design of modernpacemakers to prevent radiofre-quency signals from interferingwith the electronic circuitry in thepacemaker.29 The National Institutesof Health31 states that cell phones inthe United States do not interferewith pacemakers, but patients with
pacemakers should pay close atten-tion to their surroundings to makesure no devices are present thatmight interfere with the pacemak-ers. The American Heart Associa-tion, the Texas Heart Institute, andthe Federal Communication Com-mission all recommend keepingcordless or handheld cellular phones15 cm away from the pacemakerjust to ensure safety. If a cell phonetransmits at greater than 3 W ofpower, the antenna should be kept30 cm (12 in) away from all modelsof pacemakers. As an extra safetymeasure, to avoid any possible dis-ruption in pacemaker function,patients with pacemakers shouldhold cell phones to the ear oppositethe side of the pacemaker and shouldnot place the cell phone in a shirtpocket on the same side of the bodyas the pacemaker generator. Table 7provides general information forpatients with pacemakers.
d•tmoreTo learn more about atrioventricular block,read “Heart Blocks” by Mary G. Adams-Hamoda and Michele M. Pelter in theAmerican Journal of Critical Care, 2003;12:77-78. Available at www.ajcconline.org.
�
www.ccnonline.org CriticalCareNurse Vol 29, No. 5, OCTOBER 2009 55
Table 7 General information for patients with permanent pacemakersa
• Learn how to take radial or carotid pulse, when to call health care provider
• Carry pacemaker identification information card with you at all times
• Encourage family members to learn cardiopulmonary resuscitation
• Wear medical identification bracelet if you are pacemaker dependent
• Follow physician’s guidelines for routine pacemaker checks
• Avoid strong magnetic fields (eg, arc-welding equipment, magnetic resonance imaging machines, high-voltage commercial transformers)
• Be aware that the average pacemaker battery lasts about 5 to 8 years
• Avoid full-contact sports
• Extracorporeal shock-wave lithotripsy to dissolve kidney stones may alter pacemakerfunction (reprogramming will be required) and should be avoided if the pacemakergenerator is implanted in the abdomen
• Therapeutic radiation treatments to treat cancer may damage the pacemaker circuitry
• If you are scanned with a handheld metal detector, tell security personnel that youhave a pacemaker and that the scanner should not be held near the device for anylonger than absolutely necessary; you can ask for a personal search in place of themetal detector to avoid any risk of pacemaker malfunction
• Cell phones less than 3 W of power do not interfere with pacemakers
a Based on data from the American Heart Association28 and the Federal Communications Commission.31
by AACN on May 10, 2018http://ccn.aacnjournals.org/Downloaded from

ConclusionsHealth care professionals per-
forming physical assessmentsshould not assume that youngadults and children with slow heartrates (<50/min) are free of cardiacproblems. Cardiac monitoringshould be use to investigate theslow rhythm. Patients with CCAVBcan have subtle signs and symptomsthat can easily be attributed to othercauses or can be totally asympto-matic until sudden cardiac deathoccurs. Health professionals shouldnot be fooled into complacencybecause a patient “looks healthy.” A thorough physical examinationof patients with slow heart ratesshould include an ECG. Detection ofCCAVB by health care professionalsduring routine health maintenanceexaminations with subsequentinvestigation and treatment may bea life-saving event for patients withthis heart condition. CCN
AcknowledgmentI thank Diane Utzler, RN, at Medina General Hospi-tal, Medina, Ohio, for assistance in data collection,and Karen Crabtree for artistic assistance with Fig-ures 1 and 2.
Financial DisclosuresNone reported.
References1. Esscher EB. Congenital complete heart
block in adolescence and adult life: a follow-up study. Eur Heart J. 1981;2(4):281-288.
2. Balmer C, Fasnacht M, Rahn M, Molinari L,Bauersfeld U. Long-term follow up of chil-dren with congenital complete atrioventric-ular block and the impact of pacemakertherapy. Europace. 2002;4:345-349.
