Embed Size (px)
Citation preview

No. 10 May 2006Civil Justice Report
Medical Malpractice Awards, Insurance, and Negligence: Which Are Related?
Alexander Tabarrok Department of Economics, George Mason University
and
Amanda Agan Department of Economics, George Mason University
C E N T E R F O R L E G A L P O L I C YA T T H E M A N H A T T A N I N S T I T U T E
C L P

Civil Justice Report
May 20062

Medical Malpractice Awards, Insurance, and Negligence: Which Are Related?
May 2006 �
Table of ConTenTs
AbOuT ThE AuThORs .............................................................................................................................I
ExECuTIvE summARY ............................................................................................................................III
INTROduCTION .......................................................................................................................................1
mALPRACTICE PREmIums ANd AwARds ACROss TImE ...........................................................2
Figure 1: Premiums Track Awards Over Time ...................................................................................2
mEdICAL mALPRACTICE AwARds ANd PREmIums ACROss ThE sTATEs .............................4
Figure 2: Medical Malpractice Awards Per Doctor...........................................................................4
Figure 3: Premiums Are Higher in States with Higher Awards Per Doctor.....................................5
PROFITEERING, GREEd, ANd GOuGING? ....................................................................................6
Figure 4: Premiums Are Lower in States with Higher Concentration Ratios ..................................7
whAT’s dRIvING AwARds ..............................................................................................................6
Table 1: Explaining Variation in Awards and Claims Per Doctor .....................................................8
AN ALTERNATIvE mEThOd FOR dETERmINING mALPRACTICE...............................................9
Figure 5: The Tort System and the Review System Are Not Highly Correlated ...........................11
CONCLusION .........................................................................................................................................12
REFERENCEs ..............................................................................................................................................i
REGREssION APPENdIx .......................................................................................................................iii
COINTEGRATION ............................................................................................................................iii
Table A1 ..............................................................................................................................................iii
PREmIums ANd AwARds ...............................................................................................................iii
Table A2: Premiums Are Higher in States with Higher Awards Per Doctor ................................... iv
PREmIums ANd CONCENTRATION RATIOs ................................................................................ iv
Table A3: Higher Concentration Rates Lower Insurance Premiums .............................................. iv
muLTIPLE REGREssION: PREmIums, AwARds, CONCENTRATION RATIOs ANd PCFs .......v
Table A4: Premiums Are Higher in States with Higher Awards Per Doctor, Multiple Regression ............................................................................................................................v
AdvERsE ACTIONs PER dOCTOR .................................................................................................vi
Table A5: Variation in Adverse Actions Per Doctor is Not Associated with Percent Below Poverty Level or Partisan Judicial Elections ...........................................................vi
Table A6: Means and Standard Deviations .....................................................................................vii

Civil Justice Report
May 2006�

Medical Malpractice Awards, Insurance, and Negligence: Which Are Related?
May 2006 I
abouT The auThors
ALEXANDER TABARROK is associate professor of economics at George Mason University and director of research for The Independent Institute. His recent book (with Eric Helland), Judge and Jury: American Tort Law on Trial, examines issues such as how race and poverty impact trial decisions by juries, how judges compare to juries when awarding damages, and the influence of judicial electoral systems on the decisions of judges. Professor Tabarrok is also the editor of the books Entrepreneurial Economics: Bright Ideas from the Dismal Science, The Voluntary City: Choice, Community, and Civil Society (with David Beito and Peter Gordon), and Changing the Guard: Private Prisons and the Control of Crime. His papers have appeared in the Journal of Law and Economics, Public Choice, Economic Inquiry, the Journal of Health Economics, the Journal of Theoretical Politics, The American Law and Economics Review, Kyklos, and many other journals.
Popular articles by Professor Tabarrok have appeared in magazines and newspapers throughout the United States. He writes regularly for the blog, Marginal Revolution.
AMANDA AGAN conducts research on law, crime, housing, and other topics at George Mason University, where she also studies economics.

Civil Justice Report
May 2006II

Medical Malpractice Awards, Insurance, and Negligence: Which Are Related?
May 2006 III
exeCuTive summary
Doctors’ medical malpractice liability insurance premiums are at an all-time high. As has been widely reported in the press, escalating med-mal premiums have driven doctors to retire early, shut down their businesses, or reduce the scope of their practices. In areas of the country with particularly high premiums, there is concern that patients’ access to care has been compromised.
Insurance companies and most doctors conclude that the root cause of higher insurance costs is higher tort awards. The American Medical Association, for example, says that medical liability reform is their top priority because “rapidly increasing medical liability insurance premiums caused by esca-lating jury awards are seriously threatening patient access to care.”
On the other side of this debate are plaintiffs’ attorneys and their allied consumer groups who attribute the boom and bust “insurance cycle” to investment returns and, alternatively, accuse insurance companies of “price gouging.” Such claims are often picked up, uncritically, by the main-stream press.
Our study makes four contributions to this debate:
1. We show that medical malpractice premiums are closely related to medical malpractice tort awards. Over the long run, premiums closely track awards, and premiums adjust to short-run award variation as well. Indeed, insurance companies’ short-run reaction to award levels is the primary driver of the so-called insurance cycle. In addition, med-mal premiums are closely related to tort awards across states. The correlation in premiums and awards across the states suggests strongly that tort award levels, not investment returns, are the primary explanatory factor for changes in insurance premiums, since investment returns are unlikely to vary markedly across states.
2. We show that medical malpractice premiums are not explained by insurance industry price gouging. For the price-gouging hypothesis to make sense, insurance industries must be exercising monopoly power. Looking at insurance industry �-firm concentration ratios—a measure of market power—we find that states with more concentrated insurance industries actually have lower premiums, even when controlling for other explanatory factors.
�. We show that medical malpractice tort awards are related to some factors not rationally related to injuries. For instance, states’ judicial electoral systems have predictive value on the expected level of tort award.
�. We show that malpractice tort awards and thus insurance premiums can vary dramati-cally for reasons having little or nothing to do with negligence. We reach this conclusion through a novel test of the tort system, in which we compare awards and rates of determi-nation of negligence in the tort system with rates determined by the independent medical board review system. Although board review outcomes are imperfect, they are biased, if at all, against findings of negligence, because physicians will not allow frivolous complaints to result in disciplinary actions. The tort system shows no or even a slight negative cor-relation with the board review system’s negligence determinations, suggesting that the system is influenced by factors not related to negligence.

