Embed Size (px)
Citation preview

CLINICAL RESEARCH STUDY
Classification of Myocardial Infarction: Frequency andFeatures of Type 2 Myocardial InfarctionLotte Saaby, MD,a Tina Svenstrup Poulsen, MD, PhD,a Susanne Hosbond, MD,a Torben Bjerregaard Larsen, MD, PhD,b
Axel Cosmus Pyndt Diederichsen, MD, PhD,a Jesper Hallas, MD, DMSc,c Kristian Thygesen, MD, DMSc,d
Hans Mickley, MD, DMScaaDepartment of Cardiology, Odense University Hospital, Odense, Denmark; bDepartment of Cardiology, Aalborg University Hospital,Aalborg, Denmark; cDepartment of Clinical Pharmacology, University of Southern Denmark, Odense, Denmark; dDepartment ofCardiology, Aarhus University Hospital, Aarhus, Denmark.
Funding: ThiHeart AssociationUniversity of Sou
Conflict of InAuthorship: A
writing this manusRequests for
DMSc, DepartmenSdr Boulevard 29,
E-mail addresregionsyddanmark
0002-9343/$ -seehttp://dx.doi.org/1
ABSTRACT
BACKGROUND: The classification of myocardial infarction into 5 types was introduced in 2007 as animportant component of the universal definition. In contrast to the plaque ruptureerelated type 1 myocardialinfarction, type 2 myocardial infarction is considered to be caused by an imbalance between demand andsupply of oxygen in the myocardium. However, no specific criteria for type 2 myocardial infarction have beenestablished.METHODS: We prospectively studied unselected hospital patients who had cardiac troponin I measured onclinical indication. The diagnosis and classification of myocardial infarction were established, and thefrequency and features of type 2 myocardial infarction were investigated by use of novel developed criteria.RESULTS: From January 2010 to January 2011, a total of 7230 consecutive patients who had cardiactroponin I measured were evaluated, and 4499 patients qualified for inclusion. The diagnosis of myocardialinfarction was established in 553 patients, of whom 386 (72%) had a type 1 myocardial infarction and144 (26%) had a type 2 myocardial infarction. Patients in the group with type 2 myocardial infarction wereolder and more likely to be female, and had more comorbidities. The proportion of patients withoutsignificant coronary artery disease was higher in those with type 2 myocardial infarction (45%) than inthose with type 1 myocardial infarction (12%) (P < .001). Tachyarrhythmias, anemia, and respiratoryfailure were the most prevalent mechanisms causing type 2 myocardial infarction.CONCLUSIONS: In a cohort of patients with myocardial infarction who were admitted consecutively through1 year, the category of type 2 myocardial infarction comprised one fourth when diagnosed by the use ofnewly developed criteria. Approximately half of patients with type 2 myocardial infarction had nosignificant coronary artery disease.� 2013 Elsevier Inc. All rights reserved. � The American Journal of Medicine (2013) 126, 789-797
KEYWORDS: Troponin; Type 2 myocardial infarction; Universal definition of myocardial infarction
s study has been financially supported by the Danish, Odense University Hospital, Denmark and by thethern Denmark, Odense, Faculty of Health Sciences.terest: None.ll authors had access to the data and played a role incript.reprints should be addressed to Hans Mickley, MD,t of Cardiology, Odense University Hospital, Odense,4 Floor, 5000 Odense C, Denmark.s: [email protected] or [email protected]
front matter � 2013 Elsevier Inc. All rights reserved.0.1016/j.amjmed.2013.02.029
The clinical classification of myocardial infarction into 5types was introduced in 2007 as an important component ofthe universal definition.1 Although the spontaneous type 1myocardial infarction is related to a coronary plaque rupture,fissuring, or dissection with resulting intraluminal throm-bosis, type 2 myocardial infarction is secondary to myo-cardial ischemia resulting from increased oxygen demand ordecreased supply. Type 3 myocardial infarction is linked tounexpected cardiac death when cardiac biomarkers are
790 The American Journal of Medicine, Vol 126, No 9, September 2013
unavailable, whereas types 4 and 5 myocardial infarctionare procedure related.1 The launch of this classification hasraised clinical interest particularly in type 2 myocardialinfarction. Several clinical conditions have been proposedas being the cause of type 2 myocardial infarction,1 but so farno specific criteria have been proposed. The object of this
CLINICAL SIGNIFICANCE
� In unselected hospital patients, onefourth of all myocardial infarctions aretype 2.
� The most frequent mechanisms causingtype 2 myocardial infarction are anemia,respiratory failure, and tachyarrhythmias.
� Approximately 50% of patients withtype 2 myocardial infarction are foundin other departments than cardiology.
� Approximately 50% of patients withtype 2 myocardial infarction have nosignificant coronary artery disease.
study is to elucidate the frequencyand characteristics of type 2 myo-cardial infarction in a prospectivedesign when applying the noveldeveloped clinical criteria.
