Embed Size (px)
Citation preview

Classification, nomenclature, taxonomy,identification
• Classification is arrangement of bacteria into groups ( the same organisms can be classified differently according to the view: serotype classification, antimicrobial resistance classification…)
• Nomenclature (name) is the mean of communicating - it is binominal
• Taxonomy - science of classification, identification, nomenclature and making a system
• Identification is practical use of classification criteria to distinguish certaine organism from others

Graduating
• subspecies: serotyping Streptococcus pneumoniae type 8
• species - distinct organism with certain characteristic features, similar organism within genus Streptococcus pneumoniae, S.sp
• genera:Streptococcus, • families: Micrococaceae, • orders

Approaches to taxonomy
• Numerical, • phylogenetic, • genome size, • Guanin+cytosine content, • DNA relatedness, thermal stability of DNA
sequences, DNA relatedness under supraoptimal conditions…….
• In practice - polyphasic approche - depending on importnace and purpose of nomenclature

Bacterial identification in practice
• Pure culture• Colony morphology • gram staining - preliminary identification G+G-• growth characteristics aerobic, anaerobic• Biochemical properties genus + species• antigenic properties type• binominal nomenclature - clinical purposes• Molecular and genetic characteristic• G+C, DNA homology, thermal stability -epidemiological and
forensic puroses

Principles of diagnosis• Symptomatic patient - manifestation of infecton
• Suspection of microbial ethiology - exogenous or endogenous
• Specimen selection, collection -
• Specimen processing and microbiological examination - specific techniques
• Result communication and consultation
• Asymptomatic patient

Practical taxonomy
P ep tos trep tococcu sP ep tococcu s
S arc in aR u m in ococcu s
an aerob ic
G em ellaP ed iococcu sL eu con os tocL acotococcu s
S tap h ylococcu sM ic rococcu s
S trep tococcu sE n terococcu s
aerob ic
G +cocc i
N on -sp oreP rop ion ib ac teriu m
M ob ilu n cu sB ifid ob ac te riu m
C los trid iu m -sp ore
an aerob ic
L is te riaE rys ip e lo trixG ard n ere lla
B ac illu sC oryn eb ac te riu mA rcan ob ac te riu m
R h od ococcu s
aerob ic
G ram +rod s
G ram p os it ive
V e illon e llaM eg asp h oera
an aerob ic
N eisseriaM oraxe lla
B ran h am ella
aerob ic
G -cocc i
H aem op h ilu sL eg ion e llaB arton e llaE iken e lla ...
B ord ete llaP as teu re llaF ran c isce lla
B ru ce lla
E N TE R O B A C TE R IA C E A
N O N F E R M E N TE R SP seu d om on asA c in e tob ac te r
S ten otro fom on as ..... .
V ib rion aceaeC am p ylob ac te r
H elicob ac te r
aerob ic
L ep to trich aW olin e lla
B ac te ro id esP orp h yrom on as
P revo te llaF u sob ac te riu m
an aerob ic
G -rod s
lG ram n eg ative
B ac teria
Mycoplasma, Ureaplasma, ChlamydiaRicketsiaceae
Spirochetales - Spirochetes, Leptospira, BorreliaMycobacterium
Nocardia , Actinomycetes,
Miscellanous bacteria
Lectures 1,2
• Micrococcaceae (Staphylococcus), Streptococcaceae G+cocci
• Neisseriaceae: G- cocci
• Bacillaceae, Corynebacterium: G+rods Listeria, Erysipelotrix,
• Mycobacteria: G- acid fast rods
• Actinomyces, Nocardia: G+rods with special characteristic

Staphylococcus
• Pathogens of man• Divided in 2 groups acc to plasmacoagulase production -
artificial PC negative - common comensales of human skin and animals, some of them cause infections in some circumstances (Staphyoloc. epidermidis, warneri, haemolyticus, saprophyticus, hyicus) PC positive - Staphylococcus aureus, St. intermedius

G+cocci in clusters - gram staining

Cocci in clusters in fluorescein preparation

Growth characteristic – growing on salt media – staphylococci
Fermenting manitol –yellow – St. aureus vs. St.epidermidis

Staphylococcus aureus G+coccus • colonizes nasal passage and axillae• able to grow on salt medium (10%), catalase +, grows in
clusters, PC positive - distinguishing factor• Structure: capsule, peptidoglycan,protein A, teichooic acid,
clumping factor, cytoplasmic membrane• Toxins: alfa, beta, delta, gama, leukocidin, exfoliating,toxic
shock syndrome TSST,enterotoxin • Enzymes: coagulase, catalase, hyaluronidase,
staphylokinase, lipases, fibrinolysin, nuclease, penicilinase

Virulence factor and patogenesis• Multifactorial• adherence surface proteins (att.to fibronectin), fibrinogen/fibrin binding protein (att. to clots and traumatised cell, the most
important part of slime on biomaterial of indwelling devices), fibronectin• avoidance of host defence capsule polysaccharide, protein A - bind IgG - disruption of opsonisation, leukocidin - toxic for PMNL• damage of host tissue - toxins and enzymes

Toxíny• alfa - cytotoxický pre bb, rozrušuje bunkovú membránu a hladkú svalovinu
ciev, nekrotizujúci• beta - sfingomyelináza C, termolabilný, hydrolýza fosfolipidov, deštrukcia
tkaniva, tvorba abscesu• delta - termostabilný, cytolýza, detergentné vlastnosti• gamma - erytrocytolýza• leukocidín-zvyšovanie permeability a tvorba pórov v bb. membráne,
odolnosť voči fagocytóze• exfoliatívny toxín - zodpovedný za SSS – skin scaled sydrome, rozrušuje
medzibunkové spoje - dezmozómy v stratum granulosum kože, tvorba protektívnych protilátok - len u detí
• TSS-1 - vzniká pri raste u niektorých kmeňov St.aureus TSS – toxic shock syndrome – toxický šokový syndróm
• enterotoxíny - odolný voči hydrolýze žal. kyselinou, termostabilný, 5 typov A-E, B - pseudomembranózna kolitída, neurotoxín, hnačky a zvracanie

Enzýmy• Koaguláza - viazaná (fibrinogén - fibrín) a voľná (cez medziprodukty),
tvorba fibrínovej vrstvy a abscesu - ochrana pred fagocytózou• Kataláza - premena toxického H2O2 -- H2O + O2• Fibrinolyzín- stafylokináza - rozpúšťa fibrínový trombus• Lipáza - rôzne typy, prežívanie stafylokokov v seboroických oblastiach
- prenikanie do kože a podkožia, tvorba povrchových kožných infekcií• Hyaluronidáza - rozrušuje mukopolysacharidy v spojivovom tkanive,
šírenie• Nukleáza - termostabilný E• Penicilináza - beta laktamáza, enzým rozrušujúci betalaktámový kruh
PNC antibiotík

