Embed Size (px)
Citation preview

Hindawi Publishing CorporationDermatology Research and PracticeVolume 2012, Article ID 984096, 8 pagesdoi:10.1155/2012/984096
Clinical Study
Clear Cell Sarcoma (Malignant Melanoma) of Soft Parts:A Clinicopathologic Study of 52 Cases
O. Hocar,1 A. Le Cesne,2 S. Berissi,1 P. Terrier,2 S. Bonvalot,2 D. Vanel,3 A. Auperin,4
C. Le Pechoux,2 B. Bui,5 J. M. Coindre,5 and C. Robert1
1 Melanoma Committee, Gustave Roussy Institute, 114 Rue Edouard Vaillant, 94805 Villejuif, Cedex, France2 Sarcoma Committee, Gustave Roussy Institute, 114 Rue Edouard Vaillant, 94805 Villejuif, Cedex, France3 Department Of Radiology, Gustave Roussy Institute, 114 Rue Edouard Vaillant, 94805 Villejuif, Cedex, France4 Department Of Biostatistics And Epidemiology, Gustave Roussy Institute, 114 Rue Edouard Vaillant, 94805 Villejuif, Cedex, France5 Sarcoma Group Of Bergonie Institute, 229 Cours De L’argonne, 33076 Bordeaux, Cedex, France
Correspondence should be addressed to O. Hocar, [email protected]
Received 30 December 2011; Revised 16 March 2012; Accepted 25 March 2012
Academic Editor: Drazen Jukic
Copyright © 2012 O. Hocar et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Clear cell sarcomas are aggressive, rare soft tissue tumors and their classification among melanoma or sarcoma is still undetermineddue to their clinical, pathologic, and molecular properties found in both types of tumors. This is a retrospective study of 52patients with CCS seen between April 1979 and April 2005 in two institutions. The EWS-ATF-1 fusion transcript was studiedin 31 patients and an activating mutation of the BRAF or NRAS gene was researched in 22 patients. 30 men and 22 women,with a mean age of 33 were studied. Forty-three tumors (82.69%) were located in the extremities, specially the foot (19 tumors).Median initial tumor size was 4.8 cm (1 to 15 cm). Necrosis involving more than 50% of the tumor cells was found in 14 cases(26.92%). High mitotic rate (>10) was found in 25 cases (48.07%). The EWS/ATF-1 translocation was found in 28 (53.84%) of 31patients studied, and mutation of BRAF or NRAS was found in only 2 of 22 patients analyzed cases (3.84%). Among the tumor-associated parameters, only tumor size (>4 cm) emerged as a significant prognostic factor. Forty-nine patients had a localizeddisease at diagnosis (94.23%) and underwent surgical resection immediately (90%) or after neoadjuvant chemotherapy (CT)(10%). Various CT regimens were used in 37 patients (71.15%) with no significant efficacy. The 5- and 10-year OS rates were 59%and 41%, respectively. Tumor size was the only emerging prognosis factor in our series. Complete surgical resection remains theoptimal treatment for this aggressive chemoresistant tumor.
1. Introduction
Clear cell sarcoma (CCS) is a rare malignant tumor that wasdescribed first by Enzinger in 1965 [1]. CCS shows a predilec-tion for the deep soft tissues of the lower extremities close tothe tendon, fascia, or aponeuroses [2]. It occurs preferentiallyin adolescents and young adults and is associated with ahigh propensity of local recurrence, regional lymph nodemetastases, and distant metastases [1, 2]. Because of its closeclinic and histologic kinship with malignant melanoma (highfrequency of lymph node metastases, presence of melanin,ultrastructural evidence of melanosomes, and immuno-histochemical staining for S-100 protein and melanoma-associated antigen HMB-45), Chung and Enzinger proposedthe name malignant melanoma of soft parts [2]. However,
despite these similarities, CCS and melanoma should beconsidered 2 distinct entities. Unlike melanomas, mostCCS tumors are characterized by a recurrent chromosomaltranslocation, t(12; 22), resulting in fusion of the EWS geneon 22q12 with the ATF1 gene on 12q13 [3]. Several fusiontranscript types have been described, with a predominanceof type 1 fusing exon 8 of EWS with exon 4 of ATF1 andtype 2 fusing exon 7 of EWS with exon 5 of ATF1 [4].The prevalence of t(12; 22) fusion transcripts detected bymolecular techniques has been reported in only 3 small seriesof 10 patients, 12 patients, and 9 patient with CCS [3–5].
High incidence of activating mutations in the BRAF genehas been reported in melanoma cell lines, melanoma short-term cultures, primary and metastatic melanomas, and nevi[6]. All the mutations were detected in the kinase domain

2 Dermatology Research and Practice
of the BRAF gene and found in exons 11 and 15. Themost common mutation (V599E) is the T1796A single-basesubstitution in exon 15, leading to an exchange of valine forglutamic acid at position 599 [6].
This mutation was not reported in soft tissue sarcomasincluding a small series of 8 CCS [4]. Compared with theextensive literature regarding the histopathologic nature ofthe disease, very little is known about the clinical andmolecular features of CCS. The main obstacle to gaining athorough understanding of the clinical and molecular behav-ior of CCS is the rarity of the disease.