3. Kertesz NJ, Fenrich AL, Friedman, RA.Congenital complete atrioventricularblock. Tex Heart Inst J. 1997;24(4):301-307.
4. Camm AJ, Bexton RS. Congenital completeheart block. Eur Heart J. 1984;5:115-117.
5. Siren MK, Julkunen H, Kaaja R. Theincreased incidence of isolated congenital
heart block in Finland. J Rheumatol.1998;25:1262-1264.
6. Gordon PA. Congenital heart block: clinicalfeatures and therapeutic approaches. Lupus.2007;16:642-646.
7. Moak J, Barron K, Hougen T, et al. Congen-ital heart: development of late-onset cardiomy-opathy, a previously under appreciatedsequela. J Am Coll Cardiol. 2001;37:238-242.
8. Jaeggi ET, Fouron JC, Silverman ED, RyanG, Smallhorn J, Hornberger LK. Transpla-cental fetal treatment improves the outcomeof prenatally diagnosed complete atrioven-tricular block without structural heart dis-ease. Circulation. 2004;110(12):1542-1548.
9. Seferovi PM, Risti AD, Maksimovi R, et al.Cardiac arrhythmias and conduction distur-bances in autoimmune rheumatic diseases.Rheumatology (Oxford). 2006;45(suppl 4):iv39-iv42.
10. Gobeil F, Labbe A, Lepage S. Congenitalcomplete atrioventricular block: asympto-matic at 38 years. Can J Cardiol. 1996;12(3):297-299.
11. Jaeggi ET, Hamilton RM, Silverman ED,Zamora SA, Hornberger LK. Outcome ofchildren with fetal, neonatal or childhooddiagnosis of isolated congenital atrioven-tricular block: a single institution’s experi-ence of 30 years. J Am Coll Cardiol. 2002;39(1):130-137.
12. Michaelsson M, Riesenfeld T, Jonzon A.Natural history of congenital complete atri-oventricular block. Pacing Clin Electrophys-iol. 1997;20(8, pt 2):2098-2101.
13. Beaufort-Krol GC, Schasfoort-van LeeuwenMJ, Stienstra Y, Bink-Boelkens MT. Longi-tudinal echocardiographic follow-up inchildren with congenital complete atrioven-tricular block. Pacing Clin Electrophysiol. 2007;30(11):1339-1343.
14. Michaelsson M, Jonzon A. Isolated congen-ital complete atrioventricular block in adultlife. Circulation. 1995;92:442-449.
15. Vukomanovic V, Stajevic M, Kosutic P, et al.Age-related role of ambulatory electrocardio-graphic monitoring in risk stratification ofpatients with complete congenital atrioven-tricular block. Europace. 2007;9(2):88-93.
16. Marriott H, Conover M. Advanced Conceptsin Arrhythmias. 3rd ed. St Louis, MO: Else-vier Health Sciences; 1998.
17. Huff J. ECG Workout Exercises in ArrhythmiaInterpretation. 5th ed. Philadelphia, PA: Lip-pincott Williams & Wilkins; 2006:155.
18. Garcia T, Holtz N. 12-Lead ECG: The Art ofInterpretation. Sudbury, MA: Jones & BartlettPublishers; 2001:68-69.
19. Huszar RJ. Basic Dysrhythmias. 3rd ed. StLouis, MO: Mosby; 2002:179-181.
20. Rakel R, Bope E. Conn’s Current Therapy.Philadelphia, PA: WB Saunders Co; 2001:285.
21. Ross BA. Congenital complete atrioventric-ular block. Pediatr Clin North Am. 1990;37(1):69-77.
22. Holler T. Cardiology Essentials. Sudbury, MA:Jones & Bartlett Publishers Inc; 2008:127.
23. Beaufort-Krol CM, Stienstra Y, Bink-BoelkensM. Sinus node function in children withcongenital complete atrioventricular block.Europace. 2007;9(9):844-847.
24 Porth C. Essentials of Pathophysiology. 2nd ed.Philadelphia, PA: Lippincott Williams &Wilkins; 2007:426.
25. Dewey RC, Capeless MA, Levy AM. Use ofambulatory electrocardiographic monitor-ing to identify high-risk patients with con-
genital complete heart block. N Engl J Med.1987;316:835-839.