MATERIALS AND METHODS
Study Design andPopulationThe study comprises patientsconsecutively admitted to a 1000-bed university hospital, whichserves as a tertiary referral centerfor a region with 1.2 million in-habitants and as a local hospitalfor a catchment area of 300,000residents. The data is a part of theDEF-AMI Study (Consequences
of the universal 2007 DEFinition of Acute MyocardialInfarction studied in a Danish consecutive hospital pop-ulation). All admitted patients who had cardiac troponin I(cTnI) measured were traced through retrieval 3 times dailyat the Department of Clinical Biochemistry of the hospital.Within 24 hours after the first cTnI sampling, all patientshad a supplementary history taken by dedicated studypersonnel paying special attention to symptoms on admis-sion, clinical characteristics, and comorbidity. We onlyincluded comorbidity that could be validated by confirma-tion from the patient’s medical records or the list of currentmedication. Exclusion criteria were residence outside thelocal catchment area, age <18 years, and a cTnI sampletaken in an outpatient clinic.Biochemical AnalysisThe cTnI was analyzed on an Architect c16000 (AbbottDiagnostics, Abbott Park, Ill). This analysis has a detectionlimit of 0.01 mg/L, with an upper reference limit of the 99thpercentile of 0.028 mg/L and a coefficient of variation <10%at 0.032 mg/L. Thus, a cTnI value >0.03 mg/L is consideredthe decision limit for the diagnosis of myocardial infarction.
Imaging DataInformation on echocardiographic examinations wasretrieved from the hospital records. In addition, informationon the results of in-hospital coronary angiography wascollected from the Western Denmark Heart Registry.2 Asignificant coronary artery stenosis had to be �50% of theartery diameter. Patients were classified as having no signif-icant coronary artery disease or 1-, 2-, or 3-vessel disease
according to the number of major coronary arteries withsignificant stenoses. In the Western Denmark Heart Registry,significant left main stenoses are registered separately.
Definition of Type 2 Myocardial Infarction
In addition to the indicated diag-nostic biomarker criteria we devel-oped, partly on thebasis of data fromthe literature,1,3-6 specific clinicalstandards for the definition of type 2myocardial infarction, that is,conditions reflecting an imbalancebetween myocardial oxygen supplyand demand. Conditions with de-creased oxygen supply were:� Anemia defined as a hemoglobinconcentration <5.5 mmol/L formen and <5.0 mmol/L forwomen;
� Shock defined as systolic bloodpressure <90 mm Hg togetherwith signs of organ dysfunction(ie, metabolic acidosis, arterialoxygen tension <8 kPa, oliguria
[diuresis <30 mL/h for at least 3 hours], or encephalop-athy)3-5;
� Bradyarrhythmia requiring medical treatment or cardiacpacing;
� Coronary embolus in the presence of an increased risk ofembolism (left heart endocarditis, intracardiac muralthrombus, documented venous thrombus, and a patentforamen ovale or atrial septum defect); or
� Respiratory failure with an arterial oxygen tension <8 kPaand clinical signs of acute respiratory failure lasting �20minutes.4
Conditions with increased oxygen demand were:
� Ventricular tachyarrhythmia lasting �20 minutes;� Supraventricular tachyarrhythmia lasting �20 minuteswith a ventricular rate >150 beats/min;
� Hypertensive pulmonary edema defined as the presence ofa systolic blood pressure>160mmHg, signs of pulmonaryedema, and a need for treatmentwith nitrates or diuretics6; or
� Arterial hypertension with a systolic blood pressure>160 mmHg and concomitant left ventricular hypertrophyidentified by echocardiography or electrocardiogram.
The type of acute myocardial infarction also was cate-gorized as ST-elevation myocardial infarction or noneST-elevation myocardial infarction as defined in the universaldefinition.1 Patients with new (or presumably new) leftbundle branch block were designated as having an ST-elevation myocardial infarction. The remaining patients,including those with pacemaker rhythm and preexistingbundle branch block, were categorized as having noneST-elevation myocardial infarction.

Saaby et al Type 2 Myocardial Infarction 791
Other Types of Myocardial InfarctionPatients with type 3 myocardial infarction were not included inthis study, because cardiac biomarkers per definition are un-available in these patients.1 Type 4a, 4b, and 5 myocardial in-farctions were defined according to the universal definition.1
Classification of Patients With MyocardialNecrosis but Without Myocardial InfarctionPatients with cTnI values >0.03mg/L but without overtmyocardial ischemia were classified into the followinggroups adapted from Thygesen et al7:
� cTnI elevation related to secondary ischemia (eg, hyper-trophic cardiomyopathy, coronary vasculitis);
� cTnI elevation not related to ischemia (eg, radiofrequencyablation, cardiac incision with surgery, chemotherapy);
� cTnI elevation due to extracardiac conditions (eg, infec-tion, stroke, renal failure);
� cTnI elevation resulting from at least 2 cardiac orextracardiac conditions;
� cTnI elevation of indeterminate origin.