We describe the clinicopathological data of 52 patientswith clear cell sarcoma with emphasis on prognostic factorsand treatment outcomes. Mutational status on BRAF, NRASgene, and cytogenetic study of translocation (12, 22) (q13,q12) were also studied (Table 1).
2. Patients and Methods
Between April 1979 and April 2005, 52 consecutive casesof CCS were registered at the Gustave Roussy, Villejuif (46patients) and Bergonie, Bordeaux (6 patients) institutes.
Complete information on clinical data, treatment modal-ities, and outcome was reviewed in all cases to exclude anantecedent or a concurrent diagnosis of primary cutaneousmelanoma. When the initial biopsies were done outside theinstitutes, the histopathologic diagnosis was confirmed byGustave Roussy or Bergonie Institute expert of pathologists.Histologic criteria for the diagnosis of CCS are the intimateassociation of small solid aggregates of round-to-fusiform,pale-staining cells within the dense connective tissue of ten-dons and aponeuroses, the fine reticular stroma surroundingthe cells, the relative uniformity of cells showing abundantclear cytoplasm, and scattered multinucleated giant cells.Mitotic figures are generally infrequent. A confirmationof diagnosis is obtained by immunohistochemistry with adiffuse or focal positivity for S-100 protein and melanocyte-associated antigen HMB-45, positivity for neuron-specificenolase (NSE). Thirty-one cases were examined for thepresence of EWS/ATF1 transcripts by real-time PCR onparaffin-embedded tissues and frozen samples.
DNA was prepared from paraffin-embedded tissues of 22CCS (16 cases from GRI, 6 cases from BI) carrying the t(12;22) translocation. PCR amplification of BRAF exons 11 and15 as well as NRAS codons 12, 13, and 61 was performed, andPCR products were sequenced.
The following demographic and treatment factors wereexamined for prognostic importance: patient age (≤30years, >30 years), sex, tumor size (≤4 cm, >4 cm), location,symptoms, clinical staging, microscopic surgical margin,chemotherapy and radiotherapy, mitotic rate (>2 per 10 highpower fields after examining and averaging data from 20HPF), and presence of necrosis.
With respect to tumor location, proximal sites includedthe trunk and proximal extremities (upper arm and thigh),and distal sites included distal extremities (below or atthe elbow and below or at the knee joint). The micro-scopic surgical margin was determined histologically on the
resected specimens and was classified as negative (no tumorcells at the inked margin) or positive (tumor cells at theinked margin). Patients received multimodality treatment,including surgery, radiotherapy, and chemotherapy. Wideexcision of the primary tumor with a negative surgicalmargin was attempted whenever possible. If necessary,amputation/disarticulation was planned to achieve a nega-tive surgical margin.
All time-to-event endpoints were computed by using thekaplan-Meier method [7].
Patients who died of causes unrelated to CCS werecensored at time of death. Potential prognosis factors wereidentified by univariate analysis using the log-rank test.Independent prognostic factors were evaluated with Coxproportional-hazards regression using a stepwise selectionprocedure [8]. To arrive at a parsimonious multivariatemodel, covariates were selected into the model only if theycontributed significantly to the fit of the model. The criterionused to select covariates into the model was the score chi-square statistic. Differences at P < .05 were consideredsignificant. Statistical analyses were performed using theStatView 5 statistical package.
3. Results
The study group comprised 30 men (57.69%) and 22 women(42.30%), and patients ranged in age from 6 years to 81 years(median, 33 years). Forty-two percent of patients were aged≤30 years, and 94% were aged <60 years.
Forty-three tumors (82.69%) were located in the extrem-ities, eight tumors (15.38%) were located in the trunk, andone tumor was located in the scalp. The most commontumor site was the foot (19 tumors), followed by thehand (13 tumors), and the thigh (9 tumors). Fourteentumors (26.92%) were considered proximal, and 38 tumors(73.07%) were considered distal.
Fifty patients (96.15%) had a mass that had been enlarg-ing slowly for periods ranging from six weeks to four years(median, 15 weeks). Pain and/or tenderness were observedin 30 patients (57.69%), and this was frequently the mainreason for seeking medical advice. In two patients, acuteurinary retention was the first sign of the disease. No patientshad a history of melanoma or unusual pigmented skinlesions.
At presentation the malignant nature of the swellingwas seldom suspected, and in thirty-six patients (69.23%),a biopsy was performed. Nevertheless in sixteen patients(30.76%), the lesion was thought to be benign on clinicalgrounds, and initial clinical diagnosis included epithelial cyst(7 patients) exostose (4 patients), haematoma (2 patients),and neurinoma, lipoma, and carpal tunnel syndrome (1patient each).
Initial diagnosis was made at another institution in allcases, with incisional or excisional biopsy. All cases werereviewed by the Gustave Roussy or the Bergonie Institute softtissue pathologists.
The tumors ranged in size from 1 cm to 15 cm (median,4, 86 cm). The tumors measured <4 cm in 30 patients

Dermatology Research and Practice 3
Ta
ble
1:C
lear
cell
sarc
omas
:clin
ical
,his
tolo
gica
l,m
olec
ula
r,th
erap
euti
c,an
dfo
llow
-up
data
.