26. Weng KP, Chiou CW, Huang SH, Lin CC,Hsieh KS. The long-term outcome of chil-dren with isolated congenital complete atri-oventricular block. Acta Paediatr Taiwan.2005;46(5):260-267.
27. Hanisch D. Pediatric arrhythmias. J PediatrNurs. 2001;16:351-362.
28. Artificial pacemakers. American Heart Asso -ciation Web site. http://www.americanheart.org/presenter.jhtml?identifier=24. UpdatedJanuary 20, 2009. Accessed July 8, 2009.
29. Medtronic Web site. About bradycardia(slow heartbeat). http://www.medtronic.com/your-health/bradycardia/index.htm.Accessed July 17, 2009.
30. Cleveland RF Jr, Ulcek JL. Questions andAnswers About Biological Effects and PotentialHazards of Radiofrequency ElectromagneticFields. 4th ed. OET Bulletin 56. WashingtonDC: Office of Engineering and Technology,Federal Communications Commission:August 1999. http://www.fcc.gov/Bureaus/Engineering_Technology/Documents/bulletins/oet56e4.pdf. Accessed July 9, 2009.
31. Radiofrequency safety. Federal Communi-cations Commission Web site. http://www.fcc.gov/oet/rfsafety/rf-faqs.html#Q22.Updated December 11, 2008. Accessed July15, 2009.
56 CriticalCareNurse Vol 29, No. 5, OCTOBER 2009 www.ccnonline.org
eLettersNow that you’ve read the article, create or contributeto an online discussion about this topic using eLetters.Just visit www.ccnonline.org and click “Respond toThis Article” in either the full-text or PDF view ofthe article.
by AACN on May 10, 2018http://ccn.aacnjournals.org/Downloaded from

CE Test Test ID C0952: Complete Congenital Atrioventricular Block in a Young Man: A Case StudyLearning objectives: 1. Discuss the pathophysiology of complete congenital atrioventricular block 2. Identify the clinical features of complete congenital atrioventricular block 3. Describe 3 teaching points for a patient with a pacemaker
Program evaluationYes No
Objective 1 was met � �Objective 2 was met � �Objective 3 was met � �Content was relevant to my
nursing practice � �My expectations were met � �This method of CE is effective
for this content � �The level of difficulty of this test was: � easy � medium � difficult
To complete this program, it took me hours/minutes.
Test answers: Mark only one box for your answer to each question. You may photocopy this form.
1. What is one of the diagnostic criteria for complete congenitalatrioventricular block (CCAVB)?a. Complete heart block at birth as indicated by electrocardiographic
(ECG) findingsb. Endocarditis in fetus at 30 weeksc. Rapid heart rate at birth as indicated by echocardiographic findingsd. Incomplete atrial septal defect closure at 5 years old
2. Which of the following disorders is CCAVB associated withwhen diagnosed in utero?a. Congestive heart failure c. Fetal antibody syndromeb. Neonatal lupus syndrome d. Fetal alcohol syndrome
3. Which of the following maternal problems is associated withCCAVB?a. Gestational diabetes c. Myocarditisb. Congestive heart failure d. Connective tissue disorders
4. What are the main causes of early death due to in CCAVB?a. Myocardial infarction and sudden cardiac deathb. Cardiac failure associated with cardiomyopathy and sudden
cardiac deathc. Adam-Stokes attack with heart failure and myocarditis d. Connectives tissue disorders and myocardial infarction
5. What is the ECG characterization of CCAVB?a. No P waves only QRSb. Absent conduction of impulse from atria to ventriclec. Rapid atrial and ventricular heart ratesd. Irregular PR interval
6. What is the inherent rate of automaticity of the ventricular pacemaker?a. 100-120 minutes c. 40-60 minutesb. 60-100 minutes d. 20-40 minutes
7. What are the 2 components of cardiac output?a. Heart rate and stroke volumeb. Systolic blood pressure and heart ratec. Stroke volume and systolic blood pressured. Stroke volume and diastolic blood pressure
8. Which of the following statements about CCAVB is false?a. The signs and symptoms are not related to the baseline
ventricular rate and underlying structural defects.b. Patients may be asymptomatic until cardiac decompensation
begins to occur in adulthood.c. Common overt indications include slow heart rate, fainting, and
presyncopal spells.d. Signs and symptoms of low cardiac output and exercise intolerance
are sometimes subtle and are often contributed to other causes.