Klinické manifestácie infekcie spôsobenej St. aureus
• Koža – hnisavé ochorenie kože: vredy, abscesy, akné, karbunkul, impetigo,
• Systémové - endokarditída, pnuemónia,bakterémia, osteomyelitída, septická artritída, flebitídy, mastitídy, meningitída osteomyelitis, infekcia moč. mechúra
• Nozokomiálne infekcie a infekcie kože, katétrov, popálenín
• GIT infekcie – enterotoxín - zvracanie, hnačky
• TSS - toxic shock syndrom SSS - scalded skin syndrom
Hnisavé


Superantigen: enterotoxins and TSST
• TSST - exotoxin secreted during the growth of some strains, connected with superabsorbent tampons - fever, hypotension, shock, rash, desquamation, multi organ involvement TSST-1: 75% menstrual TSS., TSST-2 enterotoxin B and C: 50% non menstrual TSS
• Enterotoxins A-E- resistant to hydrolysing gastric enzymes and to heat 100*C (neurotoxin)
• Superantigen: superstimulation of T cells nonspecifically 1 of 5 cells instead of 1 of 10 000 with APC - cytokines released in large amounts - (any T cell with Vb element is stimulated)

Clinical manifestation of St.aureus
• Skin - stye, soil, carbuncule, impetigo, endocarditis, pnuemonia,
• General pyogenic Nosocomial and wound infection, infection of indwelling devices, burns, immunosuppression, phlebitis, mastitis,meningitis
• Toxic GIT infections - emesis, diarhea TSS - toxic shock syndrome SSS scalded skin syndrome osteomyelitis,

impetigo

folikulitis

carbuncul

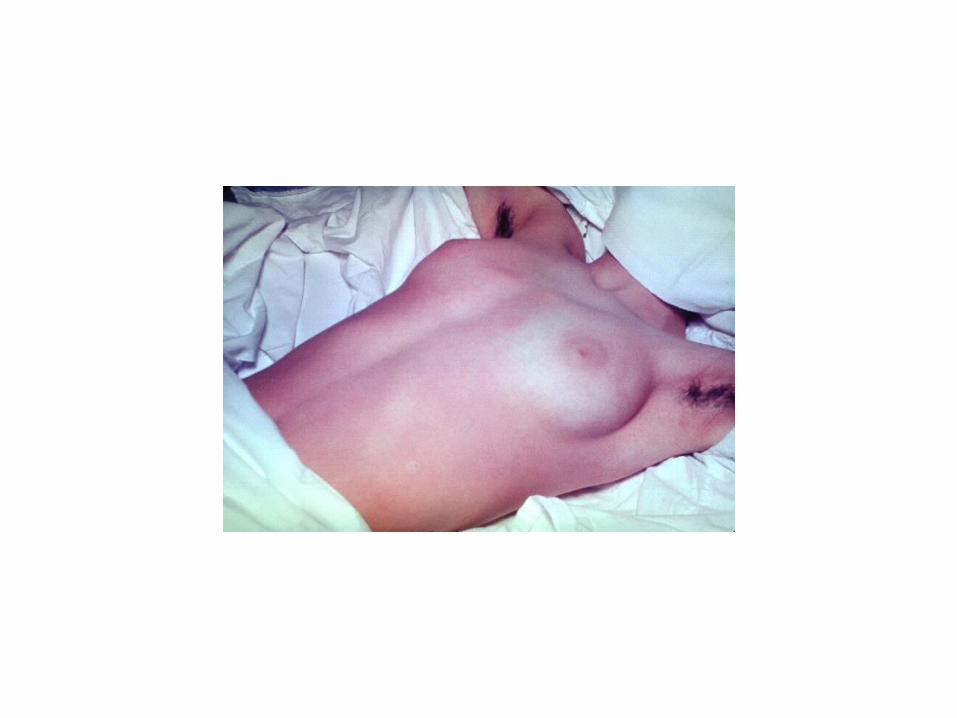
Stafylococcal scaled skin syndrom SSSS– Riter´s disease

St. epidermidis and other PC negative
• Infection of indwelling devices - catheter, shunt, artificial joint
• Infection of valve - artificial or damaged - endocarditis - indolent course - 1 year after surgery
• Staphylococcus saprophyticus - urinary infection of young sexually active women
• Contamination or ethiological agens

ATB susceptibility and resistance• Penicillin, staphylococal penicillin - oxacillin,
methicilin,TTC,CMP,ERY, KANA, GEN, STM, Fluorochinolony• Quick development of resistance : penicilinase• Now some strains are resistant to convential ATB• Hospital strains resistant to many ATB - including glycopeptides,
vancomycin, teicoplanin• MRSA - meticilin resistant St.aureus• VRSA - vancomycin resistant St.aureus - resistance transfered
from enterococci• St.epidermidis - - often meticilin resistant.

Nosocomial problem
• MRSA
• multiple resistance
• VRSA
• resistance to antiseptics and disinfectants
• Mechanism of resistance acquiring: 1)extrachromosomal plasmids, transposons or DNA insertion 2)mutation in chromosomal genes

G+cocci catalase negat.• Genus:
• Streptococcus:
• Enterococcus
• Aerococcus, Gemella, Lactococcus, Leuconostoc, Pediococcus - very rarely pathogenic in men


G+cocci, catalase negat.
• genus
• Streptococcus:
• Enterococcus
• Aerococcus, Gemella, Lactococcus, Leuconostoc, Pediococcus - seldom pathogenic for human

shapeG+cocci in chains or diplococci

Streptococcus - taxonomy and properties• Taxonomy
- according to haemolysis on blood agar : alfa - incomplete, beta - complete, gama - without haemolysis - according to serological groupes sc. Lancefield A-H, K-V, not all streptococci have this groupe specific antigen of cell wall
• A S. pyogenes bacitracin beta hemolysis• B S. agalactiae CAMP beta hemolysis• C S. anginosus beta, alfa• D S. bovis alfa, gama• - S. pneumoniae optochin + alfa• - S. salivarius optochin - alfa

Streptococcus alfa hemolysis• - S. pneumoniae optochin + alfa• - S. salivarius optochin - alfa• - Streptococcus beta hemolyticus Streptococcus alfa hemolyticus

Streptococcus – beta hemolyticus
A S. pyogenes beta hemolysis (bacitracín+)
B S. agalactiae beta hemolysis (CAMP)

Streptococcus sk A - pyogenes
• In bouillon long chains• Antigenic structure - capsule - hyaluronic acid -identical
with connective tissue - nonimunogennic• peptidoglycan• groupe and type specific antigens - -
most important M antigen - on the surface of fimbriae, virulence - T protein, R protein, F protein,
• lipoteichoic acid

Factors of patogenity and imunity
• Capsule nonimunogennic - inhibits phagocytosis
• M protein - protection against phagocytosis and cooperation with C´. Type 1,3,18 - invasive diseases., M3 a M18 - Rheumatic fever
• F protein - receptor for fibronectin (matrix of eukaryotic cells - adhesin
• Lipoteichoic acid - ?