Civil Justice Report
May 2006IV

Medical Malpractice Awards, Insurance, and Negligence: Which Are Related?
May 2006 1
mediCal malpraCTiCe awards, insuranCe, and negligenCe: whiCh are relaTed?
IntroductIon
Medical malpractice premiums are at an all-time high.1 The American Medical Association (AMA) says that at least twenty states are experiencing full-blown liability crises, with twenty-two more show-ing signs of serious problems.2 Under pressure from the tort system some doctors have retired early, shut down their businesses, or reduced the scope of their practices.� The U.S. Department of Health and Human Services says that the liability crisis is threatening access to care and jeopardizing patient safety.�
What is behind the recent increase in premiums? On one side of the debate are insurers and doc-tors, who attribute the increase to higher malpractice tort awards. On the other side are attorneys and their allied consumer groups, who typically claim that insurers are exercising monopoly power to make up for investment losses due to poor planning in the boom of the 1990s. Such claims are often picked up, uncritically, by the mainstream press. For example, writing last year in The New York Times, Joseph Treaster and Joel Brinkley argued that “legal costs do not seem to be at the root of the recent increase in malpractice insurance premiums,” which they attributed instead to the “nature of competition in the industry.”5
We make four contributions to this debate. First, we show that medical malpractice premiums are closely related to medical malpractice awards through time and across the states. Second, we show that premiums are not explained by insurance industry monopoly power. Third, given our findings that malpractice insurance premiums are determined by tort awards, and that such awards vary substantially across the states, we ask what factors determine award variation. For example, are states with high awards and premiums like teenagers who face high auto insurance premiums because of high accident rates, or are awards and premiums high because of factors not rationally related to underlying risks? We show that awards are related to some factors (such as judicial electoral systems) not rationally related to injuries. Finally, in a novel test of the tort system, we compare awards and rates of determination of negligence in the tort system with rates determined by the independent board review system. The test results suggest that awards and thus insurance premiums can vary dramatically for reasons having little or nothing to do with negligence.
1. See Congressional Budget Office (200�); Medical Liability Monitor (200�). 2. See American Medical Association (2006).�. For some anecdotal evidence, see U.S. Dept. of Health and Human Services (2002). Baker (2005) offers a con-
trary but balanced discussion. Kessler et al. (2005), Encinosa and Hellinger (2005), Helland and Showalter (2006), and Klick and Stratmann (2005) estimate the effect of liability on physician entry and exit decisions.
�. See U.S. Dept. of Health and Human Services (2002), pp. 2-�.5. Treaster and Brinkley (2005); see also Americans for Insurance Reform (2002). Baicker and Chandra (2005) say,
“[I]ncreases in malpractice payments do not seem to be the driving force behind increases in premiums” (p. �1).

Civil Justice Report
May 20062
050
0010
000
1975 1985 1995 2005Year
020
0040
0060
00A
war
ds/
Pay
out
s
2000
4000
6000
8000
1000
012
000
1975 1985 1995 2005Year
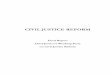
Premiums Track Awards Over Time
Premiums Awards/Payouts Premiums Awards/Payouts
FIgure one
MalpractIce preMIuMs and awards across tIMe
In their New York Times article, Treaster and Brinkley (2005) use a graph, shown as the left graph in Figure One, that they claim supports their position that medical malpractice premiums have “outpaced the rise in payments for claims.” The graph does indeed show that premiums are more variable than awards/payouts and thus may increase (or decrease) in some periods faster than awards. But this fact is not inconsistent with the idea that awards drive premiums. We can demonstrate the latter point most easily by rescaling the axes to overlay the two lines, as shown in the right graph. The rescaling has two virtues. First, the graph used in The New York Times encourages a naïve interpretation that the distance between the premiums and awards line represents profits. In fact, the graph does not show the administrative and legal costs of settling claims and defending cases that do not win, so one cannot draw any conclusions about profits from the graph. Second, and more important, the rescaled graph makes it easier to see that premiums oscillate around awards: sometimes the premium line is above the award line and sometimes it is below; but over time, the two lines move in tandem.
To test the proposition that malpractice premiums followed awards over time, we performed a “cointegration test” on the data used to create the New York Times graph, which came from the insur-ance rating agency A.M. Best.This statistical analysis demonstrated that premiums and awards are “cointegrated,” that is, linked in a stable long-run relationship.6 We also note that the data confirm that variations in awards drive premiums. The reason is that whenever two variables are cointegrated,
6. The cointegration test formally demonstrates the stable long-run relationship between premiums and awards, which exists although neither premiums nor awards show any tendency to return to their own means over time.