Classification of Patients Without MyocardialNecrosisPatients with cTnI �0.03 mg/L were classified as havingunstable angina pectoris, prior or no prior ischemic heartdisease. Unstable angina pectoris was defined as unstablechest discomfort (rest, new onset, or worsening of angina)or dynamic electrocardiographic changes indicative of
7.230 With a first cTn
4.719 Eligible for in220 Missed cTnI:
4 Haemolysis216 Only CKMB available
4.499 Include
1.961 cTnI >0.03 μg/l
553 MI
397 Type 1 MI
144 Type 2 MI
2 Type 4a MI
7 Type 4b MI
3 Type 5 MI
1.408 Myocardial necrosiswithout MI
188 Cardiac; not
425 Extracardiac
415 Multi-factoria
221 Cardiac; rela
159 Indeterminate
Figure 1 Patient inclusion. AP ¼ angina pectoris;troponin I; GP ¼ general practitioner; IHD ¼ ischem
ischemia.8 Prior ischemic heart disease was defined asa documented medical history of such a diagnosis or currentmedical treatment for ischemic heart disease.
Adjudicated Final DiagnosisThree experienced cardiologists (LS, TSP, HM) evaluated theconditions underlying the index event. The cardiac diagnoseswere based on the source information provided by the supple-mentary history obtained, laboratory sheets, and patient records.The Task Force Co-Chairman (KT) of the universal definitionwas consulted in all cases of diagnostic ambiguity to reachconsensus on the classification.1 Patients with normal cTnIvalues were classified according to the 10th edition of Interna-tional Classification of Diseases system provided at discharge.
Statistical AnalysisContinuous variables are presented as medians with inter-quartile range or as means (� standard deviation). Categoricvariables are listed as numbers (%). The Mann-WhitneyU test was used to calculate P values for continuous vari-ables. Pearson chi-square test was used to compare categoricvariables. For comparing larger contingency tables (r*ctables) the chi-square test also was used. Because less than20% of the expected numbers are less than 5 and none areless than 1, the chi-square test is considered valid. P valuesless than .05 were considered to indicate statistical signifi-cance. All analyses were performed by the study group usingSTATA version 11 (StataCorp LP, College Station, Tex).The study complied with the Declaration of Helsinki and was
I sample
2.511 Excluded:2.277 Residents outside local catchment area43 Age <18 yrs191 cTnI taken at GP or outpatient clinic
clusion
d
44 Unstable AP
491 Prior IHD
2.003 No prior IHD
related to ischemia
conditions
l conditions
2.538 cTnI ≤0.03 μg/l
ted to secondary ischemia
origin
CKMB ¼ creatine kinase MB; cTnI ¼ cardiacic heart disease; MI ¼ myocardial infarction.

792 The American Journal of Medicine, Vol 126, No 9, September 2013
approved by the Danish National Committee on BiomedicalResearch Ethics and the Danish Data Protection Agency.
RESULTScTnI was measured in 7230 hospitalized patients admittedbetween January 6, 2010, and January 5, 2011. Approxi-mately one third of patients did not meet the inclusioncriteria. Thus, 4499 patients were enrolled, and of these1961 had cTnI elevation above the 99th percentile upperreference limit. Figure 1 shows that 553 patients (12.3%)had myocardial infarction.
Classification According to the UniversalDefinitionOn the basis of the universal definition, 397 patients(71.8%) were classified as having type 1 myocardialinfarction and 144 patients (26%) were classified as havingtype 2 myocardial infarction (Table 1). When comparedwith patients with type 1 myocardial infarction, patientswith type 2 myocardial infarction were older and more
Table 1 Baseline Characteristics of 397 Patients with Type 1 Myocard
Characteristics Type 1 MI (N
Age, y (� SD) 71 (14Male, no. (%) 249 (62Risk factors, no. (%)
Diabetes 52 (13Hypercholesterolemia 158 (39Hypertension 215 (54Current smoker, no./total no. (%) 129/342 (37Family history, no./total no. (%) 103/305 (33
Medical history, no. (%)Prior MI 96 (24Prior CABG 37 (9.3Prior percutaneous coronary intervention 57 (14Heart failure 45 (11Prior stroke 54 (13Peripheral arterial disease 21 (5.3Renal failure 23 (5.8Chronic obstructive pulmonary disease 46 (11Arrhythmia 50 (12
Laboratory data, median/total no. (IQR)First troponin I, mg/L 0.27 (0.0Peak troponin I value, mg/L 2.96 (0.4Hemoglobin, mmol/L 8.2/391 (7.4Leukocytes, 10E9/L 10.1/391 (7.7Creatinine (enzymatic)-P, mmol/L 84/394 (70C-reactive protein, mg/L 5/391 (2-1
Clinical findings, median/total no. (IQR)Systolic blood pressure, mm Hg 146/395 (12Diastolic blood pressure, mm Hg 86/395 (73Heart rate, beats/min 80/393 (68
Ejection fraction, median/total no. (IQR) 50/340 (40ST-elevation MI, no. (%) 130 (32NoneST-elevation MI, no. (%) 267 (67Coronary angiography, no. (%) 281 (70
CABG ¼ coronary artery bypass grafting; IQR ¼ interquartile range; MI ¼ m
likely female. Furthermore, the patients with type 2myocardial infarction had more comorbidities (heart failure,renal failure, chronic obstructive pulmonary disease, andarrhythmias). Moreover, patients with type 2 myocardialinfarction had significantly lower peak cTnI values andmore noneST-elevation myocardial infarction whencompared with patients with type 1 myocardial infarction.The rate of coronary angiography was lower in type 2myocardial infarction, and the pattern of coronary arterydisease differed significantly with only approximately halfof patients with type 2 myocardial infarction havingsignificant coronary artery disease (Figure 2). Twelvepatients (2.2%) had type 4a (n ¼ 2), type 4b (n ¼ 7), or type5 myocardial infarction (n ¼ 3).