Toxins• Exotoxins - erytrogenic toxin -termolabil, type A,B,C -
hypersensitivity, endotoxic, cytotoxic, non specific mitogen T and imunosupresive B lymfocytes activity, rash at scarlatina
• Dick´s, Schultz´s test• Streptolysin S - oxgen stabile, lysis of ery, releasing of lysosyme,
nonimunogen• Streptolysin O - reversibily inactivated by oxygen, imunogen,
antibodies against streptolysine O - ASLO, killing of leukocytes• Streptokinase - lysis of blood trombus, spread of bacteria• DN-ase - noncytolytic, depolymerisation of free DNA - in pus,
declines viscosity of pus, spread

Streptococcal infections
• Streptococcus pyogenes HSA - pharyngitis - dif dg. from viral - scarlat fever - pharyngitis with exanthem - infectious strain gained by lysogenic conversion ability to produce erytrogenic toxin (rash with desquamation of skin, circumoral whiteness, strawberry thongue) - toxic shock syndrome - cellulitis, necrotising fasciitis, hypotension, erytrodermia, multiorgan failure, bakteraemia, M1, M3, M18 - types - erysipelas, pyodermia - purulent skin diseases



Flesh eating streptococcus
Toxic shock syndrome – celulitís and necrotising faciitis - superantigen

Streptococcal infections- late sequelae
• Febris rheumatica - rheumatic fever - nonpurulent streptococcal disease - inflamatory disease of heart, joints, vessels and submucosis - autoimmune disease related to some serotypes of M protein ( types specific antigen, factor of patogenity, numbered M18, M3…) sequelae present only after respiratory infections. Not after skin infection
• Poststreptococcal acute glomerulonefritis - specific nefritogen strains, after skin and respiratory infections

Diagnosis - laboratory
• Microscopy - gram staine, G+ cocci in chains, not colonising skin, in skin swab together with leu - significant for disease. Of any value from URT sample
• Detection of antigens - directly from clinical material (also from URT), detection of groupe specific antigens of cell wall, specific, not sensitive - negative tests should be confirmed by cultivation
• Cultivation, Identification - hemolysis, bacitracin test• Antibodies - ASLO - confirmation of preliminary streptococcal
infection in patients with RF a GNF (+ anti Dnase antibodies

Streptococcus agalactiae, HSB• newborne infections (menginitis, pneumonia), puerperal -
postpartum sepsis /colonisation of URT, GIT and vagina - danger of contamination of newborne during prolonged and preterm labour, importance of maternal imunity/
• G+ cocci in chains, beta hemolysis, dif dg.from HSA - CAMP test - strenthened hemolysis of Staf. aureus - papillon
• Strukture - polysaccharid capsule, cell wall - peptidoglycan with type and groupe specific antigens and lipoteichoic acid, cell membran
• Antigenic strukture - antibody against capsule antigens are protective - diseases in newborne
• Enzymes - Dnase, hyase,protease, hemolysin

Other streptococci
• Beta hemolytical group C,F,G - URT and skin infections never late complications
• Viridant -alfa a nonhemolytical streptococci - Streptococcus salivarius, viridans - bacteremia, subacute endokarditis, caries, intraabdominal purulent infections
• Important condition for development of disease is the preliminary damage of tissu ( tooth, valve)
• Carries - formation of dextranu from glucose

Streptococcus pneumoniae• G+cocci in pairs, diplococcus, lancet shape - candle and flame,viridant
- dif.dg - positivity of optochin test, bile solubility test - colonies are dissolved by powdre bile
• encapsulated and nonencapsulated strains- polysaccharide capsule - factor of virulence - more than 90 serotypes based on capsule antigens peptidoglycan of cell wall typical for G+ cocci (N acetylmuramic and N acetyl glukosamin net), teichoic acid and cholin ( unique substance, important for cell division)
• 2 forms of teichoicacid in cell wall - surface (C substance) and covalently bound

STREPTOCOCCUS PNEUMONIAE
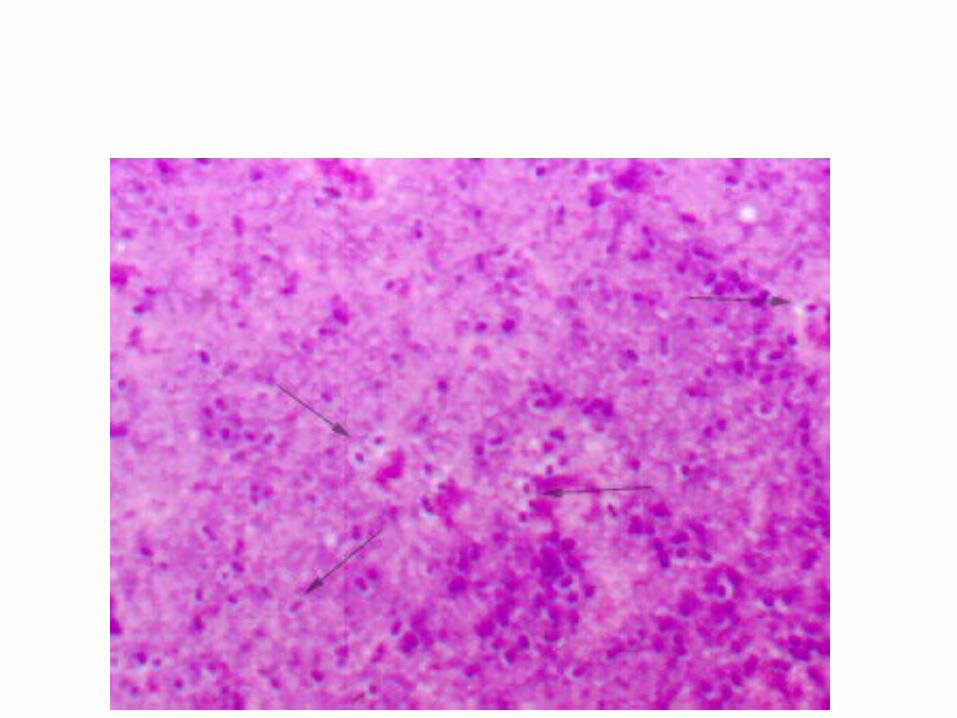
Streptococcus pneumoniae: Gram-positíve diplococcus 0.5-1.25 / um