Medical Malpractice Awards, Insurance, and Negligence: Which Are Related?
May 2006 �
there is an associated error-correction mechanism that determines what happens when the two vari-ables depart from their long-run relationship. In this case, the theoretical error-correction mechanism is easy to see: if premiums in the insurance industry long exceed awards (plus expenses), competition will drive premiums down; and if premiums long fall below awards (plus expenses), bankruptcy, exit, and survival behavior will drive premiums up. Thus, premiums should adjust to awards. And because awards are determined by tort law and judge and jury behavior, there is little reason to believe that awards will adjust to premiums. Looking at the data, we see exactly this result in the error-correction mechanism: premiums respond rapidly to changes in awards but awards do not respond to changes in premiums.7
Premiums track awards in the long run but may depart from awards in the short run. This variation does not necessarily imply that factors other than awards are important determinants of premiums in the short run. Today’s premiums must cover future awards, which are unknown. As a result, insurance firms set today’s premiums based upon their forecast of future awards. The cointegration test mentioned above showed that there is no tendency for medical malpractice awards to fluctuate around a fixed mean, so past awards are not very useful for predicting future awards. Awards from a decade ago, for example, probably tell us very little about awards in the next decade. The most useful awards for predicting future awards are the most recent ones, especially if these suggest a permanent change in the level of awards. By definition, there aren’t many recent awards. Thus, insurance companies have a very difficult job: they must forecast future awards using only a few data points. Forecasts under these conditions can be highly variable, even more variable than the series being forecast.8 Short-term depar-tures of premiums from awards, therefore, should be expected even when awards drive premiums.
Plaintiffs’ lawyers and “consumer advocacy” groups often blame periodic liability crises on the “insurance cycle” rather than on changes in tort awards. A group called Americans for Insurance Re-form (AIR) is representative of this line of thinking:
Not only has there been no real increase [in] lawsuits, jury awards or any tort system costs at any time during the last three decades, but the astronomical premium increases that some doctors have been charged during periodic insurance “crises” over this time period are in exact sync with the economic cycle of the insurance industry, driven by interest rates and investments. In other words, insurance companies raise rates when they are seeking ways to make up for declining interest rates and market-based invest-ment losses.9
But tort awards and the insurance cycle are not competing explanations for increases in premiums. As described above, the insurance cycle itself is a consequence of the unpredictability of tort awards.10 Thus, trying to dampen premiums by regulating other things—J. Robert Hunter, director of Insurance for the Consumer Federation of America, urges state regulators to “enforce the ratings laws in order to end the boom and bust swing”—is likely to be futile.11 The best way to reduce the volatility of premiums is to reduce the volatility of awards. The more predictable future tort awards are, the more predictable insurance premiums will be.
7. See the Regression Appendix for details.8. For a formal proof of this proposition, see Kleidon (1986). Industry forecasts of losses are often incorrect, il-
lustrating the difficulty in forecasting.9. AIR (2002). For a critique of AIR’s statements and studies, see Frank and Grace (2006). 10. Other factors, such as changes in interest rates and the long time lag between premiums and payouts, amplify
the cycle, but it is the underlying uncertainty in awards that is the driver of the cycle. 11. J. Robert Hunter, quoted in AIR (2006).

Civil Justice Report
May 2006�
MedIcal MalpractIce awards and preMIuMs across the states
We can factor out much of the short-run variability in premiums and awards across time by looking at the relationship across the states at a single point in time. Figure Two is a map of mean malpractice awards per doctor per year (averaged over 1999-2001). States with high mean awards are in green, and states with low awards are in gray. The variation in the average award per doctor is surprisingly large: mean awards range from a low of $1,688 in Wisconsin to a high of $10,025 in Pennsylvania.12 It is highly doubtful that medical errors and malpractice are six times more common and egregious in Pennyslvania than in Wisconsin. Later we examine whether factors related to patients or physicians can explain these striking differences.
FIgure two
$1,658—2,878$2,878—3,388$3,388—4,488$4,488—5,418$5,418—6,597$6,597—10,025
Medical Malpractice Awards Per DoctorUnited States 1999-2001 Average
0
0 100 Km
100 Miles
HAWAII
0 500 Miles
0 500 Km
ALASKA
12. The effect of interest rates on the so-called insurance cycle is a national-level phenomenon, so the fact that awards vary significantly across the states is strong evidence that the insurance cycle alone, as interpreted by consumer groups, leaves much variation in awards to be explained.

Medical Malpractice Awards, Insurance, and Negligence: Which Are Related?
May 2006 5
FIgure three
The large variation in awards lets us test whether variation in awards is associated with variation in premiums. Figure Three graphs awards per doctor against premiums and finds a strong positive association.1�
States with higher awards per doctor, simply put, have higher insurance premiums. This positive relationship remains even after we control for other variables that may affect insurance premiums in a given state, such as the �-firm concentration ratio, the number of medical malpractice cases per doctor, and whether a state has a patient compensation fund (see Regression Appendix, Table A�).
1�. Data on medical malpractice premiums are usually calculated on a state level. In some states, the Medical Li-ability Monitor breaks the data down into somewhat finer geographic regions. Where this is done, one also often finds a strong relationship between awards and rates. Bovbjerg and Bartow (200�) take a detailed look at Pennsylvania, for example, and note: “The highest Pennsylvania rates (usually in Philadelphia) are about double the lowest rates for any given insurer” (p.1�). They also examine tort awards and note “the special case of Philadelphia,” where “2�% of verdicts awarded [are] in excess of $1 million.” (p.�2). Note also that Philadelphia has the highest poverty rate of any county in Pennsylvania; see Helland and Tabarrok (200�) and below for the importance of this fact.
010
000
2000
030
000
4000
050
000
Med
-Mal
Insu
ranc
e P
rem
ium
s ($
)
2000 4000 6000 8000 10000
Awards Per Doctor
Premiums Are Higher in States withHigher Awards Per Doctor