Mechanisms Underlying Type 2 MyocardialInfarctionFigure 3 shows that anemia, tachyarrhythmias, and respi-ratory failure were the most prevalent conditions underlyingtype 2 myocardial infarction. If supraventricular and
ial Infarction and 144 Patients with Type 2 Myocardial Infarction
¼ 397) Type 2 MI (N ¼ 144) P Value
) 75 (11) .010.7) 76 (52.8) .04
.1) 40 (27.9) <.001
.8) 60 (41.8) .69
.2) 81 (56.3) .67
.7) 35/108 (32.4) .07
.8) 14/74 (18.9) .01
.2) 39 (27.1) .49) 14 (9.7) .89.4) 25 (17.4) .39.3) 34 (23.6) <.001.6) 31 (21.5) .03) 18 (12.5) .004) 20 (13.9) .002.6) 36 (25.0) <.001.6) 34 (23.6) .002
6-1.48) 0.20 (0.07-0.78) .224-15.85) 1.09 (0.43-3.24) <.001-8.9) 7.7/138 (6.2-8.9) <.001-12.8) 11.6/142 (8.9-17.6) <.001-103) 102/143 (76-141) <.0018) 21/134 (4-63) <.001
2-168) 139/140 (106-167) .01-101) 77/140 (62-96) <.001-100) 113/142 (90-131) <.001-55) 40/107 (30-55) <.001.7) 5 (3.4) <.001.3) 139 (96.6) <.001.8) 31 (21.5) <.001
yocardial infarction; SD ¼ standard deviation.

A
0
10
20
30
40
50
60
70
80
90
100
IM2epyTIM1epyT
%
No significant coronary artery disease Significant coronary artery disease
n = 33
n = 248
n = 14
n = 17
P <0.001
B
0
5
10
15
20
25
30
35
40
45
50
1 vessel disease 2-3 vessel disease Left Main disease
%
Type 1 MI Type 2 MI
n = 124
n = 6
n = 123
n = 11
n = 17n = 3
34.0=P800.0=P P = 0.38
Figure 2 Results of coronary angiography. (A) Proportion of patients with type 1 versus type 2myocardial infarction with or without significant coronary artery disease. (B) Patients are groupedaccording to the number of arteries with significant disease. Patients with left main disease are separatelyregistered. One patient with type 1 myocardial infarction with left main disease had no other significantcoronary lesions. The remaining 19 patients with left main disease had at least 1 more coronary vesselwith significant coronary artery disease. MI ¼ myocardial infarction.
Saaby et al Type 2 Myocardial Infarction 793
ventricular arrhythmias were added together, tachyarrhyth-mias played a role in 29.1% of type 2 myocardial infarctions.In 15 patients, at least 2 different mechanisms were involved.
Patients Admitted to the Coronary Care UnitVersus Other Clinical DepartmentsAlmost half of patients with type 2myocardial infarctionwereadmitted to departments other than the coronary care unit(Table 2). These patients were a mean of 11 years older andcomprised relatively more noneST-elevation myocardial
infarction cases than the coronary care unit grouping. Patientsfrom other departments had more comorbidities. Of note, theindex median cTnI value was significantly higher in patientswith myocardial infarction outside the coronary care unit, butpatients from the coronary care unit still exhibited signifi-cantly higher median peak cTnI concentrations (Table 2).
DISCUSSIONIn this study, 4499 consecutive hospitalized patients witha suspected acute myocardial infarction were evaluated

0
5
10
15
20
25
Anaem
ia
Respir
atory f
ailure
Suprav
entricu
lar ta
chya
rrhyth
mia
Multi-fa
ctoria
l
Ventric
ular ta
chya
rrhyth
mia
Pulmon
ary oe
dema
Shock
Bradya
rrhyth
mia
Hypert
ensio
n
Coronary
embo
lus
Coronary
spas
m
n = 30 n = 30n = 28
n = 15 n = 14n = 13
n = 9
n = 4n = 1 n = 0 n = 0
%
Figure 3 Mechanisms underlying myocardial oxygen demand/supply imbalance leading to type 2myocardial infarction (n ¼ 144).