STRUCTURE

G+ diplococcus in CSF fluorescent microscopy


Laboratry diagnosis
• CSM –- G-diplococci, leucocytes, antigen detection - latex agglutination in CSM, and urine Cultivation of CSM and blood - hemocultivation –
•
• ATB susceptibility

OCHORENIA SPOSOBENÉ STREPTOCOCCUS PNEUMONIAE
Neinvazívne
- Sínusitída
- Otitis media
- Pneumónia
Streptococcus pneumoniae diseases
Invazívne
- Bakteriémia
meningitída
endokarditída
peritonotída
septická artritída
iné (mäkké tkanivá)
Non encapsulate encapsulated
Localised Invasive
CRP
• CRP - C substance of str. pneumoniae - During bacterial infecions organism syntetises CRP - C reactive protein - protein of acute phase of inflammation, reacting with C substance of Str. pneumoniae

Streptococcus pneumoniae - infections
• Encapsulated strains - virulent - pneumo, (lobal, crupous -without ATB resolution after 14 days - crisis - production of anticapsular antibodies) meningitis, bakteremia - age predilection -in seniors (superinfection od viral infection of RT) and children up to 3 years ( imunologically defect, encapsulated strains T independent - protectiveantibodies ( 90 serotypes, vaccination, conjugated vaccines)
• Nonencapsulated strains - sinusitis, otitis media

KOLONIZÁCIA A PRENOS INFEKČNÉHO AGENS
nosičstvo sa môže vyskytnúť až u 60% detí predškolského veku a 30% dospelých
Nasofarynxmiesto kolonizácie
Trachea
Pacient s pneumokovou infekciou
Aerosol
Nosová dutina
Diseminácia
Inhalácia
Asymptomatický nosič

PATOGENÉZA
Otitis media
Nazofarynx
kolonizácia
Pneumónia
Bakterémia
Artritis Peritonitis
Meningitis
Sinusitis
! !
!
!
Neinvázne
Neopúzdrené kmene
Invázne
Opúzdrené kmene

ATB susceptibility
• Str. pyogenes - 100% susceptible for PNC, (in allergies macrolides ERY)
• Str. agalactiae - good susceptibility for PNC, some strains tolerate - inhibition, not resistence, resistence to ERY, TTC
• Str. salivarius - susceptible for PNC, • Str. pneumoniae - PNC, TTC, CMP, CEF., resistence for
PNC - multiresistence - decline of affinity of ATB to PBP

Enterococcus• G+ cocci, colonisisng in great quantities intestine and colon,
able to grow in the presence of bile - dif. dg. - esculin media• E. faecalis• E. faecium• urine tract infections, intraabdominal abscesses, bakteraemia• ATB nonbactericidal for enterococcie, resistence - synergic
therapia: aminoglykosides + cell wall acting• Resistence plasmid transferable - (on staphylococci too -
vancomycine)

G – Coccus

Praktical taxonomy
P ep tos trep tococcu sP ep tococcu s
S arc in aR u m in ococcu s
an aerob ic
G em ellaP ed iococcu sL eu con os tocL acotococcu s
S tap h ylococcu sM ic rococcu s
S trep tococcu sE n terococcu s
aerob ic
G +cocc i
N on -sp oreP rop ion ib ac teriu m
M ob ilu n cu sB ifid ob ac teriu m
C los trid iu m -sp ore
an aerob ic
L is te riaE rys ip e lo trixG ard n ere lla
B ac illu sC oryn eb ac teriu mA rcan ob ac teriu m
R h od ococcu s
aerob ic
G ram +rod s
G ram p os it ive
V e illon e llaM eg asp h oera
an aerob ic
N eisseriaM oraxe lla
B ran h am ella
aerob ic
G -cocc i
H aem op h ilu sL eg ion e llaB arton e llaE iken e lla ...
B ord ete llaP as teu re llaF ran c isce lla
B ru ce lla
E N TE R O B A C TE R IA C E A
N O N F E R M E N TE R SP seu d om on asA c in e tob ac ter
S ten otro fom on as ..... .
V ib rion aceaeC am p ylob ac ter
H elicob ac ter
aerob ic
L ep to trich aW olin e lla
B ac tero id esP orp h yrom on as
P revote llaF u sob ac teriu m
an aerob ic
G -rod s
lG ram n eg ative
B ac teria
Mycoplasma, Ureaplasma, ChlamydiaRicketsiaceae
Spirochetales - Spirochetes, Leptospira, BorreliaMycobacterium
Nocardia , Actinomycetes,
Miscellaneous
Family NeisseriacaeFamily Moraxellaceae - genera Branhamella,
Moraxella, Acinetobacter • Genus Neisseria• Species: N. meningitidis -colonisation of URT or
menigitis, setpicaemia- meningococcaemia - fulminant sepsis, pneumonia, arthritis N.gonorrhoeae - uretritis, cervicitis, salpingitis, proctitis, septicaemia, arthritis, conjunctivitis, pharyngitis, Pelvic inflamatory disease other neisseria - colonisation of mucous membranes and skin

Colonisation
Nasofarynxcolonisation
Pacient with the infection
AerosolInhalation
Asymptomatic carrier

PATOGENESIS
Nasopharynx
colonisationBakterémia
Meningococcaemia
Meningitis
!
Non encapsulated strains
Encapsulated strains
Colonisation
Invasion throught mucous membrane

Neisseria meningitis
• Encapsulated (polysaccharide capsule), G- diplococcus, coffee beans,
• Serogroups (13) - A - (1serotype), - B,C(several serotypes 20), -Y, W135… most frequent, 8 immunotypes

Neisseria meningitis• Pathogenicity:
colonisation of nasopharynx (pilli) - attachment to noncilliated cell of columnar epitel spread - escape to phagocytosis - antiphagocytic property of capsule toxic effect - endotoxin LPS - vascular damage (endothelial damage, inflamation of vessel wall, DIC, trombosis) - hyperproduction of membrane fragments in growing cells

Neisseria meningitis - clinical syndromes
• Meningitis - high mortality when not treated 100%• Meningococcemia - life-threatening,, trombosis of small
blood vessels, multiorgan invovement, petechiae, overwhelming disseminated intravascular coagulation with shock - destruction of adrenal glands- Waterhouse Friderichsen sy, - chronic septicaemia

Neisseria meningitis -therapy
• Therapy - PNC(genetic alteration of PBP ),CMP, cephalosporin,
• Eradication - (spread of strains) sulphonaminds, rifampicin
• Vaccination - A,C,Y,W vaccine - not for children under 2, conjugate vaccine - immunogenic for children, B vaccine - polysaccharide is weak immunogene