Civil Justice Report
May 20066
1�. Quoted in Center for Justice and Democracy (2005).15. Id.16. In a competitive market, sellers have no pricing power but must accept the market price, which equals long-
run average cost. If prices exceed long-run average cost, new entrants will compete away excess profits until prices are driven back to that level.
proFIteerIng, greed, and gougIng?
In addition to blaming recent spikes in medical malpractice premiums on the “insurance cycle,” trial lawyers and their advocates are wont to accuse medical malpractice insurers of “illegal pricing.” Connecticut attorney general Richard Blumenthal calls for “more aggressive oversight to prevent and punish profiteering”:
Federal and state regulators should thoroughly scrutinize recent rate increases and take appropriate corrective action. Affordable medical malpractice insurance is critical to public health. Expensive insurance rates become a matter of life and death when they drive doctors out of business—as is happening in Connecticut … Insurance company greed can be hazardous to our health.1�
Echoing Blumenthal, AIR’s J. Robert Hunter argues that “insurance companies are price-gouging their doctors.” 15
A necessary condition for so-called price gouging is lack of competition.16 If price gouging is a problem, therefore, we should find that prices are higher when there is less competition. To test the price-gouging hypothesis, we calculated a measure of competition by state, the “�-firm concentration ratio.” A �-firm concentration ratio of 60 percent, for example, means that together the largest four firms have a 60 percent market share. If lack of competition is driving up rates, we should find a positive relationship between medical malpractice premiums and the concentration ratio.
Figure Four on the following page shows that, in contrast to the prediction of the price-gouging hypothesis, medical malpractice premiums decrease as the concentration ratio increases. Although the negative relationship is not strong, we certainly do not find the positive relationship that we would expect from the price-gouging hypothesis. Again, this negative relationship between medical malprac-tice premiums and the insurance industry concentration ratio holds, even after controlling for awards and patient compensation funds (see Regression Appendix, Table A�).
what’s drIvIng awards?
If medical malpractice awards are the major source of changes in insurance premiums, it is impor-tant to understand the factors that drive awards. If awards are primarily driven by factors that bear a rational relationship to medical malpractice, the fact that awards are higher in some states than in others may simply show that the tort system is functioning properly. But if awards are higher in some states than in others for reasons having little to do with medical malpractice, we may question whether the tort system is doing its job. If awards vary for reasons other than malpractice, for example, they cannot be acting as a deterrent, nor can they be providing just compensation.
We test whether awards vary due to variations in true malpractice rates in two ways. First, we look directly at whether variation can be explained by variables such as income per capita or infant mortality, variables that might plausibly be related to malpractice awards or rates, or whether awards are more affected by factors that are less plausibly related to true malpractice. Second, we conduct a novel test of the tort system by comparing it with the medical review system.
Medical malpractice awards per doctor can be high for two reasons: either the average award per claim is very high; or there are many claims per doctor (or both). Breaking medical malpractice awards

Medical Malpractice Awards, Insurance, and Negligence: Which Are Related?
May 2006 7
per doctor into two components, the award per claim and the number of claims per doctor, is useful: some variables may affect awards and others the number of claims.17
With only fifty states, the number of variables that we can examine is limited (because the number of data points limits what statisticians call “degrees of freedom”). Thus, we focus on the few that we think are most likely to be important or that have previously been shown to be important in the literature. We include the death rate and the infant mortality rate in our data. Although deaths are not necessarily indicative of malpractice, it is likely that awards will be higher in cases involving death—and deaths may, in themselves, encourage litigation. We include the percentage of people below the poverty level because Helland and Tabarrok (200�, 2006) find that awards increase dramatically in relation to county poverty rates. As county poverty rates increase from 0-5 percent to 20-25 percent, for example, Helland and Tabarrok find that the average award triples from $�00,000 to $1.2 million.18 Similarly, Helland and Tabarrok (2002, 2006) find that awards are higher against out-of-state defendants in states using partisan judicial elections, so we include partisan elections as a potentially important variable.19 (Both of the latter effects will be harder to pick up in state data than in the more disaggregated data used in
010
000
2000
030
000
4000
05 0
000
Med
-Mal
Insu
ranc
e P
rem
ium
s ($
)
40 50 60 70 80 90
Concentration Ratio
Premiums Are Lower in States withHigher Concentration Ratios
FIgure Four
17. Let MMPerDoc denote the mean malpractice award per doctor then MMPerDoc=Awards/Doctors=Awards/Claims*Claims/Doctors.
18. One can see the same effect within states. See note 11 and Bovbjerg and Bartow (200�), for example. 19. Helland and Tabarrok argue that elected judges are likely to be biased towards plaintiffs when the defendant
is an out-of-state corporation because the plaintiff is a constituent while the defendant is not.

Civil Justice Report
May 20068
the cited papers.) Finally, awards are likely to be higher in states with higher per-capita income, for the simple reason that economic damages will by definition be higher, all else being equal. The results are presented in Table 1.
table 1: explaInIng varIatIon In awards and claIMs per doctor
Award Per Claim Claims Per Doctor
Death Rate Per 1,000 10,399 0.001 (5,636)* (0.001)
Infant Mortality (Deaths Per 1,000 Live Births) 895 -0.0003 (5,321) (0.001)
Percent Below Poverty Level -20 0.0014 (3,141) (0.0006)**
Partisan Electoral System for Judges 35,905 -0.003 (18,691)* (0.003)
Personal Income Per Capita 9.2 0.0004 (2.3)*** (0.0004)
Constant -146,581 -0.006 (101,312) (0.019)
Observations 50 50
R-squared 0.43 0.16
Standard errors in parentheses * significant at 10% ** significant at 5% *** significant at 1%
Focusing first on the mean award per claim, we find that an increase in the death rate of one per 1,000 (slightly smaller than one standard deviation) increases the mean award by $10,000. The infant mortality rate appears to have no effect on the mean award per claim, nor does the percentage of the population living below the poverty level. States that use partisan elections to select their judges, however, have awards per claim on average $�5,000 higher (about 18 percent) than states using other methods to select their judges. As expected, awards also increase in relation to per-capita income. An increase of $�,000 in per-capita income (just over one standard deviation) increases awards by ap-proximately $�6,000.
Turning to claims per doctor, we find that the only statistically significant relationship is that in-creases in the percentage of the population living below the poverty level are correlated with increases in the number of claims per doctor. The effect is surprisingly large: an increase of one percentage point in the poverty rate (one-third of one standard deviation) increases the number of claims per doctor by approximately 6 percent.20
The regression results are a mixed bag for our perspective on the tort system. Some of the variation in awards per claim can be explained by factors that rationally relate to awards, such as income per
20. An increase of .001� claims per doctor compared to the mean claims per doctor of .02� is approximately 6 percent. (Running claims per doctor in logs produces a coefficient of 6.6 percent.)