Cas
eA
geSe
xSi
teSi
ze(c
m)
Trea
tmen
t(∗
)C
HT
regi
men
sSu
rgic
alm
argi
nL
Rec
(∗∗ )
LNM
et(∗∗ )
Met
(∗∗ )
FU (∗∗ )
Stat
us
EW
S-A
TF1
Mit
oses
Nec
rose
Gra
deB
RA
F15
NR
AS
611
36F
Bu
ttoc
k6
Surg
+R
+C
TIV
Apo
sn
on
o77
804
pos
100
2n
egn
eg2
23F
Shou
lder
9C
T+
Surg
+R
Adr
ipo
sn
on
o9
124
pos
341
3n
egn
eg3
11M
Hee
l4
CT
+Su
rg+
RI
neg
no
no
2340
4po
s12
13
neg
neg
453
FFo
ot6
CT
+Su
rg+
RIV
An
eg14
no
716
1po
s6
12
neg
neg
557
FFo
rear
m5
Surg
+R
neg
23n
on
o45
0po
s5
02
neg
neg
623
MFo
ot2,
5Su
rg+
R+
CT
MA
ID;M
TX
,Cn
egn
on
on
o11
0po
s5
02
neg
neg
734
FFo
rear
m4
Surg
+C
T+
RA
dri,I
,Cis
pl,F
,D
itic
pos
10
08
4po
s18
13
ni
ni
820
MH
and
4C
T+
surg
+R
Adr
i,D
TIC
,lim
bp
erf
neg
no
no
no
280
pos
101
2n
in
i
946
FH
and
1,2
Surg
neg
24n
on
o40
0po
s5
12
ni
ni
1054
MFo
ot3
Surg
+C
TM
AID
;MT
X,C
pos
1n
o5
244
pos
182
3n
in
i11
45F
Foot
3Su
rg+
Rpo
sn
on
on
o12
?po
s8
12
ni
ni
1248
MFo
ot1,
8Su
rg+
Rpo
sn
on
on
o60
0po
s3
23
neg
neg
1337
MFo
ot2
Surg
+R
+C
T4
E+
I,D
pos
no
no
5712
01
pos
20
2n
in
i14
33M
Leg
4Su
rg+
R+
CT
6I
neg
no
8787
964
pos
102
2n
in
i15
31M
Foot
?Su
rg+
CT
+R
INF+
Adr
i+T
/EI
neg
no
010
164
pos
202
3n
in
i16
37F
Foot
2Su
rg+
R+
CT
Adr
i+I
pos
no
no
no
870
pos
90
2n
egn
eg17
42F
Leg
6Su
rg+
CT
+R
Adr
i+I
pos
no
54n
o60
1n
eg15
12
neg
neg
1851
MT
hig
h15
Surg
+R
+C
TA
dri+
I+D
TIC
pos
24n
o33
604
pos
122
3n
in
i19
9M
Sacr
um
7Su
rg+
R+
CT
IVA
pos
12n
o12
204
ni
41
2n
in
i20
31M
Kn
ee10
Surg
+C
T+
RI+
C+
V+
DIT
Cn
egn
o18
no
204
pos
21
2n
egn
eg21
45M
Kn
ee4
Surg
+C
T+
RV
AC
An
egn
on
on
o48
0n
i3
22
ni
ni
2229
FFo
ot3
Surg
+R
neg
12n
o16
404
pos
91
2n
egn
eg23
26M
Foot
3Su
rg+
CT
+R
Adr
i+I
neg
144
no
228
312
1po
s5
12
neg
neg
2438
FT
hig
h6
Surg
+C
T+
RV
AC
Apo
s12
3652
604
ni
91
2n
in
i
2517
MB
ehin
dbl
adde
r4
Surg
+C
TA
dri+
In
egn
on
on
o65
0po
s10
12
ni
ni
266
FA
rm8
Surg
+C
TV
+C
arbo
+ep
iru
bici
npo
s1
0n
o18
00
ni
91
3n
in
i
2715
FSc
apu
la5
Surg
+C
TC
arbo
+A
dria
,IL
2po
s10
no
1224
4n
i2–
41
2n
in
i
2836
MT
ibia
3Su
rg+
CT
Adr
i+I
pos
1620
2228
4n
i10
12
ni
ni
2915
FSc
apu
la5
Surg
+C
TIV
A,I
L2,
DT
ICn
egn
on
on
o12
0n
i4
12
ni
ni
3020
FSc
alp
4Su
rg+
CT
+R
I+A
dri
pos
8472
9612
04
neg
21
2n
egn
eg31
33F
Han
d3
Surg
+C
T+
RA
dri
pos
4830
3652
4n
i10
12
ni
ni
3232
MPe
lvis
9Su
rg+
CT
+R
I+A
dri
neg
610
2132
4n
i10
12
ni
ni
3312
FFo
ot3
Surg
+C
T+
RIV
Apo
sn
on
on
o14
40
ni
21
3n
in
i34
14M
Wri
st5
a6
Surg
+C
T+
RIV
An
egn
on
on
o12
00
ni
101
2n
in
i
3529
MH
eel
2Su
rg+
CT
+R
V+
DIT
C+
Adr
i+
Cn
eg24
no
7682
4n
i19
12
ni
ni

4 Dermatology Research and Practice
Ta
ble
1:C
onti
nu
ed.