Neisseria meningitis - immunity
• Bactericidal antibodies(serogroup) (only in type B serotype ab are also protective) and complement - protective
• polysaccharide capsule - susceptibility of children under 3 years - T independent Ag
• susceptibility of infant after decline of maternal antibodies• Acquired immunity - 2 weeks after asymptomatic colonisation• Transmission by droplets, prolonged close contact (millitary,
crowded communities) • Sporadic and epidemic spread

Laboratory diagnosis
• CSF - Gram stain - G-diplococci, leucocytes, antigen detection - latex agglutination in CSF, urine
• cultivation of CSF and blood culture - chocolatised agar + 5%CO2, !not refrigerator! biochemical properties - dif dg. from other meisseria serogroupe typisation - agglutination,
• ATB susceptibility test
• from nasopharyngeal swab - dif. dg. from non pathogenic neisseria - biochemical test

Microscopy .Gram
Latex aglutination Ag
Cultivation
PCR


Sampling, transport
Thay Martin
Room temperature
Cultivation
Chocolate agar
Oxidase +
Neisseria gonorrhoeae• Most common sexually transmitted disease (STD) uretritis,
cervicitis, arthritis, conjunctivitis, local complications• G- diplococci, 5 different types of colonies (T1-5),
cytochromoxidase positivity, glucose fermentation• Structure: capsule, pilli - in virulent strains(T1,2) -
attachment, OMP - outer membrane protein- I.,II.,III, Iron binding protein - removal of iron from host cells - iron essential for metabolism of gonococci, LPS-endotoxin, protease, penicillinase

Pathogenesis and immunity• Attachment - pilli, penetration and multiplication and pssage
throughthe cells into subepitelial space. Nonpilliated are avirulent. Protein I interfere with neutrophil degranulation. Endotoxin - tissue destruction.
• IgG and C´: individuals with C´deficiencis are at increased risk for systemic disease.
• Only humans, asymptomatic reservoir• Multiple infections - lack of protective immunity -
antibodies against pilin protein - antigenic diversity

Clinical signs• Infection in men - uretritis+complication
• in women- cervicitis - ascending genital inf.
• Disseminated infection with septicaemia, skin, joints infections:(fever, artralgias-migratory,suppurative monoarthritis-wrist, knee, ankles, rash over extremities
• Perihepatitis, purulent conjunctivities in newborne, anorectal gonorrhoe in homosexual, pharyngitis
• Chemoprophylaxis - - ineffective

Cultivation +ATB• Neisseria gonorrhoe - PNC – penicilinase production
- chromosome type of resistence - changes in cell surface, - ceftriaxon. TTC, chinolons, makrolides - azitromycin – therapy of chlamydia infection
• Microscopy: Vagina swab in susp. gonorrhoe: - Gram staining: G - diplococci, coffee beans, epitelial cells., leukocytes. From culture colonies: G- diplococci
• Cultivation: Swab from vagina or discharge – on blood agar, modified blood agar, chocolate agar + ATB – inhibition of contaminating flora, Grey cololnies after application of cytocromoxidase – become black – slide sc. Gram, - biochemical tests for diff.dg. from other Neisseria

Genus:Bacillus - G+sporeforming bacilli, aerobic and facultatively anaerobic
• Bacillus anthracis,Bacillus cereus,Other Bacillus sp.• Bacillus cereus - 2 enterotoxins - heat stable -
emetic form - contaminated rice - heat resistant spores survive initial cooking that kills vegetative cells, germinate, multiply and toxin is not destroyed by reheting - heat labile - diarrheal form - adenylcyclase-cAMP system stimulation in intestinal cells - fluid accumulation -contaminated meat and vegetable - toxin is produced in situ, longer incubaion
• Panophthalmitis - traumatic eye infection (soil, penetrating object), complete loss, massive destruction - toxins - necrotic - heat labile enterotoxin -cereolysin -hemolysin - phospholipase C - lecithinase
• Ubiquitous, isolation witout symptoms = contamination• Other Bacillus - immunosupressed patients - shunt and catheter inf.
Bacillus anthracis• Spore and capsule not seen in clinical specimens• Antrax toxin - 3 antigenically distinct components: -protective Ag, lethal factor, edema
factor - alone not active, • Pathogenesis: capsule - antiphagocytic, Ab are not protective, toxins - protective + lethal or
edema f.• Human diseases - cutaneous - inoculation - painless papule, ulcer, necrosis
- inhalation - rapid progresive diffuse pulmonary involvement - respiratory failure - 95% mortality - gastrointestinal - ingestion - rare - mesenteric adenopathy, hemorrhage, ascites, 90% mortality
• Cultivation - on nonselective media, rapidly growing adherent colonies, no hemolysis, Non motility,liquifaction of agar Microscopy: caput medusae - serpentine chains,
• Therapy - PNC (TTC, CMP)., control of animal antrax, vaccination.

Non sporeforming G+ bacilli - heterogenous group
• Corynebacterium - coryneforms, diphtheroids- C. diphteriae (diphtheria), C. jeikeium (oportunistic). C. urealyticum(urinary tranct inf.), C. pseudodiphthericum (endocarditis), C. ulcerans (pharyngitis)
• Arcanobacterium haemolyticum - pharyngitis• Actinomyces - granulomatous ulcerative inf.• Rhodococcus - suppurative pneumonia, opportunistic• Listeria - meningitis, septicemia, granulomatosis infantiseptica• Erysipelothrix - erysipeloid, septicemia, endocarditis

Corynebacterium• Pleiomorphic G+ rod, arranging to short chains,
forming china letters• Metachromatic granules – the final colour is defferent
from original stain and from other parts of cell• Special cell wall structure – mesodiaminopimel acid,
mycolic acid – taxonomically near Mycobacteria• C. diphtheriae – preventable disease – inhalation –
asymptomatic carriage or disease• C. JL – jeikeium – opportunistic pathogen
hematological disorders

Pathogenesis
• Diphtheric toxin – tox gen – lysogenic conversion
• AB toxin – blacking protosynthesis – prolongation of peptid chain on ribosomes
• Schick skin test – detection of neutralisation antibodies when i-d appôicated diphtheria toxin

Lysogenic conversion
• Strain of C. diphtheriae gains his toxigenicity by lysogenic conversion - thanks to bacterophage. Bacterial virus - bactrophage is able to transfere genetic information about the production of toxin - tox gen - fom one cell ( toxigenic) to the other (non toxigenic) C. diphtheriae cell.