Medical Malpractice Awards, Insurance, and Negligence: Which Are Related?
May 2006 9
capita and the death rate. But factors bearing little relationship to malpractice—such as whether a state uses partisan elections to select its judges—appear to be at least as important. The R-squared statistic indicates that the variables in the regression can explain only �� percent of the variation in awards per claim, so a majority of the variation in awards remains unexplained, which is even more the case in the claims per doctor regression, where we can explain only 16 percent of the variation.
an alternatIve Method For deterMInIng MalpractIce
To further test the efficacy of the tort system, we examine a parallel, independent, much less studied system for determining whether medical malpractice has been committed. Every state has a medical review board that investigates and disciplines physicians who have allegedly violated professional codes of conduct or the law. Patients and others can make a complaint to the board alleging medical negligence or conduct potentially leading to negligence (such as being under the influence of alcohol or drugs). Patients and others, including coworkers and employees, can also report physicians to the board for sexual misconduct, excessive or improper drug prescriptions, and billing fraud.21
After a complaint is filed to the medical review board, it is investigated; the exact procedure var-ies by state, but most follow a similar process. Complaints are assigned to a trained professional who investigates the case, determines the facts, and (for cases with sufficient merit) prepares material for a panel to judge. Medical board investigators, unlike attorneys in medical malpractice lawsuits, do not represent the patient or the physician but are intended to be impartial. Should the case pass the initial review, it is forwarded to a committee made up of physicians and laypeople for a decision regarding disciplinary action.
The medical board has significant authority to discipline physicians, including the authority to suspend, revoke, or limit a physician’s license to practice medicine. Under threat of revocation, the board can require physicians to submit to a competency exam that may lead to probation, monitoring, and mandatory retraining. Medical boards can also issue fines. In extreme cases, a medical board will refer cases to the local district attorney for criminal review.
Complaints to medical review boards that lead to disciplinary action must be reported to the Na-tional Practitioner Data Bank, where these types of reports are known as “adverse actions.” Between 1999 and 2001, almost 12,000 adverse actions were reported to the NPDB. Censure, probation, suspen-sion, and revocation of license or clinical privileges constituted just over 50 percent of the disciplinary actions taken. We will use these data to compare the review system with the tort system.
The medical review board system for determining negligence differs in a number of ways from the tort system. In two respects, the medical review system may be an inferior method of determining negligence:
n Even if investigators are trained to be independent, the medical review system is dominated by physicians, who may be reluctant to penalize other physicians.
n Medical boards do not have the authority to award damages to the victim. They can only discipline physicians. As a result, injured patients have fewer monetary incentives to com-plain than to sue.
21. In Virginia, for example, the most common allegations include “substandard care, diversion of prescription drugs for illegal purposes, improper prescribing, sexual misconduct, improper advertising, inadequate record keep-ing, unsanitary conditions and unprofessional conduct.” For more information, see the website for the medical board of Virginia: http://www.dhp.state.va.us/Enforcement/enf_DisciplineProcess; for New York: http://www.health.state.ny.us/nysdoh/opmc/understd2.htm; and for California: http://www.medbd.ca.gov/Complaint_Info.htm.

Civil Justice Report
May 200610
These potential problems, however, must be evaluated alongside several advantages of the review system:
n Complaints are cheap, and lawsuits are expensive. As a result, the review system may capture more negligent actions than the tort system.
n It’s difficult to sue if there is no injury. Complaints, however, can occur without injuries. A physician who abuses alcohol, for example, may have his license revoked even if no injury has yet occurred.
n Medical boards can take very serious disciplinary action, such as revoking a physician’s license. Such actions can be more serious than even a multimillion-dollar tort award, espe-cially given that physicians can insure against a tort award but not license revocation.
n Since suits are expensive, they are only brought for the most serious injuries. The medical review system may be especially likely, therefore, to discover problems before they lead to serious injury.
n In the tort system, only the affected parties may sue, but complaints against physicians can come from parties other than the patient, including concerned citizens, employers and employees, and other health-care professionals. In fact, health-care professionals are usually required to report physicians whom they suspect to be guilty of misconduct.
When the above factors are balanced, it is not obvious that the medical review system will under-state malpractice. Further research on that issue would be valuable. For our purposes, we do not need to make this determination; what we are interested in is how well the review system correlates with true malpractice.
The medical review system might, in theory, understate malpractice. But, by the same reasoning, when a physician is disciplined by a review board, we can be confident that the offending action was serious. As a result, malpractice as determined by the medical review system ought to correlate well with true malpractice—even if it understates the level of malpractice. Assume, for example, that the medical review system uncovers only one out of every three serious cases of malpractice. Neverthe-less, states with a great deal of malpractice as determined by review boards will also be states with a great deal of true malpractice—just at a higher absolute level.22 This argument suggests a test of the tort system.
The review system is likely to correlate well with true malpractice (because physicians will not allow frivolous complaints to result in disciplinary actions); if the tort system works well, it will also correlate with true malpractice and thus with the review system. If the tort system works poorly, however, it will not correlate with true malpractice or with the review system. Thus, we can test the quality of the tort system by examining whether states with high levels of review-board-determined malpractice also
22. We acknowledge that states may vary in the vigor with which they enforce review board claims. As such, high malpractice levels as measured by review boards may reflect different enforcement levels and, over time, lower actual malpractice. To capture fully the interplay between malpractice levels and board outcomes would require further study, such as a cross-sectional, time-series look at review board outcomes. For our present purposes, it is sufficient to note that at any given point in time, we would expect that high levels of malpractice actions enforced by state review boards should correlate with higher tort claims or awards, particularly for the most serious malpractice findings, if the tort system’s outcomes are consistent with true malpractice.