Cas
eA
geSe
xSi
teSi
ze(c
m)
Trea
tmen
t(∗
)C
HT
regi
men
sSu
rgic
alm
argi
nL
Rec
(∗∗ )
LNM
et(∗∗ )
Met
(∗∗ )
FU (∗∗ )
Stat
us
EW
S-A
TF1
Mit
oses
Nec
rose
Gra
deB
RA
F15
NR
AS
6136
28M
Wri
st3
a4
Surg
+C
T+
RIV
A,I
L2,
DT
ICpo
sn
on
o24
394
ni
111
2n
in
i37
10M
Hip
5,5
Surg
+C
T+
RIV
Apo
s68
72n
o12
00
pos
181
2n
egn
eg38
24M
Foot
3Su
rg+
Rpo
sn
on
on
o15
60
ni
31
2n
egn
eg39
13M
Leg
3Su
rg+
CT
+R
VA
CA
neg
3030
no
348
0n
i21
12
ni
ni
4047
FFo
ot3
Surg
+C
T+
RV
AC
An
eg24
no
no
240
1n
i12
12
ni
ni
4176
Ffo
ot4
Surg
pos
12n
o12
424
ni
21
3n
in
i42
34M
Wri
st1
Surg
+C
T+
RV
AC
An
eg56
no
no
264
0po
s10
12
neg
pos
4340
MLe
g4
Surg
+C
T+
RV
AC
Apo
s60
no
8496
4n
eg7
22
neg
neg
4412
FFo
ot14
Surg
+R
neg
36n
on
o84
0n
i5
22
ni
ni
4573
MSc
apu
la10
Surg
+C
T+
RA
dri+
V+
C+
Pla
tpo
s48
3624
964
ni
292
3n
in
i
4620
MSc
apu
la6
CT
+Su
rg+
RA
dri+
V+
DT
IC+
Cpo
s18
1818
244
pos
81
2n
egn
eg
4733
MFo
ot5
Surg
+C
TF
pos
164
431
4po
s9
12
neg
neg
4881
FFo
ot3
Surg
pos
240
no
250
254
4n
i9
22
ni
ni
4946
MFo
ot4
Surg
+C
T+
RI
neg
6072
250
260
4po
s24
23
pos
neg
5047
MH
and
6Su
rg+
CT
+R
VA
CA
neg
no
no
9614
44
pos
152
2n
egn
eg51
29F
Foot
2Su
rgpo
sn
o60
no
601
ni
102
2n
in
i
5230
Mkn
ee10
Surg
+C
T+
RC
+V
+A
dri+
DT
ICpo
sn
o6
1836
4po
s5
22
neg
neg
((∗ )
Surg
:su
rger
y,R
:rad
ioth
erap
y,C
T:c
hem
oth
erap
y.(∗∗ )
LRec
:loc
alre
curr
ence
(mon
ths)
,LN
Met
:loc
oreg
ion
ally
mph
nod
em
etas
tasi
s(m
onth
s),M
et:d
ista
ntm
etas
tasi
s(m
onth
s),a
nd
FU:f
ollo
wu
p(m
onth
s).
Stat
us:
0:al
ive
wit
hn
odi
seas
e,1:
aliv
ew
ith
dise
ase,
and
4:di
edof
dise
ase.
Mit
oses
:n
um
ber
ofm
itos
espe
rte
nh
igh
pow
erfi
elds
.n
eg:
neg
ativ
e,po
s:po
siti
ve,
ni:
not
iden
tifi
ed.
Nec
rosi
s:0:
no
nec
rosi
s,1:
less
than
50%
ofn
ecro
sis,
2:m
ore
than
50%
ofn
ecro
sis)
.A
:ac
tin
omyc
inD
;A
dri:
Adr
ibla
stin
a,C
:cy
clop
hos
pham
ide,
Car
bo:
carb
opla
tin
,ci
splt
:ci
spla
tin
;D
ITIC
:da
carb
azin
e,E
PI:
eopo
side
,F:
fote
mu
stin
e;I:
ifos
fam
ide,
IL2:
Inte
rleu
kin
2,IV
A:
ifos
fam
ide
(3g/
m2)
+da
ctin
omyc
in(1
,5m
g/m
2)
+vi
ncr
isti
ne
(1,5
mg/
m2);
Lim
bpe
rf:
regi
onal
isol
ated
limb
per
fusi
onw
ith
mel
phal
anan
dtu
mor
nec
rosi
sfa
ctor
alph
a,M
TX
:met
hot
rexa
te,M
AID
:dox
oru
bici
n(1
5m
g/m
2)
+da
carb
azin
e(2
50m
g/m
2/j
)+
ifos
fam
ide
(2–2
,85
g/m
2/j
),V
:vin
cris
tin
e;V
AC
A:c
yclo
phos
pham
ide
(1,2
g/m
2)
+do
xoru
bici
n(3
0m
g/m
2)
+da
ctin
omyc
in(0
,5m
g/m
2)
+vi
ncr
isti
ne
1,5
mg/
m2;I
NF:
intr
fero
n;T
:tax
ol.