Enzymes
• Phospholipasa D – dermonecrotic toxin – spread – increasing of vascular permeability – C. ulcerans
• Urease – alkalinisation of urine calculi C. urealyticum
• ATB resistance – selection of resistent strains – C. urealyticum, C.JK – resistent to ATB used for urinary infections

Clinical syndromes• Diphtheria – depend on immunity and place of
infection – asymptomatic colonisastion. Mild infection or fulminant diphtheria
• Pseudomembrane on tonsils, pharynx, nose and general symptomes and complication (myocarditis)
• Skin diphtheria • Therapy –ATB .PNC, ERY – elimination of bacteria,
not threating intoxication, antitoxin, immunisation• Debacilisation of carrierers – • Protective immunity in skin forme

Lab. dg. of corynebacterium
• Diagnosis of the disease is based on clinical picture and epidemiological history. Lab. dg. is long and complicated Appropriate sampling
• Microscopy - smear with Gram staining and Albert´s staining does not distinguish between C. diphtheriae and other Corynebacteria.
• Cultivation: Blood agar - 3 typs od colonies - mitis, gravis, intermedius, Loffler´s medium, tellurit medium brown colonies with halo
• Biochemical identification- differentiation from other corynebacteria present in throat
• toxigenicity of the strain - ELEK,
• ATB susceptibility

Cultivation of Corynebacteria
• C. diphtheriae - blood agar
• C. pseudodiphthericum - blood agar, inverse CAMP
• C. diphtheriae on tellurit medium - brown colonies with brouwn ring - halo

Detection of toxigenicity of C. diphtheriae
• ELEK´s test of toxigenicity - imunodiffusion of suspension of tested strain and antidiphtheric serum in agar - zone of precipitation
• Annimal mode: application of diphtheria toxin i.d. ………………..necrosis
• antidiphtheric serum (i.p. or i.d.) + toxin …no necrosis
Arcanobacterium
• A.haemolyticum - colonise human, responsible for pharyngitis (+/- scarlet fever-like rash), cutaneusinf., endocarditis, meningitis - in older patients
• Missdiagnosed as Str. pyogenens, grows slowly, weak hemolysis
• 2 toxins - hemolysin and phospholipase D
• enzymes neuraminidase

Erysipelotrix• E. rusiopathiae: G+ non spore forming facultative anaerobic bacillus,
worldwide distribution in animals• Cultivation in reduced oxygen athmosphere, small grayish, alfa hemolytic
colonies, 2-3 days, sample from deep tissue or deep aspirates.• Erysipeloid - occupational disease (butchers, meat processors) after
subcutaneous innoculatio -localised skin infection -generalised cutaneous forme -septicaemia - associated with endocarditis (undamaged heart valve - aortic)
• Therapy PNC, ERY,CLI (sulfonamids, vancomycin, aminoglycosides - resistent)

Listeria

Rhodococcus• G+, obligate aerobic, red-pigmented, acid fast, mycolic acid.
Veterinary pathogen. Present in soil• Intracellular - surviving in macrophages• Granulomatous inflammation with abscess formation (lung,lymph
nodes, menings, pericardium, skin) - immnosupressed• Cultivation - nonselected media, aerobically, pigmented colonies
after 4 and more days• Therapy : prolonged - multiple ATB able to penetrate into
macrophages

Gardnerella• Morphologically resemples gram neganive bacilli, has cell wall structure
of gram +, nonmotile, not capsule• part of normal vaginal flora • present in bacterial vaginosis together with obligate anaerobes -
Mobiluncus, Peptostreptococcus,absence of Lactobacillus. Present in postpartum bacteremia, endometritis, vaginal abscesses
• Lab. dg. - simple isolation is not prooving, importance of microscopic examination - clue cells - epitelial cells covered with G variable bacilli (Gardnerella) and G- small curved bacilli (Mobiluncus), absence of G+ bacilli (Lactobacilli)
• Therapy: ampicilin, metronidasol

Nocardia• G+strictly aerobe rods. Similar to quickly growing mycobacteria,
saprophytes in environment. Acid fast., Mycolic acid• Nocardia asteroides, N. brasiliensis, N. madurae• pneumonia - with confluent abscess formation, exogenous inhalation• skin infection - A. brasilinensis - localised celulitis, purulent sinuses with
chronical granulomatous inflamation - mycetoms• Madurmycosis - chronical granulomatous infection of bone and soft
tissue, deformations, (Sudam, Northern Africa, East India)• diseminated - CNS - brain abscesses, in immunocompromised• Lab. Dg. - microscopy - modified Ziehl Neelsen, Gram +, cultivation -
standard media -2-30 days, colonies adherent to agar, cream, orange rose color, chalky consistence
• Therapy: surgery+ATB 3 months sulphonamids, amikacin, imipenem, broad spectrum to be effective if fungal ethiology

Lectures 3,4,
• Anaerobes
• Enterobacteriacea
• Vibrionaceae
• Campylobacter
• Helicobacter

Anaerobe gram + sporulating rods• Clostridia - 100 species, some are aerotolerant - C. histolyticum some looks
lide G-. Commonly present in soil, water, GIT
• C. perfringens - Bacteraemia, myonecrosis - gas gangren, infection of soft tissu, necrotising enteritis
• C. tetani - tetanus
• C. botulinum - botulismus - infant, wound, food intoxication.
• C. difficile - pseudomembranous colitis connected with ATB, 2 toxins, part of FMF, exposition to ATB kills other colon flora - overgrowth of C. difficile
• C. septicum - not injury connected myonecrosis, patients imunodepresed - Ca of colon - interruption of colon wall integrity and spread of Clostridium to tissues

Clostridium tetani• Motile rod, sporulating, G+ often looks like G-. Very sensitive to oxygen,
metabolically poorly active.
• Heat labile neurotoxin- tetanospasmin - released after lysis of cell. AB toxin - block of neurotransmmiters in CNS on inhibitory synapses - not regulated excitationon synapses - spastic paralysis
• present in soil, GiT. Vegetative forms are sensitive to oxygen. Spores survive for years
• Generalised tetanus, localised tetanus, tetanus of new bornes - drug abusers tetanus
• Therapy - PNC, antitoxin, - toxin bound on nerve endings is protected and cannot be neutralised. Symptomatic therapy
• Vaccination
• Lab dg. - toxin detection - annimal model, microcopy - G+rod with spores terminally located - enlarging the rod