9. Which of the following could be a subtle sign or symptom ofcardiac fatigue?a. Severe chest pain with exerciseb. Syncopec. Tiredness and frequent naps d. Acute dyspnea
10. Which of the following ECG characteristics is an unfavorableprognostic sign because it may be related to potential myocardialdamage in patients with CCAVB?a. Ventricular rhythm with a QRS complex >120 ms and a QTc >450 msb. Atrial rhythm with a QRS complex <80 ms and a PR interval of
0.16 msc. Ventricular rhythm with a QRS complex <80 ms and a QTc <400 ms d. Atrial rhythm with flutter waves and intermittent QRS at 3:1 rate
11. What are the 2 primary goals of pacemaker insertion for apatient with CCAVB?a. Decrease in functional capacity and prevention of paroxysmal
nocturnal dyspneab. Increase in functional capacity and prevention of sudden cardiac
deathc. Correction of heart rhythm and stabilization of thrombocytopeniad. Reversal of connective tissue disorder and prevention of pancytopenia
12. Patients with pacemakers should do which of the following?a. Not use cell phones because they damage the pulse generatorb. Avoid participating in all types of sportsc. Have pacemaker checks done only when they feel palpations or dizzyd. Avoid strong magnet fields because pacemaker functioning may
be altered
For faster processing, takethis CE test online atwww.ccnonline.org
(“CE Articles in this issue”)or mail this entire page to:
AACN, 101 Columbia Aliso Viejo, CA 92656.
Test ID: C0952 Form expires: October 1, 2011 Contact hours: 1.0 Fee: AACN members, $0; nonmembers, $10 Passing score: 9 correct (75%) Category: CERP A, Synergy CERP ATest writer: Jane Baron, RN, CS, ACNP
1. �a�b�c�d
Name Member #
Address
City State ZIP
Country Phone
RN Lic. 1/St RN Lic. 2/St
Payment by: � Visa � M/C � AMEX � Discover � Check
Card # Expiration Date
SignatureThe American Association of Critical-Care Nurses is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation.
AACN has been approved as a provider of continuing education in nursing by the State Boards of Nursing of Alabama (#ABNP0062), California (#01036), and Louisiana (#ABN12). AACN programming meets the standards for most other states requiring mandatory continuing education credit for relicensure.
9. �a�b�c�d
8. �a�b�c�d
7. �a�b�c�d
6. �a�b�c�d
5. �a�b�c�d
4. �a�b�c�d
3. �a�b�c�d
2. �a�b�c�d
12. �a�b�c�d
11. �a�b�c�d
10. �a�b�c�d
by AACN on May 10, 2018http://ccn.aacnjournals.org/Downloaded from

Connie S. ChronisterCongenital Complete Atrioventricular Block in a Young Man: A Case Study
http://ccn.aacnjournals.org/Published online ©2009 American Association of Critical-Care Nurses
10.4037/ccn2009297 45-56 29 2009;Crit Care Nurse
http://ccn.aacnjournals.org/cgi/external_ref?link_type=PERMISSIONDIRECTPersonal use only. For copyright permission information:
http://ccn.aacnjournals.org/subscriptions/Subscription Information
http://ccn.aacnjournals.org/misc/ifora.xhtmlInformation for authors
http://www.editorialmanager.com/ccn Submit a manuscript
http://ccn.aacnjournals.org/subscriptions/etoc.xhtmlEmail alerts
362-2049. Copyright ©2016 by AACN. All rights reserved. bimonthly by AACN, 101 Columbia, Aliso Viejo, CA 92656. Telephone: (800) 899-1712, (949) 362-2050, ext. 532. Fax: (949) Critical Care Nurse is an official peer-reviewed journal of the American Association of Critical-Care Nurses (AACN) published
by AACN on May 10, 2018http://ccn.aacnjournals.org/Downloaded from