Dermatology Research and Practice 5
(57.69%) and between 4 cm and 15 cm in 21 patients(40.38%). Tumor size was unknown in one patient.
In all cases, the tumor cells were arranged in nests, clefts,and an alveolar pattern, separated by fibrous septa. Somedyscohesive cells were seen lying in spaces. The cells showednecrosis less than 50% in 33 patients (63.46%), more than50% in 14 patients (26.92%), and no evidence of necrosis in 5patients (09.61%). Of the fourteen patients who had necrosismore than 50%, ten patients died. The number of mitoseswas less than 10 per high power fields (10 HPF) in 27 patients(51.92%), between 10 and 20 per 10 HPF in 21 patients(40.38%), and more than 20 per HPF in 4 patients (7.69%).Forty tumors (76.92%) were grade 2, and twelve tumors(23.07%) were grade 3 using the FNCLCC grading system.
HMB45 was diffusely positive in forty-four tumors(84.61%) and focally positive in 8 patients (15.38%). S100protein was largely positive in forty-four patients (84.61%),focally positive in 5 cases (09.61%), and negative in 3 cases(5.76%). Melan A and MITF were expressed in many cases(76.92% and 84.6% of cases, resp.) including S100 protein-negative tumors. Vimentin could be detected in 3 cases(5.76%). None of our cases had expressions of keratin.Only one of the 22 CCS harboured a BRAF mutation(V599E); it was the well-known valine to glutamic acidchange in position 599. No exon 11 mutation were found.One mutation of NRAS (codon 61) was also found with nooverlap with the BRAF mutation. The EWS/ATF-1 fusiontranscript was detected in 28 patients of the 31 paraffin-embedded CCS, and 3 of the 31 patients were negative. Thetwo tumours that presented a BRAF or NRAS mutation alsopresented the ATF1-EWS fusion gene and were consideredatypical. However, the absence of cutaneous involvement,histologic features (spindle and a few epithelioid cellsarranged in a nested pattern), and immunohistochemistry(diffuse positivity for S100 protein and HMB45) stronglysuggested a diagnosis of CCS.
Forty-nine patients (94.23%) presented with localizeddisease; forty-four patients (84.61%) of them underwentsurgical resection of primary tumor. Nineteen patients(36.53%) underwent complete surgical resection with neg-ative margins; twenty-five patients (48.07%) had residualmicroscopic disease and underwent adjuvant therapy espe-cially radiotherapy.
The last five patients with localized disease receivedneoadjuvant chemotherapy before surgical resection in orderto reduce tumors size and make surgical resection possible.
Two patients (3.84%) presented with disease metastaticto lymph nodes. One patient presented with disease me-tastatic to both lymph nodes and lung.
Definitive surgical management included wide local exci-sions in 29 patients, local excision in 11 patients, radicalcompartment resection in 4 patients, and amputation in 3patients. Adjuvant treatment was given to 42 patients andconsisted of radiotherapy in 40 patients (76.92%) witha median of 50 grays. This radiotherapy was associatedto adjuvant chemotherapy in 10 patients, and 2 patientsreceived adjuvant chemotherapy alone.
patients (55, 76%) developed local recurrence. The timeinterval from initial treatment to local relapses ranged from
1 month to 20 years, with a median of 38 months. Localrecurrence was seen in 55% of the 29 patients at 5 years and63% at 10 years. Sixteen of these patients received additionalsurgical treatment and 3 had amputation. Of the other 10patients (19.23%), they were already known to have regionallymph node metastases and/or had disseminated disease.Of the 29 patients (55, 76%) who had local recurrences, 19(36.53%) died of the tumors, three (5.76%) are alive withdisease, but only seven (13.46%) patients are alive free ofdisease.
No local recurrences occurred in 23 patients (44.23%)who had surgical resection with negative margins (16patients) or with positive margins associated to adjuvantradiotherapy (7 patients). The overall survival rate withoutlocal recurrence was 30% at 5 years and 16% at 10years.
Nineteen patients developed regional lymph node metas-tases at 5 years in 34% and at 10 years in 41% of them.Of these patients, six (11.53%) had lymph node metastaseswithin less than 1 year of the followup, three patients (5.76%)between 1 and 2 years, and 10 patients (19.23%) between 2and 7 years of the followup. Regional lymph node dissectionwas performed on fourteen patients and was associated withregional isolated limb perfusion with melphalan and tumornecrosis factor alpha in one case. Five patients had alreadydistant metastases.
Thirty patients developed distant metastases: 43% ofthem at 5 years and 62% at 10 years. Of them, twenty-seven patients died because of disease and three are alivewith disease (time of followup: 09, 63, 84 months). Distantmetastases most frequently involved the lungs (27 patients),bones (2 patients), and distant lymph nodes (1 patient).
Twenty-four patients received some form of chemother-apy, and three patients had surgical treatment (accessiblemetastases sites and single localisation).