794 The American Journal of Medicine, Vol 126, No 9, September 2013
according to the principles of the universal definition and withparticular emphasis on novel clinical standard criteria for theclassification of type 2 myocardial infarction. Thus, 553patients had acute myocardial infarction, of whom 26% wereclassified as having type 2 myocardial infarction. Approxi-mately half of patientswith type2myocardial infarction did nothave significant coronary artery disease on coronaryangiography.
Few original studies addressing the frequency of type 2myocardial infarction are available. However, in line withour results, Javed et al9 found a 29.6% frequency of type 2myocardial infarction in a study of 216 patients. On theother hand, when Melberg et al10 retrospectively reclassified1093 patients with myocardial infarction, they found thatonly 1.6% had a type 2 myocardial infarction. Furthermore,in selected patients with acute coronary syndrome under-going percutaneous coronary intervention, only 3.5% of themyocardial infarctions were classified as type 2.11,12
Because of the lack of internationally accepted criteriafor diagnosing type 2 myocardial infarction, we developedcriteria to assess the imbalance between myocardial oxygendemand and oxygen supply including the clinical conditionsproposed by the Task Force, for example, coronary arteryspasm, coronary embolism, anemia, arrhythmias, hyperten-sion, or hypotension.1 However, many patients withpulmonary disease, anemia, septicemia, renal failure, stroke,tachycardia, or hypotension may have elevation of troponinvalues,1,7,10,13-15 and in clinical practice it is often difficultto decide whether these elevations occur in an ischemicsetting. Another challenge is to decide whether the patienthas a type 1 or 2 myocardial infarction. According to theuniversal definition, a typical increasing or decreasingpattern in troponin values has to be present to fulfill thediagnosis of myocardial infarction.1 By use of this crucial
criterion and our prespecified type 2 myocardial infarctioncriteria, we found that anemia, supraventricular tachyar-rhythmias, and respiratory failure were the 3 most prevalentmechanisms, each leading to 20% of type 2 myocardialinfarctions (Figure 3). Anemia generally is present in 6% to43% of patients with acute myocardial infarction dependingon patient characteristics and the definition used.16 Lowerhemoglobin levels have consistently been associated with anadverse clinical outcome in the general population and inpatients with cardiovascular disease.17,18 The exact mecha-nism underlying the link between anemia and a poor prog-nosis is not clearly understood, but a number of physiologicadaptive processes aimed at maintaining adequate totaloxygen delivery to the tissues may be relevant.18 To avoidoverestimation of the importance of anemia as the under-lying type 2 myocardial infarction mechanism, we deliber-ately used a restrictive definition with hemoglobin cutofflimits lower than those of the World Health Organizationdefinition19 and at the same time fulfilling the criteria of“severe anemia” proposed by other researchers.20