Medical Malpractice Awards, Insurance, and Negligence: Which Are Related?
May 2006 11
play host to large numbers of malpractice torts.Our test finds that the tort system and review system do not correlate. Figure Five shows that ad-
verse actions per doctor in the medical review board system do not correlate with the number of medi-cal malpractice cases per doctor in the tort system, nor do they correlate with the average award per doctor. Because not all adverse actions necessarily imply substandard care—billing fraud, for example, is not directly causative of poor care, even if one suspects that there might be a behavioral link—we conduct separate analyses for all review board adverse actions and those most likely to be associated with malpractice.2� Column 1 of Figure Five looks at the correlation between all adverse actions and medical malpractice cases (row 1) and awards (row 2); and column 2 looks at the correlation between those adverse actions most likely to affect actual medical performance and malpractice claims (row 1) and awards (row 2).
0.0
05.0
1.0
15.0
2
Ad
vers
e A
ctio
ns P
er D
oc
.01 .02 .03 .04 .05MM Claims Per Doctor
All Adverse Actions
0.0
02.0
04.0
06
Ad
vers
e A
ctio
ns P
er D
oc
.01 .02 .03 .04 .05MM Claims Per Doctor
AAs most related to Malpractice
0.0
05.0
1.0
15.0
2
Ad
vers
e A
ctio
ns P
er D
oc
2000 4000 6000 8000 10000Award per Doctor
All Adverse Actions
0.0
02.0
04.0
06
Ad
vers
e A
ctio
ns P
er D
oc
2000 4000 6000 8000 10000Award per Doctor
AAs most related to Malpractice
The Tort System and the Review System AreNot Highly Correlated
FIgure FIve
2�. Adverse actions most likely to be associated with malpractice include alcohol abuse, narcotics violations, unprofessional conduct, incompetence, negligence, patient abuse or neglect, and allowing unlicensed persons to practice.

Civil Justice Report
May 200612
In no case is the correlation large; in some cases, it is actually slightly negative. What these results indicate is that the two systems we have for determining malpractice, the tort system and the medical review system, result in very different determinations of malpractice. Surely, one of them is wrong!
One suggestive finding comparing the two systems is that adverse actions per doctor do not cor-relate at all with any of the political factors such as partisan elections or the percent of persons living below the poverty level that do correlate with tort awards.2� Determining in greater detail the relative errors and faults of the two systems, however, is an important area for future research.
conclusIon
The recent spike in medical malpractice premiums has generated many claims about the cause, ranging from insurance cycles to price gouging. A common theme seems to pervade these claims: the idea that premiums are reacting to something other than awards. Our results, in contrast, support the common sense idea that premiums are driven primarily by awards. The cointegration test shows that premiums track awards in the long run. Premiums also track tort awards across the states; premiums are higher in states that have higher awards. Other theories do not fit the facts: medical malpractice premiums, for example, are actually slightly lower in states with higher concentration ratios, which would not hold true if price gouging were the problem.
If awards are a major influence on premiums, it is important to understand what drives awards. Our analysis showed that some factors plausibly related to the incidence, extent, or cost of medical malpractice are related to awards—awards increase in states with higher income per capita and higher death rates, for example. But awards also appear to be related to factors not plausibly related to mal-practice, such as partisan judicial elections. Even accounting for all these variables leaves a large amount of unexplained variation across states in average medical malpractice awards.
As a further test of the medical liability system’s effectiveness, we also compared the tort system with the medical review board system for determining medical malpractice. While both systems help determine medical malpractice, they have different methods of doing so. Regardless of their differences, if the tort system were working well, we would expect that the number of adverse actions would be correlated with the number of medical malpractice claims. We find, quite to the contrary, that there is little correlation between the two, and what correlation exists is slightly negative. Whether the medical review board system could or should substitute for the tort system is a question for further research.
2�. See the Regression Appendix for details.