Various chemotherapeutic regimens for musculoskeletalsarcomas or for malignant melanoma, in adjuvant aim orin curative one, were employed, including actinomycin,Adriblastina, cyclophosphamide, carboplatine, cisplatine;dacarbazine, etoposide, fotemustine; iosfamide, interleukin2, ifosfamide (3 g/m2) + dactinomycin (1,5 mg/m2) +vincristine (1,5 mg/m2); regional isolated limb perfu-sion with melphalan and tumor necrosis factor alpha,methotrexate, MAID: doxorubicine (15 mg/m2) + dacar-bazine (250 mg/m2/j) + ifosfamide (2–2,85 g/m2/j), vin-cristine; VACA: cyclophosphamide (1,2 g/m2) + doxoru-bicine (30 mg/m2) + dactinomycin (0,5 mg/m2) + vincristine1,5 mg/m2; intrferon and taxol.
In twenty-one patients, chemotherapy was discontinued,usually after three courses, because of tumor progression(18 patients) or major hematotoxicity (3 patients). Localradiotherapy for distant metastases sometimes briefly allevi-ated the pain and was mostly given to patients with skeletalmetastases.
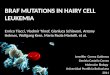
The overall survival rate was 59% at 5 years and 41%at 10 years (Figure 1). Median time of follow up was 120months (11–348). On multivariate analysis, only tumor size(P : 0.01) emerged as a significant prognostic factor (Table 2and Figure 2).

6 Dermatology Research and Practice
77810101414171921272936435052
0
0.2
0.4
0.6
0.8
1
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
59%
41%
Overall survival
YearsAge
Figure 1: Overall survival of 52 patients with clear cell sarcoma.
Table 2: Multivariate analysis of overall survival.
Variable Number5-year survival
univariate PEvent-freeSurvival
Sex
Men 30 0,83 0,70
Women 22
Age
≤30 y 22 0,32 0,38
>30 y 30
Size
≤4 cm 30 0,06 0,01
>4 cm 21
Mitoses
<10 27 0,61 0,44
≥10 25
Necrosis
<50% 38 0,66 0,47
≥50% 14
Grade
2 40 0,19 0,16
3 12
4. Discussion
These results confirmed the known clinical features ofCCS originally reported by Enzinger [1]: arising primarilyin young adults, predominance in distal extremities, andpresenting as a slowly enlarging mass that has been evidentfor several months or even years. The principal sites of theneoplasm are the extremities, especially the region of thefoot and ankle. The head, neck, and trunk regions are onlyrarely involved. In our study, forty-three tumors (82.69%)were located in the extremities. The most common tumorsite was the foot (19 tumors). Fourteen tumors (26.92%)were considered proximal, and 38 tumors (73.07%) wereconsidered distal. Our findings also revealed several impor-tant factors that predict the clinical behavior of CCS anddisclosed problems awaiting solution.
0
0.2
0.4
0.6
0.8
1
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Years
Size <= 4Size > 4
Risk30 27 22 15 15 12 7 6 4 4 4 4 4 2 1 121 14 8 6 5 4 3 2 2 1 1
Event-free survival
log rank P = 0.01
Figure 2: Event-free survival of 52 patients with clear cell sarcomaaccording to tumor size (P = 0.01).
Over half of all clear cell sarcoma reported in theliterature measured less than 4 cm [2], a finding in accordwith our series in which 57.69% of patients had lesions thatmeasured less or equal to 4 cm. CCS mainly afflicts youngadults between the ages of 20 to 40 years [4, 5], but inrare instances it may occur in the extremes of ages. In ourstudy, the mean age was 33 and 26 years (range 6–81 years).Although some reports have found predominance in females[6], the gender distribution between males and females isequal [2]. CCS was slightly more common in male than fe-male patients in our series.
CCS is characterized by a recurrent chromosomal trans-location t(12; 22), which results in fusion of the EWS geneon 22q with the ATF1 gene on 12q [4]. This genomic abnor-mality may represent a good marker for identifying thesetumors. In the current study, 90.32% of the analyzed tumors(28 of 31 tumors) had this translocation.
As previous studies [4–7], our data further suggests thatCCS and conventional melanoma develop through differ-ent genetic pathways. Indeed, CCS is a sarcoma subtype,and the characteristic EWS/ATF1 translocation, resultingin the chimeric protein EWS/ATF1, is responsible for themelanocytic differentiation. EWS/ATF1 can bind the tran-scription factor MITF which in turn can lead to melanocyticdifferentiation with expression of the protein involved inmelanin synthesis: tyrosinase, melanin, HMB45. Because ofthe extensive clinical, histologic, and immunohistochemicalsimilarities with melanoma, we decided to analyze whetherCCS also has mutations in the BRAF and NRAS gene. Nomutation of the BRAF nor NRAS gene was identified in95.54% of the analyzed tumors (21 of 22 tumors). Thetwo tumours which were found to harbor mutations in theBRAF and NRAS gene also presented the ATF1-EWS fusiongene and were considered atypical. However, the absenceof cutaneous involvement, histologic features (spindle anda few epithelioid cells arranged in a nested pattern), and

Dermatology Research and Practice 7
immunohistochemistry (diffuse positivity for S100 proteinand HMB45) strongly suggested a diagnosis of CCS.