Data on the importance of troponin elevation associ-ated with supraventricular tachyarrhythmias are limited. Ina recent retrospective study,21mild elevation of cTnI inpatientswith supraventricular tachycardia was found to be associatedwith greater than triple the risk of future cardiovascular events,including acute myocardial infarction. The exact mechanismformyocardial necrosis is unknown, but it is believed that thereis an increase in oxygen consumption by the myocardiumduring a prolonged period of tachycardia and a reduction of theoxygen supply by a shortening of the diastole.22,23 Causes ofrespiratory failure in our study included decompensated acuteheart failure, severe pneumonia, and exacerbation of chronicobstructive pulmonary disease. Proposed underlying mecha-nisms in these patients are hypoxia causing imbalance between
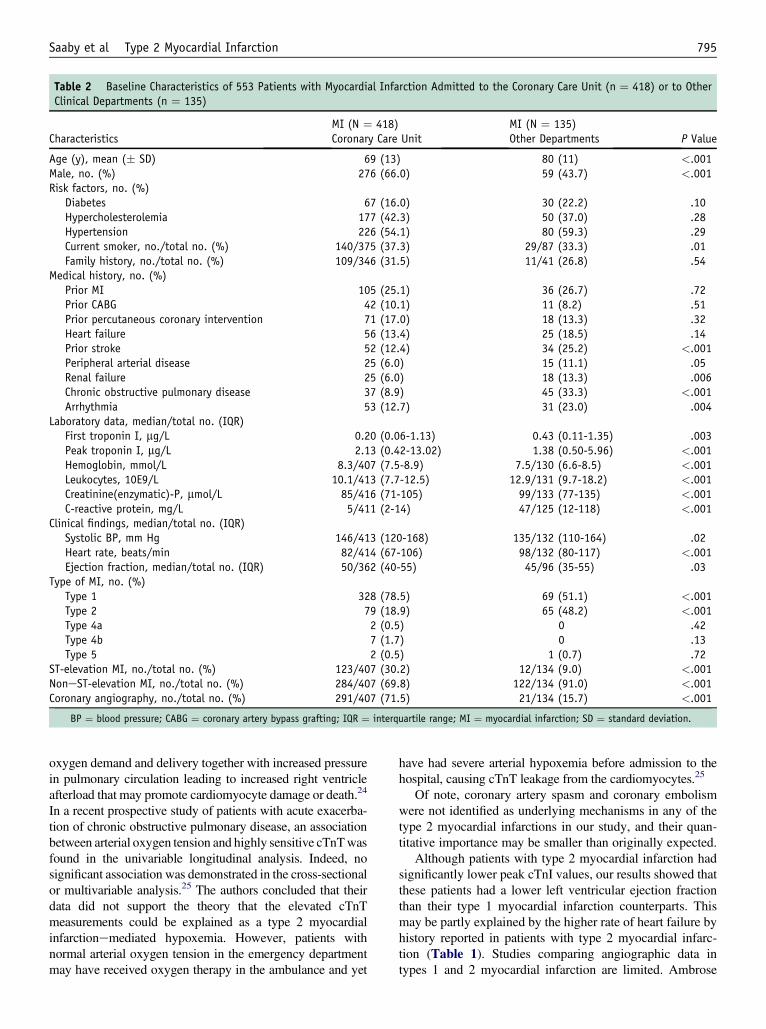
Table 2 Baseline Characteristics of 553 Patients with Myocardial Infarction Admitted to the Coronary Care Unit (n ¼ 418) or to OtherClinical Departments (n ¼ 135)
CharacteristicsMI (N ¼ 418)Coronary Care Unit
MI (N ¼ 135)Other Departments P Value
Age (y), mean (� SD) 69 (13) 80 (11) <.001Male, no. (%) 276 (66.0) 59 (43.7) <.001Risk factors, no. (%)
Diabetes 67 (16.0) 30 (22.2) .10Hypercholesterolemia 177 (42.3) 50 (37.0) .28Hypertension 226 (54.1) 80 (59.3) .29Current smoker, no./total no. (%) 140/375 (37.3) 29/87 (33.3) .01Family history, no./total no. (%) 109/346 (31.5) 11/41 (26.8) .54
Medical history, no. (%)Prior MI 105 (25.1) 36 (26.7) .72Prior CABG 42 (10.1) 11 (8.2) .51Prior percutaneous coronary intervention 71 (17.0) 18 (13.3) .32Heart failure 56 (13.4) 25 (18.5) .14Prior stroke 52 (12.4) 34 (25.2) <.001Peripheral arterial disease 25 (6.0) 15 (11.1) .05Renal failure 25 (6.0) 18 (13.3) .006Chronic obstructive pulmonary disease 37 (8.9) 45 (33.3) <.001Arrhythmia 53 (12.7) 31 (23.0) .004
Laboratory data, median/total no. (IQR)First troponin I, mg/L 0.20 (0.06-1.13) 0.43 (0.11-1.35) .003Peak troponin I, mg/L 2.13 (0.42-13.02) 1.38 (0.50-5.96) <.001Hemoglobin, mmol/L 8.3/407 (7.5-8.9) 7.5/130 (6.6-8.5) <.001Leukocytes, 10E9/L 10.1/413 (7.7-12.5) 12.9/131 (9.7-18.2) <.001Creatinine(enzymatic)-P, mmol/L 85/416 (71-105) 99/133 (77-135) <.001C-reactive protein, mg/L 5/411 (2-14) 47/125 (12-118) <.001
Clinical findings, median/total no. (IQR)Systolic BP, mm Hg 146/413 (120-168) 135/132 (110-164) .02Heart rate, beats/min 82/414 (67-106) 98/132 (80-117) <.001Ejection fraction, median/total no. (IQR) 50/362 (40-55) 45/96 (35-55) .03
Type of MI, no. (%)Type 1 328 (78.5) 69 (51.1) <.001Type 2 79 (18.9) 65 (48.2) <.001Type 4a 2 (0.5) 0 .42Type 4b 7 (1.7) 0 .13Type 5 2 (0.5) 1 (0.7) .72
ST-elevation MI, no./total no. (%) 123/407 (30.2) 12/134 (9.0) <.001NoneST-elevation MI, no./total no. (%) 284/407 (69.8) 122/134 (91.0) <.001Coronary angiography, no./total no. (%) 291/407 (71.5) 21/134 (15.7) <.001
BP ¼ blood pressure; CABG ¼ coronary artery bypass grafting; IQR ¼ interquartile range; MI ¼ myocardial infarction; SD ¼ standard deviation.