Medical Malpractice Awards, Insurance, and Negligence: Which Are Related?
May 2006 i
reFerences
Americans for Insurance Reform (AIR). 2002. “Medical Malpractice Insurance: Stable Losses/Un-stable Rates.” Available online at http://www.centerjd.org/air/StableLosses.pdf.
---------. 2006. “New Report Confirms: Medical Malpractice Insurance Crisis is Over.” Available online at: http://www.centerjd.org/air/pr/060227.pdf.
American Medical Association. 2006. “America’s Medical Liability Crisis: A National View.” Avail-able online at: http://www.ama-assn.org/ama/noindex/category/11871.html.
Baicker, Katherine, and Amitabh Chandra. 2005. “Defensive Medicine and Disappearing Doctors?” Regulation 28 (Fall): 2�-�1.
Baker, Tom. 2005. The Medical Malpractice Myth. University of Chicago Press.
Bovbjerg, Randall R., and Anna Bartow. 200�. “Understanding Pennsylvania’s Medical Malpractice Crisis.” Pew Project on Liability Reform. Available online at: http://medliabilitypa.org/research/ report060�/UnderstandingReport.pdf.
Center for Justice and Democracy. 2005. “Two Leading State Attorneys General and State Insur-ance Commissioner Strongly Challenge the Insurance Industry’s Price-Gouging of Doctors—Call for Oversight” (July). Available online at: http://www.centerjd.org/press/release/050707.htm.
Congressional Budget Office. 200�. “Economic and Budget Brief: Limiting Tort Liability for Medical Malpractice.” Available online at: http://www.cbo.gov/showdoc.cfm?index=�968&sequence=0.
Demsetz, Harold. 197�. “Industry Structure, Market Rivalry, and Public Policy.” Journal of Law and Economics, (April): 1-9.
Encinosa, William, and Fred Hellinger. 2005. “Have State Caps on Malpractice Awards Increased the Supply of Physicians?” Health Affairs 2�: 250-59.
Frank, Ted, and Martin Grace. 2006. “Faulty Studies from Center for Justice & Democracy Are Stunting the Medical-Malpractice Debate.” AEI Liability Outlook 2 (April).
Helland, Eric, and Mark H. Showalter. 2006. “The Impact of Liability on the Physician Labor Market.” Working Paper, Claremont-McKenna College Department of Economics.
Helland, Eric, and Alexander Tabarrok. 2006. Judge and Jury: American Tort Law on Trial. Indepen-dent Institute.
---------. 200�. “Race, Poverty, and American Tort Awards: Evidence from Three Datasets.” The Journal of Legal Studies �2 (2): 27-58
---------. 2002. “The Effect of Electoral Institutions on Tort Awards.” American Law and Economics Review � (2): ��1-70.
Kessler, Daniel P., William M. Sage, and David J. Becker. 2005. “Impact of Malpractice Reforms on the Supply of Physician Services.” JAMA 29�: 2618-2625.
Kleidon, Allan W. 1986. “Variance Bounds Tests and Stock Price Valuation Models.” Journal of Politi-cal Economy 9� (October): 95�-1001.
Klick, Jonathan and Thomas Stratmann. 2005. “Does Medical Malpractice Reform Help States Retain Physicians and Does It Matter?” http://ssrn.com/abstract=870�92.
Medical Liability Monitor. 200�. Medical Liability Monitor 29, no. 10: 1.

Civil Justice Report
May 2006ii
Sloan, Frank A., et al. 2005. “Public Medical Malpractice Insurance: An Analysis of State-Operated Patient Compensation Funds.” DePaul Law Review 5�, no. 2: 2�7-276.
Treaster, Joseph, and Joel Brinkley. 2005. “Behind Those Medical Malpractice Rates.” The New York Times (February 22).
U.S. Department of Health and Human Services. 2002. “Confronting the New Health Care Crisis: Improving Health Care quality and Lower Costs by Fixing our Medical Liability System.” Available online at: http://aspe.hhs.gov/daltcp/reports/litrefm.htm.

Medical Malpractice Awards, Insurance, and Negligence: Which Are Related?
May 2006 iii
regression appendix
coIntegratIon
The cointegrating equation is Awards (DLP) - .859 Premiums (DPW) (.10�) with details as shown in the following table.
table a1
Equation Parms chi2 P>chi2
_ce1 1 69.00807 0.0000
Identification: beta is exactly identified Johansen normalization restriction imposed
beta Coef. Std. Err. z P>| z | [95% Conf. Interval]
_ce1 DLP 1 . . . . . DPW -.8596209 .1034802 -8.31 0.000 -1.062438 -.6568036 _cons 2492.02 . . . . .
The key terms in the error-correction representation (not shown) are .08 Awards (.05�) and .�077 Pre-miums (.112) (standard errors in parentheses). The larger coefficient on the latter relative to the former indicates that it is premiums that adjust to awards. There are also lags of each term in the ECM. Details are available upon request.
preMIuMs and awards
Table A2 is the regression represented in Figure Three. It shows that higher medical malpractice awards are associated with higher medical malpractice premiums, just as we would expect from basic eco-nomic analysis. A one-dollar increase in awards is associated with an increase in insurance premiums of $2.89. In the long run we expect a one-to-one relationship between awards and premiums, which is exactly what we found in the cointegration analysis. The greater than one-to-one relationship we found here could be due to unmodeled factors or factors specific to the 1999-2001 period. Using data on individual-level physician malpractice premiums and an estimated measure of individual liability, Helland and Showalter (2006) show that premiums increase one-to-one with awards.

Civil Justice Report
May 2006iv
table a2: preMIuMs are hIgher In states wIth hIgher awards per doctors
Insurance Premiums
Awards Per Doctor 2.897 (0.555)**
Constant 6,640.557 (2,769.690)*
Observations 50
R-squared 0.36
Standard errors in parentheses * significant at 5%; ** significant at 1%
preMIuMs and concentratIon ratIos
Table A� is the regression represented in Figure Four. It shows, contrary to the price-gouging hypothesis, that states with higher concentration ratios tend to have lower insurance premiums. A ten-percent-age-point increase in the concentration ratio is associated with a decrease in insurance premiums of $2,5�0, or about a 1� percent decrease evaluated at the mean insurance premium. The negative rela-tionship between prices and the concentration ratio is consistent with Demsetz’s (197�) argument that efficient firms lower prices and increase their market shares. Wal-Mart, for example, dominates many markets because of its lower prices. Although the relationship is consistent with Demsetz’s efficiency argument, our goal here is merely to point out that this relationship is prima facie evidence against the price-gouging hypothesis.
table a3: hIgher concentratIon rates lower Insurance preMIuMs
Insurance Premiums
4-Firm Concentration Ratio -254.537 (112.647)*
Constant 38,017.323 (8,070.791)**
Observations 50
R-squared 0.10
Standard errors in parentheses * significant at 5%; ** significant at 1%