Therefore, we support the hypothesis that CCS belongsto the soft tissue sarcoma family and that the melaninsynthesis is due to the specific action of the chimericEWF/ATF1 protein via MITF activation. Molecular geneticabnormalities have been reported in 3 small series of CCSinvolving 10 patients, 12 patients, and 9 patients [3–5].To our knowledge, the current study represents the largestreported series of patients with CCS with emphasis onmutational statue on BRAF, NRAS gene, and cytogeneticstudy of translocation (12, 22) (q13, q12).
Size constituted the only criterion that was useful as apredictor of the biologic behaviour of CCS (Table 3). In ourseries, on multivariate analysis, only tumor size (P : 0.01)emerged as a significant prognostic factor.
Tumor necrosis was also a significant indicator of poorprognosis, independent of tumor size [11, 12]. Indeed, wefound that the presence of necrosis more than 50% associatedwith worse outcome. Of fourteen patients who had necrosismore than 50%, ten patients died, but on multivariateanalysis, it was not a significant prognostic factor.
Unlike most soft tissue sarcomas, CCS often metastasizesto regional lymph nodes [1, 2]. Sixteen of our patients hadlymph node metastases. A marked tendency for regionallymph node metastases has been observed by other authors,Chung and Enzinger reported a 53% rate, and Eckardt etal. [18] a 33% rate of lymph node metastases. Although wefound lymph node metastases to be slightly less frequent thanpulmonary metastases, they tended to occur earlier in thecourse of the disease. The role of regional lymph node dissec-tion in CCS has not been established to date. Some authorsrecommend prophylactic elective lymph node dissection,whereas others suggest lymphadenectomy only in patientswho show clinical lymphadenopathy [19]. Sentinel lymphnode biopsy, which has been used successfully for the stagingof patients with breast cancer and melanoma, may allow earlydetection of lymph node metastasis in patients with CCS[19, 20]. It is quite possible that, with diligent staging usingsentinel node biopsy, some patients who are believed to havelocalized disease in the current series will turn out not to havelocalized disease, and this would have a significant impacton the analyses. Further investigations of the usefulness ofsentinel lymph node biopsy in CCS are warranted.
Complete excision of the primary tumors appears tobe the optimal approach to treatment, a conclusion that isshared by others [15]. Of the 29 patients who had local recur-rences, 19 died of the tumors and 3 are alive with disease.These results suggest that local recurrence has a negativerole in the management of CCS. In our series, successfultreatment was best accomplished by excision with a widesurgical margin, with or without adjuvant radiation therapy.The presence of metastases, either at initial diagnosis or laterin courses of the disease, was an ominous factor; no patientssurvived free of disease once metastatic CCS occurred.
The overall prognosis for CCS is poor [1–3]. In mostcases, the disease pursues a relentlessly progressive courseand terminates in death due to wide-spread dissemination.Although rapidly fatal progression may occur, late metastases
Table 3: Clinicopathologic studies of clear cell sarcoma.
Reference YearNo. of
patientsFive-yearsurvival
Prognosticfactors
Sara et al. [9] 1990 17 40 Size
El-Naggar et al.[10]
1991 11 NA DNA content
Lucas et al. [11] 1992 35 67 Size, necrosis
Montgomery etal. [12]
1993 58 63 Size∗, necrosis∗
Deenik et al.[13]
1999 30 30Size,
radiotherapy
Finley et al. [14] 2001 8 55 Size
Ferrari et al.[15]
2002 28 66Size, site, IRS
group
Takahira et al.[16]
2004 14 33 Mitosis
Kawai et al. [17] 2007 75 47Size,∗ depth, sex,
TNM
Current study 2005 52 59stage, surgicalmargin size∗
NA indicates not available; IRS group, Intergroup RhabdomyosarcomaStudy Group.∗Multivariate analysis.
are quite common after many years of freedom from disease.In our series, the 5-year survival was 59% at 5 years and41% at 10 years. Similar findings have been reported in theliterature (Table 3), with local recurrence or metastases (orboth) occurring as late as 29 years after the initial surgery[2, 15]. Thus, once a diagnosis of CCS is made, the patient isat risk for recurrent disease for many years and must be fol-lowed closely. Awareness of delayed progression is especiallyimportant considering the young age of the most patients.
The rarity of the disease makes it difficult to draw conclu-sive statements, but clear cell sarcoma shares many featureswith melanoma, including histological, immunophenotypic,ultrastructural, and similarities in gene expression patterns.However, clear cell sarcoma is genetically distinct lackingmelanoma-associated BRAF mutations and instead harbor-ing recurrent and characteristic chromosomal translocationsinvolving the EWSR1 gene. Although the term malignantmelanoma of soft parts persist, it is important that thislesion be loosely considered a MM, but rather segregated asa unique tumor of soft tissue.
Conflict of Interests
The authors have not identified conflict of interests.
Acknowledgment
No benefits in any form have been received or will be receivedfrom a commercial party related directly or indirectly to thesubject of this paper.