Saaby et al Type 2 Myocardial Infarction 795
oxygen demand and delivery together with increased pressurein pulmonary circulation leading to increased right ventricleafterload that may promote cardiomyocyte damage or death.24
In a recent prospective study of patients with acute exacerba-tion of chronic obstructive pulmonary disease, an associationbetween arterial oxygen tension and highly sensitive cTnTwasfound in the univariable longitudinal analysis. Indeed, nosignificant association was demonstrated in the cross-sectionalor multivariable analysis.25 The authors concluded that theirdata did not support the theory that the elevated cTnTmeasurements could be explained as a type 2 myocardialinfarctionemediated hypoxemia. However, patients withnormal arterial oxygen tension in the emergency departmentmay have received oxygen therapy in the ambulance and yet
have had severe arterial hypoxemia before admission to thehospital, causing cTnT leakage from the cardiomyocytes.25
Of note, coronary artery spasm and coronary embolismwere not identified as underlying mechanisms in any of thetype 2 myocardial infarctions in our study, and their quan-titative importance may be smaller than originally expected.
Although patients with type 2 myocardial infarction hadsignificantly lower peak cTnI values, our results showed thatthese patients had a lower left ventricular ejection fractionthan their type 1 myocardial infarction counterparts. Thismay be partly explained by the higher rate of heart failure byhistory reported in patients with type 2 myocardial infarc-tion (Table 1). Studies comparing angiographic data intypes 1 and 2 myocardial infarction are limited. Ambrose

796 The American Journal of Medicine, Vol 126, No 9, September 2013
et al26 recently reported on 224 patients with myocardialinfarction who were selected because of the availabilityof an in-hospital angiogram and the diagnosis of a type 1(n ¼ 193) and type 2 myocardial infarction (n ¼ 31).Nonobstructive coronary artery disease was present in35.5% of patients with type 2 myocardial infarction versus11.4% of patients with type 1 myocardial infarction.26 Theseobservations are supported by our data. Thus, we found that45.2% of patients with type 2 myocardial infarction and11.7% of patients with type 1 myocardial infarction did nothave significant coronary artery disease. Finally, 1-vesseldisease—also in accordance with the findings by Ambroseet al26—seems to be more than twice as prevalent in type 1than in type 2 myocardial infarction (Figure 2).
Our study design also allowed a comparison betweenpatients admitted to the coronary care unit and patientsadmitted to other departments. Of note, the first cTnI valueobtained was lower in patients in the coronary care unit thanin other departments (Table 2). However, subsequent cTnIvalues were higher in patients in the coronary care unit. Thisobservation is most likely due to differences in patient char-acteristics, clinical routines, andmyocardial infarction types inthe 2 settings. Thus, the time delay from symptom start to cTnImeasurement in departments outside the coronary care unit ismost likely longer because patients had more atypical symp-toms andmore comorbidity. Of interest, approximately half ofpatients with a type 2 myocardial infarction were admitted toother departments than the department of cardiology.
Study LimitationsFirst, a complete cardiac examination was not performed inevery patient because diagnostic procedures, such as echo-cardiographyand coronary angiography,wereperformed at thediscretion of the treating physicians. Second, only 1 cTnImeasurement is available in some patients. However, inpatients with ST-elevation myocardial infarction undergoingprimary percutaneous coronary intervention, the diagnosis ofamyocardial infarctionwill frequently bemadedespite the lackof serial cTnI measurements. Also, in most patients hospital-ized more than 24 hours after the onset of symptoms, a singleelevated cTnI value in an ischemic setting would be sufficientto meet the diagnostic myocardial infarction criteria.1 Third, itshould be noted that the proportion of type 4a myocardialinfarction is surprisingly low, but according to the standards ofthe hospital, the cTnI is only measured after percutaneouscoronary intervention in case of clinical symptoms ofmyocardial infarction. Last, the detailed type 2 myocardialinfarction criteria proposed by our study group do not neces-sarily represent “the gold standard.” Indeed, we consider thiswork as a stepping stone in the development and adaption ofa globally accepted definition of myocardial infarction.
CONCLUSIONSThis prospective study on the classification and features ofpatients with myocardial infarction defined according to the
universal definition demonstrates that 26% of these patientshad type 2 myocardial infarction when novel developedclinical criteria were used. Patients with type 2 myocardialinfarction generally had more severe clinical characteristicsthan patients with type 1 myocardial infarction. Approxi-mately half of patients with type 2 myocardial infarction hadno significant coronary artery disease.
ACKNOWLEDGMENTSThe authors thank Jens Lauritsen, MD, PhD, for taking careof the database.
References1. Thygesen K, Alpert JS, White HD. Universal definition of myocardial
infarction. Eur Heart J. 2007;28:2525-2538.2. Schmidt M, Maeng M, Jakobsen CJ, et al. Existing data sources for
clinical epidemiology: The Western Denmark Heart Registry. ClinEpidemiol. 2010;2:137-144.
3. Dellinger RP, Levy MM, Carlet JM, et al. Surviving Sepsis Campaign:international guidelines for management of severe sepsis and septicshock: 2008. Crit Care Med. 2008;36:296-327.
4. Celli BR, MacNee W, Agusti A, et al. Standards for the diagnosis andtreatment of patients with COPD: a summary of the ATS/ERS positionpaper. Eur Respir J. 2004;23:932-946.