Clostridium botulinum• Heterogenous group of nutritionally requiring sporulating bacteria 4 groups I - IV based on
proteolytical activities and type of toxin. 7 antigenically different botulo toxins A,B,C alfa, D, E, F, G - A,B,E most frquent. AB toxin , heat labile - 20minút /80*C
• blocking neuromuscular transmition on synapies of periferal nerves.• After consumption of contaminated food, cans., wound botulismus or infant botulismus
after honey consumption in infant less than 1 year.• Blurred vission, dilated pupils, dry tongue, constipation, aches, flacid palsy - complete
recovery after years. Wound botulismus - very rare Children botulismus- 1976 - in vivo production of neurotoxin from colon colonisating clostridia (in 6m - 1y of age) - progresive flacid palsy, - mortality 1% - often attributed to other reasons( SIDS)
• Dg. - clinical, detection of clostridia and toxin Th. - antitoxin, PNC- destruction of spores and prevention of germinating of spores

Clostridium perfringens• Colonisation of serious disease, hemolysis, biochemical activity. Production of letal toxins
(alfa, beta, epsilon, iota, heatlabile enterotoxin) with life threating biological effect and ensymes. Types A-E: A v in environment, B-E in colon. A gas gangrene and intoxikcation, C necrotising enteritis
• Bacteraemia - often not significant, transient from contaminant from skin. Gas gangrene - life threating, histotoxic clostridium, after injury, very painful, devitalised tissue with gas production. (C.
septicum, histolyticum, novyi) Celullitis, fasciitis - after wound colonisation - often not significant - or very progresive destruction ( C. septicum) Necrotising enteritis - intestine, type C, 50% lethal Intoxiction from food - short incubation time, watery diarhea - ingestion of contaminated food, toxin - heat labile protein
• Microscopy - G+rod withou leu from clinical material Th - surgery, high dose of PNC, antitoxin, hyperbaric chamber

G+rods anaerobes• Not sporulating -
Actinomycetaceae Actionomyces israeli, A.naeslundii ---cerebral, cerevicofacial, abdominal actinomycosis, chronic purulent disease with abscess formation. Lab.dg. Samplling from depth of sinuses, sulphur
granules, colonies in shape of tooth - molar, requiring and long cultivation, Th: surgery +ATB prolonged PNC -Propionibacteriaceae Propionibacterium acnes --- colonisation of skin, external ear, conjunctive.
Opportunistic infection in patients with foreign bodies. Lab. dg. On common media - anaerobe -Mobiluncus ---gram variable, morphology of G+, requiring cultivation, colonisation of genital tract of women - vaginosis - defect of eubiosis, overgrowth - not inflamatory
disease -Bifidobacteriaceae, Eubacteriaceae,- Lactobacillaceae . -part of FMF of GIT, femal genitals
• Sporulating - strictly anaerobe, spores, tykpicall situated, proteolytical properties, production of toxins,
intoxikcation, anaerobe injurie Clostridium botulinum, C. tetani, C. septicum,C. novyi

G-rods anaerobe• Bacteroides fragilis - obligate anaerobe rods, not sporulating, important
part of FMF in oropharynx, UGT, GIT. - pleuropneumonia, intraabdominal abscess, genital infection. Endogenous a polymicrobe infections, formation of abscess in destruction of barieres. Lab.dg. strict anaerobe sampling and cultivation and transport , stimulation of growth in 20% of bile. Th surgery + ATB, - production of betalactamase, Metronidazol
• B. stearothermophilus- sporesy used for testing of effectivity of sterilisers
• Prevotella, Porphyromonas, Fusobacterium, Leptotricha, Wolinella

G+cocci anaerobe• Peptostreptococcus, -Peptococcus,- Sarcina, -
Coprococcus, - Ruminococcus -colonising skin and mucous membrane of GIT, UGT, oportunistic pathogens often in connection with foreign bodies, requiring cultivation, slowly growing - pleuropneumonia after aspiration, sinusitis, brain abscess, spread from orofarynx or lungs, intraabdominal infection and sepsis spread from colon, pelvic infection (endometriis, abscess, sepsis, vaginosis) infection of soft tissue (celulitis), endocarditis, osteomyelitis
• Lab.dg - differenciation from colonnising flora, transport and sampling under anaerobe condition, prolonged cultivation
• Th - PNC, cefalosporins, imipenem, CMP - often polymicrobial ethiology.

• G-koky anaeróbne• Veillonella, Megasphera -present in orofarynx, low
virulence, in cultivation and diseases usually present in mixture

Physiology and structure of Enterobacteriaceae
• G- rods, usually motile (flagella, not spore forming, facultative anaerobes, nutritionally not requiring, biochemical active catalase +, oxidase -, cytochromoxidase COX - = dif.dg.from Pseudomonadaceae
• Lactose fermentation + or -, rezistence to bile salts, capsule - dif.dg from other Enterobacteriaceae
• 3 types of antigens:
• - somatic O antigen - most important cell wall ag, heatstabile, LPS lipopoly saccharide consists of 3 parts - O polysaccharide, core polysaccharide and lipid A - with endotoxin activity
• - capsular K antige - heatlabile cross reacting with antibodies against other bacteria. In Salmonella typhi under name of Vi antigen
• - flagellar H antigen - heatlabile, antigen and phase variation

Biological effect of endotoxin• Part of G- bacteria cell wall - released after its destruction - by
ATB• Fever• leukopaenia followed by leukocytosis• activation of complement• Thrombocytopaenia• Disseminated intravascular coagulopathy DIC• decreased periferal circulation and perfussion of big organs• shock

E. coli• Present in GIT• causes - endogennous infections after breaking of immune barieres from physiological flora ( z
focus in UGT or GIT, most important cause of G- sepses), Infection of urinary tract (most out patients infections - rises from GIT strains, specific serotypes binding with specific adhesis to epitel receptors), - gastroenteritis - neonatal meningitis
• enterotoxigen ETEC - production of heatstabile and heat labile toxin, mild water diarhoea, travellers diarhoea,
• enteroinvsive EIEC - spread to epithelial cell of the colon, destruction of epithel, fever, blood and leu in stool, Confirmation of invasivness - Sereny´s test - innoculation of strain do conjunctiva of annimal- results in inflamation enteropathogenic EPEC - serious child diarhoea , shiga-like toxin, able to adhere to erytrocytes
• enterohemorhagi EHEC - production of verotoxin. From non complicated diarhoea to
hemorhagic colitis and . Hemolytic-uremic sy - type 0157:H7, - acute kidney insufficiency, trombocytopaenia, in children under do 5 r.

Salmonella• 1500 serotypes, different names according to place of identification• DNA analysis = 1 species (S. enterica) and its 7 subgroupes• Present in annimals, spread by contaminnated food - primary from
contaminated annimal products - eggs - salmonella disease of hens. Secondary - from carrier or patients. Need of big innoculun 106-8 - spread by food where it can multiply
• Salmonellosis - enteritis - infection of colon, fever, nausea, vomiting, headaches. Dg.: Stool sample 3 x consecutively. Lactose negative colonies, biochemical identifiction. Serotyping by slide agglutination according to Kauffmann White scheme - epidemiological purposes (S. enteritidis, S. infantis, S. agona, S. kentucky…………………….)