8 Dermatology Research and Practice
References
[1] F. M. Enzinger, “Clear-cell sarcoma of tendons and aponeu-roses: an analysis of 21 cases,” Cancer, vol. 18, pp. 1163–1174,1965.
[2] E. B. Chung and F. M. Enzinger, “Malignant melanoma of softparts. A reassessment of clear cell sarcoma,” American Journalof Surgical Pathology, vol. 7, no. 5, pp. 405–413, 1983.
[3] J. Zucman, O. Delattre, C. Desmaze et al., “EWS and ATF-1gene fusion induced by t(12;22) translocation in malignantmelanoma of soft parts,” Nature Genetics, vol. 4, no. 4, pp. 341–345, 1993.
[4] I. Panagopoulos, F. Mertens, M. Debiec-Rychter et al., “Molec-ular genetic characterization of the EWS/ATF1 fusion gene inclear cell sarcoma of tendons and aponeuroses,” InternationalJournal of Cancer, vol. 99, no. 4, pp. 560–567, 2002.
[5] R. M. Patel, E. Downs-Kelly, S. W. Weiss et al., “Dual-color,break-apart fluorescence in situ hybridization for EWS generearrangement distinguishes clear cell sarcoma of soft tissuefrom malignant melanoma,” Modern Pathology, vol. 18, no. 12,pp. 1585–1590, 2005.
[6] N. H. Segal, P. Pavlidis, W. S. Noble et al., “Classificationof clear-cell sarcoma as a subtype of melanoma by genomicprofiling,” Journal of Clinical Oncology, vol. 21, no. 9, pp. 1775–1781, 2003.
[7] E. Kaplan and P. Meier, “Nonparametric estimation fromincomplete observations,” American Statistical Association, vol.53, pp. 457–481, 1958.
[8] D. Cox, “Regression models and life-tables,” Journal of theRoyal Statistical Society: Series B, vol. 34, pp. 187–220, 1972.
[9] A. S. Sara, H. L. Evans, and R. S. Benjamin, “Malignantmelanoma of soft parts (clear cell sarcoma): a study of 17 cases,with emphasis on prognostic factors,” Cancer, vol. 65, pp. 367–374, 1990.
[10] A. K. El-Naggar, N. G. Ordonez, A. Sara, D. McLemore, andJ. G. Batsakis, “Clear cell sarcomas and metastatic soft tissuemelanomas: a flow cytometric comparison and prognosticimplications,” Cancer, vol. 67, no. 8, pp. 2173–2179, 1991.
[11] D. R. Lucas, A. G. Nascimento, and F. H. Sim, “Clear cellsarcoma of soft tissues: Mayo Clinic experience with 35 cases,”American Journal of Surgical Pathology, vol. 16, no. 12, pp.1197–1204, 1992.
[12] E. A. Montgomery, J. M. Meis, A. G. Ramos, D. M. Frisman,and K. L. Martz, “Clear cell sarcoma of tendons and aponeu-roses: a clinicopathologic study of 58 cases with analysis ofprognostic factors,” International Journal of Surgical Pathology,vol. 1, pp. 89–100, 1993.
[13] W. Deenik, W. J. Mooi, E. J. Rutgers et al., “Clear cell sarcoma(malignant melanoma) of soft parts: a clinicopathologic studyof 30 cases,” Cancer, vol. 86, pp. 969–975, 1999.
[14] J. William Finley, B. Hanypsiak, B. Mcgrath, W. Kraybill, andJ. F. Gibbs, “Clear cell sarcoma: the Roswell Park experience,”Journal of Surgical Oncology, vol. 77, no. 1, pp. 16–20, 2001.
[15] A. Ferrari, M. Casanova, G. Bisogno et al., “Clear cell sarcomaof tendons and aponeuroses in pediatric patients: a reportfrom the Italian and German Soft Tissue Sarcoma CooperativeGroup,” Cancer, vol. 94, no. 12, pp. 3269–3276, 2002.
[16] T. Takahira, Y. Oda, S. Tamiya et al., “Alterations of thep16INK4a/p14ARF pathway in clear cell sarcoma,” CancerScience, vol. 95, no. 8, pp. 651–655, 2004.
[17] A. Kawai, A. Hosono, R. Nakayama et al., “Clear cell sarcomaof tendons and aponeuroses: a study of 75 patients,” Cancer,vol. 109, no. 1, pp. 109–116, 2007.
[18] J. J. Eckardt, D. J. Pritchard, and E. H. Soule, “Clear cellsarcoma. A clinicopathologic study of 27 cases,” Cancer, vol.52, no. 8, pp. 1482–1488, 1983.
[19] W. B. Al-Refaie, M. W. Ali, D. Z. Chu, I. B. Paz, and S. L.Blair, “Clear cell sarcoma in the era of sentinel lymph nodemapping,” Journal of Surgical Oncology, vol. 87, no. 3, pp. 126–129, 2004.
[20] F. Picciotto, A. Zaccagna, G. Derosa et al., “Clear cell sarcoma(malignant melanoma of soft parts) and sentinel lymph nodebiopsy,” European Journal of Dermatology, vol. 15, no. 1, pp.46–48, 2005.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com