5. Dickstein K, Cohen-Solal A, Filippatos G, et al. ESC Guidelinesfor the diagnosis and treatment of acute and chronic heart failure2008: the Task Force for the Diagnosis and Treatment of Acuteand Chronic Heart Failure 2008 of the European Society ofCardiology. Developed in collaboration with the Heart. Eur HeartJ. 2008;29:2388-2442.
6. Nieminen MS, Harjola VP. Definition and epidemiology of acute heartfailure syndromes. Am J Cardiol. 2005;96:5G-10G.
7. Thygesen K, Mair J, Katus H, et al. Recommendations for the use ofcardiac troponin measurement in acute cardiac care. Eur Heart J.2010;31:2197-2204.
8. Braunwald E. Unstable angina. A classification. Circulation. 1989;80:410-414.
9. Javed U, Aftab W, Ambrose J, et al. Frequency of elevated troponin Iand diagnosis of acute myocardial infarction. Am J Cardiol. 2009;104:9-13.
10. Melberg T, Burman R, Dickstein K. The impact of the 2007 ESC-ACC-AHA-WHF Universal definition on the incidence and classifi-cation of acute myocardial infarction: a retrospective cohort study. Int JCardiol. 2010;139:228-233.
11. Morrow D, Wiviott SD, White HD, et al. Effect of the novel thieno-pyridine prasugrel compared with clopidogrel on spontaneous andprocedural myocardial infarction in the Trial to Assess Improvement inTherapeutic Outcomes by Optimizing Platelet Inhibition with Prasu-grel-Thrombolysis in Myocardial Infarction 38: an application of theclassification system from the universal definition of myocardialinfarction. Circulation. 2009;119:2758-2764.
12. Bonaca MP, Wiviott SD, Braunwald E, et al. American College ofCardiology/American Heart Association/European Society of Cardi-ology/World Heart Federation universal definition of myocardialinfarction classification system and the risk of cardiovascular death:observations from the TRITON-TIMI 38. Circulation. 2012;125:577-583.
13. McAllister D, Maclay JD, Mills NL, et al. Diagnosis of myocardialinfarction following hospitalisation for exacerbation of COPD. EurRespir J. 2012;39:1097-1103.
14. Januzzi JL, Filippatos G, Nieminen M, Gheorghiade M. Troponinelevation in patients with heart failure: on behalf of the third UniversalDefinition of Myocardial Infarction Global Task Force: Heart FailureSection. Eur Heart J. 2012;33:2265-2271.
Saaby et al Type 2 Myocardial Infarction 797
15. Jensen JK, Kristensen SR, Bak S, et al. Frequency and significance oftroponin T elevation in acute ischemic stroke. Am J Cardiol. 2007;99:108-112.
16. Anker SD, Voors A, Okonko D, et al. Prevalence, incidence, andprognostic value of anaemia in patients after an acute myocardialinfarction: data from the OPTIMAAL trial. Eur Heart J. 2009;30:1331-1339.
17. Sarnak MJ, Tighiouart H, Manjunath G, et al. Anemia as a risk factorfor cardiovascular disease in The Atherosclerosis Risk in Communities(ARIC) study. J Am Coll Cardiol. 2002;40:27-33.
18. Muzzarelli S, Pfisterer M. Anemia as independent predictor of majorevents in elderly patients with chronic angina. Am Heart J. 2006;152:991-996.
19. Nutritional anaemias. Report of a WHO scientific group. World HealthOrgan Tech Rep Ser. 1968;405:5-37.
20. Valeur N, Nielsen OW, McMurray JJ, et al. Anaemia is an independentpredictor of mortality in patients with left ventricular systolicdysfunction following acute myocardial infarction. Eur J Heart Fail.2006;8:577-584.
21. Chow GV, Hirsch GA, Spragg DD, et al. Prognostic significance ofcardiac troponin I levels in hospitalized patients presenting withsupraventricular tachycardia. Medicine. 2010;89:141-148.
22. Zellweger MJ, Schaer BA, Cron TA, et al. Elevated troponin levels inabsence of coronary artery disease after supraventricular tachycardia.Swiss Med Wkly. 2003;133:439-441.
23. Bakshi TK, Choo MKF, Edwards CC, et al. Causes of elevated troponinI with a normal coronary angiogram. Intern Med J. 2002;32:520-525.
24. Høiseth AD, Neukamm A, Karlsson BD, et al. Elevated high-sensi-tivity cardiac troponin T is associated with increased mortality afteracute exacerbation of chronic obstructive pulmonary disease. Thorax.2011;66:775-781.
25. Høiseth AD, Omland T, Hagve TA, et al. Determinants of high-sensitivity cardiac troponin T during acute exacerbation of chronicobstructive pulmonary disease: a prospective cohort study. BMC PulmMed. 2012;12:22.
26. Ambrose J, Loures-Vale A, Javed U, et al. Angiographic correlates intype 1 and 2 MI by the universal definition. J Am Coll Cardiol Img.2012;5:463-464.

