Medical Malpractice Awards, Insurance, and Negligence: Which Are Related?
May 2006 v
MultIple regressIon: preMIuMs, awards, concentratIon ratIos and pcFs
Table A� demonstrates that we get similar results to those graphed when we include awards per doctor, the �-firm concentration ratio, and whether a state has a patient compensation fund (PCF) together in a multiple regression.
Four states have mandatory PCFs: Pennsylvania, Indiana, Kansas, and New Mexico. For a fee, these funds provide excess professional liability insurance to those in the medical profession. The fees were added to the rates reported by various insurance companies in the MLM data so that we are compar-ing what physicians pay in total for $1m/$�m worth of liability insurance in each state. The negative coefficient on the variable indicates that total fees are lower in states with PCFs. One explanation is that fees in states with PCFs are underpriced. Pennylvania long underpriced insurance, for example, and then had to catch up with surcharges and, more recently, through subsidiziation of rates by taxpayers. In New Mexico there is no current subsidy, but in 200� the Department of Insurance issued a report indicating that the PCF was underfunded, thus suggesting that taxpayers could be called upon to take up some of the burden in the future.25 (See Sloan et al. (2005) for more on PCFs.)
table a4: preMIuMs are hIgher In states wIth hIgher awards per doctors, MultIple regressIon
Insurance Premiums
Awards Per Doctor 2.801 (0.515)**
4-Firm Concentration Ratio -220.714 (87.807)*
Patient Compensation Fund -5,278.284 (2,657.307)
Constant 23,548.193 (6,907.875)**
Observations 50
R-squared 0.48
Standard errors in parentheses significant at 5%; ** significant at 1%
25. Another potential explanation is that we have underestimated average PCF fees. In the MLM price data, rates are broken down into internal medicine, general surgery, and OB/Gyn. PCF fee charges are broken down much more specifically, with many more specialties. We chose the fee rate that best matched either internal medicine, general surgery, or OB/Gyn, and made sure that these fees would follow the trend that internists pay the least and OB/Gyns the most.

Civil Justice Report
May 2006vi
adverse actIons per doctor
Table A5 presents the results mentioned in the text, that unlike tort awards adverse actions per doctor do not correlate with political factors such as partisan elections or the percent below the poverty level.
table a5: varIatIon In adverse actIons per doctor Is not assocIated wIth percent below poverty level or partIsan JudIcIal electIons
Adverse Actions Per Doctor
Personal Income Per Capita 1998 -2.55e-07 (1.84e-07)
Death Rate Per 1,000 in 2000 -0.00022 (0.00045)
Infant Mortality, Deaths Per 1000 Live Births 2002 -0.00023 (0.00042)
Percent Below Poverty Level 0.00015 (0.00025)
Partisan Electoral System -0.0018 (0.0014)
Constant 0.015 (0.008)*
Observations 50
R-squared 0.13
Standard errors in parentheses * significant at 10%; ** significant at 5%; *** significant at 1%

Medical Malpractice Awards, Insurance, and Negligence: Which Are Related?
May 2006 vii
table a6: Means and standard devIatIons
Mean Standard Deviation
Medical Malpractice Claims (1999-2001) 1,046.6 1,467.3
Medical Malpractice Insurance Premium (1999-2001) 20,001.9 9,226.9
Internal Medicine 8,145.9 4,482.4
General Surgery 27,019.8 1,3242.1
OB/Gyn 44,672.9 21,537.6
Award Per Doctor (1999-2001) 4,612.0 1,915.6
Award Per Claim (1999-2001) 198,759.1 55,946.9
Claims Per Doctor (1999-2001) 0.024 0.009
Adverse Actions (1999-2001) 236.4 269.6
Concentration Ratio 70.8 11.2
Death Rate Per 1,000 (2000) 8.9 1.3
Infant Mortality (Deaths Per 1,000 live births) (2000) 7.0 1.5
Percent Below Poverty Level (1999) 11.9 0.1
Personal Income Per Capita (1998) 26,030.3 3,776.6
Patient Compensation Fund 0.16
Partisan Electoral System for Judges 0.2

Director
James R. CoplandFellows
Peter w. huberwalter K. Olson
Would you prefer to receive this publication via e-mail? If so, please supply us with your e-mail address by con-tacting us at [email protected] or 212-599-7000. Previous publications are also available.
The mission of the Center for Legal Policy (CLP) is to advance reform of the civil justice system through offering incisive, rigorous, and sound analysis of the problems, as well as effective, practical solutions.
CLP sponsors a series of books written by senior fellows Peter huber and walter Olson, such as The Litigation Explosion, Judging science, The Excuse Factory, and hard Green. These interesting and accessible publications have established CLP fellows as leading national authorities who communicate as much to the layperson as to senior policy makers. In addition, the CLP hosts conferences, lectures, and luncheon forums designed to present critical legal reform issues to a prominent and diverse audience of legal scholars, attorneys, industry representatives, and media. The CLP publications are the Civil Justice Report, which publishes innovative legal research by prominent scholars, and the Civil Justice Forum, which publishes transcripts from CLP events. The CLP also publishes Trial Lawyers, Inc. reports that examine the size, scope, and inner workings of America’s lawsuit industry and the PointOfLaw.com web magazine that brings together information and opinion on the u.s. litigation system.
The manhattan Institute is a 501(C)(3) nonprofit organization. Contributions are tax-deductible to the fullest extent of the law. EIN #13-2912529
M A N H A T T A N I N S T I T U T E F O R P O L I C Y R E S E A R C H
M
52 Vanderbilt Avenue • New York, NY 10017www.manhattan-institute.org
INon-Profit
OrganizationUS Postage
PAIDPermit 04001
New York, NY