Salmonella typhi• Typhoid fevers - fever with deterioration - systemic disease -
penetration to lamina propria, lymphatic nodes, RES (multiplication in hepari - spread via bile vesicle to intestine - , spleen, bone marrow), blood - bakteraemia, exanthem - roseola, fever, headache. GIT symptomes not always present - perforation . Carriage of Salmonella.
• Dg. - sample of stool, repeated after stimulation by MgSO4. Typical lood of cultivation. Serotypisation by slide agglutination. Detection of antibodies Vidal reaction. Vi agglutintiona
• Th. - CMP• Salmonella paratyphi A, B, C - Typhus like, milder

Shigella• 4 species - Sh. dysenteriae, Sh. flexneri, Sh. boydii, Sh. sonnei a
38 serotypes• Dysentheria - watery diarhoea with blood, often epidemic,
transmitted with contaminated hands. Surviving in water 6 months. Small infectious dosis - 200 bacteria. Disease of small intestine first withou invasion. Production of enterotoxin - invasion and destruction of epitel, ulcers formation - pus and blood in stool
• Dg. Based on biochemical activity - characteristics of cultivation - without smell, not gas, lactose negative. Serotype differenciation - slide agglutination

Yersinia• 7 species - Y.pestis, Y. pseudotuberculosis, Y. enterocolitica, + oportunistic
Yersíniae
• Y. pestis - plague - urban and forest type, not GIT disease. Adapted to i.c. parasitismus, not surviving in nature. Virulence factors - i.c. surviving, , polysaccharide capsule, endotoxin, . Urban plague - circulating between rats, transmitted by insect to man during rodent bacteraemia. Replication in colon of insect and transmission to other rodent or man is on by chance. Forest pôague - Not controlled.
• 2 clinical formes - bubonic - 7 days after biting by insect - painful lymphadenopathy75% lethality - pneumonic - 2 days after inhalation - fever, pneumonia, inhalation spread by droptets, epidemia letality 90%

Yersinia enterocolitica• Enterocolitis in colder environment, most activity in
22*C, food borne infection, diarrhoea, fever. Chronic disease - terminal ileum, mesenteritis immitation of appendicitis. Extraintestinal symptomes - arthritis, hepatitis, osteomyelitis -
• Dg. - cultivation or serology by agglutination in extraintestinal sy
• blood borne infection - bacteraemia and endotoxic shock (blood cans - cooled)

Klebsiella
• G- rod with typical structure• Encapsulated– mucous look of colonies - increased
virulence, notmotile• Klebsiella pneumoniae – pneumonia in patients not able
to clean from bronchial stroma and lungs the aspirate Necrotic destrukction of alveols. Bloody sputum. Infection of tissue and urinary tract
• K. rhinoscleromatis - sclerom• K. ozaenae – atrofic disease of nose musous membrane

Vibrionaceae• G- curved rods aerobe and anaerobe growth. Present in water• Oxidase test – posit. – diff. Dg from Enterobakteriaceae• V.cholerae - gastroenteritis• V. parahaemolyticus - gastroenteritis• V. vulnificans – bakteraemia, infection of wound, celullitis –
exposition to contaminated water, GIT – row sea fruits• V. alginolyticus – infection of wound and soft tissue, otitis externa• Other vibrias – infection of wound and moderate GIT infections• Plesiomonas – GIT infections from raw sea fruits• Aeromonas – opportunistic (…pijavice, after microsurgery)

V. cholerae• Growing in 18* - 37*C• Serologically – 6 groups based on O antigen (patogennic are O1)• Vibrio cholerae O1 – 2 biotypes – el tor a cholerae and each present in
2 serologic subgroupes – ogawa a inaba• Adherence, not invasive. • Production of AB toxin – cholera enterotoxin – binding on specific
receptors of intestin, causing secretion of Na, K a bicarbonate to lumen – liquid lost - 1 liter in hr. (hypovolaemia, arythmia, kidney insufficiency). Not adhering bacteria are avirulentné
• In waters of Asia, human carriage and sea annimals. Spread by contaminated water and food. Necessity of big innoculum – 103-5. Less in condition of patients achlorhydria ( 104 bacteria after bicarbonate)

Diagnosis and therapy of Vibrio• Microscopy – small, motile – native smear or darkfield• Cultivation – selective media – not supporting acid
environment and drying– enriche alkalin buillon pH 8,6• Dif. dg. V. cholerae a other vibiras
(halofile, requiring 1%NaCl)• Therapia V. cholerae – ATB for debacilisation only,
exotoxinu. (TTC,ERY, CMP, COT)., symptomatic - solution replacement V. parahemolyticus – mild disease, would infection – ATB – TTC)

CampylobacterComma shape, G-, motile, 11 species,7 subspeciesRequiring microaerophil defined environment, 42*C, passing
through bacterial filters - selective isoloation Campylobacter jejuni – gastroenteritis in patients with decreased
immunity –hypogamaglobulinemia, decreased acidity of stomac liquid. Infection of epitel of jejunum, ileum and colon results in oedematous , bloody mucus with abscess formation.Infiltration to lamina propria. Enterotoxin, cytopatic toxin, endotoxin. Poultry, food neutralising pH reduced infection dosis.
C.coli - gastroenteritis, C. fetus – septicaemia, artritis, trombophlebitis, meningitis
Lab dg.: cultivation on selective media, microscopy - of stool - leu, antigen detection, Th.: ERY

Helicobacter• Spiral rods, G-, in connection with gastritis, gastric and
duodenal ulcer, susp.Ca – Gastrospirillum hominis• Pathogenesis – production of urease – formation of cloud
of NH4, that protects bacteria from acid in stomac - motility - mucinase formation – spread to mucous layer - adherence – attachment to intracelular junction – inflamation with mononuclear infiltration in lamina propria.Escape to IgA specific antibodies because of its location in mucous layer
• Interhuman transmission• Th. ATB . Bismuth, nitroimidasol a amoxicilin or TTC

Laboratory diagnosis• Biopsy taken during endoscopy: Microscopy –
hematoxylin eosin staining, Gram staaining. ! Desinfection and contamination of endoscopic devices
• Detection of alkalic metabolits of urease activity. Rapid testt – 1-2 hrs – from bioptic material or breath test
• Cultivation - from bioptic material – enrichee media – blood, haemin, charcoal - problems: activity of inhibition caused by desinfection of endoscopes
• Serology: Detection of IgA ! Interpretation – prolonged presence not discriminating between acute and pass infection.